Back to Journals » Risk Management and Healthcare Policy » Volume 16
Associations Among Organizational Capabilities, Organizational Performance and the Medical Alliance Implementation Effect in Community Health Centers in China: A Moderated Mediation Model
Received 13 June 2023
Accepted for publication 13 September 2023
Published 27 September 2023 Volume 2023:16 Pages 1969—1983
DOI https://doi.org/10.2147/RMHP.S425782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Chengsen Cui,1,2,* Bo Lv,1,* Kai Meng1,3
1School of Public Health, Capital Medical University, Beijing, People’s Republic of China; 2China Center for Health Development Studies, Peking University, Beijing, People’s Republic of China; 3High Quality Development Research Center, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kai Meng, School of Public Health, Capital Medical University, No. 10 Xitoutiao, Youanmenwai Street, Fengtai District, Beijing, 100069, People’s Republic of China, Tel/Fax +86-10-83911577, Email [email protected]
Purpose: Community health centers (CHCs) are an important part of the healthcare system worldwide. Based on the dual process model of organizational capabilities, this study explores the relationship between organizational capabilities and the organizational performance of CHCs, as well as the role played by the medical alliance implementation effect.
Methods: In this study, whole-group sampling was used to extract CHCs. All 135 CHCs in 8 of 16 districts of Beijing were selected as subjects. The organizational capabilities of the CHCs and the medical alliance implementation effect were evaluated using a questionnaire survey of 1957 managers and 3622 medical staff, respectively. A pathway analysis of the mediating role of the organizational capabilities of CHCs and the moderating role of the medical alliance implementation effect was conducted using Mplus 8.0.
Results: The development capabilities had a positive impact on basic capabilities (β = 0.878, P < 0.001), and core capabilities (β = 0.952, P < 0.001), but had no direct impact on organizational performance. Basic capabilities positively affected organizational performance (β = 1.163, P < 0.001), and core capabilities negatively affected organizational performance (β =- 0.886, P = 0.004). Both basic capabilities (β =1.022, P < 0.001) and core capabilities (β =- 0.843, P = 0.005) played a mediating role in the relationship between development capabilities and organizational performance. The moderating role of the medical alliance implementation effect was not significant.
Conclusion: This study found that strengthening the organizational capabilities of CHCs can effectively improve their performance, with the development of basic capabilities being a primary concern. The medical alliance implementation effect has not had a significant impact on organizational performance, and the cooperation between CHCs and high-level hospitals should be further promoted to give full play to the medical alliance’s role and improve the organizational performance of CHCs.
Keywords: community health centers, organizational capabilities, organizational performance, medical alliance implementation effect, China
Introduction
Primary health care services, which address the health problems of the majority of the population at the lowest cost and in the most effective way, are valued and developed by many countries.1 The current aging trend and the increasing prevalence of chronic diseases make it even more important to improve countries’ primary health care services capabilities.2–4 The Primary Health Care Performance Initiative (PHCPI) was launched in 2015 in 135 low- and middle-income countries to upgrade primary health care systems, and the Astana Declaration of 2018 states that governments should improve primary health care services capacity, strengthen infrastructure, and build sustainable primary health care systems.5 It can be seen that upgrading the primary health care system is a unified goal for all countries.
China’s health service system consists mainly of hospitals and community health centers (CHCs), CHCs are institutions providing basic medical and public health services in cities, with functions such as diagnosis, referral, and health management, and which play a role as the bottom of the net in the health service system.6,7 With the implementation of the deepening reform of the medical and health system and the promotion of the hierarchical diagnosis and treatment system, CHCs are required to provide residents with high-quality primary health care services, and it is therefore particularly important to improve the performance of CHCs. Through continuous development, the number of health technicians in CHCs has increased, the effective control rate of chronic diseases has improved, and patient satisfaction has increased.8 However, China’s CHCs are still lacking in terms of their development. Their allocation of medical resources is relatively insufficient, their operational efficiency needs to be improved, their medical service capabilities need to be strengthened, and the proportion of residents visiting CHCs decreased from 61.81% in 2009 to 51.96% in 2019.9–12 The organizational performance of CHCs has not reached the expected results, on the one hand, it may be due to the lack of scientific salary distribution, and its failure to form effective incentives. On the other hand, it may be due to the imperfect operation and management system of CHCs and the lack of high-level talent and medical equipment. Similarly, primary health care systems also need to be improved in several countries, for example, the satisfaction of older people with primary health care services was relatively low in Brazil, and the allocation of primary health care resources was insufficient in Ghana and Malaysia.3,13,14 Therefore, further research is needed to promote the development of the primary health care system.
Several studies have developed tools for evaluating the performance of primary health care systems.15,16 Some studies have further assessed the current status of national primary health care system performance.17–20 However, the literature exploring the factors influencing organizational performance in primary health care systems is relatively sparse. Several studies have shown that the implementation of health reforms, collaborative governance in the health sector, and the leadership of health managers influence the performance of primary health care systems.21–23 Medical resource management capability, human resource management capability, and quality of medical services as factors affecting the performance of primary health care organizations.24,25 These studies have focused on the effects of policy factors and single capability on organizational performance, but the organizational performance of CHCs may be affected by a variety of factors, both internal and external, and the effects of the comprehensive capabilities of CHCs on organizational performance need to be further explored. The organizational capabilities of CHCs reflect its comprehensive capabilities, which refer to the ability to dynamically adapt and optimize the external environment using organizational structures and processes, combined with the knowledge of organizational members.26 It restructures and integrates the organization’s internal and external resource structures to enable the organization to respond to changes in the external environment. Studies in the field of business management have explored the correlation between organizational capabilities and organizational performance of firms,27,28 but the impact of organizational capabilities on organizational performance in the field of healthcare needs to be further verified. Medical alliances have been fully implemented in China, which is a form of medical resource integration, consisting of a medical institution with a high level of medical technology as the “core hospital”, combined with partner hospitals and CHCs in the region, to promote the vertical flow of high-quality medical resources and enhance the medical service capacity of CHCs. However, the medical alliance implementation effects in China vary relatively widely and the effects on the organizational performance of CHCs may differ.
In conclusion, the influence of the organizational capabilities of CHCs and the medical alliance implementation effects on organizational performance is still unclear. Therefore, the purpose of this study was to investigate the mechanisms by which the organizational capabilities of CHCs influence organizational performance and whether the medical alliance implementation effects play a moderating role in the relationship.
Research Hypothesis
In the course of the development of organizational capability theory, static capability theory and dynamic capability theory are formed, which are the relationship between succession and development.29 Since the applicability of static capability theory in dynamic environments is limited, Teece proposed dynamic capability theory based on the integration of firm capability theory and dynamic evolution theory, ie, the ability of a firm to integrate, construct, or reset internal and external competitive capabilities to adapt to a rapidly changing external environment, which reflects a firm’s integrated capabilities to gain new competitive advantages within the constraints of a given path and market position.30,31 Organizational capability theory and the dual process model of organizational capabilities illustrate that organizational capabilities can provide organizations with a sustained competitive advantage, resulting in differences in performance between organizations.32,33 Therefore, strengthening organizational capabilities may be a key initiative for improving organizational performance. The dual process model of organizational capabilities assumes that the dynamic capabilities of an organization can promote the development of static capabilities, which leads to the formation of new and optimized organizational capabilities. Through such a dynamic evolutionary process, organizational capabilities are continuously developed and revised, thus enabling the organization to gain a competitive advantage.34 According to a study, the organizational capabilities of CHCs can be divided into basic, core, and development capabilities, with basic and core capabilities being static capabilities and development capabilities being dynamic capabilities.26 Basic capabilities refer to the ability of an institution to meet medical resource allocation requirements and to be able to provide the most basic health care services to residents. Core capabilities include a series of management capabilities that enable the service delivery and daily operation of CHCs. Development capabilities are progressive capabilities of CHCs, and organizations with such capabilities can continuously optimize their service models, enhance their service capabilities, and address potential risks, thus gaining an advantageous position in future development.26 Therefore this study proposes hypothesis 1:
H1: Basic capabilities and core capabilities play a mediating role in the process by which the development capabilities of CHCs influence organizational performance. H1a: Basic capabilities play a mediating role in the process by which development capabilities influence organizational performance. H1b: Core capabilities play a mediating role in the process by which development capabilities influence organizational performance.
Zott35 argue that institutions with the same organizational capabilities may still have different organizational performance, so further exploration of the factors that influence the relationship between organizational capabilities and organizational performance is merited. CHCs in China have commonly established medical alliances with higher-level hospitals, but different forms of medical alliances may have different effects on organizational performance.36,37 A better effect of medical alliances implementation maybe improve the basic medical service capabilities and management capabilities of CHCs, promote the rational allocation of medical staff, improve the satisfaction of medical staff, and enhance the basic and core capabilities of CHCs, which may have a positive impact on organizational performance.38–40 In contrast, a poor effect of medical alliance implementation affects the improvement of the medical service capabilities of CHCs and cannot promote its development. Therefore this study proposes hypothesis 2:
H2: The medical alliance implementation effect has a moderating effect on the process by which the organizational capabilities influence organizational performance of CHCs. H2a: The medical alliance implementation effect has a moderating effect on the process by which development capabilities affect organizational performance through basic capabilities. H2b: The medical alliance implementation effect has a moderating effect on the process by which development capabilities affect organizational performance through core capabilities. H2c: The medical alliance implementation effect has a moderating effect on the process by which development capabilities directly affect organizational performance.
In summary, this study constructs a moderated mediation model to explore the mediating roles of basic and core capabilities and the moderating role of the medical alliance implementation effect (Figure 1).
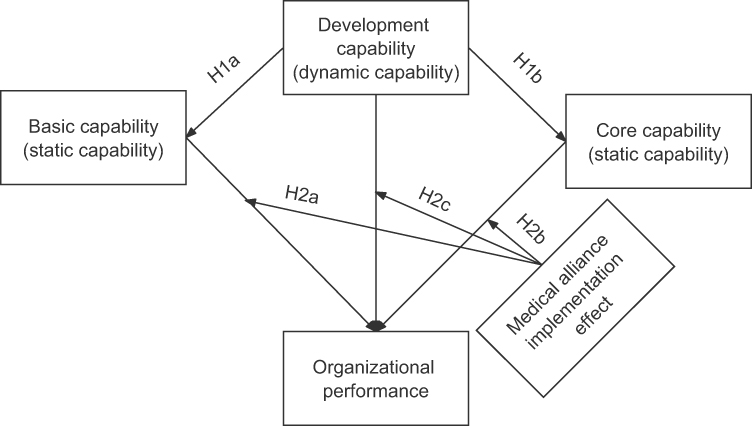 |
Figure 1 Proposed model. |
Materials and Methods
Survey Respondents
There are 16 districts in Beijing, and 8 of them (D, F, H, M, Y, S, T, and Q) were selected for this study. These 8 districts cover all functional areas in Beijing and are representative of the city’s population, economy, and health resource allocation in CHCs. A whole-group sampling method was used to select all CHCs in the 8 districts that were normally open in 2019, and a total of 135 CHCs were included, accounting for 39.13% of the total number of CHCs in Beijing in 2019.
Organizational Performance Evaluation
This study used the Community Health and Basic Public Health Services Performance Assessment Index System that was officially developed by the Beijing Health Commission to evaluate the performance of each CHC. The index system was released in 2021, the Beijing Health Commission evaluated the performance of CHCs in 16 districts in Beijing through the index system, indicating that the index system is reliable and valid. The index system contains four primary indicators, service provision, comprehensive management, sustainable development, and social evaluation, and ten secondary indicators, with a full score of 100 points, and detailed and operable assessment and scoring criteria and calculation of scores. For example, the development rate of the total number of outpatient visits in CHCs (tertiary indicator) was calculated as follows: the total number of outpatient visits in CHCs in the current year/total number of outpatient visits in CHCs in the previous year. The scoring criteria are as follows: ① the indicator is greater than or equal to 1, full score (1 point); ② the indicator is less than 1, the score = 1 - decline rate×3. The data required for the score came from the “Beijing Municipal Health Institutions Annual Report”, “Beijing Health Statistical Yearbook”, “Beijing Municipal Statistical Yearbook” and statements submitted by various CHCs. Two research team members and a research team leader rated each CHC’s performance. First, two members completed the evaluation independently, then the scores with differences were discussed and agreed upon, and finally, the scores that still had differences were reviewed by the most authoritative person in charge of the subject group to determine the final organizational performance score of each CHC.
Organizational Capabilities Measurement
Questionnaire Survey
In this study, a preconstructed and validated index system for evaluating the organizational capabilities of CHCs was used as a measurement tool. The index system was constructed using the Delphi method, incorporating 3 primary indicators, 9 secondary indicators, and 37 tertiary indicators; among them, the primary indicators of organizational capabilities included basic capabilities, core capabilities, and development capabilities.26 The weights of the indicators at each level were calculated using hierarchical analysis and the percentage weighting method. The self-assessment questionnaire was designed based on this index system and evaluated from a score of 1 (very nonconforming) to 5 (very conforming), and the total organizational capabilities score of an organization were determined by weighting the scores of all respondents from this CHC. The Cronbach’s α coefficient of the questionnaire was 0.993, and the KMO value was 0.986 (P<0.001), indicating the good reliability and validity of the questionnaire. The Questionnaire Star platform was used to conduct the questionnaire survey and collect data, and the respondents completed the anonymous online questionnaire independently after scanning the QR code through their mobile phones.
Questionnaire Respondents
Since the managers of the CHCs know the most about the operation of the CHCs, 15 middle managers from each CHC who were familiar with the operation of their institution were selected to evaluate the organizational capabilities. A total of 2025 middle managers were surveyed, and those who did not meet the requirements were excluded to ensure the quality of the completed questionnaires. The exclusion criteria were (1) questionnaires with incomplete answers and (2) questionnaires with all options the same. (3) After the questionnaire was developed, the minimum completion time was defined as 80 seconds, so questionnaires completed in less than 80 seconds were excluded. Finally, a total of 1957 valid questionnaires were returned in this study, and the effective recovery rate was 96.64%.
Evaluation of the Medical Alliance Implementation Effect
Questionnaire Survey
In this study, the evaluation of the medical alliance implementation effect referred was performed with the Medical Alliances Comprehensive Performance Assessment Index System issued by the National Health Commission in 2018. Combined with previous studies, four representative indexes were included in this study including referral work, training and support work, scientific research cooperation, and information construction. These indexes were measured with four questions, namely, “How effective is the referral work carried out by the medical alliances?”, “What is the effect of the training and support work carried out by the medical alliances?”, “What is the effect of scientific research cooperation in medical alliances?”, and “How effective is the information development of medical alliances?” Each question was evaluated from 1 (very bad) to 5 (very good), and the weights of the four questions were calculated by principal component analysis to obtain a comprehensive score for the medical alliance implementation effect. The Cronbach’s α coefficient of the questionnaire was 0.963, and the KMO value was 0.865 (P<0.001), indicating the good reliability and validity of the questionnaire. The Questionnaire Star platform was used to conduct the questionnaire survey and collect data, and the respondents completed the anonymous online questionnaire independently after scanning the QR code through their mobile phones.
Questionnaire Respondents
This part of the survey was targeted at the medical staff of CHCs. 40 medical staff from each of the 135 CHCs were randomly selected for the questionnaire survey, and a total of 5400 questionnaires were distributed. The exclusion criteria for the questionnaire were as follows: (1) medical staff who were not familiar with the implementation of medical alliances in the institution and (2) it has been calculated that the questionnaire completion time should generally be greater than 130 seconds, in order to ensure the quality of the data, exclude questionnaires with a response time of less than 130 seconds. Finally, 3622 valid questionnaires were returned in this study, and the effective recovery rate was 67.07%.
Data Analysis
This study used SPSS 26.0 and Mplus 8.0 to analyse the data. Descriptive analysis was used to analyse the basic demographic characteristics of the questionnaire respondents, basic information about the CHCs, organizational performance, organizational capabilities, and medical alliance implementation effects. Pearson correlation analysis was used to test the correlation between variables.
Both the entropy method and principal component analysis method can objectively evaluate the weights of the index are widely used.41 Entropy measures the uncertainty of variables, the greater the amount of information in the data, the smaller the uncertainty, and the smaller the entropy value, the entropy method uses the information contained in the data to calculate the weight of the index.42,43 Principal component analysis distills multiple potentially relevant variables into independent factors by dimensionality reduction and derives linear relationships between variables by extracting relevant information from the data.44 The data of this study is suitable for obtaining a comprehensive variable through a linear combination of the four relevant indexes to indicate the medical alliance implementation effect, therefore principal component analysis was used. First, we calculated the linear combination number, formula = factor loading coefficient/square root of corresponding eigenvalues. Next, the composite score coefficient was calculated with the formula  . Finally, the index weights were calculated and normalized to the composite score coefficient.45 Principal component analysis was used to integrate the four variables of referral work (X1), training and support work (X2), scientific research cooperation (X3), and information construction (X4) into a new comprehensive evaluation variable (Y), which was calculated as follows:
. Finally, the index weights were calculated and normalized to the composite score coefficient.45 Principal component analysis was used to integrate the four variables of referral work (X1), training and support work (X2), scientific research cooperation (X3), and information construction (X4) into a new comprehensive evaluation variable (Y), which was calculated as follows:

This study divided organizational capabilities into three subcapabilities, explored their pathways of influence on organizational performance, and included the medical alliance implementation effect as a moderating variable in the model. Since all variables were observable variables, it is appropriate to apply path analysis. The model included organizational performance as the dependent variable, development capabilities as the independent variable, basic capabilities and core capabilities as mediating variables, and the medical alliance implementation effect as the moderating variable to establish a moderated multiple parallel mediation model. The moderating variable acts in the second half of the two mediating effects. In order to eliminate the influence of collinearity, each variable was standardized for variables, and the parameter estimation method used the maximum likelihood estimation (ML). The bootstrap method was used to sample 1000 times for model simulation, thus increasing the stability of the results, and Mplus 8.0 was used for path analysis.
Ethical Considerations
This study is based on a research study approved by the ethics committee of Capital Medical University. The study was performed in accordance with the Declaration of Helsinki. Informed written consent was obtained from all the participants before the start of this study. By completing a consent form, the participants were informed about the purpose and method of the study. The participants were also informed that the researchers were committed to answering their questions and that their information would be kept confidential.
Results
Basic Information of the Survey Respondents
The similar staffing structure of surveyed managers and medical staff. The managers were mainly female (1347 people, 68.83%). They were mainly aged 31–40 years old (885 people, 45.22%), and their education level was mainly undergraduate (1195 people, 61.06%). A total of 1454 (74.30%) had junior or intermediate titles, and 1379 (70.46%) had fewer than 20 years of experience. The medical staff were mainly female (2502 people, 69.08%). They were mainly aged 31–40 years old (1362 people, 37.06%), and their education level was mainly undergraduate (1916 people, 52.90%). A total of 2720 (75.10%) had junior or intermediate titles, and 2496 (68.91%) had worked for fewer than 20 years (Table 1).
 |
Table 1 Basic Information of Managers and Medical Staff |
In 135 CHCs, the maximum number of health technicians was 228 and the minimum was 16. The maximum number of beds in CHCs was 150 and some CHCs had no beds. The total number of consultations was 714,161 at the highest and 14,305 at the lowest. The maximum number of permanent residents served by CHCs was 230,979 and the minimum was 4317. The average number of health technicians in CHCs in T district was the highest (111 people), while the average number of health technicians in Q district was the lowest (49 people). The average number of beds in CHCs in M district was the highest and the average number of beds in CHCs in D district was the lowest with 42 and 4 beds respectively. The average total number of consultations in CHCs in D district was the highest at 224,317 and the average total number of consultations in CHCs in Q district was the lowest at 78,873. The average number of permanent residents served in CHCs in T district was the highest at 71,625 and the average number of permanent residents served in CHCs in Q district was the lowest at 17,162 (Table 2).
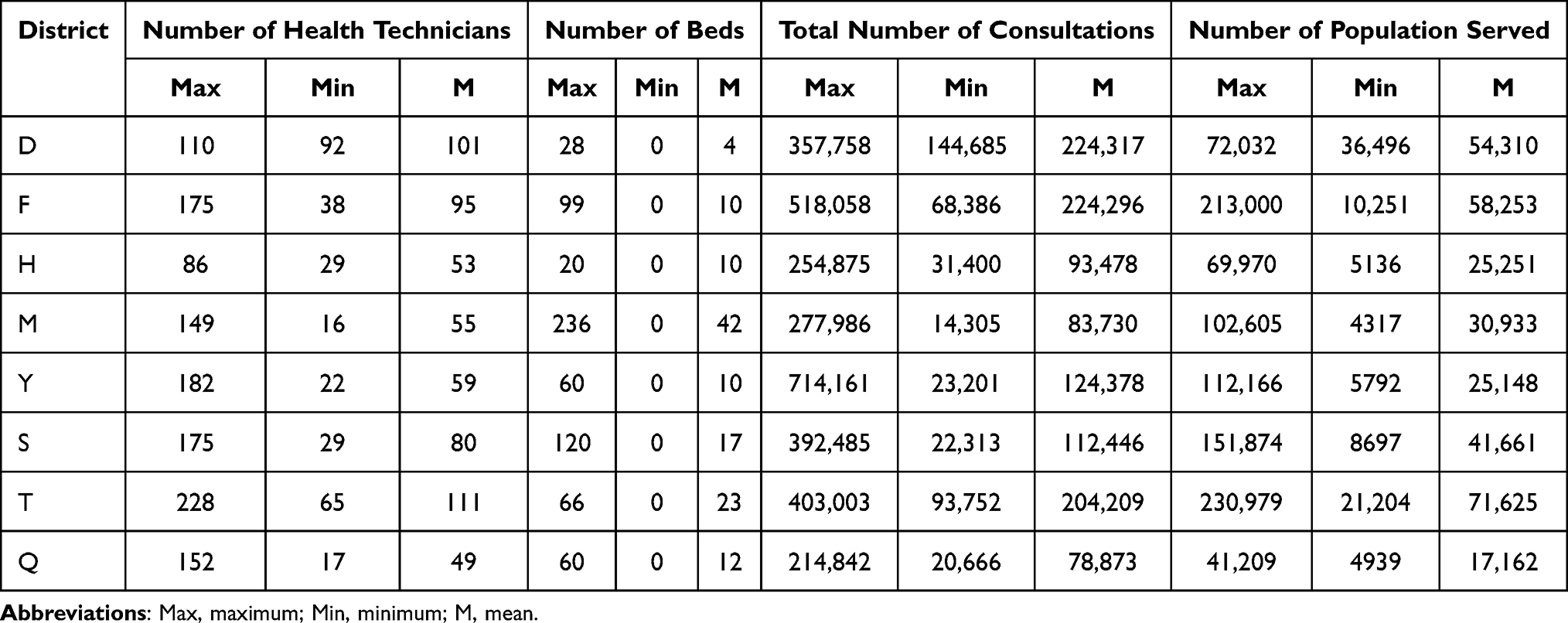 |
Table 2 Basic Information of Community Health Centers |
Principal Component Analysis of the Evaluation of the Medical Alliance Implementation Effect
The results of the principal component analysis showed a KMO value of 0.865 (P<0.001), indicating that the data were suitable for principal component analysis. One principal component was formed, with an eigenvalue of 3.607 and a percentage of cumulative variance of 90.17%. The factor loadings of referral work, training and support work, scientific research cooperation, and information construction were 0.939, 0.956, 0.950 and 0.953, respectively. The final weights of referral work index, training and support work index, scientific research cooperation index, and information construction index were 0.247, 0.252, 0.250, and 0.251, respectively (Table 3).
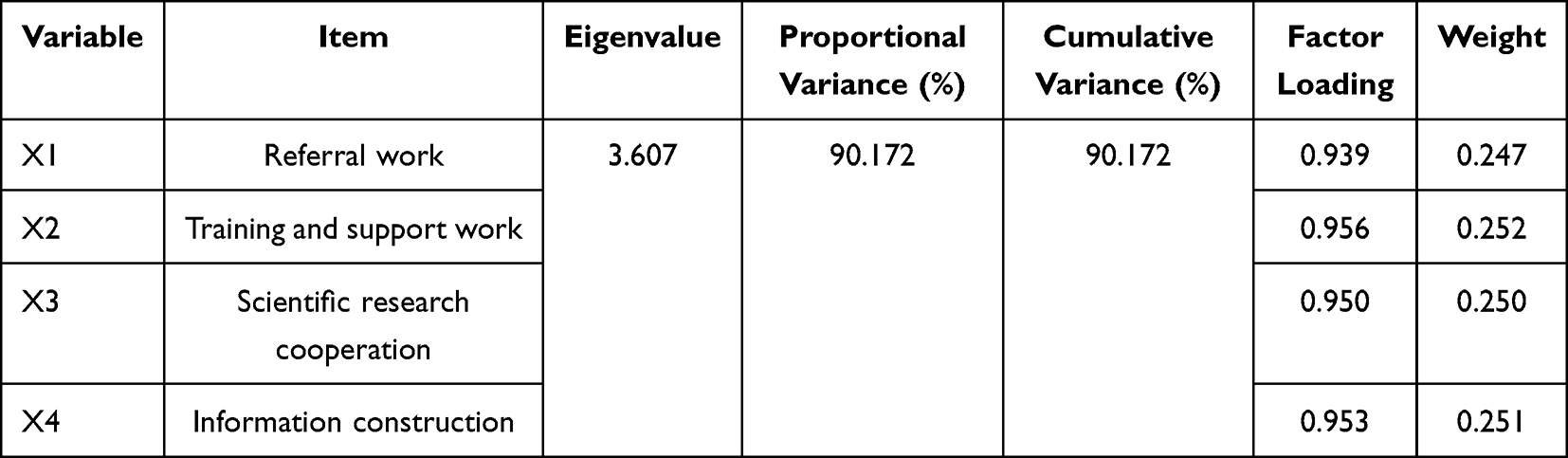 |
Table 3 Principal Component Analysis of Evaluation of Medical Alliance Implementation Effect |
Correlation Analysis of Organizational Performance, Organizational Capabilities and the Medical Alliance Implementation Effect
The average organizational performance score of the 135 CHCs was 72.156 ± 7.035. The average development capabilities score was 4.192±0.398. The average core capabilities score was 4.306±0.380. The average basic capabilities score was 4.166±0.348. The average score of the medical alliance implementation effect was 3.775±0.334. The results of the correlation analysis showed that organizational performance and basic capabilities were positively correlated with the medical alliance implementation effect. Development capabilities were positively correlated with core capabilities, basic capabilities, and the medical alliance implementation effect. Core capabilities were positively correlated with basic capabilities and the medical alliance implementation effect. Basic capabilities and the medical alliance implementation effect were positively correlated (Table 4).
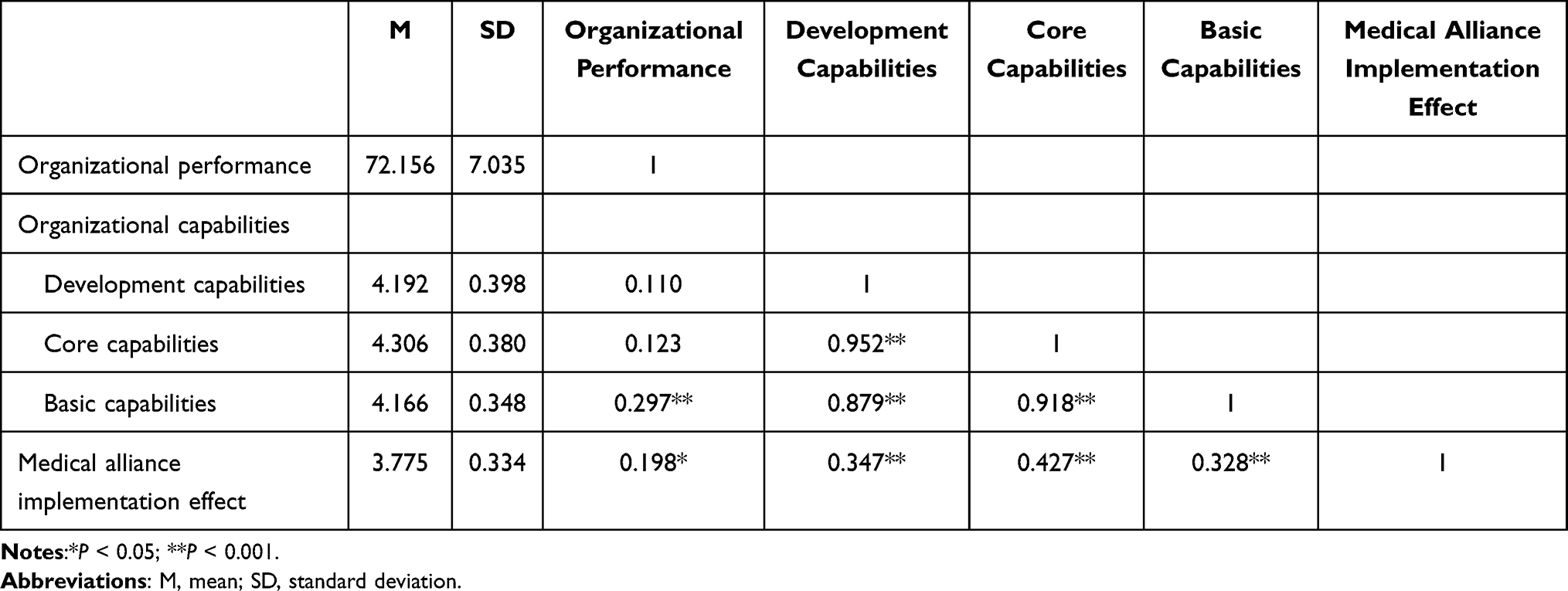 |
Table 4 Correlation Analysis of Variables |
Path Analysis Result
The model was corrected by MI values, and the results of the model showed that RMSEA=0.097, SRMR=0.050, CFI=0.971, and TLI=0.963, indicating that the model fit was relatively good. There was a significant positive effect of basic capabilities on organizational performance (β=1.163, P< 0.001), and the second half of the path of the mediation model held. There was a significant positive effect of development capabilities on basic capabilities (β=0.878, P<0.001), and the first half of the path of the mediation model held, indicating that there may be a mediating effect of basic capabilities. There was a significant negative effect of core capabilities on organizational performance (β=−0.886, P<0.05), the second half of the path of the mediation model held, and there was a significant positive effect of development capabilities on core capabilities (β=0.952, P<0.001), indicating that there may be a mediating effect of core capabilities. However, development capabilities had no direct effect on organizational performance. The basic capabilities×medical alliance implementation effect, core capabilities×medical alliance implementation effect, and development capabilities×medical alliance implementation effect interactions did not have a significant effect on organizational performance, indicating that the medical alliance implementation effect may not play a moderating role.
According to the results, the mediating effect of basic capabilities was significant (β=1.022, 95% CI [0.606, 1.413]) and positively affected organizational performance. The mediating effect of core capabilities was significant (β=−0.843, 95% CI [−1.388, −0.237]) and negatively affected organizational performance. When the medical alliance implementation effect score was low, the mediating effects of basic capabilities and core capabilities were significant. When the medical alliance implementation effect score was high, the mediating effect of basic capabilities was significant, while that of core capabilities was not. However, the difference between the mediating effects of basic and core capabilities when the medical alliance implementation effect scores were taken as high and low values, respectively, was not significant, indicating that the medical alliance implementation effect did not play a moderating role. The absolute value of the mediating effect of basic capabilities was greater than that of the mediating effect of core capabilities, and the difference between the two mediating effects was statistically significant, indicating that the mediating effect of basic capabilities was significantly higher than the mediating effect of core capabilities (Table 5 and Figure 2).
 |
Table 5 Path Analysis Results |
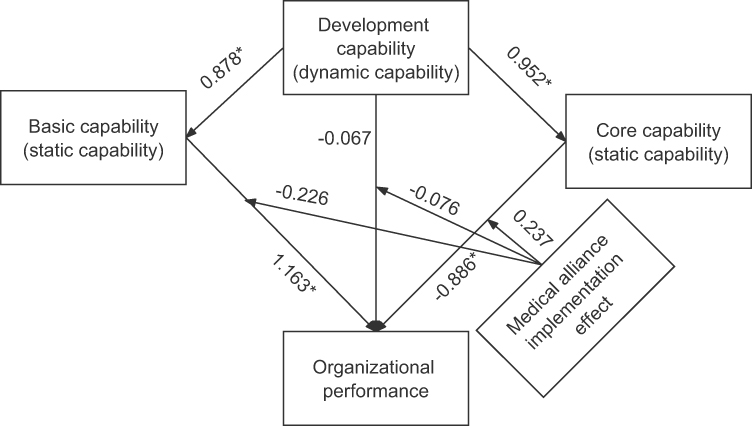 |
Figure 2 Results of the model. Notes: The coefficients on the path were standardized coefficients; *P < 0.05. |
Discussion
This study divided organizational capabilities into basic, core, and development capabilities, introduced the medical alliance implementation effect, proposed research hypothesizes based on organizational capability theory and the dual process model of organizational capabilities, and explores the impact of organizational capabilities on organizational performance and whether the medical alliance implementation effect plays a moderating role. The results showed that the development capabilities of CHCs could not directly influence organizational performance but had an impact on organizational performance through the mediating role of basic and core capabilities, which was a fully mediated model. The mediating role of basic capabilities positively affected organizational performance, the mediating role of core capabilities negatively affected organizational performance, and the mediating role of basic capabilities was significantly stronger than the mediating role of core capabilities. The moderating effect of the medical alliance implementation effect in the process by which organizational capabilities affects organizational performance was not significant, indicating that the role of organizational capabilities on organizational performance was not affected by the medical alliance implementation effect. This study provided new ideas for countries to improve the organizational performance of CHCs.
The strong development capabilities of CHCs can enable organizations to optimize internal and external resources and occupy a dominant position in the future. Organizations with good teamwork and culture-building skills are the basis for a strong development capabilities. Strengthening the culture building of CHCs helps improve their basic medical service capabilities, and outstanding teamwork capabilities are conducive to better development of family doctor contracting services.46,47 Learning capabilities are one of the important dimensions of development capabilities. Lu also classified the learning capabilities of primary health care institutions as a dynamic capabilities and proved that the learning capabilities of primary health care institutions have a positive impact on service volume.48 The basic capabilities of CHCs includes medical services, public health services, and resource allocation capabilities. The improvement of development capabilities contributes to the improvement of medical services, proving that development capabilities positively influence basic capabilities. The medical service level is an important embodiment and key assessment dimension of the organizational performance of medical institutions, which could have a positive impact on the organizational performance of CHCs.49,50 For CHCs, having good public health services is also an effective way to improve organizational performance.51 The findings of this study are similar to those of Kim52 and Mabuchi,21 who found that the capability to allocate human and physical resources in CHCs was able to positively influence organizational performance, probably because human and physical resources are the basis for the provision of healthcare services. In summary, CHCs with strong development capabilities can promote their serviceability and resource allocation ability to have a positive impact on organizational performance.
Organizations has a good culture and teamwork atmosphere and contribute to the development of systems and the implementation of decisions. Positioning capabilities are an important dimension of development capabilities. An organization with strong positioning capabilities can set scientific and realistic development goals after fully analyzing the internal and external environment, which lays the foundation for the efficient management of the organization; thus, the development capabilities of the CHCs may positively influence their core capabilities. The results of this study differ from those of the Desta study, which showed a positive effect of management capabilities on the performance of primary health care institutions.24 The reason for this difference may be because the core capabilities of CHCs are a reflection of internal integrated management capabilities. China pays more attention to the management capabilities of tertiary hospitals but not enough attention to the management capabilities of CHCs, which may be related to the functional positioning of CHCs mainly to provide basic medical services for residents and the relatively simple institutional setup and operation management. Complex management may also reduce the operational efficiency of organizations and thus affect performance.53,54 Managers who devote more energy to management work may compromise their own work in the health service, thus affecting organizational performance. Therefore, the results of this study suggest that the mediating role of core capabilities negatively affects organizational performance, but the relationship between these two needs further validation. The mediating roles of basic capabilities and core capabilities have opposite effects on organizational performance, but the mediating role of basic capabilities is stronger than the mediating role of core capabilities, so organizational capabilities can positively affect organizational performance. This is in line with Cui’s findings that strengthening organizational capabilities is one of the important paths to enhance organizational performance.55
The results of this study showed that the medical alliance implementation effect did not play a moderating role in the process by which organizational capabilities affect organizational performance. This indicates that the medical alliance implementation effect in China has no significant impact on the performance of CHCs. The results of this study are similar to those from China, where the Sun’s study showed that the impact of medical alliance implementation on residents’ choice of medical care has yet to be improved, and the effect of medical cost control was not significant.56 Feng’s study showed that China’s medical alliances were developing rapidly, but their impact on the performance of CHCs was not obvious.57 The medical alliance is a complex system, and the development of a CHC is influenced by the core hospitals within the medical alliances as well as by the external environment, requiring significant management effort to promote the sustainable development of collaboration between institutions.58 However, since the types of medical alliances in China are mostly loosely defined and since unified management of human and financial resources has not been achieved, the overall effect of the operation of medical alliances may be poor.59 At the same time, due to the lack of unified interests among the subjects within medical alliances, they may choose to compete with each other due to conflicting interests or changes in the external environment.60 The establishment of close medical alliances is an effective way to improve the medical alliance implementation effect. Related studies have shown that the close medical alliances leads to significant improvements in patient satisfaction, two-way referrals, training and support effects, research collaboration, and information technology in CHCs.39,61–63 Therefore, the government should form a mechanism to guarantee the sustainable development of medical alliances and promote the development of medical alliances with close collaboration. So as to effectively realize the sinking of quality medical resources and improve the service performance of CHCs.
Strengths and Limitations
The empirical results of this study fill a gap in the international literature on the role of organizational capabilities on organizational performance in CHCs and provide new ideas for improving the performance of CHCs in other countries. However, there are some limitations to this study, firstly the study was conducted on 135 CHCs, which was a relatively small sample size. In this study, medical staff and managers were selected as the questionnaire respondents, the questionnaire respondents of organizational capabilities evaluation were 1957, and the questionnaire respondents of implementation effect evaluation of medical alliance were 3622, which was representative to a certain extent. The bootstrap method was also used to sample 1000 times for model simulation, which made the results more stable. Second, the organizational capabilities of CHCs and the medical alliance implementation effect were subjectively evaluated by CHC managers and medical staff and therefore lack objectivity. Finally, as the study population was from Beijing, China, which is relatively rich in healthcare resources and has relatively well-developed CHCs, the generalization of the results of this study is limited and is more applicable to countries with a similar health system to that of China. In future studies, more CHCs in representative districts can be selected for the survey to increase the number of subjects and to prove the robustness of the results of this study so that the findings can be widely disseminated. The evaluation of the organizational capabilities of the CHCs and medical alliance implementation effect can also be validated through objective data from the CHCs to ensure the accuracy of the evaluation results.
Conclusion
This study investigated the relationship between organizational capabilities and organizational performance in CHCs based on the dual process model of organizational capabilities. The study found that the development capabilities of CHCs have an impact on organizational performance through the mediation of basic and core capabilities, while development capabilities cannot act directly on organizational performance. However, the medical alliance implementation effect did not play a moderating role in the relationship between organizational capabilities and organizational performance in CHCs. The empirical results of this study provide new ideas for other countries to improve the performance of CHCs. Strengthening the organizational capabilities of CHCs can effectively improve their performance, with the development of basic capabilities being the primary concern. The role of core capabilities and the medical alliance implementation effect on organizational performance need to be further validated by more research.
Abbreviations
CHCs, community health centers; Max, maximum; Min, minimum; M, mean; SD, standard deviation; 95% CI; 95% confidence interval.
Data Sharing Statement
The datasets obtained and analyzed during the current study are available from the corresponding author on reasonable request. Email: [email protected].
Ethics Approval and Informed Consents
This study is based on a research study approved by the ethics committee of Capital Medical University (NO. Z2021SY011). The study was performed in accordance with the Declaration of Helsinki. Informed written consent was obtained from all the participants before the start of this study. By completing a consent form, the participants were informed about the purpose and method of the study. The participants were also informed that the researchers were committed to answering their questions and that their information would be kept confidential.
Consent for Publication
The details in present study can be published, and that the persons providing consent have been shown the article contents to be published.
Acknowledgments
The authors thank all the people who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (72274128). The funders had no role in any aspects of this study, including the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lahariya C. Health & wellness centers to strengthen primary health care in India: concept, progress and ways forward. Indian J Pediatr. 2020;87(11):916–929. doi:10.1007/s12098-020-03359-z
2. Da LPA, Ramalho A, Viana J, et al. The effect of commissioning on Portuguese Primary Health Care units’ performance: a four-year national analysis. Health Policy. 2021;125(6):709–716. doi:10.1016/j.healthpol.2021.02.008
3. Addi B, Doe B, Oduro-Ofori E. Towards quality primary health care: the dilemma of Community-Based Health Planning and Services (CHPS) in health service provision in Ghana. J Health Organ Manag. 2021. doi:10.1108/JHOM-06-2021-0219
4. Subba SH, Pradhan SK, Sahoo BK. Empowering primary healthcare institutions against COVID-19 pandemic: a health system-based approach. J Fam Med Primary Care. 2021;10(2):589–594. doi:10.4103/jfmpc.jfmpc_1416_20
5. Hoa NT, Derese A, Markuns JF, Tam NM, Peersman W. Development and validation of the Vietnamese Primary Care Assessment Tool - provider version. Prim Health Care Res Dev. 2019;20:e86. doi:10.1017/S1463423619000458
6. Zhang L, Li J, Ma T, et al. Usual source of care and experiences with primary care among community health service centre patients in Changchun, China: a cross-sectional survey. Health Soc Care Community. 2020;28(6):1979–1988. doi:10.1111/hsc.13009
7. Lu C, Zhang Z, Lan X. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: a case study of Beijing. Soc Sci Med. 2019;235:112386. doi:10.1016/j.socscimed.2019.112386
8. Dai T, Wang F, Li YB. Effect on primary healthcare comprehensive reform in China. Chin J Health Policy. 2013;6:1–8.
9. Chen Q, Xiao JF, Liu RM, et al. A comparative study of the development of three types of institutions in China’s health care service system from 2009–2019. China Public Health Manag. 2021;37:593–596.
10. Zhang A, Nikoloski Z, Albala SA, et al. Patient choice of health care providers in china: primary care facilities versus hospitals. Health Syst Reform. 2020;6(1):e1846844. doi:10.1080/23288604.2020.1846844
11. Qin C, Liu M, Guo X, et al. Human resources in primary health-care institutions before and after the new health-care reform in China from 2003 to 2019: an interrupted time series analysis. Int J Environ Res Public Health. 2022;19(10):6042. doi:10.3390/ijerph19106042
12. Tan J, Wang X, Pan J. The effect of population distribution measures on evaluating spatial accessibility of primary health-care institutions: a case study from China. Geospat Health. 2021;16(1). doi:10.4081/gh.2021.936
13. Siqueri CAS, Pereira GA, Sumida GT, et al. What are the implications of problem-solving capacity at Primary Health Care in older adult health? Einstein. 2022;20:eGS6791. doi:10.31744/einstein_journal/2022GS6791
14. Perialathan K, Johari MZ, Jaafar N, et al. Enhanced primary health care intervention: perceived sustainability and challenges among implementers. J Prim Care Community Health. 2022;12:21501327211014096.
15. Barbazza E, Kringos D, Kruse I, et al. Creating performance intelligence for primary health care strengthening in Europe. BMC Health Serv Res. 2019;19(1):1006. doi:10.1186/s12913-019-4853-z
16. Senn N, Breton M, Ebert ST, Lamoureux-Lamarche C, Lévesque JF. Assessing primary care organization and performance: literature synthesis and proposition of a consolidated framework. Health Policy. 2021;125(2):160–167. doi:10.1016/j.healthpol.2020.10.004
17. Al Rashidi B, Al Wahaibi AH, Mahomed O, et al. Assessment of key performance indicators of the primary health care in Oman: a cross-sectional observational study. J Prim Care Community Health. 2020;11:2150132720946953.
18. Barbazza E, Allin S, Byrnes M, et al. The current and potential uses of Electronic Medical Record (EMR) data for primary health care performance measurement in the Canadian context: a qualitative analysis. BMC Health Serv Res. 2021;21(1):820. doi:10.1186/s12913-021-06851-0
19. Rashidian A, Jahanmehr N, Farzadfar F, et al. Performance evaluation and ranking of regional primary health care and public health systems in Iran. BMC Health Serv Res. 2021;21(1):1168. doi:10.1186/s12913-021-07092-x
20. Tenbensel T, Burau V. Contrasting approaches to primary care performance governance in Denmark and New Zealand. Health Policy. 2017;121(8):853–861. doi:10.1016/j.healthpol.2017.05.013
21. Mabuchi S, Sesan T, Bennett SC. Pathways to high and low performance: factors differentiating primary care facilities under performance-based financing in Nigeria. Health Policy Plan. 2018;33(1):41–58. doi:10.1093/heapol/czx146
22. Sitienei J, Manderso L, Nangami M, Gholipour K. Community participation in the collaborative governance of primary health care facilities, Uasin Gishu County, Kenya. PLoS One. 2021;16(3):e0248914. doi:10.1371/journal.pone.0248914
23. Flores JSE, San SM. Assessing the impact of the 2008 health reform in Ecuador on the performance of primary health care services: an interrupted time series analysis. Int J Equity Health. 2021;20(1):169. doi:10.1186/s12939-021-01495-2
24. Desta BF, Abitew A, Beshir IA, et al. Leadership, governance and management for improving district capacity and performance: the case of USAID transform: primary health care. BMC Fam Pract. 2021;21(1):252. doi:10.1186/s12875-020-01337-0
25. Aziz SZ, Hanif I. Primary care and health system performance in Pakistan: a study of basic health units of South Punjab. J Pak Med Assoc. 2016;66:1632–1636.
26. Cui C, Meng K. Development of an index system for evaluating the organisational capabilities of primary medical institutions: a modified Delphi study in China. BMJ open. 2021;11(12):e055422. doi:10.1136/bmjopen-2021-055422
27. Li Y, Si YH. The impact of knowledge management strategies on organizational effectiveness. J Intell. 2010;29:42–47.
28. Ke X, Jin X. Empirical evidence of enterprise organizational capability system evaluation. Bus Manag. 2011;08:91–94.
29. E B. A resource-based view of the firm. Strategic Manag J. 1984;5:171–180.
30. Teece DJ, Pisano G, Shuen A. Dynamic capabilities and strategic management. Strategic Manag J. 1997;18(18):509–533. doi:10.1002/(SICI)1097-0266(199708)18:7<509::AID-SMJ882>3.0.CO;2-Z
31. Graeme C, Roger D. Competence-based management development: rhetoric and reality. J Eur Industr Train. 1995;5:11–18.
32. Barney J. Firm Resources and Sustained Competitive Advantage. J Manage. 1997;17:99–120.
33. Barney JB. Looking inside for competitive advantage. Acad Manag Execut. 1995;9:49–61.
34. Schreyögg G. How dynamic can organizational capabilities be? Towards a dual‐process model of capability dynamization. Strategic Manag J. 2007;1:15–24.
35. Zott C, Strategic S, Journal M, et al. Dynamic capabilities and the emergence of intraindustry differential firm performance: insights from a simulation study. Strategic Manag J. 2003;24(24):97–125. doi:10.1002/smj.288
36. Xiong ZJ, Zhang W, Du SQ. Study on the implementation status and effect of the “medical association” model under the tiered diagnosis and treatment system. China Health Manag. 2020;37:248–251.
37. Yang F, Yang Y, Liao Z. Evaluation and analysis for Chinese Medical Alliance’s Governance Structure Modes based on Preker-Harding Model. Int J Integr Care. 2020;20(4):14. doi:10.5334/ijic.5417
38. He XR, Sun XT, Gong FF, et al. A comprehensive evaluation of the effect of human resource management reform within a tight-knit medical association. Mod Hosp Manag. 2022;20:66–69.
39. Xiong X, Zhou S, Huo Z, et al. GIS-based method to delimit spheres of influence for a medical consortium: experience of a pediatric medical consortium, Shanghai. Int J Health Plann Manage. 2022;34(1):294–308. doi:10.1002/hpm.2630
40. Wang Y, Xiang L, Chen J, et al. The downward referral experiences of stroke caregivers in the regional medical alliance in China: a phenomenological study. Medicine. 2022;101(42):e31151. doi:10.1097/MD.0000000000031151
41. Wu RM, Zhang ZW, Yan WJ, et al. A comparative analysis of the principal component analysis and entropy weight methods to establish the indexing measurement. PLoS One. 2022;17(1):e0262261. doi:10.1371/journal.pone.0262261
42. Ziarh GF, Asaduzzaman M, Dewan A, Nashwan MS, Shahid S. Integration of catastrophe and entropy theories for flood risk mapping in peninsular Malaysia. J Flood Risk Manag. 2021;14(1):1–13. doi:10.1111/jfr3.12686
43. Mukhametzyanov I. Specific character of objective methods for determining weights of criteria in MCDM problems: entropy, CRITIC and SD. Decis Making Apps Manag Engineering. 2021;4:76–105.
44. Conlon KC, Mallen E, Gronlund CJ, Berrocal VJ, Larsen L, O’Neill MS. Mapping human vulnerability to extreme heat: a critical assessment of heat vulnerability indices created using principal components analysis. Environ Health Perspect. 2020;128(9):97001. doi:10.1289/EHP4030
45. Mei YH, Zhou GY, Li Z, et al. Factors influencing clinical pharmacist service satisfaction from the perspective of inpatients - based on factor analysis and multiple linear regression analysis. Pharmacopoeia. 2022;2022:1–8.
46. Cai LQ, Sheng Q, Gong SH. Analysis of the problems and countermeasures of family doctor contract service teams using the team effectiveness model. China Primary Health Care. 2020;34:23–26.
47. LiX Q. Reflections on the cultural construction of primary hospitals. Public Relat World. 2022;14:13–14.
48. Lu S. A conceptual model of dynamic capacity of primary health care institutions and the mechanism of interaction with resources and service output [dissertation]. Wu Han: Huazhong University of Science and Technology; 2020.
49. Xiong X, Gao J, Zhang B, et al. Introduction of Chinese hospital ranking method from the aspect of theoretical framework, practical choice and social effect. J Hosp Manag Health Policy. 2017;1:4–400. doi:10.21037/jhmhp.2017.11.01
50. Dong S, Millar R, Shi C, et al. Rating hospital performance in China: review of publicly available measures and development of a ranking system. J Med Internet Res. 2021;23(6):e17095. doi:10.2196/17095
51. Yuan L, Ding ZF. A comparative analysis of performance appraisal indicators in China’s public health care institutions. Chin J Hosp Manag. 2021;37:534–537.
52. Kim JH, Bell GA, Bitton A, et al. Health facility management and primary health care performance in Uganda. BMC Health Serv Res. 2022;22(1):275. doi:10.1186/s12913-022-07674-3
53. Xiong HL. Accelerating the construction of information technology to achieve high efficiency and quality development of hospital economic management. Bohai Econ Outlook. 2021;4:105–106.
54. Han J. Hospital strategic planning and budget management practices. Finance Econ. 2019;26:70–71.
55. Cui CS, Zhuang N, Meng K. A study on the path of organizational performance improvement of primary health care institutions in Beijing based on system dynamics. China Pharmaceutical Herald. 2022;19:173–179.
56. Sun W, Zhu H, Zhang L, et al. Do medical alliances truly work? Perspectives on health service utilisation among outpatients with chronic diseases in Shanghai. China Aust J Primary Health. 2023;29(4):332–340. doi:10.1071/PY22115
57. Feng C, Zhu J, Chen Y. The evolution and inter-sectoral interaction mechanism of China’s national medical alliance: an analysis based on complex systems theory. Int J Health Plann Manage. 2022;37(3):1454–1476. doi:10.1002/hpm.3413
58. Axelsson R, Axelsson SB. Integration and collaboration in public health--a conceptual framework. Int J Health Plann Manage. 2006;21(1):75–88. doi:10.1002/hpm.826
59. Yang ZG, Miao JG. Problems and countermeasures of the operation of medical association. Chin Hosp Director. 2021;17:56–59.
60. Edgren L. The meaning of integrated care: a systems approach. Int J Integr Care. 2008;8(5):e68. doi:10.5334/ijic.293
61. Chen YL, He WT, Liu Z, et al. Practice and effectiveness of the “hospital-based” service model in a tightly-knit medical association: the example of West China Hospital of Sichuan University. Mod Prevent Med. 2020;47:1032–1034.
62. Liang T, Liao C, Wei S. Comparison and analysis of the application of loose and close medical association management models. Chin J Health Inform Manag. 2019;16:370–374.
63. Zhang H, Wu Y, Sun W, et al. How does people-centered integrated care in medical alliance in China promote the continuity of healthcare for internal migrants: the moderating role of respect. Front Public Health. 2023;10:1030323. doi:10.3389/fpubh.2022.1030323
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.