Back to Journals » Journal of Inflammation Research » Volume 19
Asthma and Allergic Bronchopulmonary Aspergillosis: Understanding, Insights, and State-of-the-Art
Authors Saxena P, Muthu V, Sehgal IS, Agarwal R ![]()
Received 3 December 2025
Accepted for publication 17 February 2026
Published 10 March 2026 Volume 2026:19 546322
DOI https://doi.org/10.2147/JIR.S546322
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Tara Strutt
Puneet Saxena,1 Valliappan Muthu,2 Inderpaul Singh Sehgal,2 Ritesh Agarwal2
1Department of Internal Medicine, Military Hospital, Suratgarh, Rajasthan, India; 2Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India
Correspondence: Ritesh Agarwal, Department of Pulmonary Medicine, Post Graduate Institute of Medical Education and Research (PGIMER), Sector-12, Chandigarh, 160012, India, Email [email protected]
Abstract: Allergic bronchopulmonary aspergillosis (ABPA) is a severe asthma endotype arising from dysregulated immune responses to Aspergillus fumigatus in susceptible individuals. ABPA is characterized by exaggerated type 2 immune responses, markedly elevated serum total IgE and A. fumigatus-specific IgE and IgG levels, peripheral blood eosinophilia, and imaging abnormalities, including bronchiectasis and mucus impaction. Genetic predisposition involving HLA genotypes and immune-related polymorphisms contributes to disease susceptibility. The 2024 International Society of Human and Animal Mycology guidelines provide standardized criteria that integrate clinical, immunological, and radiological parameters to identify ABPA and distinguish it from overlapping diagnoses. Management employs a dual approach: anti-inflammatory therapy with systemic corticosteroids targets dysregulated immunity, while antifungal therapy with triazoles reduces airway fungal burden. The relapsing-remitting disease course necessitates systematic monitoring using clinical assessment, total IgE levels, and serial imaging to detect relapses, distinguish them from asthma exacerbations or infections, and optimize treatment intensity. Despite substantial progress in understanding the pathobiology of ABPA, high-quality evidence for optimal management strategies remains limited. Future research should focus on precision medicine approaches, novel biomarkers, and inhaled antifungal therapies to improve outcomes in this severe asthma phenotype. This review provides clinicians with comprehensive information on the pathobiology, diagnosis, classification, and evidence-based management strategies for ABPA, aiming to improve outcomes for patients with this severe asthma endotype.
Plain Language Summary: Allergic bronchopulmonary aspergillosis (ABPA) is a serious lung condition that develops in some asthma patients when the common environmental mould Aspergillus fumigatus persists in the airways. The fungus is found everywhere in the environment, but most people tolerate exposure without problems. However, individuals with ABPA develop excessive immune responses to the fungus, causing severe asthma symptoms and progressive damage to the airways (bronchiectasis). ABPA affects approximately 11% of asthma patients worldwide and represents one of the most serious asthma phenotypes.
Unlike typical asthma, which responds well to inhaled steroids, ABPA often requires treatment with oral corticosteroids or antifungal medications (or both) to control both the immune overreaction and the fungal burden in the lungs. Early diagnosis is crucial in preventing irreversible lung damage. Diagnosis requires demonstrating sensitization to the fungus by blood tests showing elevated total IgE levels and Aspergillus-specific antibodies, combined with elevated eosinophils and characteristic findings on lung imaging, such as bronchiectasis.
Universal screening of all asthma patients for fungal sensitization enables early detection, timely treatment, and prevents disease progression. Early treatment with oral corticosteroids or antifungal medications can prevent progressive lung damage and improve long-term outcomes. Because ABPA tends to relapse, patients require regular monitoring with blood tests measuring IgE levels and periodic lung imaging to detect relapses early and adjust treatment intensity accordingly. This comprehensive approach ensures better disease control and quality of life for ABPA patients.
Keywords: allergic bronchopulmonary aspergillosis, asthma, triazoles, bronchiectasis, Aspergillus
Introduction
Asthma is a chronic inflammatory disease of the airways characterized by chest tightness, wheezing, breathlessness, cough, and sputum production. The disease typically exhibits diurnal and seasonal variability, bronchial hyperresponsiveness, and reversible airflow limitation. A substantial proportion of asthma patients have an allergic phenotype, with nearly 50–60% demonstrating atopy, defined as a genetic predisposition to mount IgE-mediated immune responses to various allergens.1–3 The environment contains abundant respirable organic and inorganic particulate matter, some of which can induce immune sensitization, especially in individuals with atopy. Common aeroallergens implicated in allergic asthma include dust mites, animal dander, pollens, and fungal spores. Among these, fungal aeroallergens have gained increasing attention due to their ubiquity and potential to induce persistent airway inflammation.
Aspergillus species, especially A. fumigatus, are among the most prevalent fungal spores in ambient air, with concentrations varying by geography and season.4,5 A study from rural India reported total ambient fungal spore concentrations ranging from 82–2365 and 156–2022 per cubic meter over two consecutive years.4 A. fumigatus is the most extensively studied fungal species implicated in allergic sensitization and allergic bronchopulmonary aspergillosis (ABPA). Fungi other than Aspergillus species may cause a clinically similar condition, termed allergic bronchopulmonary mycosis (ABPM). However, ABPA accounts for nearly 95% of cases, whereas ABPM due to other fungi, including Alternaria, Penicillium, Cladosporium, and, less commonly, Bipolaris, Curvularia, Schizophyllum commune, Drechslera hawaiiensis, or Candida species, is relatively uncommon. These fungi may cause sensitisation with or without progression to ABPM in susceptible hosts.6–8
In most individuals, exposure to environmental fungal spores does not result in clinically significant disease. However, people with asthma, particularly those with atopy, airway epithelial dysfunction, impaired mucociliary clearance, and defective innate immune responses, are more likely to develop fungal sensitization and ABPA/ABPM. Thus, ABPA is a specific endotype of asthma and a potentially treatable trait warranting clinical attention. The objective of the review is to summarize current evidence and evolving consensus on ABPA in patients with asthma. We examine the relationship between asthma and ABPA, with particular emphasis on pathobiology, immunological mechanisms, clinical assessment, diagnostic strategies, and therapeutic approaches.
Epidemiology and Spectrum of Fungal Allergy Syndromes in Asthma
The relationship between asthma and ABPA is complex (Table 1) and represents a continuum of fungal-associated airway disorders. Despite the widespread environmental presence of Aspergillus species, only a minority of asthma patients develop Aspergillus sensitization (AS). An even smaller proportion progresses to severe asthma with fungal sensitization (SAFS), and only a subset ultimately develops ABPA/ABPM. Disease expression in ABPA is heterogeneous, and the factors underlying this heterogeneity remain incompletely understood. Among patients with ABPA, some develop bronchiectasis (ABPA-B), whereas others lack radiological abnormalities and are classified as serological ABPA (ABPA-S). Patients with asthma and AS are referred to as having A. fumigatus-associated asthma (AFAA).9 Although AS and ABPA predominantly occur in asthmatics, they can develop in non-asthmatic individuals with other predisposing airway disorders.10
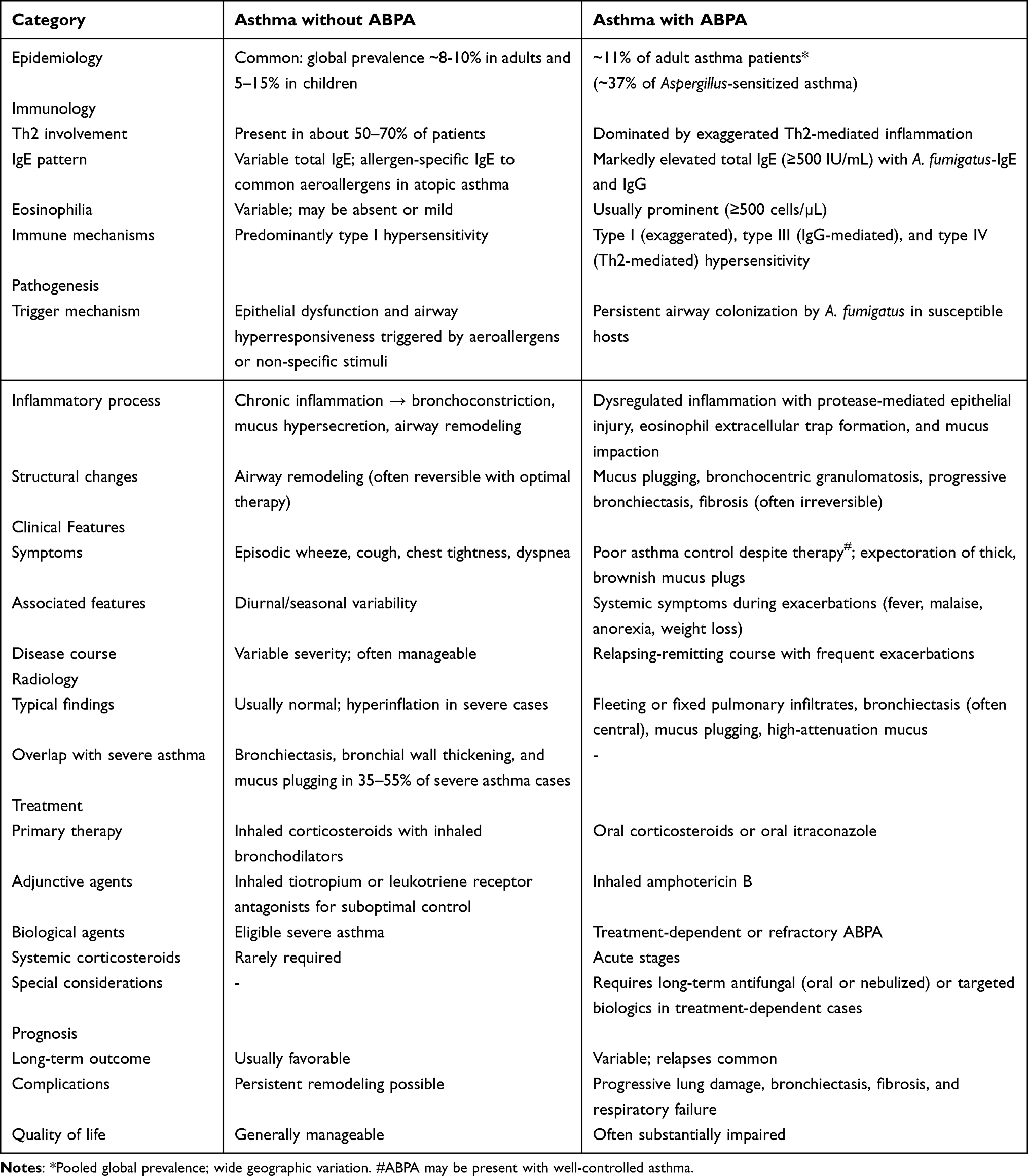 |
Table 1 Differences Between Asthma with and Without Allergic Bronchopulmonary Aspergillosis (ABPA) |
AS or ABPA-S are generally not associated with bronchiectasis and do not warrant ABPA-specific therapy beyond optimal asthma management. In contrast, ABPA-B requires targeted treatment with oral glucocorticoids, antifungal agents, or biological therapies.11 Some authors advocate an umbrella term, allergic fungal airway disease (AFAD), to encompass all airway conditions (asthma, cystic fibrosis, bronchiectasis) associated with fungal sensitization, irrespective of clinical phenotype.12,13 However, retaining condition-specific nomenclature better reflects underlying pathobiology, facilitates treatment stratification, and enables focused research (Figure 1).
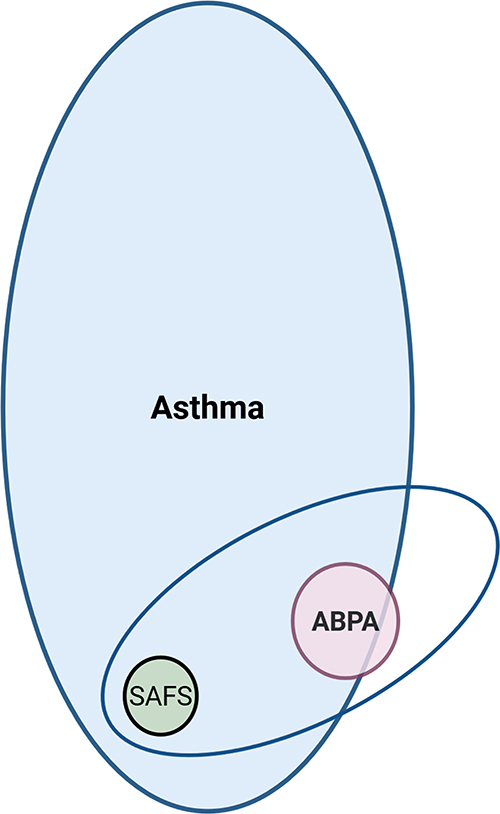 |
Figure 1 This Venn diagram illustrates the relationship between bronchial asthma, Aspergillus sensitization (AS), and allergic bronchopulmonary aspergillosis (ABPA). Asthma without demonstrable IgE sensitization to A. fumigatus constitutes the majority of cases (approximately 75%). AS alone refers to individuals with raised A. fumigatus-IgE but without asthma or ABPA and may also be detected in the general population (6% of healthy adults), reflecting the environmental ubiquity of A. fumigatus spores. Sensitization alone represents airway exposure and IgE production, but without the predisposing factors or immune dysregulation necessary for clinical disease. Approximately 25% of asthma patients exhibit elevated A.fumigatus-IgE. These individuals are classified as having A. fumigatus-associated asthma (AFAA) when asthma remains well-controlled, or severe asthma with fungal sensitization (SAFS) when asthma is poorly controlled. SAFS refers to severe asthma associated with sensitization to any fungal species (not restricted to A. fumigatus), and no other evident cause of severe asthma. SAFS is characterized by exaggerated type 2 inflammation but lacks the additional immunological dysregulation and tissue damage seen in ABPA. ABPA represents the most severe disease phenotype, occurring at the intersection of asthma, AS, and additional immunopathological dysregulation. ABPA is characterized by markedly elevated total IgE, A. fumigatus-specific IgE and IgG, eosinophilia, and imaging abnormalities. Approximately 11% of asthma patients develop ABPA, and nearly 37% of Aspergillus-sensitized asthma patients have ABPA. Uncommonly, ABPA can also occur without a prior asthma diagnosis. |
A pooled analysis of 86 worldwide studies involving over 25,000 asthma patients estimated a prevalence of approximately 25% for AS and 11% for ABPA, with nearly 37% of Aspergillus-sensitized asthma patients meeting diagnostic criteria for ABPA.14,15 Marked geographic variation in ABPA prevalence has been reported, reflecting differences in environmental fungal burden, host genetics, study setting (community versus referral centers), and diagnostic criteria. The prevalence of ABPA is generally lower in children. In a systematic review including 2,468 children with asthma across 16 studies, AS prevalence was 16.1%, while ABPA was identified in 9.9% of all asthmatic children and 20.5% of those with AS.16 Notably, ABPA in this review was reported exclusively from studies conducted in India. In contrast, a recent Turkish cohort study involving 2,599 children reported AS in 35.1% and ABPA in 2.7%, underscoring significant regional heterogeneity.17
Several challenges complicate the accurate estimation of ABPA prevalence in people with asthma.18 Most studies are conducted in referral centers, which may overestimate population prevalence.15 Community-based studies are resource-intensive, requiring systematic asthma diagnosis, measurement of A. fumigatus-IgE, and comprehensive evaluation of sensitized individuals for ABPA.19 The challenge is further compounded by the occurrence of ABPA in patients with well-controlled asthma,20 making symptom-based screening unreliable for epidemiological studies.
Pathobiology
The inflammatory cascade in allergic asthma is driven by type 2 helper T-cell (Th2)-mediated immune responses, with contributions from both innate and adaptive immunity. Inhaled aeroallergens disrupt or activate the airway epithelium, leading to the release of epithelial-derived alarmins, including thymic stromal lymphopoietin (TSLP), interleukin (IL)-33, and IL-25. These alarmins activate group 2 innate lymphoid cells (ILC2), which rapidly produce IL-5, IL-9, and IL-13, initiating early type 2 inflammation independent of antigen presentation.21 Sustained allergic sensitization, however, depends on adaptive immune responses. Dendritic cells (DCs), activated directly by alarmins and allergens, process and present antigens to naïve CD4+ cells, promoting Th2 differentiation through IL-4, IL-5, and IL-13-mediated signaling.22 IL-5 plays a central role in eosinophil differentiation, maturation, and survival, thereby driving eosinophilic inflammation (Figure 2). IL-5 also contributes to mast cell and basophil maturation through direct and indirect interactions, facilitating coordinated type 2 immune responses.23,24 The recruitment of Th2 cells, monocytes, and eosinophils into the airway wall culminates in bronchoconstriction, mucus hypersecretion, and airflow obstruction.9,21 With chronic antigen exposure, these processes result in airway remodeling, goblet cell hyperplasia, smooth muscle hypertrophy, and basement membrane thickening.25,26
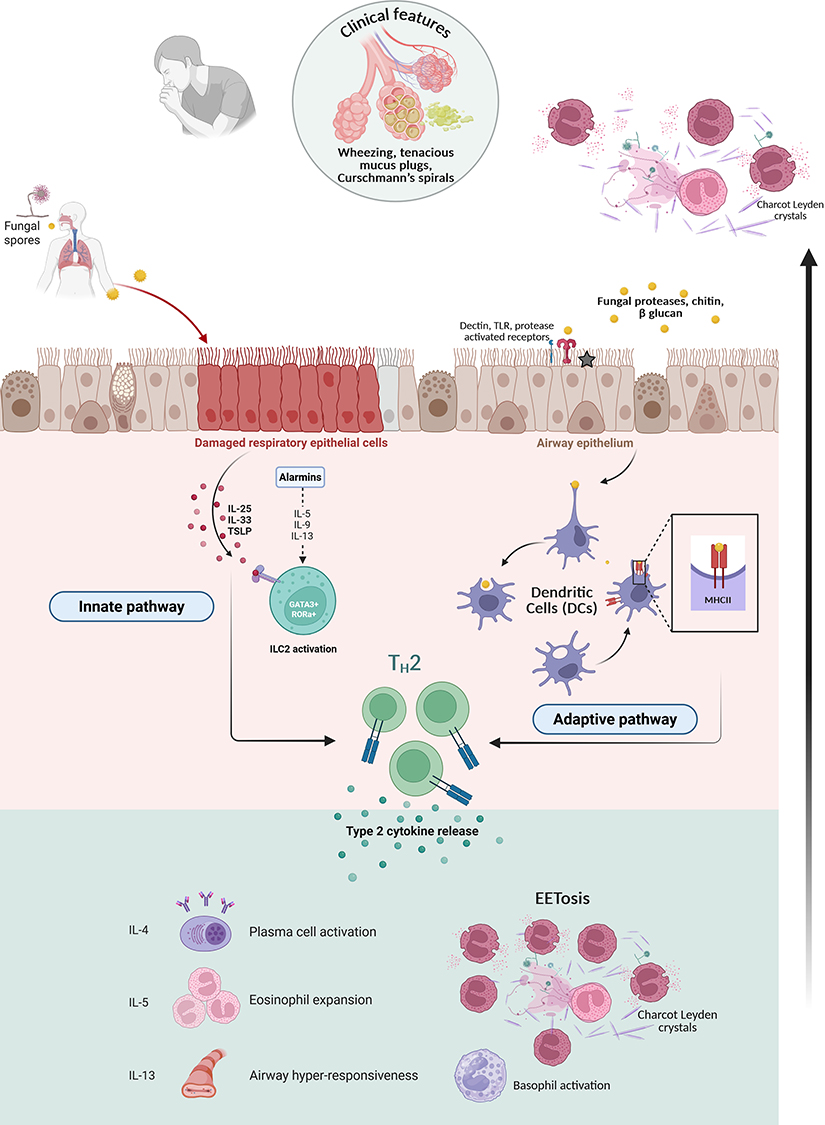 |
Figure 2 This schematic illustrates the innate and adaptive immune responses triggered by inhalation of fungal spores. Following airway deposition, fungal spores germinate and release bioactive products that directly activate or damage the airway epithelium, leading to epithelial dysfunction. Injured epithelial cells release alarmins, namely TSLP (thymic stromal lymphopoietin), interleukin (IL)-33, and IL-25, which activate group 2 innate lymphoid cells (ILC2). Activated ILC2 rapidly secrete type 2 cytokines (IL-5, IL-9, and IL-13), generating early type 2 inflammation independent of dendritic cell (DC) involvement or prior antigen sensitization. IL-5 promotes eosinophil recruitment, activation, and survival within the airways. Early consequences include bronchial hyperreactivity, goblet cell stimulation with mucus hypersecretion, and the formation of Charcot-Leyden crystals secondary to eosinophil degradation. This pathway produces early inflammation independent of sensitization. Consequently, alarmins activate DCs, which process fungal antigens and present them to naïve T-helper (Th0) cells, promoting differentiation into Th2 cells. Th2 cells provide help to naïve B cells through CD40-CD40L interactions and secretion of IL-4 and IL-13, inducing isotype class switching to IgE. Differentiated plasma cells produce fungal-specific IgE, which binds to high-affinity IgE receptors (FcεRI) on mast cells and basophils. Upon re-exposure to fungal antigens, IgE cross-linking triggers degranulation of mast cells and basophils, while Th2 cytokines (IL-4, IL-5) further amplify eosinophilic inflammation. These innate and adaptive immune responses perpetuate bronchial hyperreactivity, mucus production, and chronic type 2 inflammation. In susceptible individuals, persistent fungal exposure and sustained immune activation culminate in chronic, sensitization-dependent disease characteristic of ABPA. |
Fungal conidia vary widely in size (2–70 µm) and may deposit throughout the respiratory tract, from the nasal cavity to the distal bronchioles.27 In immunocompetent individuals, innate airway defenses, including mucociliary clearance, antimicrobial peptides, and phagocytosis, effectively eliminate fungal spores.28 In susceptible hosts (cystic fibrosis, allergic asthma), impaired innate defenses allow fungal spores to persist, germinate, and become biologically active in the airways.
A. fumigatus conidia (2–3 µm in diameter), a thermotolerant species, are initially immunologically inert due to their hydrophobic surface and the RodA protein layer.29 Upon germination, however, hyphal components, including β-glucans, proteases, chitins, glycosidases, and nucleic acids, act as pathogen-associated molecular patterns (PAMPs). These are recognized by pattern recognition receptors, including protease-activated receptors, toll-like receptors (TLRs), C-type lectin receptors (CLRs), mannose-binding lectins (MBLs), receptor for advanced glycation end products (RAGE), and dectins, which are expressed on epithelial cells and DCs.30
Additionally, A. fumigatus secretes a range of proteases and mycotoxins that disrupt epithelial barrier integrity and amplify immune recognition. Gliotoxin is a major virulent factor that impairs ciliary function and, along with fumagillin and helvolic acid, disrupts epithelial tight junctions. Ribotoxins, particularly restrictocin, induce epithelial cell death, increase epithelial permeability, and promote alarmin release. These processes expose core fungal antigens, which serve as the primary triggers of the IgE-mediated immune responses.31 This leads to AS through Th2-driven class switching of B lymphocytes.30,32 TLR-2 dependent pathways, often accompanied by upregulation of TLR-6, are preferentially activated, while protective TLR-4 and TLR-9-mediated responses are relatively suppressed.30,33 Persistent Aspergillus colonization results in activation of both DC-mediated Th2 and Th17 lymphocyte responses.9,30 Fungal persistence is facilitated by virulence factors such as aflatoxin B1, gliotoxin, and melanin that impair adherence, phagocytosis, and macrophage function.31,34,35 Regulatory T cells (Tregs) are also activated through TLR-2 signalling, exerting variable modulatory effects on Th2 and Th17 responses.9,30
In susceptible individuals, dysregulated type 2 inflammation, driven by Th2 cells and ILC2, with contributions from Th17 and neutrophils, leads to mucus plugging and tissue damage characteristic of ABPA/ABPM.36,37 Eosinophils form extracellular DNA traps that entangle fungal elements but fail to eradicate them. Eosinophilic extracellular trap cell death (EETosis) plays a pivotal role in the formation of tenacious mucus plugs.38 Progressive inflammation and obstruction lead to eosinophilic pneumonia, bronchocentric granulomatosis, bronchiolitis obliterans, and bronchiectasis. Histopathological findings typically include dense eosinophilic infiltrates, Charcot-Leyden crystals (crystallized galectin-10), and Curschmann’s spirals.7
Although severe asthma with or without ABPA shares overlapping inflammatory pathways,39 IgG-mediated inflammatory processes and progressive lung damage are less prominent in severe asthma without ABPA. Asthma is predominantly mediated by type 1 (IgE-mediated) hypersensitivity reactions to aeroallergens. In contrast, ABPA and ABPM are characterized by an exaggerated inflammatory response, involving additional type 3 (IgG-mediated immune complex) and type 4 (T-cell-mediated) hypersensitivity mechanisms, resulting in amplified tissue injury.40
Genetics of ABPA in Asthma
Asthma arises from complex interactions between genetic susceptibility and environmental exposures,8 characterized by polygenic inheritance and locus heterogeneity, whereby distinct genetic variants can result in similar clinical phenotypes.41–44 Key asthma-associated loci include the ORM1-like protein 3 and gasdermin protein (ORMDL3/GSDMB) region on chromosome 17q12-q21, IL13-RAD50-IL4 locus on chromosome 5q31, and variants in TSLP, IL-33, and its receptor ST2 (IL1RL1), many of which confer ethnic-specific associations.42 Additional polymorphisms involve genes encoding MHC-class II molecules (HLA-DQA1, HLA-DQB1), TLR1, ZPBP2, GSDMA, and IL6R.41,43–47
Fungal sensitization and ABPA/ABPM demonstrate distinct genetic predispositions involving genes that regulate innate and adaptive immunity, as well as mucociliary function and epithelial integrity.48–53 A nonsense single-nucleotide polymorphism (SNP, rs35699176) in zinc finger protein 77 (ZNF77) disrupts epithelial barrier function, promotes extracellular matrix accumulation, and facilitates fungal colonization.54 Several SNPs distinguish SAFS from atopic asthma without SAFS, particularly in genes related to pattern recognition (TLR3, TLR9, dectin-1), immune regulation (IL-10, MBLs), chemotaxis (CCL2, CCL17), fibrinolysis (plasminogen), and adenosine signaling (A2A receptor).51
ABPA-specific genetic associations include polymorphisms in surfactant protein A, which influence disease severity and clinical expression.55 Polymorphisms in the IL-4 receptor alpha chain and early endosome antigen 1 (involved in phagocytosis) genes predispose to exaggerated Aspergillus-specific humoral and cellular immune responses.52,56 Specific SNPs in IL13 (rs20541), IL4R (rs3024656), and TLR3 (rs1879026), as well as macrophage gene expression variants, have been associated with ABPA development.50 HLA genotype remains a critical determinant, conferring susceptibility or protection against fungal sensitization and ABPA, and influencing the skewing of immune responses toward type 2 inflammation.57
Clinical Features
ABPA affects individuals across all age groups, with notable geographic variation in the age at presentation. Patients in Japan and France tend to present at a higher mean age compared with those in India and China.58–60 Within the asthma population, approximately 17–18% have difficult-to-treat asthma, while only 3–4% fulfill criteria for severe asthma.61 Both AS and ABPA are recognized asthma endotypes and are frequently associated with poor asthma control, severe symptoms, and high medication requirements.62,63
Although a minority of patients with ABPA may be minimally symptomatic, most exhibit poor asthma control. A characteristic clinical feature is the expectoration of thick, tenacious mucoid sputum, often with a brown-black discoloration, reported in approximately one-third of patients.64,65 Other symptoms include hemoptysis, low-grade fever, malaise, anorexia, and weight loss.7 These manifestations overlap substantially with SAFS and chronic respiratory infections (particularly tuberculosis), creating diagnostic challenges.
Wheeze remains the predominant auscultatory finding in both asthma and ABPA. Crackles are uncommon in asthma alone (approximately 12%) but occur more frequently in the presence of ABPA or associated bronchiectasis.66 Patients with advanced disease may demonstrate features of lung collapse, hypoxemia, and pulmonary hypertension.67
Imaging
Characteristic Findings of ABPA
Imaging abnormalities in ABPA arise from eosinophilic pneumonia, mucus impaction, chronic airway inflammation, and fibrosis. Chronic airway inflammation manifests as bronchial wall thickening (BWT) and bronchiectasis. Although central bronchiectasis is considered a characteristic feature of ABPA, up to 40% of patients may also demonstrate peripheral bronchiectasis.68 Eosinophilic pneumonia produces transient parenchyma abnormalities, including consolidation, ground-glass opacities (GGO), centrilobular nodules with tree-in-bud appearance, and fleeting opacities. Mucus impaction results in characteristic fleeting opacities and classic “toothpaste” or “finger-in-glove” shadows, representing mucus-filled, dilated bronchi, and may cause segmental or lobar atelectasis.
High-resolution computed tomography (CT) of the chest is indispensable for the initial evaluation of ABPA, as it delineates the extent of bronchiectasis and helps exclude alternate diagnoses. High-attenuation mucus (HAM), defined by attenuation greater than that of paraspinal muscles or ≥70 Hounsfield units, is highly specific (100%) for ABPA diagnosis, independent of other imaging features, and is associated with poorer disease control and prognosis.69 For follow-up, chest radiography is usually sufficient, with repeat HRCT reserved for clinical indications. Many radiological opacities, such as mucus plugging, consolidations, GGOs, BWT, and nodules, may regress with effective treatment; however, discordance between radiological, clinical, and immunological responses is frequently observed.70
Advanced ABPA is characterized by extensive bronchiectasis, pleuroparenchymal fibrosis, cavitation, and architectural distortion. A subset of patients may develop concomitant chronic pulmonary aspergillosis, necessitating careful treatment adjustment.71,72 Recently, inverted mucoid impaction signal (high T1 and low T2 signal intensity) on magnetic resonance imaging (MRI) showed high sensitivity (94%), and specificity (100%) in cystic fibrosis-related ABPA.73,74 However, MRI provides limited incremental diagnostic value over CT in asthmatic ABPA.75
Imaging Overlap with Severe Asthma
Several imaging abnormalities observed in ABPA may also be present in severe asthma without ABPA, complicating differential diagnosis.76–78 In a retrospective analysis of 108 patients with severe asthma (excluding ABPA), 55% demonstrated at least one HRCT abnormality, including bronchiectasis (35%; cylindrical or varicose) and BWT (33%), with lower frequencies of atelectasis, mosaic attenuation, emphysema, and tree-in-bud opacities.78 Although other etiologies of bronchiectasis were not systematically excluded, these findings underscore the need to evaluate all asthma patients with bronchiectasis or other unexplained CT abnormalities for ABPA.77 Comorbid conditions such as chronic rhinosinusitis and gastroesophageal reflux disease may contribute to airway injury and bronchiectasis in asthma. Consequently, imaging abnormalities suggestive of ABPA should prompt comprehensive clinical, immunological, and radiological assessment to establish an accurate diagnosis and guide appropriate management.79
Screening and Diagnosis of ABPA in Asthma
In the absence of a single gold-standard diagnostic test, the diagnosis of ABPA relies on a composite assessment integrating predisposing conditions with clinical, immunological, and radiological findings. Optimal combinations of diagnostic tests and thresholds have been derived using latent class analyses of large asthma cohorts.80–84 The International Society for Human and Animal Mycoses (ISHAM) ABPA working group recently updated recommendations for diagnosing AS, ABPA, and ABPM in patients with asthma (Table 2 and Figure 3).85 This revised diagnostic framework improves diagnostic accuracy compared with earlier criteria.81,86–88
 |
Table 2 The 2024 Updated ISHAM Diagnostic Criteria for ABPA/ABPM |
 |
Figure 3 This diagnostic algorithm provides a systematic approach to evaluating patients with asthma for allergic bronchopulmonary aspergillosis (ABPA) using the 2024 International Society for Human and Animal Mycoses (ISHAM) working group criteria. Black boxes indicate disease categories, blue boxes denote actions or presentation, and Orange boxes represent assessment or decision points. In patients with predisposing conditions (bronchial asthma, cystic fibrosis, bronchiectasis, or chronic obstructive pulmonary disease) or a compatible clinical-radiological presentation, the initial step is to identify fungal sensitization (serum Aspergillus fumigatus [Af]-specific IgE ≥0.35 kUA/L). If Af-IgE is below this threshold, ABPA is unlikely, and further evaluation is not required unless clinical suspicion for non-Aspergillus fungal disease remains high (*). In those with AS, a serum total IgE value ≥500 IU/mL indicates systemic immune activation (lower IgE levels may be acceptable if all other diagnostic components are fulfilled). Patients meeting essential criteria (AfIgE plus total IgE) undergo assessment for three additional components: blood eosinophil count ≥500 cells/µL, elevated AfIgG, and chest CT findings consistent with ABPA. ABPA diagnosis requires meeting ALL essential criteria PLUS any two of these three additional components. Radiological classification based on chest CT includes: (1) ABPA-S (serological ABPA): immunological criteria fulfilled, but there is no bronchiectasis; (2) ABPA-B (ABPA with bronchiectasis): bronchial dilation (bronchus-to-artery ratio >1); (3) ABPA-MP (ABPA with mucus plugging): mucus-impacted airways without high attenuation mucus; (4) ABPA-HAM (ABPA with high-attenuation mucus): mucus plugs with radiographic density ≥70 Hounsfield units or exceeding paraspinal muscle density; (5) ABPA-CPF (ABPA with chronic pleuroparenchymal fibrosis): irreversible architectural distortion, pleural involvement, and possible cavitation with or without mycetoma. |
Initial Screening for AS
In tertiary care settings, all adult asthma patients, irrespective of disease severity, and all children with difficult-to-treat asthma should be screened for ABPA by measuring serum A. fumigatus-specific IgE (AfIgE).20,85 AfIgE is quantified using standardized fluorescent enzyme immunoassay (FEIA) platforms. A cut-off of 0.35 KUA/L provides excellent sensitivity (99%) but modest specificity (72%), making it suitable for initial screening.83 An optimized cut-off of 0.7 KUA/L significantly improves specificity while maintaining acceptable sensitivity, thereby providing superior overall diagnostic accuracy in clinical practice.82 Skin-prick testing with crude Aspergillus antigen is a less preferable alternative, with reported sensitivity ranging from 88–94%. Measurement of mx-4 IgE, which assesses sensitization to four Aspergillus species (A. fumigatus, A. flavus, A. niger, and A. terreus), has not demonstrated diagnostic superiority over AfIgE alone.89 In AfIgE-negative patients with strong clinical or radiological suspicion, evaluation for sensitization to other fungi should be considered, particularly when non-Aspergillus species are identified in respiratory samples.
Assessment of Type 2 Inflammation and Dysregulation
Asthma patients with documented fungal sensitization should undergo further evaluation for exaggerated type 2 inflammation by measuring serum total IgE levels. A total IgE level exceeding 500 IU/mL is considered positive (sensitivity >97%, specificity 49.3%), although lower levels may be acceptable in the presence of other supportive diagnostic features.
Patients who meet criteria for sensitization and elevated total IgE should be evaluated for additional immunological and structural manifestations of disease, including type 1 hypersensitivity (blood eosinophils), type 3 hypersensitivity (A. fumigatus-IgG [AfIgG]), and radiological abnormalities. Blood eosinophil counts ≥500 cells/µL are considered positive, though values may fluctuate with treatment or intercurrent infections; historical values therefore provide valuable diagnostic context.90 Although sputum eosinophil counts more accurately reflect eosinophilic lung inflammation, their technical complexity and limited availability necessitate reliance on peripheral blood eosinophils as a surrogate marker.
AfIgG can be measured using automated enzyme immunoassays, lateral-flow assays, or traditional precipitation-based methods, such as counter-immunoelectrophoresis. Automated immunoassays and lateral-flow methods are preferred owing to superior diagnostic performance.91–94 Ideally, cut-offs should be validated for specific populations and assay platforms; in their absence, manufacturer-recommended thresholds may be used.85
Diagnostic Criteria
The diagnosis of ABPA requires evidence of fungal sensitization (positive AfIgE) and immunological disease activity (total IgE ≥ 500 IU/mL), in addition to at least two of the following three features: elevated blood eosinophil count, positive AfIgG, or radiological abnormalities consistent with ABPA (Table 2). For ABPM, fungus-specific IgE and IgG replace their Aspergillus counterparts, and microbiological confirmation of the implicated fungus (from two sputum or one bronchoalveolar lavage sample) is included as an additional diagnostic component. It is important to acknowledge that airway mycobiota comprise multiple fungi, and the organism isolated from the respiratory sample may not necessarily be the primary driver of sensitization or disease activity.95–98 Nevertheless, fungal cultures remain valuable, particularly for evaluating azole resistance in patients with suboptimal response to antifungal treatment.
Newer Tests
Recombinant A.fumigatus Antigens
Several A. fumigatus antigens (rAsp f1-f34) have been identified, with recombinant forms of rAsp f1, f2, f3, f4, and f6 currently available for clinical use. Measurement of IgE against these recombinant antigens can aid in the diagnosis of ABPA/ABPM. Among them, rAsp f1-specific IgE offers the best balance of sensitivity and specificity, while multiplex testing with rAsp f1, f2, and f4 improves diagnostic accuracy compared to single-antigen testing.99 However, the utility of these assays is increasingly constrained by the 2024 ISHAM guideline redefinition of ABPA to include disease caused by all Aspergillus species. Consequently, A. fumigatus-specific recombinant antigens may fail to identify non-fumigatus ABPA. This highlights the need for pan-Aspergillus antigen detection strategies rather than reliance on single species antigens. Further assay standardization, population-specific validation, and refinement of multiplex approaches are required before widespread clinical adoption.100,101
Basophil Activation Test (BAT)
Basophils contribute to ABPA immunopathogenesis through allergen-specific IgE-mediated activation. Cross-linking of basophil-bound IgE by fungal antigens induces upregulation of surface activation markers, such as CD63 and CD203c, measured by flow cytometry.102,103 However, in one study, BAT had limited diagnostic accuracy in distinguishing ABPA complicating asthma from AFAA or A. fumigatus unsensitized asthma.104 In contrast, BAT appears to perform better in ABPA associated with cystic fibrosis patients, likely reflecting a higher airway fungal burden. Additionally, false-positive results may occur in atopic individuals, a phenotype far more prevalent in asthma than cystic fibrosis, further limiting the utility of BAT in asthmatic populations.104,105
Fraction of Exhaled Nitric Oxide (FeNO)
Type 2 airway inflammation is associated with increased inducible nitric oxide synthase (iNOS) expression in the bronchial epithelium, primarily driven by IL-4 and IL-13. FENO therefore serves as a noninvasive marker of type 2 airway inflammation and may help monitor disease activity and treatment response in ABPA.106–108 FENO levels are higher in patients with ABPA or ABPM compared to those with AS alone or non-sensitised asthma. Among patients with ABPM, higher FeNO correlated with higher eosinophil counts and greater mucus-plug burden.107 Elevated FeNO has also been associated with increased risk of relapse and the need for prolonged systemic glucocorticoid therapy.106 Although promising, the precise role of FeNO in diagnosis and longitudinal monitoring remains to be further validated.
Classification and Staging
Radiological Classification of ABPA
The 2024 ISHAM revision introduces a standardized radiological classification system for ABPA, with important implications for disease severity assessment and prognosis. Based on chest CT findings, ABPA is classified into five radiological categories (Figure 3). The presence of HAM or extensive bronchiectasis (≥10 segments on CT) identifies patients with higher disease activity, more severe clinical manifestations, and poorer outcomes. Chronic pleuroparenchymal fibrosis (CPF) represents irreversible structural lung changes and is associated with progressive functional impairment, reduced quality of life, and an increased risk of complications such as pulmonary hypertension and recurrent infections. In patients with ABPA-CPF, concomitant chronic pulmonary aspergillosis should be actively excluded, given its therapeutic and prognostic implications.109
ABPA Clinical Classification
The 2024 ISHAM revision simplifies the earlier seven-stage system into five clinically relevant disease states (Figure 4).85 This streamlined staging system facilitates early identification of relapses, reliably distinguishes true ABPA exacerbations from common mimics (such as asthma or infective bronchiectasis exacerbations), and guides initiation, escalation, or de-escalation of therapy. Importantly, it helps standardize communication among clinicians, enabling meaningful comparisons across clinical studies by relying on objective, reproducible criteria rather than subjective clinical judgment.
- Acute ABPA: This category includes both newly diagnosed patients (first presentation fulfilling ABPA diagnostic criteria) and disease exacerbations in previously diagnosed individuals. An exacerbation is defined by ≥2 weeks of worsening respiratory symptoms and/or radiological deterioration, accompanied by a ≥50% increase in serum total IgE from the patient’s last stable or remission value. This multiparameter definition minimizes misclassification due to isolated symptom fluctuations or nonspecific radiological findings. Potential mimics must be carefully excluded. Asthma exacerbations present with worsening symptoms without corresponding immunological (IgE rise) or radiological changes, whereas bronchiectasis exacerbations are characterized by infective features (bacterial/ viral), without IgE elevation or new ABPA-related radiological abnormalities.
- Response: Treatment response is evaluated at eight weeks using integrated criteria defined by clinical (≥50% reduction in symptoms compared to baseline) improvement, along with either radiological (≥50% clearance of opacities) or immunological (≥20% reduction in serum total IgE) improvement. Patients demonstrating optimal response continue pharmacotherapy for a total duration of 4 months. Patients who fail to achieve an adequate response require reassessment, with exclusion of alternative diagnoses, evaluation of medication adherence, measurement of itraconazole trough levels, assessment of azole resistance, and evaluation for concurrent infections or other complications. Treatment escalation or modification is guided by these findings.
- Remission: Remission denotes sustained disease control sufficient to allow discontinuation of systemic corticosteroids for at least 6 months. Patients in remission demonstrate stable clinical status, immunological (total IgE elevation <50% from nadir), and radiological stability. ABPA-specific therapy is discontinued, while standard asthma therapy and periodic surveillance continue. Some patients maintain remission only with antifungal therapy or targeted biologics.
- Treatment-dependent ABPA: Treatment-dependent ABPA is characterized by an inability to discontinue ABPA-specific therapy without relapse. Patients in this category are defined as experiencing: (i) ≥2 consecutive exacerbations within 3 months after stopping ABPA-specific treatment; or (ii) clinical (recurrent symptoms, airflow limitation deterioration), radiological (new or worsening infiltrates), or immunological (serum total IgE elevation) worsening within 4 weeks of glucocorticoid tapering on two separate occasions.
- Advanced ABPA: Advanced ABPA is characterized by irreversible end-organ damage defined by extensive bronchiectasis (typically ≥10 CT segments) and pulmonary hypertension or chronic type 2 respiratory failure. Notably, immunological activity may persist despite structural damage, and ABPA-specific therapy may still be required to prevent further disease progression.
 |
Figure 4 This clinical staging and management algorithm illustrates treatment strategies of allergic bronchopulmonary aspergillosis (ABPA) at each stage. Orange boxes represent disease categories, green boxes denote therapeutic interventions, and blue boxes indicate assessment or decision points. Disease trajectories: Optimal (remission): Newly diagnosed/exacerbation → treatment initiation → assessment at 8 weeks → response → completion of 4-month therapy → remission → discontinuation of ABPA-specific therapy → periodic surveillance. *Exacerbation: Patients with ABPA exacerbation are treated similarly to those with newly diagnosed ABPA. Those with frequent exacerbations (≥2 in 1–2 years) may be treated with a combination of oral corticosteroids (OCS) and itraconazole for 4 months. #Treatment-dependent ABPA: Defined by the inability to discontinue ABPA-specific therapy without relapse and typically requires long-term treatment with prolonged antifungals (6–12 months of itraconazole), biological agents, or nebulized amphotericin B. **Advanced ABPA: Management prioritizes symptom control, complication prevention (including infection risk and pulmonary hypertension management), and quality-of-life optimization. Complicated (treatment-dependent): Initial response achieved, but relapse occurs on tapering → prolonged monotherapy or combination therapy → remission or recurrent relapse cycles. Progressive: Treatment-dependent disease with inadequate control → progressive lung damage → cor pulmonale and respiratory failure → advanced ABPA. Relapsing: Remission achieved → stability ≥6 months → relapse with symptoms, radiological worsening, and IgE elevation → reinitiation of treatment. Monitoring frequency by stage: → Acute ABPA: every 8 weeks during treatment; Treatment-dependent ABPA: every 8–12 weeks; Remission: every 4–6 months; Advanced ABPA: every 8–12 weeks with multidisciplinary care. |
Management
The two central pathogenic processes in ABPA are persistent airway fungal colonization and an exaggerated type 2 immune response. Accordingly, treatment principles include controlling immunological activity and reducing airway fungal burden.
All asthma patients, irrespective of ABPA, receive inhaled corticosteroids (ICS) combined with bronchodilators for both symptom relief and disease control,110 with dosages individualized according to clinical response. Leukotriene receptor antagonists or inhaled long-acting muscarinic antagonists may be added in patients with suboptimal control despite moderate-dose ICS. After exclusion and management of comorbid conditions, many severe asthma patients benefit from targeted biologics.111
Anti-Inflammatory Therapy
Systemic corticosteroids remain a cornerstone of therapy for acute ABPA, including both newly diagnosed disease and exacerbations. The 2024 ISHAM guidelines recommend medium-dose oral corticosteroids (OCS) for approximately four months.85,112 A commonly used dosing protocol consists of oral prednisolone at 0.5 mg/kg/day, 0.25 mg/kg/day, and 0.125 mg/kg/day, each for four weeks, with subsequent tapering by 5 mg every two weeks until discontinuation (Table 3). Biological agents targeting IL-5, IL-4, IL-13, IgE, or thymic stromal lymphopoietin (TSLP) suppress type-2 inflammation and reduce OCS dependence. However, despite growing real-world evidence, high-quality evidence remains limited, with only one randomized trial published to date.113–118 Consequently, biologics are currently recommended primarily for treatment-dependent ABPA.85
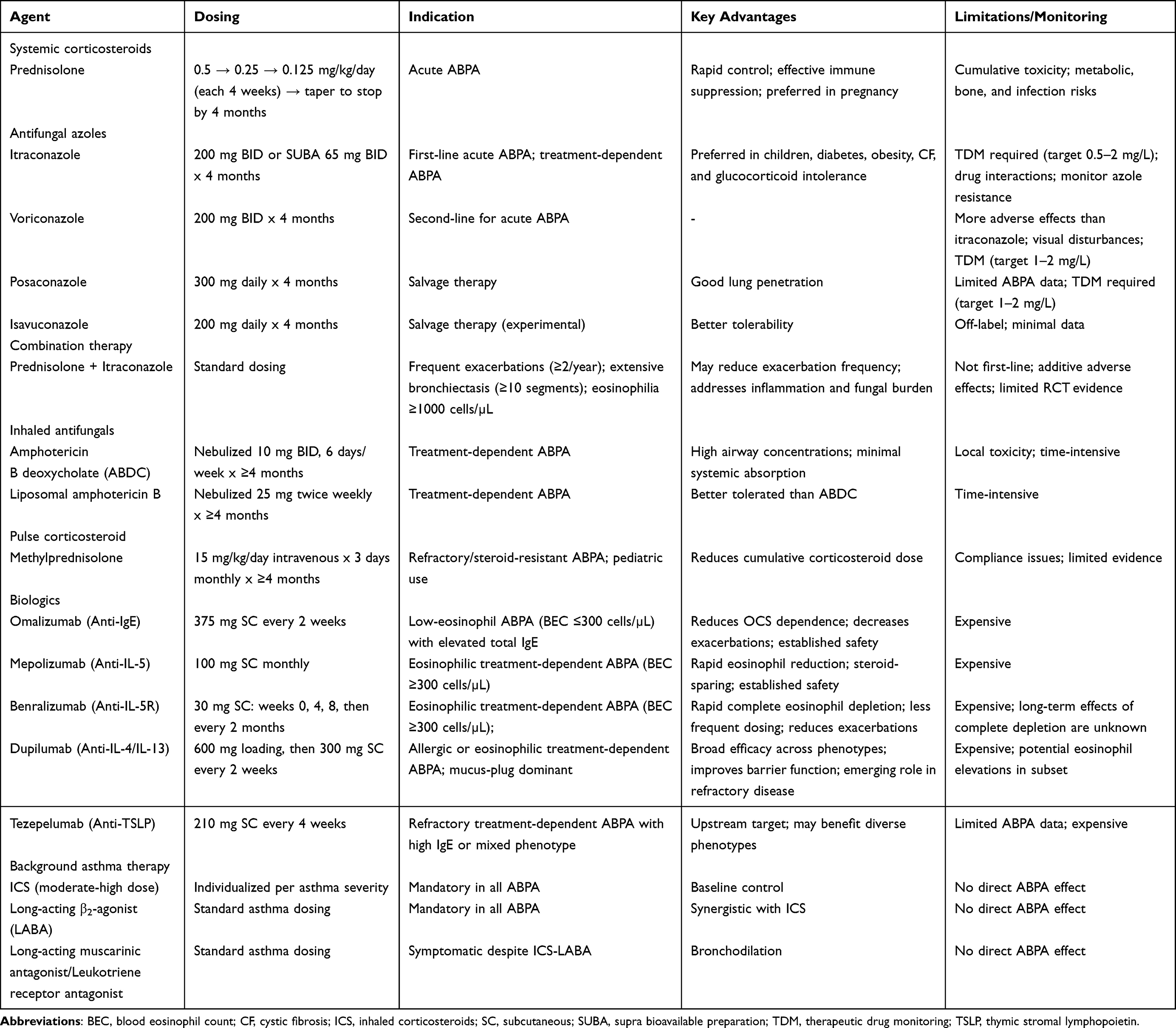 |
Table 3 Pharmacotherapy for Allergic Bronchopulmonary Aspergillosis (ABPA) |
Anti-Fungal Therapy
Oral triazoles, primarily itraconazole, constitute another first-line treatment option in ABPA (Table 3).85,119–130 Itraconazole is the most extensively studied azole and is typically given for four months at a dose of 200 mg twice daily (or 130 mg twice daily for the supra-bioavailable [SUBA] preparation). Prolonged therapy may be required in refractory disease or in patients with frequent relapses, although long-term use is limited by adverse effects, drug interactions, and cost. Common adverse effects of itraconazole include headache and gastrointestinal symptoms, while more serious side effects include hepatotoxicity, hypokalemia, peripheral edema, and cardiac dysfunction in susceptible individuals. Voriconazole can additionally cause photosensitivity, QT interval prolongation, and neuro-psychiatric effects. The monthly cost of therapy in India ranges from approximately ₹1,200 to ₹2,500 (about $15 to $30 USD). Therapeutic drug monitoring (TDM) is recommended to ensure adequate bioavailability, particularly with conventional itraconazole preparations, and remains advisable with SUBA preparations as well.131–134 Patients with suboptimal clinical response warrant evaluation for azole resistance, and treatment should be modified accordingly.135–138
Inhaled amphotericin is reserved for patients with treatment-dependent ABPA, azole intolerance, or azole resistance.58,130,139–141 Although two randomized trials of nebulized amphotericin B deoxycholate and liposomal amphotericin B did not meet their primary endpoints, secondary endpoint analyses suggested potential benefits, supporting further investigation with optimized dosing strategies.58,130
Novel inhaled triazole formulations, including itraconazole, voriconazole, and opelconazole, are under development and may expand therapeutic options for long-term management.142–145 Inhaled itraconazole has demonstrated encouraging results in Phase 1 and Phase 2 studies and is proceeding to Phase 3 evaluation.144 Inhaled voriconazole remains in pre-clinical and phase 1 development,143 while a phase 3 study of inhaled opelconazole in invasive aspergillosis was terminated early after interim analysis.
Management by Disease Stage (Figure 4)
Acute ABPA: For newly diagnosed disease or exacerbations, monotherapy with either OCS or triazoles is recommended (Table 3). Triazoles demonstrate efficacy comparable to OCS in most patients and are preferred when minimizing OCS exposure is clinically desirable (obesity, diabetes mellitus, osteoporosis, chronic bacterial colonization, and other corticosteroid-related risk factors).126,146 OCS are preferred in patients with poorly controlled asthma, underlying liver disease, or in clinical situations where a rapid therapeutic response is required, or triazoles are contraindicated. In patients with poor asthma control and significant symptoms, an alternative strategy is an initial 2-week combination of OCS, followed by continuation of azole therapy for a total of 4 months.85 Patients with frequent exacerbations, especially those with extensive bronchiectasis or peripheral blood eosinophil count ≥1000 cells/µL, may benefit from combination therapy with OCS and itraconazole for 4 months.129
Treatment-dependent ABPA: These patients often require prolonged triazole therapy, biological agents, or inhaled antifungal drugs after acute disease is controlled with oral prednisolone or itraconazole. Careful attention to minimizing adverse effects associated with pharmacotherapy is essential.
Remission: ABPA-specific antifungal and anti-inflammatory therapies are typically discontinued during remission, while standard asthma therapies continue. Patients achieving remission with antifungal or biologic agents require periodic reassessment to determine ongoing therapy requirements. Structured monitoring every 4–6 months includes clinical assessment, serum total IgE measurement, and spirometry, enabling early detection of disease deterioration.85
Advanced ABPA: In advanced disease, management priorities extend beyond immunological control to include symptom management, complication prevention, and quality-of-life optimization. Bronchiectasis management parallels approaches for non-ABPA bronchiectasis.79 Long-term oxygen therapy (PaO2 ≤55 mmHg or cor-pulmonale), vaccinations (pneumococcus, annual influenza, and others), pulmonary rehabilitation, and airway clearance techniques are guided by established recommendations for other chronic lung conditions.79 Although a recent trial failed to demonstrate the benefit of nebulized hypertonic saline in reducing bronchiectasis exacerbations,147 patients with ABPA-associated bronchiectasis may still benefit, given the predominance of mucus plugging. Patients with chronic bacterial colonization and frequent (≥2 moderate/≥1 severe) exacerbations should receive inhaled antibiotics or long-term macrolides, guided by sputum culture results.148–150 Infection with non-tuberculous mycobacteria must be excluded before macrolide initiation. Patients experiencing recurrent bronchiectasis exacerbations despite optimized ABPA therapy may benefit from brensocatib,151 though its role in ABPA-associated bronchiectasis requires dedicated randomized trials.
Disease Monitoring and Response Assessment
ABPA is characterized by a relapsing-remitting course, necessitating systematic monitoring to distinguish true disease relapses from alternative causes of clinical deterioration. Core monitoring parameters include symptom assessment (preferably quantified using validated objective tools), chest radiography, and serum total IgE measurement. Optimal treatment response at 8 weeks is defined by ≥50% symptom improvement, accompanied by a ≥20% reduction in serum IgE levels or ≥50% radiological resolution. Relapse or exacerbation is defined by sustained (≥2 weeks) worsening of symptoms or radiological worsening combined with a ≥50% rise in serum total IgE. Importantly, symptom worsening or imaging may result from asthma exacerbations unrelated to fungal triggers, intercurrent infections, bronchiectasis exacerbation, and other comorbidities,85,152 all of which must be systematically excluded before escalating ABPA-specific therapy (Figure 4).
Asthma patients without AS should be re-evaluated every 2–5 years, as sensitization may emerge over time due to ongoing environmental exposure.153 Patients with AS but without ABPA require closer monitoring, with serum IgE reassessed every 6–12 weeks or whenever asthma control deteriorates without an alternative explanation.
Management of ABPA in the Pediatric Population
ABPA is less common in children than in adults, though both AS and ABPA in asthma are reported more frequently in developing countries, especially India.16 Management is particularly challenging due to concerns regarding OCS toxicity, especially effects on growth, bone density, and glucose metabolism.154 Monthly intravenous methylprednisolone pulses have been used in children with cystic fibrosis and ABPA to reduce cumulative toxicity155 but robust pediatric data is lacking.156,157 Triazole therapy is complicated by variable bioavailability and poor tolerance.158,159 Posaconazole may be better tolerated and more likely to achieve therapeutic levels in children. A recent trial evaluating the optimal dosing strategy for posaconazole in children with cystic fibrosis and Aspergillus infection was prematurely terminated due to poor recruitment.160 Among biologics, omalizumab and mepolizumab are approved for children ≥6 years, while benralizumab is approved for those aged ≥12 years. Current guidelines recommend treating children with ABPA similarly to adults, acknowledging that most recommendations are extrapolated from adult and expert consensus. Prospective validation in children is urgently needed.
Challenges and Future Directions
Current standards of care for ABPA, including universal screening for AS, systematic diagnosis using multiple serological tests and HRCT, therapeutic drug monitoring for azole therapy, serial measurement of total serum IgE, and the use of costly biologics for treatment-dependent disease, pose a significant challenge in resource-limited and austere settings. This is particularly problematic in developing countries, where, paradoxically, ABPA is more prevalent, and limits the feasibility of implementing the recommended diagnostic and therapeutic guidelines in clinical practice. Future research should prioritize simplifying diagnostic algorithms and management strategies for ABPA. Validation of more affordable and accessible diagnostic tests and treatments is essential to improve the delivery of quality care and to enable early diagnosis and treatment in high-burden settings.161,162
Despite decades of research, ABPA diagnosis relies on an integrated interpretation of multiple clinical, immunological, and radiological parameters, with no single definitive gold-standard test. Future investigations should focus on identifying novel biomarkers and imaging features to enhance diagnostic accuracy, enable reliable disease monitoring, and guide treatment selection across the spectrum of AS, ABPA, and ABPM. Concurrently, precision therapies targeting dysregulated inflammatory processes with biological agents, along with technological advances in inhaled antifungal delivery systems, are expected to further improve clinical outcomes and patient quality of life.142,163
Conclusion
Patients with asthma and atopy exhibit heterogeneous responses to environmental fungal exposure, particularly to thermophilic moulds such as Aspergillus species. The clinical spectrum of these interactions ranges from asymptomatic fungal sensitization and poorly controlled asthma to ABPA with structural lung damage. Although asthma with and without ABPA shares overlapping pathobiological mechanisms and clinical features, systematic differentiation remains essential for accurate diagnosis, appropriate therapeutic targeting, and prognostication.
Universal screening of asthma patients for AS, followed by comprehensive evaluation of sensitized individuals for ABPA, represents the cornerstone of early diagnosis and prevention of disease progression. Affected patients require treatment with anti-inflammatory or antifungal therapy, and when indicated, biological agents or inhaled antifungal drugs tailored to disease severity and phenotype. High-quality translational research and clinical trials remain essential to fully elucidate ABPA pathobiology, clarify the natural course of ABPA within asthma populations, and establish evidence-based management protocols. These efforts will facilitate precision-medicine approaches enabling individualized risk stratification, optimized treatment selection, and improved prognostication for patients across the asthma-ABPA spectrum, ultimately improving outcomes and reducing the burden of long-term complications associated with ABPA.
Data Sharing Statement
Data sharing does not apply to this article as no new data were created or analyzed in this study.
Author Contributions
Conceptualization: RA; Data curation: PS, RA; Methodology: PS, VM, ISS, RA; Supervision: VM, ISS, RA; Writing – original draft: PS, VM, ISS, RA; Writing – review & editing: PS, VM, ISS, RA.
All authors have given final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received for this review or during the preparation of this manuscript.
Disclosure
RA- received institutional grants from Cipla Pharmaceuticals, India, for conducting research in ABPA. The authors report no other conflicts of interest in this work.
References
1. Arbes SJ Jr, Gergen PJ, Vaughn B, Zeldin DC. Asthma cases attributable to atopy: results from the Third National Health and Nutrition Examination Survey. J Allergy Clin Immunol. 2007;120(5):1139–23. doi:10.1016/j.jaci.2007.07.056
2. Wang F, He XY, Baines KJ, et al. Different inflammatory phenotypes in adults and children with acute asthma. Eur Respir J. 2011;38(3):567–574. doi:10.1183/09031936.00170110
3. Douwes J, Pearce N. Epidemiology of respiratory allergies and asthma. In: Ahrens W, Pigeot I, editors. Handbook of Epidemiology. Springer New York; 2014:2263–2319.
4. Adhikari A, Sen MM, Gupta-Bhattacharya S, Chanda S. Airborne viable, non-viable, and allergenic fungi in a rural agricultural area of India: a 2-year study at five outdoor sampling stations. Sci Total Environ. 2004;326(1–3):123–141. doi:10.1016/j.scitotenv.2003.12.007
5. Mullins J, Hutcheson PS, Slavin RG. Aspergillus fumigatus spore concentration in outside air: cardiff and St Louis compared. Clin Allergy. 1984;14(4):351–354.
6. Rönmark E, Bunne J, Bjerg A, et al. Prevalence and risk factors for allergic sensitization: 3 cross-sectional studies among schoolchildren from 1996 to 2017. J Allergy Clin Immunol Glob. 2023;2(4):100150. doi:10.1016/j.jacig.2023.100150
7. Saxena P. Allergic bronchopulmonary aspergillosis: what’s new. Curr Pulmonol Rep. 2025;14(1):1–14.
8. Barnes C. Fungi and atopy. Clin Rev Allergy Immunol. 2019;57(3):439–448. doi:10.1007/s12016-019-08750-z
9. Agarwal R, Muthu V, Sehgal IS. Relationship between Aspergillus and asthma. Allergol Int. 2023;72(4):507–520. doi:10.1016/j.alit.2023.08.004
10. Muthu V, Sehgal IS, Prasad KT, et al. Allergic bronchopulmonary aspergillosis (ABPA) sans asthma: a distinct subset of ABPA with a lesser risk of exacerbation. Med Mycol. 2020;58(2):260–263. doi:10.1093/mmy/myz051
11. Moss RB. Severe fungal asthma: a role for biologics and inhaled antifungals. J Fungi. 2023;9(1):85. doi:10.3390/jof9010085
12. Rick EM, Woolnough K, Pashley CH, Wardlaw AJ. Allergic fungal airway disease. J Investig Allergol Clin Immunol. 2016;26(6):344–354. doi:10.18176/jiaci.0122
13. Woolnough K, Fairs A, Pashley CH, Wardlaw AJ. Allergic fungal airway disease: pathophysiologic and diagnostic considerations. Curr Opin Pulm Med. 2015;21(1):39–47. doi:10.1097/mcp.0000000000000129
14. Agarwal R, Muthu V, Sehgal IS, et al. Prevalence of aspergillus sensitization and allergic bronchopulmonary aspergillosis in adults with bronchial asthma: a systematic review of global data. J Allergy Clin Immunol Pract. 2023;11(6):1734–1751e3. doi:10.1016/j.jaip.2023.04.009
15. Agarwal R, Muthu V, Sehgal IS, et al. Prevalence of aspergillus sensitization and allergic bronchopulmonary Aspergillosis in bronchial asthma: a systematic review of Indian studies. Lung India. 2023;40(6):527–536. doi:10.4103/lungindia.lungindia_69_23
16. Agarwal R, Muthu V, Sehgal IS, et al. Aspergillus sensitization and allergic bronchopulmonary aspergillosis in asthmatic children: a systematic review and meta-analysis. Diagnostics. 2023;13(5):922. doi:10.3390/diagnostics13050922
17. Celik E, Kocacik Uygun D, Kaya MA, Gungoren MS, Keven A, Bingol A. Aspergillus-sensitized asthma in children. Pediatr Allergy Immunol. 2024;35(8):e14212. doi:10.1111/pai.14212
18. Agarwal R, Muthu V, Sehgal IS. Allergic bronchopulmonary aspergillosis. In: Jackson DJ, McDonald VM, Pavord ID, editors. Asthma (ERS Monograph). European Respiratory Society; 2025:352–372.
19. Soundappan K, Muthu V, Dhooria S, et al. Population prevalence of allergic bronchopulmonary aspergillosis in asthma: an epidemiological study of 43,261 participants from North India. Clin Exp Allergy. 2023;53(7):777–780. doi:10.1111/cea.14299
20. Sehgal IS, Saxena P, Dhooria S, et al. Is the prevalence of allergic bronchopulmonary aspergillosis greater in severe asthma? J Allergy Clin Immunol Pract. 2024;12(12):3269–3273e1. doi:10.1016/j.jaip.2024.09.002
21. Del Giacco SR, Bakirtas A, Bel E, et al. Allergy in severe asthma. Allergy. 2017;72(2):207–220. doi:10.1111/all.13072
22. van Helden MJ, Lambrecht BN. Dendritic cells in asthma. Curr Opin Immunol. 2013;25(6):745–754. doi:10.1016/j.coi.2013.10.002
23. Januskevicius A, Vasyle E, Rimkunas A, Malakauskas K. Integrative cross-talk in asthma: unraveling the complex interactions between eosinophils, immune, and structural cells in the airway microenvironment. Diagnostics. 2024;14(21). doi:10.3390/diagnostics14212448
24. Varricchi G, Bagnasco D, Borriello F, Heffler E, Canonica GW. Interleukin-5 pathway inhibition in the treatment of eosinophilic respiratory disorders: evidence and unmet needs. Curr Opin Allergy Clin Immunol. 2016;16(2):186–200. doi:10.1097/aci.0000000000000251
25. Akar-Ghibril N, Casale T, Custovic A, Phipatanakul W. Allergic endotypes and phenotypes of asthma. J Allergy Clin Immunol Pract. 2020;8(2):429–440. doi:10.1016/j.jaip.2019.11.008
26. Ogulur I, Mitamura Y, Yazici D, et al. Type 2 immunity in allergic diseases. Cell Mol Immunol. 2025;22(3):211–242. doi:10.1038/s41423-025-01261-2
27. Denning DW, Pfavayi LT. Poorly controlled asthma - Easy wins and future prospects for addressing fungal allergy. Allergol Int. 2023;72(4):493–506. doi:10.1016/j.alit.2023.07.003
28. Tiwary M, LeMessurier KS, Samarasinghe AE. Murine models of eosinophil function in fungal and viral infections. Methods Mol Biol. 2021;2241:99–112. doi:10.1007/978-1-0716-1095-4_9
29. Aimanianda V, Bayry J, Bozza S, et al. Surface hydrophobin prevents immune recognition of airborne fungal spores. Research Support, Non-U.S. Gov’t. Nature. 2009;460(7259):1117–1121. doi:10.1038/nature08264
30. Tiwary M, Samarasinghe AE. Initiation and pathogenesis of severe asthma with fungal sensitization. Cells. 2021;10(4):913. doi:10.3390/cells10040913
31. Tomee JF, Kauffman HF. Putative virulence factors of Aspergillus fumigatus. Clin Exp Allergy. 2000;30(4):476–484. doi:10.1046/j.1365-2222.2000.00796.x
32. Stolarski B, Kurowska-Stolarska M, Kewin P, Xu D, Liew FY. IL-33 exacerbates eosinophil-mediated airway inflammation. J Immunol. 2010;185(6):3472–3480. doi:10.4049/jimmunol.1000730
33. Patin EC, Thompson A, Orr SJ. Pattern recognition receptors in fungal immunity. Semin Cell Dev Biol. 2019;89:24–33. doi:10.1016/j.semcdb.2018.03.003
34. Knutsen AP. Immunopathology and immunogenetics of allergic bronchopulmonary aspergillosis. J Allergy. 2011;2011:785983. doi:10.1155/2011/785983
35. Stappers MHT, Clark AE, Aimanianda V, et al. Recognition of DHN-melanin by a C-type lectin receptor is required for immunity to aspergillus. Nature. 2018;555(7696):382–386. doi:10.1038/nature25974
36. Ueki S, Hebisawa A, Kitani M, Asano K, Neves JS. Allergic bronchopulmonary aspergillosis-a luminal hypereosinophilic disease with extracellular trap cell death. Front Immunol. 2018;9:2346. doi:10.3389/fimmu.2018.02346
37. Omokawa A, Ueki S, Kikuchi Y, et al. Mucus plugging in allergic bronchopulmonary aspergillosis: implication of the eosinophil DNA traps. Allergol Int. 2018;67(2):280–282. doi:10.1016/j.alit.2017.08.002
38. Muniz VS, Silva JC, Braga YAV, et al. Eosinophils release extracellular DNA traps in response to Aspergillus fumigatus. J Allergy Clin Immunol. 2018;141(2):571–585e7. doi:10.1016/j.jaci.2017.07.048
39. Liegeois MA, Hsieh A, Al-Fouadi M, et al. Cellular and molecular features of asthma mucus plugs provide clues about their formation and persistence. J Clin Invest. 2025;135(6). doi:10.1172/jci186889
40. Wardlaw AJ, Rick EM, Pur Ozyigit L, Scadding A, Gaillard EA, Pashley CH. New perspectives in the diagnosis and management of allergic fungal airway disease. J Asthma Allergy. 2021;14:557–573.
41. Bouzigon E, Forabosco P, Koppelman GH, et al. Meta-analysis of 20 genome-wide linkage studies evidenced new regions linked to asthma and atopy. Eur J Hum Genet. 2010;18(6):700–706. doi:10.1038/ejhg.2009.224
42. Demenais F, Margaritte-Jeannin P, Barnes KC, et al. Multiancestry association study identifies new asthma risk loci that colocalize with immune-cell enhancer marks. Nat Genet. 2018;50(1):42–53. doi:10.1038/s41588-017-0014-7
43. Ntontsi P, Photiades A, Zervas E, Xanthou G, Samitas K. Genetics and epigenetics in asthma. Int J Mol Sci. 2021;22(5). doi:10.3390/ijms22052412
44. Tsuo K, Zhou W, Wang Y, et al. Multi-ancestry meta-analysis of asthma identifies novel associations and highlights the value of increased power and diversity. Cell Genom. 2022;2(12):100212. doi:10.1016/j.xgen.2022.100212
45. Ferreira MAR, Mathur R, Vonk JM, et al. Genetic architectures of childhood- and adult-onset asthma are partly distinct. Am J Hum Genet. 2019;104(4):665–684. doi:10.1016/j.ajhg.2019.02.022
46. Vicente CT, Revez JA, Ferreira MAR. Lessons from ten years of genome-wide association studies of asthma. Clin Transl Immunol. 2017;6(12):e165. doi:10.1038/cti.2017.54
47. Bønnelykke K, Ober C. Leveraging gene-environment interactions and endotypes for asthma gene discovery. J Allergy Clin Immunol. 2016;137(3):667–679. doi:10.1016/j.jaci.2016.01.006
48. Kanaujia R, Arora A, Chakrabarti A, Rudramurthy SM, Agarwal R. Occurrence of cystic fibrosis transmembrane conductance regulator gene mutations in patients with allergic bronchopulmonary aspergillosis complicating asthma. Mycopathologia. 2022;187(2–3):147–155. doi:10.1007/s11046-022-00631-y
49. Kanaujia R, Arora A, Chakrabarti A, Rudramurthy SM, Agarwal R. Polymorphisms in innate and adaptive immune genes in subjects with allergic bronchopulmonary aspergillosis complicating asthma. Mycopathologia. 2024;189(2):23. doi:10.1007/s11046-024-00834-5
50. Overton NL, Denning DW, Bowyer P, Simpson A. Genetic susceptibility to allergic bronchopulmonary aspergillosis in asthma: a genetic association study. Allergy Asthma Clin Immunol. 2016;12:47. doi:10.1186/s13223-016-0152-y
51. Overton NL, Simpson A, Bowyer P, Denning DW. Genetic susceptibility to severe asthma with fungal sensitization. Int J Immunogene. 2017;44(3):93–106. doi:10.1111/iji.12312
52. Overton NLD, Brakhage AA, Thywissen A, Denning DW, Bowyer P. Mutations in EEA1 are associated with allergic bronchopulmonary aspergillosis and affect phagocytosis of Aspergillus fumigatus by human macrophages. PLoS One. 2018;13(3):e0185706. doi:10.1371/journal.pone.0185706
53. Agarwal R, Khan A, Aggarwal AN, Gupta D. Link between CFTR mutations and ABPA: a systematic review and meta-analysis. Mycoses. 2012;55(4):357–365. doi:10.1111/j.1439-0507.2011.02130.x
54. Gago S, Overton NLD, Ben-Ghazzi N, et al. Lung colonization by Aspergillus fumigatus is controlled by ZNF77. Nat Commun. 2018;9(1):3835. doi:10.1038/s41467-018-06148-7
55. Saxena S, Madan T, Shah A, Muralidhar K, Sarma PU. Association of polymorphisms in the collagen region of SP-A2 with increased levels of total IgE antibodies and eosinophilia in patients with allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol. 2003;111(5):1001–1007.
56. Knutsen AP, Kariuki B, Consolino JD, Warrier MR. IL-4 alpha chain receptor (IL-4Ralpha) polymorphisms in allergic bronchopulmonary aspergillosis. Clin Mol Allergy. 2006;4:3. doi:10.1186/1476-7961-4-3
57. Chauhan B, Hutcheson PS, Slavin RG, Bellone CJ. MHC restriction in allergic bronchopulmonary aspergillosis. Front Biosci. 2003;8:s140–8.
58. Godet C, Couturaud F, Marchand-Adam S, et al. Nebulised liposomal amphotericin-B as maintenance therapy in allergic bronchopulmonary aspergillosis: a randomised, multicentre trial. Eur Respir J. 2022;59(6):2102218. doi:10.1183/13993003.02218-2021
59. Oguma T, Taniguchi M, Shimoda T, et al. Allergic bronchopulmonary aspergillosis in Japan: a nationwide survey. Allergol Int. 2018;67(1):79–84. doi:10.1016/j.alit.2017.04.011
60. Agarwal R, Sehgal IS, Muthu V, Dhar R, Armstrong-James D. Allergic bronchopulmonary aspergillosis in India. Clin Exp Allergy. 2023;53(7):751–764. doi:10.1111/cea.14319
61. Hekking PW, Wener RR, Amelink M, Zwinderman AH, Bouvy ML, Bel EH. The prevalence of severe refractory asthma. J Allergy Clin Immunol. 2015;135(4):896–902. doi:10.1016/j.jaci.2014.08.042
62. Wardlaw AJ. Allergic fungal airway disease is a distinct endotype of difficult-to-treat asthma. J Allergy Clin Immunol Pract. 2021;9(12):4268–4269. doi:10.1016/j.jaip.2021.10.007
63. Mistry H, Ajsivinac soberanis HM, Kyyaly MA, et al. The clinical implications of Aspergillus fumigatus sensitization in difficult-to-treat asthma patients. J Allergy Clin Immunol Pract. 2021;9(12):4254–4267.e10. doi:10.1016/j.jaip.2021.08.038
64. Agarwal R, Gupta D, Aggarwal AN, Saxena AK, Chakrabarti A, Jindal SK. Clinical significance of hyperattenuating mucoid impaction in allergic bronchopulmonary aspergillosis: an analysis of 155 patients. Chest. 2007;132(4):1183–1190. doi:10.1378/chest.07-0808
65. Chakrabarti A, Sethi S, Raman DS, Behera D. Eight-year study of allergic bronchopulmonary aspergillosis in an Indian teaching hospital. Mycoses. 2002;45(8):295–299.
66. Aviles-Solis JC, Jácome C, Davidsen A, et al. Prevalence and clinical associations of wheezes and crackles in the general population: the Tromsø study. BMC Pulm Med. 2019;19(1):173. doi:10.1186/s12890-019-0928-1
67. Agarwal R, Sehgal IS, Dhooria S, et al. Allergic bronchopulmonary aspergillosis. Indian J Med Res. 2020;151(6):529–549. doi:10.4103/ijmr.IJMR_1187_19
68. Agarwal R, Khan A, Garg M, Aggarwal AN, Gupta D. Chest radiographic and computed tomographic manifestations in allergic bronchopulmonary aspergillosis. World J Radiol. 2012;4(4):141–150. doi:10.4329/wjr.v4.i4.141
69. Phuyal S, Garg MK, Agarwal R, et al. High-attenuation mucus impaction in patients with allergic bronchopulmonary aspergillosis: objective criteria on high-resolution computed tomography and correlation with serologic parameters. Curr Probl Diagn Radiol. 2016;45(3):168–173. doi:10.1067/j.cpradiol.2015.07.006
70. Godet C, Brun AL, Couturaud F, et al. CT imaging assessment of response to treatment in allergic bronchopulmonary aspergillosis in adults with bronchial asthma. Chest. 2024;165(6):1307–1318. doi:10.1016/j.chest.2024.02.026
71. Sehgal IS, Choudhary H, Dhooria S, et al. Is there an overlap in immune response between allergic bronchopulmonary and chronic pulmonary aspergillosis? J Allergy Clin Immunol Pract. 2019;7(3):969–974. doi:10.1016/j.jaip.2018.08.034
72. Lowes D, Chishimba L, Greaves M, Denning DW. Development of chronic pulmonary aspergillosis in adult asthmatics with ABPA. Respir Med. 2015;109(12):1509–1515. doi:10.1016/j.rmed.2015.09.007
73. Dournes G, Berger P, Refait J, et al. Allergic bronchopulmonary aspergillosis in cystic fibrosis: MR imaging of airway mucus contrasts as a tool for diagnosis. Radiology. 2017;285(1):261–269. doi:10.1148/radiol.2017162350
74. Ciet P, Bertolo S, Ros M, et al. State-of-the-art review of lung imaging in cystic fibrosis with recommendations for pulmonologists and radiologists from the “iMAging managEment of cySTic fibROsis” (MAESTRO) consortium. Eur Respir Rev. 2022;31(163). doi:10.1183/16000617.0173-2021
75. Sodhi KS, Gupta P, Shrivastav A, et al. Evaluation of 3 T lung magnetic resonance imaging in children with allergic bronchopulmonary aspergillosis: pilot study. Eur J Radiol. 2019;111:88–92. doi:10.1016/j.ejrad.2018.12.021
76. Coman I, Pola-Bibián B, Barranco P, et al. Bronchiectasis in severe asthma: clinical features and outcomes. Ann Allergy Asthma Immunol. 2018;120(4):409–413. doi:10.1016/j.anai.2018.02.016
77. Crimi C, Ferri S, Campisi R, Crimi N. The link between asthma and bronchiectasis: state of the art. Respiration. 2020;99(6):463–476. doi:10.1159/000507228
78. García-Clemente M, Enríquez-Rodríguez AI, Iscar-Urrutia M, et al. Severe asthma and bronchiectasis. J Asthma. 2020;57(5):505–509. doi:10.1080/02770903.2019.1579832
79. Chalmers JD, Haworth CS, Flume P, et al. European Respiratory Society clinical practice guideline for the management of adult bronchiectasis. Eur Respir J. 2025;66(6):2501126. doi:10.1183/13993003.01126-2025
80. Agarwal R, Maskey D, Aggarwal AN, et al. Diagnostic performance of various tests and criteria employed in allergic bronchopulmonary aspergillosis: a latent class analysis. PLoS One. 2013;8(4):e61105. doi:10.1371/journal.pone.0061105
81. Saxena P, Choudhary H, Muthu V, et al. Which are the optimal criteria for the diagnosis of allergic bronchopulmonary aspergillosis? A latent class analysis. J Allergy Clin Immunol Pract. 2021;9(1):328–335e1. doi:10.1016/j.jaip.2020.08.043
82. Agarwal R, Saxena P, Muthu V, et al. Optimal ImmunoCAP Aspergillus fumigatus-specific IgE threshold for detecting allergic bronchopulmonary aspergillosis in adults with asthma: a diagnostic accuracy study. Clin Exp Allergy. 2026;56(1): 61–67. doi:10.1111/cea.70148
83. Agarwal R, Sehgal IS, Saxena P, et al. A decision tree analysis to evaluate the optimal approach to screen allergic bronchopulmonary aspergillosis in asthmatic patients. J Asthma. 2025;62(5):761–766. doi:10.1080/02770903.2024.2439994
84. Agarwal R, Saxena P, Muthu V, et al. Evaluation of simpler criteria for diagnosing allergic bronchopulmonary aspergillosis complicating asthma. Front Cell Infect Microbiol. 2022;12:861866. doi:10.3389/fcimb.2022.861866
85. Agarwal R, Sehgal IS, Muthu V, et al. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses. Eur Respir J. 2024;63(4):2400061. doi:10.1183/13993003.00061-2024
86. Agarwal R, Chakrabarti A, Shah A, et al. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. Clin Exp Allergy. 2013;43(8):850–873. doi:10.1111/cea.12141
87. Asano K, Hebisawa A, Ishiguro T, et al. New clinical diagnostic criteria for allergic bronchopulmonary aspergillosis/mycosis and its validation. J Allergy Clin Immunol. 2021;147(4):1261–1268e5. doi:10.1016/j.jaci.2020.08.029
88. Rosenberg M, Patterson R, Mintzer R, Cooper BJ, Roberts M, Harris KE. Clinical and immunologic criteria for the diagnosis of allergic bronchopulmonary aspergillosis. Ann Intern Med. 1977;86(4):405–414. doi:10.7326/0003-4819-86-4-405
89. Agarwal R, Sehgal IS, Muthu V, et al. Comparative diagnostic performance of mx4-IgE versus species-specific IgE for identifying allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol Pract. 2025;13(9):2509–2511e1. doi:10.1016/j.jaip.2025.05.038
90. Asano K, Ueki S, Tamari M, Imoto Y, Fujieda S, Taniguchi M. Adult-onset eosinophilic airway diseases. Allergy. 2020;75(12):3087–3099. doi:10.1111/all.14620
91. Hunter ES, Page ID, Richardson MD, Denning DW. Evaluation of the LDBio Aspergillus ICT lateral flow assay for serodiagnosis of allergic bronchopulmonary aspergillosis. PLoS One. 2020;15(9):e0238855. doi:10.1371/journal.pone.0238855
92. Piarroux RP, Romain T, Martin A, et al. Multicenter Evaluation of a Novel Immunochromatographic Test for Anti-aspergillus IgG Detection. Front Cell Infect Microbiol. 2019;9:12. doi:10.3389/fcimb.2019.00012
93. Sehgal IS, Dhooria S, Prasad KT, Muthu V, Aggarwal AN, Agarwal R. Comparative diagnostic accuracy of immunoprecipitation versus immunoassay methods for detecting Aspergillus fumigatus-specific IgG in allergic bronchopulmonary aspergillosis: a systematic review and meta-analysis. Mycoses. 2022;65(9):866–876. doi:10.1111/myc.13488
94. Sehgal IS, Muthu V, Dhooria S, et al. Sensitivity and specificity of LDBio Aspergillus ICT lateral flow assay for diagnosing allergic bronchopulmonary aspergillosis in adult asthmatics. Mycoses. 2024;67(2):e13700. doi:10.1111/myc.13700
95. Matsuse H, Tsuchida T, Fukahori S, et al. Dissociation between sensitizing and colonizing fungi in patients with allergic bronchopulmonary aspergillosis. Ann Allergy Asthma Immunol. 2013;111(3):190–193. doi:10.1016/j.anai.2013.06.022
96. Oguma T, Ishiguro T, Kamei K, et al. Clinical characteristics of allergic bronchopulmonary mycosis caused by Schizophyllum commune. Clin Transl Allergy. 2024;14(1):e12327. doi:10.1002/clt2.12327
97. Takahashi H, Hamakawa M, Ishida T, Watanabe A. Allergic bronchopulmonary mycosis in Schizophyllum commune with positive Aspergillus-specific IgE antibodies: a case report. Respirol Case Rep. 2024;12(7):e01433. doi:10.1002/rcr2.1433
98. Sehgal IS, Choudhary H, Dhooria S, et al. Prevalence of sensitization to Aspergillus flavus in patients with allergic bronchopulmonary aspergillosis. Med Mycol. 2019;57(3):270–276. doi:10.1093/mmy/myy012
99. Muthu V, Singh P, Choudhary H, et al. Diagnostic cutoffs and clinical utility of recombinant Aspergillus fumigatus antigens in the diagnosis of allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol Pract. 2020;8(2):579–587. doi:10.1016/j.jaip.2019.08.041
100. Muthu V, Sehgal IS, Dhooria S, Aggarwal AN, Agarwal R. Utility of recombinant Aspergillus fumigatus antigens in the diagnosis of allergic bronchopulmonary aspergillosis: a systematic review and diagnostic test accuracy meta-analysis. Clin Exp Allergy. 2018;48(9):1107–1136. doi:10.1111/cea.13216
101. Muthu V, Singh P, Choudhary H, et al. Role of recombinant Aspergillus fumigatus antigens in diagnosing Aspergillus sensitisation among asthmatics. Mycoses. 2020;63(9):928–936. doi:10.1111/myc.13124
102. Gernez Y, Walters J, Mirkovic B, et al. Blood basophil activation is a reliable biomarker of allergic bronchopulmonary aspergillosis in cystic fibrosis. Eur Respir J. 2016;47(1):177–185. doi:10.1183/13993003.01068-2015
103. Gernez Y, Waters J, Tirouvanziam R, Herzenberg L, Moss R. Basophil activation test determination of CD63 combined with CD203c is not superior to CD203c alone in identifying allergic bronchopulmonary aspergillosis in cystic fibrosis. J Allergy Clin Immunol. 2016;138(4):1195–1196. doi:10.1016/j.jaci.2016.04.002
104. Prasad KT, Muthu V, Sehgal IS, et al. The utility of the basophil activation test in differentiating asthmatic subjects with and without allergic bronchopulmonary aspergillosis. Mycoses. 2020;63(6):588–595. doi:10.1111/myc.13081
105. Michel M, Sereme Y, Mankouri F, et al. Basophil activation test with aspergillus molecules: the case for ABPA. Front Allergy. 2022;3:898731. doi:10.3389/falgy.2022.898731
106. Zhang LS, Wu YF, Lu HW, et al. Fractional exhaled nitric oxide, a potential biomarker for evaluating glucocorticoids treatment and prognosis in allergic bronchopulmonary aspergillosis. Ann Allergy Asthma Immunol. 2024;133(2):168–176.e1. doi:10.1016/j.anai.2024.05.010
107. Matsuda K, Oishi K, Suizu J, et al. Fractional exhaled nitric oxide as a biomarker for the evaluating asthmatic patients with allergic bronchopulmonary mycosis. Respir Investig. 2025;63(6):1369–1376. doi:10.1016/j.resinv.2025.11.002
108. Chen H, Zhang X, Zhu L, et al. Clinical and immunological characteristics of Aspergillus fumigatus-sensitized asthma and allergic bronchopulmonary aspergillosis. Front Immunol. 2022;13:939127. doi:10.3389/fimmu.2022.939127
109. Sehgal IS, Dhooria S, Muthu V, Prasad KT, Agarwal R. An overview of the available treatments for chronic cavitary pulmonary aspergillosis. Expert Rev Respir Med. 2020;14(7):715–727. doi:10.1080/17476348.2020.1750956
110. Agarwal R, Khan A, Aggarwal AN, Gupta D. Is the SMART approach better than other treatment approaches for prevention of asthma exacerbations? A meta-analysis. Meta-Analysis. Monaldi Arch Chest Dis. 2009;71(4):161–169.
111. Asano K, Suzuki Y, Tanaka J, Kobayashi K, Kamide Y. Treatments of refractory eosinophilic lung diseases with biologics. Allergol Int. 2023;72(1):31–40. doi:10.1016/j.alit.2022.10.004
112. Agarwal R, Aggarwal AN, Dhooria S, et al. A randomised trial of glucocorticoids in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur Respir J. 2016;47(2):490–498. doi:10.1183/13993003.01475-2015
113. Voskamp AL, Gillman A, Symons K, et al. Clinical efficacy and immunologic effects of omalizumab in allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol Pract. 2015;3(2):192–199. doi:10.1016/j.jaip.2014.12.008
114. Jin M, Douglass JA, Elborn JS, et al. Omalizumab in allergic bronchopulmonary aspergillosis: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2023;11(3):896–905. doi:10.1016/j.jaip.2022.12.012
115. Chen P, Yu Y, He L, et al. Efficacy of omalizumab in adult patients with allergic bronchopulmonary aspergillosis: a multicentre study in China. Clin Exp Med. 2024;24(1):6. doi:10.1007/s10238-023-01267-y
116. Chen X, Zhi H, Wang X, et al. Efficacy of biologics in patients with allergic bronchopulmonary aspergillosis: a systematic review and meta-analysis. Lung. 2024;202(4):367–383. doi:10.1007/s00408-024-00717-y
117. Tomomatsu K, Yasuba H, Ishiguro T, et al. Real-world efficacy of anti-IL-5 treatment in patients with allergic bronchopulmonary aspergillosis. Article. Sci Rep. 2023;13(1):5468. doi:10.1038/s41598-023-32246-8
118. Darragh K, Akuthota P. Corticosteroid-sparing effect of biologics in patients with allergic bronchopulmonary aspergillosis. Ann Allergy Asthma Immunol. 2024. doi:10.1016/j.anai.2024.01.010
119. Jacobs SE, Saez-Lacy D, Wynkoop W, Walsh TJ. Successful treatment of allergic bronchopulmonary aspergillosis with isavuconazole: case report and review of the literature. Open Forum Infect Dis. 2017;4(2):ofx040. doi:10.1093/ofid/ofx040
120. Yakut N, Kadayifci EK, Eralp EE, Gokdemir Y. Successful treatment of allergic bronchopulmonary aspergillosis with posaconazole in a child with cystic fibrosis: case report and review of the literature. Lung India. 2020;37(2):161–163. doi:10.4103/lungindia.lungindia_288_19
121. Denning DW, Van Wye JE, Lewiston NJ, Stevens DA. Adjunctive therapy of allergic bronchopulmonary aspergillosis with itraconazole. Chest. 1991;100(3):813–819.
122. Germaud P, Tuchais E. Allergic bronchopulmonary aspergillosis treated with itraconazole. Chest. 1995;107(3):883.
123. Antoniu SA. Itraconazole for severe asthma with fungal sensitivity. Expert Opin Pharmacother. 2009;10(7):1231–1233.
124. Pizzimenti S, Heffler E, Badiu I, Bussolino C, Raie A, Rolla G. Itraconazole as “bridge therapy” to anti-IgE in patients with severe asthma with fungal sensitization. Conference Abstract. Clin Transl Allergy. 2013;3.
125. Curran AK, McIntyre KT, Tracy HS, et al. Pulmonary delivery of PUR1900 enables high lung exposure of itraconazole relative to oral dosing. Pediatric Pulmonol. 2016;51:319. doi:10.1002/ppul.23576
126. Agarwal R, Dhooria S, Singh Sehgal I, et al. A randomized trial of itraconazole vs prednisolone in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Chest. 2018;153(3):656–664. doi:10.1016/j.chest.2018.01.005
127. Hava DL, Tan L, Johnson P, et al. A phase 1/1b study of PUR1900, an inhaled formulation of itraconazole, in healthy volunteers and asthmatics to study safety, tolerability and pharmacokinetics. Br J Clin Pharmacol. 2020;86(4):723–733. doi:10.1111/bcp.14166
128. Lin CY, Huang YC, Huang HY, et al. Effectiveness of low-dose itraconazole in fungal-associated severe asthma: a retrospective study. J Asthma Allergy. 2020;13:453–461. doi:10.2147/jaa.S276289
129. Agarwal R, Muthu V, Sehgal IS, et al. A randomised trial of prednisolone versus prednisolone and itraconazole in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur Respir J. 2022;59(4):2101787. doi:10.1183/13993003.01787-2021
130. Ram B, Aggarwal AN, Dhooria S, et al. A pilot randomized trial of nebulized amphotericin in patients with allergic bronchopulmonary aspergillosis. J Asthma. 2016;53(5):517–524. doi:10.3109/02770903.2015.1127935
131. Liu J, Vanderwyk KA, Donnelley MA, Thompson Iii GR. SUBA-itraconazole in the treatment of systemic fungal infections. Future Microbiol. 2024;19(13):1171–1175. doi:10.1080/17460913.2024.2362128
132. Abbotsford J, Foley DA, Goff Z, Bowen AC, Blyth CC, Yeoh DK. Clinical experience with SUBA-itraconazole at a tertiary paediatric hospital. J Antimicrob Chemother. 2021;76(1):249–252. doi:10.1093/jac/dkaa382
133. Jin H, Wang T, Falcione BA, et al. Trough concentration of voriconazole and its relationship with efficacy and safety: a systematic review and meta-analysis. J Antimicrob Chemother. 2016;71(7):1772–1785. doi:10.1093/jac/dkw045
134. Agarwal K, Bruggemann R, Chowdhary A, Meis JF, Gaur SN. Serum level directed itraconazole therapy in allergic bronchopulmonary aspergillosis. Eur Respir J. 2016;48. doi:10.1183/13993003.congress-2016.OA4956
135. Singh A, Sharma B, Mahto KK, Meis JF, Chowdhary A. High-frequency direct detection of triazole resistance in Aspergillus fumigatus from patients with chronic pulmonary fungal diseases in India. J Fungi. 2020;6(2). doi:10.3390/jof6020067
136. Moin S, Farooqi J, Jabeen K, Laiq S, Zafar A. Screening for triazole resistance in clinically significant Aspergillus species; report from Pakistan. Antimicrob Resist Infect Control. 2020;9(1):62. doi:10.1186/s13756-020-00731-8
137. Meis JF. Azole resistant Aspergillus fumigatus-global epidemiology of clinical and environmental resistance. Conference Abstract. Mycoses. 2016;59:5. doi:10.1111/myc.12463
138. Vermeulen E, Maertens J, De Bel A, et al. Nationwide surveillance of azole resistance in aspergillus diseases. Antimicrob Agents Chemother. 2015;59(8):4569–4576. doi:10.1128/aac.00233-15
139. Muthu V, Dhooria S, Sehgal IS, et al. Nebulized amphotericin B for preventing exacerbations in allergic bronchopulmonary aspergillosis: a systematic review and meta-analysis. Pulm Pharmacol Ther. 2023;81:102226. doi:10.1016/j.pupt.2023.102226
140. Garcia M, Le Moal G, Cadranel J, Roblot F, Godet C. Efficacy of nebulized liposomal amphotericin B in the treatment of ABPA in an HIV/HBV co-infected man: case report and literature review. J Asthma. 2019;56(1):84–86. doi:10.1080/02770903.2018.1429467
141. Fukushima C, Matsuse H, Obase Y, et al. Liposomal amphotericin B fosters the corticosteroids’ anti-inflammatory effect on murine allergic bronchopulmonary aspergillosis model airways. Inflammation. 2019;42(6):2065–2071. doi:10.1007/s10753-019-01069-z
142. Muthu V, Sehgal IS, Agarwal R. Aerosolized antifungals for the treatment of pulmonary fungal diseases. Curr Fungal Infect Rep. 2024;18(2):154–162. doi:10.1007/s12281-024-00495-3
143. Caponetti G, Sala F, Cervetti A, Colombo D, Tiberio E, Singh D. Phase I study of the safety, tolerability and pharmacokinetics of inhaled voriconazole in healthy volunteers and subjects with stable asthma Pharmacol Res Perspect. 2025;13(1):e70064. doi:10.1002/prp2.70064
144. AgarwaI R, Chaudhry D, Gupta SN, et al. A phase 2, dose-finding study of inhaled itracaonazole in ABPA-complicating asthma. Eur Respir J. 2025;PA4768(Suppl).
145. Nwankwo L, Lewis White P, Barry S, et al. Successful treatment of an allergic bronchopulmonary aspergillosis patient with inhaled antifungal opelconazole. J Allergy Clin Immunol Pract. 2025;13(8):2171–2173.e1. doi:10.1016/j.jaip.2025.05.018
146. Agarwal R, Dhooria S, Sehgal IS, et al. A randomised trial of voriconazole and prednisolone monotherapy in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur Respir J. 2018;52(3):1801159. doi:10.1183/13993003.01159-2018
147. Bradley JM, O’Neill B, McAuley DF, et al. Hypertonic saline or carbocisteine in bronchiectasis. N Engl J Med. 2025. doi:10.1056/NEJMoa2510095
148. Altenburg J, de Graaff CS, Stienstra Y, et al. Effect of azithromycin maintenance treatment on infectious exacerbations among patients with non-cystic fibrosis bronchiectasis: the BAT randomized controlled trial. JAMA. 2013;309(12):1251–1259. doi:10.1001/jama.2013.1937
149. Serisier DJ, Martin ML, McGuckin MA, et al. Effect of long-term, low-dose erythromycin on pulmonary exacerbations among patients with non-cystic fibrosis bronchiectasis: the BLESS randomized controlled trial. JAMA. 2013;309(12):1260–1267.
150. Clement A, Tamalet A, Leroux E, Ravilly S, Fauroux B, Jais JP. Long term effects of azithromycin in patients with cystic fibrosis: a double blind, placebo controlled trial. Thorax. 2006;61(10):895–902. doi:10.1136/thx.2005.057950
151. Chalmers JD, Burgel PR, Daley CL, et al. Phase 3 trial of the DPP-1 inhibitor brensocatib in bronchiectasis. N Engl J Med. 2025;392(16):1569–1581. doi:10.1056/NEJMoa2411664
152. Agarwal R, Sehgal IS, Muthu V, et al. Long-term follow-up of allergic bronchopulmonary aspergillosis treated with glucocorticoids: a study of 182 subjects. Mycoses. 2023;66(11):953–959. doi:10.1111/myc.13640
153. Watai K, Fukutomi Y, Hayashi H, et al. De novo sensitization to Aspergillus fumigatus in adult asthma over a 10-year observation period. Letter. Allergy. 2018;73(12):2385–2388. doi:10.1111/all.13566
154. Chesshyre E, Wooding E, Sey E, Warris A. Aspergillus in Children and Young People with Cystic Fibrosis: a Narrative Review. J Fungi. 2025;11(3). doi:10.3390/jof11030210
155. Singh Sehgal I, Agarwal R. Pulse methylprednisolone in allergic bronchopulmonary aspergillosis exacerbations. Letter. Eur Respir Rev. 2014;23(131):149–152. doi:10.1183/09059180.00004813
156. Cohen-Cymberknoh M, Blau H, Shoseyov D, et al. Intravenous monthly pulse methylprednisolone treatment for ABPA in patients with cystic fibrosis. Clinical Trial Research Support, Non-U.S. Gov’t. J Cyst Fibros. 2009;8(4):253–257. doi:10.1016/j.jcf.2009.04.008
157. Thomson JM, Wesley A, Byrnes CA, Nixon GM. Pulse intravenous methylprednisolone for resistant allergic bronchopulmonary aspergillosis in cystic fibrosis. Pediatr Pulmonol. 2006;41(2):164–170. doi:10.1002/ppul.20333
158. Aaron SD, Vandemheen KL, Freitag A, et al. Treatment of Aspergillus fumigatus in patients with cystic fibrosis: a randomized, placebo-controlled pilot study. PLoS One. 2012;7(4):e36077. doi:10.1371/journal.pone.0036077
159. Bentley S, Gupta A, Balfour-Lynn IM. Subtherapeutic itraconazole and voriconazole levels in children with cystic fibrosis. J Cyst Fibros. 2013;12(4):418–419. doi:10.1016/j.jcf.2012.09.007
160. Chesshyre ELD, Bradbury JD, Cook H, et al. The impact of the COVID-19 pandemic and the changing landscape of CF on the cASPerCF trial: a real-world experience. Trials. 2024;25(1):645. doi:10.1186/s13063-024-08510-1
161. Sehgal IS, Muthu V, Seidel D, et al. EQUAL ABPA Score 2024: a tool to measure guideline adherence for managing allergic bronchopulmonary aspergillosis. Mycoses. 2024;67(10):e13810. doi:10.1111/myc.13810
162. Wang T, Tan JB, Liu XL, Zhao I. Barriers and enablers to implementing clinical practice guidelines in primary care: an overview of systematic reviews. BMJ Open. 2023;13(1):e062158. doi:10.1136/bmjopen-2022-062158
163. Luo RG, Wu YF, Lu HW, et al. Th2-skewed peripheral T-helper cells drive B-cells in allergic bronchopulmonary aspergillosis. Eur Respir J. 2024;63(5). doi:10.1183/13993003.00386-2024
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.