Back to Journals » Pragmatic and Observational Research » Volume 9
Attitudes and beliefs related to reporting alcohol consumption in research studies: a case from Jordan
Authors Alhashimi FH, Khabour OF ![]() , Alzoubi KH
, Alzoubi KH ![]() , Al-shatnawi SF
, Al-shatnawi SF ![]()
Received 29 April 2018
Accepted for publication 23 August 2018
Published 9 October 2018 Volume 2018:9 Pages 55—61
DOI https://doi.org/10.2147/POR.S172613
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Price
Farah H Alhashimi,1 Omar F Khabour,1 Karem H Alzoubi,2 Samah F Al-shatnawi2
1Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, Jordan
Background: Acceptability of alcohol consumption varies wildly across cultures. Several factors such as religious beliefs and social desirability might influence reporting of such behaviors to researchers during relevant investigations.
Aims: This study aimed at assessing reporting of alcohol consumption during participation in research studies in Jordan, and identifying potential reasons and ethical challenges associated with reporting this behavior.
Subjects and methods: A sample of 400 Jordanians was anonymously surveyed regarding alcohol consumption reporting.
Results: The study showed a tendency of not reporting alcohol consumption in research (56.8%). Religious belief and trust issues regarding reporting sensitive information during participation in research were significantly the main reasons of not reporting alcohol drinking (P<0.05), while social shame effect was limited to rural areas (P<0.05).
Conclusion: Raising Jordanians’ awareness of benefits of reporting alcohol consumption is highly recommended. Improving confidence in privacy and data confidentiality among Jordanians might help in improving the level of reporting during participation in research.
Keywords: ethics, alcohol consumption, reporting, culture, privacy and confidentiality, Jordan
Introduction
Health-related behaviors (such as tobacco use, alcohol use, physical inactivity, and licit or illicit drug use) are considered as primary factors contributing to poor health outcomes, such as cardiovascular diseases and cancer. Studies showed that excessive alcohol consumption is a major risk factor for many health problems such as liver cirrhosis and cancer1–3 and a leading cause of infectious diseases such as tuberculosis and AIDS.4,5 Therefore, assessing such behavior is essential in medical research and clinical practice. Denying and underreporting of alcohol use behaviors may lead to several negative consequences such as manipulating risk curves causing inaccurate etiological fractions of health-related problems,6 inaccurate diagnosis, and interference with early prevention and interventions.
Alcohol consumption is a complex behavior that has multiple determinants. Previous studies have shown that social and cultural factors play a significant role in alcohol use behaviors. In addition to their effect on the actual behaviors of alcohol consumption, these factors may highly influence the acceptability of such behaviors. Compared to different western societies, alcohol consumption is less accepted in the Arabic-Islamic societies. Many studies have shown that religious and sociocultural values are two major factors that often negatively influence alcohol drinking within Muslim societies.7–11 It is clearly stated in the Holy Quran and Al-Hadith, the two major resources for Islamic rules, that drinking alcohol is generally forbidden.12 Thus, Muslim societies view alcohol drinking as a sin. Furthermore, a recent study has reported that alcohol consumption in Islamic countries is highly linked to stigma and social embarrassment.13 Nevertheless, the impact of these factors on the reporting of alcohol consumption during participation in scientific research in Islamic countries has never been studied.
Based on a recently conducted literature review, Ghandour et al14 concluded that epidemiological data regarding alcohol use behaviors in Arabic countries are scattered and the picture on alcohol consumption remains unclear. This review highlighted the needs for more research on alcohol consumption in Arabic countries, as the number of published (peer-reviewed) alcohol-related studies from these countries over the past decades was strikingly low. According to the global report on alcohol consumption by the WHO, high rates of alcohol consumption per capita were reported in several Arabic countries including the UAE, Tunisia, Sudan, and Bahrain. In Jordan, using self-filled questionnaires, alcohol consumption was reported by only 3.0% of university students.2,15,16 In a study by Hadidi et al,17 56.8% alcohol-positive cases among drug abuse–related deaths from forensic pathology reports were reported in Jordan. Thus, alcohol use in Jordan might be higher than what is reported in research studies. In this study, reporting of alcohol consumption within scientific research in a Jordanian sample was investigated. In addition, possible ethical challenges that might influence the reporting of alcohol consumption in Jordan were also examined.
Subjects and methods
Participants and procedure
A sample of 400 Jordanian adults (≥18 years) was solicited to participate in this cross-sectional study. This sample was conveniently recruited from the capital Amman and other urban and rural areas that represent the middle and northern parts of Jordan. Participants were conveniently invited to participate from public places such as gardens, shops, malls, and bus stations. Participants who agreed to participate were asked to complete a voluntary and anonymous questionnaire designed to assess reporting of alcohol consumption in research and the reasons of not reporting. Before participation, potential respondents received a cover letter with a full description of the study purposes, the consequent benefits, and the approximate time (5–10 minutes) needed to fill the questionnaire. Potential participants were assured that participation was voluntary, and that they could refuse to participate or even withdraw at any time without any consequences. Participants were not compelled to provide answers to every survey question but were encouraged to be as complete as possible. The Institutional Review Board of the Jordan University of Science and Technology approved this study. No written informed consent was required for participation in the study. However, completing and returning the survey was deemed an informed consent.
Study measures
A closed-ended questionnaire that assesses the reporting patterns of alcohol consumption and the related ethical challenges among Jordanian population was developed. Four experts in this field, which included a researcher, an ethicist, a physician, and a socialist, tested the instrument’s content validity to ensure that items of this instrument were appropriate to the target construct and assessment objectives within the targeted population. Besides the judgment of the leading experts in the field, the instrument was pilot-tested on 50 participants to ensure clarity and reading comprehensibility. The items used in the measurement tool were adjusted to fit the purposes of the study and the culture of the Jordanian society. Demographic items including direct questions about age, gender, religious beliefs, social position/career, and place of living were included in the questionnaire. To avoid any possible social embarrassment or harms imposed on participants, items related to the reporting patterns of actual alcohol consumption were indirect. All of these questions began with “Suppose you drink Alcohol …” or “Do you think that most people report alcohol consumption…” and were typed/used in culturally appropriate Arabic expressions. Several questions explored possible reasons for not reporting alcohol consumption. They included the following: 1) social measure, which was explored by asking the participants to report alcohol consumption when they knew the researcher or were living in a country where alcohol consumption was culturally acceptable; 2) religious measure that was explored by asking the participants whether declaring alcohol consumption is religiously accepted; and 3) trust level between researchers that involves privacy, confidentiality, and misuse of information. The questionnaire is available upon request.
Statistical analysis was conducted using SPSS® version 24 for windows (IBM Corporation, Armonk, NY, USA). Demographic data and categorical variables were summarized using frequency tables. Chi-squared test was used to measure differences between variables. A P-value of <0.05 was considered statistically significant for all applied statistical tests.
Results
Demographic characteristics
A total of 400 Jordanians participated in this study with 44.8% male and 55.2% female. The response rate of the questionnaire was 95.2%. About 38.7% of the participants were aged 18–34.9 years and 61.2% were aged ≥35 years. The majority of the participants were Muslims (88.5%). More than two-thirds of the participants (71.5%) were living in urban areas, 16.3% in rural areas, and 12.3% in Amman.
Reporting of alcohol consumption in research studies
Of the 400 participants, 56.8% reported that they believed most people would not report alcohol consumption during participation in scientific research studies. This percentage was slightly higher than that of participants who reported the opposite belief (43.2%). Muslims and participants from rural areas were most likely to think that most people will not report their actual alcohol consumption behaviors to the research team (P<0.05, Table 1).
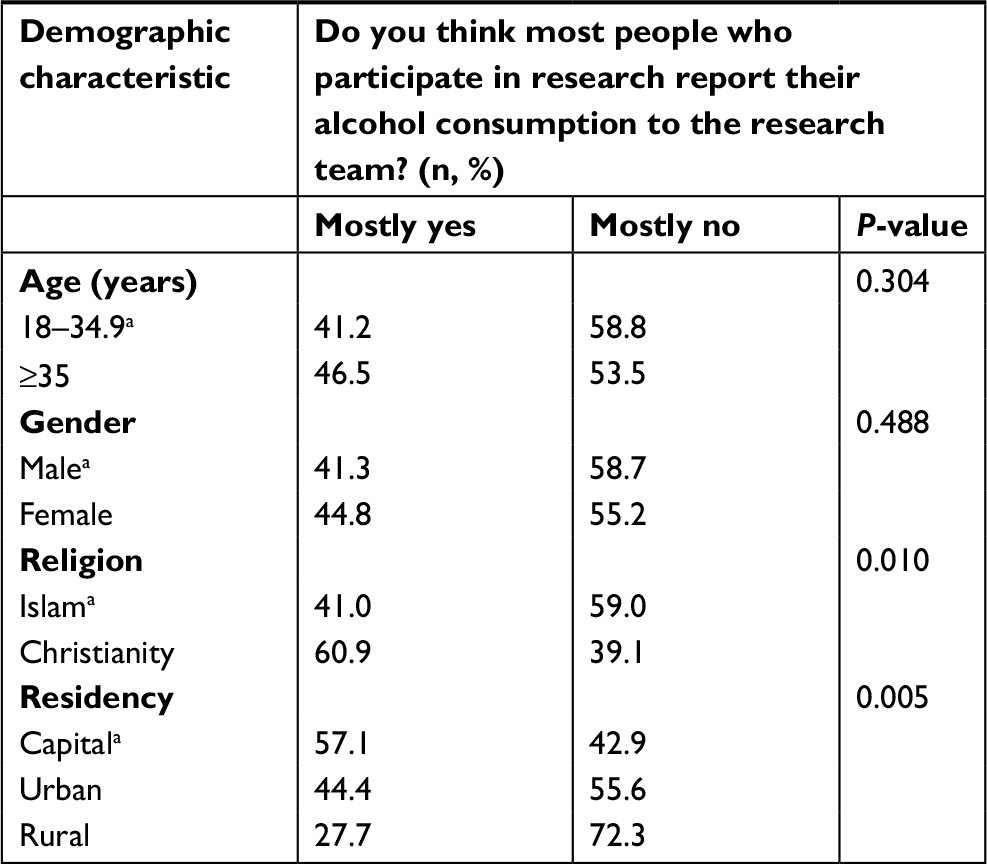 | Table 1 Reporting of alcohol consumption when participation in scientific research according to demographic characteristics Note: aReference group. |
Factors associated with reporting of alcohol consumption in research
Table 2 presents the religious and social factors associated with reporting of alcohol consumption in research. The majority of the participants (92.7%) considered that reporting alcohol consumption was Haram “forbidden” and doubled the sin of consumption, which prevented them from reporting. About two-thirds of the participants refused reporting of alcohol consumption even if they move to a country where drinking alcohol is a part of culture and norms. This refusal was significantly higher among participants aged ≥35 years (P<0.05).
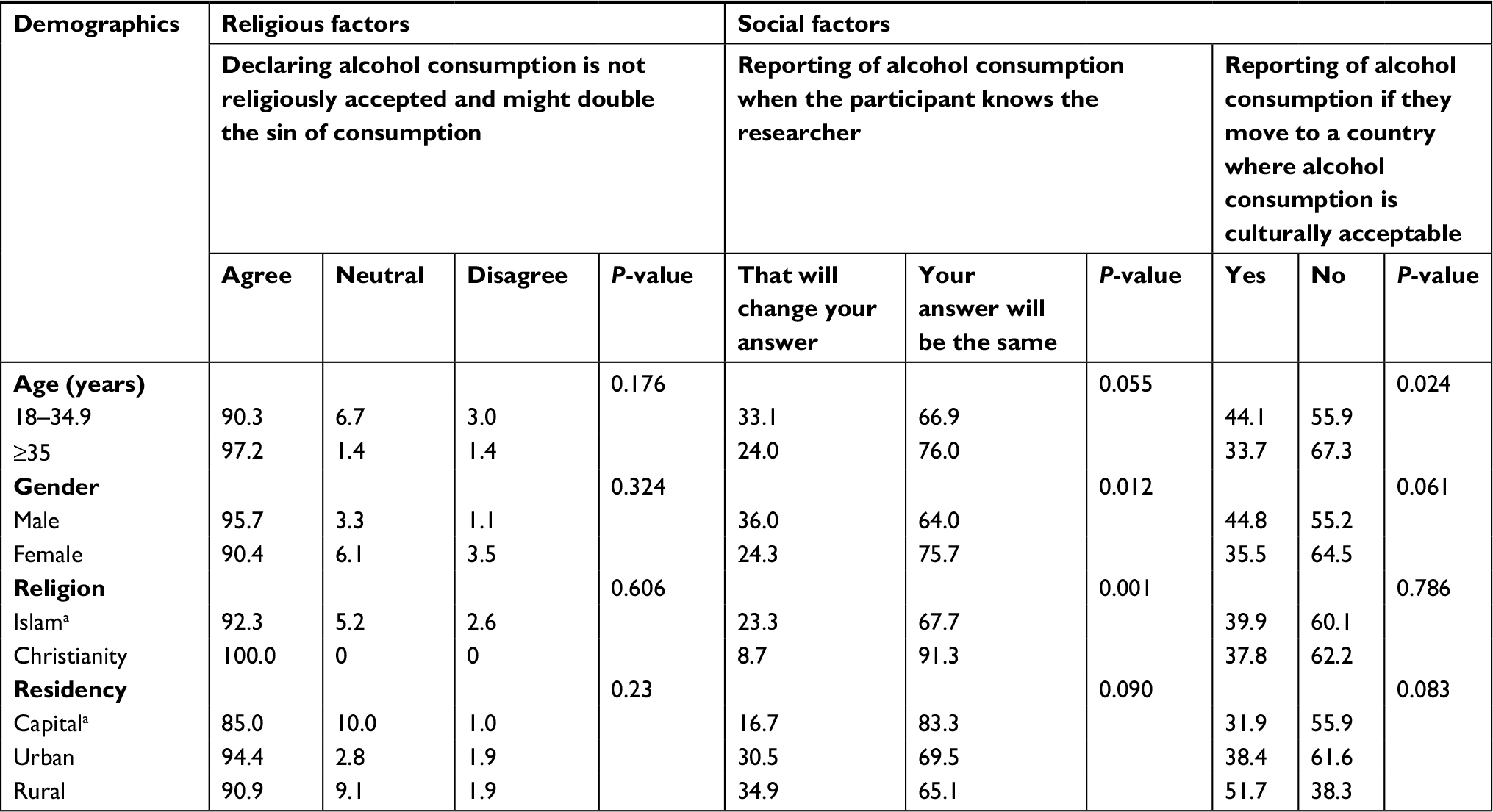 | Table 2 Factors that affect reporting of alcohol consumption in research according to demographic characteristics (N=400, %) Note: aReference group. |
Regarding the social domains, most participants (70.5%) indicated that knowing the researcher was not significantly associated with their answer about their actual alcohol consumption behaviors. Table 2 shows that Christians (P<0.001) and female participants (P<0.05) were most likely to report alcohol consumption even if they personally knew the researcher. Furthermore, current results showed that drinking alcohol in public was not acceptable for 88.4% of the participants because of religious reasons (63.5%) and social reasons (26.1%).
Table 3 shows the relationship between the participants’ trust in the research team and their viewpoint about reporting of alcohol consumption behavior during participation in a research. Participants with low trust levels (8.1%) were most likely to believe that most people will not report their actual alcohol consumption to the research team because of the belief that their data would not be kept confidential (P<0.05) and their fear of data misuse by the research team or any other body (P<0.05). In addition, of the 55.7% participants with high trust levels in the research team, half reported most people have similar doubts regarding their data privacy and fears of data misuse (P<0.05).
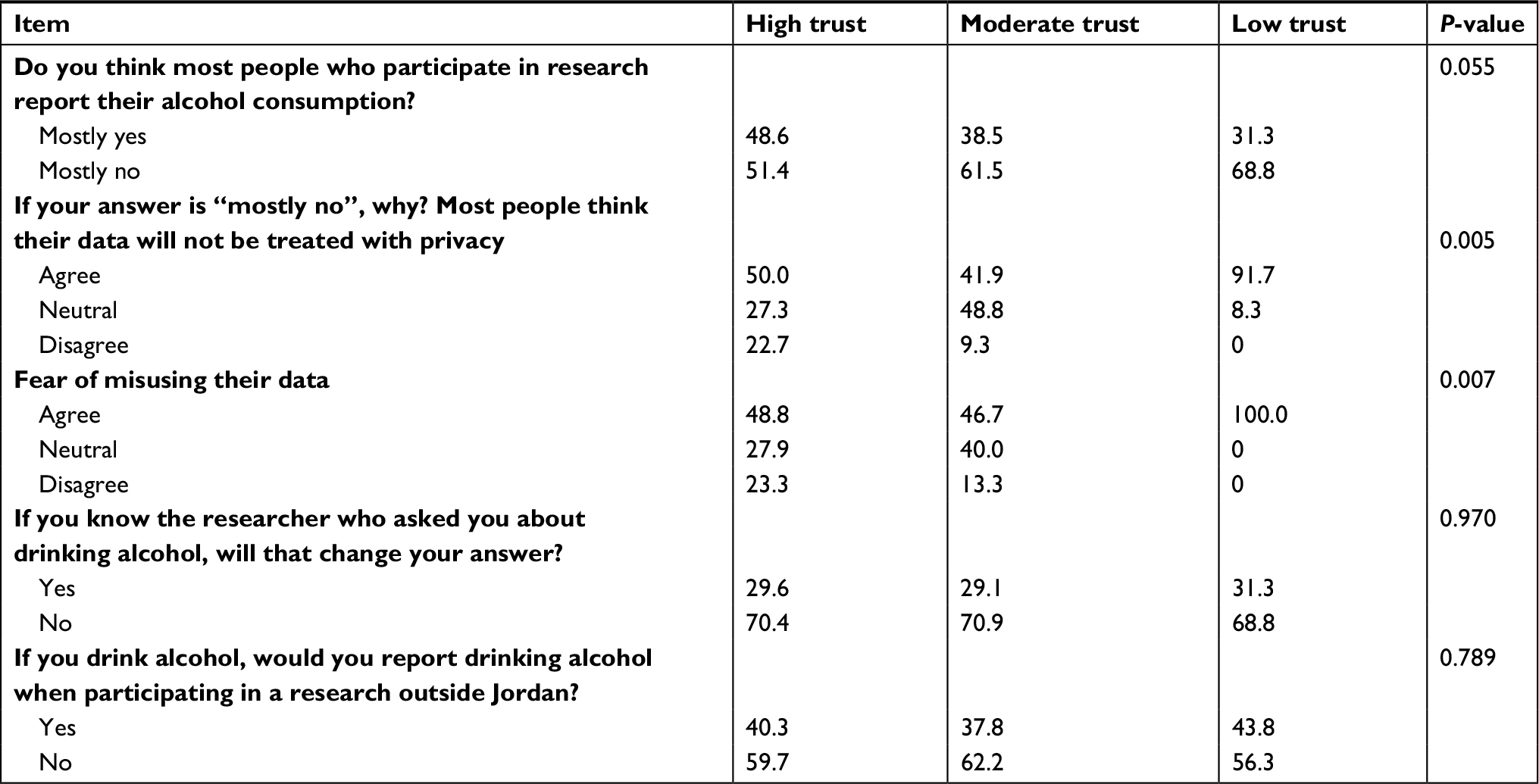 | Table 3 Reporting of alcohol consumption when participation in scientific research according to the trust degree of the research team (N=400, %) |
Discussion
The study examined the attitudes and beliefs related to reporting alcohol consumption in research studies in Jordan. The results showed that the prevalence of not reporting alcohol consumption in a research among a sample of Jordanians was high. This was significantly associated with being Muslims and being a resident of the rural areas in Jordan. Current results also indicate that religious beliefs have higher negative influence on reporting alcohol consumption when compared to social factors. The majority of participants (92.7%) considered reporting alcohol consumption is forbidden and may double their sins. Furthermore, even living in foreign cultures that accept alcohol consumption could not overrule religious-related factors. This is the first study that examined the influence of religious beliefs on reporting alcohol consumption, and therefore, comparing this finding to previous literature is not possible. However, Ghandour et al14 reported that religious beliefs were inversely related to alcohol use behaviors among different religious groups in Lebanon, substantially among Muslims. Religious practice was also highlighted as a protective factor against alcohol use behaviors among American Muslim college students.11,18 Thus, similar to alcohol consumption, reporting alcohol consumption by users might be influenced by religious beliefs and could be associated with stigma and social embarrassment among Jordanians as documented in a former report.13 The image regarding reporting of alcohol consumption could be explained by local culture that depends largely on its tribal nature, which rejects alcohol drinkers.8 The social rejection could be leading to unpleasant consequences such as distortion of the reputation of the drinker’s whole family and friends, job loss, and being dismissed for marriage requests. On the other hand, concerning reporting alcohol consumption in research, most of the participants (≥35 years old) refused to report alcohol consumption despite moving to countries where alcohol-drinking behavior is culturally common. Within this age period, people might be more resistant to new cultural values. Moreover, if the researcher is an acquaintance of one of the participants, this would not affect the reporting of alcohol consumption as reported by a majority of the participants (70.5%).
The third factor that was significantly associated with underreported alcohol consumption in research was the participant’s level of trust in the research team. Trust is a considerable factor in research participation.19 Positive correlation between the level of trust in the research team and participation in biomedical research was reported in previous studies.20–22 This study confirms previous results by Ahram et al23 indicating that Jordanians had low level of trust in the scientific community due to fears of confidentiality breach and misuse of their data, which might affect their participation in research that includes reporting personal sensitive information. This indicates serious trust problem among Jordanians regarding receptivity to participate in research studies that include reporting sensitive issues such as alcohol consumption behaviors.
The association between not reporting alcohol consumption in scientific research and religious beliefs demonstrates the effect of Islamic teachings on Muslims. Islam prohibits the consumption of alcohol following the Holy Quran and Sunnah, the two major sources of Islamic rules. It is clearly declared that drinking alcohol itself is considered “Haram”, which means forbidden.12 God states that drinking alcohol has much potential harms than benefits in Quran verse (2:219), which is as follows: They ask thee concerning wine and gambling. Say: “In them is a great sin, and some profit, for men; but the sin is greater than the profit.” Consequently, from an Islamic point of view, declaration of alcohol consumption results in a bigger sin as the declaration might motivate others to start drinking alcohol.
The study shows that participants with a low trust level did not report alcohol consumption both because of fear from data misuse and dealing with their information without privacy. Surprisingly, participants with a high trust level in the research team also refused to report alcohol consumption. This could be explained by the high social sensitivity toward alcohol consumption in our culture. In other words, the high trust level may not overrule the phenomenon of not reporting alcohol consumption.
This study used culturally acceptable questions and indirect phrases, which increased the validity of our results. In contrary, direct questions such as “Have you consumed alcoholic drinks during the past three months?”24 have raised doubts about the validity of obtained results.7,25 Jalilian et al24 reported only 10.1% of participants answered “yes” to direct alcohol consumption questions and reported high rejection rate to participate in the study. Developing trust between participants and the research team is required to ensure the validity of such direct questions because alcohol consumption is considered a stigmatized behavior in Arab countries.
Given the importance of reporting of alcohol consumption during research studies and the sensitive nature of such information in the culture of the studied population, ethical obligations are imposed on researchers to respect participants’ willingness to report their actual drinking patterns and to minimize the risk of information disclosure. Informed consent process is the core in protecting participants’ autonomy and ensuring data confidentiality. Informed consent should state adequate information about the research benefits and risks. Thus, asking about sensitive information such as alcohol drinking pattern and its consequent possible risks should be stated clearly in the informed consent form. Then, participants could fairly assess the risks/benefits ratio of participating in the research.
The risks of reporting alcohol consumption, religious breach, and social embarrassment could reach their lowest level when the researcher guarantees data confidentiality through anonymous surveys or coding the identifiable data and limiting access to the coding key by password protection, for example. Explaining the ways of protecting participants’ data in the informed consent form is recommended, since it may enhance participants’ trust in the research team to report their actual drinking behavior.
This study represents the first unique step to control the ethical challenges regarding reporting of alcohol consumption in research in Jordan. One of the limitations of the study is that it did not investigate alcohol consumption in the examined population; instead, it measured the attitudes and beliefs toward reporting alcohol consumption. Further studies on alcohol drinkers are highly recommended to evaluate the actual reporting of alcohol consumption and drinking patterns in Jordan and to determine the associated ethical challenges and other possible potential reasons, comparable to previous international studies that explored the reasons of this common problem26 and methods to correct it.27 Self-report surveys are a well-documented reason for underreporting28–31 as well as certain drinking patterns found to be associated with underreporting.26
Conclusion
Raising awareness of the benefits of reporting alcohol consumption is highly recommended. Improving confidence in privacy and data confidentiality among Jordanians might help in improving the level of reporting during participation in research.
Acknowledgments
This project was carried out as part of “The Research Ethics Education Program in Jordan” and has been supported by National Institute of Health grant (number 1R25TW010026-01, Al-delaimy, Wael, PI).
Disclosure
The authors report no conflicts of interest in this work.
References
Baan R, Straif K, Grosse Y, et al; WHO International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of alcoholic beverages. Lancet Oncol. 2007;8(4):292–293. | ||
WHO. Global Status Report on Alcohol and Health. Geneva, Switzerland: WHO; 2014. | ||
Shield KD, Parry C, Rehm J. Chronic diseases and conditions related to alcohol use. Alcohol Res. 2013;35(2):155–173. | ||
Lönnroth K, Williams BG, Stadlin S, Jaramillo E, Dye C. Alcohol use as a risk factor for tuberculosis – a systematic review. BMC Public Health. 2008;8:289. | ||
Baliunas D, Rehm J, Irving H, Shuper P. Alcohol consumption and risk of incident human immunodeficiency virus infection: a meta-analysis. Int J Public Health. 2010;55(3):159–166. | ||
Dawson DA, Room R. Towards agreement on ways to measure and report drinking patterns and alcohol-related problems in adult general population surveys: the Skarpö conference overview. J Subst Abuse. 2000;12(1-2):1–21. | ||
Almarri TS, Oei TP. Alcohol and substance use in the Arabian Gulf region: a review. Int J Psychol. 2009;44(3):222–233. | ||
Amundsen EJ, Rossow I, Skurtveit S. Drinking pattern among adolescents with immigrant and Norwegian backgrounds: a two-way influence? Addiction. 2005;100(10):1453–1463. | ||
Bilal AM, Makhawi B, Al-Fayez G, Shaltout AF. Attitudes of a sector of the Arab-Muslim population in Kuwait towards alcohol and drug misuse: an objective appraisal. Drug Alcohol Depend. 1990;26(1):55–62. | ||
Ghandour LA, Karam EG, Maalouf WE. Lifetime alcohol use, abuse and dependence among university students in Lebanon: exploring the role of religiosity in different religious faiths. Addiction. 2009;104(6):940–948. | ||
Karam EG, Maalouf WE, Ghandour LA. Alcohol use among university students in Lebanon: prevalence, trends and covariates. The IDRAC University Substance Use Monitoring Study (1991 and 1999). Drug Alcohol Depend. 2004;76(3):273–286. | ||
Tarighat-Esfanjani A, Namazi N. Erratum to: nutritional concepts and frequency of foodstuffs mentioned in the Holy Quran. J Relig Health. 2016;55(3):820. | ||
Lankarani KB, Afshari R. Alcohol consumption in Iran. Lancet. 2014;384(9958):1927–1928. | ||
Ghandour L, Chalak A, El-Aily A, et al. Alcohol consumption in the Arab region: what do we know, why does it matter, and what are the policy implications for youth harm reduction? Int J Drug Policy. 2016;28:10–33. | ||
Hamaideh S, Mudallal R, Al-Mudallal H, Abu Hammoudeh M. Prevalence, types and predictors of illicit substance use among the Hashemite University students in Jordan. Jordan Med J. 2010;44(2):125–132. | ||
Mansour A, Marmash L. Health concerns and risk behaviors among university students in Jordan. Jordan Med J. 2007;41(2):80–89. | ||
Hadidi MS, Ibrahim MI, Abdallat IM, Hadidi KA. Current trends in drug abuse associated fatalities – Jordan, 2000–2004. Forensic Sci Int. 2009;186(1-3):44–47. | ||
Abu-Ras W, Ahmed S, Arfken CL. Alcohol use among U.S. Muslim college students: risk and protective factors. J Ethn Subst Abuse. 2010;9(3):206–220. | ||
Baik SH, Arevalo M, Gwede C, et al. Development and validation of the Biomedical Research Trust Scale (BRTS) in English and Spanish. J Empir Res Hum Res Ethics. 2016;11(4):346–356. | ||
Cousins GMH, Ring L. Public Perceptions of Biomedical Research: A Survey of the General Population in Ireland. Dublin: Health Research Board; 2005. | ||
Khalil SS, Silverman HJ, Raafat M, El-Kamary S, El-Setouhy M, Attitudes E-SM. Attitudes, understanding, and concerns regarding medical research amongst Egyptians: a qualitative pilot study. BMC Med Ethics. 2007;8:9. | ||
Trauth JM, Musa D, Siminoff L, Jewell IK, Ricci E. Public attitudes regarding willingness to participate in medical research studies. J Health Soc Policy. 2000;12(2):23–43. | ||
Ahram M, Othman A, Shahrouri M. Public support and consent preference for biomedical research and biobanking in Jordan. Eur J Hum Genet. 2013;21(5):567–570. | ||
Jalilian F, Karami Matin B, Ahmadpanah M, et al. Socio-demographic characteristics associated with cigarettes smoking, drug abuse and alcohol drinking among male medical university students in Iran. J Res Health Sci. 2015;15(1):42–46. | ||
Al-Ansari EA, Negrete JC. Screening for alcoholism among alcohol users in a traditional Arab Muslim society. Acta Psychiatr Scand. 1990;81(3):284–288. | ||
Boniface S, Kneale J, Shelton N. Drinking pattern is more strongly associated with under-reporting of alcohol consumption than socio-demographic factors: evidence from a mixed-methods study. BMC Public Health. 2014;14(11):1297. | ||
Stockwell T, Zhao J, Greenfield T, Li J, Livingston M, Meng Y. Estimating under- and over-reporting of drinking in national surveys of alcohol consumption: identification of consistent biases across four English-speaking countries. Addiction. 2016;111(7):1203–1213. | ||
Stockwell T, Zhao J, Chikritzhs T, Greenfield TK. What did you drink yesterday? Public health relevance of a recent recall method used in the 2004 Australian National Drug Strategy Household Survey. Addiction. 2008;103(6):919–928. | ||
Stockwell T, Zhao J, Macdonald S. Who under-reports their alcohol consumption in telephone surveys and by how much? An application of the ‘yesterday method’ in a national Canadian substance use survey. Addiction. 2014;109(10):1657–1666. | ||
Livingston M, Callinan S. Underreporting in alcohol surveys: whose drinking is underestimated? J Stud Alcohol Drugs. 2015;76(1):158–164. | ||
Gmel G, Rehm J. Measuring alcohol consumption. Contemp Drug Probl. 2004;31(3):467–540. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.