Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Associations of Thyroid Function Tests with Lipid Levels and Adverse Pregnancy Outcomes During the First Trimester
Authors Liu WY, Zhu YT, Xu XM, Zhang JR, Gan XP, Cheng DC, Lu F, Lu C
Received 7 December 2021
Accepted for publication 4 March 2022
Published 31 March 2022 Volume 2022:15 Pages 973—981
DOI https://doi.org/10.2147/DMSO.S352073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Wen-Yu Liu,1,* Yu-Ting Zhu,2,* Xian-Ming Xu,1 Jia-Rong Zhang,3 Xu-Pei Gan,1 De-Cui Cheng,1 Feng Lu,4 Cong Lu1
1Department of Obstetrics and Gynecology, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 201600, People’s Republic of China; 2Department of Gynecology Maternal and Child Health Hospital of Jiading District, Shanghai, 201800, People’s Republic of China; 3Department of Obstetrics and Gynecology, Zhongshan Hospital, Fudan University, Shanghai, 200030, People’s Republic of China; 4Department of Obstetrics and Gynecology, Songjiang Maternal and Child Health-Care Hospital, Shanghai, 201600, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Cong Lu, Department of Obstetrics and Gynecology, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, No. 650 of Xinsongjiang Road, Songjiang District, Shanghai, 201600, People’s Republic of China, Tel +86-021-37798537, Email [email protected] Feng Lu, Department of Obstetrics and Gynecology, Songjiang Maternal and Child Health-Care Hospital, No. 1010 of Xilin North Road, Songjiang District, Shanghai, 201600, People’s Republic of China, Tel +86-18918282005, Email [email protected]
Objective: The present study aims to evaluate the relationship of thyroid function during the first trimester of pregnancy with lipid levels and pregnancy outcomes.
Methods: Women who delivered babies at the Shanghai General Hospital between March 2019 and December 2019 with a known pregnancy outcome and complete data were included in the present study (n = 1779). A retrospective cohort study of all subjects with available first-trimester thyroid function testing and lipid levels data was conducted, and the relationship of thyroid function with lipid levels and pregnancy outcomes was evaluated. The data were analyzed using the SPSS software for statistical correlation.
Results: The proportion of caesarean sections was higher in women with hypothyroxinemia (HIA) and hypothyroidism than in women with euthyroidism. Hypothyroidism was shown to be related with polyhydramnios, preterm labor and hypertriglyceridemia. HIA was correlated with increased rates of gestational diabetes mellitus (GDM), preeclampsia, gestational hypertension and hypertriglyceridemia. Compared with the euthyroidism group, the hypothyroidism group had a higher apolipoprotein A1 (Apo A1) level and apolipoprotein B level; the subclinical hypothyroidism group had a higher total cholesterol (TC) level and low-density lipoprotein cholesterol level; the HIA group had higher triglyceride, high-density lipoprotein cholesterol levels and lower TC, Apo A1 levels. TC levels were positively correlated with the thyroid-stimulating hormone level and negatively correlated with free thyroxine (FT4) level, and free triiodothyronine and FT4 levels were positively correlated with GDM occurrence.
Conclusion: Thyroid function in early pregnancy is associated with dyslipidemia and pregnancy outcomes; conventional screening of thyroid diseases in early pregnancy may help improve lipid levels and decrease adverse pregnancy outcomes.
Keywords: first trimester, thyroid function tests, adverse pregnancy outcome, dyslipidemia
Introduction
It is well recognized that thyroid function can influence lipid synthesis, mobilization, and degradation. Thyroid hormones are crucial for the regulation of lipids, which play an essential role in fetal development and health maintenance in pregnant women. Since the fetal thyroid gland does not functionally mature until 20 weeks of pregnancy, the fetal demand for thyroid hormones depends on maternal supply in the first half of the pregnancy.1 As a result, women with thyroid dysfunction have an increased risk of maternal-fetal complications, including stillbirths, preeclampsia (PE), and neonatal morbidity.2
Thyroid diseases, which include hypothyroxinemia (HIA), hypothyroidism, subclinical hypothyroidism (SCH), hyperthyroidism and subclinical hyperthyroidism, are endocrine diseases with the highest incidence except gestational diabetes mellitus (GDM) occurring during pregnancy,3 and they severely affect pregnancy outcomes. The pathogenesis of thyroid diseases during pregnancy is still unclear, especially in terms of lipid metabolism. Studies have shown correlation of SCH in adults with increased levels of total cholesterol (TC), low-density lipoprotein (LDL), non-high density lipoprotein, and triglyceride (TG) and decreased levels of high-density lipoprotein (HDL).4
However, reports on the correlation of thyroid gland dysfunction with dyslipidemia and pregnancy outcomes in pregnant women have shown controversial results. Furthermore, most studies focus on the late pregnancy period, with little mention of the first trimester. Due to controversies and limitations in literature, there is a need for a comprehensive cohort for the evaluation of lipid trends in euthyroidism and thyroid disorders.
The optimum management strategy for maternal thyroid dysfunction during pregnancy is still largely unexplored. Early diagnosis and appropriate treatment of thyroid diseases during pregnancy are essential in order to maintain the health of the mother and child. The purpose of the present study is to evaluate the relationship of thyroid dysfunction during the first trimester of pregnancy with lipid levels and pregnancy outcomes. An observational hospital-based cohort study in Shanghai, China was conducted to investigate the relationship of multiple types of maternal thyroid dysfunction in early pregnancy with lipid trends and unfavorable pregnancy outcomes. Pregnancy and fetal outcomes included GDM, caesarean section (CS), pregnancy-induced hypertension (PIH), PE, preterm birth (PTB), low birth weight (LBW), macrosomia, fetal distress, polyhydramnios, postpartum hemorrhage (PPH), hypertriglyceridemia.
Materials and Methods
The present retrospective cohort study was performed in the city of Shanghai, China. Pregnant women presenting for delivery in Shanghai General Hospital Affiliated with Shanghai JiaoTong University between March 2019 and December 2019 were recruited in the study. The study design was approved by the hospital’s ethics committee ([2021]036) and written informed consent was obtained from all subjects.
Inclusion criteria: women were in the early pregnancy period with a singleton pregnancy. Exclusion criteria: (1) women with multiple pregnancies; (2) women with congenital malformations of newborns; (3) women who underwent medical abortion or experienced intrauterine fetal death; (4) women with liver and kidney diseases, malignant tumors, diabetes mellitus, and hereditary hyperlipidemia. Pregnancy outcomes, blood lipids and thyroid hormone levels of pregnant women were downloaded from the hospital medical records and laboratory information system respectively. The gestational age was determined by the last menstrual period and confirmed via ultrasound in the first three months of pregnancy using the crown-rump length up to the 13th week. The trimesters were as follows: trimester 1 = before 12 weeks; trimester 2 = 13–27 weeks; and trimester 3 = 28 weeks to delivery.
The information regarding thyroid function tests (TFTs) was classified into six categories (hypothyroidism, SCH, HIA, euthyroidism, hyperthyroidism, and subclinical hyperthyroidism) according to the 2017 version of the American Thyroid Association (ATA)5 guideline. Category 6 included pregnant women with normal thyroid function and was used as the control group.
According to 2017 ATA, maternal hypothyroidism is defined as the presence of elevated thyroid-stimulating hormone (TSH) and decreased in serum free thyroxine (FT4) levels during gestation. Meanwhile, SCH is defined as elevated TSH with a normal FT4 concentration, and HIA is defined as normal TSH levels but decreased FT4 levels in women. Hyperthyroidism is defined as decreased TSH concentration with increased FT4 concentration, and subclinical hyperthyroidism is defined as decreased TSH concentration with normal FT4 concentration. Euthyroidism is defined as normal TSH and FT4 concentration.
The normal references of FT4 and TSH were set at 11.7–19.7 pmol/L and 0.03–3.52 mIU/mL in accordance with the 2017 ATA and the reference range criteria developed by the International Peace Maternity and Child Health Hospital.6 The free triiodothyronine (FT3):FT4 ratio was determined by dividing plasma concentrations of FT3 by FT4.
The serum TSH, FT3, FT4, thyroid peroxidase antibody (TPOAb), TG, TC, HDL, LDL, apolipoprotein A1 (Apo A1), apolipoprotein B (Apo B), and apolipoprotein E (Apo E) levels were measured. The obstetric outcomes assessed PTB (defined as birth at <37 weeks of gestation7), increased rate of CS, GDM (one or more plasma venous glucose values of ≥5.1 mmol/L at 0 h, ≥10.0 mmol/L at 1 h, or ≥8.5 mmol/L at 2 h after a 2-h, 75-g oral glucose tolerance test8), PPH (PPH volume of >500 mL for natural birth or >1000 mL for CS), polyhydramnios (amniotic fluid index ≥ 25cm), hypertriglyceridemia (TG > 1.87mmol/l), PIH (defined as systolic blood pressure >140 mmHg and diastolic blood pressure >90 mmHg9) and PE (PIH+ significant proteinuria).
The assessed perinatal outcomes included LBW (neonatal birth weight of <2.5 kg), macrosomia (birth weight ≥4000 g), and fetal distress. No data were provided on whether participants had received drugs to treat thyroid dysfunction during pregnancy. The effect of thyroid hormone levels caused by the drugs cannot be ruled out; this may lead to the bias.
Statistical Analysis
The SPSS 26 (SPSS Inc, Chicago, IL, USA) program was used for statistical analysis. In addition to descriptive statistical analysis (percentage, average and standard deviation), the inter-group comparisons were made according to data distribution. The Chi-square test or Fisher’s exact test (sample size of <5) was used for the categorical data. Logistic regression was used to model binary outcomes. Coefficients were exponentiated into odds ratios and 95% confidence intervals were calculated. Models included maternal age, gravidity (defined as the number of times that a woman has been pregnant.), and parity (defined as the number of times that she has given birth to a fetus with a gestational age of 28 weeks or more) as covariates were constructed. The Student’s t-test, ANOVA testing and multiple linear regression models were used to study the association of the thyroid hormone level with lipid levels and adverse pregnancy outcomes. A p value of <0.05 was considered statistically significant.
Results
A total of 1650 women were included in the final analysis; of these, 784 (47.5%) had normal TFT results and 866 (52.5%) had abnormal results with hypothyroidism, SCH, HIA, hyperthyroidism, and subclinical hyperthyroidism occurring in 5.6%, 2.6%, 43.4%, 0.5%, and 0.4% of subjects, respectively. The patient age range was 17–47 years (mean ± SD = 30.2 ± 4.2).
The patients were divided into different thyroid abnormalities. Table 1 shows the general characteristics of the patients involved in the study and the distribution of thyroid dysfunction during pregnancy. Maternal thyroid hormone disorder data and adverse pregnancy outcomes are shown in Table 2.
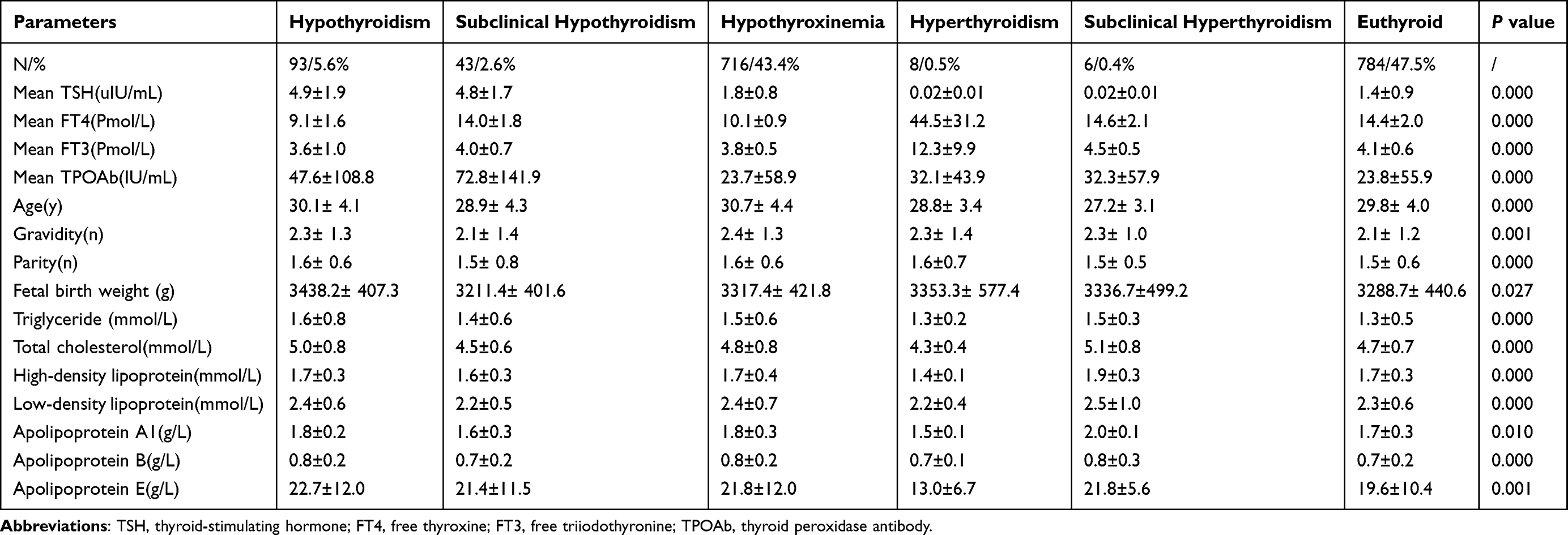 |
Table 1 Descriptive Statistics [Mean ± SD or N (%)] of Maternal Characteristics, Thyroid and Lipid Levels in the Study Population (N = 1650) |
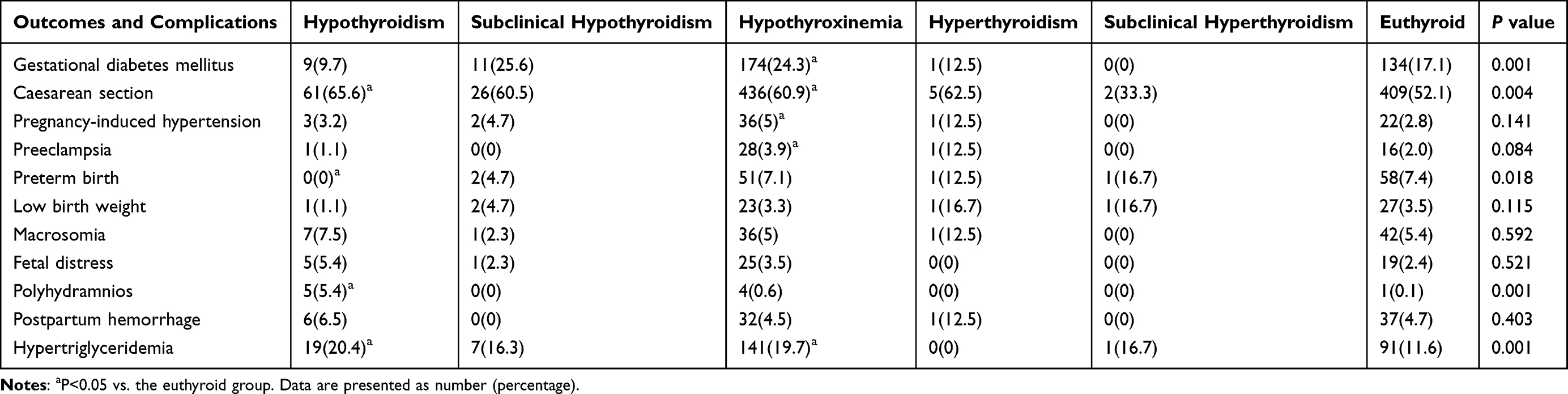 |
Table 2 The Chi-Square Test or Fisher’s Exact Test for Adverse Pregnancy Outcomes According to Thyroid Function in the First Trimester |
Compared with the normal subgroup, there were significant differences in some results and complications in the thyroid disease subgroup. A total of 720 (43.4%) patients delivered through natural labor, and 968 patients delivered by CS (56.6%). The proportion of CS was present in 60.9% and 65.6% subjects and was significantly higher in the HIA group and hypothyroidism group compared with the normal group.
Subjects who met the criteria for hypothyroidism showed a correlation with adverse pregnancy outcomes, such as polyhydramnios and hypertriglyceridemia. And HIA is correlated with an increased rate of GDM, PIH, PE and hypertriglyceridemia. No significant differences were identified in PPH, LBW, macrosomia and fetal distress among the six groups. SCH, subclinical hyperthyroidism and hyperthyroidism had no adverse effects on our pregnancy outcomes. Maternal thyroid hormone dysfunction and lipid levels in adjusted logistic regression models are shown in Table 3.
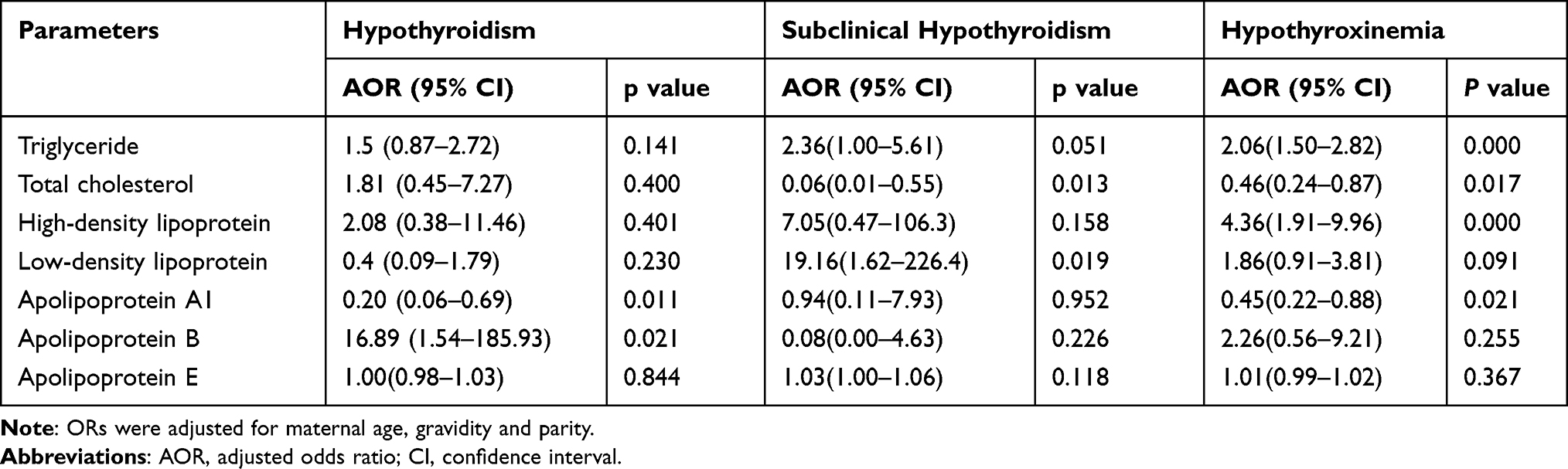 |
Table 3 Odds Ratios Calculated from Logistic Regression Analysis for Thyroid Hormone Dysfunction and Lipid Levels |
There were significant differences in age, gravidity, and parity among the six groups (Table 1). When adjusted for age, gravidity, and parity and compared to the euthyroidism group, the hypothyroidism group had higher Apo A1 and Apo B levels; the SCH group had higher TC and LDL levels; the HIA group had higher TC, TG, HDL, and Apo A1 levels.
Since the cases with hyperthyroidism and subclinical hyperthyroidism were limited in number, the authors of the present study were unable to comment on the relationship between them and dyslipidemia. In addition, the relationship of TSH, FT4, FT3, FT3/FT4, and TPOAb levels with lipid levels and adverse pregnancy outcomes in multivariable regression analyses are presented in Table 4. The associations of FT4 with maternal age and FT3 with gravidity and parity were statistically significant.
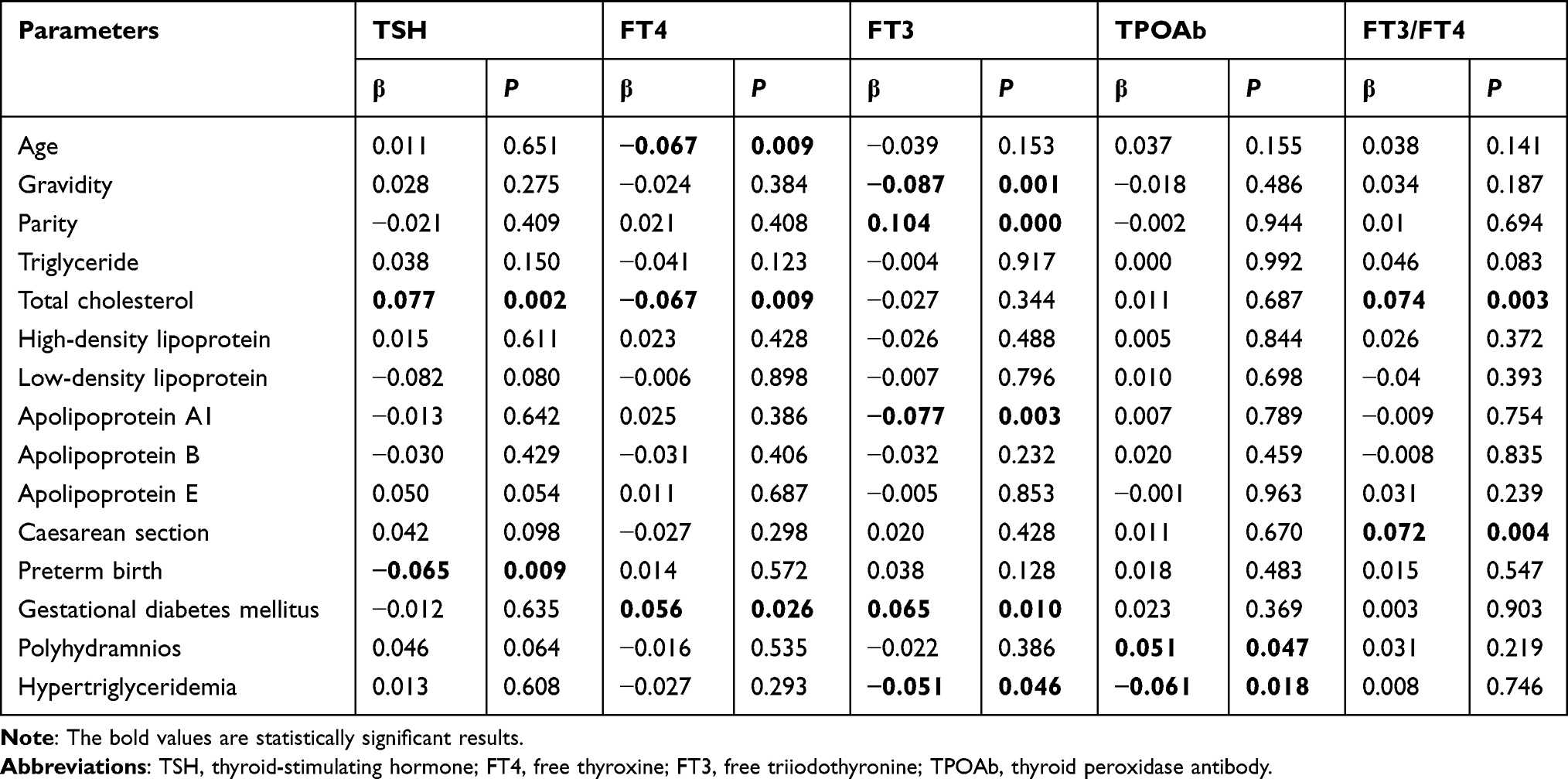 |
Table 4 Characteristics of the Study Participants Divided by First-Trimester TSH, FT4, FT3, TPOAb, FT3/FT4 Ratio Concentration |
In the multiple regression analysis, TC was positively correlated with TSH and negatively correlated with FT4. Higher FT3/FT4 ratios (suggesting higher peripheral deiodinase activity leading to conversion of FT4 to FT3) resulted in a higher TC level and CS rate. The FT3 and FT4 levels were positively correlated with GDM, and there was no apparent association between FT3, FT4, and TSH levels and TG, LDL, HDL, Apo B, and Apo E level abnormalities. There were negative correlations between hypertriglyceridemia and FT3 and TPOAb; however, there were no significant associations between TPOAb and lipid levels.
Discussion
It is well known that excessive or deficient thyroid hormone levels in pregnant women can have serious impact on the fetal and maternal outcomes at all stages of pregnancy. However, the association between the thyroid gland and lipids is not well understood.
The present study shows that hypothyroidism and HIA in pregnant women may result in an increased CS rate; this may be caused by associated pregnancy complications, such as polyhydramnios and PE. Whether otherwise uncomplicated hypothyroidism increases the risk of CS warrants further study.
The present study also found that HIA is positively associated with PIH; however, no association was found between PIH and other thyroid dysfunctions. This is consistent with relevant literature. According to relevant literature, PIH is associated with hypothyroidism in the third trimester of pregnancy, not in the first trimester.10 Therefore, it can be concluded that pregnancy outcomes depends not only on the thyroid status of the pregnant woman but also on the gestational age at which maternal thyroid dysfunction occurs. Specifically, the relationship between the risk of PTB and maternal thyroid function has been contradictory; some studies have shown a positive correlation,11 while most studies have not shown an increased risk of PTB.12,13
No association was found between SCH and an increased risk of PTB in the present study; this is consistent with relevant literature.14 However, there was a significant negative association between PTB and hypothyroidism and between TSH and PTB. According to relevant literature, there is an increased risk of PTB in women with hypothyroidism.15 These differences may be related to the relatively small sample size in this study.
Although the prospective associations between different thyroid markers and GDM have been widely studied, the conclusions are different, and the mechanisms are still unclear. The null association of TSH with GDM in the present study is consistent with previous findings.16
Lower serum FT4 concentration or higher FT3/FT4 ratio in early pregnancy was associated with an increased risk of GDM;17 however, the results of this study showed that FT3 and FT4 levels were positively correlated with GDM. Although there is limited evidence for a prospective association between the FT3/FT4 ratio and GDM, the cross-sectional studies conducted by the authors of the present study indicated that a higher FT3/FT4 ratio was correlated with TC and the CS rate.
There is a considerable gap in the understanding of the association between thyroid hormones and GDM and their underlying mechanisms in early pregnancy. An inverse association was found between maternal FT4 in early pregnancy and birth weight.18 Furthermore, the present study showed that women with hyperthyroidism and subclinical hyperthyroidism have a higher rate of LBW, which was statistically significant and consistent with related literature.
Whether pregnant women with TPOAb positivity have a higher risk of poor pregnancy outcomes is debatable. The results of the logistic regression analysis in the present study showed that TPOAb positivity was (1) associated with an increased risk of polyhydramnios and (2) significantly negatively associated with birth weight (β = −0.084, p = 0.001, data not shown).
Furthermore, there were negative correlations between hypertriglyceridemia and TPOAb but no significant associations between TPOAb and lipid levels. The TC, TG, Apo B, and Apo E levels were higher in the HIA group and the SCH group had a higher TC and LDL level than in the euthyroidism group, it can be roughly concluded that mild thyroid gland dysfunction during the first trimester of pregnancy is associated with dyslipidemia. The results of this research showed that TC is positively correlated with TSH and negatively correlated with FT4, and FT3 is negatively correlated with Apo A and hypertriglyceridemia. The mechanism behind the effect of thyroid function on lipid profiles is not completely understood and requires further research.
Thyroid hormones can reduce Apo B lipoproteins via a non-LDL receptor pathway, leading to decreased liver Apo B production.19 Therefore, a close surveillance in terms of lipid profiles could be considered in subjects with low normal serum FT4 levels. The performance of screening tests to evaluate thyroid function during routine pregnancies remains controversial. The 2017 ATA guidelines recommend thyroid function screening for pregnant women with high-risk factors. A multicenter cohort study in China found that thyroid function screening only for pregnant women with related high-risk factors may lead to missed diagnosis in approximately 81.6% of women with hypothyroidism and 80.4% of women with hyperthyroidism.20 According to the current findings, the prevalence of thyroid dysfunction in early trimester was 52.5% in the pregnant population. The results of the present study indicated that the possibility of adverse outcome of mother and infant increases when pregnancy is complicated with thyroid disorders. Thus, routine thyroid screening of women in early pregnancy can be recommended.
As the present paper is a cross-sectional and retrospective observational study with data from a single center, it cannot ascertain that the observed unfavorable metabolic parameters are caused by changes in thyroid function. The present study acknowledges a number of other limitations: (1) our study had regional specificity due to factors such as dietary habits and geographical differences; and (2) the causal relationship between the lipid metabolism disorder and thyroid dysfunction could not be determined.
In addition, thyroglobulin assessment in future studies for a thorough evaluation of thyroid-autoimmunity-associated thyroidal responses during pregnancy may be informative.
Despite the study’s limitations, the discovered associations were highly significant; the study provided sufficient power to consider a variety of potential confounding factors, including maternal pregnancy complications that may affect pregnancy outcomes, such as GDM and PIH. The strength of this study is that it contains all the results of all deliveries, has a wide range of possible confounding parameters, and all TFT was performed in a centralized laboratory.
To sum up, according to the results of this study and previous studies, some of them seem to be inconsistent; differences in laboratory methods, kits, ethnic, genetic, and environmental factors in this research and other similar studies could explain these inconsistencies.
In view of the current findings, all pregnant women should consider routine TFT in the early stages of pregnancy. Future interventional studies are needed in order to assess the benefit of routine thyroid function screening in early pregnancy. Furthermore, the current study was conducted in one hospital; larger sample size and prospective methodological studies are needed in multiple centres in the future to validate current results and to understand the role of lipid types in the link between thyroid dysfunction and adverse pregnancy outcomes.
Conclusions
The prevalence rate of thyroid dysfunction in early pregnancy was high (52.5%). Thyroid dysfunction is related to poor metabolic phenotype during pregnancy. Maternal thyroid hormones, TSH and TPOAb, in early pregnancy are associated with dyslipidemia and various adverse pregnancy outcomes. Conventional screening of maternal thyroid diseases in early pregnancy may help improve lipid levels and decrease several adverse pregnancy outcomes. Larger sample size studies are needed in the future to confirm current findings and clarify potential mechanisms.
Abbreviations
PE, preeclampsia; HIA, hypothyroxinemia; SCH, subclinical hypothyroidism; GDM, gestational diabetes mellitus; TC, total cholesterol; LDL, low-density lipoprotein; HDL, high-density lipoprotein; TG, triglyceride; CS, cesarean section; PIH, pregnancy-induced hypertension; PTB, preterm labor; LBW, low birth weight; PPH, postpartum hemorrhage; TFT, thyroid function tests; ATA, American Thyroid Association; TSH, thyroid stimulating hormone; FT4, free thyroxine; FT3, free triiodothyronine; TPOAb, thyroid peroxidase antibody; Apo A1, apolipoprotein A1; Apo B, apolipoprotein B; Apo E, apolipoprotein E.
Ethics Statement
The study design was approved by the ethics committee of Shanghai General Hospital ([2021]036) and written informed consent was obtained from all subjects. This study was conducted in accordance with the declaration of Helsinki. The patients were selected from those who visited antenatal clinics of Shanghai General Hospital.
Acknowledgments
We thank the staff of laboratory and medical record section in Shanghai General Hospital for their help in technical assistance and information service. We are thankful to Xianming Xu Director for allowing us to carry out this work.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. de Escobar GM, Obregon MJ, Del Rey FE. Maternal thyroid hormones early in pregnancy and fetal brain development. Best Pract Res Clin Endocrinol Metab. 2004;18:225–248. doi:10.1016/j.beem.2004.03.012
2. Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocr Rev. 2010;31(5):702–755. doi:10.1210/er.2009-0041
3. Khan I, Okosieme OE, Lazarus JH. Current challenges in the pharmacological management of thyroid dysfunction in pregnancy. Expert Rev Clin Pharmacol. 2017;10:97–109. doi:10.1080/17512433.2017.1253471
4. Rastgooye Haghi A, Solhjoo M, Tavakoli MH. Correlation between subclinical hypothyroidism and dyslipidemia. Iran J Pathol. 2017;12(2):106–111. doi:10.30699/ijp.2017.24867
5. Alexander EK, Pearce EN, Brent GA, et al. 2017 guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. J Am Thyroid Assoc. 2017;27(3):315–389. doi:10.1089/thy.2016.0457
6. Yang X, Meng Y, Zhang Y, et al. Thyroid function reference ranges during pregnancy in a large Chinese population and comparison with current guidelines. Chin Med J (Engl). 2019;132(5):505–511. doi:10.1097/CM9.0000000000000051
7. Crump C, Sundquist J, Winkleby MA, Sundquist K. Gestational age at birth and mortality from infancy into mid-adulthood: a national cohort study. Lancet Child Adolesc Health. 2019;3:408–417. doi:10.1016/S2352-4642(19)30108-7
8. International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diab Care. 2010;33(3):676–682. doi:10.2337/dc09-1848
9. Kintiraki E, Papakatsika S, Kotronis G, Goulis DG, Kotsis V. Pregnancy-induced hypertension. Hormones (Athens). 2015;14(2):211–223. doi:10.14310/horm.2002.1582
10. Leung AS, Millar LK, Koonings PP, Montoro M, Mestman J. Perinatal outcome in hypothyroid pregnancies. Obstet Gynecol. 1993;81:349–353.
11. Su PY, Huang K, Hao JH, et al. Maternal thyroid function in the first twenty weeks of pregnancy and subsequent fetal and infant development: a prospective population-based cohort study in China. J Clin Endocrinol Metab. 2011;96:3234–3241. doi:10.1210/jc.2011-0274
12. Ashoor G, Maiz N, Rotas M, et al. Maternal thyroid function at 11–13 weeks of gestation and spontaneous preterm delivery. Obstet Gynecol. 2011;117:293–298. doi:10.1097/AOG.0b013e318205152c
13. Chen LM, Du WJ, Dai J, et al. Effects of subclinical hypothyroidism on maternal and perinatal outcomes during pregnancy: a single center cohort study of a Chinese population. PLoS One. 2014;9(10):e109364. doi:10.1371/journal.pone.0109364
14. Sheehan PM, Nankervis A, Araujo E, et al. Maternal thyroid disease and preterm birth: systematic review and meta-analysis. J Clin Endocrinol Metab. 2015;100:4325–4331. doi:10.1210/jc.2015-3074
15. Arbib N, Hadar E, Sneh-Arbib O, Chen R, Wiznitzer A, Gabbay-Benziv R. First trimester thyroid stimulating hormone as an independent risk factor for adverse pregnancy outcome. J Matern Fetal Neonatal Med. 2017;30(18):2174–2178. doi:10.1080/14767058.2016.1242123
16. Rawal S, Tsai MY, Hinkle SN, et al. A longitudinal study of thyroid markers across pregnancy and the risk of gestational diabetes. J Clin Endocrinol Metab. 2018;103(7):2447–2456. doi:10.1210/jc.2017-02442
17. Wang Y, Sun F, Wu P, et al. A prospective study of early-pregnancy thyroid markers, lipid species, and risk of gestational diabetes mellitus. J Clin Endocrinol Metab. 2021;dgab637. doi:10.1210/clinem/dgab637
18. Vrijkotte TG, Hrudey EJ, Twickler MB. Early maternal thyroid function during gestation is associated with fetal growth, particularly in male newborns. J Clin Endocrinol Metab. 2017;102(3):1059–1066. doi:10.1210/jc.2016-3452
19. Goldberg IJ, Huang LS, Huggins LA, et al. Thyroid hormone reduces cholesterol via a non-LDL receptor-mediated pathway. Endocrinology. 2012;153(11):5143–5149. doi:10.1210/en.2012-1572
20. Wang W, Teng W, Shan Z, et al. The prevalence of thyroid disorders during early pregnancy in China: the benefits of universal screening in the first trimester of pregnancy. Eur J Endocrinol. 2011;164:263–268. doi:10.1530/EJE-10-0660
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.