")
Back to Journals » Journal of Blood Medicine » Volume 14
Autoimmune Hemolytic Anemia Caused by Cold Agglutinin Antibodies in Systemic Lupus erythematosus—a Rare Association: Case Report
Authors Osorio-Toro LM , Quintana-Ospina JH, Melo-Burbano LÁ , Ruiz-Jiménez PA, Daza-Arana JE , Rivas-Tafurt GP , Izquierdo-Loaiza JH
Received 11 May 2023
Accepted for publication 11 August 2023
Published 4 September 2023 Volume 2023:14 Pages 507—511
DOI https://doi.org/10.2147/JBM.S420937
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Luis Miguel Osorio-Toro,1– 3 Jhon Herney Quintana-Ospina,1– 3 Luis Álvaro Melo-Burbano,1– 3 Paola Andrea Ruiz-Jiménez,1– 3 Jorge Enrique Daza-Arana,1,4 Giovanna Patricia Rivas-Tafurt,1,2 Jorge Hernán Izquierdo-Loaiza1,2
1Specialization in Internal Medicine, Department of Health, Universidad Santiago de Cali, Santiago de Cali, Colombia; 2Department of Research and Education, Clínica de Occidente S.A, Santiago de Cali, Santiago de Cali, Colombia; 3Genetics, Physiology, and Metabolism Research Group (GEFIME), Universidad Santiago de Cali, Santiago de Cali, Colombia; 4Health and Movement Research Group, Universidad Santiago de Cali, Santiago de Cali, Colombia
Correspondence: Jorge Enrique Daza-Arana, Specialization Program in Internal Medicine, Department of Health, Universidad Santiago de Cali, Calle 5 # 62-00, Santiago de Cali, Colombia, Tel +57 3108923676, Fax +57 3108923676, Email [email protected]
Abstract: Autoimmune hemolytic anemias (AIHAs) are rare and heterogeneous disorders characterized by the destruction of red blood cells by warm or cold antibodies. Hemolytic anemia associated with warm antibodies is the most common, whereas cold antibodies are rare and infrequent in cases published in the scientific literature. Herein, we present the case of a young patient with systemic lupus erythematosus (SLE) and autoimmune hemolytic anemia caused by cold antibodies. Initially, infectious etiology and hematological malignancy were considered, which were ruled out. She required management in the intensive care unit due to severe hematological involvement and responded well to immunomodulatory therapy. This case illustrates the importance of a strong clinical suspicion of AIHA due to cold agglutinins associated with SLE when faced with similar clinical symptoms in order to achieve a timely diagnosis and provide optimal therapy.
Keywords: autoimmune hemolytic anemia, systemic lupus erythematosus, autoimmune diseases, antibodies
Introduction
Autoimmune hemolytic anemias (AIHAs) are rare and heterogeneous disorders characterized by the destruction of red blood cells by warm or cold antibodies.1 Cold-antibody autoimmune hemolytic anemia, also known as cold agglutinin disease when it is primary, is a type of hemolysis caused by immunoglobulin M (IgM) antibodies directed against the polysaccharide antigens of the red blood cell membrane,2 accounting for 15%–30% of AIHAs.3 The red blood cell-associated glycan that is the target of cold agglutinin antibodies are those containing N-polylactosamine.4 Cold agglutinin syndrome is a hemolytic disorder caused by cold antibodies; however, it arises as a result of another clinical disease, with systemic lupus erythematosus (SLE) being an uncommon cause.5 SLE is a multisystem disease with several clinical presentations,6 including hemolytic anemia, which affects less than 10% of patients and is generally caused by warm IgG antibodies. It is rare to detect hemolytic anemia mediated by cold antibodies in this disease,7 and the literature contains only a few descriptions of cases of hemolytic anemia caused by cold antibodies in SLE.7–9 As a result of the rare association between these two entities, our report is significant.
Case Presentation
A 22-year-old female patient with no relevant medical history was admitted to the emergency room of a third-level clinic for clinical symptoms that began 10 days before admission, including intermittent fever up to 39°C, general malaise, headache, myalgia, a mild self-limiting rash episode, diarrhea, and occasional emesis. On physical examination, the patient had mild pallor, icteric sclerae, supraclavicular and cervical adenopathies, synovitis in bilateral metacarpophalangeal joints, and grade II edema in the lower limbs. Paraclinical testing was performed (Table 1), and infectious etiology and hematological neoplasia were ruled out. The classification criteria for SLE were met.10 The patient was anti-DNA negative, a kidney biopsy was recommended because of the presence of proteinuria, which was consistent with class II mesangial lupus nephritis.
 |
Table 1 Clinical Laboratory Findings |
Autoimmune hemolytic anemia was also confirmed, with laboratory data revealing a cold agglutinin titer Positive dilution 1/128 at 4°C, hemoglobin 6.2 g/dl, hematocrit 18.1% and monospecific direct antiglobulin strongly positive for C3d and negative for IgG, leading to the diagnosis of cold agglutinin syndrome.11 The patient was transferred to the intensive care unit because of severe hematological involvement, as demonstrated by pancytopenia. Treatment was initiated with dexamethasone at a dose of 40 mg intravenously daily for 4 days and hydroxychloroquine at a dose of 200 mg daily orally, and the three cell lines showed clinical improvement and hematological recovery without the need for blood transfusions. Renal function remained stable and I did not present any other complications. The patient was discharged from the hospital after receiving outpatient treatment with prednisone at a dose of 5 mg daily orally, hydroxychloroquine at a dose of 200 mg daily orally and mycophenolate mofetil at a dose of 500 mg every 12 hours for one week and thereafter at a dose of 500 mg every 8 hours. She made steady progress to her rheumatology follow-up in the outpatient department with no new relapses.
In this case report, all procedures were performed according to the ethical and bioethical standards of the Scientific Committee of the Clínica de Occidente and the Declaration of Helsinki of 1964 and its later versions. Informed consent was obtained from the study subject prior to her participation and the publication of this study.
Discussion
Autoimmune hemolytic anemia is a rare disease with an annual incidence of 1–3 individuals out of every 100,000.12 AIHA occurs in 10% of patients with SLE and is generally associated with warm antibodies; cold hemagglutinin disease has also been rarely observed. This paper describes the case of a patient with autoimmune hemolytic anemia due to cold agglutinins in the context of de novo SLE.
Cold hemagglutination and its association with hemolysis were described for the first time in 1903. The binding of antibodies to red blood cells activates the classical pathway of the complement system, which leads to the formation of the membrane attack complex and intravascular hemolysis. Furthermore, if the classical pathway fails, erythrocytes are opsonized with complement proteins (particularly C3b and C4b), which increase phagocytosis in the liver and spleen, leading to extravascular hemolysis.7 Haptoglobin levels were low in our patient, suggesting intravascular hemolysis.
The anti-erythrocyte antibodies in SLE are mainly warm IgG, but mixed AIHA has also been reported. Our case had characteristics of cold IgM AIHA.9 Cold agglutinin AIHA can be primary (cold agglutinin disease) or secondary (cold agglutinin syndrome) to infections, malignancies, or autoimmune conditions.13 Secondary etiologies other than SLE were ruled out in our case.
Corticosteroids result in remission in less than 20% of patients with cold agglutinin disease, and unacceptably high maintenance doses are often required to achieve a sustained response in the few responders. Thus, corticosteroid-sparing alternatives should be considered, with bendamustine or rituximab being the preferred treatments for these patients.14 However, in cold agglutinin syndrome, as in the case of our patient, the only established therapy is the treatment of the underlying disease.15 In our case, corticosteroids were administered and a favorable clinical and paraclinical response was observed, as reported in other similar cases in the literature with an adequate response.7–9
The cases described in the literature are female, generally all in the second and third decades of life; only one case was described in a female patient in the fifth decade of life (case 2). In no case was there evidence of a history of comorbidities prior to diagnosis. Most cases with short duration of the disease. Case 1, case 3 and our case presented hypocomplementemia, which spoke of disease activity. We do not have information on the complement levels of case 2. All cases have elevated bilirubin levels at the expense of the indirect. The only case that showed renal compromise due to SLE up to the time of diagnosis was ours. All received immunosuppressive treatment with a good response, only case 2 received biologics with a good haematological response (Table 2).
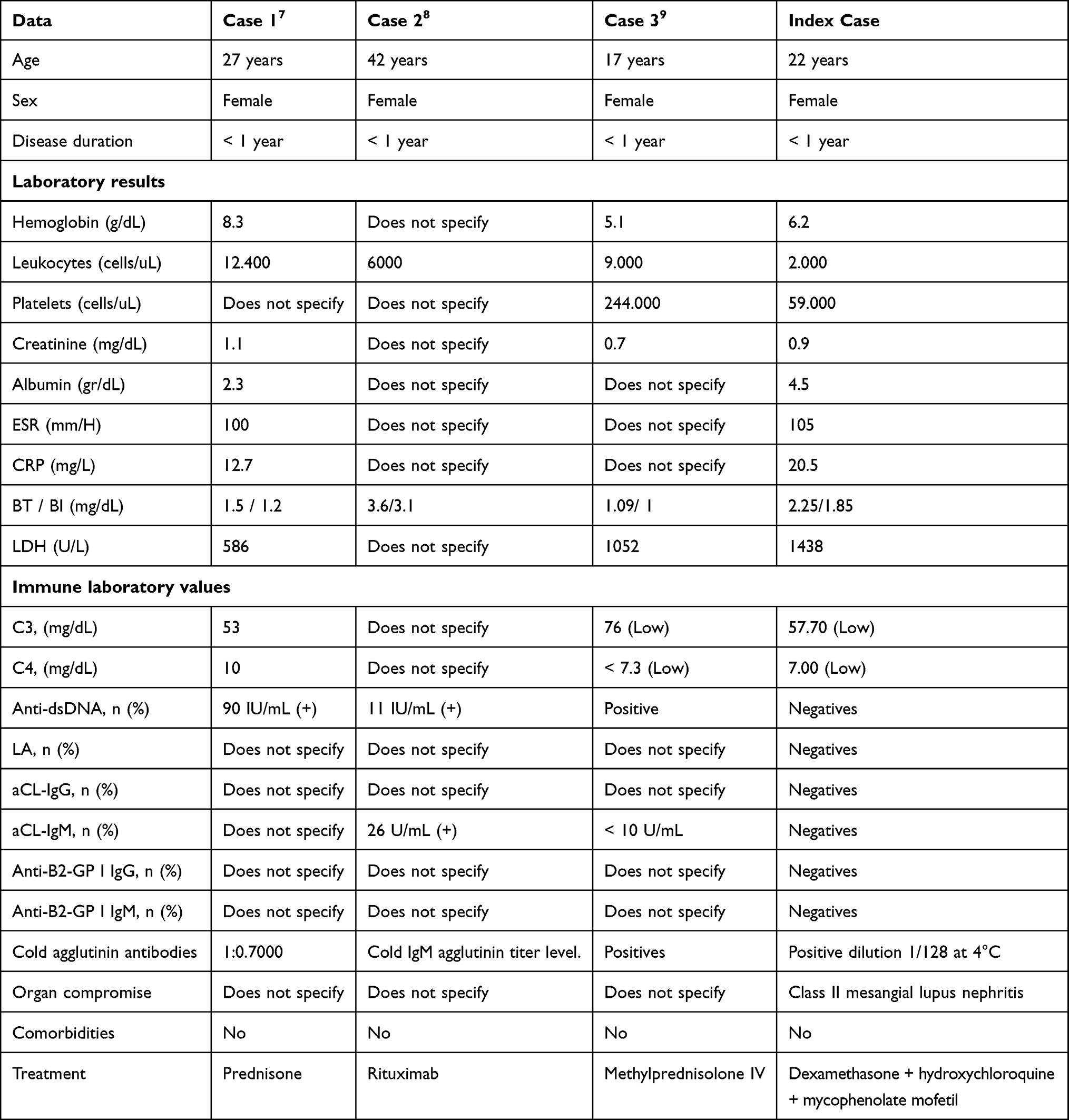 |
Table 2 Cases of Hemolytic Anemia Caused by Cold Agglutinin Antibodies Reported in the Literature |
Conclusion
AIHA due to cold agglutinins associated with SLE is extremely rare, it is key to know other entities that lead to confusion in the final diagnosis of this pathology, such as lymphoproliferative and infectious disorders. Given the focus on different treatment regimens, the difference between cold agglutinin syndrome and the disease should be clear, since in the syndrome the treatment focuses on the management of the underlying disease. Our patient responded strongly to management with dexamethasone, hydroxychloroquine and mycophenolate.
Abbreviations
AIHA, autoimmune hemolytic anemia; SLE, systemic lupus erythematosus; IgM, immunoglobulin M.
Acknowledgments
The research team’s activities were sponsored by Clínica de Occidente S.A. and the Universidad Santiago de Cali. However, the authors declare full autonomy when conducting all phases of the study.
Funding
This research has been funded by Dirección General de Investigaciones of Universidad Santiago de Cali under call No. 02-2023.
Disclosure
Dr Giovanna Patricia Rivas-Tafurt reports personal fees from Amgen and Bristol Myers Squibb, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Jäger U, Barcellini W, Broome CM, et al. Diagnosis and treatment of autoimmune hemolytic anemia in adults: recommendations from the First International Consensus Meeting. Blood Rev. 2020;41:100648. doi:10.1016/j.blre.2019.100648
2. Velasco Montes J, Oriñuela González I, Sanjuan López AZ, Ortiz de Zárate Ibarra Z. Anemia hemolítica por aglutininas frías y cáncer de origen desconocido [Cold agglutinin disease and cancer of unknown origin]. Rev Esp Geriatr Gerontol. 2010;45(3):172–173. doi:10.1016/j.regg.2009.12.002
3. Sokol RJ, Hewitt S, Stamps BK. Autoimmune haemolysis: an 18-year study of 865 cases referred to a regional transfusion centre. Br Med J. 1981;282(6281):2023–2027. doi:10.1136/bmj.282.6281.2023
4. Bua RO, Messina A, Sturiale L, Barone R, Garozzo D, Palmigiano A. N-Glycomics of Human Erythrocytes. Int J Mol Sci. 2021;22(15):8063. doi:10.3390/ijms22158063
5. Berentsen S, Tjønnfjord GE. Diagnosis and treatment of cold agglutinin mediated autoimmune hemolytic anemia. Blood Rev. 2012;26(3):107–115. doi:10.1016/j.blre.2012.01.002
6. Rivas-Larrauri F, Yamazaki-Nakashimada MA. Systemic lupus erythematosus: ¿Is it one disease? Reumatol Clin. 2016;12(5):274–281. doi:10.1016/j.reuma.2016.01.005
7. Srinivasan N, Oswal A, Garg S, Nahar J, Gosmonova A, Nahar R. Cold agglutinin induced hemolysis in a newly diagnosed systemic lupus erythematosus. Am J Med Sci. 2010;339(3):270–273. doi:10.1097/MAJ.0b013e3181ac3bd5
8. Chaubey VK, Chhabra L. Cold agglutinin-induced haemolysis in association with antinuclear antibody-negative SLE. BMJ Case Rep. 2013;2013(jun10 1):bcr2013009337–bcr2013009337. doi:10.1136/bcr-2013-009337
9. Mohanty B, Ansari MZ, Kumari P, Sunder A. Cold agglutinin-induced hemolytic anemia as the primary presentation in SLE - A case report. J Family Med Prim Care. 2019;8(5):1807–1808. doi:10.4103/jfmpc.jfmpc_298_19
10. Aringer M, Petri M. New classification criteria for systemic lupus erythematosus. Curr Opin Rheumatol. 2020;32(6):590–596. doi:10.1097/BOR.0000000000000740
11. Berentsen S. New Insights in the Pathogenesis and Therapy of Cold Agglutinin-Mediated Autoimmune Hemolytic Anemia. Front Immunol. 2020;11:590. doi:10.3389/fimmu.2020.00590
12. Michel M. Classification and therapeutic approaches in autoimmune hemolytic anemia: an update. Expert Rev Hematol. 2011;4(6):607–618. doi:10.1586/ehm.11.60
13. Berentsen S, Ulvestad E, Langholm R, et al. Primary chronic cold agglutinin disease: a population based clinical study of 86 patients. Haematologica. 2006;91(4):460–466.
14. Berentsen S. How I treat cold agglutinin disease. Blood. 2021;137(10):1295–1303. doi:10.1182/blood.2019003809
15. Berentsen S, Barcellini W. Autoimmune Hemolytic Anemias. N Engl J Med. 2021;385(15):1407–1419. doi:10.1056/NEJMra2033982
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.