")
Back to Journals » Journal of Asthma and Allergy » Volume 16
Asthma and Susceptibility to COVID-19 in Australian Children During Alpha, Delta and Omicron Waves of the COVID-19 Pandemic
Authors Chan M, Owens L, Gray ML, Selvadurai H, Jaffe A, Homaira N
Received 30 May 2023
Accepted for publication 1 September 2023
Published 13 October 2023 Volume 2023:16 Pages 1139—1155
DOI https://doi.org/10.2147/JAA.S421158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Mei Chan,1 Louisa Owens,1,2 Melinda Louise Gray,2 Hiran Selvadurai,3,4 Adam Jaffe,1,2 Nusrat Homaira1,2,5
1Discipline of Paediatrics and Child Health, School of Clinical Medicine, Faculty of Medicine, University of New South Wales, Sydney, NSW, Australia; 2Respiratory Department, Sydney Children’s Hospital, Randwick, NSW, Australia; 3Respiratory Medicine, Children’s Hospital at Westmead, Westmead, NSW, Australia; 4Discipline of Child and Adolescent Health, Sydney Medical School, University of Sydney, Sydney, NSW, Australia; 5James P Grant School of Public Health, BRAC University, Dhaka, 1213, Bangladesh
Correspondence: Nusrat Homaira, Discipline of Paediatrics and Child Health, School of Clinical Medicine, Faculty of Medicine, University of New South Wales, Sydney, NSW, 2031, Australia, Tel +612 93825526, Email [email protected]
Purpose: Earlier coronavirus-19 (COVID-19) pandemic reports did not implicate increased disease burden in asthmatics while subsequent findings have been inconsistent. To date, the impact of COVID-19 on childhood asthma remains undetermined and is further complicated with ongoing emergence of new variants. This study aimed to investigate association between asthma and COVID-19 for children in New South Wales (NSW), Australia and compare its differences across four major outbreaks from alpha, delta and omicron variants/subvariants.
Methods: This is a retrospective cross-sectional study of all children aged ≤ 17 years old who sought care for COVID-19 at Sydney Children’s Hospitals Network (SCHN) between 1 January 2020 and 31 May 2022.
Results: Of the 18,932 children with polymerase chain reaction (PCR) confirmed COVID-19 who attended SCHN, 60% received their care during delta wave, and 5.41% (n = 913) had prior diagnosis of asthma. Among children with COVID-19, the odds of having asthma were lower during alpha (aOR = 0.43; 95% CI, 0.19– 0.83) and delta wave (aOR = 0.84; 95% CI, 0.73– 0.96), but were higher during omicron wave (aOR = 1.56; 95% CI, 1.23– 1.95). Length of hospital stay (LOS) for asthmatic children were increased by 0.55 days and 1.17 days during delta and the second omicron wave, respectively. Intensive care and mechanical ventilation requirements were not significantly different between asthmatic and non-asthmatic children. Eleven deaths were reported but none had asthma.
Conclusion: Although children with asthma were more susceptible to COVID-19 infections during omicron waves compared to that of alpha or delta waves, they were not at greater risk of COVID-19 severity at any stage of the outbreak regardless of the predominant SARS-CoV-2 variants/subvariants.
Keywords: asthma, COVID-19, pandemic, childhood
Corrigendum for this paper has been published.
Introduction
Since first reported in December 2019 till 1 August 2023, coronavirus-19 (COVID-19) disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus has infected more than 768 million people resulting in 6.9 million deaths worldwide.1 In Australia, over 11.5 million COVID-19 cases have been reported so far (as of 1 August 2023) with fatalities exceeding 22 thousand people.2 New South Wales (NSW), the most populous state in Australia,3 is the worst-hit state accounting for more than one-third of the total cases and mortalities.4
In the past 3 years, NSW has witnessed multiple waves of COVID-19 pandemic caused by three major variants of SARS-CoV-2 virus (ie alpha, delta and omicron). Alpha was the original SARS-CoV-2 strain or variant of concern dominating before June 2021 and its impact was controlled by a series of lockdown and restriction measures imposed by the government. The delta variant was first identified in NSW in mid-June 2021 which led to a bigger and more severe wave of COVID-19, resulting in the reintroduction of wider lockdown and stricter social restrictions. After November 2021, delta was quickly displaced by the omicron variant, a highly transmissible and mutable version of SARS-CoV-2, which has been associated with a series of COVID-19 outbreaks in 2022.5,6
Many chronic conditions including cancer, diabetes, obesity, hypertension, heart diseases, kidney and liver diseases are considered risk factors for SARS-CoV-2 infection and serious outcomes.7 Given that respiratory viral infections are the most common triggers of asthma exacerbation, it was anticipated that asthma could predispose patients to infection and severe COVID-19. Surprisingly, earlier pandemic studies from China had reported less than 1% of the patients hospitalized for COVID-19 infection had a prior diagnosis of asthma.8 A large epidemiology study of 72,314 cases in China also excluded asthma as a risk factor for COVID-19 infection or severity.9 In Mexico, asthma was reported in just 3% of the cases with positive results for the virus.10 However, in contrast to these reports, several studies from the United States and United Kingdom found that asthma was more prevalent among individuals with COVID-19 than those without.11–13 Therefore, it remains unclear whether patients with asthma are more susceptible to infection and severe outcome from COVID-19 than those without asthma. Also, these findings were mostly based on data prior to delta and omicron outbreaks; whether asthma confers similar effects on the newly emerged SARS-CoV-2 variants/subvariants is largely unknown.
The majority of the existing data on asthma and COVID-19 were derived from the adult populations; there are very limited data available on the relation of childhood asthma with risk of contracting SARS-CoV-2 or poor health outcomes from COVID-19 and conflicting results have been reported. In a recent study on COVID-19 related hospitalization including data to September 2021, children with asthma were found to have more than two-fold increase in risk of hospitalization.14 This is contrary to earlier findings by other authors who reported either protective or no effect of asthma against COVID-19.15,16 Since the immuno-response of children to the virus is different from that of the adults,17 it is important to determine whether children with asthma are at risk of COVID-19 infection and severity so that appropriate and safe recommendations can be provided to their parents or carers. In this study, we aim to investigate the risk of developing COVID-19 and the impact of COVID-19 on health outcomes in children with asthma across four major waves of COVID-19 outbreaks when alpha, delta, omicron BA.1 and omicron BA.2 were the predominantly circulating variants/subvariants.
Materials and Methods
Study Design and Setting
We conducted a multicentre, retrospective cross-sectional study using electronic medical records from the Sydney Children’s Hospitals Network (SCHN), the largest paediatric healthcare provider in Southern Hemisphere. SCHN is made up of two large tertiary paediatric hospitals, the Children’s Hospital at Westmead and Sydney Children’s Hospital at Randwick. Each year, there are more than 56,000 in-patient admissions, 97,000 emergency department (ED) presentations and 1.2 million outpatient attendances at SCHN. On average, there are approximately 2500 paediatric asthma hospital presentations across the network annually.18 De-identified data on relevant variables were extracted from the medical records by Patient Information Unit and provided to study investigators. In March 2020, soon after the COVID-19 outbreak, the COVID-19 Outpatient Response Team (CORT)/VirtualKids was set up by SCHN, in addition to the Hospital in the Home (HITH) outreach service, to provide healthcare at home for children tested positive for COVID-19 who did not require in-patient care but still needed medical follow-up or monitoring for their conditions.
Study Participants
Any children aged ≤17 years old with polymerase chain reaction (PCR) confirmed COVID-19 who were admitted to the SCHN as in-patients or received ambulatory care (ie including ED and outreach care under CORT/VirtualKids and HITH) between 1 January 2020 and 31 May 2022 were included in this study. Eligible participants were identified using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-AM) diagnostic codes associated with COVID-19 (U07.1). In Australia, U07.1 ICD-10-AM code was effective from 1 January 2020 according to the National Independent Health and Aged Care Pricing Authority (IHACPA).19 Patients with only rapid antigen test performed were not included. The study cohort was divided into two groups (ie asthma and non-asthma) and all children in the asthma group had previous physician-diagnosed asthma and previous hospital/ED encounters associated with ICD-10-AM codes of allergic asthma (J45.0), non-allergic asthma (J45.1), mixed asthma (J45.8), asthma unspecified, (J45.9) and status asthmaticus (J46) within the past two years before being tested positive for COVID-19. Any co-morbidities in the child were identified based on relevant ICD-10-AM codes recorded in the medical records (list of co-morbidities included is provide in Supplementary Table 1).
Statistical Analysis
We compared children with asthma vs those without on their risks of developing COVID-19, and severity of disease as measured by COVID-19-related length of hospital stay (LOS), ICU admission, mechanical ventilation uses and mortality. Descriptive statistics including mean, standard deviation (SD) and frequency were calculated, where appropriate. Differences between groups were evaluated by using Pearson’s chi-squared test for categorical data (Fisher’s exact test for sample size <5) and Student’s t-test for continuous data. Subgroup analyses were performed over four discrete periods/waves based on the dominant circulating variants after first detected in NSW: 1 January 2020 to 15 June 2021 (alpha wave), 16 June 2021 to 31 October 2021 (delta wave), 1 November 2021 to 28 February 2022 (omicron BA.1 wave), 1 March 2022 to 31 May 2022 (omicron BA.2 wave), wherein, alpha, delta, omicron BA.1 and omicron BA.2 were the respective dominant variants/subvariants of SARS-CoV-2 virus.
Multivariable logistic regression analysis to estimate adjusted odds ratio (aOR) and 95% confidence interval (95% CI) was used to evaluate socio-demographic factors and health outcomes associated with asthma in children with COVID-19. Associations with continuous data were analysed by using linear regression. Health outcomes used to assess disease severity included LOS, ICU stays, mechanical ventilation uses and deaths. LOS was based on number of day that patients spent in hospital at SCHN for their COVID-19 episodes. ICU stays referred to time (in hour) patients spent in ICU at SCHN within their COVID-19 hospitalization. Mechanical ventilation referred to invasive respiratory support delivered by mechanical ventilator via endotracheal tube. Deaths referred to those occurred in the hospitals at SCHN within three months following a primary diagnosis of COVID-19. Adjustment for covariates, including age, sex, country of birth, any co-morbidities, socio-economic status and type of care (ie in-patient or ambulatory) were achieved by multivariate analyses. In-patient care referred to care delivered within the hospital wards or ICUs. Ambulatory care referred to ED presentations or care delivered virtually or at home by CORT/VirtualKids or HITH. Socio-economic status was assessed based on the child’s postcode of residence using the Australian Bureau of Statistics Socio-Economic Indexes for Areas (SEIFA), Index of Relative Socioeconomic Advantage and Disadvantage (IRSAD) and stratified into five categories from least (Quintile 1) to most advantaged (Quintile 5) according to the postal area decile ranking.20 Obesity was defined as weight for age ≥95th percentile. All statistical analyses were performed using R program version 4.1.1 for Windows with two-sided tests at 5% level of significance.
Ethics Approval
This retrospective study was approved by the Sydney Children’s Hospitals Network Human Research Ethics Committee (2021/ETH12487) dated 9 March 2022. Exemption for participant consent was approved by the ethics committee, and the study was conducted in accordance with the Declaration of Helsinki. All data were treated confidentially.
Results
During 1 January 2020 and 31 May 2022, there were 18,932 children with COVID-19 who were under the care of SCHN. Most of the cases (59.64%) were reported during the second wave when delta was the predominant SARS-CoV-2 variant, while the initial variant (alpha) only contributed to 2.4% of all cases (Figure 1 and Table 1). None of the children in our study had more than one hospital encounter with COVID-19.
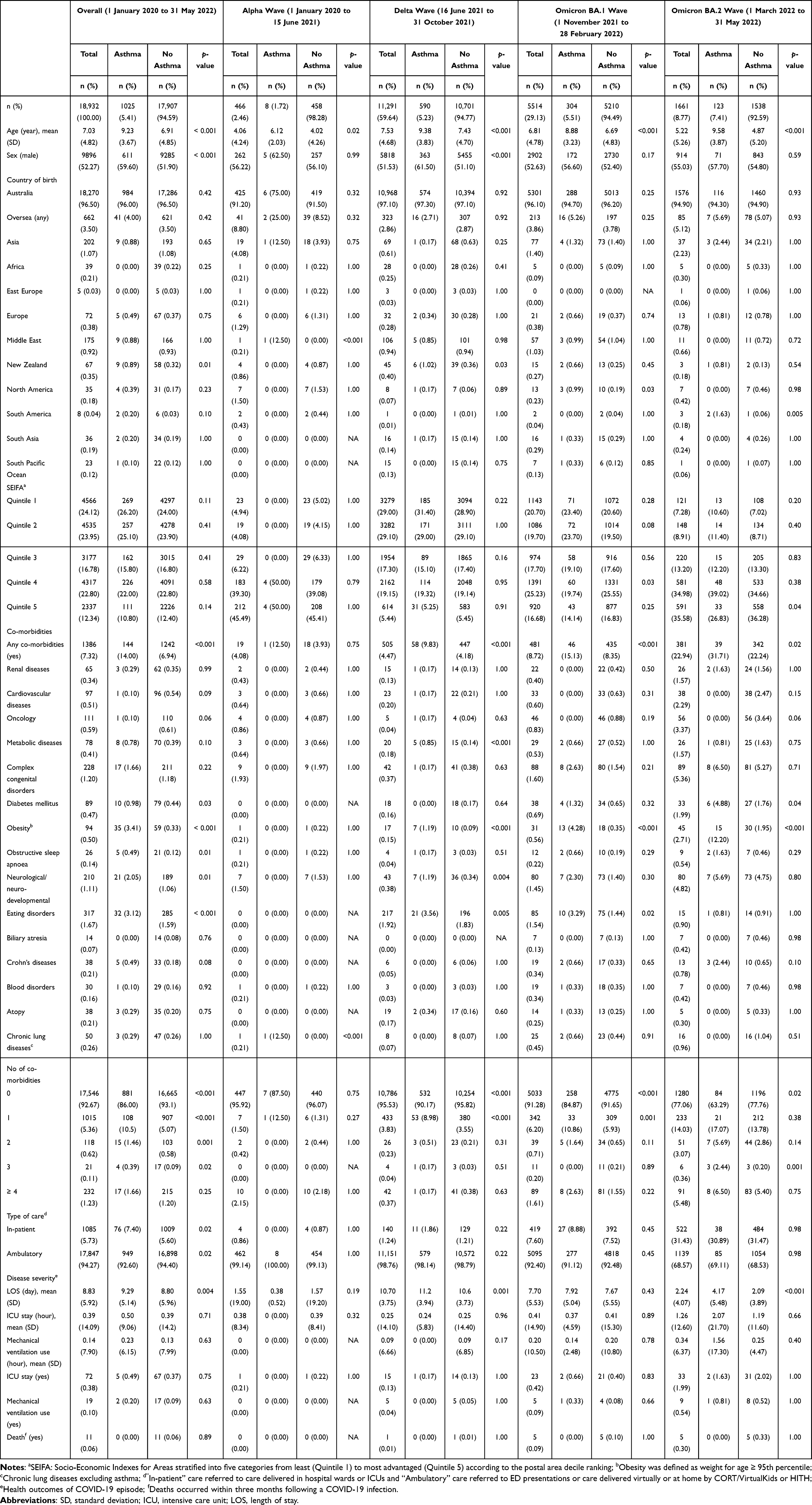 |
Table 1 Socio-Demographic and Clinical Characteristics of Children with and without Asthma Presenting to SCHN with COVID-19 Between 1 January 2020–31 May 2022 |
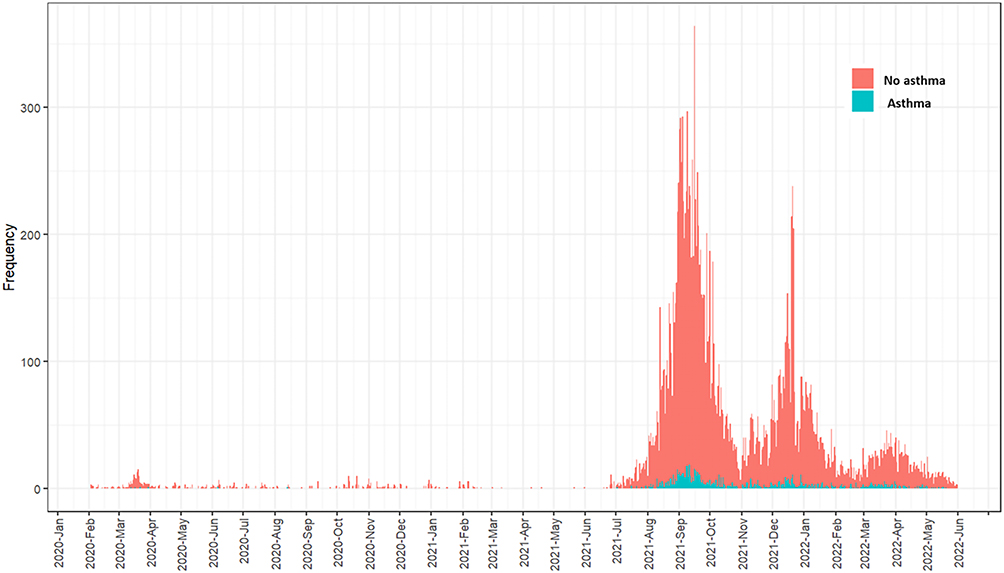 |
Figure 1 Distribution of children with and without asthma who were under the care of Sydney Children’s Hospitals Network in NSW between 1 January 2020–31 May 2022. |
Of the 18,932 children with COVID-19, 913 (5.41%) were asthmatic (Table 1). As shown in Table 2, children with COVID-19 were less likely to have a prior diagnosis of asthma during the alpha (aOR = 0.43; 95% CI 0.19–0.83) and delta waves (aOR = 0.84; 95% CI, 0.73–0.96), but were more likely to have had a diagnosis of asthma during the omicron waves (aOR = 1.56; 95% CI, 1.23–1.95).
 |
Table 2 Socio-Demographic Predictors and Clinical Outcomes Associated with COVID-19 in Children with and without Asthma Presenting to SCHN Between 1 January 2020–31 May 2022 |
Demographic Characteristics
The average age of the study cohort was seven years old. Children with asthma were significantly older (mean = 9.23 years; SD = 3.67; range 3–17 years) than those without (mean = 6.91 years; SD = 4.85; range 0–17 years) (Table 1). This was consistent across all four waves studied (Table 1). Overall, there were more asthmatic boys than girls (59.60% vs 40.40%) with COVID-19 requiring hospital or ambulatory care, especially during the delta wave (61.50% vs 38.50%). Approximately 97% (n = 18,270) of the COVID-19 cases studied were born in Australia. Most of the children with COVID-19 came from less advantageous socio-economic background within SEIFA 1 to 2 quintile (n = 9101, 48.07%) but there was no significant difference between children with asthma and without asthma (p > 0.05) (Table 1).
Co-Morbidities and Asthma
Children with asthma who had other underlying conditions were 82% (95% CI, 1.48–2.22) more likely to be needing in-patient or ambulatory care than those without asthma but had other co-morbidities, and the likelihood was greater with increasing number of co-morbidities (Table 2). However, the association was wave-dependent and was only significant with the delta (aOR = 2.30; 95% CI, 1.69–3.07) and omicron BA.1 wave (aOR = 1.63; 95% CI, 1.12–2.31) (Table 3).
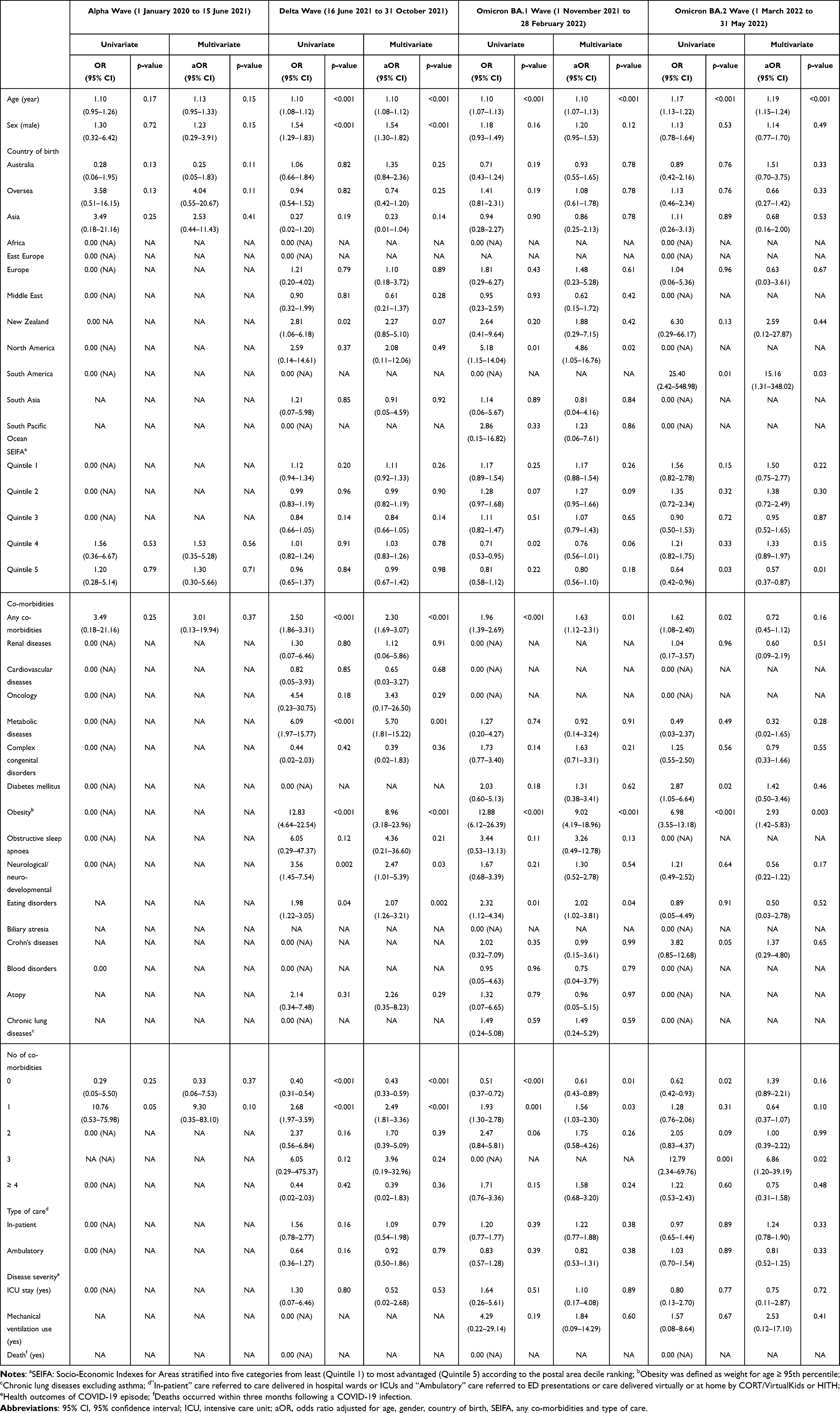 |
Table 3 Differences in Socio-Demographic and Clinical Outcomes Between Children with and without Asthma Presenting to SCHN with COVID-19 Between 1 January 2020–31 May 2022 as Stratified by Alpha, Delta and Omicron Waves |
Disease Severity
Of the 18,932 children with COVID-19, only 5.73% (n = 1085) required in-patient care. Most of the COVID-19 patients received ambulatory care in ED or at home via CORT/VirtualKids and HITH (n = 17,847, 94.27%) (Table 1). Although children with asthma who had COVID-19 were more likely to require in-patient care, the association was not statistically significant after adjusting for covariates (aOR = 1.30; 95% CI, 0.99–1.68) (Table 2), regardless of the waves or variants (Table 3).
The average LOS for children requiring COVID-19 care was 8.83 days (SD = 5.92) while children with asthma had longer LOS than those without (9.29 days; SD = 5.14 vs 8.80 days; SD = 5.96) (Table 1). Subgroup analysis by waves indicated that children with asthma had a significant increase in LOS by 0.55 days (SE = 0.16; p<0.001) during the delta wave and by 1.17 days (SE = 0.34; p=0.001) during the omicron BA.2 wave (Table 4).
 |
Table 4 Estimated Differences in Health Outcomes for Children with Asthma Compared with Children without Asthma Presenting to SCHN with COVID-19 Between 1 January 2020–31 May 2022 |
Throughout the study period, there were 72 (0.38%) children with COVID-19 needing ICU care with an average ICU stay of 0.39 hours (SD = 14.09) (Table 1). Nearly half of the ICU admissions occurred during the omicron BA.2 wave (n = 33) and had the longest ICU stay (mean=1.26 hours) (Table 1). However, children with asthma were not at greater risk of being admitted to ICU at any waves (Tables 2–4).
Mechanical ventilation uses were reported in 19 (0.1%) children with COVID-19, of which, only two had asthma and both had the disease during the omicron waves (Table 1). Average time of mechanical ventilation uses was 0.14 hours (SD = 7.90). The likelihood of requiring mechanical ventilation was not significantly different between asthma and non-asthma groups (Table 2 and Table 3), except during omicron BA.2 wave, wherein, the average hours with mechanical ventilation were increased by 1.5 hours (p=0.01) in children with asthma compared to those without (Table 4).
Mortality was rare for children with COVID-19. There were 11 deaths recorded during the study period, none of the deaths occurred in children with asthma (Table 1).
Discussion
The findings of this study suggest a variation in the association between asthma and COVID-19, depending on the type of SARS-CoV-2 variants circulating. In our cohort, children with COVID-19 were less likely to be asthmatic during alpha and delta waves, but with the emergence of omicron variant, we observed an increase in risk of COVID-19 infection among children with asthma compared with those without. Although children with asthma, in general, required longer duration of hospitalization, they were not at greater risk of COVID-19 severity, in terms of ICU admissions, mechanical ventilation uses or mortality, in comparison to those without asthma across the multiple waves of the pandemic.
Our results are in line with previous studies of early pandemic that patients with asthma were not at heighten risk of COVID-19 infection or severe outcomes.8,21–23 Most of these studies included data prior to mid-2021 when alpha SARS-CoV-2 was the dominant variant. Data on delta and omicron variants are scarce. In our study, it appeared that children with asthma were more susceptible to omicron than alpha or delta infection and hospitalizations. A recent study on the first omicron wave also showed a 2.2-fold increase in the risk of COVID-19 hospitalization for elderly residents living in aged care facilities.24 However, there are no comparable study in paediatric population.
The observed difference in infection during omicron waves may be linked to the differences in pathogenesis between the ancestral SARS-CoV-2 and the newly emerged omicron variants. It is now well established that both angiotensin-converting enzyme 2 (ACE2) and transmembrane protease serine 2 (TMPRSS2) expressions are crucial for the entry of the original SARS-CoV-2 virus (ie alpha variant) into the cells, wherein, ACE2 provides a binding site for the spike protein of SARS-CoV-2 virus and TMPRSS2 cleaves the spike protein to enable cellular membrane fusion,25–28 allowing the virus to enter the cell cytoplasm and initiate replication. In patients with asthma, both ACE2 and TMPRSS2 are usually under expressed which might have limited cellular entry and prevent infection from the virus.25,29 Infectivity of delta variant was still dependent heavily on the ACE2-TMPRSS2 pathway.30 However, there are evidence to suggested that SARS-CoV-2 omicron variants may have altered cell tropism and cell entry pathway by using alternative receptors other than ACE2.31
Despite the higher number of children requiring acute or ambulatory care during delta outbreak, both ICU care or mechanical ventilation were lower compared with the omicron waves. For children with asthma, there was no need for mechanical ventilation uses during alpha and delta waves, and the time of mechanical ventilation uses did not differ between children with and without asthma across all the waves, except the second omicron wave. To date, data on COVID-19 severity, in terms of ICU admission and mechanical ventilation uses, are lacking. However, previous studies from the United States have suggested that children with asthma were likely to suffer worse asthma outcomes from omicron than prior variants.32,33 In a study of 372 patients with asthma presenting with COVID-19, asthma exacerbations were found to have increased by up to 3-fold during omicron wave compared to the delta or pre-delta waves.32 In another study of 81,000 COVID-19 cases, omicron infection was associated with higher rates of corticosteroid uses and antibiotic prescriptions for patients with asthma.33
It is worth noting that the number of COVID-19 cases during alpha wave was significantly lower than any other periods, especially among children with asthma. In addition to the lower infectivity of alpha SARS-CoV-2 variant, it could be attributed to the strict lockdown and restrictive measures imposed during that period. In March 2020, residents in NSW were ordered to stay home, limit their non-essential travels and public gathering when SARS-CoV-2 virus first appeared in Australia. Further restrictions such as social distancing and mask mandate were introduced in the following months.34 Australian border had been closed for international travel since the beginning of the outbreak and was only fully open in July 2022.35 The positive effect of these public health measures in mitigating COVID-19 spread has been well documented. Previous study from our group also found a significant reduction of 50–70% in asthma hospital presentations during the lockdown periods in NSW.36 In a separate meta-analysis of 35 studies, the authors found that adoption of non-pharmaceutical public health interventions was associated with a 4.68% decrease in daily cases, 4.80% decrease in daily deaths, 1.90% decrease in the COVID-19 reproduction number and 16.5% decrease in COVID-19 daily ICU admission.37
COVID-19 fatality in children has been reported to be rare. In Australia, more than 15,000 deaths were registered and certified as having died from COVID-19 from the beginning of the pandemic to 31 January 2023. Among all the deaths reported, only 12 occurred in children aged ≤19 years old, accounting for approximately 0.07% of all COVID-19 deaths.38 Here, in consistent with the national data, we reported 11 deaths (0.05%) occurring within 3 months following a COVID-19 diagnosis. Additionally, most of the deaths occurred during the omicron waves, which is in line with reports from other countries,39 and is likely due to the large number of children infected during these periods. Further, among the 11 deaths, only one was certified as having died from COVID-19 and this child did not have any underlying conditions. The remaining deaths were not registered as directly caused by COVID-19 and they all had serious or complicated co-morbidities such as malignancy and complex congenital disorders, suggesting that the impact of COVID-19 on childhood mortality might have been underestimated. Nevertheless, there was no death recorded among children with asthma, which is in concordance with findings of a meta-analysis that presence of asthma was not associated with risk of mortality from COVID-19.40
Our study has some limitations. First, information on need for asthma medications (eg inhaled corticosteroids and biologic therapies) and asthma severity was not available. Although it has been suggested that biologic therapies for asthma such as omalizumab may be protective against severe COVID-19,41 previous findings on inhaled corticosteroids and COVID-19 outcomes in asthma patients were inconclusive.42–44 According to the Global Initiative for Asthma (GINA),45 classification of asthma severity will require information of medication uses and lung function test eg forced expiratory volume (FEV1) measurements, which were unavailable for this study. Nevertheless, inconsistent results have been reported on the association between severe/uncontrolled asthma and severe COVID-19 in adults.46,47 Second, the effect of vaccination was not taken into account as these data were unavailable in the medical records. Nonetheless, its clinical significance might be limited as COVID-19 vaccine was not rolled out for children under 12 years in Australia until February 2022 in the mid of omicron waves, and its efficacy and effectiveness has been shown to be modest against omicron variants by other authors.48 Finally, data used in this study was derived exclusively from NSW, and hence, may not be applicable to other states or countries. Nevertheless, NSW is the most densely populated state of the country, and our analysis was based on a very large cohort of children over multiple waves of the pandemic, which is the biggest strength of this study.
Conclusion
In our study based on a cohort of almost 19,000 children, we demonstrated that while asthma in children might not have been a risk factor for COVID-19 infection during the early stages of the pandemic, it was linked to greater susceptibility to infection during the periods when omicron was the predominantly circulating strain of SARS-CoV-2 virus. However, the risk of severe COVID-19 in children with asthma was no greater than in children without asthma across the multiple waves of pandemic.
As we move toward a phase where COVID-19 becomes endemic, it is important that we monitor emerging new variants and the impact of the disease in children with asthma who are already at higher risk of an acute exacerbation due to common respiratory infections. Our findings have significant implication regarding clinical decision-making on rapid diagnosis and management of COVID-19 in children with asthma.
Abbreviations
COVID-19, Coronavirus-19; SARS-CoV-2, Severe acute respiratory syndrome coronavirus 2; NSW, New South Wales; ICU, Intensive care unit; SCHN, Sydney Children’s Hospitals Network; CORT, COVID-19 Outpatient Response Team; HITH, Hospital in the Home; PCR, Polymerase chain reaction; ED, Emergency department; ICD-10-AM, International Classification of Diseases, Tenth Revision, Clinical Modification; LOS, Length of stay; SD, standard deviation; aOR, adjusted odds ratio; 95% CI, 95%; confidence interval; SEIFA, Socio-Economic Indexes for Areas; IRSAD, Index of Relative Socioeconomic Advantage and Disadvantage; GINA, Global Initiative for Asthma; FEV1, Forced expiratory volume.
Data Sharing Statement
Access to the dataset analysed during the current study is not permitted without the express permission of the approving Human Research Ethics Committees. There is no additional data available.
Ethics Approval
This retrospective study was approved by the Sydney Children’s Hospitals Network Human Research Ethics Committee (2021/ETH12487) dated 9 March 2022. Exemption for participant consent was approved by the ethics committee, and the study was conducted in accordance with the Declaration of Helsinki. All data were treated confidentially.
Acknowledgments
Dr Nusrat Homaira was supported through Early Career Fellowship Scheme of the National Health and Medical Research Council of Australia (APP1158646). We are grateful to Kavith Sutharsan, Jane Shrapnel and Jake Davis from the Management Support and Analysis Unit, and clinicians and laboratory staff at the Sydney Children’s Hospitals Network and NSW Health Pathology (South Eastern Area Laboratory Service). The authors would like to thank Rotary Club of Sydney Cove for their continued support in our research endeavours. This work was supported by the Rotary Club of Sydney Cove. The funding organization had no role in the study design, analyses or drafting of the manuscript.
Disclosure
Dr Nusrat Homaira reports grants from Rotary club of Sydney Cove, grants from National Health and Medical Research Council of the Australian Government, during the conduct of the study. The authors declare no other conflict of interest.
References
1. World Health Orgnaizaiton. WHO coronavirus (COVID-19) dashboard. World Health Orgnaizaiton; 2023 [updated August 2, 2023]. Available from: https://covid19.who.int/.
2. World Health Orgnaizaiton. WHO coronavirus (COVID-19) dashboard. World Health Orgnaizaiton; 2023 [updated August 2, 2023]. Available from: https://covid19.who.int/region/wpro/country/au.
3. Australian Bureau of Statistics. National, state and territory population. Australian Bureau of Statistics; 2022 [updated March 16, 2023]. Available from: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/sep-2022.
4. NSW Health. COVID-19 in NSW. NSW Government; 2023 [updated March 17, 2023]. Available from: https://www.health.nsw.gov.au/Infectious/covid-19/Pages/stats-nsw.aspx.
5. Australian Bureau of Statistics. Effects of COVID-19 strains on the Australian economy. Australian Bureau of Statistics; 2022.
6. Department of Health and Aged Care. Weekly COVID-19 reporting|Australian Government Department of Health and Aged Care. Department of Health and Aged Care; 2023.
7. World Health Organization. Coronavirus disease (COVID-19); 2023. Available from: https://www.who.int/health-topics/coronavirus#tab=tab_1.
8. Li X, Xu S, Yu M, et al. Risk factors for severity and mortality in adult COVID-19 inpatients in Wuhan. J Allergy Clin Immunol. 2020;146(1):110–118. doi:10.1016/j.jaci.2020.04.006
9. Wu Z, McGoogan JM. Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
10. Bedolla-Barajas M, Morales-Romero J, Bedolla-Pulido TR, et al. Low prevalence of asthma in Mexican children and adults with a positive rtRT-PCR test for SARS-CoV-2: a cross-sectional study during the 2020 pandemic. Allergol Immunopathol. 2021;49(3):1–7. doi:10.15586/aei.v49i3.7
11. Garg S, Kim L, Whitaker M, et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019 - COVID-NET, 14 States, March 1–30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(15):458–464. doi:10.15585/mmwr.mm6915e3
12. Docherty AB, Harrison EM, Green CA, et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: prospective observational cohort study. BMJ. 2020;369:m1985. doi:10.1136/bmj.m1985
13. Williamson EJ, Walker AJ, Bhaskaran K, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584(7821):430–436. doi:10.1038/s41586-020-2521-4
14. Dolby T, Nafilyan V, Morgan A, Kallis C, Sheikh A, Quint JK. Relationship between asthma and severe COVID-19: a national cohort study. Thorax. 2023;78(2):120–127. doi:10.1136/thoraxjnl-2021-218629
15. Sousa BLA, Brentani A, Costa Ribeiro CC, et al. Non-communicable diseases, sociodemographic vulnerability and the risk of mortality in hospitalised children and adolescents with COVID-19 in Brazil: a cross-sectional observational study. BMJ Open. 2021;11(9):e050724. doi:10.1136/bmjopen-2021-050724
16. Beken B, Ozturk GK, Aygun FD, Aydogmus C, Akar HH. Asthma and allergic diseases are not risk factors for hospitalization in children with coronavirus disease 2019. Ann Allergy Asthma Immunol. 2021;126(5):569–575. doi:10.1016/j.anai.2021.01.018
17. Yuan Y, Wang QP, Sun D, et al. Differences in Immune Responses between Children and Adults with COVID-19. Curr Med Sci. 2021;41(1):58–61. doi:10.1007/s11596-021-2318-1
18. Sydney Children’s Hospitals Network. Sydney Children’s Hospitals Network, 2021 Annual Review. Sydney: Sydney Children’s Hospitals Network; 2021.
19. Independent Health and Aged Care Pricing Authority. How to classify COVID-19 – guidance for data analysts using ICD-10-AM Eleventh Edition. Independent Health and Aged Care Pricing Authority; 2022. Available from: https://www.ihacpa.gov.au/sites/default/files/2022-12/How%20to%20classify%20COVID-19%20%E2%80%93%20Guidance%20for%20data%20analysts%20using%20ICD-10-AM%20Eleventh%20Edition.PDF.
20. Australian Bureau of Statistics. Socio-economic indexes for areas. Australian Bureau of Statistics; 2023 [updated May 6, 2022]. Available from: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa.
21. Kalyanaraman Marcello R, Dolle J, Grami S, et al. Characteristics and outcomes of COVID-19 patients in New York City’s public hospital system. PLoS One. 2020;15(12):e0243027. doi:10.1371/journal.pone.0243027
22. Rao S, Hurst JH, Zhao C, et al. Asthma and the risk of SARS-CoV-2 infection among children and adolescents. Pediatrics. 2022;149(6). doi:10.1542/peds.2021-056164
23. Floyd GC, Dudley JW, Xiao R, et al. Prevalence of asthma in hospitalized and non-hospitalized children with COVID-19. J Allergy Clin Immunol Pract. 2021;9(5):2077–2079.e2072. doi:10.1016/j.jaip.2021.02.038
24. Ellis RJ, Moffatt CR, Aaron LT, et al. Factors associated with hospitalisations and deaths of residential aged care residents with COVID-19 during the Omicron (BA.1) wave in Queensland. Med J Aust. 2023;218(4):174–179. doi:10.5694/mja2.51813
25. Radzikowska U, Ding M, Tan G, et al. Distribution of ACE2, CD147, CD26, and other SARS-CoV-2 associated molecules in tissues and immune cells in health and in asthma, COPD, obesity, hypertension, and COVID-19 risk factors. Allergy. 2020;75(11):2829–2845. doi:10.1111/all.14429
26. Wark PAB, Pathinayake PS, Kaiko G, et al. ACE2 expression is elevated in airway epithelial cells from older and male healthy individuals but reduced in asthma. Respirology. 2021;26(5):442–451. doi:10.1111/resp.14003
27. Morrison CB, Edwards CE, Shaffer KM, et al. SARS-CoV-2 infection of airway cells causes intense viral and cell shedding, two spreading mechanisms affected by IL-13. Proc Natl Acad Sci U S A. 2022;119(16):e2119680119. doi:10.1073/pnas.2119680119
28. Walls AC, Park YJ, Tortorici MA, Wall A, McGuire AT, Veesler D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell. 2020;181(2):281–292.e286. doi:10.1016/j.cell.2020.02.058
29. Wang JY, Pawankar R, Tsai HJ, Wu LS, Kuo WS. COVID-19 and asthma, the good or the bad? Allergy. 2021;76(2):565–567. doi:10.1111/all.14480
30. Chavda VP, Bezbaruah R, Deka K, Nongrang L, Kalita T. The delta and omicron variants of SARS-CoV-2: what we know so far. Vaccines. 2022;10(11):1926. doi:10.3390/vaccines10111926
31. Lim S, Zhang M, Chang TL. ACE2-independent alternative receptors for SARS-CoV-2. Viruses. 2022;14(11):2535. doi:10.3390/v14112535
32. Gaietto K, Snyder O, Bergum N, et al. Differences in COVID-19-triggered pediatric asthma exacerbations across variant waves. Eur Respir J. 2022;60(suppl 66):1353.
33. Kudlaty E, Guo A, Patel G, Watts M, Peters A. Rates of corticosteroid and antibiotic prescriptions are significantly increased with omicron as compared to alpha and delta variants of COVID-19 in patients with asthma. J Allergy Clin Immunol. 2023;151(2):AB331. doi:10.1016/j.jaci.2022.12.766
34. Wikipedia. COVID-19 pandemic in New South Wales. WikiMedia Foundation; 2023 [updated March 8, 2023]. Available from: https://en.wikipedia.org/wiki/COVID-19_pandemic_in_New_South_Wales.
35. Walker L. Australia has opened its borders to unvaccinated travellers. Here’s what you need to know. ABC: ABC News Website; 2022. Available from: https://www.abc.net.au/news/2022-07-06/australia-opens-borders-to-unvaccinated-travellers/101212102.
36. Homaira N, Hu N, Owens L, et al. Impact of lockdowns on paediatric asthma hospital presentations over three waves of COVID-19 pandemic. Allergy Asthma Clin Immunol. 2022;18(1):53. doi:10.1186/s13223-022-00691-1
37. Iezadi S, Gholipour K, Azami-Aghdash S, et al. Effectiveness of non-pharmaceutical public health interventions against COVID-19: a systematic review and meta-analysis. PLoS One. 2021;16(11):e0260371. doi:10.1371/journal.pone.0260371
38. Australian Bureau of Statistics. COVID-19 Mortality in Australia: deaths registered until 31 January 2023. Australian Bureau of Statistics; 2023. Available from: https://www.abs.gov.au/articles/covid-19-mortality-australia-deaths-registered-until-31-january-2023.
39. Flaxman S, Whittaker C, Semenova E, et al. Assessment of COVID-19 as the underlying cause of death among children and young people aged 0 to 19 years in the US. JAMA Netw Open. 2023;6(1):e2253590. doi:10.1001/jamanetworkopen.2022.53590
40. Wang Y, Chen J, Chen W, et al. Does asthma increase the mortality of patients with COVID-19? A systematic review and meta-analysis. Int Arch Allergy Immunol. 2021;182(1):76–82. doi:10.1159/000510953
41. Poddighe D, Kovzel E. Impact of anti-type 2 inflammation biologic therapy on COVID-19 clinical course and outcome. J Inflamm Res. 2021;14:6845–6853. doi:10.2147/JIR.S345665
42. Ren J, Pang W, Luo Y, et al. Impact of allergic rhinitis and asthma on COVID-19 infection, hospitalization, and mortality. J Allergy Clin Immunol Pract. 2022;10(1):124–133. doi:10.1016/j.jaip.2021.10.049
43. Dupont A, Couffignal C, Arias C, et al. Outcomes and risk factors with COVID-19 or influenza in hospitalized asthma patients. Respir Res. 2022;23(1):342. doi:10.1186/s12931-022-02265-6
44. Green I, Merzon E, Vinker S, Golan-Cohen A, Magen E. COVID-19 susceptibility in bronchial asthma. J Allergy Clin Immunol Pract. 2021;9(2):684–692.e681. doi:10.1016/j.jaip.2020.11.020
45. Global Initiative for Asthma. Pocket guide for asthma management and prevention (for adults and children older than 5 years). Global Initiative for Asthma; 2020 [updated 2020]. Available from: https://ginasthma.org/wp-content/uploads/2020/04/Main-pocket-guide_2020_04_03-final-wms.pdf.
46. Zein JG, Mitri J, Bell JM, Lopez D, Strauss R, Attaway AH. The relationship of asthma severity to COVID-19 outcomes. J Allergy Clin Immunol Pract. 2022;10(1):318–321 e312. doi:10.1016/j.jaip.2021.10.041
47. Selberg S, Karlsson Sundbaum J, Konradsen JR, et al. Multiple manifestations of uncontrolled asthma increase the risk of severe COVID-19. Respir Med. 2023;216:107308. doi:10.1016/j.rmed.2023.107308
48. Lin DY, Gu Y, Xu Y, et al. Effects of vaccination and previous infection on omicron infections in children. N Engl J Med. 2022;387(12):1141–1143. doi:10.1056/NEJMc2209371
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.