Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Associations Between Renal Dysfunction Subtypes and Vertebral Fracture in Patients with Type 2 Diabetes: A Longitudinal Study
Authors Hu N, Zhang Y ![]() , Wei Z, Yu R, Zhang Y, Chen X
, Wei Z, Yu R, Zhang Y, Chen X
Received 4 March 2025
Accepted for publication 27 May 2025
Published 11 June 2025 Volume 2025:18 Pages 1915—1924
DOI https://doi.org/10.2147/DMSO.S522430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Nandong Hu,1,2,* Yiping Zhang,2,* Zicheng Wei,2 Rui Yu,2 Yingying Zhang,3 Xiao Chen2
1Department of Radiology, Renji Hospital, School of Medicine, Shanghai Jiaotong Universty, Shanghai, 200127 People’s Republic of China; 2Department of Radiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China; 3Department of Cardiology, the First People’s Hospital of Taian, Tai’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao Chen, Department of Radiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China, Email [email protected] Yingying Zhang, Department of Cardiology, the First People’s Hospital of Taian, Tai’an, People’s Republic of China, Email [email protected]
Purpose: Renal dysfunction and vertebral fracture are both common in patients with type 2 diabetes mellitus (T2DM). However, the association between renal dysfunction and vertebral fracture has rarely been evaluated longitudinally. In this longitudinal study, we evaluated the associations between different subtypes of renal dysfunction and vertebral fracture (VF) in patients with type 2 diabetes.
Methods: This study recruited T2DM patients aged 50 years or older whose computed tomography (CT) imaging screening revealed no VFs from January 2019–December 2021. The participants were followed up annually until January 2024. The Genant score was used to define new-onset VFs. The renal dysfunction phenotypes were as follows: no renal dysfunction, estimated glomerular filtration rate (eGFR) decline or proteinuria, and eGFR decline + proteinuria. Cox proportional hazards models were used to assess the association between renal dysfunction and VF.
Results: A total of 135 patients developed new VFs over a median follow-up period of two years. A total of 270 patients without fractures were matched according to follow-up time and body mass index. Bone CT attenuation (HU) (adjusted hazard ratio (HR) = 0.97, 95% confidence interval (CI) 0.99– 0.99) was independently associated with VF. eGFR decline or proteinuria and eGFR decline + proteinuria were associated with VF (adjusted HR = 1.98, 95% CI 1.35– 2.92; adjusted HR = 2.53, 95% CI 1.30– 4.92). Subgroup analyses revealed associations in women, patients without accompanying neuropathy, patients without vascular lesions, and patients who did not receive insulin therapy. The addition of renal dysfunction improved the area under the curve of the clinical model from 0.817 (95% CI: 0.78– 0.85) to 0.839 (95% CI: 0.80– 0.87) (p < 0.05).
Conclusion: Renal dysfunction was associated with VF in patients with T2DM. The addition of renal dysfunction improved the ability of bone mass to predict VF.
Keywords: type 2 diabetes mellitus, renal dysfunction, vertebral fracture
Introduction
Diabetes is a worldwide public health issue. It has many negative effects on an individual’s overall health,1 including damage to bone health.2,3 Studies have shown that people with diabetes have a significantly increased risk of fracture compared with the general population.4–6 In addition, diabetic nephropathy (DKD), a typical microvascular complication of diabetes mellitus, is a serious threat to the health of diabetic patients and increases morbidity and mortality.7 Diabetic nephropathy not only leads to a gradual decline in renal function and eventually leads to end-stage renal disease (ESRD),7 which requires dialysis or kidney transplantation but also increases cardiovascular risk.8 It has been shown that 20% to 40% of diabetic patients may develop diabetic nephropathy during the course of their disease.9
Chronic kidney disease (CKD) is associated with an increased risk of bone disease and fracture, and the incidence of fracture increases with declining kidney function.2 With the decline in renal function and interactions with bone and blood vessels, disorders of mineral metabolism emerge, leading to the clinical syndrome of chronic kidney disease-mineral and bone disease (CKD-MBD). Protein urine is the main clinical hallmark of DKD, which is different from CKD. However, the association between renal dysfunction and the risk of fracture in diabetes patients has not been well studied. A cross-sectional study demonstrated that diabetic kidney disease was associated with fracture risk in T1DM patients10 but not in T2DM patients. However, a longitudinal study in Korea revealed that the renal dysfunction subtype was associated with the risk of hip fracture in T2DM patients.4 These conflicting results indicate that further studies are needed. In addition, 60 mL/min/1.73 m² is usually used to define CKD. However, for T2DM patients, an eGFR less than 90 mL/min/1.73 m² may also be a clinical means. However, few studies have investigated the role of an eGFR less than 90 mL/min/1.73 m² in the treatment of bone fractures. Moreover, the relationship between renal dysfunction and spine fracture in patients with T2DM has not been well studied. We hypothesized that T2DM-associated renal decline may be associated with vertebral fractures. Therefore, the aim of this longitudinal study was to determine the relationship between renal function and vertebral fractures in a Chinese population with T2DM who underwent CT screening.
Materials and Methods
Study Participants
The ethics committee reviewed the study and approved exemption from full ethics review, as it is a secondary analysis of the existing dataset, which is consistent with the policies outlined in the Measures of Ethical Review of Life Science and Medical Research Involving Humans. All the data generated or analyzed during the study are included in the published paper. T2DM patients aged 50 years or older who did not have VFs and who underwent CT for screening between January 2019 and December 2021 at our institution were eligible for inclusion in this study. Those with a medical history of malignant tumors, severe liver dysfunction (twofold elevation in functional biomarkers or/or medical history), pathological fracture, long-term use of steroids, Nutcracker syndrome and those receiving anti-osteoporosis therapy were excluded. A total of 768 participants were followed up annually until January 2024. Chronic kidney disease was defined on the basis of an estimated glomerular filtration rate < 90 mL/min/1.73 m2. Diabetes mellitus (DM) and liver dysfunction are defined as follows: serum biomarkers or medical history. For participants with new fractures, follow-up ended when the fracture occurred. One hundred and thirty-five cases of spine fracture were observed during the follow-up. A total of 270 patients were matched as a nonfracture control population at a ratio of 1:2.
Patient Data Collection
Detailed information on the data collection was reported in our previous study.11 Briefly, the following data were retrospectively collected: 1) general information, including sex, age, smoking, alcohol consumption, biological use, and insulin treatment; and 2) laboratory tests, including aspartate aminotransferase (AST), albumin, alkaline phosphatase (ALP), hemoglobin, creatinine, blood glucose, high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c), total cholesterol (TC), triglyceride (TG), and triglyceride glucose (TYG54) levels.
Definition of Renal Dysfunction and Vertebral Fracture
We classified the renal function phenotype by the presence of proteinuria and the estimated glomerular filtration rate (eGFR).4 As follows: without renal dysfunction, eGFR decline or proteinuria, eGFR decline + proteinuria.
Vertebral fracture (VF) was defined by computed tomography (CT) Genant grade scoring. When the height loss of the vertebral body was greater than 20%, fracture was considered in the present study. The vertebral fracture was evaluated by two radiologists. Fracture was considered if both of them considered a fracture present or if they disagreed, and the third radiologist considered a fracture present.
Statistical Analysis
Statistical analyses were performed via the commercial software SPSS (version 22.0.) or R (version 4.6.1). The data are shown as the means ± standard deviations (SDs) or numbers (percentages). Mann‒Whitney U-test, Student’s t test, or chi‒square test. For missing data, multiple imputation was used for data substitution. Subgroup analyses were performed for women, men and patients older than 60 years. Subgroup analyses revealed associations mainly in women and in patients with or without accompanying neuropathy or vascular lesions or who received insulin therapy. The association between renal dysfunction and VF was evaluated by Cox regression analysis. Age, bone mass, sex, liver function, smoking and drinking habits, vascular disease, neuropathy, insulin treatment and the serum ALB level were confounders. The ability of renal dysfunction to predict VF was evaluated by both Cox regression and logistic regression-based receiver operating characteristic (ROC) analysis (SPSS). The DeLong test was used to compare the area under the ROC curve (AUC). The sample size was estimated via PASS software, with β = 0.90 and ɑ = 0.05. A hazard ratio (HR) of 3 was used because a previous study reported that the HR was 3.21 in patients with an eGFR decline + proteinuria.4 The estimated sample size was 340–440 at a power of 0.86–0.93. A P value < 0.05 indicated statistical significance.
Results
General Information
One hundred and sixty-three patients had combined renal dysfunction, and 242 patients did not have renal dysfunction. The differences in the general data of T2DM patients with and without renal dysfunction are shown in Table 1. The age of patients without renal dysfunction was significantly lower than that of patients with renal dysfunction (73.13 ± 8.09 vs 74.96 ± 8.39, p = 0.015). Similar results were observed for smoking (14.5% vs 36.2%, p < 0.001), drinking (5.4% vs 15.3%, p < 0.001), ALP (83.36 ± 43.99 vs 95.83 ± 66.36, p = 0.02), blood glucose (82 7.76 ± 83 3.65 vs 8.64 ± 0.39, p < 0.001), HDL-c (1.33 ± 0.35 vs 1.33 ± 0.39, p < 0.001), TG (1.44 ± 0.77 vs 1.57 ± 1.03, p < 0.001), and the incidence of fracture (21.9% vs 50.3%, p < 0.001). The level of albumin in patients without renal dysfunction was significantly greater than that in patients with renal dysfunction (40.23 ± 4.53 vs 39.14 ± 5.57, p = 0.001). Similar results were observed for LDL-c (2.54 ± 0.91 vs 2.48 ± 1.02, p < 0.001) and total cholesterol (TC) (4.41 ± 1.31 vs 4.35 ± 1.39, p < 0.001). There were no statistically significant differences between the two groups in terms of sex; bone CT attenuation (HU); AST; hemoglobin; creatinine; insulin treatment; vascular disease; neuropathy; or coronary artery calcification.
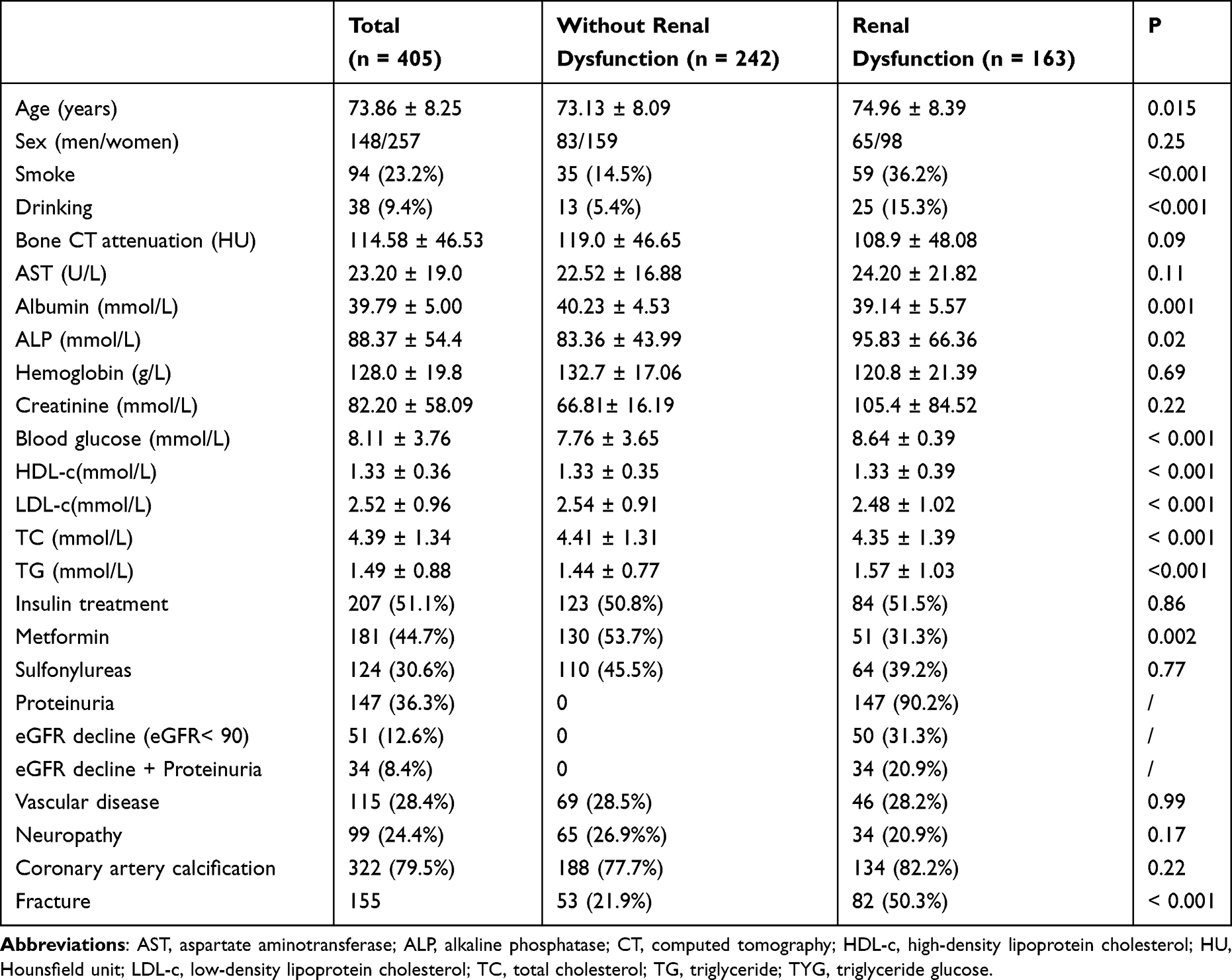 |
Table 1 Baseline Characteristics of the Patients |
Associations Between Renal Dysfunction and Vertebral Fractures
We subsequently investigated the association between renal dysfunction and the risk of vertebral fracture (Table 2). The cumulative hazard ratio (adjusted for age, sex, bone mass, liver function, smoking and drinking habits) for predicting proteinuria was 2.04 [95% confidence interval (CI): 1.41–2.94] compared with no proteinuria. After further adjustment for vascular disease, neuropathy, and insulin treatment, the hazard ratio was 2.00 (95% confidence interval (CI): 1.38–2.91). We defined renal dysfunction as eGFR decline or proteinuria and eGFR decline + proteinuria. The cumulative hazard curves of the three groups are shown in Figure 1. eGFR decline or proteinuria and eGFR decline + proteinuria were associated with VF (adjusted HR =1.98, 95% CI 1.35–2.92; adjusted HR = 2.53, 95% CI 1.30–4.92) in the fully adjusted model.
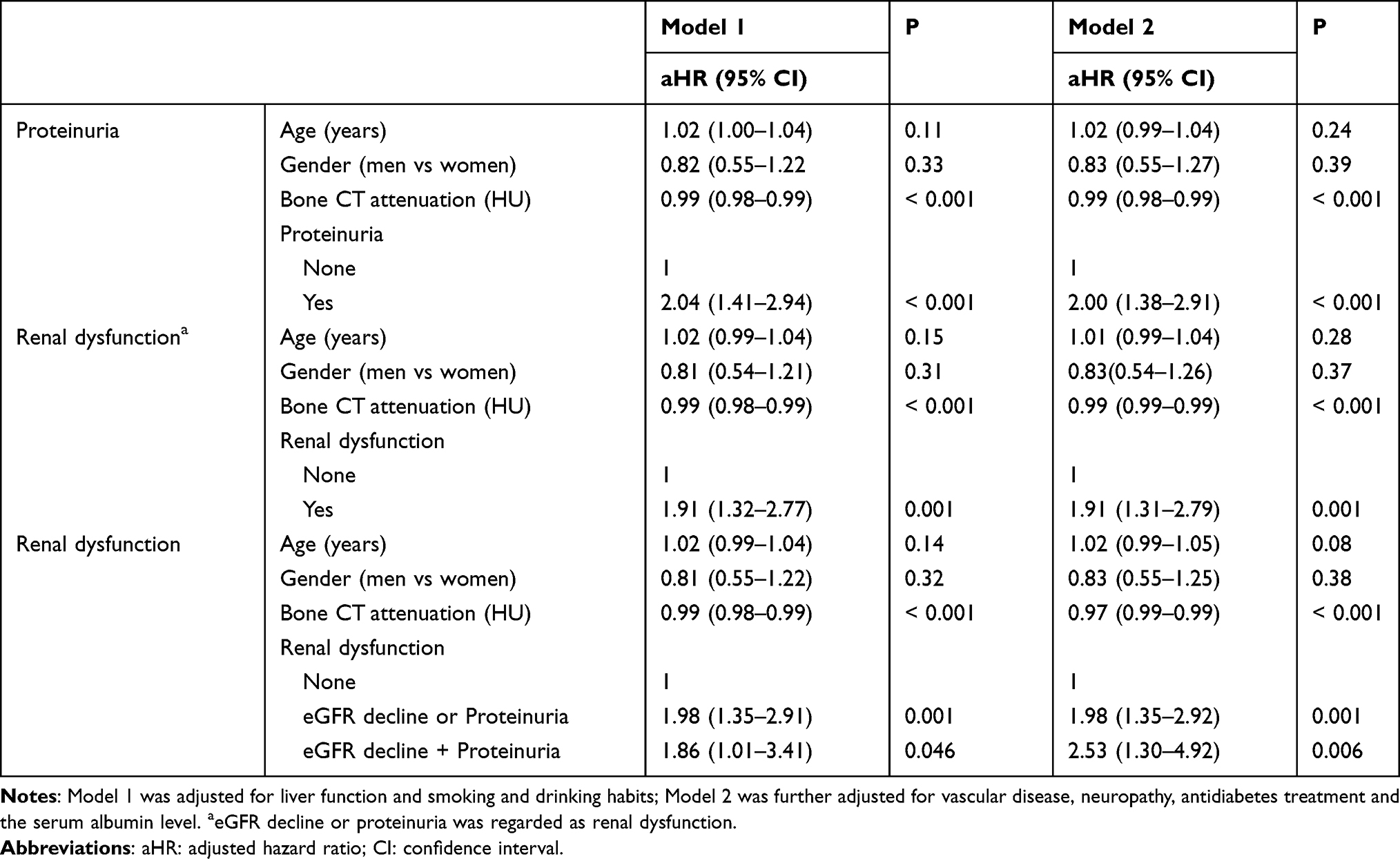 |
Table 2 Association Between Renal Dysfunction and the Risk of Vertebral Fracture |
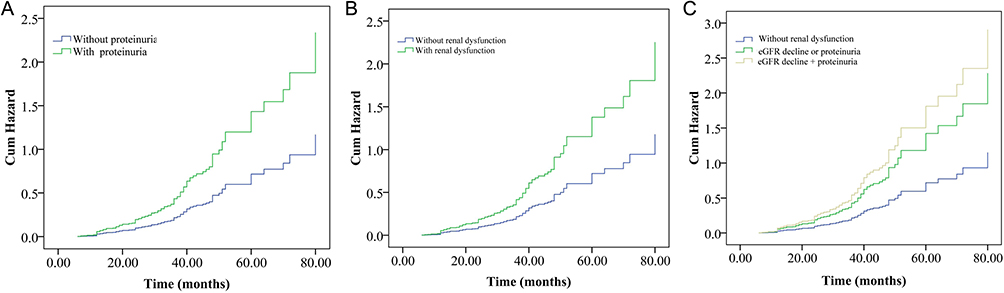 |
Figure 1 The cumulative hazard curve of vertebral fracture divided by different phenotypes of renal dysfunction. (A) with or without proteinuria; (B) with or without renal function (eGFR decline or proteinuria); (C) without renal dysfunction, eGFR decline or proteinuria and eGFR decline + proteinuria. Log rank test for all three models: p < 0.001. |
Subgroup Analysis
Subgroup analyses were performed to determine the associations between proteinuria.
The risk of spine fracture was divided by sex, smoking habits, neuropathy, vascular lesions, and insulin treatment (Figure 2). The associations with proteinuria were observed in women (HR, 1.95, 95% CI 1.24–3.07), smoking patients (HR, 2.72, 95% CI 1.41–5.25), patients without accompanying neuropathy (HR, 1.95, 95% CI 1.31–2.90), those without vascular lesions (HR, 2.1, 95% CI 1.36–3.24), those who had not received insulin therapy (HR, 2.08, 95% CI 1.28–3.38), those receiving metformin therapy (HR = 2.27, 95% CI: 1.46–3.50), and those receiving sulfonylureas (HR =3.91, 95% CI: 2.29–6.68). We also observed similar results between renal dysfunction and VFs (Figure 3).
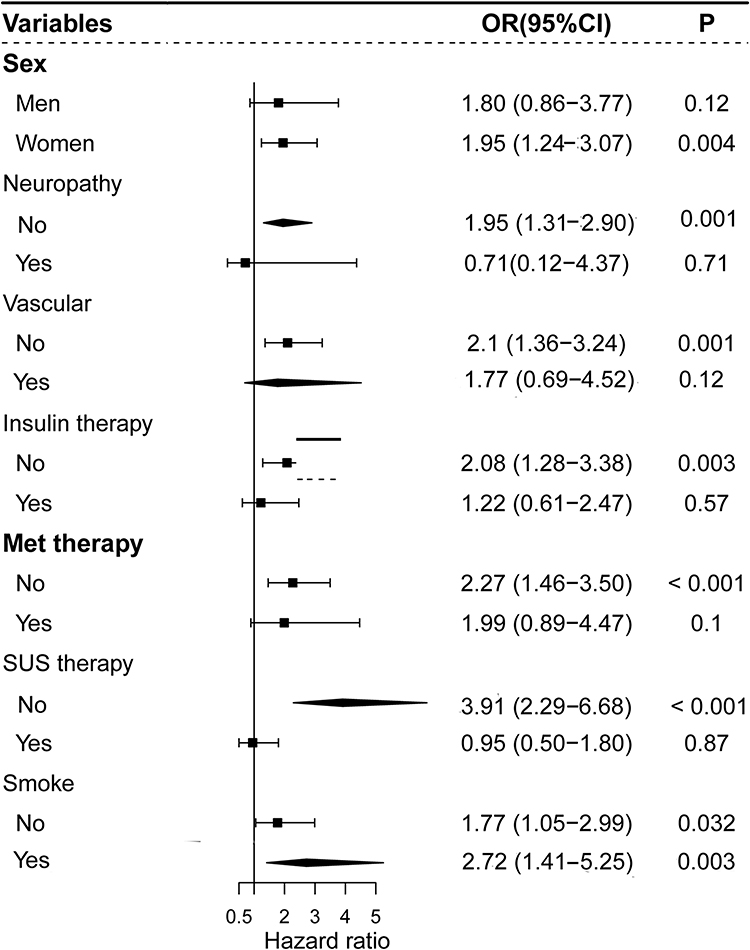 |
Figure 2 Subgroup analyses were performed to determine the associations between proteinuria and the risk of spine fracture divided by sex, smoking habits, neuropathy, vascular lesions, and insulin, metformin (Met) and sulfonylureas (SUs) treatment. |
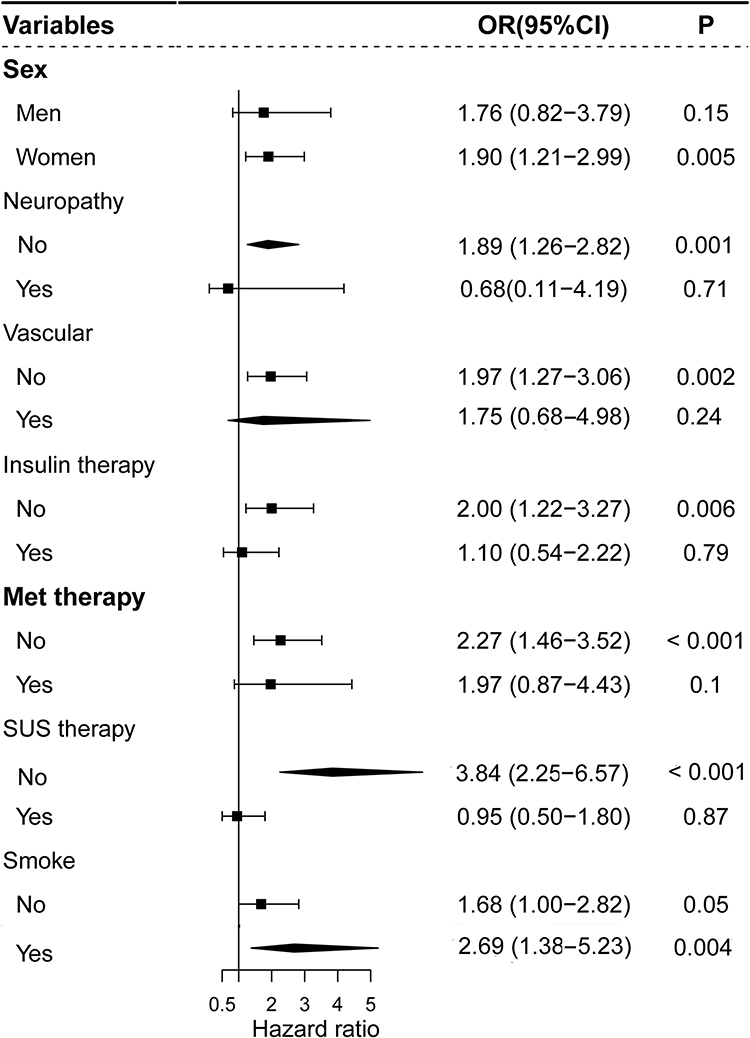 |
Figure 3 Subgroup analyses were performed to determine the associations between renal dysfunction (CKD or proteinuria) and the risk of spine fracture divided by sex, smoking habits, neuropathy, vascular lesions, and insulin, metformin (Met) and sulfonylureas (SUs) treatment. |
The Role of Renal Dysfunction in Predicting Fracture
Figure 4A shows the discriminative performance of baseline bone mass, neuropathy, hemoglobin level, insulin treatment and the combined model for predicting VF risk. The addition of renal dysfunction improved the AUC from 0.82 to 0.84 (AUC, 0.84, 95% CI 0.80–0.87 vs 0.82, 95% CI 0.78–0.85; p = 0.041) (Figure 4A). The time-dependent ROC curve also revealed that the performance of the combined model was greater than that of the model without renal dysfunction in predicting the 2–4 year risk of VF (Figure 4B).
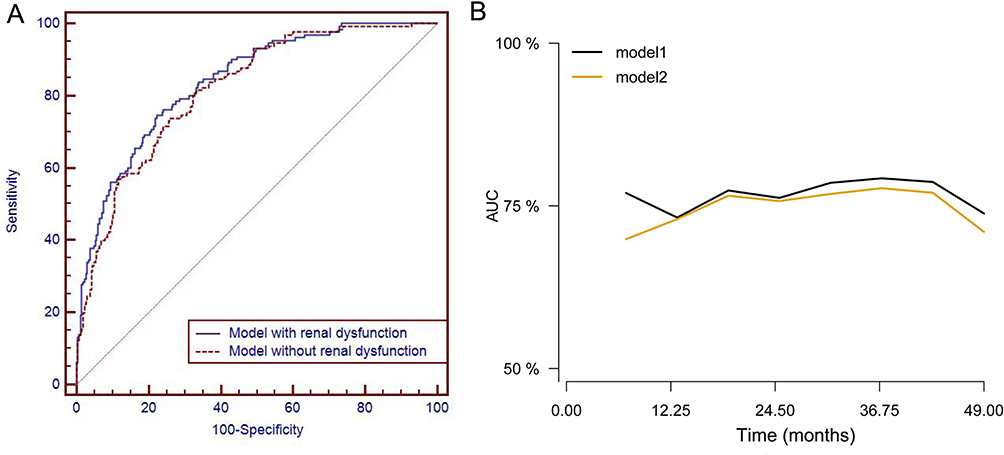 |
Figure 4 Two models were developed for predicting vertebral fracture. One model was based on baseline bone mass, neuropathy, renal dysfunction, hemoglobin level, and insulin treatment (Model 1). Another model did not include renal dysfunction (Model 2). Logistic regression (A) area under the curve (AUC) = 0.839 (95% CI: 0.80–0.87) vs 0.817 (95% CI: 0.78–0.85), p = 0.041) and Cox regression (B)-based analyses both revealed that the model with renal dysfunction had better performance. |
Discussion
Renal dysfunction or proteinuria and fracture are both common in T2DM patients. However, the associations between renal dysfunction phenotypes and the risk of VFs have not been well investigated in longitudinal studies. The present study included T2DM patients who underwent CT scans, and we found that proteinuria was associated with VFs. In addition, T2DM patients with renal dysfunction (proteinuria or eGFR decline and proteinuria + eGFR decline) were associated with VFs. Renal dysfunction also improved the performance of the clinical model in predicting fracture.
People with diabetes face a greater risk of fracture.12–14 High blood glucose levels affect the function of bone cells, reducing bone formation and enhancing bone breakdown.15,16 This is related mainly to the following factors:2,17–19 insulin resistance and persistent hyperglycemia in patients with T2DM can affect bone metabolism, leading to a slowing of bone tissue renewal; patients with diabetes usually have high levels of systemic inflammation in their bodies, and a prolonged state of inflammation is detrimental to bone health; and an imbalance between bone formation and resorption can occur. Studies have shown that bone formation may be inhibited in patients with diabetes, whereas bone resorption is increased.20 This imbalance ultimately leads to osteoporosis. In addition, some medications used to treat type 2 diabetes, such as thioureas and insulin, may affect bone metabolism.21 Moreover, complications of diabetes have long been associated with the risk of fracture. One of the common complications of diabetes is neuropathy, which reduces the patient’s sensation of pain and temperature and increases the risk of falls,22 which in turn may lead to fractures. Diabetes may also affect muscle function, reducing muscle strength and coordination,23 which can also increase the likelihood of falls.
Diabetic kidney disease (DKD) occurs in approximately 20% to 40% of people with diabetes and remains the most common cause of ESRD in most countries.7 There is an association between DKD and fractures. This is mainly because people with diabetic nephropathy may experience a range of pathological changes that affect bone health. Diabetic nephropathy leads to renal hypoplasia, and the kidneys are important sites for vitamin D activation; renal insufficiency may lead to vitamin D deficiency, which in turn affects calcium absorption and leads to disturbances in calcium and phosphorus metabolism.24–26 These changes can cause osteoporosis and increase the risk of fracture. Diabetes itself is associated with a chronic inflammatory state, and prolonged hyperglycemia can increase bone resorption and decrease bone formation, leading to bone loss.27 Additionally, certain medications used to treat diabetes (eg, insulin, thioureas, etc.) may affect bone metabolism. Kidney insufficiency (especially in advanced stages) affects the body’s ability to remove metabolic waste and may also directly or indirectly damage bone tissue.
This study revealed that diabetes patients with DKD had a greater risk of vertebral fracture than diabetes patients without DKD did, which was consistent with the findings of previous clinical studies.28 More significantly, we also found that the risk of vertebral fracture in diabetes patients with proteinuria was greater than that in diabetes patients without proteinuria. Even after adjusting for other confounding factors, proteinuria still has a significant synergistic effect on the increased risk of vertebral fractures, and similar results have been reported in previous studies on hip fractures,4 emphasizing the importance of proteinuria as a predictive factor for fracture risk. In addition, our study suggested that renal dysfunction should be incorporated into FRAX or other fracture risk calculators in T2DM patients and that early anti-fracture therapy may be needed in patients with renal dysfunction. Future studies are warranted to validate the potential benefits of early anti-fracture intervention.
In our study, we also defined renal dysfunction on the basis of both proteinuria and the eGFR. Furthermore, we analyzed the relationship between renal function grade and the risk of vertebral fracture. We found that renal function, both proteinuria and eGFR decline and proteinuria + eGFR decline, was associated with the incidence of vertebral fractures. In addition, other authors have noted that renal function may also be a significant predictor of hip fractures as well as other site fractures.4 Thus, renal dysfunction can be an important parameter for assessing fracture risk. These findings suggest that we should strengthen the monitoring and intervention of bone health in the management of patients with renal dysfunction to reduce the risk of fracture. We also investigated the additive value of renal dysfunction in predicting fractures. Our data showed that renal dysfunction or proteinuria was associated with VF. Moreover, our data further showed that the addition of renal dysfunction significantly improved the performance of the clinical model in predicting VF.
Our study has several limitations. First, the conclusions may be limited by the relatively small number of participants with VFs and short-term follow-up, so we were unable to conduct a more detailed analysis of the proteinuria group. Second, we used the CT values of the vertebral bodies instead of the BMD values of the participants, which were not included in the analysis, as there were no available data. Bone CT attenuation is highly correlated with BMD. Third, bone quality is also a critical factor for fracture. However, bone quality markers, such as the trabecular bone score, were not determined in our study. Fourth, we did not explore the specific mechanisms involved in the relationship between renal dysfunction and fracture. Fifth, kidney function trajectory and other time-varying covariates were not evaluated because our study aimed to explore the association between baseline renal function and fracture risk. Finally, this study is based on Chinese population data only; therefore, its conclusions are applicable mainly to that population. This limits the generalization and application of the findings to populations of other ethnicities backgrounds.
In conclusion, this study demonstrated that DKD is associated with an increased risk of vertebral fractures in patients with T2DM. The presence of renal dysfunction in patients with T2DM should be considered an additional risk factor for vertebral fractures. Notably, proteinuria is a major determinant of the early CKD stage. Our findings provide evidence to further understand the association between renal function and fracture risk and emphasize the importance of assessing and improving renal function in the clinical setting for fracture prevention.
Abbreviations
BMD, bone mineral density; CI, confidence interval; CT, computed tomography; HR, hazard ratio; IR, insulin resistance; TBS, trabecular bone score; TyG, triglyceride glucose; T2DM, type 2 diabetes mellitus; VFs, vertebral fractures.
Data Sharing Statement
No further data will be shared besides what is included in the manuscript. However, all the data generated or analyzed during this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The ethics committee reviewed the study and approved exemption from full ethics review, as it is a secondary analysis of the existing dataset, which is consistent with the policies outlined in the Measures of Ethical Review of Life Science and Medical Research Involving Humans. The study was conducted in accordance with the Declaration of Helsinki. The need for informed consent was waived by the Ethics Committee of the affiliated hospital of Nanjing University of Chinese Medicine because of the retrospective nature of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure Statement
The authors report no conflicts of interest in this work.
Funding
This study was funded by the National Natural Science Foundation of China (81773460) and the Medical Development and Medical Assistance Foundation of Jiangsu Province Hospital of Chinese Medicine.
References
1. Bjornstad P, Drews KL, Caprio S, et al. Long-term complications in youth-onset type 2 diabetes. N Engl J Med. 2021;385(5):416–426.
2. Hauge SC, Frost M, Hansen D. Understanding bone disease in patients with diabetic kidney disease: a narrative review. Curr Osteoporos Rep. 2020;18(6):727–736. doi:10.1007/s11914-020-00630-2
3. Hofbauer LC, Busse B, Eastell R, et al. Bone fragility in diabetes: novel concepts and clinical implications. Lancet Diabetes Endocrinol. 2022;10(3):207–220. doi:10.1016/S2213-8587(21)00347-8
4. Lee SE, Yoo J, Kim KA, Han K, Choi HS. Hip fracture risk according to diabetic kidney disease phenotype in a Korean population. Endocrinol Metab. 2022;37(1):148–158. doi:10.3803/EnM.2021.1315
5. Sheu A, Greenfield JR, White CP, Center JR. Assessment and treatment of osteoporosis and fractures in type 2 diabetes. Trends Endocrinol Metab. 2022;33(5):333–344. doi:10.1016/j.tem.2022.02.006
6. Forner P, Sheu A. Bone health in patients with type 2 diabetes. J Endocr Soc. 2024;8(7):bvae112. doi:10.1210/jendso/bvae112
7. Valencia WM, Florez H. How to prevent the microvascular complications of type 2 diabetes beyond glucose control. BMJ. 2017;356:i6505.
8. Solini A, Penno G, Bonora E, et al. Diverging association of reduced glomerular filtration rate and albuminuria with coronary and noncoronary events in patients with type 2 diabetes: the renal insufficiency and cardiovascular events (RIACE) Italian multicenter study. Diabetes Care. 2012;35(1):143–149. doi:10.2337/dc11-1380
9. Tuttle KR, Jones CR, Daratha KB, et al. Incidence of chronic kidney disease among adults with diabetes, 2015-2020. N Engl J Med. 2022;387(15):1430–1431. doi:10.1056/NEJMc2207018
10. Vestergaard P, Rejnmark L, Mosekilde L. Diabetes and its complications and their relationship with the risk of fractures in type 1 and 2 diabetes patients. Calcif Tissue Int. 2009;84(1):45–55. doi:10.1007/s00223-008-9195-5
11. Wang J, Wei Z, Wang Y, et al. Pancreatic fat infiltration is associated with risk of vertebral fracture in older patients with type 2 diabetes: a longitudinal multicenter study. Diabe Res Clin Pract. 2024;217:111904. doi:10.1016/j.diabres.2024.111904
12. Chao CT, Wang J, Huang JW, Chan DC, Hung KY, Chien KL. Chronic kidney disease-related osteoporosis is associated with incident frailty among patients with diabetic kidney disease: a propensity score-matched cohort study. Osteoporos Int. 2020;31(4):699–708. doi:10.1007/s00198-020-05353-9
13. Behanova M, Haschka J, Zwerina J, et al. The doubled burden of diabetic bone disease: hip fracture and posthip fracture mortality. Eur J Endocrinol. 2021;184(5):627–636. doi:10.1530/EJE-20-1155
14. Lee J, Han K, Park SH, et al. Associations of variability in body weight and glucose levels with the risk of Hip fracture in people with diabetes. Metabolism. 2022;129:155135. doi:10.1016/j.metabol.2022.155135
15. Park SK, Jung JY, Oh CM, et al. Fasting glucose level and the risk of incident osteoporosis in the Koreans. Bone. 2021;142:115690. doi:10.1016/j.bone.2020.115690
16. Zhuo M, Chen Z, Zhong ML, et al. Association of insulin resistance with bone mineral density in a nationwide health check-up population in China. Bone. 2023;170:116703. doi:10.1016/j.bone.2023.116703
17. Sheu A, White CP, Center JR, et al. Bone metabolism in diabetes: a clinician’s guide to understanding the bone-glucose interplay. Diabetologia. 2024;67(8):1493–1506. doi:10.1007/s00125-024-06172-x
18. Liu Q, Yang Z, Xie C, et al. The hyperglycemia and hyperketonemia impaired bone microstructures: a pilot study in rats. Front Endocrinol. 2020;11:590575. doi:10.3389/fendo.2020.590575
19. Lee HS, Hwang JS. Impact of type 2 diabetes mellitus and antidiabetic medications on bone metabolism. Curr Diab Rep. 2020;20(12):78. doi:10.1007/s11892-020-01361-5
20. Sanches CP, Vianna AGD. Barreto FC.The impact of type 2 diabetes on bone metabolism. Diabetol Metab Syndr. 2017;9:85.
21. Khosla S, Samakkarnthai P, Monroe DG, Farr JN. Update on the pathogenesis and treatment of skeletal fragility in type 2 diabetes mellitus. Nat Rev Endocrinol. 2021;17(11):685–697. doi:10.1038/s41574-021-00555-5
22. Feldman EL, Callaghan BC, Pop-Busui R, et al. Diabetic neuropathy. Nat Rev Dis Primers. 2019;5(1):42. doi:10.1038/s41572-019-0097-9
23. Salom Vendrell C, García Tercero E, Moro Hernández JB, Cedeno-Veloz BA. Cedeno-Veloz BA.Sarcopenia as a little-recognized comorbidity of type II diabetes mellitus: a review of the diagnosis and treatment. Nutrients. 2023;15(19):4149. doi:10.3390/nu15194149
24. Pittas AG, Dawson-Hughes B, Sheehan P, et al. Vitamin D supplementation and prevention of type 2 diabetes. N Engl J Med. 2019;381(6):520–530. doi:10.1056/NEJMoa1900906
25. Lips P, Eekhoff M, van Schoor N, et al. Vitamin d and type 2 diabetes. J Steroid Biochem Mol Biol. 2017;173:280–285. doi:10.1016/j.jsbmb.2016.11.021
26. Ye YW, Lu K, Yin Y, et al. Association between serum 25-hydroxyvitamin d and fasting blood glucose in osteoporosis patients. Sci Rep. 2023;13(1):18812. doi:10.1038/s41598-023-45504-6
27. Weinberg Sibony R, Segev O, Dor S, Raz I. Overview of oxidative stress and inflammation in diabetes. J Diabetes. 2024;16(10):e70014. doi:10.1111/1753-0407.70014
28. Ziolkowski S, Liu S, Montez-Rath ME, et al. Association between cause of kidney Failure and fracture incidence in a national us dialysis population cohort study. Clin Kidney J. 2022;15(12):2245–2257. doi:10.1093/ckj/sfac193
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.