")
Back to Journals » Clinical Interventions in Aging » Volume 18
Attitudes of Older Adult Patients and Caregivers Towards Deprescribing of Medications in Ethiopia
Authors Gadisa DA , Gebremariam ET , Yimer G, Deresa Urgesa E
Received 8 December 2022
Accepted for publication 17 June 2023
Published 24 July 2023 Volume 2023:18 Pages 1129—1143
DOI https://doi.org/10.2147/CIA.S400698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Diriba Alemayehu Gadisa,1 Esayas Tadesse Gebremariam,1 Getnet Yimer,2,3 Efa Deresa Urgesa4
1Pharmacy Department, College of Medicine and Health Sciences, Ambo University, Ambo, Oromia, Ethiopia; 2Department of Genetics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 3Penn Center for Global Genomics & Health Equity, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 4Contract Director Management Department, Ethiopian Pharmaceutical Supply Service, Addis Ababa, Ethiopia
Correspondence: Diriba Alemayehu Gadisa, Email [email protected]; [email protected]
Background: Deprescribing is essential for reducing inappropriate medication use and polypharmacy. For a holistic approach, it is essential to know how older adult patients and their caregivers perceive deprescribing.
Objective: To assess the attitude of older adult patients and caregivers towards deprescribing medication at Ambo University Referral Hospital.
Methodology: Institutional-based cross-sectional study was conducted using the revised Patients’ Attitude Towards Deprescribing tool (rPATD). The data was analyzed using the SPSS-25 software. Backward linear regression and logistic regression were used to measure association between outcome and determinant variables. The two-sided P-value ≤ 0.05 with 95% confidence interval was utilized for reporting significant factors.
Results: One hundred fifty-six (81.3%) of the respondents (ie, 85.0% of older adult and 77.2% of caregivers) agreed to stop one or more of their regular medications if the physician said it was possible despite 98 (51.0%) of them (ie, 49.0% of older adult and 53.3% of caregivers) being satisfied with their/their care recipient’s medications. On the overall aggregate mean score, the respondents had a neutral position (2.6– 3.59) regarding the burden and concerns of stopping medications whereas the majority of them disagree (1.0– 2.59) with the inappropriateness of the medication they were taking and agreed (3.6– 5.0) with the need for their involvement in treatment decision making. Concerns about stopping medicine scores (AOR = 0.440, 95% CI = 0.262– 0.741, P = 0.035) and perceived levels of medication inappropriateness (AOR = 0.653, 95% CI = 0.456– 0.936, P = 0.020) was significantly associated with the willingness to discontinue and overall satisfaction with their medicine regimen respectively.
Conclusion: The majority of older adult patients and caregivers would like to deprescribe if the physicians recommended it. The perceived concerns of stopping and inappropriateness of the medicines were associated with the willingness to deprescribe and overall satisfaction with their medicine respectively. Healthcare providers should prompt the deprescribing process with older adult patients and caregivers by addressing their concerns about stopping medications.
Keywords: attitude, caregiver, deprescribing, older adult patients, Ethiopia
Background
The use of many drugs is a common phenomenon among older adult who often present with age-related multimorbidity and it tends to become a major public health concern globally because of its risk for polypharmacy and potentially inappropriate medications (PIMs).1,2 Both polypharmacy and PIM are associated with lower quality of life, adverse drug reactions, increased hospitalizations, and mortality rates.1 In developed nations, 30% to 60% of older adult patients aged ≥65 years are exposed to polypharmacy.3 Up to three out of every four older adult patients are thought to take five or more medicines daily.4
Polypharmacy is defined by the World Health Organization (WHO) as the administration of many drugs at the same time or the administration of an excessive number of drugs.5 This could further be classified into cumulative, continuous, and simultaneous polypharmacy, based on the time window of the medications used.2 This ascertains that there is no universal standard definition for polypharmacy in terms of the number of medicine, the duration of the therapy, and the healthcare setting.6 However, the most commonly reported definition of polypharmacy in literature is a numerical-only definition which is the regular use of at least five medications.7,8 This threshold does not account for whether the medications are appropriate or not as per the deprescribing guidelines such as Beers9 and STOPP/START criteria.10 It can be appropriate (ie, when potential benefits outweigh potential harms) but increases the risk of older adult patients experiencing adverse drug reactions, hospital admission, and impaired physical and cognitive function.4,11
Polypharmacy increases the risk of receiving potentially inappropriate medications6,12,13 which are adverse risks that exceed their health benefits when compared with alternative therapies.14 The increasing intake of multiple medications which may be recommended in the disease-specific guidelines could be inappropriate for the older adult patient when person-centered care is taken into account.15
This ensures that taking more medications as per disease-specific guidelines always does not translate to better health for older adult patient.16 Therefore, devising different preventive strategies, such as deprescription17 and unorthodox prescriptive interventions like social prescribing,16 should not be delayed for older adult patients with multimorbidity to minimize the burden of polypharmacy and PIM.18
Deprescribing is the supervised process of medication’s dose reduction and medication/s withdrawal in which its actual or possible risks outweigh existing or potential benefits in the context of an individual patient’s treatment goals, the present level of functioning, life expectancy, values, and preferences.19,20 The purpose of deprescribing is to maximize the benefit through treatment optimization that tailored to individual patient circumstances.21 However, guidelines have been written for the management of single disease states rather than addressing the multimorbidity that affects many older adult people.15 Therefore, due to the paucity of guidelines to manage and optimize treatment in older adult patients with multimorbidity, the process of deprescribing will create anxiety and challenge for both patients and healthcare providers.1,8 Tailoring medication decisions often entail beyond protocol decision-making, a complex process involving emotional and cognitive work for healthcare professionals and patients.8 This initiates Turk et al and other authors to outline a person-centered approach such as shared-decision making, continuity of care, the development of trust, monitoring, and a multidisciplinary approach to tackle deprescribing-related challenges.1,17 Therefore, deprescribing is a patient-centered intervention that requires collaborative decision-making, informed patient consent, and healthcare provider participation.22
By adhering to a person-centered and multidisciplinary approach, deprescribing is a practical and relatively safe medicine optimization practice.23 Understanding how older adults understand deprescribing is crucial to ensure a holistic approach to undertaking deprescribing.24 Patients’ involvement is critical in collaboration with caregivers, prescribers, and other healthcare professionals to enhance the benefits of deprescribing.25
Despite the potential health benefits of deprescribing, healthcare providers,26 patients’ and caregivers’27 argue that discontinuing medications is a challenge in implementing deprescribing. Fear of discontinuing medications started by another doctor, a lack of information about how to deprescribe medications, and concern about the effects of medication withdrawal are all barriers to deprescribing medication.28
According to a systematic review and meta-analysis by Gebreyohannes et al,29 the total prevalence of polypharmacy and PIM usage in the older adult population in Ethiopia was 33% and 37%, respectively, and its impact on the healthcare system of the country is rapidly increasing.30 Interestingly, Tegegn et al30 reported that 81.6% of older adult patients in Ethiopia had agreed to stop one of their medicines if their doctors said it was possible.
Overall, although few studies reveal the burden of polypharmacy in Ethiopia, there is a lack of an objective piece of evidence on the attitudes of both older adult patients and caregivers toward deprescribing in the country.30,31 So far Tegegn et al30 reported the attitudes of older adult patients toward deprescribing in one University hospital in Ethiopia but they did not include the attitude of caregivers. Therefore, this study aimed to assess the perception of both older adult patients and caregivers towards the concept of deprescribing and their willingness to reduce their medications at Ambo University Referral Hospital (AURH), Ethiopia. Besides, it also aimed to assess the older adult patients’ and caregivers’ overall satisfaction with the medication they were taking. Henceforth, as part of the optimal health care of older adult individuals, this study may help healthcare providers in dealing with regular medication reviews for deprescribing unsuitable prescriptions, which may result in overall good treatment outcomes. Finally, yet importantly, as this study is the first in Ethiopia, it can be used as an initial point of reference for those who will have the interest to perform similar studies on this topic.
Methods
Study Area
The study was conducted at Ambo University Referral Hospital (AURH) which is found in Ambo town, Oromia Regional State, Ethiopia. The hospital catchment population is more than 1,000,000. Ambo town is located 114 km away from the capital city, Addis Ababa.
Study Design and Period
An institutional-based cross-sectional study design was employed to assess the attitudes of older adult patients and caregivers towards the deprescribing of medications at AURH. The study was carried out from July 25, 2021 to August 25, 2021, G.C.
Sampling
The sample size was computed based on a single population proportion,  . The proportion (P) of rPATD in this group is taken as 81.6% to get a possible large sample size based on the previous study on older adult patients.30 A total of 234 sample size was calculated using the level of significance (α) = 0.05 which gives Zα/2 = 1.96, a marginal error (d) of 5%, p = 0.816, and q=1-p. However, from the hospital registry, the total number of older adult patients (age ≥65 years) with at least one chronic disease and who had a follow-up at AURH outpatient clinics till the first day of the data collection period was 973 (ie, N = 973). Since the target population is less than 10,000 (ie, 973 < 10,000), the sample size correction formula (
. The proportion (P) of rPATD in this group is taken as 81.6% to get a possible large sample size based on the previous study on older adult patients.30 A total of 234 sample size was calculated using the level of significance (α) = 0.05 which gives Zα/2 = 1.96, a marginal error (d) of 5%, p = 0.816, and q=1-p. However, from the hospital registry, the total number of older adult patients (age ≥65 years) with at least one chronic disease and who had a follow-up at AURH outpatient clinics till the first day of the data collection period was 973 (ie, N = 973). Since the target population is less than 10,000 (ie, 973 < 10,000), the sample size correction formula ( ) was employed to get the final sample size (nf). Then, the minimum final sample size was calculated to be 187. Accordingly, a total of 192 participants, 100 older adult patients (ie, aged ≥65 years) with at least one chronic disease and who were regularly taking at least one medication as well as 92 older adult patient’s caregivers whose age is ≥18 years were included in the study. Older adult participants and caregiver participants were recruited independently, ie, they were not paired. Older adult patients who were below 65 years of age and who had severe physical or psychological problems and patients, and caregivers who refused to participate were excluded from the study.
) was employed to get the final sample size (nf). Then, the minimum final sample size was calculated to be 187. Accordingly, a total of 192 participants, 100 older adult patients (ie, aged ≥65 years) with at least one chronic disease and who were regularly taking at least one medication as well as 92 older adult patient’s caregivers whose age is ≥18 years were included in the study. Older adult participants and caregiver participants were recruited independently, ie, they were not paired. Older adult patients who were below 65 years of age and who had severe physical or psychological problems and patients, and caregivers who refused to participate were excluded from the study.
Data Collection and Analysis
The data was collected by two graduate pharmacy students using structured questionnaires. The rPATD questionnaire developed by Reeve et al,32 which is a validated multidimensional questionnaire, that measures patients’ attitudes related to medication discontinuation was used. The rPATD questionnaire is a 22-item and 19-item questionnaire for older adults and caregivers, respectively. The tool has four major factors, namely the burden factor (five items), appropriateness factor (five items), concerns about stopping factor (five items), and involvement factor (five items), and additional two global questions are also considered. All statements have five-point Likert scale answer options, which are strongly agreed, agree, neutral, disagree, and strongly disagree. The scores were summed to achieve a total score per domain (strongly agree = 5 to strongly disagree = 1).
We calculated the average score for each of the four factors, namely the burden factor, inappropriateness factor, concern factor, and involvement factor.32 Domain scores range between 1 and 5, with higher scores indicative of a greater perceived burden of their medication, concerns about stopping the medicine, belief in the appropriateness of withdrawal, and involvement in their medication management.33
We received permission to use rPATD questionnaire. Accordingly, the questionnaire in English version was translated into Afaan Oromo (ie, the working language of the study area), and back to English to ensure that the translated version gives the proper meaning by two individuals fluent in both languages. The Afaan Oromo version of the questionnaire was piloted on 15 older patients and caregivers of older adult patients with at least one chronic disease and had been receiving at least one medication for that. Those involved in the pilot were eventually excluded from the actual study. After all necessary corrections were made to the questionnaire based on the feedback from the pilot study, the finalized rPATD Afaan Oromo version was utilized for final data collection.
After the data were checked for completeness and consistency, it was entered and analyzed using SPSS version 25. A backward linear regression model was used to assess the influence of study participants’ socio-demographics and clinical characteristics on inappropriateness, concerns about stopping, involvement, and burden after the average factor scores were categorized into disagree (1–2.5), neutral (2.6–3.5), and agree (3.6–5) as previously proposed by Crutzen and his co-authors.34
Backward binary logistic regression analysis was conducted for the two global questions of rPATD after patients’ willingness to deprescribe and satisfaction with medication response were combined as “agree” and “strongly agree” into “agree” and all other responses (ie, neutral, disagree and strongly disagree) into “disagree” as proposed by Tegegn et al.30 A P-value less than 0.05 was taken as the independent significant predictor and Bonferroni corrections were used to correct for multiple testing.
Study Variables
Dependent (Outcome) Variables
The burden, appropriateness, concern about stopping medications, involvement factors, and the two global questions of rPATD were the dependent variables of the study.
Independent Variables
Income, Belief, Number of medications, Comorbidities, Marital status, Sex, Health insurance, Place of residence, Age, Level of education, and Occupation were independent variables entered into the model for the study. Additionally, the burden, appropriateness, concern about stopping medications, and involvement factors scores were used as a predictor variable for the two global questions.
Results
Socio-Demographic and Clinical Characteristics of the Respondents
A total of 196 study participants were approached, and 192 of them completed the questionnaire which give a response rate of 98%. Four questionnaires were discarded due to incompleteness. Of the total number of participants, 34 (17.4%) received 5 and more medications concurrently. The median number of their daily medications was 3 (three). For older adult patients, the three most common reasons to visit the hospital were hypertension 123 (64%), heart failure 54 (28.1%), and diabetes mellitus 48 (25%). One hundred and ten (57.3%) of the older adult patients had health insurance.
The older adult patients had a mean (SD) age of 69.6 (5.3) years. The majority of them were female 51 (51.0%), married 81 (81.0%), protestant 46 (46.0%), farmer 49 (49.0%), urban residence 58 (58.0%), had informal education 54 (54.0%) and lived at home with someone 98 (98.0%) (Table 1).
 |
Table 1 Socio-Demographic and Clinical Characteristics of Study Participants at AURH, from July 25 to August 25, 2021; N=192 |
Caregivers who participated in the study had a mean (SD) age of 33.1 (11.3) years. The majority of them were males 65 (70.7%), protestant 49 (53.3%), married 59 (64.1%), had tertiary education 35 (38.0%), and lived at home with someone 87 (94.6%) (Table 1).
Attitudes Towards Deprescribing
Older Adult Patients’ Perception of Deprescribing
Among a total of 100 older adult patients, 48% of them thought that they spent a lot of money on their medications and 44% of them felt medicines were a burden to them. Besides, 71% of them had a feeling that taking their medicines every day was convenient (Figure 1A). Even though more than 67% of them perceived their medicines were appropriate, the majority of the participants (65%) would like their doctor to reduce the dose of one or more of their medicines (Figure 1B). However, most of the respondents (69%) would worry about missing out on future health benefits if one of their medications was stopped (Figure 1C). In the involvement factor, the majority of the respondents (68%) would like to be involved in making decisions about their medicines with their doctors (Figure 1D). If the doctor said it was possible, 85% of the participants would have the willingness to stop one or more of their regular medications despite a significant number of them (49%) being satisfied with the medications they were taking (Figure 1E).
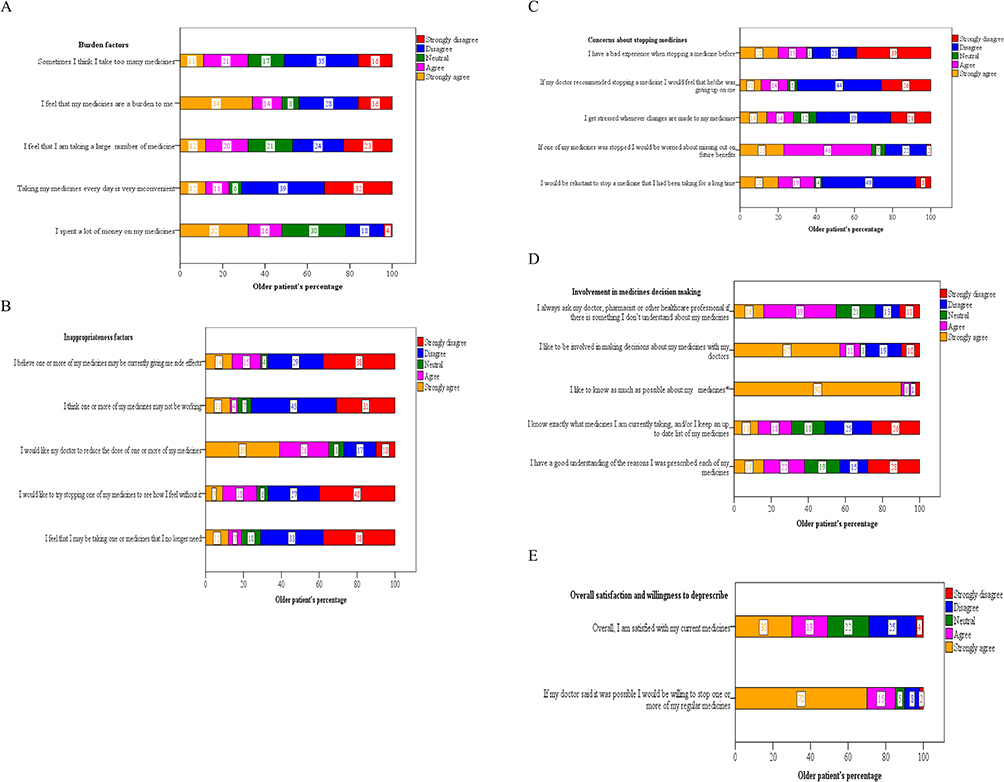 |
Figure 1 (A) Attitudes of older adult patients at AURH towards medication burden factors of revised Patients’ Attitude Towards Deprescribing, n=100. (B) Attitudes of older adult patients at AURH towards inappropriateness of medication factors of revised Patients’ Attitude Towards Deprescribing, N=100. (C) Attitudes of older adult patients at AURH towards concerns about stopping medications of revised Patients’ Attitude Towards Deprescribing, N=100. (D) Attitudes of older adult patients at AURH towards involvement in medicine decision making of revised Patients’ Attitude Towards Deprescribing, N=100. *Neutral = 0.0%; *Strongly disagree = 3%. (E) Attitude of older patients at AURH towards overall satisfaction, and willingness to deprescribe of revised Patient Attitude Towards Deprescribing, N=100. Note: This is the results of the translated version of the revised Patients’ Attitude Towards Deprescribing (rPATD) questionnaire with permision from the authors: Reeve, Emily, et al “Development and validation of the Revised Patients’ Attitudes Towards Deprescribing (rPATD) questionnaire: Versions for Older Adults and Caregivers” Drugs and aging. 2016;33(12):913-928. Translated into Afaan Oromo in June 2021 by two individuals in the research team.32 |
Caregivers’ Perception Towards Deprescribing
The majority of caregivers agreed or strongly agreed with all the questions about the burden and involvement factors (Figure 2A and D). More than half of caregivers (52.2%) would like the doctor to reduce the dose of one or more of their care recipient’s medicines (Figure 2B). In addition, 69.6% of caregivers said they did not think their doctors were giving up on them if they suggested stopping one of their care recipient’s prescriptions (Figure 2C). The majority of them (77.2%) would accept the doctor’s recommendations to deprescribe at least one of their care recipient’s medicines despite their overall satisfaction (53.3%) with the medicines their care recipients were taking (Figure 2E).
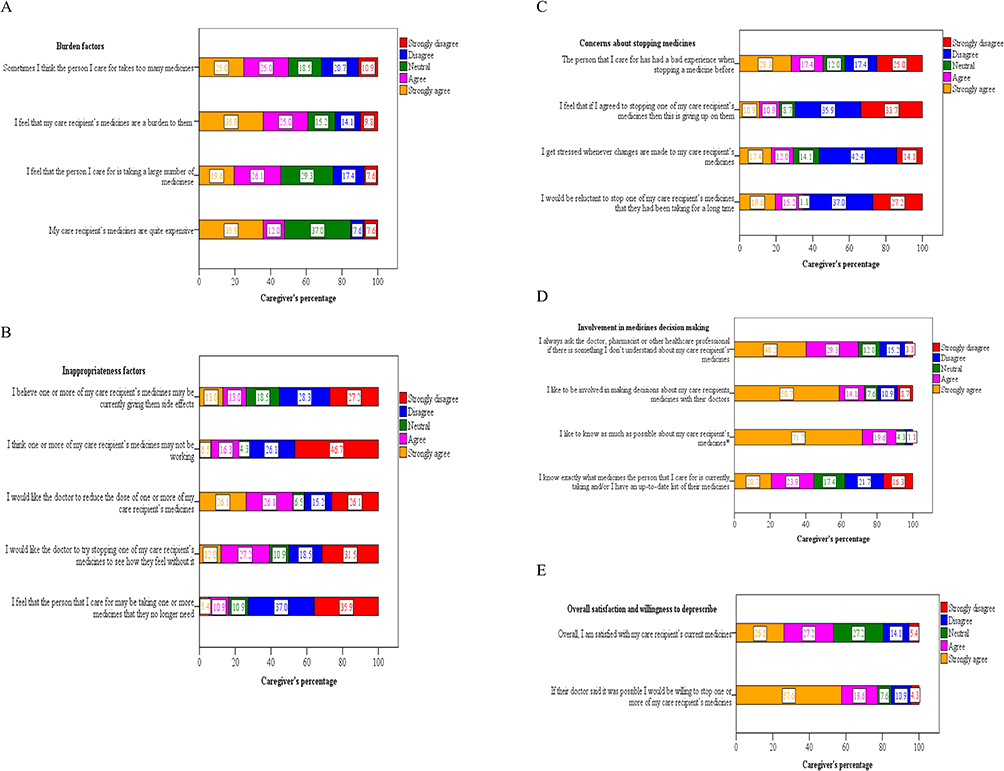 |
Figure 2 (A) Attitudes of caregivers at AURH towards medication burden factors of revised Patients’ Attitude Towards Deprescribing, N=92. (B) Attitudes of caregivers at AURH towards inappropriateness of medication factors of revised Patients’ Attitude Towards Deprescribing, N=92. (C) Attitudes of caregivers at AURH towards concerns about stopping medications of revised Patients’ Attitude Towards Deprescribing, N=92. (D) Attitudes of caregivers at AURH towards involvement in medicine decision making of revised Patients’ Attitude Towards Deprescribing, N=92. *Disagree = 3.3%. (E) Attitude of caregivers at AURH towards overall satisfaction, and willingness to deprescribe of revised Patients’ Attitude Towards Deprescribing, N=92. Note: This is the results of the translated version of the revised Patients’ Attitude Towards Deprescribing (rPATD) questionnaire with permision from the authors: Reeve, Emily, et al “Development and validation of the Revised Patients’ Attitudes Towards Deprescribing (rPATD) questionnaire:Versions for Older Adults and Caregivers” Drugs Aging. 2016; 33(12) :913-928. Translated into Afaan Oromo in June 2021 by two individuals in the research team.32 |
An overall aggregate factor score showed that the study participants (ie, older adult patients and their caregivers) had a neutral position in their attitude (ie, the overall mean score was between 2.6 and 3.59) regarding perceived burden and concerns about stopping medication despite 77 (40.1%) of them perceived that they were burdened by their medications. The majority disagreed with the inappropriateness of their medications (ie, the overall mean score was between 1.0 and 2.59), and they would like to involve actively in their medications decision-making (ie, the overall mean score was between 3.6 and 5.0). Besides, 156 (81.3%) of the respondents agreed to stop one or more of their regular medications if the physicians said it was safe to do so although 98 (51.0%) of them were satisfied with the medications they were taking (Table 2).
 |
Table 2 Aggregate Factor Score on the General Attitudes Toward Deprescribing Among Study Participants at AURH, from July 25 to August 25, 2021; N=192 |
Influence of Patient Sociodemographic and Clinical Characteristics on Attitudes Towards Deprescribing
The perceived burden of medication was decreased as age increased (B=−0.01, 95% CI = −0.017- −0.004, P = 0.001), and being a female was also associated with the lower perceived burden of medication (B=−0.288, 95% CI = −0.542- −0.052, P = 0.027). But when the patients’ medicine intake increased, there was a greater chance that they would feel the medication’s burden (B = 0.280, 95% CI = 0.196–0.365, P < 0.001) (Table 3).
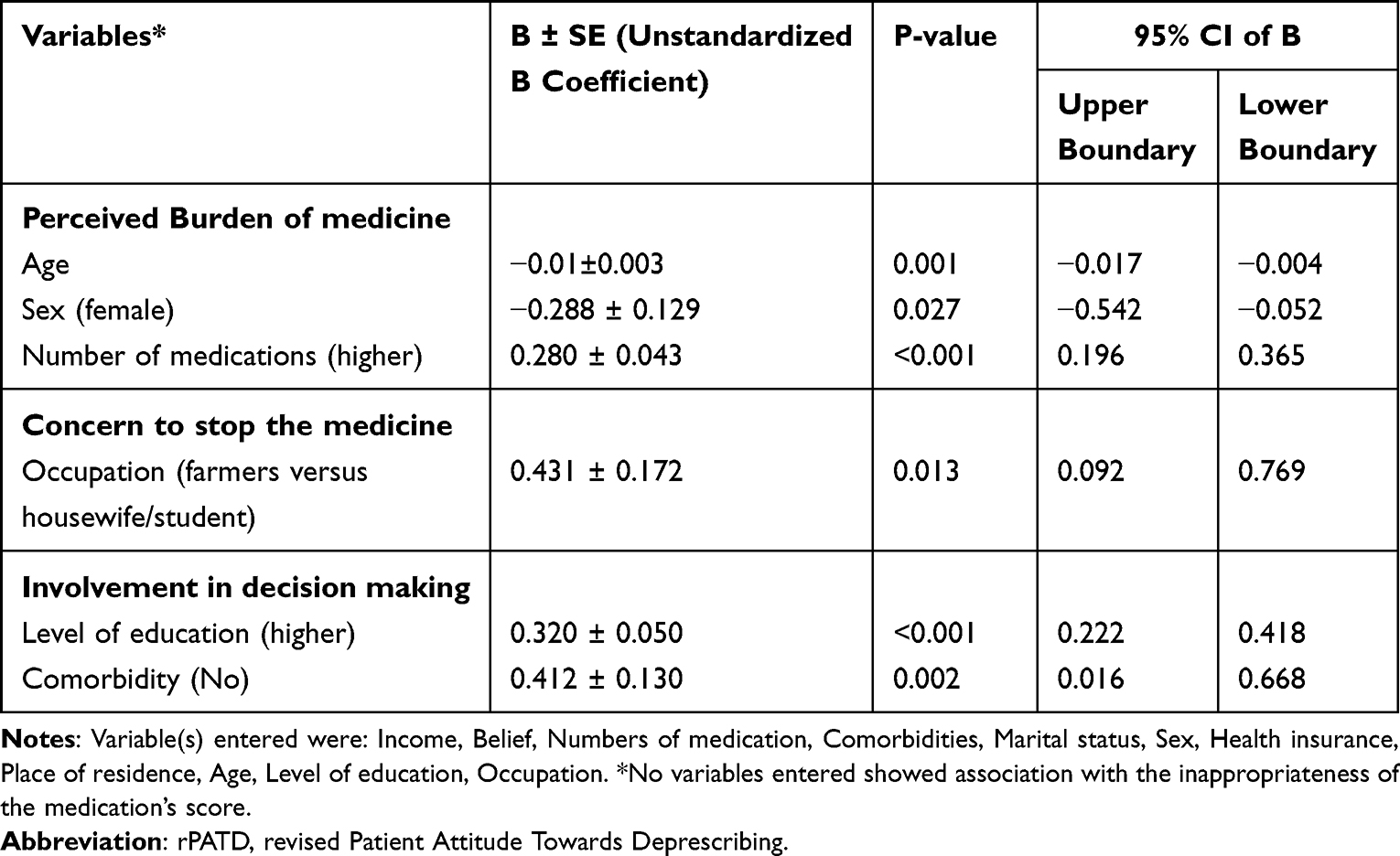 |
Table 3 Association of Socio-Demographics and Clinical Variables with the Four Factors Scales of the rPATD on the Backward Linear Regression Model Among the Study Participant at AURH, from July 25 to August 25, 2021; N=192 |
Patients’ socio-demographic and clinical characteristics included in this study showed no association with the inappropriateness of the medication’s domain. Being a farmer (B = 0.431, 95% CI = 0.092–0.761, P = 0.013) was the sole predictor linked with concerns about quitting the drug Besides, having higher education level (B = 0.320, 95% CI = 0.222–0.418, <0.001), and having no comorbidity (B = 0.412, 95% CI = 0.002–0.016, P = 0.002) were the two independent factors that strongly linked with the willingness to involve in medication’s decision making (Table 3).
The backward binary logistics regression analysis identified two independent factors that were significantly associated with willingness to discontinue at least one of the medications and one independent factor for satisfaction with the medications they were taking. As a result, being single in marital status and having a higher score of concerns to stop their regular medication decreases the likelihood of deprescribing at least one of their medications by 76.2% (AOR = 0.238, 95% CI = 0.063–0.901, P = 0.035) and 56% (AOR = 0.440, 95% CI = 0.262–0.741, P = 0.002) than their counterparts respectively. On the other hand, an increase in the score for the medication’s perceived inappropriateness reduces their overall satisfaction with the medications they were taking by 34.7% (AOR = 0.653, 95% CI = 0.456–0.936, P = 0.020) (Table 4).
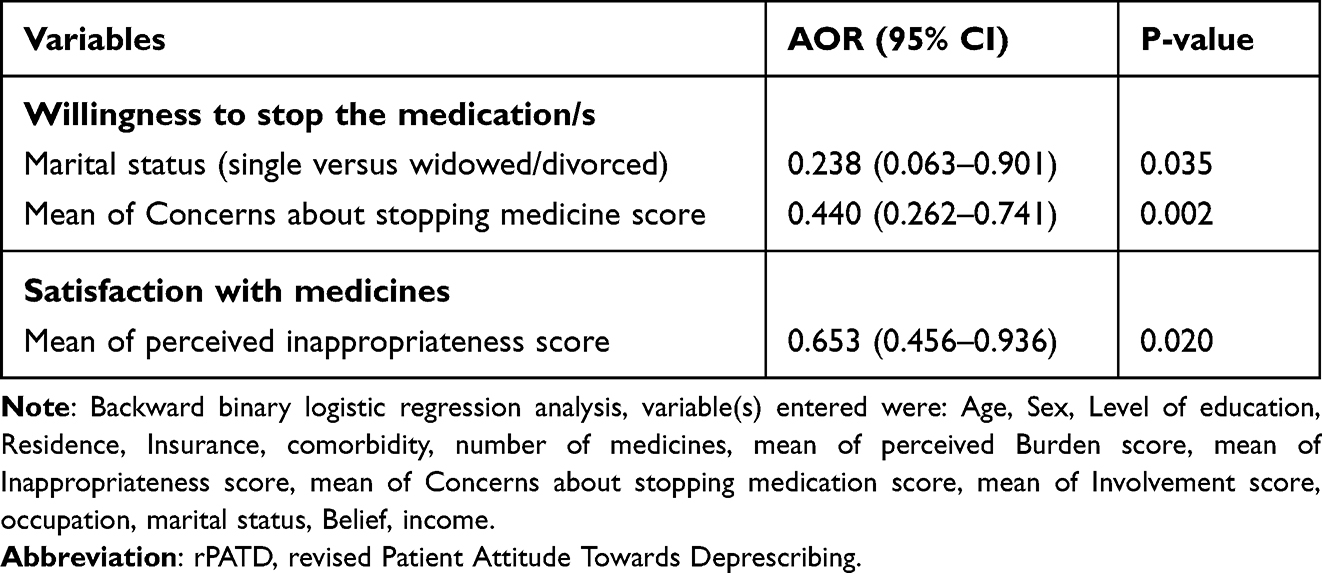 |
Table 4 Association of Socio-Demographics and Clinical Variables with the Two Global Questions of the rPATD on the Backward Binary Logistic Regression Model Among the Study Participant at AURH, from July 25 to August 25, 2021; N=192 |
Discussion
The global population is aging rapidly and older adult patients are at the greatest risk for drug-related harm.35 They are at greater risk of multimorbidity and thus complicated prescriptions that led to polypharmacy and potentially inappropriate medications.36 According to Planelles and his co-authors most recent meta-analysis37 on older adult patients, PIM prevalence was extremely high (87.7%).The occurrence of PIM is mostly attributed to aging, comorbidities, and polypharmacy, according to numerous research.37,38 PIM is also linked to a higher risk of falling, hospitalization, mortality, a general decline in quality of life, and other negative drug events in older adult people.39–41
Deprescribing is a crucial and efficient strategy for minimizing PIM usage and preventing harmful medication events or outcomes in older adult patients. Deprescribing entails lowering medicine doses, terminating unsuitable pharmacological therapy, and selecting other, safer therapies.35,42,43 However, since deprescribing often entails beyond-protocol decision-making and complex process, it will cause anxiety and concern for clinicians and patients.17,41 Hence, to begin the deprescribing process, patients and healthcare professionals should come to an understanding30 that calls for investigating the perspectives of older adult patients or caregivers on deprescribing.
Polypharmacy is on the rise globally as a result of aging and multimorbidity in older adult patients.1,35,37 Similar to research by Tegegn et al30 and Liew et al,41 the median number of patients in our study taking daily drugs was three (range: 1–6). But when compared to other studies, such as those by Kua et al11 and Achterhof et al,44 which reported the mean of daily medicine as 5.7 and 8.00, respectively, it was remarkably low. The availability of medication, prophylactic use, life expectancy, and the multimorbidity disparity between low-income individuals could all contribute to this gap.
According to the definition used, the prevalence of polypharmacy ranged from 4 to 57% in a review by Jordan Guillota et al.2 Additionally, Delara et al45 indicated that the prevalence of polypharmacy among adult patients older than 65 years was 45% in a systematic review and meta-analysis study. Even in high-income nations, it is sometimes reported to reach as high as 60%.46 Our finding appeared to be lower, 34 (17.4%). This might be partially explained by differences in the study population, since, in our case, about half of the older patients lacked comorbidity. Furthermore, the advent of evidence-based medicine; the increase in multimorbidity and longevity; access to an increasing number of treatments, and the increasing expectations for treatment from patients and their caregivers are among the factors highlighted to increasing polypharmacy.1
The percentage of older adult patients and/or their caregivers who were willing to deprescribe at least one of the drugs used to manage polypharmacy and the usage of PIM ranged from 49 to 98%.33,47,48 Our finding was within the reported range (ie, 85%). However, other studies conducted across the world, including those in Nepal (54.7%),24 Japan (67.8%),49 Switzerland (74.3%)44 and (77.0%),50 in Gondar city, Ethiopia (81.6%),30 in Malaysia (82.7%),51 in Singapore (83.0%),11 Quebec, Canada (84.5%),52 in Netherlands (88.0%)34 and (92.0%),53 in Italy (89.0%),54 in Canada (93.0%)23 and in the UK (97.3%)55 showed differences in the willingness of older adult patients to deprescribe their medications if their physician said it was possible.
We noted that older adult persons’ willingness to discontinue their medications extends to their caregivers as well (ie, 77.2%). The prevalence of caregivers’ attitudes towards willingness to discontinue their care recipients’ medications was reported to be 49–94%.33 Studies from Malaysia (65.4%),51 Quebec, Canada (70.5%)52 and UK (80.5%)55 have shown a difference in caregivers’ willingness to discontinue their care recipients’ medications. Moreover, we observed the difference in willingness to discontinue the medications between the older adult patients and caregivers (ie, 85% versus 77.2%) which might be due to the preference of caregivers to play a passive role in medical decision-making for their care recipients.33
The report of various results across the globe regarding the willingness of older adult patients or caregivers towards discontinuing medication might arise from the type of health care setting, geographical location, the use of specific medication, the number of medications involved, multimorbidity, the type of health care professionals initiating the process, the socioeconomic status the country, the number of visits the medical institution, the level of education, age, the level of effective communication with health care professionals and the type of population included.49,50,56–59 We also witnessed that the majority of the studies conducted in high-income countries have reported a higher willingness to discontinue their medications than those conducted in low to middle-income countries including Ethiopia. These disparities could be due to higher health literacy among patients living in high-income countries than others.60,61
We found that being satisfied 51% of the study participants, who reported being satisfied with the medication they were taking did not let that stop them from considering stopping at least one of their medications if their physician suggested it. This paradox was also confirmed by other authors.11,30,34 This will demonstrate how poorly the rPATD tool predicts whether a patient intends to stop taking their medication.33 Therefore, doctors should not rely exclusively on patients’ contentment with their medications because this may not be sufficient to find pertinent deprescribing chances.52 Also, it is recommended that the two general questions of the rPATD be interpreted in conjunction with the other domains rather than separately,33 since this may help to avoid misunderstandings.
According to our study’s findings about rPATD burden factors, roughly half of older adult patients and their caregivers believed that they had to spend a lot of money on their medications. However, the majority of older adult patients (71.0%) were feeling that taking their medicines every day is convenient despite a higher willingness to stop taking medications. Economic factors should therefore always be taken into account when choosing medications and providing care for older adult patients, as they need lengthier attention, various prescriptions, and a lower level of production to pay for their therapeutic expenditures.30 The substantial significance that deprescribing plays in helping patients save money is something that healthcare practitioners should also discuss.62
More than half of the study subjects in both groups wanted their doctors to lower the dosage of one or more of their prescription drugs. Even so, they are reluctant to quit taking one or more of the drugs they were taking (ie, 57% of older adult patients and 64.2% of caregivers). However, more than two-thirds of them continued to feel that they were taking the right medicine and expressed concern about losing out on any potential future benefits if their treatment had ended. This gives a clue that patients should be informed that some medications may be stopped if they exhibit side effects, provide no benefit, or are no longer necessary.63 Moreover, deprescribing is safe, feasible, well-tolerated, and has significant advantages62 including lowering morbidity and mortality, improving quality of life, lowering hospital admissions, lowering the risk of falls, and improving mental status.18,39,64
More importantly, the majority of the study participants (≥56.5%) would not get stressed if changes had been made to their medication regimen. Seemingly, they would not consider the doctors giving up on them if the doctors recommended stopping at least one of their medications. These reflect that patients were willing to have medications deprescribed and that older adult patients/caregivers trust their medical provider for deprescribing. As a result, the healthcare provider should proactive and build trust and relationships with their patients or caregivers for shared informed decisions to initiate a process of deprescribing65,66 by utilizing different standard guidelines such as beer’s criteria9 and STOPP/START criteria.10
Interestingly, in the current study, more than 90% of the participants said they wanted to know as much as they could about their medications. However, a significant number of the participants (ie, ≥40%) either did not know the exact medicine they were taking or had no good understanding of the reason their medicines were prescribed for. Similarly, similar results were reported by Tegegn et al30 and Graabaek et al.67 These can be one of the obstacles to starting the process of deprescribing with patients or caregivers. Therefore, since deprescribing is an essential part of prescribing,64 the discussion needs to start at the beginning of medication use (ie, when negotiating with the patients to start the medicine) rather than when considering discontinuing.17
The majority of respondents (55% of the older adult patients and 69.5% of the caregivers) said they would like to ask their doctors, pharmacists, or other healthcare providers if there is any misunderstanding regarding their drugs to have a thorough understanding. This suggests that older adult patients and their caregivers want to be informed about their drugs, ask their doctor questions, and participate in clinical decision-making.30 This is crucial to the patient-provider connection because it emphasizes the concepts of trust, confidence in professionals, and shared decision-making, all of which are essential for better patient outcomes.17,30,66
The idea of the patient-provider relationship is crucial, as two-thirds of the survey participants wanted to actively participate in the decision-making process with their healthcare professionals. A study also indicated that the process of deprescribing would be facilitated by having a positive relationship with the physicians.50 Deprescribing may therefore be facilitated in part by efforts to promote caregivers’ and older adult patients’ involvement in medication use.4,11
In general, older adult patients and their caregivers are open to discussion about deprescribing and even they seek opportunities to commence communication about deprescribing with healthcare professionals.65 Healthcare professionals should not downplay their importance as they are the ones that start the deprescribing process.67 Therefore, in their regular clinical practice, doctors should take into account and provide a chance for dialogue about deprescribing with elder patients or caregivers.11,33,65,66 At the same time, the discussions about deprescribing need to be tailored to individual patients’ circumstances17 such as life expectancy, the disease or medicine being discussed, the patient’s level of frailty, and their views.22,53,62,66,67
On aggregate factors score, the study participants are ambivalent regarding the perceived burden of the medications and the concerns regarding stopping one or more of their medications even though they believed that they had received appropriate medications. Besides, they are eager to be actively involved in medicine decision-making with their healthcare provider. Therefore, health professionals should use a patient-centered approach to weigh the risks and benefits of every medicine against the particular goals of the older adult patient’s treatment, to reduce the overall number of drugs administered11 At the same time, the physicians need to aware about the risk of the patients being feeling well on their current medicines and being convinced that they need all their medicines, which might create barriers to deprescribing.50
Our current investigation discovered several variables influencing several rPATD domains. Global research on the elements that contribute to deprescribing has shown mixed results.24,34,50,52 However, in our study, it was shown that patient sociodemographic and clinical variables had an impact on attitudes toward the perceived burden of the drug, concerns about stopping, and involvement in medicine decision-making apart from the perceived inappropriateness of medications. Accordingly, younger age, female sex, and receiving a higher number of medicines were associated only with a higher perceived burden of the medication.
Being a farmer in occupation was associated with patients’ general concerns about stopping medications. Level of education (ie, higher level) and having no comorbidity were associated with the eagerness of being involved in medicine decision-making score. A study in Singapore also indicated that having higher educational background increases their seeking for involvement in medical decision-making11 which might relate to the health literacy status of the patients.60
For the two general questions of rPATD in our study, we noticed that having higher perceived concerns for stopping the medication and the perceived level of medication inappropriateness affect the patients’ and/or caregivers’ willingness to discontinue the medication and overall satisfaction with the medication respectively. Shrestha et al18 and other authors53 also reported that the perceived level of concerns regarding stopping medication affects the willingness to deprescribe. In our case, factors like age, sex, and the number of medications the patient received seemed not to affect the willingness of the older adult patients to deprescribe. And similar findings were reported by different authors33,34,50 though conflicting results reported in studies by Shrestha et al and Aoki et al.18,49 Hence, healthcare providers ought to decrease the patients’ concern about stopping medication by building trust with their patients and communicating evidence about the risks of medication use and medication discontinuation.18,50 Hence, healthcare providers ought to decrease the patients’ concern about stopping medication by building trust with their patients and communicating evidence about the risks of medication use and medication discontinuation.18 Deprescribing is not always associated with PIM usage because patients are not always aware of the unnecessary drug, therefore it is equally necessary to address the perceived inappropriateness of particular medications.47
Strength and Limitation
The study is the first in assessing the attitudes of both older adult patients and caregivers toward deprescribing among older adult patients with chronic disease in Ethiopia. And we believe that we generated knowledge that may be used as a base to educate future deprescribing actions and contribute to the implementation of shared decision-making in medication optimization activities. However, the results might need careful interpretation for generalizability as this study was conducted in a selected single hospital. So, further exploration might be needed to clarify whether the attitudes among older adult patients and caregivers in other parts of Ethiopia remain the same. Moreover, we could not determine the discordance between older adult patients and caregivers as both were not paired. Besides, this study did not include the perspectives of the doctors, pharmacists, and other concerned health professionals regarding deprescribing which could have helped us to gather more information about the topic.
Conclusion
The majority of the older adult patients and caregivers would be willing to have one or more of their or their care recipients’ regular medications deprescribed if their doctor said it was possible albeit their perceived appropriateness of the medications received. The majority of them would like to involve actively in making decisions about their medicines with their healthcare providers. Having higher perceived concerns for stopping the medication and higher perceived medicine inappropriateness were factors associated with willingness to deprescribe and overall satisfaction with their medicine respectively. Healthcare providers should prompt the deprescribing process with older adult patients and caregivers by addressing their concerns about stopping medications. This may require adopting and/or developing deprescribing guidelines and algorithms in order to undertake deprescribing processes, as even there is no one yet in Ethiopia.
Ethical Declaration
The study was reviewed and approved by Ambo University department of pharmacy with a formal letter (Phar/48/013). Verbal informed consent was taken from the patients and caregivers, and it was approved by the department committee. The data collected were handled with strong confidentiality. In general, the study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge all data collectors for their efforts & colleagues who provided constructive advice in conducting this research. We are also grateful to Ambo University Referral Hospital for allowing us to conduct the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors of this manuscript declare that they have no competing interests.
References
1. Barnett NL, Oboh L, Smith K. Patient-centred management of polypharmacy: a process for practice. Eur J Hosp Pharm. 2015;23:113–117. doi:10.1136/ejhpharm-2015-000762
2. Guillot J, Maumus-robert S, Bezin J. Polypharmacy: a general review of definitions, descriptions and determinants. Therapies. 2020;75:407–416. doi:10.1016/j.therap.2019.10.001
3. Page AT, Clifford RM, Potter K, Schwartz D, Etherton-Beer CD. The feasibility and effect of deprescribing in older adults on mortality and health: a systematic review and meta-analysis. Br J Clin Pharmacol. 2016;82:583–623. doi:10.1111/bcp.12975
4. Jansen J, Naganathan V, Carter SM, et al. Too much medicine in older people? Deprescribing through shared decision making. BMJ. 2016;353. doi:10.1136/bmj.i2893
5. WHO Centre for Health Development (Kobe J). A glossary of terms for community health care and services for older persons. Kobe, Japan: WHO Centre for Health Development; 2004. Available from: https://apps.who.int/iris/handle/10665/68896.
6. Tao L, Qu X, Gao H, Zhai J, Zhang Y, Song Y. Polypharmacy and potentially inappropriate medications among elderly patients in the geriatric department at a single-center in China. Medicine. 2021;100:1–8. doi:10.1097/MD.0000000000027494
7. Masnoon N, Shakib S, Kalisch-ellett L, Caughey GE. What is polypharmacy ? A systematic review of definitions. BMC Geriatr. 2017;230:1–10. doi:10.1186/s12877-017-0621-2
8. Rankin A, Cadogan CA, Patterson SM, et al. Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst Rev. 2018;2018(9). doi:10.1002/14651858.CD008165.pub4
9. Fick DM, Semla TP, Steinman M, et al. American Geriatrics Society 2019 updated AGS beers criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
10. O’mahony D, O’sullivan D, Byrne S, O’connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015;44(2):213–218. doi:10.1093/ageing/afu145
11. Kua CHH, Reeve E, Tan DS, et al. Patients’ and caregivers’ attitudes toward deprescribing in Singapore. J Gerontol A Biol Sci Med Sci. 2021;76(6):1053–1060. doi:10.1093/gerona/glaa018
12. Mallet L, Spinewine A, Huang A. The challenge of managing drug interactions in elderly people. Lancet. 2007;370(9582):185–191. doi:10.1016/S0140-6736(07)61092-7
13. Hajjar ER, Cafiero AC, Hanlon JT. Polypharmacy in Elderly Patients. Am J Geriatr Pharmacother. 2007;5:345–351. doi:10.1016/j.amjopharm.2007.12.002
14. Secora A, Alexander GC, Ballew SH, Coresh J, Grams ME. Kidney function, polypharmacy, and potentially inappropriate medication use in a community-based cohort of older adults. Drugs Aging. 2018;35(8):735–750. doi:10.1007/s40266-018-0563-1
15. Wallace E, Salisbury C, Guthrie B, Lewis C, Fahey T, Smith SM. Managing patients with multimorbidity in primary care. BMJ. 2015;350. doi:10.1136/bmj.h176
16. Nwadiugwu MC. Frailty and the risk of polypharmacy in the older person: enabling and preventative approaches. J Aging Res. 2020;2020:1–6. doi:10.1155/2020/6759521
17. Turk A, Wong G, Mahtani KR, et al. Optimising a person - centred approach to stopping medicines in older people with multimorbidity and polypharmacy using the DExTruS framework: a realist review. BMC Med. 2022;297:1–18. doi:10.1186/s12916-022-02475-1
18. Shrestha S, Poudel A, Cardona M, Steadman KJ, Nissen LM. Impact of deprescribing dual-purpose medications on patient-related outcomes for older adults near end-of-life: a systematic review and meta-analysis. Ther Adv Drug Saf. 2021;12:1–16. doi:10.1177/20420986211052343
19. Gillespie RJ, Harrison L, Mullan J. Deprescribing medications for older adults in the primary care context: a mixed studies review. Health Sci Rep. 2018;1(7):e45. doi:10.1002/hsr2.45
20. Halli-Tierney AD, Scarbrough C, Carroll D. Polypharmacy: evaluating risks and deprescribing. Am Fam Physician. 2019;100(1):32–38.
21. Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: the process of deprescribing. JAMA Intern Med. 2015;175(5):827–834. doi:10.1001/jamainternmed.2015.0324
22. Triantafylidis LK, Hawley CE, Perry LP, Paik JM. The role of deprescribing in older adults with chronic kidney disease. Drugs Aging. 2018;35:973–984. doi:10.1007/s40266-018-0593-8
23. Reeve E, Wolff JL, Skehan M, Bayliss EA, Hilmer SN, Boyd CM. Assessment of attitudes toward deprescribing in older medicare beneficiaries in the United States. JAMA Intern Med. 2018;178(12):1673–1680. doi:10.1001/jamainternmed.2018.4720
24. Shrestha SS, Giri R, Sapkota HP, et al. Attitudes of ambulatory care older Nepalese patients towards deprescribing and predictors of their willingness to deprescribe. Ther Adv Drug Saf. 2021;12:1–11. doi:10.1177/20420986211019309
25. Reeve E, Shakib S, Hendrix I, Roberts MS, Wiese MD. Review of deprescribing processes and development of an evidence-based, patient-centred deprescribing process. Br J Clin Pharmacol. 2014;78(4):738–747. doi:10.1111/bcp.12386
26. Sirois C, Ouellet N, Reeve E. Community-dwelling older people’s attitudes towards deprescribing in Canada. Res Soc Admin Pharma. 2017;13(4):864–870. doi:10.1016/j.sapharm.2016.08.006
27. Anderson K, Stowasser D, Freeman C, Scott I. Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: a systematic review and thematic synthesis. BMJ Open. 2014;4(12):e006544. doi:10.1136/bmjopen-2014-006544
28. Farrell B, Tsang C, Raman-wilms L, Irving H. What are priorities for deprescribing for elderly patients ? Capturing the voice of practitioners: a modified delphi process. PloS One. 2015;1–16. doi:10.1371/journal.pone.0122246
29. Gebreyohannes AS, Emayehu FD. Prevalence of polypharmacy and risks of potentially inappropriate medication use in the older population in a developing country: a systematic review and meta-analysis. Gerontology. 2021. doi:10.1159/000516075
30. Tegegn HG, Tefera YG, Erku DA, et al. Older patients’ perception of deprescribing in resource-limited settings: a cross-sectional study in an Ethiopia university hospital. BMJ Open. 2018;8(4):20590. doi:10.1136/bmjopen-2017-020590
31. Bhagavathula AS, Gebreyohannes EA, Fialova D. Prevalence of polypharmacy and risks of potentially inappropriate medication use in the older population in a developing country: a systematic review and meta-analysis. Gerontology. 2021;68:136–145. doi:10.1159/000516075
32. Reeve E, Low LF, Shakib S, Hilmer SN. Development and validation of the revised Patients’ Attitudes Towards Deprescribing (rPATD) questionnaire: versions for older adults and caregivers. Drugs Aging. 2016;33:913–928. doi:10.1007/s40266-016-0410-1
33. Chock YL, Wee YL, Gan SL, Teoh KW, Ng KY, Lee SWH. How willing are patients or their caregivers to deprescribe: a systematic review and meta-analysis. J Gen Intern Med. 2021;36(12):3830–3840. doi:10.1007/s11606-021-06965-5
34. Crutzen S, Abou J, Smits SE, et al. Older people’s attitudes towards deprescribing cardiometabolic medication. BMC Geriatr. 2021;366:1–12. doi:10.1186/s12877-021-02249-z
35. Rochon PA, Petrovic M, Cherubini A, et al. Polypharmacy, inappropriate prescribing, and deprescribing in older people: through a sex and gender lens. Lancet Healthy Longev. 2021;2:e290–e300. doi:10.1016/S2666-7568(21)00054-4
36. Major GL, Mills A, Lowthian JA. Deprescribing attitudes of older adults receiving medication management support from home-based nurses. J Am Geriatr Soc. 2019;67(8):1756–1757. doi:10.1111/jgs.16015
37. Díaz Planelles I, Navarro-Tapia E, García-Algar Ó, Andreu-Fernández V. Prevalence of potentially inappropriate prescriptions according to the new STOPP/START criteria in nursing homes: a systematic review. Healthcare. 2023;422:1–25. doi:10.3390/healthcare11030422
38. Morin L, Laroche ML, Texier G, Johnell K. Prevalence of potentially inappropriate medication use in older adults living in nursing homes: a systematic review. J Am Med Dir Assoc. 2016;17:862.e1–862.e9. doi:10.1016/j.jamda.2016.06.011
39. Kua CH, Mak VSL, Lee SWH. Health outcomes of deprescribing interventions among older residents in nursing homes: a systematic review and meta- analysis. J Am Med Dir Assoc. 2019;20:362–372. doi:10.1016/j.jamda.2018.10.026
40. Krustev T, Milushewa P, Tachkov K. Impact of polypharmacy, drug-related problems, and potentially inappropriate medications in geriatric patients and its implications for Bulgaria—narrative review and meta-analysis. Front Public Health. 2022;743138:1–12. doi:10.3389/fpubh.2022.743138
41. Liew NY, Chong YY, Yeow SH, Kua KP, Saw PS, Lee SWH. Prevalence of potentially inappropriate medications among geriatric residents in nursing care homes in Malaysia: a cross-sectional study. Int J Clin Pharm. 2019;41(4):895–902. doi:10.1007/s11096-019-00843-1
42. Hilmer SN, Gnjidic D. The effects of polypharmacy in older adults. Clin Pharmacol Ther. 2009;85(1):86–88. doi:10.1038/clpt.2008.224
43. Woodward MC. Deprescribing: achieving better health outcomes for older people through reducing medications. J Pharma Pract Res. 2003;33:323–328. doi:10.1002/jppr2003334323
44. Achterhof AB, Rozsnyai Z, Reeve E, et al. Potentially inappropriate medication and attitudes of older adults towards deprescribing. PLoS One. 2020;15(10):1–14. doi:10.1371/journal.pone.0240463
45. Delara M, Murray L, Jafari B, et al. Prevalence and factors associated with polypharmacy: a systematic review and meta-analysis. BMC Geriatr. 2022;601:1–12. doi:10.1186/s12877-022-03279-x
46. Wastesson JW, Morin L, Tan ECK, Johnell K. An update on the clinical consequences of polypharmacy in older adults: a narrative review. Expert Opin Drug Saf. 2018;17(12):1185–1196. doi:10.1080/14740338.2018.1546841
47. Oktora MP, Yuniar CT, Amalia L, Abdulah R, Hak E, Denig P. Attitudes towards deprescribing and patient-related factors associated with willingness to stop medication among older patients with type 2 diabetes (T2D) in Indonesia: a cross-sectional survey study. BMC Geriatr. 2023;23(21):1–11. doi:10.1186/s12877-022-03718-9
48. Weir KR, Ailabouni NJ, Schneider CR, Hilmer SN, Reeve E. Consumer attitudes towards deprescribing: a systematic review and meta-analysis. J Gerontol. 2022;77(5):1020–1034. doi:10.1093/gerona/glab222
49. Aoki T, Yamamoto Y, Ikenoue T, Fukuhara S. Factors associated with patient preferences towards deprescribing: a survey of adult patients on prescribed medications. Int J Clin Pharm. 2019;41(2):531–537. doi:10.1007/s11096-019-00797-4
50. Rozsnyai Z, Jungo KT, Reeve E, et al. What do older adults with multimorbidity and polypharmacy think about deprescribing? The LESS study - a primary care-based survey. BMC Geriatr. 2020;435:1–11. doi:10.1186/s12877-020-01843-x
51. Kua KP, Saw PS, Lee SWH. Attitudes towards deprescribing among multi-ethnic community-dwelling older patients and caregivers in Malaysia: a cross-sectional questionnaire study. Int J Clin Pharm. 2019;41(3):793–803. doi:10.1007/s11096-019-00829-z
52. Rakheja B, Sirois C, Ouellet N, Roux B, Laroche ML. Attitudes toward deprescribing in older adults and caregivers: a survey in Quebec, Canada. J Appl Gerontol. 2022;41(5):1376–1384. doi:10.1177/07334648211069553
53. Edelman M, Jellema P, Hak E, Denig P, Blanker MH. Patients’ attitudes towards deprescribing alpha-blockers and their willingness to participate in a discontinuation trial. Drugs Aging. 2019;36(12):1133–1139. doi:10.1007/s40266-019-00712-6
54. Galazzi A, Lusignani M, Chiarelli MT, et al. Attitudes towards polypharmacy and medication withdrawal among older inpatients in Italy. Int J Clin Pharm. 2016;38(2):454–461. doi:10.1007/s11096-016-0279-4
55. Scott S, Clark A, Farrow C, et al. Attitudinal predictors of older peoples’ and caregivers’ desire to deprescribe in hospital. BMC Geriatr. 2019;19(108). doi:10.1186/s12877-019-1127-x
56. Bužančić I, Dragović P, Pejaković TI, Markulin L, Ortner-Hadžiabdić M. Exploring patients’ attitudes toward deprescribing and their perception of pharmacist involvement in a European country: a cross-sectional study. Patient Prefer Adherence. 2021;15:2197–2208. doi:10.2147/PPA.S323846
57. Lukacena KM, Keck JW, Freeman PR, Harrington NG, Huffmyer MJ, Moga DC. Patients’ attitudes toward deprescribing and their experiences communicating with clinicians and pharmacists. Ther Adv Drug Saf. 2022;13:204209862211164. doi:10.1177/20420986221116465
58. Martinez AI, Spencer J, Moloney M, Badour C, Reeve E, Moga DC. Attitudes toward deprescribing in a middle-aged health disparities population. Res Soc Admin Pharma. 2020;16(10):1502–1507. doi:10.1016/j.sapharm.2020.02.014
59. Oktora MP, Edwina AE, Denig P. Differences in older patients’ attitudes toward deprescribing at contextual and individual level. Front Public Health. 2022;795043:1–7. doi:10.3389/fpubh.2022.795043
60. Howard DH, Sentell T, Gazmararian JA. Impact of health literacy on socioeconomic and racial differences in health in an elderly population. J Gen Intern Med. 2006;21(8):857–861. doi:10.1111/j.1525-1497.2006.00530.x
61. Tang C, Wu X, Chen X, Pan B, Yang X. Examining income-related inequality in health literacy and health-information seeking among urban population in China. BMC Public Health. 2019;19(1). doi:10.1186/s12889-019-6538-2
62. Ibrahim K, Cox NJ, Stevenson JM, Lim S, Fraser SDS, Roberts HC. A systematic review of the evidence for deprescribing interventions among older people living with frailty. BMC Geriatr. 2021;21:258. doi:10.1186/s12877-021-02208-8
63. Hoel RW, Giddings Connolly RM, Takahashi PY. Polypharmacy management in older patients. Mayo Clin Proc. 2021;96(1):242–256. doi:10.1016/j.mayocp.2020.06.012
64. Farrell B, Mangin D. Deprescribing is an essential part of good prescribing. J Am Geriatr Soc. 2015;63(11):2227–2246. doi:10.1111/jgs.13702
65. Kennie-Kaulbach N, Cormier R, Kits O, et al. Influencers on deprescribing practice of primary healthcare providers in Nova Scotia: an examination using behavior change frameworks. Med Access. 2020. doi:10.1177/2399202620922507
66. Lundby C, Glans P, Simonsen T, et al. Attitudes towards deprescribing: the perspectives of geriatric patients and nursing home residents. J Am Geriatr Soc. 2021;69(6):1–11. doi:10.1111/jgs.17054
67. Graabæk T, Lundby C, Ryg J, Søndergaard J, Pottegård A, Nielsen DS. “I simply don’t know, because I don’t know which drugs I get”: perspectives on deprescribing among older adults with limited life expectancy and their relatives. Basic Clin Pharmacol Toxicol. 2021;128(1):115–127. doi:10.1111/bcpt.13476
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.