Back to Journals » Clinical Interventions in Aging » Volume 20
Associations Between Hearing Impairment and Dysphagia with Cognitive Frailty in Nursing Homes Older Adults
Authors Yuan J, Wang X, Song J, Zhuo Y, Yang X, Jiang Y, Yang X, Li Y ![]()
Received 15 June 2025
Accepted for publication 19 November 2025
Published 1 December 2025 Volume 2025:20 Pages 2293—2301
DOI https://doi.org/10.2147/CIA.S547235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Zhi-Ying Wu
Jiamin Yuan,1,* Xiaoling Wang,1,* Jiao Song,1 Yan Zhuo,2 Xue Yang,1 Yangyang Jiang,1 Xiaorong Yang,3 Ying Li1
1The Center of Gerontology and Geriatrics, National Clinical Research Center for Geriatrics, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 2West China Hospital, Sichuan University, Sichuan, People’s Republic of China; 3Department of Outpatient Department, West China Hospital, Sichuan University / West China School of Nursing, Sichuan University, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Li, Email [email protected] Xiaorong Yang, Email [email protected]
Objective: To establish the prevalence of cognitive frailty (CF) among older adults residing in nursing homes and to evaluate the relationship between this condition and the prevalence of hearing impairment and dysphagia.
Measurements: A cross-sectional study of 451 individuals 60+ years of age living in nursing homes in Chengdu, Sichuan, China. The FRAIL and Chinese Mini Mental Status (CMMS) scales were respectively employed to measure physical frailty (PF) and cognitive functionality, with the results being used to separate subjects into four groups: cognitively intact non-PF individuals (“robust” group), cognitively impaired non-PF individuals (“MCI-only” group), cognitively intact individuals with PF (“PF only” group), and cognitively impaired individuals with PF (“CF” group). Individuals in these groups were evaluated for demographic characteristics, geriatric syndrome, and disease status. Hearing impairment was screened by self-report, and dysphagia was screened using the Eating Assessment Tool (EAT-10). Risk factors were evaluated through a stepwise logistic regression approach.
Results: In total, 451 individuals (144 male, 307 female; mean age: 84.15± 5.63 years) were enrolled in this study. CF was found it impact 18.6% of this cohort. Risk factors significantly associated with CF in stepwise logistic regression analyses included hearing impairment (P=0.008, OR=3.936, 95% CI=1.433– 10.813) and dysphagia (P=0.046, OR=3.441, 95% CI=1.021– 11.601). The CF group also contained a larger proportion of individuals affected by dysphagia and hearing impairment relative to the MCI-only and robust groups, respectively.
Conclusion: CF affects approximately 20% of older adults in nursing home environments, and both hearing impairment and dysphagia are strongly associated with an increased risk of CF.
Keywords: cognitive frailty, dysphagia, hearing loss, nursing homes
Introduction
With the rapid aging of the global population, maintaining quality of life in later years has become a critical public health priority. This focus has directed research attention toward conditions that threaten independent living, notably dementia and frailty. A key aspect of healthy aging involves sustaining physical, cognitive, and social engagement, with regular physical activity being a cornerstone for preserving functional capacity and well-being.1 Within this context, frailty refers to a complex age-related condition in which patients experience multi-organ reductions in normal physiological capacity culminating in the progressive impairment of normal social, cognitive, psychological, and physical functioning.2,3 Older adults with significant impairment in one or more cognitive domains (such as memory, attention, or executive function) that interferes with daily activities are diagnosed with dementia.4 Several reports have documented a significant association between physical frailty (PF) and the incidence of dementia or cognitive impairment.5,6 Patricia et al, for example, conducted a prospective observational cohort study wherein they found frailty to be associated with a 63% higher chance of mild cognitive impairment (MCI), with this relationship being maintained even after controlling for disability, vascular diseases, vascular risk factors, and symptoms of depression.7 Aron et al further observed that PF close to death was closely associated with the extent of Alzheimer’s disease (AD) pathology upon postmortem examination, suggesting that AD pathology may play a role in frailty incidence.8
In 2013, researchers first proposed the concept of cognitive frailty (CF) as a term to describe the complex geriatric syndrome affecting patients with both PF and cognitive impairment (clinical dementia rating [CDR] = 0.5) who do not meet the criteria for dementia.9 Importantly, CF is considered to be a reversible condition such that identifying and managing it in its early stages is essential as a means of preventing further physical decline or the incidence of dementia.10 Relative to older individuals exhibiting only cognitive impairment or PF, the incidence of CF can predict a greater risk of dysfunction, disability, falls, AD, and mortality.11 Given its reversible nature and potential as a target for intervention, it is vital that CF-related risk factors be identified to enable more reliable screening and interventional approaches.12
Beyond cognitive and physical function, other age-related physiological declines have also been linked to frailty. For instance, the process of swallowing is generally separated into the oral preparatory, oral transport, pharyngeal, and esophageal phases.13 Patients suffering from oropharyngeal dysphagia (OD) face difficulties in the formation of a food bolus and/or the safe movement of this food from the mouth into the esophagus. OD can contribute to the incidence of debilitating complications such as malnutrition, dehydration, aspiration pneumonia, asphyxiation, and death.14 OD is particularly common among older adults, with an estimated prevalence rate of 27–91%.15
Similarly, the cumulative impacts of the aging process can contribute to hearing loss. Age-related hearing loss (ARHL) is the most prevalent form in older adults,16 with roughly 50% of adults aged 60–70 exhibiting hearing loss sufficient to impact communication.17 Hearing loss is related to significant medical and psychological morbidity, including symptoms of depression, a greater risk of cognitive impairment and frailty, and the impairment of activities of daily living (ADL).18
A few prior studies have documented associations between frailty and the prevalence of hearing impairment or dysphagia. For example, Ning et al found that hearing impairment was associated with frailty, in which social participation and depressive symptoms partly mediate the association.19 In addition, a meta-analysis showed that decreased oral function and dysphagia may be important features of frailty and sarcopenia in older adults in the community.20 No publications, however, have focused on the relationship between CF, hearing impairment, and dysphagia. This work reviews the existing literature on risk factors associated with cognitive frailty, with an emphasis on its potential relationship with hearing loss and dysphagia.
Materials and Methods
Study Population
This was a cross-sectional analysis of adults 60+ years of age recruited using a convenience sampling method from four different nursing homes in Chengdu (Sichuan, China) from April 2019 to November 2019. Adults were eligible for inclusion if they were 60+ years of age and able to walk a minimum of 50 meters independently or with the use of a walking aid. Subjects were excluded if they (1) had been diagnosed with any major neurocognitive disorders or exhibited a total Chinese Mini Mental Status (CMMS) score < 10, as scores below this threshold represent profound cognitive impairment that compromises the validity of self-reported measures and the ability to provide informed consent or complete study assessments; (2) had severe functional dependence, defined as requiring assistance in ≥3 basic activities of daily living (ADLs), based on the Barthel Index; (3) were suffering from acute diseases such as respiratory, renal, liver, or heart failure; or (4) had any malignancies associated with a life expectancy < 6 months). Of 496 individuals initially recruited, 24 were ultimately excluded because they failed to meet the inclusion criteria, while 21 were excluded owing to severe cognitive impairment (n=10), severe disability (n=5), severe chronic diseases (n=4), and malignant tumors (n=2). Ultimately, 451 individuals 62–96 years of age were enrolled in the final study (Figure 1). The ethics committee of West China Hospital, Sichuan University approved this study, and all patients or their legal guardians provided informed consent.
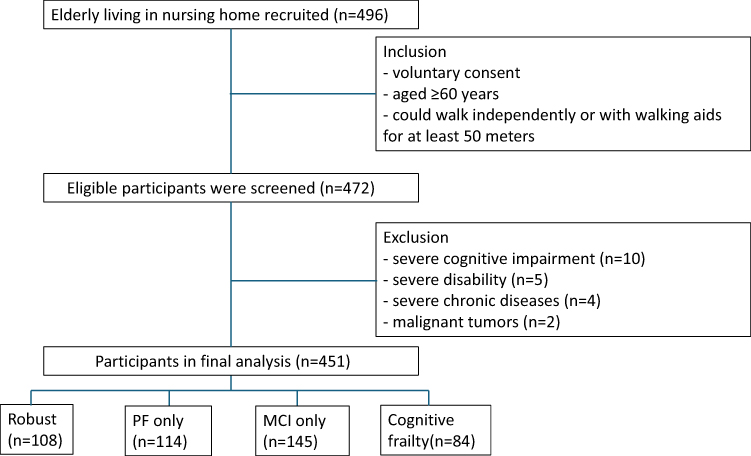 |
Figure 1 Study flow diagram.PF, physical frailty; MCI, mild cognitively impaired. |
Physical Frailty and Cognitive Function Analyses
PF was analyzed with the FRAIL scale,21 which consists of 5 dichotomous items including unintended weight loss, resistance, fatigue, illnesses, and ambulation, and was validated in the Chinese elderly population.22 Each of these items was scored with up to 1 total point, and higher total scores were indicative of more severe PF, as categorized into the robust (score = 0), pre-frail (score = 1–2), and frail (score = 3–5) severity levels.23 Participants were defined as having PF if they were classified as frail or pre-frail.12 The details of all assessment instruments, including the number of items, scoring range, and cut-off values, are provided in Supplementary Table S1.
The diagnosis of MCI uses the Chinese version of CMMS published by Wang et al in 1989, adopting the following cutoff values: ≤ 17 for illiterate individuals, ≤ 20 for individuals with primary school education, and <24 for individuals with secondary school or higher education24 Although the CMMS is not the gold standard for MCI diagnosis, it is widely used for screening purposes in large-scale geriatric studies.25
Based on their frailty and MCI status, participants were grouped into the following subsets: (1) robust: individuals with normal cognition and without PF; (2) PF only: individuals with normal cognition and PF; (3) MCI only: individuals with MCI but without PF; and (4) CF: individuals exhibiting both MCI and PF.
Dysphagia
The EAT-10 questionnaire was implemented to evaluate the severity of dysphagia. The EAT-10 questionnaire was self-administered with assistance from trained staff when necessary. This self-report tool was designed to assess the severity of self-perceived dysphagia at baseline and to monitor changes in the severity of this condition in response to particular interventions.26 It includes 10 items, each of which is scored between 0 (no problem) to 4 (severe problem). All scores are then summed together, with dysphagia being defined by a total score of at least 3.26 This approach identifies individuals at risk for clinically significant dysphagia rather than providing a definitive diagnosis. The EAT-10 screens for perceived swallowing difficulties but is not specific to oropharyngeal dysphagia.
Hearing Impairment
Hearing functions were assessed based on self-report. Hearing function was evaluated by asking participants to rate their hearing as good, fair, poor, or deaf. Study participants were considered to be suffering from hearing impairment if they used a hearing aid or selected any response other than “Good”. Although self-reported hearing has limitations, it is widely accepted as a screening tool in geriatric populations and shows acceptable concordance with audiometric testing.27–29 Thus, the measure used in this study serves as a screening indicator for hearing impairment risk. It is important to note that this method does not differentiate between ARHL and other etiologies of hearing loss.
Comprehensive Geriatric Assessment
ADLs were assessed using the Barthel index (BI), while the Lawton scale was used to assess instrumental ADLs (IADLs), with higher scores on either scale being indicative of greater functional independence.30,31 ADLs ranged from normal (Barthel index=100) to impaired (Barthel index <100).32 Disability was defined as the need for assistance with one or more instrumental ADLs, as assessed by the Lawton scale.33 Mood was evaluated with the Geriatric depression scale (GDS), with higher scores indicating the presence of depression symptoms.34 A score ≥5 on the 15-item GDS-15 scale was considered indicative of depression.33 Participant medical records were assessed to detect the presence of chronic diseases including renal disease, heart failure, angina pectoris, stroke, tumors, diabetes, myocardial infarctions, hypertension, asthma, chronic obstructive pulmonary disease, and arthritis (categorized as 0, 1–2, ≥3).
Statistical Analyses
Continuous and interval data are respectively reported as means ± standard deviations and the median (25–75 percentile). Categorical variables were reported using frequencies and proportions. Missing data were handled using listwise deletion for the primary analyses. Demographic characteristics, geriatric syndrome, and disease state were compared among the four groups using ANOVAs, Kruskal–Wallis, and chi-square tests. For significant ANOVA results, post hoc comparisons were conducted using the Bonferroni test. When P-values were < 0.05, chi-square partitions were used to identify significant differences among subgroups for categorical variables, with the significance threshold set at P < 0.008 to account for multiple comparisons using a Bonferroni correction. Factors significantly independently associated with CF were identified through multivariate logistic regression with stepwise selection. Variables with P < 0.1 in univariate analysis were considered for entry into the model. Model fitness was assessed using the Hosmer-Lemeshow test, and multicollinearity among variables was evaluated prior to model building. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs). P < 0.05 was the significance threshold for all other analyses. SPSS 25.0 was used for all statistical testing.
Results
This study enrolled 451 subjects (144 male, 307 female) with a mean age of 84.15±5.63 years (range: 62–96), of whom 108 (23.9%), 114 (25.4%), 145 (32.1%), and 84 (18.6%) were classified into the robust, PF-only, MCI-only, and CF groups. Of the adults with PF (n=198), 42.4% exhibited MCI, while of the adults with MCI (n=229), 36.7% exhibited PF (Figure 2).
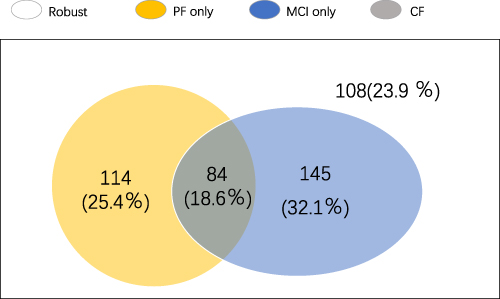 |
Figure 2 Venn diagram of the prevalence of robust, PF only, MCI only and CF status. |
The characteristics of study subjects grouped according to frailty and cognitive impairment status are shown in Table 1. These four differences exhibited significant differences with respect to age (P < 0.001), ADL disability (P < 0.001), IADL disability (P < 0.001), depression (P < 0.001), visual impairment (P=0.008), hearing impairment (P=0.003), number of chronic diseases (P < 0.001), and dysphagia (P=0.002). There were also significant differences among these groups with respect to the prevalence of chronic diseases including arthritis, renal disease, COPD, asthma, angina pectoris, and stroke. The CF group exhibited a larger proportion of dysphagia patients as compared to the robust group and a larger proportion of individuals with hearing impairment relative to the MCI-only group.
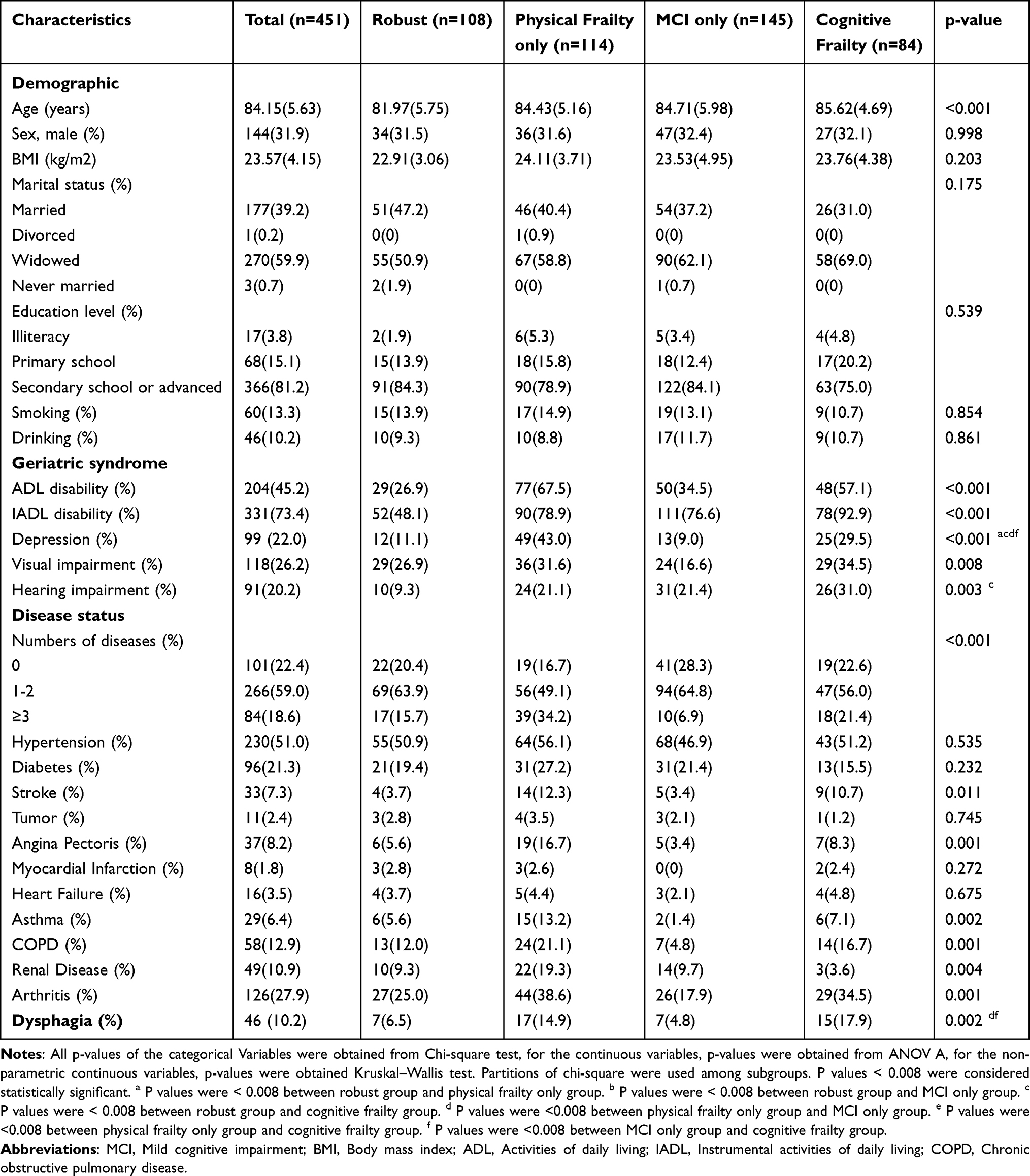 |
Table 1 Characteristics of the Participants According to Cognitive Frailty Status |
Next, stepwise logistic regression models were used to identify significant factors associated with these different groups (Table 2). In univariate analyses, hearing impairment (P=0.017, OR=2.613, 95% CI=1.185–5.765) and dysphagia (P=0.049, OR=2.529, 95% CI=1.004–6.366) were found to be potentially associated with PF-only patients as compared to individuals in the robust group. Similarly, hearing impairment (P=0.012, OR=2.655, 95% CI=1.244–5.711) was associated with patients in the MCI-only group relative to the robust group, and hearing impairment (P<0.001, OR=4.393, 95% CI=1.977–9.761) and dysphagia (P=0.018, OR=3.137, 95% CI=1.216–8.094) were associated with the CF group relative to the robust group. Following adjustment for age, gender, ADL, education level, numbers of diseases and IADL, both hearing impairment (P=0.008, OR=3.936, 95% CI=1.433–10.813) and dysphagia (P=0.046, OR=3.441, 95% CI=1.021–11.601) were found to be significantly associated with CF status relative to robust status.
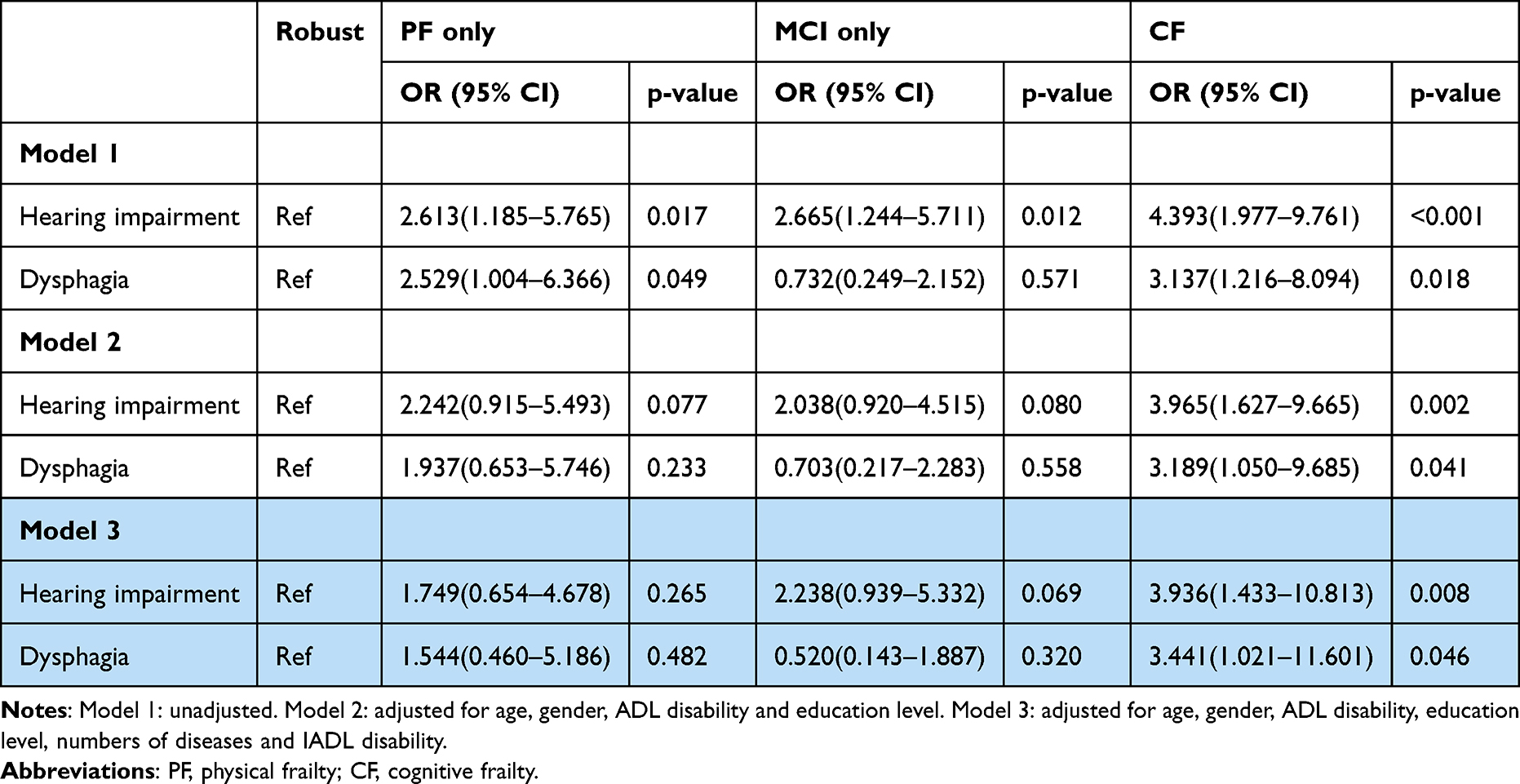 |
Table 2 Multiple Stepwise Logistic Regressions: Factors Significantly Associated with PF Only, MCI Only, CF and Robust. (N=451) |
Discussion
The 18.6% prevalence rate of CF detected in this study among older adults in nursing homes was higher than what has been reported previously.35,36 This may be attributable to the more advanced average age of these subjects (84.15±5.63 years), given that older adults face a higher risk of PF.33 Over 40% of these older adults with PF were classified as exhibiting CF, while over 30% of individuals exhibiting MCI were also classified as exhibiting CF. Significant overlap between cognitive impairment and PF was thus detected in this elderly cohort, in line with past data.12,32 Regression analyses further revealed for the first time that dysphagia and hearing impairment were associated with CF. This suggests these deficits are not merely comorbidities but integral to CF’s pathophysiology, potentially acting through mechanisms like poor nutrition, social isolation, and reduced neuroplasticity. Consequently, they represent actionable targets for early intervention, such as hearing aids or swallowing therapy, to mitigate CF progression.
Regarding dysphagia, there have been some tentative links between the risk of dysphagia and CF prevalence. In their study of 3,475 Japanese adults 65+ years of age, Nishida et al, for example, observed an independent association between dysphagia and physical, cognitive, oral, and psychological frailty.37 However, in contrast to the study by Bahat et al which analyzed 1,138 individuals 60+ years of age and detected a link between frailty and dysphagia,38 our analysis did not find a significant association between physical frailty alone and dysphagia. The risk of dysphagia can impair the intake of nutrients, thus contributing to the incidence of malnutrition and frailty.39 Oral diseases have also been potentially linked to cognitive disorders in some cases. For example, periodontal disease and number of teeth have been shown to be associated with cognitive decline or incident dementia risk, although cognitive decline was not consistently related to the number of decayed or missing teeth.40
There have been some tentative links between dysphagia and CF incidence. In their study of 3,475 Japanese adults 65+ years of age, Nishida et al, for example, observed an independent association between dysphagia and physical, cognitive, oral, and psychological frailty.37 While PF and dysphagia have previously been linked, the same was not observed in the present analysis. Bahat et al analyzed 1,138 individuals 60+ years of age in their analysis and ultimately detected a link between frailty and dysphagia.38 Dysphagia can impair the intake of nutrients, thus contributing to the incidence of malnutrition and frailty.39 Oral diseases have also been potentially linked to cognitive disorders in some cases. For example, periodontal disease and number of teeth have been shown to be associated with cognitive decline or incident dementia risk, although cognitive decline was not consistently related to the number of decayed or missing teeth.41,42
Similarly, our study provides new insights into hearing impairment. Here, hearing impairment was found to be related to CF prevalence for the first time. We interpret this association as evidence that sensory decline is an integral aspect of the frailty syndrome as a whole. These findings underscore the potential utility of routine hearing assessments in geriatric screenings as a non-invasive marker of cognitive frailty risk. While previous reports have previously documented a relationship between hearing impairment and both PF and MCI individually, our study found that the association became significant only when both PF and MCI coexisted as CF. Hearing impairment has been predicted to be associated with cognitive functional declines. Peters et al, for example, determined that hearing-impaired individuals exhibited greater declines in cognitive function at follow-up relative to individuals without such impairment, and this relationship remained intact even after adjusting for the more advanced age of individuals with hearing impairment.43 Impaired hearing can contribute to greater loneliness and social isolation, both of which can contribute to more rapid cognitive decline and the incidence of AD.44 Elderly individuals suffering from impaired hearing also need to devote some portion of their cognitive reserve to compensating for defects in auditory processing, potentially reducing the neural resources that they have available for perceptual speed, working, memory, or other cognitive processes such that deleterious AD-related pathological changes may occur more rapidly, culminating in earlier onset dementia symptoms.45 Hearing impairment and PF have also previously been linked such that impaired hearing has even been incorporated into certain frailty index scales including the 70-item CSHA Frailty Index from the Clinical Examination and Frailty Index-CGA.46,47 The discrepancies between the present results and some prior studies may stem from differences in the operational definition of frailty and cognitive impairment, as well as the study population. Unlike previous studies that often focused on community-dwelling elders, our cohort consisted exclusively of nursing home residents who typically exhibit a higher baseline level of functional and cognitive vulnerability, which may alter the manifestation and interplay of these geriatric syndromes.
These results are subject to several limitations. A key consideration is that all conditions, including cognitive frailty, dysphagia, and hearing impairment, were identified using screening tools rather than diagnostic assessments. As such, the results reflect risk or likelihood rather than confirmed diagnoses, and the findings should be interpreted as indicative of associations rather than as measures of clinical prevalence. Future studies should incorporate objective measures, such as pure-tone audiometry for hearing and instrumental swallowing assessments like videofluoroscopy for dysphagia, to validate these findings. In addition, while the overall sample size of 451 participants is adequate for a nursing home study, some subgroup analyses were limited by smaller numbers, which may reduce statistical power and is reflected in the wide confidence intervals for some estimates. Furthermore, while we adjusted for major comorbidities in our analysis, residual confounding due to unmeasured variables cannot be excluded. Finally, a limitation of this study is that the sample size was not predetermined by an a priori power analysis. However, a post hoc analysis revealed adequate power (90.26%) for our key findings, mitigating this concern to some extent.
Conclusion
In summary, screening-identified cognitive frailty affects nearly one in five nursing home residents in this study and is significantly associated with an increased risk of dysphagia and hearing impairment. Our results advocate for a holistic clinical approach that includes routine dysphagia and hearing impairment screening, followed by targeted interventions such as swallowing therapy and hearing aids, to mitigate the risk and progression of CF in this vulnerable population. Longitudinal studies and interventional trials are needed to further explore these associations and establish effective prevention and management protocols.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the research ethics committee of Sichuan University (protocol code 2019-64, and approval date February 21st, 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors are grateful to the staffs of Chengdu Jinxin Geriatrics Hospital for their support.
Funding
This study was supported by Health Care Scientific and Technology Project of Sichuan Province (2023-105, 2023-123) and the Projects of Science and Technology Department of Sichuan Province (2024NSFSC1602, 2024YFFK0324).
Disclosure
The authors declare no conflicts of interest.
References
1. Parra-Rizo MA, Vásquez-Gómez J, Álvarez C, et al. Predictors of the level of physical activity in physically active older people. Behav Sci. 2022;12(9):331. doi:10.3390/bs12090331
2. Taylor JA, Greenhaff PL, Bartlett DB, et al. Multisystem physiological perspective of human frailty and its modulation by physical activity. Physiol Rev. 2023;103(2):1137–1191. doi:10.1152/physrev.00037.2021
3. Fried LP, Cohen AA, Xue Q-L, et al. The physical frailty syndrome as a transition from homeostatic symphony to cacophony. Nat Aging. 2021;1(1):36–46. doi:10.1038/s43587-020-00017-z
4. Oh ES. Dementia. Ann Intern Med. 2024;177(11):Itc161–itc176. doi:10.7326/annals-24-02207
5. Robertson D, Savva G, Kenny R. Frailty and cognitive impairment--a review of the evidence and causal mechanisms. Ageing Res Rev. 2013;12(4):840–851. doi:10.1016/j.arr.2013.06.004
6. Fabrício D, Chagas M, Diniz B. Frailty and cognitive decline. Transl Res. 2020;221:58–64. doi:10.1016/j.trsl.2020.01.002
7. Boyle P, Buchman A, Wilson R, Leurgans S, Bennett D. Physical frailty is associated with incident mild cognitive impairment in community-based older persons. J Am Geriatr Soc. 2010;58(2):248–255. doi:10.1111/j.1532-5415.2009.02671.x
8. Buchman A, Schneider J, Leurgans S, Bennett D. Physical frailty in older persons is associated with Alzheimer disease pathology. Neurology. 2008;71(7):499–504. doi:10.1212/01.wnl.0000324864.81179.6a
9. Kelaiditi E, Cesari M, Canevelli M, et al. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutr Health Aging. 2013;17(9):726–734. doi:10.1007/s12603-013-0367-2
10. Wang S, Li Q, Wang S, et al. Sustained frailty remission and dementia risk in older adults: a longitudinal study. Alzheimers Dement. 2024;20(9):6268–6277. doi:10.1002/alz.14109
11. Bu Z, Huang A, Xue M, et al. Cognitive frailty as a predictor of adverse outcomes among older adults: a systematic review and meta-analysis. Brain Behav. 2021;11(1):e01926. doi:10.1002/brb3.1926
12. Kwan R, Leung AYM, Yee A, et al. Cognitive frailty and its association with nutrition and depression in community-dwelling older people. J Nutr Health Aging. 2019;23(10):943–948. doi:10.1007/s12603-019-1258-y
13. Crosby TW, Lebowitz J, Balou S, et al. Correlation of the VFSS esophageal screen to high-resolution esophageal manometry. Laryngoscope. 2025;135(7):2283–2290. doi:10.1002/lary.32157
14. Rajati F, Ahmadi N, Naghibzadeh ZA, Kazeminia M. The global prevalence of oropharyngeal dysphagia in different populations: a systematic review and meta-analysis. J Transl Med. 2022;20(1):175. doi:10.1186/s12967-022-03380-0
15. Serra-Prat M, Hinojosa G, López D, et al. Prevalence of oropharyngeal dysphagia and impaired safety and efficacy of swallow in independently living older persons. J Am Geriatr Soc. 2011;59(1):186–187. doi:10.1111/j.1532-5415.2010.03227.x
16. Lin FR. Age-Related Hearing Loss. N Engl J Med. 2024;390(16):1505–1512. doi:10.1056/NEJMcp2306778
17. Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences by demographic characteristics among US adults data from the national health and nutrition examination survey, 1999-2004. Arch Intern Med. 2008;168(14):1522–1530. doi:10.1001/archinte.168.14.1522
18. Ye X, Zhu D, Chen S, He P. The association of hearing impairment and its severity with physical and mental health among Chinese middle-aged and older adults. Health Qual Life Outcomes. 2020;18(1):155. doi:10.1186/s12955-020-01417-w
19. Ning H, Zhang H, Xie Z, Jiang W, Xie S. Relationship of hearing impairment, social participation and depressive symptoms to the incidence of frailty in a community cohort. J Am Geriatr Soc. 2023;71(4):1167–1176. doi:10.1111/jgs.18164
20. Sakai K, Nakayama E, Yoneoka D, et al. Association of oral function and dysphagia with frailty and sarcopenia in community-dwelling older adults: a systematic review and meta-analysis. Cells. 2022;11(14):2199. doi:10.3390/cells11142199
21. Morley J, Malmstrom T, Miller D. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012;16(7):601–608. doi:10.1007/s12603-012-0084-2
22. Ma L, Chhetri JK, Zhang Y, et al. Integrated care for older people screening tool for measuring intrinsic capacity: preliminary findings from ICOPE pilot in China. Front Med. 2020;7:576079. doi:10.3389/fmed.2020.576079
23. Cai Y, Xu W, Xiao H, Liu H, Chen T. Correlation between frailty and adverse outcomes among older community-dwelling chinese adults: the china health and retirement longitudinal study. J Nutr Health Aging. 2020;24(7):752–757. doi:10.1007/s12603-020-1368-6
24. Zhang ZWM. Application of the Chinese version of the mini-mental state examination (MMSE). Shanghai Arch Psychiatry. 1989;007:108–111.
25. Zhuang L, Yang Y, Gao J. Cognitive assessment tools for mild cognitive impairment screening. J Neurol. 2021;268(5):1615–1622. doi:10.1007/s00415-019-09506-7
26. Belafsky P, Mouadeb DA, Rees CJ, et al. Validity and reliability of the eating assessment tool (EAT-10). Ann Otol Rhinol Laryngol. 2008;117(12):919–924. doi:10.1177/000348940811701210
27. Zhao Y, Ding Q, Lin T, et al. Combined vision and hearing impairment is associated with frailty in older adults: results from the West China health and aging trend study. Clin Interventions Aging. 2022;17:675–683. doi:10.2147/cia.S362191
28. Maharani A, Dawes P, Nazroo J, Tampubolon G, Pendleton N. Visual and hearing impairments are associated with cognitive decline in older people. Age Ageing. 2018;47:575–581. doi:10.1093/ageing/afy061
29. Cavazzana A, Röhrborn A, Garthus-Niegel S, et al. Sensory-specific impairment among older people. An investigation using both sensory thresholds and subjective measures across the five senses. PLoS One. 2018;13(8):e0202969. doi:10.1371/journal.pone.0202969
30. Mahoney F, Barthel D. FUNCTIONAL EVALUATION: THE BARTHEL INDEX. Maryland State Medl J. 1965;14:61–65.
31. Lawton M, Brody E. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3 Part 1):179–186. doi:10.1093/geront/9.3_Part_1.179
32. Ge M, Zhang Y, Zhao W, et al. Prevalence and its associated factors of physical frailty and cognitive impairment: findings from the West China health and aging trend study (WCHAT). J Nutr Health Aging. 2020;24(5):525–533. doi:10.1007/s12603-020-1363-y
33. Tang H, Zhu H, Sun Q, Qin H, Wang S. Transitions in the cognitive frailty states in community-living older adults: a 6-year prospective Cohort study. Front Aging Neurosci. 2021;13:774268. doi:10.3389/fnagi.2021.774268
34. Ertan T, Eker E. Reliability, validity, and factor structure of the geriatric depression scale in Turkish elderly: are there different factor structures for different cultures? Inter Psychogeriatrics. 2000;12(2):163–172. doi:10.1017/s1041610200006293
35. Zhao Y, Lu Y, Zhao W, et al. Long sleep duration is associated with cognitive frailty among older community-dwelling adults: results from West China health and aging trend study. BMC Geriatr. 2021;21(1):608. doi:10.1186/s12877-021-02455-9
36. Tseng SH, Liu L-K, Peng L-N, et al. Development and validation of a tool to screen for cognitive frailty among community-dwelling elders. J Nutr Health Aging. 2019;23(9):904–909. doi:10.1007/s12603-019-1235-5
37. Nishida T, Yamabe K, Honda S. Dysphagia is associated with oral, physical, cognitive and psychological frailty in Japanese community-dwelling elderly persons. Gerodontology. 2020;37(2):185–190. doi:10.1111/ger.12455
38. Bahat G, Yilmaz O, Durmazoglu S, et al. Association between dysphagia and frailty in community dwelling older adults. J Nutr Health Aging. 2019;23(6):571–577. doi:10.1007/s12603-019-1191-0
39. de Sire A, Ferrillo M, Lippi L, et al. Sarcopenic dysphagia, malnutrition, and oral frailty in elderly: a comprehensive review. Nutrients. 2022;14(5):982. doi:10.3390/nu14050982
40. Asher S, Stephen R, Mäntylä P, Suominen AL, Solomon A. Periodontal health, cognitive decline, and dementia: a systematic review and meta-analysis of longitudinal studies. J Am Geriatr Soc. 2022;70(9):2695–2709. doi:10.1111/jgs.17978
41. Tonsekar PP, Jiang SS, Yue G. Periodontal disease, tooth loss and dementia: is there a link? A systematic review. Gerodontology. 2017;34(2):151–163. doi:10.1111/ger.12261
42. Wu B, Fillenbaum GG, Plassman BL, Guo L. Association between oral health and cognitive status: a systematic review. J Am Geriatr Soc. 2016;64(4):739–751. doi:10.1111/jgs.14036
43. Peters CA, Potter JF, Scholer SG. Hearing impairment as a predictor of cognitive decline in dementia. J Am Geriatr Soc. 1988;36(11):981–986. doi:10.1111/j.1532-5415.1988.tb04363.x
44. Sharma RK, Chern A, Golub JS. Age-related hearing loss and the development of cognitive impairment and late-life depression: a scoping overview. Semin Hear. 2021;42(01):10–25. doi:10.1055/s-0041-1725997
45. Boyle PA, Wilson RS, Schneider JA, Bienias JL, Bennett DA. Processing resources reduce the effect of Alzheimer pathology on other cognitive systems. Neurology. 2008;70(17):1534–1542. doi:10.1212/01.wnl.0000304345.14212.38
46. Shafiee A, Arabzadeh Bahri R, Rajai S, et al. Frailty as a predictor of adverse outcomes in burn patients: a systematic review. BMC Geriatr. 2023;23(1):680. doi:10.1186/s12877-023-04302-5
47. Giger AW, Ditzel HM, Lund CM, et al. Geriatric screening and frailty intervention in older patients with cancer. Ugeskr Laeger. 2024;186. doi:10.61409/v06230352
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Healthcare Professionals’ Knowledge, Skills, and Information Needs Pertaining to Hearing Loss and Hearing Aids in Swedish Nursing Homes: A Cross-Sectional Study and Psychometric Evaluation
Bjuresäter K, Bergström Andrén M, Mäki-Torkko E, Anderzén-Carlsson A, Carlsson PI
Journal of Multidisciplinary Healthcare 2024, 17:4693-4707
Published Date: 9 October 2024