Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Autoimmune Polyendocrinopathy Induced by an Antibody (KN046) That Simultaneously Inhibits PD-L1 and CTLA-4: A Case Report and Literature Review
Authors Li M ![]() , Wu C, Liu Y, Zhang R
, Wu C, Liu Y, Zhang R ![]() , Yang Q, Shi Z, Sun W, Hu X
, Yang Q, Shi Z, Sun W, Hu X
Received 4 January 2022
Accepted for publication 6 April 2022
Published 22 April 2022 Volume 2022:15 Pages 1253—1260
DOI https://doi.org/10.2147/DMSO.S353403
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Min Li,* Chenchen Wu,* Yan Liu, Ranran Zhang, Qingqing Yang, Zhaoming Shi, Weihua Sun, Xiaolei Hu
Department of Endocrinology, The First Affiliated Hospital of Bengbu Medical College, Bengbu, Anhui Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaolei Hu, Department of endocrinology, The First Affiliated Hospital of Bengbu Medical College, No. 287 Changhuai Road, Bengbu, Anhui Province, 233000, People’s Republic of China, Tel +8613855216339, Email [email protected]
Abstract: Endocrine adverse reactions are one of the most common adverse reactions in the treatment of immune checkpoint inhibitors (ICIs), mainly involving the pituitary gland, pancreas, thyroid gland, adrenal gland and other glands, resulting in corresponding endocrine dysfunction. We report a 45-year-old man with non-small-cell lung cancer who developed hypophysitis 11 months after initiation of treatment with an anti-PD-L1/CTLA-4 bispecific antibody (KN046) that blocks both programmed death ligand-1 (PD-L1) and cytotoxic T-lymphocyte antigen-4 (CTLA-4), followed by regular oral replacement doses of prednisone and levothyroxine tablets. The patient was diagnosed with type 1 diabetes mellitus (T1DM) with diabetic ketoacidosis (DKA) 25 months after the start of immunotherapy, presenting with acute hyperglycemic symptoms, ketoacidosis, and negative diabetic autoantibodies. By describing a case of KN046 immunotherapy involving multiple endocrine glands and reviewing relevant literature, we were able to summarize the clinical characteristics of KN046 immunotherapy-induced endocrine system-related immune-related adverse events (irAEs) for use in early detection, diagnosis and treatment.
Keywords: type 1 diabetes, immune checkpoint inhibitors, immune-related adverse reactions, KN046
Introduction
In recent years, break through progress has been made in immunotherapy of malignant tumors, and it has become a new treatment method for refractory or recurrent tumors. Immune checkpoint inhibitors (ICIs) can target programmed death-1 (PD-1), Cytotoxic T-lymphocyte antigen-4 (CTLA-4) and programmed death ligand-1 (PD-L1) to reactivate the killing function of effector T cells in tumor cells, thus exerting an antitumor effect.1 Currently, ICIs are divided into three main types: PD-1 inhibitors, PD-L1 inhibitors and CTLA-4 inhibitors. Due to their unique mechanism of action, their adverse reactions are different from those of traditional chemoradiotherapy and targeted therapy, and immune dysfunction is the most common – therefore, adverse reactions to ICIs are called immune-related adverse events (irAEs).2 Endocrine adverse reactions are one of the most common adverse reactions and mainly involve the pituitary gland, thyroid gland, pancreas, adrenal gland and other endocrine glands, resulting in corresponding endocrine dysfunction. The mechanism of irAEs is not clear, but it has been determined that it is related to the excessive immune response caused by ICIs. This article reports a case of irAEs related to type 1 diabetes mellitus (T1DM) and diabetic ketoacidosis (DKA) after the occurrence of hypophysitis during immunotherapy and includes a review of the related literature to analyze the clinical characteristics of the disease and provide a basis for the diagnosis and treatment of endocrine system irAEs caused by such drugs.
Case Report
1.The patient was a 45-year-old man with a body mass index of 25.51 kg/m2. In January 2018, a chest CT examination was performed due to cough and sputum, and it showed a mass in the right lower lung. An additional chest enhanced CT scan and bronchoscopy biopsy led to a diagnosis of right middle and lower lobe adenocarcinoma. In view of the rapid growth of the lesion and the difficulty of surgery, no surgical treatment was performed. The patient received pemetrexed, gemcitabine and platinum chemotherapy successively, routine blood tests were performed, and liver and kidney function and blood glucose were monitored regularly during chemotherapy; no abnormalities were found. Later, due to obvious adverse reactions to chemotherapy drugs, the patient was enrolled in the “Phase II clinical trial to evaluate the efficacy, safety and drug resistance of KN046 in subjects with advanced non-small-cell lung cancer” in July 2019 using KN046 (recombinant humanized PD-L1/CTLA-4 bispecific single-domain antibody Fc fusion protein injection), the clinical trial identifier number:KN046-201. The patient received KN046 223.5 mg intravenous drip treatment successively from July 2019 to July 2021 every 14 days as a cycle. After 11 months of starting treatment (June 2020), the patient went to the doctor due to fatigue, and hypopituitarism was found. At that time, the levels of cortisol and adrenocorticotropic hormone and thyroid hormone levels were lower than normal. An MRI of the pituitary gland was normal. After that, prednisone tablets (7.5 mg) and levothyroxine tablets (75 μg) were taken daily as replacement therapy, and the symptoms improved.
2. On July 26, 2021, the patient developed nausea, vomiting and poor appetite without obvious causes and did not improve after receiving fluid reinfusion and gastric protection at the local hospital for “acute gastroenteritis”. On August 2, 2021, the patient was admitted to our hospital due to a fasting blood glucose (FBG) result of 360 mg/dl and HbA1c of 9.25%. The patient had no history of diabetes or hypertension. The patient regularly underwent routine biochemical review during immunotherapy, and his FBG was 72–90 mg/dl. The last routine biochemical review suggested that the FBG was 100.8 mg/dl on July 20, 2021. On admission, the body temperature was 36.6 °C, heart rate was 120 beats/min, breathing was 21 breaths/min, blood pressure was 136/105 mmHg, and blood oxygen saturation (SpO2) was 99%. At that time, he was conscious, poor in spirit, short of breath, and had dry skin.
3. Auxiliary examination: The blood glucose level of the fingertip was 291.6 mg/dl, and the blood ketone level of the fingertip was 6.4 mmol/L upon admission. The results of arterial blood gas analysis were as follows: pH: 7.14, partial pressure of carbon dioxide (PaCO2): 21 mmHg, partial pressure of oxygen (PaO2): 102 mmHg, bicarbonate: 7.1 mmol/L, residual alkali: −21.9 mmol/L; routine urinalysis: 3+ of ketone and + of glucose; HbA1c was 9.25% (normal range 4.0–6.5%) in the outpatient department. These data indicated the onset of diabetic ketoacidosis. Further examination results showed that there were no obvious abnormalities in the contrast-enhanced MRI scan of the pituitary gland (Figure 1) and the high-resolution CT of the pancreas, and the other laboratory examinations are shown in Table 1.
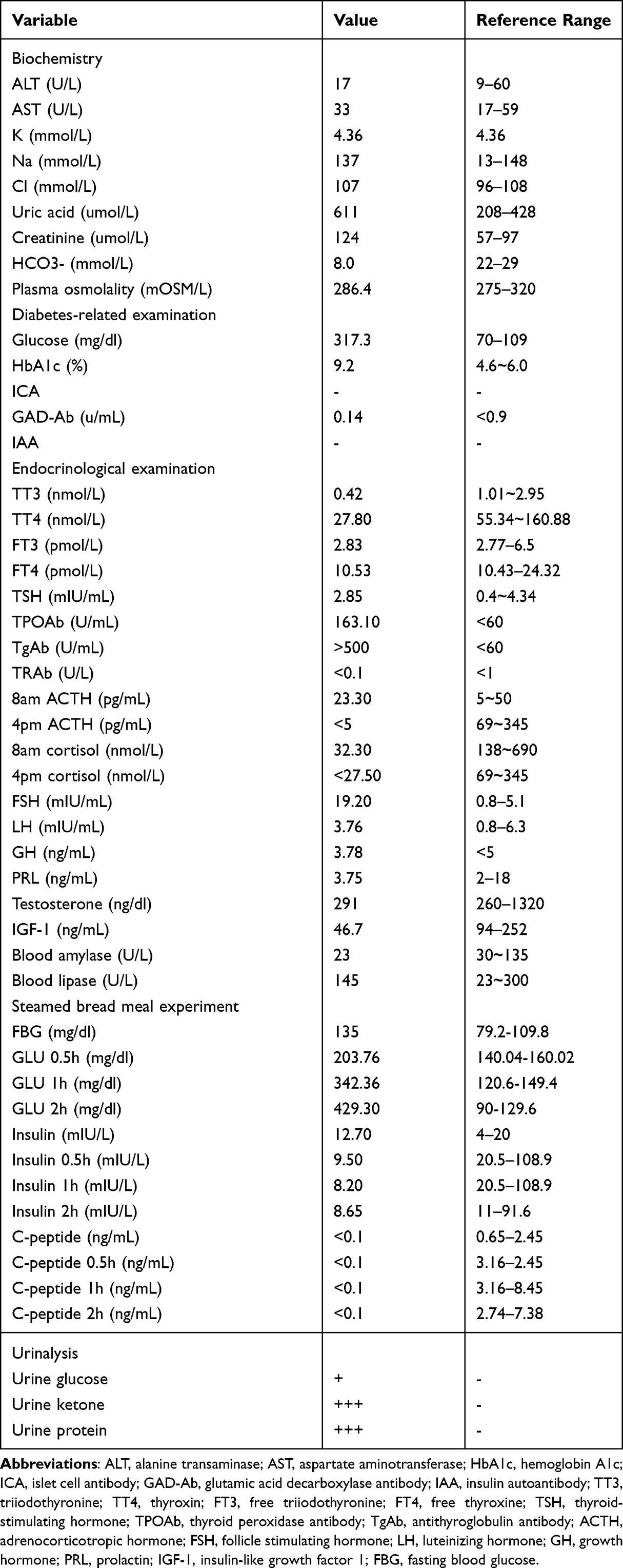 |
Table 1 Laboratory Results for the Patient |
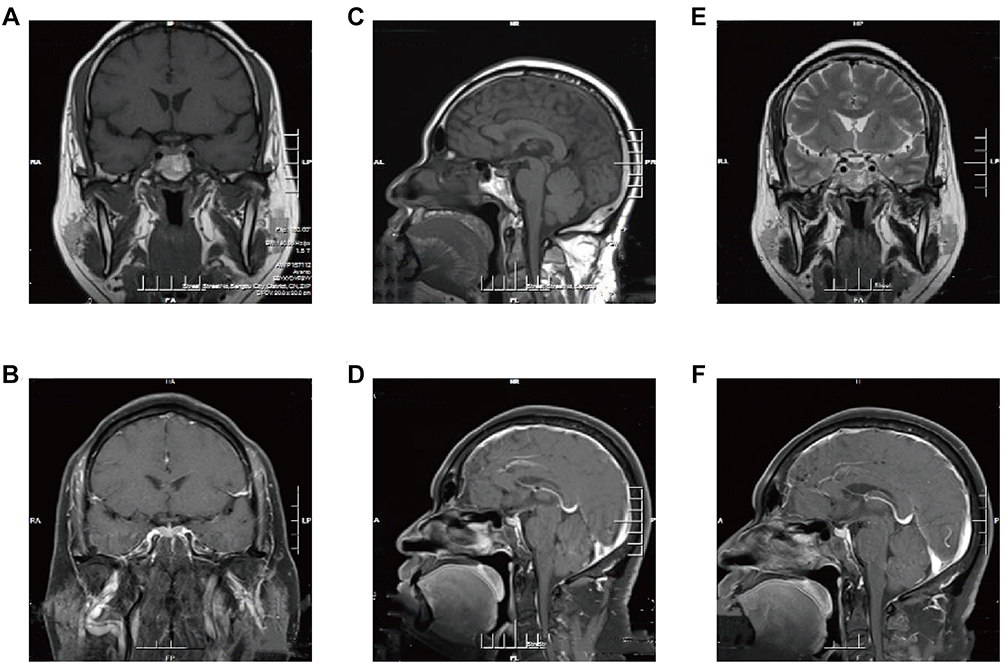 |
Figure 1 Sagittal and coronal slices of the pituitary MRI (A) Precontrast T1-weighted coronal slices MRI image. (B) Postcontrast T1-weighted coronal slices MR image. (C) Precontrast T1-weighted sagitta slices MRI image. (D) Postcontrast T1-weighted sagitta slices MR image. (E) Precontrast T2-weighted coronal slices MRI image. (F) Postcontrast T2-weighted sagitta slices MR image. |
4. Diagnosis and treatment: The patient had no history of diabetes, and his FBG was within normal range according to regular tests; however, his HbA1c was high, so postprandial blood glucose could not be ruled out during KN046 immunotherapy. Insulin and C-peptide levels could hardly be detected after admission, suggesting that islet β cell function had been lost. The patient was diagnosed with hypopituitarism for more than a year. Considering that immunotherapy involved the pituitary and caused hypophysis, HbA1c and postprandial blood glucose levels had not been monitored in the past. Therefore, based on the patient’s medical history and auxiliary examination, and referring to the domestic expert consensus (expert consensus on immune-related adverse reactions of the endocrine system caused by immune checkpoint inhibitors (2020)) for the recommended diagnostic criteria and disease classification of endocrine irAEs caused by ICIs, the following diagnoses were considered: 1. Immune checkpoint inhibitor-associated diabetes mellitus complicated by ketoacidosis, CTCAE grade 3; 2. Hypopituitarism hypofunction pituitary gland inflammation disease immune-checkpoint inhibitors correlation, CTCAE grade 2.3 The patient received intravenous fluid and insulin therapy in addition to oral rehydration and potassium. Intravenous insulin therapy was then followed by multiple injections of insulin aspart. For patients to stop taking prednisone and prior to administration of levothyroxine sodium replacement therapy, the hospital laboratory tests suggest that ACTH and cortisol levels are low, furthermore, Thyroxine was reduced, and thyroid stimulating hormone (TSH) was at the lower limit. To avoid pituitary induced crisis, the patients was temporarily placed on a 100 mg hydrocortisone intravenous drip. Nausea and vomiting ceased, and appetite improved markedly. After that, the prednisone tablets were substituted with low-dose therapy, and a physiological dose of levothyroxine sodium was supplemented. The patient has been treated with multiple daily subcutaneous insulin injections since August 5, 2021, and blood glucose gradually decreased and stabilized.
Discussion
The main cause of irAEs induced by ICIs is excessive activation of T lymphocytes, while endocrine-related irAEs mainly include hypophysitis, thyroiditis, diabetes, and adrenal cortical hypofunction, and so on. Among them, hypophysitis and thyroiditis are the most common, while diabetes is relatively rare. Previous studies have focused on the incidence of a single endocrine irAEs; however, people with one autoimmune disease are at higher risk of developing a second autoimmune disease.4,5
A meta-analysis of ICI treatment found that 85 of 6472 patients had hypophysitis,6 but the clinical symptoms of hypophysitis were mostly atypical.7,8 The most common symptoms were headache and fatigue, and multiple hormone deficiencies were also common,9,10 including TSH, ACTH, follicle stimulating hormone and luteinizing hormone. Early pituitary MRI examination was helpful for differential diagnosis.11 There is currently no consensus on the pathogenesis of ICI-associated hypophysitis, and studies have found that the presence of antipituitary gland autoantibodies and human leukocyte antigens (HLAs) in the serum of patients may increase the susceptibility of ICIs-induced hypophysitis.12 The occurrence time of hypophysitis was related to ICI type,10 among which the incidence of PD-L1/PD-1 plus CTLA-4 inhibitor was the highest (6.4%), followed by CTLA-4 inhibitor (3.2%), PD-1 inhibitor (0.4%) and PD-L1 inhibitor (less than 0.1%).7,13 Some studies have shown that the incidence of hypophysitis induced by CTLA-4 inhibitor therapy is much higher in men than in women.6,9 The higher incidence in males may be explained by the positive effect of androgens on the expression of CTLA-4.12 Therefore, it is suggested that male patients treated with ICIs need to pay attention to the occurrence of hypophysitis, especially in those treated with CTLA-4 inhibitor or combination therapy, and the onset time is mostly within the first half-year after treatment.3 In this case, the patient was male, and hypopituitarism was found due to fatigue after KN046 immunotherapy, which was consistent with the sex characteristics of hypophysitis-related cases reported in the past, but the onset time was later than in most related cases. This patient was admitted to the hospital due to ICI involving pancreatic injury and causing DKA, and the patient’s previous hypopituitarism was considered to be due to hypophysitis caused by ICI treatment. After admission, pituitary-related target gland hormone levels were tested, and the levels of TT3, TT4, cortex alcohol and ACTH were still low, which may be related to the patient’s decision to stop taking levothyroxine tablets and prednisone tablets after the onset of this disease. At the same time, a pituitary MRI showed no abnormalities, which may be related to the patient’s longer onset and long-term hormone replacement therapy.
Diabetes is a relatively rare adverse reaction to ICIs, mainly seen in PD-1 inhibitor treatment, with a few cases occurring in PD-L1 inhibitor treatment and only a few cases reported in CTLA-4 inhibitor treatment.14 PD-L1 is widely expressed not only in lymphoid tissues, but also in target organs including pancreatic b cells. Blocking the interaction of PD-1 and PD-L1 might stimulate T cell proliferation and activation then leading to the destruction of b cells, providing a possible mechanism for anti-PD-1 induced T1DM.15 A meta-analysis of 7551 patients from 38 randomized clinical trials showed that ICI induced diabetes in 0.2% (13 cases).6 The combination of anti-CTLA-4 with anti-PD-1 or PD-L1 increased the frequency of irAEs by 60% compared with ICI monotherapy.16 Among these cases, the median time of onset was 20 weeks, with most cases associated with monotherapy against PD-1/PD-L1 occurring after 10 weeks.14 Similarly, a small number of patients developed T1DM later. Stamatouli et al described a case of T1DM at 228 weeks (54 months) after initial treatment.14 The onset time of T1DM in this case was 25 months after receiving KN046 immunotherapy, and the onset was sudden and reached the diagnostic criteria of ICI-related diabetes recommended by Chinese experts.3 This reminds clinicians to regularly monitor the indicators related to islet function during immunotherapy, and they still need to pay more attention even after a long period of treatment.
ICI-related diabetes has a more acute onset and rapid progression, and the symptoms may be present in a short time, with high blood glucose or DKA symptoms. During immune therapy, patients have no obvious thirst or polyuria, such as with nonspecific symptoms of diabetes, and periodically tested fasting glucose levels are within normal range. Therefore, in patients with clinical symptoms that are not obvious or with no specific symptoms, dynamic monitoring of other indicators is also required. According to European and American guidelines,2,17–20 regular monitoring of blood glucose levels is recommended to detect type 1 or type 2 diabetes; however, even routine monitoring of blood glucose levels may not detect or predict its occurrence. After the onset of ICI-related diabetes, insulin and C-peptide often rapidly decreased to less than one-third of the normal value and may not return to normal for a long time. Therefore, we believe that dynamic monitoring of C-peptide levels is an effective means to predict ICI-related diabetes. In this case, the C-peptide level was too low to be detected after onset. This suggests that islet β cell function was severely impaired after KN046 therapy, and some cases have reported that partial recovery of islet function can be achieved in individual patients due to the release of glycotoxicity or the onset of the honeymoon phase.21,22 Diabetes autoantibody positivity is not necessarily related to the occurrence of ICI-related diabetes but may be related to the occurrence time of diabetes. The onset time of ICI-associated T1DM with antibody positivity was shorter, and DKA occurred more frequently than in patients with insulin autoantibody negativity.14 The patient’s diabetes autoantibodies were negative, and the onset time was long, which was consistent with the onset characteristics of most cases at present.
In contrast to previous related cases, hypopituitarism was found in this patient for 14 months before the occurrence of DKA, suggesting that patients after ICI treatment may have multiple endocrine gland injuries. And such events have also been reported. For example, Giulia Lanzolla reported a case of hyperglycemia after 2 cycles of the PD-L1 inhibitor atezolizumab and DKA, primary adrenal hypofunction, and hypophysitis with pituitary insufficiency after 4 cycles of treatment.23 Malik Asif Humayun also reported a case of T1DM secondary to hypophysitis during treatment with nivolumab, a PD-1 inhibitor, in combination with ipilimumab, a CTLA-4 inhibitor.24 Laura Boswell reported a case of hypophysitis in the course of immunotherapy with ipilimumab, a CTLA-4 inhibitor, and then explosive T1DM after the cessation of combined immunotherapy.25 Therefore, patients undergoing immunotherapy need to pay close attention to changes in endocrine and glandular functions during treatment, and even after the treatment ends.26 We should not let our guard down, and especially in the course of combined immunotherapy, we should pay close attention to the function of other glands after the injury of one endocrine gland. More importantly, the new drug KN046 used in this patient was a PD-L1/CTLA-4 bispecific antibody independently developed by Jiangsu Corning & Jerry’s Co. LTD. Its innovative design includes the fusion of CTLA-4 and PD-L1 single-domain antibodies with different mechanisms, which can simultaneously recognize PD-L1 and CTLA-4 and effectively enhance the killing of tumor cells.27 It is different from the combined immunotherapy used in previous cases, which may have caused injury to multiple endocrine glands in this patient, and the onset of the disease is late because of its unique therapeutic mechanism. In this case, a patient with polyendocrinopathy damage occurred during immunotherapy with KN046, and a trial on KN046 proposed a smart reagent that binds a nanoprobe and a double-blocking immunotherapy antibody, which improves the anti-tumor efficacy while having a high safety profile, which may reduce the incidence of irAEs.27 At present, we have not inquired about the endocrine-related irAEs caused by KN046 immunotherapy.
Due to lack of thyroid hormone function in this example patient, we were unable to determine whether the hypothyroidism is due to autoimmune thyroiditis or pituitary gland inflammation. However, the thyroid hormone function test results show that the TPOAb and TGAb levels were higher, and TRAb was negative, which may have been caused by autoimmune thyroiditis. It is also impossible to rule out whether thyroid dysfunction is caused by ICI-related thyroid damage. To determine the etiology, thyroid puncture can be performed to determine the pathological type. The causes of ICI-related thyroid dysfunction are related to the patient’s underlying thyroid disease, TSH levels, autoantibody titers, fluorodeoxyglucose uptake, and tumor immune microenvironment status.3
Unfortunately, the vast majority of patients described in these articles received no baseline assessment of endocrine gland function; thus, we cannot know how many had a silent metabolic/endocrine disorder before ICI therapy, and how many developed these conditions at a later date. Therefore, the strong need to have clear indications to assess patients before ICI therapy, along with a well-defined follow-up, plainly emerges.28
Conclusion
ICIs are widely used and can significantly prolong the survival period of tumor patients. However, we need to pay attention to various adverse reactions while focusing on their therapeutic effect. Among them, endocrine-related irAEs have unknown pathogenesis and complex clinical manifestations, which may endanger life in severe cases. In the course of ICI combination therapy, especially with immunosuppressive drugs such as KN046 that block both PD-L1 and CTLA-4 targets at the same time, patients may suffer damage to multiple endocrine glands, and it is necessary to pay close attention to the patient’s endocrine system irAEs for a long time, even after treatment.
Consent for Publication
Written informed consent for publication of their details was obtained from the patient. Based on the hospital there is no need for ethical clearance for the case report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Dougan M, Pietropaolo M. Time to dissect the autoimmune etiology of cancer antibody immunotherapy. J Clin Invest. 2020;130(1):51–61. doi:10.1172/JCI131194
2. Haanen J, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28:iv119–iv142. doi:10.1093/annonc/mdx225
3. Immune-endocrinology Group, Chinese society of Endocrinology, Chinese Medical Association. Chinese expert consensus on immune checkpoint inhibitors-induced endocrine immune-related adverse events (2020). Chin J Endocrinol Metab. 2021;37(01):1–16.
4. De Block C, De Leeuw I, Decochez K, et al. The presence of thyrogastric antibodies in first degree relatives of type 1 diabetic patients is associated with age and proband antibody status. J Clin Endocrinol Metab. 2001;86(9):4358–4363. doi:10.1210/jcem.86.9.7833
5. De Block C, De Leeuw I, Vertommen J, et al. Beta-cell, thyroid, gastric, adrenal and coeliac autoimmunity and HLA-DQ types in type 1 diabetes. Clin Exp Immunol. 2001;126(2):236–241. doi:10.1046/j.1365-2249.2001.01668.x
6. Barroso-Sousa R, Barry W, Garrido-Castro A, et al. Incidence of endocrine dysfunction following the use of different immune checkpoint inhibitor regimens: a systematic review and meta-analysis. JAMA Oncol. 2018;4(2):173–182. doi:10.1001/jamaoncol.2017.3064
7. Faje A, Sullivan R, Lawrence D, et al. Ipilimumab-induced hypophysitis: a detailed longitudinal analysis in a large cohort of patients with metastatic melanoma. J Clin Endocrinol Metab. 2014;99(11):4078–4085. doi:10.1210/jc.2014-2306
8. Albarel F, Gaudy C, Castinetti F, et al. Long-term follow-up of ipilimumab-induced hypophysitis, a common adverse event of the anti-CTLA-4 antibody in melanoma. Eur J Endocrinol. 2015;172(2):195–204. doi:10.1530/EJE-14-0845
9. Scott E, Long G, Guminski A, Clifton-Bligh R, Menzies A, Tsang V. The spectrum, incidence, kinetics and management of endocrinopathies with immune checkpoint inhibitors for metastatic melanoma. Eur J Endocrinol. 2018;178(2):173–180. doi:10.1530/EJE-17-0810
10. Chang L, Barroso-Sousa R, Tolaney S, Hodi F, Kaiser U, Min L. Endocrine toxicity of cancer immunotherapy targeting immune checkpoints. Endocr Rev. 2019;40(1):17–65. doi:10.1210/er.2018-00006
11. Joshi M, Whitelaw B, Palomar M, Wu Y, Carroll P. Immune checkpoint inhibitor-related hypophysitis and endocrine dysfunction: clinical review. Clin Endocrinol (Oxf). 2016;85(3):331–339. doi:10.1111/cen.13063
12. Frasca F, Piticchio T, Le Moli R, et al. Recent insights into the pathogenesis of autoimmune hypophysitis. Expert Rev Clin Immunol. 2021;17(11):1175–1185. doi:10.1080/1744666X.2021.1974297
13. Sznol M, Postow M, Davies M, et al. Endocrine-related adverse events associated with immune checkpoint blockade and expert insights on their management. Cancer Treat Rev. 2017;58:70–76. doi:10.1016/j.ctrv.2017.06.002
14. Stamatouli A, Quandt Z, Perdigoto A, et al. Collateral damage: insulin-dependent diabetes induced with checkpoint inhibitors. Diabetes. 2018;67(8):1471–1480. doi:10.2337/dbi18-0002
15. Yadav D, Sarvetnick N. Costimulation and pancreatic autoimmunity: the PD-1/PD-L conundrum. Rev Diabet Stud. 2006;3(1):6–10. doi:10.1900/RDS.2006.3.6
16. Wolchok J, Chiarion-Sileni V, Gonzalez R, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2017;377(14):1345–1356. doi:10.1056/NEJMoa1709684
17. Higham C, Olsson-Brown A, Carroll P, et al. Society for endocrinology endocrine emergency guidance: acute management of the endocrine complications of checkpoint inhibitor therapy. Endocr Connect. 2018;7(7):G1–G7. doi:10.1530/EC-18-0068
18. Thompson J, Schneider B, Brahmer J, et al. NCCN guidelines insights: management of immunotherapy-related toxicities, Version 1.2020. J Natl Compr Cancer Netw. 2020;18(3):230–241. doi:10.6004/jnccn.2020.0012
19. Brahmer J, Lacchetti C, Schneider B, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American society of clinical oncology clinical practice guideline. J Clin Oncol. 2018;36(17):1714–1768. doi:10.1200/JCO.2017.77.6385
20. Puzanov I, Diab A, Abdallah K, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J Immunother Cancer. 2017;5(1):95. doi:10.1186/s40425-017-0300-z
21. Kumagai R, Muramatsu A, Nakajima R, et al. Acute-onset type 1 diabetes mellitus caused by nivolumab in a patient with advanced pulmonary adenocarcinoma. J Diabetes Investig. 2017;8(6):798–799. doi:10.1111/jdi.12627
22. Matsumura K, Nagasawa K, Oshima Y, et al. Aggravation of diabetes, and incompletely deficient insulin secretion in a case with type 1 diabetes-resistant human leukocyte antigen DRB1*15:02 treated with nivolumab. J Diabetes Investig. 2018;9(2):438–441. doi:10.1111/jdi.12679
23. Lanzolla G, Coppelli A, Cosottini M, Del Prato S, Marcocci C, Lupi I. Immune checkpoint blockade anti-PD-L1 as a trigger for autoimmune polyendocrine syndrome. J Endocr Soc. 2019;3(2):496–503. doi:10.1210/js.2018-00366
24. Kikuchi F, Saheki T, Imachi H, et al. Nivolumab-induced hypophysitis followed by acute-onset type 1 diabetes with renal cell carcinoma: a case report. J Med Case Rep. 2021;15(1):214. doi:10.1186/s13256-020-02656-7
25. Humayun M, Poole R. A case of multiple immune toxicities from Ipilimumab and pembrolizumab treatment. Hormones. 2016;15(2):303–306. doi:10.14310/horm.2002.1656
26. Boswell L, Casals G, Blanco J, et al. Onset of fulminant type 1 diabetes mellitus following hypophysitis after discontinuation of combined immunotherapy. A case report. J Diabetes Investig. 2021;12(12):2263–2266. doi:10.1111/jdi.13604
27. Jiang C, Zhang L, Xu X, et al. Engineering a smart agent for enhanced immunotherapy effect by simultaneously blocking PD-L1 and CTLA-4. Adv Sci. 2021;8(20):e2102500. doi:10.1002/advs.202102500
28. Ruggeri R, Campennì A, Giuffrida G, et al. Endocrine and metabolic adverse effects of immune checkpoint inhibitors: an overview (what endocrinologists should know). J Endocrinol Invest. 2019;42(7):745–756. doi:10.1007/s40618-018-0984-z
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.