")
Back to Journals » Patient Preference and Adherence » Volume 17
Associations of Attitudes and Practice Toward Oral Health, Socioeconomic Status, Self-Rated Oral Health, Subjective Oral Symptoms, and Oral Health-Related Quality of Life Among Residents in Eastern China: A Structural Equation Modeling Approach
Authors Zhao C, Zhou H, Ge S, Zhan Z, Zhang S, Liao S
Received 8 May 2023
Accepted for publication 7 July 2023
Published 17 July 2023 Volume 2023:17 Pages 1689—1703
DOI https://doi.org/10.2147/PPA.S420513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Chen Zhao,1,* Haoyun Zhou,2,* Shaowen Ge,1 Zhaojun Zhan,1 Shunhua Zhang,3 Shengkai Liao1
1Department of Stomatology, First Affiliated Hospital of Bengbu Medical College, Bengbu, 233004, People’s Republic of China; 2School of Public Health, Bengbu Medical College, Bengbu, 233030, People’s Republic of China; 3School of Medical Imaging, Bengbu Medical College, Bengbu, 233030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shengkai Liao, Department of Stomatology, First Affiliated Hospital of Bengbu Medical College, Bengbu, 233004, People’s Republic of China, Email [email protected]
Background and Purpose: The purpose of this study was to investigate the relationships among attitudes and practice about oral health, socioeconomic status, subjective oral symptoms, self-rated oral health, and oral health-related quality of life (OHRQoL) in a group of people from eastern China.
Methods: Between January 2021 to February 2022, 2502 (87.4%) of the 2863 participants completed an online questionnaire. OHRQoL, Socio-demographics characteristics, attitudes and practice toward oral health, self-rated oral health and subjective oral symptoms were all covered by the questionnaires. Based on the hypothetical model, structural equation modeling with the bootstrap method was used to examine the interactions and the strength of the correlations between the measured variables.
Results: The final model demonstrated acceptable data fit. Socioeconomic status (β = − 0.051), attitudes (β = − 0.100) and practice (β = − 0.127) toward oral health, self-rated oral health (β = − 0.493) and subjective oral symptoms (β = 0.294) were all significantly correlated with OHRQoL. Socioeconomic status was directly linked to attitudes (β = 0.046) and practice (β =0.070) about oral health, and attitudes play the role of intermediary between practice and socioeconomic status (β = 0.018). OHRQoL was indirectly linked with attitudes mediated by practice (β = − 0.092), practice mediated by subjective oral symptoms (β = − 0.107), subjective oral symptoms mediated by self-rated oral health (β = 0.031). OHRQoL was correlated with income, educational level, and socioeconomic status. Self-rated oral health was related to educational level and socioeconomic status.
Conclusion: In a sample of eastern China residents, OHRQoL was influenced by socioeconomic status, attitudes and practice toward oral health, subjective oral symptoms, and self-rated oral health.
Keywords: oral health-related quality of life, socioeconomic status, self-rated oral health, structural equation modeling, eastern China
Introduction
Oral health is a vital part of overall wellness. Oral diseases have a strong effect on personal satisfaction and well-being.1 Poor oral health will greatly impair a person’s quality of life and have negative effects on appearance, pronunciation, smile, eating and social interaction etc.2 According to the report of the 4th national oral health epidemiology survey,3 the caries rate of permanent teeth in minors was 41.9%, and the caries rate of adults was 89%; the periodontal health rate of the 12-year-old age group was 41.6%; the 15-year-old age group was 34.8%; and the periodontal health rate decreased gradually with the increase of age; the periodontal health rate of the 35–44-year-old age group was 9.1%; and the 55–64-year-old age group was only 5.0%. The awareness rate of oral health knowledge among Chinese residents was 60.1%, and 84.9% of the participants had a positive attitude toward oral health care, but the percentage of people with good oral health habits was relatively low. The rate of brushing twice a day or more was not more than 50% in all age groups, and the rate of dental floss usage is still very low. With the development of social-psychological-biomedical model, a clinical research outcome index called oral health-related quality of life (OHRQoL) has been proposed.4
OHRQoL is a multifaceted concept that encompasses a person’s subjective assessment of their oral status, functional and social-emotional health, self-consciousness, well-being, aspirations, and satisfaction.5,6 It may reflect the degree to which oral health affects general well-being and happiness in particular spheres of life (such as physical, psychological, functional, etc.).7,8
In order to formulate effective oral health promotion strategies, clarifying the elements that impact residents’ OHRQoL and how they interact is crucial. Previous research has shown that people’s OHRQoL is negatively correlated with their socioeconomic status.9–11 According to our earlier studies, OHRQoL was impacted by attitudes and practice toward oral health and self-rated oral health.12 Additionally, a study among Japanese university students was conducted to examine the connection between self-rated oral health, subjective oral symptoms, and OHRQoL.13 However, few studies have integrated these factors and examined the relationship between them with OHRQoL. Furthermore, it is unclear whether these factors have a direct or indirect relationship with OHRQoL.
Socioeconomic status is a multidimensional variable, usually represented by income and education.14 Previous research has demonstrated the complex connection between individual socioeconomic status and oral health.15 People with lower socioeconomic status have poor oral health, which also affects their OHRQoL negativity.16–18 The reason may be that the lower socioeconomic status leads to the lack of material resources and access to dental services, which leads to a higher oral disease level. Yuandong Qin et al19 reported a link between socioeconomic status and adopting a good attitude toward oral health. Studies have demonstrated that socioeconomic factors affect practice related to oral health.20,21 A study in Brazil using the structural equation modeling (SEM) method discovered that socioeconomic status was related to OHRQoL and self-rated oral health in an indirect way, mediated by dental status and dental pain.22 However, the direct and indirect ways in which socioeconomic status plays a role in OHRQoL have yet to be fully investigated. Moreover, due to the differences of society, culture and race, there are different behavioral characteristics, therefore, further research into the connection between socioeconomic status and OHRQoL in view of Chinese national conditions is required.
As oral health is recognized socially, emotionally and functionally, the use of subjective indicators is receiving more and more attention.23 As a common index in epidemiology, self-rated oral health can not only easily evaluate the general oral health status of participants,13 but also a comprehensive assessment of multiple aspects of oral health and its determinants.24,25 It provides an overview of subjective reactions, values, and cultural beliefs as well as objective health status.26 In addition, the indexes of self-rated oral health and subjective oral symptoms can help dentists better understand the oral health status of patients and make better clinical decisions.
Multiple factors have been connected to self-rated oral health. Arwa Z et al23 in Canada clarified that the poorer the subjective oral symptoms, the worse the self-rated oral health and OHRQoL. Bado FMR et al27 in Brazil reported that significant correlations between low self-rated oral health, income, and educational level were discovered. self-rated oral health has shown the inequality of socioeconomic status.28–30 However, People of different nationalities and cultural backgrounds have different views on oral health. There are not too many studies in China focusing on the connection among self-rated oral health, subjective oral symptoms, and OHRQoL. Besides, the strength of the associations among self-rated oral health, subjective oral symptoms, and OHRQoL has not been extensively studied.
Attitudes and practice toward oral health, subjective oral symptoms and OHRQoL are all latent variables that make it challenging to assess directly. Traditional multivariate statistical techniques can only determine that different factors have an effect on OHRQoL; it is unable to assess the complicated causal relationships when possible constructs are involved. On the contrary, SEM is viewed as a group of statistical models that attempt to explain how various variables relate to one another.31 In addition, SEM can provide results for the direct and indirect effects of every construct in a model as well as results for the mediating effect in any study,32,33 making up for the defects of traditional multivariate statistical technique.
Our study aimed to determine the relationships among attitudes and practice about oral health, socioeconomic status, self-rated oral health, subjective oral symptoms, and OHRQoL in a group of people from eastern China using structural equation modeling method.
Methods
Participants and Data Collection
Residents of Anhui Province in eastern China between the ages of 10 and 70 were surveyed between January 2021 and February 2022. There were 2502 participants in the study’s overall sample. The adequate sample size used in this study supported the reliability of our findings.
In this study, we adopted the snowball sampling strategy and convenience sampling method to issue an anonymous online questionnaire through WeChat (a Chinese messaging app). All submitted questionnaires were examined and verified by the submitter to ensure that they were completed in full. We randomly selected one community in each of the 16 cities in Anhui Province, each community neighborhood committee randomly selected five community service grid WeChat groups and sent the link to the questionnaire, encouraging the residents who participated in filling out the questionnaire to forward the link to their family and friends. A Wechat account can only fill out one questionnaire, thus avoiding the situation that the same person fills in multiple questionnaires. It takes about 10–15 minutes to complete a questionnaire. The questionnaire is widely distributed to residents through WeChat group, rather than to individuals. As a result, the precise number of surveys issued and the response rate are difficult to examine.
Instructions before completing the questionnaire: (1) purpose and protocol of the study; (2)it is anonymous and does not involve privacy; (3) participant has no problems with reading or understanding; (4) the study is entirely voluntary, and participants give their consent after being informed (When the participant is a minor, he/she needs to be accompanied by his/her parent or legal guardian to complete the questionnaire and obtain informed consent from the parent or legal guardian). At the end of the instructions, participants or his/her legal guardian need to check the box “Yes, I fully understand and agree” in order to officially enter the questionnaire. Exit at any time during the survey process without any explanation. Participants were excluded if the questionnaire was incomplete or logically incorrect or if they were not residents of Anhui Province.
In total, 2863 residents were recruited for our study, with 361 being excluded due to excessive missing values (>10%) or logical errors. Ultimately, we obtained 2502 reliable and complete questionnaires, and the effective response rate was 87.4%. This study does not involve major psychological stress events and will not cause psychological harm to participants, which is in line with the ethical principle of benefit and harmlessness. The Ethics Committee of Bengbu Medical College in China approved the study (2021199).
Hypotheses
To anticipate the correlations between the variables that were measured in this study, we put out the following hypotheses (Figure 1).
 |
Figure 1 The ideal SEM. Ellipses represent potential variables, rectangles represent observed variables. Abbreviations: OHRQoL, oral health-related quality of life; SESI, socioeconomic status index; SROH, self-rated oral health. |
Hypothesis 1 (H1): Attitudes and practice toward oral health, self-rated oral health and subjective oral symptoms influence OHRQoL significantly.
Hypothesis 2 (H2): Attitudes and practice toward oral health are influenced by socioeconomic status index (SESI).
Hypothesis 3 (H3): Attitudes related to oral health significantly affect practice, meanwhile, they all have an effect on subjective oral symptoms.
Hypothesis 4 (H4): Subjective oral symptoms significantly affect self-rated oral health.
Instruments
After consulting a significant amount of literature and getting the approval of various specialists, the initial questionnaire was created. Before the formal survey, 100 randomly selected residents were presurveyed. And then a 2-week test-retest examination was conducted with the participation of 50 volunteers from a pilot sample. According to the pre-survey and test–retest examination results, combined with expert opinions, the questionnaire was improved, and the final version of the questionnaire was obtained. OHRQoL, socio-demographic traits, self-rated oral health, attitudes and practice toward oral health, subjective oral symptoms were all covered by the questionnaire.
Six items were used to measure attitudes toward oral health, such as, “Do you believe that routine dental exams are good for your oral health ?” “Yes”, “uncertain”, and “No” were the choices, and they received the scores “2”, “1” and “0”, respectively. The final scores of attitudes toward oral health ranged from 0 to 12. Better attitudes were reflected in higher scores.
Four items were used to measure practice toward oral health, for example, “Do you replace your toothbrush approximately every three months ?” The possible response was two options, whereby 0 was “No”, 1 was ‘Yes’. The final practice scores ranged from 0 to 4. Better practice was reflected in higher scores.
Five indicators were used to assessed subjective oral symptoms, which include asking about the frequency of gum bleeding, tooth pain, dentine hypersensitivity, etc. The results: “Never = 0”, “Occasionally = 1” and “Often = 2”. The final subjective oral symptoms scores ranged from 0 to 10. The higher the score, the worse the subjective oral symptoms.
The self-rated oral health was evaluated using the query, “In general, What do you think about your current oral health status?” We used a Likert scale of five points to evaluate it, where “1” represented “very poor” and “5” was “very good”.34,35 The self-assessment of oral health is better when the score is higher.
Currently, the definition and classification of damage, impairment, and physical and mental flaws by the World Health Organization, as well as the theoretical framework of oral health put forward by Locker, serve as the foundation for the widely used OHRQoL scales.36 At the same time, the scale also verify the idea of oral health-related quality of life as a multi-dimensional idea. Including bodily function, psychological health status, social engagement, disease and treatment-related symptoms.37
In this study, we employed the Chinese version of the OHIP-14 (Oral Health Impact Profile-14), a simplified form of the OHIP-49, to assess OHRQoL.38 There are 14 items in total, which were divided into the following 4 dimensions: diminished independence, pain and discomfort, psychological discomfort, physical discomfort. It was assessed using a Likert scale with five choices, where 0 represented “never” and 4 represented “very often”, and total score was 0–56. A lower OHIP-14 score indicated a better oral health status. The validity, reliability, and accuracy of OHIP-14 have been verified.39,40 Cronbach’s α for the OHIP-14 CHN in our study was 0.97.
The socioeconomic status consists of two objective indicators: education level and annual household income as well as one compositive indicator: socioeconomic status index (SESI).
Based on the highest educational level of the participants, data on education were divided into three categories: low education (<6 years of education)= 0, middle education (6–12 years of education)= 1 and high education (>12 years of education)= 2. Annual household income was collected in 2 categories: 0 was <50,000 and 1 was ≥50,000 CNY/year. SESI is obtained by combining education and income, and total score was 0–3.14
According to the median, the comprehensive scores of SESI of the respondents are divided into three grades: low (0,1 point), middle (2 point) and high (3 point).
Cronbach’s alpha was 0.895, KMO (Kaiser-Meyer-Olkin) was 0.949, and the p-value of Bartlett’s test was 0.000 for this questionnaire.
Statistical Analyses
For data analysis, we used IBM® SPSS® Statistics version 22.0. We applied mean ± standard deviation or frequency and percentage to characterize the demographic parameters and oral health status of the respondents. For all data analyses, A p value of < 0.05 denotes statistical significance. We used the Spearman’s rank coefficient to analyze the linear correlations between the variables. The associations among OHRQoL, self-rated oral health, subjective oral symptoms, socioeconomic status, attitudes and practice toward oral health were examined using structural equation modelling. To determine if the research variables were normally distributed, the Skewness-Kurtosis test was applied.
According to our hypothesis, confirmatory factor analysis (CFA) was applied to rate the quality of the measurement model. To test the significance and strength of mediating effects among variables in the final model, we apply the bootstrap method. Moreover, we used the bias-corrected bootstrap 95% confidence interval (CI) to determine the significance and strength of direct and indirect effects. We applied the maximum likelihood estimate (MLE) method to estimate the parameters. Chi-square/degrees of freedom (χ2/df), standardized root-mean-square residual (SRMR), root mean square error of approximation (RMSEA), adjusted goodness of fit index (AGFI), and other indexes were applied to evaluate the fitness of the model. We applied the Mann–Whitney U-test and the Kruskal–Wallis H-test to compare the differences between several groups of the variables.
Results
Characteristics of the Participants
We analyzed 2502 residents (1047 males and 1455 females), aged between 10 and 70 years old. Demographic characteristics data, self-rated oral health and the degree of SESI are showed in Table 1.
 |
Table 1 Demographic Characteristics, Self-Rated Oral Health and SESI Degree of Participants (n = 2502) |
Correlation Analysis Among Variables
Zero-order correlations between the measures are showed in Table 2. Self-rated oral health, oral health related attitudes, practice and OHRQoL were significantly correlated with all measurements. Except for SESI, subjective oral symptoms were substantially linked with all other parameters. A similar relationship was seen for the OHRQoL dimension of psychological discomfort.
 |
Table 2 Correlation Analysis Among Variables |
Hypothetical Model Testing
In the results, all variables were considered to be normal (skewness <3 and kurtosis <8). We removed the path from “attitudes” and “subjective oral symptoms” since the path coefficient was not statistically significant (p > 0.05). Additionally, several error terms of the relevant variables were connected using modification indices (AMOS) because the initial model did not fit the sample data well. Finally, the standardized path coefficients of the final model showed statistical significance (all p<0.05) after model modification (Figures 2 and 3).
 |
Figure 2 Direct effects in the final model (bootstrapped standardized estimates). Solid lines represent direct effects. *p<0.05; **p < 0.01; ***p < 0.001. Ellipses represent potential variables, rectangles represent observed variables. Abbreviations: OHRQoL, oral health-related quality of life; SESI, socioeconomic status index; SROH, self-rated oral health. |
 |
Figure 3 Indirect effects in the final model (bootstrapped standardized estimates). Dashed lines represent indirect impacts. *p<0.05; ***p < 0.001. Ellipses represent potential variables, rectangles represent observed variables. Abbreviations: OHRQoL, oral health-related quality of life; SESI, socioeconomic status index; SROH, self-rated oral health. |
Furthermore, all of the fitness indicators of SEM model met the acceptable standards ultimately.41–43 The fitness indicators of the initial model and the final model were compared with the recommended criteria (Table 3).
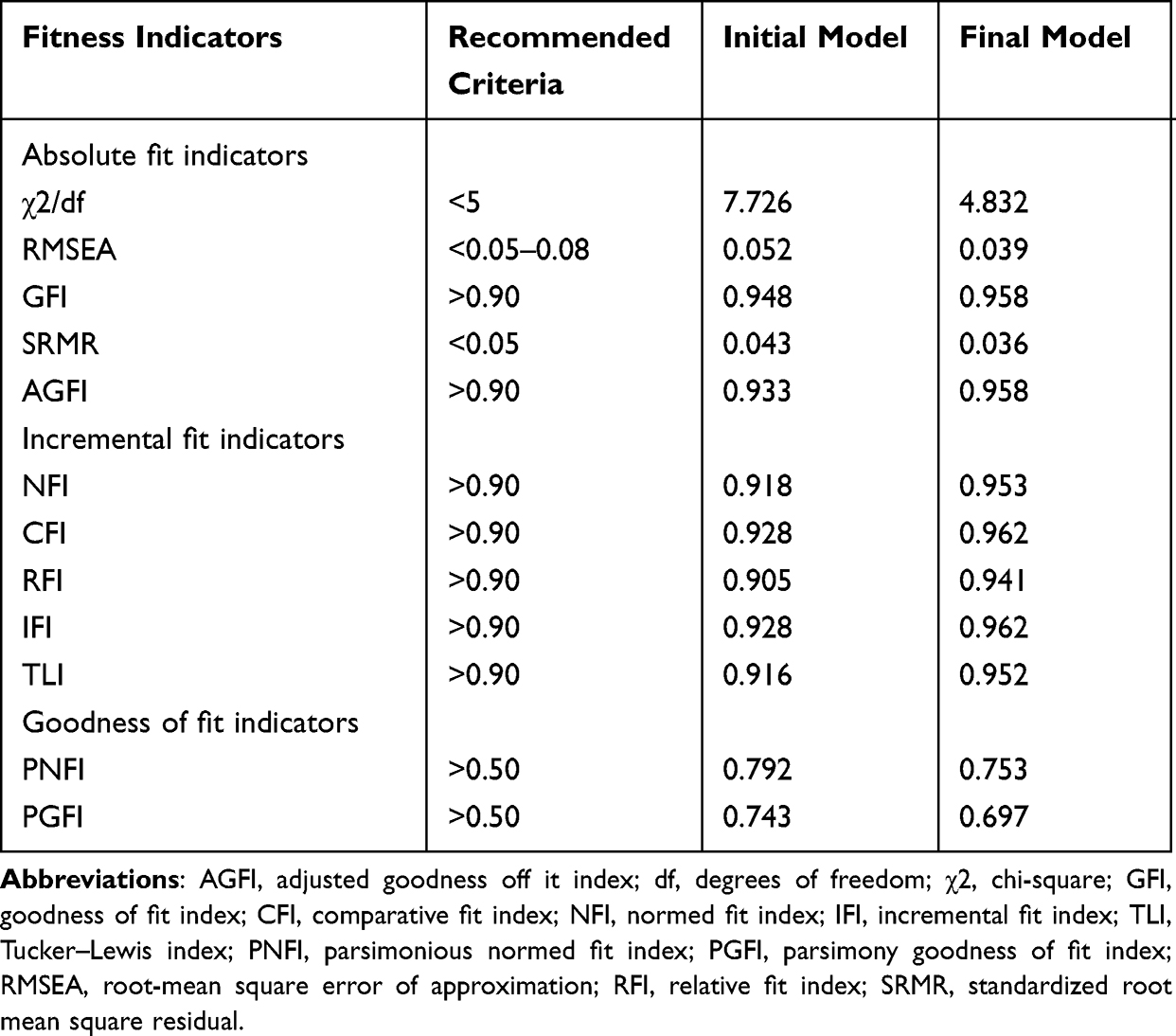 |
Table 3 The Fitness Indicators of SEM Models |
Analysis of the Final Model
Figures 2, 3 and Table 4 indicate that OHRQoL was significantly and directly related to attitudes (β = −0.100) and practice (β = −0.127) toward oral health, subjective oral symptoms (β = 0.294) and self-rated oral health (β = −0.493). Attitudes (β = 0.046) and practice (β =0.070) toward oral health were directly predicted by SESI. Oral health related attitudes were directly related with practice (β = 0.392). Subjective oral symptoms were directly linked to oral health related practice (β = −0.392) and self-rated oral health (β = −0.493). In addition, OHRQoL was found to be indirectly related to attitudes mediated by practice (β = −0.092), practice mediated by subjective oral symptoms (β = −0.107), subjective oral symptoms mediated by self-rated oral health (β = 0.031). SESI indirectly affected practice through attitudes (β = 0.018).
 |
Table 4 Standardized Direct, Indirect, and Total Effects for the Final Model |
Furthermore, subjective oral symptoms were the most influential factor on OHRQoL, followed by practice, attitudes, and self-rated oral health. And they had respective total effective values of 0.325, −0.234, −0.191, and −0.063.
As shown in Table 5, Figures 4 and 5 that income, education level, and SESI were all significantly correlated with OHRQoL, while self-rated oral health was only correlated with education level and SESI significantly.
 |
Table 5 Univariate Analyses of Socioeconomic Status, OHRQoL and Self-Rated Oral Health |
 |
Figure 4 Disparitiies in OHIP-14 scores by educational level (a), income (b) and SESI (c). Abbreviations: SESI, socioeconomic status index; CNY, Chinese Yuan; OHIP-14, Oral Health Impact Profile-14. |
 |
Figure 5 Disparitiies in self-rated oral health by educational level (a) and SESI (b). Abbreviations: SESI, socioeconomic status index; SROH, self-rated oral health. |
Graphs of OHRQoL versus self-rated oral health at various levels of education was shown in Figure 6. The figure demonstrate that higher OHIP-14 scores among those with lower income (6b). Those with the poorest self-rated oral health have the highest OHIP-14 scores (6a, b).
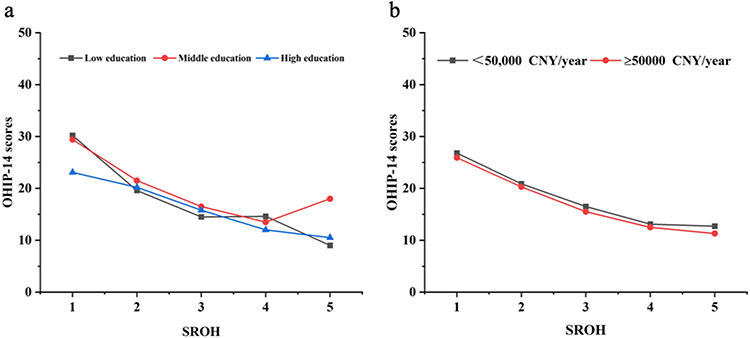 |
Figure 6 The relationship between OHIP-14 scores and SROH under different levels of education (a) and income (b). Abbreviations: SROH, self-rated oral health; OHIP-14, Oral Health Impact Profile-14; CNY, Chinese Yuan. |
Discussion
In the SEM analysis, our study identified the relationships among attitudes and practice toward oral health, socioeconomic status, self-rated oral health, subjective oral symptoms and OHRQoL in a group of people from eastern China. The findings demonstrated a significant and direct relationship between attitudes and practice toward oral health, subjective oral symptoms, self-rated oral health and OHRQoL. Among them, subjective oral symptoms were the most influential factor on OHRQoL. Attitudes and practice toward oral health were directly predicted by socioeconomic status. Oral health related attitudes were directly related with practice. Subjective oral symptoms was directly linked to oral health related practice and self-rated oral health. The relationship between OHRQoL and other parameters has attracted the attention of many researchers.9–12 As far as we are aware, the associations among attitudes and practice toward oral health, socioeconomic status, self-rated oral health, subjective oral symptoms and OHRQoL were examined for the first time using SEM in a sample of people from eastern China.
In China, the government has recently shown interest in improving oral health status and improving living conditions of residents. The score of OHIP-14 in this study was 15.92 ± 12.89, it was relatively low compared to the results according to a survey in Japanese university students.13 This may be due to the large age range of our subjects and people of different nationalities and cultural backgrounds have different views on oral health.
Socioeconomic status is a multidimensional variable that includes economic ability, education level, occupation and social prestige.44 Household income and education level were the most frequently applied indicators of socioeconomic status in the current epidemiological investigation.9
In our study, socioeconomic status was directly linked to attitudes and practice toward oral health, that is, poor socioeconomic status resulted in poor attitudes and practice toward oral health. The findings of our research were in line with those of the survey carried out by Rong Min Qiu et al.45 They claimed that socioeconomic status had an impact on children’s oral health through the attitudes and behaviors related to oral health of their caregivers. Qi Zhang et al20 in China have reported that residents in rural areas and with low education had low level of attitudes and practice toward oral health. Furthermore, practice was found to be indirectly related to socioeconomic status mediated by attitudes. This means that residents benefit from positive psychological factors for better oral health-related practice.
Moreover, we found that attitudes and practice towards oral health were directly related to OHRQoL. This finding was confirmed by our earlier research.12 But unlike previous study, our study found that, via practice, oral health-related attitudes can affect OHRQoL indirectly and significantly. The reason may be that the previous study only focused on college students, and the age range was relatively narrow. Besides, psychological discomfort of OHRQoL was significantly correlated with all measurements, except socioeconomic status. This finding was also differed from the previous study. A meta-analysis showed that material and psychological problems are more likely to have an influence on people with low socioeconomic status, which have a detrimental impact on the psychological and social aspects of OHRQoL.9
This phenomenon could be interpreted as meaning that our study was conducted among residents of eastern China, and the type and scope of population are limited.
As revealed by earlier findings, socioeconomic status and oral health status are linked in a complex manner15,46 and lower the individuals’ socioeconomic status, the poorer their OHRQoL.9,10 Therefore, socioeconomic status can be used as a predictor of OHRQoL to help identify the target population with greater risk of oral diseases. By helping people with low socioeconomic status to establish a positive oral health attitude, it may be able to improve their oral health practices, so as to obtain better OHRQoL, and ultimately achieve the goal of improving the quality of life and well-being of residents.
In our study, the relationships between subjective oral symptoms, self-rated oral health and OHRQoL are showed directly and significantly. This findings were supported by previous surveys. The research done by Vettore MV et al22 in Brazilian adolescents showed that poor subjective oral symptoms predict worse self-rated oral health and poor OHRQoL. In addition, oral health related practice could indirectly influence OHRQoL via subjective oral symptoms. Subjective oral symptoms could indirectly influence OHRQoL via self-rated oral health. This imply that subjective oral symptoms and self-rated oral health are very important as predictors of OHRQoL and since the role of oral health in society, emotion and function has been recognized, the use of subjective indicators has received more and more attention.
In correlation analysis among variables, We found that self-rated oral health and socioeconomic status were associated significantly, while subjective oral symptoms were not. This indicates that poor self-rated oral health caused by low socioeconomic status may not need to be reflected via subjective oral symptoms. This underlying mechanism unlike previous investigations. Vettore MV et al22 using SEM reported that higher socioeconomic status predicts better self-rated oral health and subjective oral symptoms and poorer subjective oral symptoms was a meaningful mediator of the relationship between lower socioeconomic status and poorer self-rated oral health. The reason may be that previous study was conducted among Brazilian adolescents, and our subjects had a wider range of age and more diverse views on oral symptoms.
In our investigation, OHRQoL was significantly associated with income, educational level and socioeconomic status. This finding was supported by previous studies. Maria Augusta Bessa Rebelo et al17 reported in Brazil that education level was linked to OHRQoL via clinical dental status and poor dental status was associated with lower income, which was also connected to poorer OHRQoL. Janice Simpson de Paula et al11 found that monthly income had strong influence on OHRQoL. However, unlike to the results in which Bado FMR et al27 found that people with higher education level linked to poor OHRQoL, we found that people with middle education level had the worst OHRQoL. Therefore, further research on the relationship between education level of Chinese residents and OHRQoL should be carried out.
In addition, self-rated oral health was significantly linked to education level and socioeconomic status. The findings were similar to the survey in which Bado FMR et al27 reported that associations were found between self-rated oral health and education level. But in our study, self-rated oral health was unrelated to income. This is contrary to previous research results. Vettore MV et al22 using SEM found that higher income predicted better self-rated oral health. The different results may be due to people with different national conditions, cultural backgrounds and age spans have different views on oral health. This may also mean that compared with income, education level has a greater influence on self-rated oral health.
In our study, we also found the significantly connection between practice related to oral health, subjective oral symptoms and self-rated oral health. This finding has been proved by the survey that Supa Pengpid et al47 carried out in Kenya, in which they found factors linked to self-rated oral health include oral conditions and practice related to oral health. This means that the positive oral health care behavior helps to build a better self-perception of oral health, thus improving residents’ overall oral condition.
The outcomes of the path analysis in the model show that the path coefficient of attitudes toward subjective oral symptoms was not statistically significant. However, previous studies have shown that compared to physical health problems, disease-related attitudes better explained the variation in subjective health index.26 The various survey designs, various country circumstances, and various participant demographics could all be contributing factors to the various outcomes.(SEM vs cross-sectional study, residents aged 10 to 70 in Anhui Province, eastern China vs independent-living older individuals aged over 65 years old from the city of Campinas, Brazil).
This study has several limitations. First, our research uses SEM method, which has the disadvantage that it is unable to establish inferential causality in the research. Second, self-reported questionnaire design has its flows, in which it could lead to bias and residents providing socially acceptable responses. Third, the fact that our study only included residents of Anhui Province in eastern China may account for the lack of universality of the research. Fourth, in the SEM analysis, the attitudes and practice toward oral health, socioeconomic status, subjective oral symptoms, self-rated oral health and OHRQoL were included. However, there may be additional factors, such as factors of age,2,17 gender,48,49 occupation46 and family structure.11 Therefore, it is crucial to carry out more in-depth research in the future employing longitudinal designs and a larger population. Notwithstanding the limitations described, our findings provide a basis for the formulation of oral health policies and oral disease control strategies in different periods and may facilitate the restructuring of the existing dental services under the National Social Security Scheme towards creating a better patient care system.
Conclusion
Our study revealed that OHRQoL was significantly associated with socioeconomic status, attitudes and practice toward oral health, subjective oral symptoms and self-rated oral health. socioeconomic status was directly linked to attitudes and practice toward oral health. Attitudes play the role of intermediary between practice and socioeconomic status. In addition, OHRQoL was indirectly linked with attitudes mediated by practice. Practice mediated by subjective oral symptoms, subjective oral symptoms mediated by self-rated oral health. OHRQoL was linked to income, educational level and socioeconomic status, self-rated oral health was linked to educational level and socioeconomic status. However, oral health related attitudes failed to affect subjective oral symptoms in this model. The findings of this research may help medical workers and policy makers better understand residents from diverse socioeconomic status origins, identify those who are more susceptible to having poor OHRQoL or poor oral health, so as to formulate better oral health promotion strategies, improve the overall oral health literacy of residents, and thereby residents obtain better OHRQoL and well-being.
Abbreviations
SEM, Structural equation modelling; SESI, Socioeconomic status index; OHRQoL, Oral health-related quality of life; OHIP-14, Oral Health Impact Profile-14; KMO, Kaiser–Meyer–Olkin; CFA, Confirmatory factor analysis; CFI, Comparative fit index; df, degrees of freedom; χ2, Chi-square; TLI, Tucker-Lewis index; GFI, Goodness of fit index; AGFI, Adjusted goodness of fit index; NFI, Normed fit index; RFI, Relative fit index; IFI, Incremental fit index; PNFI, Parsimonious normed fit index; CI, confidence interval; PGFI, Parsimony goodness of fit index; SRMR, Standardized root mean square residual; MLE, Maximum likelihood estimate; RMSEA, Root mean square error of approximation; CNY, Chinese Yuan.
Data Sharing Statement
On reasonable request, the corresponding author provides the datasets used and/or analyzed during the current study.
Ethics Approval and Consent to Participate
The Medical Ethics Committee of Bengbu Medical College approved the protocol of the research (project code 2021199). The ethical guidelines established by the institutional and national research committees, the 1964 Helsinki statement and its later amendments or similar ethical standards, were followed in all procedures carried out in studies involving human participants. Participants read the informed consent and select “I have read the informed consent form carefully and hope to continue” prior to the enrollment of this study. The ethics committee gave its approval to the informed consent protocol.
Acknowledgments
The researchers appreciate all of the people who took part in the study and all of the kind participants who assisted us in carrying it out.
Funding
This study was funded by the Key projects of Humanities and Social Sciences of Bengbu Medical College (No. 2020byzd224sk), the Innovation and Entrepreneurship Training Program for college Students in Anhui Province (No. S202010367051), and the Postgraduate Research Innovation Project of Bengbu Medical College (No. Byycxz22073).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Locker D, Matear D, Stephens M, Jokovic A. Oral health-related quality of life of a population of medically compromised elderly people. Community Dental Health. 2002;19(2):90–97.
2. Baniasadi K, Armoon B, Higgs P, et al. The Association of Oral Health Status and socio-economic determinants with Oral Health-Related Quality of Life among the elderly: a systematic review and meta-analysis. Int J Dent Hyg. 2021;19(2):153–165. doi:10.1111/idh.12489
3. Record of the Press Conference on the results obtained from the 4th national oral health epidemiology survey. Available from: https://www.gov.cn/xinwen/2017-09/20/content_5226224.htm.
4. Kragt L, Dhamo B, Wolvius EB, Ongkosuwito EM. The impact of malocclusions on oral health-related quality of life in children-A systematic review and meta-analysis. Clin Oral Investig. 2016;20(8):1881–1894. doi:10.1007/s00784-015-1681-3
5. Hakami Z, Chung HS, Moafa S, et al. Impact of fashion braces on oral health related quality of life: a web-based cross-sectional study. BMC Oral Health. 2020;20(1):236. doi:10.1186/s12903-020-01224-1
6. Uzarevic Z, Bulj A. Oral Health-Related Quality of Life among Croatian University Students. Int J Environ Res Public Health. 2021;18(12:564).
7. Locker D, Allen F. What do measures of ‘oral health-related quality of life’ measure? Community Dent Oral Epidemiol. 2007;35(6):401–411. doi:10.1111/j.1600-0528.2007.00418.x
8. Meredith P, Strong J, Ford P, Branjerdporn G. Associations between adult attachment and: oral health-related quality of life, oral health behaviour, and self-rated oral health. Qual Life Res. 2016;25(2):423–433. doi:10.1007/s11136-015-1089-1
9. Knorst JK, Sfreddo CS, de FMG, Zanatta FB, Vettore MV, Ardenghi TM. Socioeconomic status and oral health-related quality of life: a systematic review and meta-analysis. Community Dent Oral Epidemiol. 2021;49(2):95–102. doi:10.1111/cdoe.12616
10. Sfreddo CS, Moreira CHC, Nicolau B, Ortiz FR, Ardenghi TM. Socioeconomic inequalities in oral health-related quality of life in adolescents: a cohort study. Qual Life Res. 2019;28(9):2491–2500. doi:10.1007/s11136-019-02229-2
11. de Paula JS, Leite ICG, de Almeida AB, Ambrosano GMB, Mialhe FL. The impact of socioenvironmental characteristics on domains of oral health-related quality of life in Brazilian schoolchildren. BMC Oral Health. 2013;13(1):10. doi:10.1186/1472-6831-13-10
12. Zheng S, Zhao L, Ju N, Hua T, Zhang S, Liao S. Relationship between oral health-related knowledge, attitudes, practice, self-rated oral health and oral health-related quality of life among Chinese college students: a structural equation modeling approach. BMC Oral Health. 2021;21(1):99. doi:10.1186/s12903-021-01419-0
13. Yamane-Takeuchi M, Ekuni D, Mizutani S, et al. Associations among oral health-related quality of life, subjective symptoms, clinical status, and self-rated oral health in Japanese university students: a cross-sectional study. BMC Oral Health. 2016;16(1):127. doi:10.1186/s12903-016-0322-9
14. Wang Y, Pan L, Wan S, et al. Association of Socioeconomic Status and Overweight/Obesity in Rural-to-Urban Migrants: different Effects by Age at Arrival. Front Public Health. 2020;8:622941. doi:10.3389/fpubh.2020.622941
15. Wang L, Cheng L, Yuan B, Hong X, Hu T. Association between socio-economic status and dental caries in elderly people in Sichuan Province, China: a cross-sectional study. BMJ Open. 2017;7(9):e016557. doi:10.1136/bmjopen-2017-016557
16. Vettore MV, Aqeeli A. The roles of contextual and individual social determinants of oral health-related quality of life in Brazilian adults. Qual Life Res. 2016;25(4):1029–1042. doi:10.1007/s11136-015-1118-0
17. Rebelo MA, Cardoso EM, Robinson PG, Vettore MV. Demographics, social position, dental status and oral health-related quality of life in community-dwelling older adults. Qual Life Res. 2016;25(7):1735–1742. doi:10.1007/s11136-015-1209-y
18. Chaffee BW, Rodrigues PH, Kramer PF, Vitolo MR, Feldens CA. Oral health-related quality-of-life scores differ by socioeconomic status and caries experience. Community Dent Oral Epidemiol. 2017;45(3):216–224. doi:10.1111/cdoe.12279
19. Qin Y, Zhang R, Yuan B, et al. Structural equation modelling for associated factors with dental caries among 3-5-year-old children: a cross-sectional study. BMC Oral Health. 2019;19(1):102. doi:10.1186/s12903-019-0787-4
20. Zhang Q, Li Z, Wang C, et al. Prevalence and predictors for periodontitis among adults in China, 2010. Glob Health Action. 2014;7:24503. doi:10.3402/gha.v7.24503
21. Cho HJ, Lee HS, Paik DI, Bae KH. Association of dental caries with socioeconomic status in relation to different water fluoridation levels. Community Dent Oral Epidemiol. 2014;42(6):536–542. doi:10.1111/cdoe.12110
22. Vettore MV, Ahmad SFH, Machuca C, Fontanini H. Socio-economic status, social support, social network, dental status, and oral health reported outcomes in adolescents. Eur J Oral Sci Apr. 2019;127(2):139–146. doi:10.1111/eos.12605
23. Gazzaz AZ, Carpiano RM, Aleksejuniene J. Socioeconomic status, social support, and oral health-risk behaviors in Canadian adolescents. J Public Health Dent. 2021;81(4):316–326. doi:10.1111/jphd.12478
24. Arantes R, Frazao P. Subjective oral symptoms associated with self-rated oral health among Indigenous groups in Central-West Brazil. Community Dent Oral Epidemiol. 2018;46(4):352–359. doi:10.1111/cdoe.12375
25. Borrell LN, Baquero MC. Self-rated general and oral health in New York City adults: assessing the effect of individual and neighborhood social factors. Community Dent Oral Epidemiol. 2011;39(4):361–371. doi:10.1111/j.1600-0528.2010.00603.x
26. Lhdn TO, Fagundes MLB, Silva DDD, et al. Self-rated general and oral health and associated factors in independently-living older individuals. Braz Oral Res. 2020;34:e079. doi:10.1590/1807-3107bor-2020.vol34.0079
27. Bado FMR, De Checchi MHR, Cortellazzi KL, Ju X, Jamieson L, Mialhe FL. Oral health literacy, self-rated oral health, and oral health-related quality of life in Brazilian adults. Eur J Oral Sci. 2020;128(3):218–225. doi:10.1111/eos.12695
28. Bhat M, Bhat S, Roberts-Thomson KF, Do LG. Self-Rated Oral Health and Associated Factors among an Adult Population in Rural India-An Epidemiological Study. Int J Environ Res Public Health. 2021;18(12):75.
29. Mejia G, Armfield JM, Jamieson LM. Self-rated oral health and oral health-related factors: the role of social inequality. Aust Dent J Jun. 2014;59(2):226–233. doi:10.1111/adj.12173
30. Hakeberg M, Wide Boman U. Self-reported oral and general health in relation to socioeconomic position. BMC Public Health. 2017;18(1):63. doi:10.1186/s12889-017-4609-9
31. Cheung MW. Some reflections on combining meta-analysis and structural equation modeling. Res Synth Methods. 2019;10(1):15–22. doi:10.1002/jrsm.1321
32. Tarka P. An overview of structural equation modeling: its beginnings, historical development, usefulness and controversies in the social sciences. Qual Quant. 2018;52(1):313–354. doi:10.1007/s11135-017-0469-8
33. Abid A, Jie S, Aslam W, Batool S, Lili Y. Application of structural equation modelling to develop a conceptual model for smallholder’s credit access: the mediation of agility and innovativeness in organic food value chain finance. PLoS One. 2020;15(8):e0235921. doi:10.1371/journal.pone.0235921
34. Furuta M, Ekuni D, Takao S, Suzuki E, Morita M, Kawachi I. Social capital and self-rated oral health among young people. Community Dent Oral Epidemiol Apr. 2012;40(2):97–104. doi:10.1111/j.1600-0528.2011.00642.x
35. Azusa K, Daisuke E, Shinsuke M, et al. Relationships between self-rated oral health, subjective symptoms, oral health behavior and clinical conditions in Japanese university students: a cross-sectional survey at Okayama University. BMC Oral Health. 2013;13:62.
36. Locker D. Measuring oral health:A conceptual framework. Community Dent Health. 1988;5(1):3–18.
37. Lj XWN. Validation of a Chinese version of the oral health impact profile-14. Zhonghua Kou Qiang Yi Xue Za Zhi. 2006;41(4):242–245.
38. Slade GD. Derivation and validation of a short-form oral health impact profile. Comtnunity Dent Oral Epidetniol. 1997;25:284–290.
39. Brennan DS. Oral Health Impact Profile, EuroQol, and Assessment of Quality of Life instruments as quality of life and health-utility measures of oral health. Eur J Oral Sci. 2013;121(3 Pt 1):188–193. doi:10.1111/eos.12035
40. Brennan DS, Singh KA, Spencer AJ, Roberts-Thomson KF. Positive and negative affect and oral health-related quality of life. Health Qual Life Outcomes. 2006;4:83. doi:10.1186/1477-7525-4-83
41. Wang T, Ren M, Shen Y, et al. The Association Among Social Support, Self-Efficacy, Use of Mobile Apps, and Physical Activity: structural Equation Models With Mediating Effects. JMIR Mhealth Uhealth. 2019;7(9):e12606. doi:10.2196/12606
42. Astrom AN, Lie SA, Gulcan F. Applying the theory of planned behavior to self-report dental attendance in Norwegian adults through structural equation modelling approach. BMC Oral Health. 2018;18(1):95. doi:10.1186/s12903-018-0558-7
43. Ju N, Liao S, Zheng S, Hua T, Zhang S. Structural equation modeling to detect predictors of breast self-examination behavior: implications for intervention planning. J Obstet Gynaecol Res. 2021;47(2):583–591. doi:10.1111/jog.14550
44. Paula A, Braveman CC, Egerter S, et al. Socioeconomic Status in Health Research: one Size Does Not Fit All. JAMA. 2005;294(22):2879–2888.
45. Rong Min Qiu ECL, Hui Zhi Q, Zhou Y. Factors related to children’s caries: a structural equation modeling approach. BMC Public Health. 2014;14:1071.
46. Parat K, Radic M, Boric K, Perkovic D, Biocina Lukenda D, Martinovic Kaliterna D. Association of low socioeconomic status and physician assessment of disease severity with oral health-related quality of life in patients with systemic sclerosis: a pilot study from Croatia, a country in transition. J Int Med Res. 2018;46(12):5127–5136. doi:10.1177/0300060518791089
47. Pengpid S, Peltzer K. Self-rated oral health status and social and health determinants among community dwelling adults in Kenya. Afr Health Sci. 2019;19(4):3146–3153. doi:10.4314/ahs.v19i4.37
48. Locker D. Disparities in oral health-related quality of life in a population of Canadian children. Community Dent Oral Epidemiol. 2007;35(5):348–356. doi:10.1111/j.1600-0528.2006.00323.x
49. Piovesan C, Antunes JL, Guedes RS, Ardenghi TM. Impact of socioeconomic and clinical factors on child oral health-related quality of life (COHRQoL). Qual Life Res. 2010;19(9):1359–1366. doi:10.1007/s11136-010-9692-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.