Back to Journals » Clinical Interventions in Aging » Volume 21
Associations Among Oral Health, Nutritional Status, and Care Dependency in Korean Long-Term Care Facilities
Authors Kim HN ![]() , Park H
, Park H ![]() , Cha JM
, Cha JM ![]() , Lim J, Suh H, Jung H
, Lim J, Suh H, Jung H ![]() , Lim HS
, Lim HS
Received 10 August 2025
Accepted for publication 13 January 2026
Published 6 February 2026 Volume 2026:21 559701
DOI https://doi.org/10.2147/CIA.S559701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Ha-Neul Kim,1 Hansol Park,1 Ji-Min Cha,1 Jijun Lim,2 Hyewon Suh,2 Hoiin Jung,3 Hee-Sook Lim1
1Department of Gerontology, AgeTech-Service Convergence Major, Graduate School of East-West Medical Science, Kyung Hee University, Yongin, Republic of Korea; 2Special Care Dental Hospital, Seoul, Republic of Korea; 3Department of Preventive Dentistry & Public Oral Health, Yonsei University College of Dentistry, Seoul, Republic of Korea
Correspondence: Hee-Sook Lim, Department of Gerontology, AgeTech-Service Convergence Major, Graduate School of East-West Medical Science, Kyung Hee University, Yongin, Republic of Korea, Tel +82-31-201-2936, Email [email protected]
Background: Korea’s population is aging rapidly, yet the oral health and nutritional status of long-term care facility residents remain limited in terms of systematic management and research, despite its importance to quality of life.
Purpose: This study aimed to compare the oral health and nutritional status of older adults in Long-Term Care Facilities (LTCFs) according to their Long-Term Care (LTC) grades and to examine the interrelationship between these two factors.
Methodology: A cross-sectional study was conducted among 180 older adults aged 65 years or older residing in two public long-term care facilities in Korea. Participants were classified into an institution-based benefits group (Grades 1– 2) and a home-based benefits group (Grades 3– 5) according to their Long-Term Care (LTC) grades. Oral health status, including oral hygiene management, chewing ability, and oral dryness, and nutritional status, assessed using the Mini Nutritional Assessment (MNA), were evaluated. Multiple linear regression analysis was conducted to identify oral health factors affecting MNA scores.
Results: The institution-based group showed significantly poorer physical function, oral hygiene behavior, chewing ability, and nutritional status compared to the home-based group. Malnutrition was observed in 73.9% of the institution-based group versus 26.9% in the home-based group (p< 0.001). Regression analysis identified significant predictors of nutritional status: oral dryness (p< 0.001), chewing ability (p=0.001), oral care dependency (p=0.024), plaque or calculus (p=0.025), and food debris (p=0.016).
Conclusion: Oral health significantly impacts nutritional status among older adults in LTCFs. Those with higher LTC grades are at greater risk of both oral and nutritional deterioration. These findings highlight the urgent need for integrated, multidisciplinary care approaches addressing oral health and nutrition concurrently in LTC settings.
Keywords: aged, long-term care, oral health, nutritional status, interprofessional relations
Introduction
Population aging is recognized as a critical global issue, and Korea is among the Organization for Economic Co-operation and Development (OECD) countries experiencing the most rapid progression toward an aged society.1 According to Statistics Korea (2024), the proportion of the population aged 65 years and above will account for 19.2% of the total population, and this figure is projected to increase continuously, surpassing 30% by 2036 and 40% by 2050.2 This rapid aging has led to an increased economic and psychosocial burden on older adults and their caregivers, which has emerged as a major social concern. To address these challenges, Korea introduced the Long-Term Care Insurance (LTCI) system in 2008.3 The LTCI aims to provide physical and household support to older adults, ultimately improving their quality of life.4
The LTCI targets individuals aged 65 years and above or those under 65 years who experience significant difficulty performing activities of daily living for at least six months due to chronic diseases or disabilities.4 Eligibility for benefits is determined by assessing an individual’s physical and cognitive impairment levels according to standardized procedures.3 The LTCI benefits encompass institutional services such as Long-Term Care Facilities (LTCFs) and community-based services, including daily living support at home. The specific type and amount of support provided depends on the level of physical and cognitive impairment.3 However, despite the introduction of new care services for older adults, the LTCI has primarily focused on providing social support, raising concerns that it does not adequately address beneficiaries’ healthcare needs.5 Older adults with a high level of care dependency often experience difficulties in maintaining oral hygiene or adequate food intake due to functional and cognitive decline, leading to deterioration in both oral health and nutritional status.6 Such deterioration may further accelerate physical decline, thereby increasing care dependency and creating a potentially destructive cycle.7
Indeed, older adults utilizing LTCFs continue to exhibit poor oral health and nutritional status, resulting in persistent health deterioration and diminished quality of life.8–12 Several studies have indicated that oral health extends beyond dental status; tooth loss, impaired chewing ability, and oral pain restrict food intake, leading to an insufficient intake of essential nutrients. Consequently, this results in poor nutritional status, reduced immunity, and increased risk of chronic diseases.13–15
Although the significance of the association between oral health and nutritional status has been consistently highlighted, previous studies have predominantly focused on individual components, such as natural tooth retention, denture use, and oral dryness, as oral health indicators.16,17 Conversely, while some studies have suggested the necessity of analyzing the impact of oral health on nutritional status from a multidisciplinary perspective, incorporating factors such as dementia severity and Long-Term Care (LTC) Grade, comprehensive assessments encompassing these dimensions are limited.18–20
Oral health management is increasingly being recognized as an essential factor in enabling older adults to maintain adequate dietary intake and manage their overall health and quality of life.21 There is a growing need to develop integrated and comprehensive care systems that reflect these considerations.22 However, these integrated systems have not been sufficiently implemented in Korean LTCFs. Therefore, this study aimed to investigate the differences in oral health and nutritional status according to LTC Grades among older adults utilizing LTCFs and comprehensively examine the association between these two variables.
Materials and Methods
Study Design and Participants
This cross-sectional study was conducted from January to July 2025, and older adults were recruited from two municipal LTCFs located in Seoul and Gyeonggi, Korea. These facilities had formally expressed their willingness to participate and were accessible to the research team. In order to ensure consistency and reliability in data collection, the survey was conducted exclusively at these two facilities. An a priori power analysis for multiple regression was conducted using G*Power 3.1. Assuming a medium effect size (f2=0.15), a statistical power of 0.80, and 12 predictors, the minimum required sample size was calculated to be 127 participants. In order to account for an anticipated attrition rate approximately 20%, the target sample size was established at approximately 160 participants. Consequently, all subjects within the selected facilities who met the inclusion criteria were invited to participate, and no random sampling procedure was applied. Participants were individuals aged 65 years or older who had been assessed and classified into LTC Grades by the National Health Insurance Service (NHIS) and were residing in the selected facilities. A total of 193 eligible participants were recruited. However, five participants dropped out due to health-related issues, and six withdrew consent before the study, resulting in 182 participants. Subsequently, two participants classified as LTC grade 6 were excluded from the analysis, leaving a final analytic sample of 180 participants. All participants or their legal guardians provided written informed consent after receiving detailed explanations of the purpose and procedures of the study. This study was approved by the Institutional Review Board of Kyung Hee University (approval no. KHGIRB-24-660, approved on December 20, 2024).
Classification Criteria of LTC Grade
LTC grades are determined based on criteria established by the National Health Insurance Service (NHIS), using a 52-item assessment that evaluates physical and cognitive functional dependency, behavioral changes, nursing care needs, and rehabilitation requirements. Grades range from 1 (highest level of dependency) to 6 (cognitive support level).4 Individuals classified as Grades 1–2 are eligible for institution-based benefits and may be admitted to long-term care facilities (LTCFs). In contrast, those classified as Grades 3–5 primarily receive home-based benefits, such as services from daycare centers or community-based home care, although some may qualify for institutional care under specific conditions.8 In this study, individuals with Grade 6, who are not eligible for institutional care, were excluded. Accordingly, participants were categorized into two groups: an institution-based benefits group (Grades 1–2) and a home-based benefits group (Grades 3–5).
Sociodemographic Characteristics
The sociodemographic characteristics collected in this study included LTC Grade, age, sex, type of care facility, length of stay, height, weight, mid-arm circumference, calf circumference, body mass index, communication ability, mobility level, sitting ability, and neck mobility. Data was obtained from the most recent facility records or measured and evaluated directly by experienced professionals.
Oral Health Status and Hygiene Management
The oral health status of the participants was assessed using oral examinations performed by a dental specialist experienced in this field. The evaluation items were developed based on international WHO guidelines for conducting standardized oral health surveys.23 Additional items were included to reflect the specific characteristics of older adults residing in LTCFs. As standardized assessment tools for LTCF residents are limited in Korea, dental specialists consulted and adapted the Oral Hygiene Management Manual for Residents of Long-Term Care Insurance Facilities (2019 edition), published by the Japanese Society of Gerodontology, considering the vulnerabilities and limitations of the target population.24 Oral hygiene management and status assessment included toothbrush use (yes / no), denture cleanser use (yes / no / no denture use), frequency of oral hygiene care (less than once / once / twice or more), ability to keep mouth open during oral care (impossible / difficult / possible), dependency level in oral care (completely dependent / requires assistance / independent), mouthwash use (impossible / possible), reasons for inability to use mouthwash (cognitive impairment / dysphagia / aspiration risk / not applicable), severity of halitosis (unpleasant odor beyond 15 cm / unpleasant odor within 15 cm / minimal odor), plaque or calculus level (severe / moderate / minimal), and presence of food debris (moderate / mild / none). Oral and dental health conditions were evaluated based on the number of natural teeth, number of lower and upper functional teeth (including artificial teeth such as dentures or prosthetic crowns), oral dryness status (increased friction, adherence to mucosa / slight friction, no adherence to mucosa / moist, smooth, and lubricated slight friction, no adherence to mucosa), presence of oral soft tissue abnormalities (eg, ulceration, inflammation, or mucosal lesions; present / absent), and the need for dental treatment (yes / no).
Dental Function and Nutritional Status
Participants’ nutritional status was evaluated using the Mini Nutritional Assessment (MNA), a standardized instrument designed to assess the nutritional condition of older adults. Based on MNA scores, participants were categorized into three groups: well-nourished, at risk of malnutrition, and malnourished.25 Dental function was assessed by evaluating participants’ ability to chew foods of varying textures. The evaluation criteria were derived from the Korean Oral Frailty Screening Tool, which classifies foods by hardness into four categories.26
Statistical Analysis
Differences in sociodemographic characteristics, oral health, and nutritional status between the groups were analyzed using independent sample t-tests and chi-squared tests. Continuous variables were expressed as means and standard deviations, and categorical variables as frequencies and percentages. To identify oral health factors associated with nutritional status scores among older adults in LTCFs, multiple linear regression analysis was conducted with the MNA score. All analyses were performed using IBM SPSS Statistics version 28.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at a p-value <0.05.
Results
Differences in Demographic and Functional Status by LTC Grade
Table 1 presents the sociodemographic characteristics of the participants. The mean age was 84.8 years, and 80% were female. Approximately 85% of participants resided in long-term care facilities (LTCFs), with a significantly greater proportion utilizing daycare centers in the home-based benefit group (p=0.005). The mean duration of facility utilization was notably longer in the institution-based group (38.5 months) compared to the home-based group (26.4 months; p=0.005). Mid-arm and calf circumferences were significantly lower in the institution-based group (p=0.001 and p<0.001, respectively). The proportion of underweight individuals was considerably higher in the institution-based group (43.5%) than in the home-based group (16.4%; p<0.001). Communication (p<0.001) and mobility (p=0.002) limitations more frequent in the institution-based group, whereas no significant differences were observed in sitting and neck mobility between the groups.
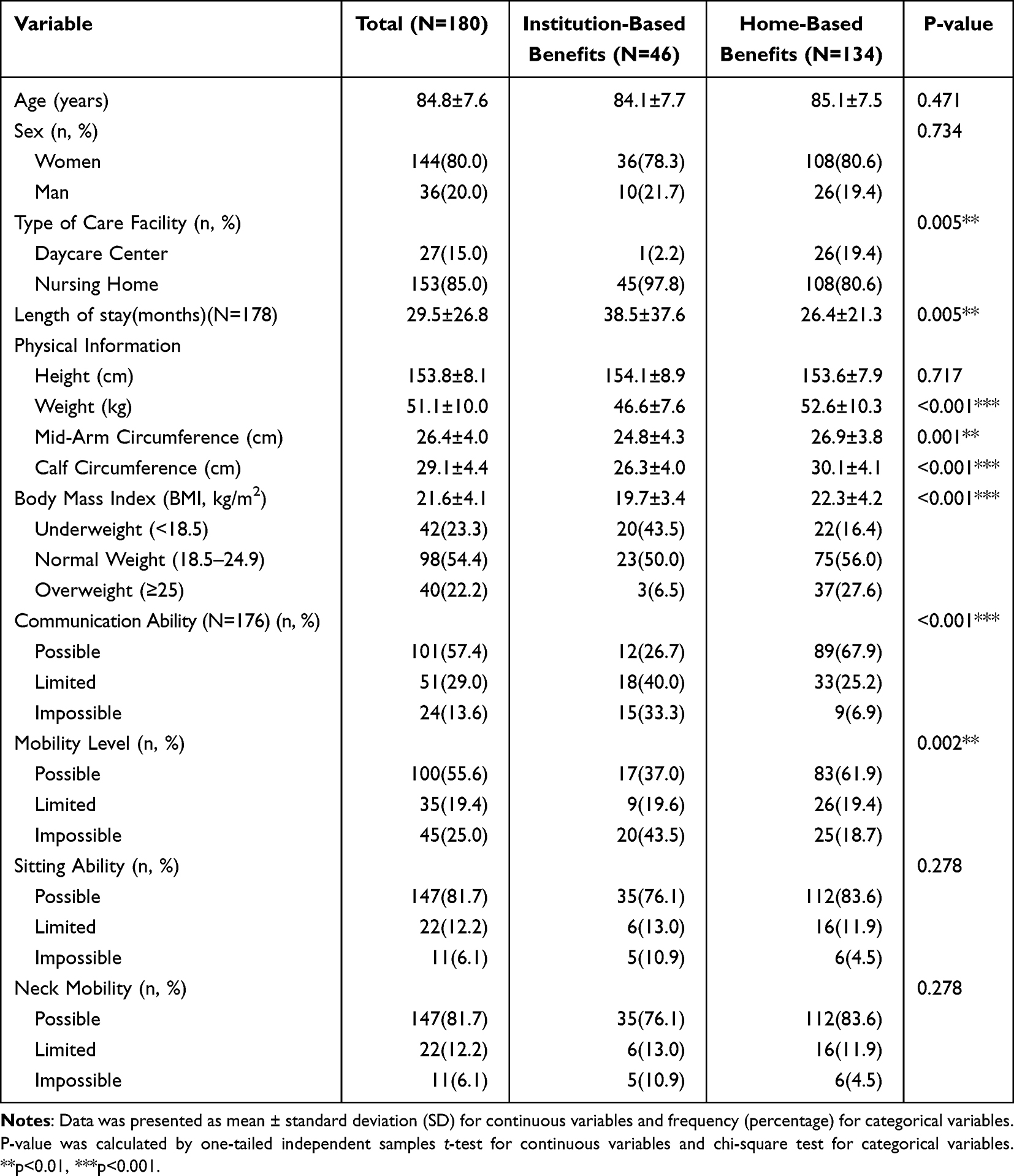 |
Table 1 Sociodemographic Characteristics |
Disparities in Oral Hygiene Practices Between LTC Groups
Oral hygiene management and status of the participants are shown in Table 2. Overall, 94.4% of the participants practiced toothbrushing; however, the institutional-based benefits group included a higher proportion of non-brushers (15.2%) than the home-based benefits group (2.2%; p<0.001). Participants in the institution-based group were shown to have a lower propensity for performing oral hygiene less than twice daily (p=0.031) and an increased frequency of inability to keep their mouths open during oral care (p<0.001). Although 41.3% of the participants in the institution-based benefits group could independently perform oral care, another 41.3% required full assistance from others (p=0.001). Mouthwash use was substantially more restricted in the institution-based group (47.8%; p<0.001), with cognitive impairment, swallowing difficulty, and aspiration risk being common barriers (p<0.001). Although no significant differences were observed in halitosis or plaque levels, food debris was more prevalent in the institution-based group (p=0.004).
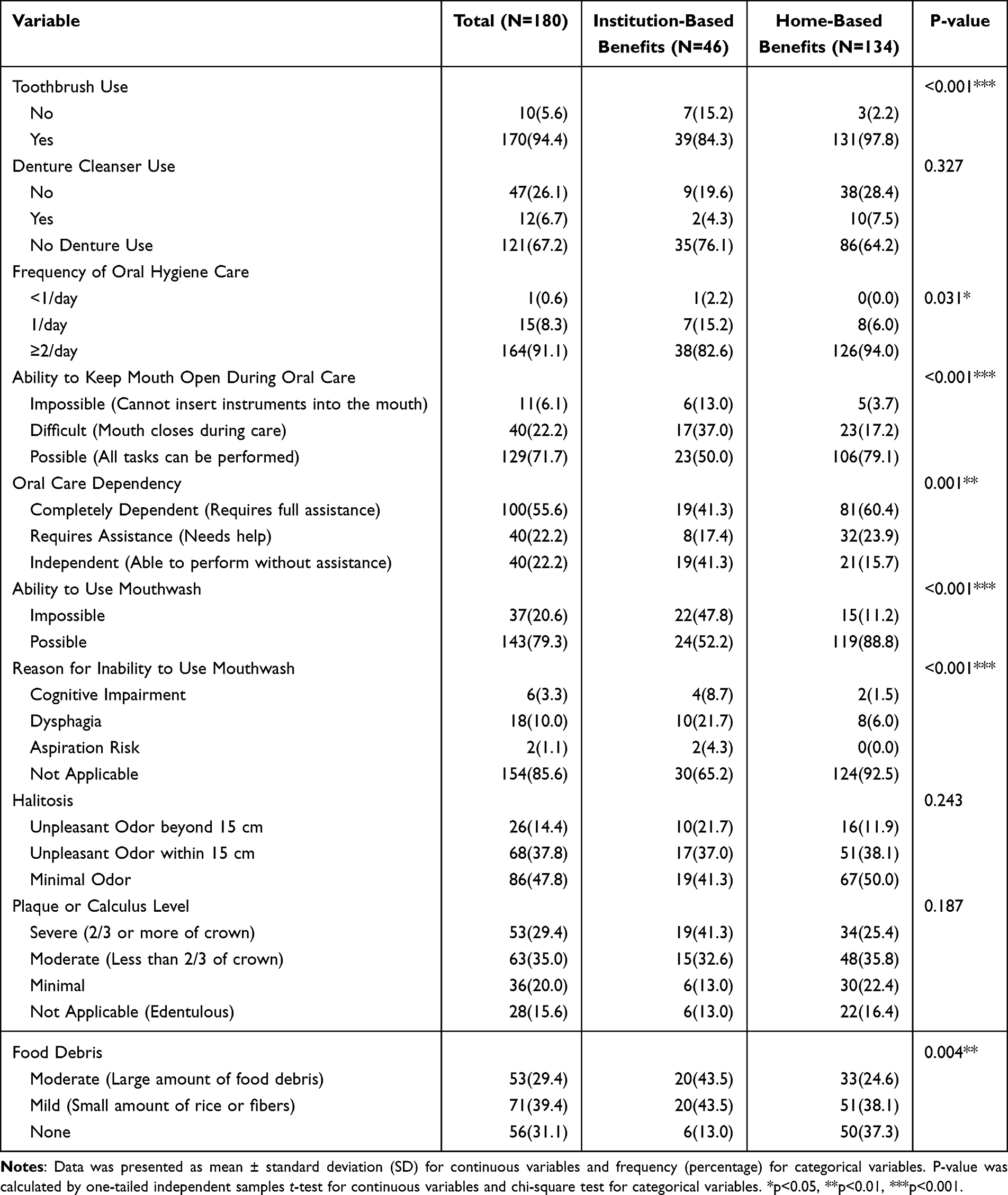 |
Table 2 Oral Hygiene Management and Status |
Comparative Oral Health Conditions and Dental Care Requirements
Table 3 outlines the oral and dental health conditions of the participants. No notable differences were observed between the groups in the number of natural teeth, functional teeth, or incidence of oral dryness, though oral dryness was more common in the institution-based group (32.9% vs 50.7%, p=0.073). A significant disparity was noted in the necessity for dental treatment related to caries, with the institution-based group demonstrating a higher proportion (76.1%) than the home-based group (20.9%; p=0.003). Although other dental treatment needs (extraction, prosthetic treatment, soft tissue care, and scaling) were not to a significant degree different, they were more to a greater degree frequently reported in the institution-based group.
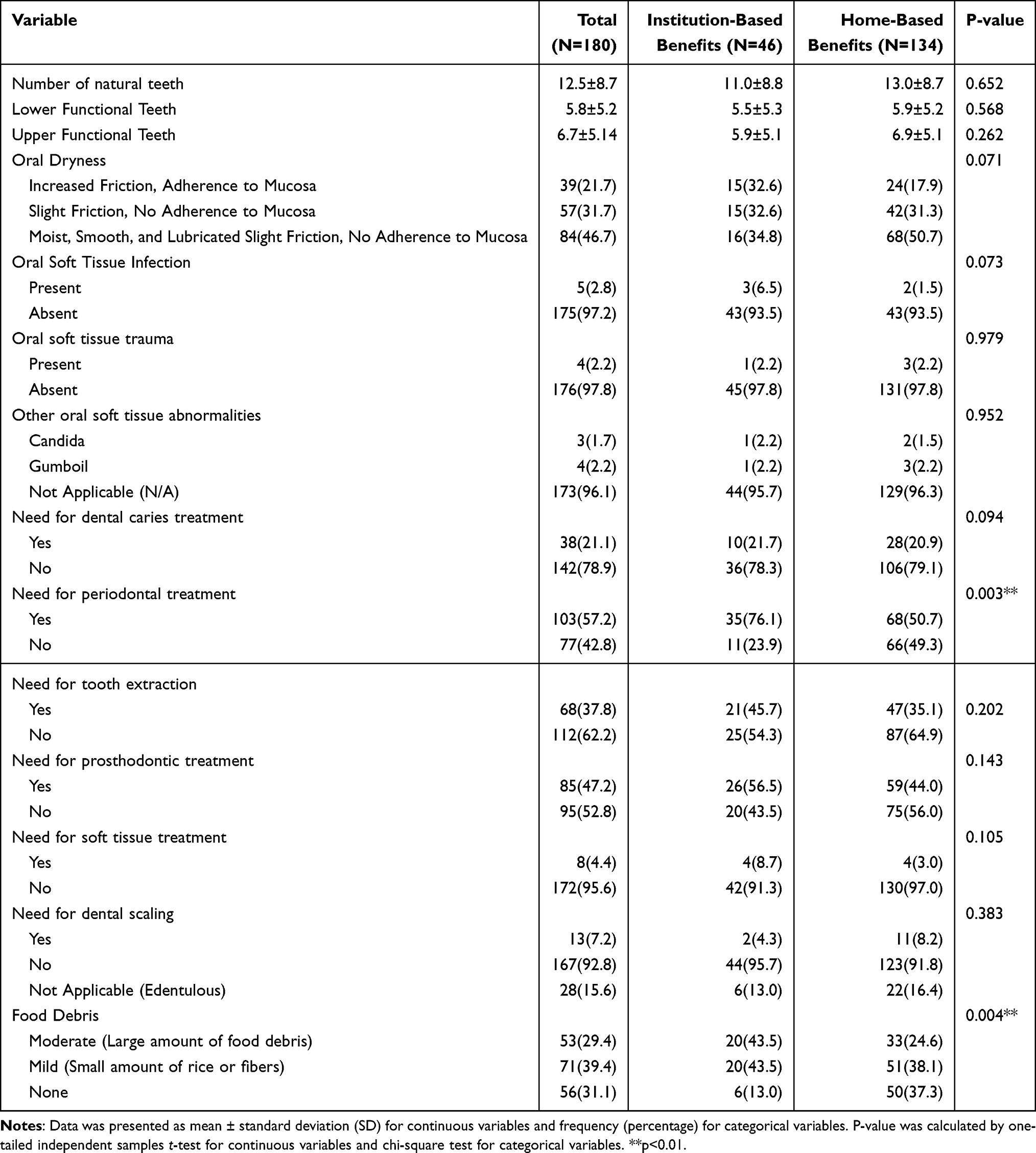 |
Table 3 Oral and Dental Health Condition |
Group Differences in Chewing Ability and Nutritional Status
Table 4 displays data on dental function and nutritional status. Malnutrition was identified in 73.9% of the institution-based group, with the remaining 26.1% classified as at risk; no participants in this group were well-nourished. In contrast, 6% of the home-based group were well-nourished, and 26.9% were malnourished (p<0.001). Chewing ability was also significantly lower in the institution-based group (p<0.001), with 34.8% unable to chew any food and only 17.4% able to chew all food types.
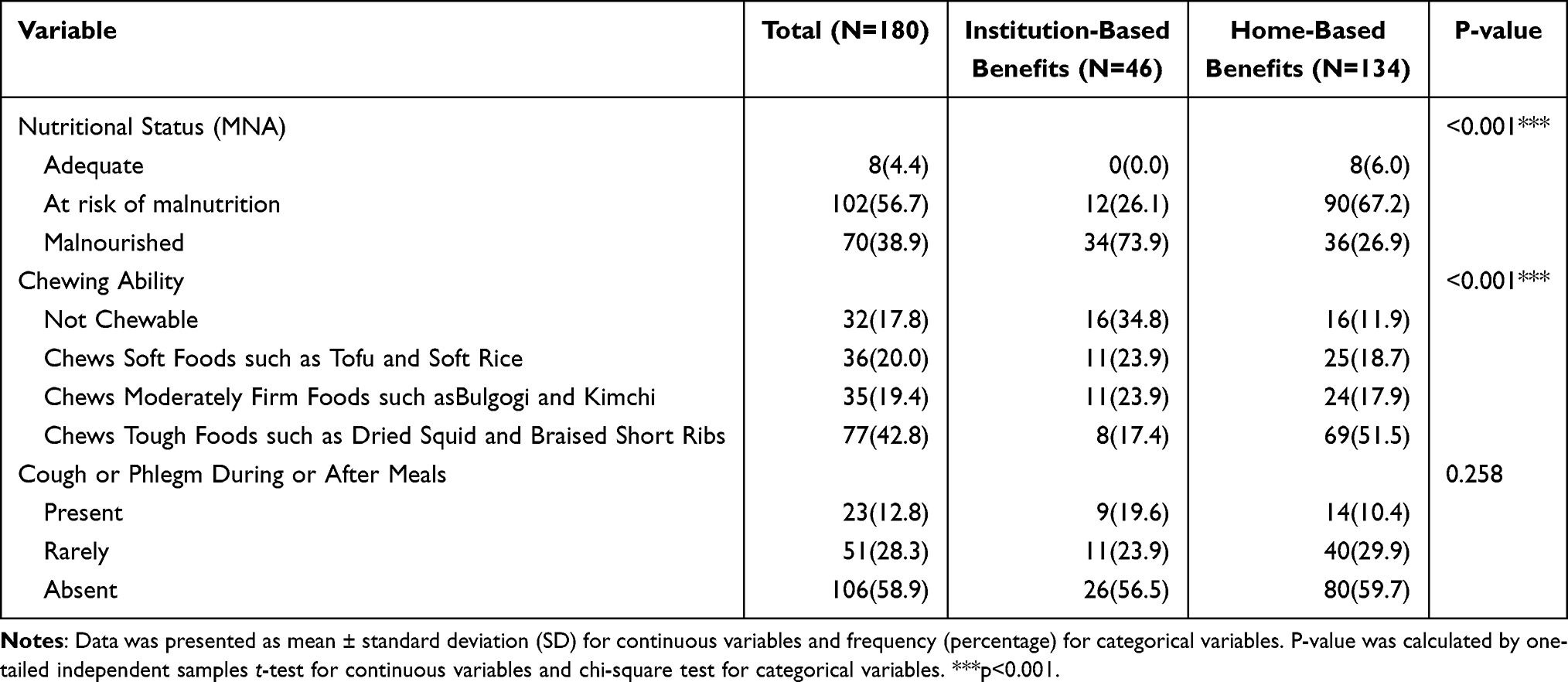 |
Table 4 Dental Function and Nutritional Status |
Oral Health Determinants of Nutritional Status in LTC Residents
Multiple linear regression analysis using backward elimination was conducted to identify oral health factors influencing nutritional status as measured by MNA scores in LTCF residents. Results are presented in Table 5. The model was statistically significant (F=13.716, p<0.001), with an adjusted R2 of 0.542. Higher frequency of daily oral care (β=0.147, p=0.024), better oral moisture status (β=0.241, p<0.001), greater chewing ability (β=0.234, p=0.001), and lower severity of LTC grade were positively associated with MNA scores. Conversely, higher plaque or calculus levels (β=−0.153, p=0.025) and greater food debris accumulation (β=−0.168, p=0.016) were inversely associated with nutritional status.
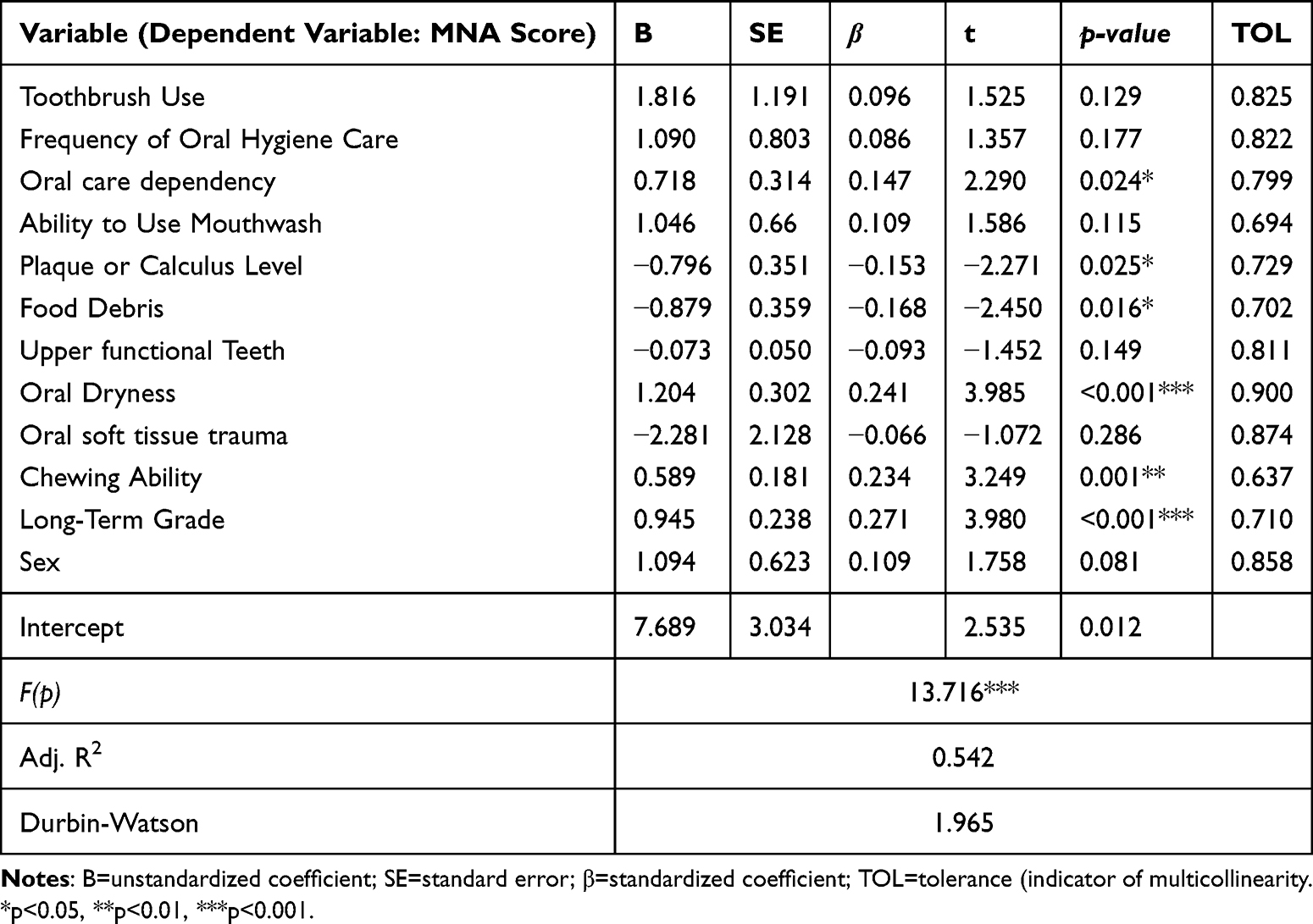 |
Table 5 Regression Analysis: Factors Influencing MNA Score |
Discussion
Older adults receiving institution-based long-term care benefits (Grades 1–2) demonstrated significantly poorer oral health and nutritional status than those receiving home-based benefits (Grades 3–5). A key finding was that participants in the institution-based benefits group (Grades 1–2), who exhibited greater dependency, had significantly poorer physical function, oral health, and nutritional status than those in the home-based benefits group (Grades 3–5). These disparities were evident across anthropometric indicators, oral hygiene behavior, chewing ability, and Mini Nutritional Assessment (MNA) scores.
Multiple linear regression analysis (Table 5) identified oral health factors significantly associated with nutritional status. Higher frequency of daily oral care, better oral moisture, and greater chewing ability were positively correlated with MNA scores, while increased plaque or calculus and food debris were negatively associated. The adjusted R2 of 0.542 suggests that over half of the variance in nutritional outcomes is explained by oral health-related variables, underscoring the critical role of oral conditions in determining nutritional health among LTCF residents.
These findings reaffirm the multifaceted role of oral health in influencing not only dental outcomes but also systemic nutrition and quality of life.14,15 Impaired mastication and oral dryness reduce the ability to consume a diverse diet, thereby heightening the risk of malnutrition and related comorbidities.27,28 These results are consistent with previous literature indicating that poor oral function is a determinant of undernutrition in aging populations.29,30 Moreover, international health agencies increasingly emphasize the integration of oral and nutritional care as foundational to healthy aging.31,32
Despite these associations, this study found that oral hygiene practices in LTCFs remain suboptimal in quality. Although over 90% of participants reported brushing at least twice daily, nearly half of the institution-based group exhibited visible food debris and plaque. This suggests that the effectiveness of oral care, rather than its frequency, plays a pivotal role. Prior studies have shown that structured caregiver training in oral hygiene techniques leads to significant improvements in oral cleanliness, indicating the need for continuous professional.33–35
Furthermore, the institution-based group demonstrated a significantly greater need for dental care, with untreated caries being particularly prevalent, thus highlighting delayed access to preventive services.36 This supports global findings that structural barriers, such as insufficient dental staffing, limited caregiver education, and lack of standardized oral protocols, hinder the provision of adequate oral care in LTCFs.36,37
International strategies offer instructive examples. Public Health England’s national oral health guidelines include mandatory hygiene routines, caregiver education, and access to professional services for residents in care facilities. Japan’s community-based integrated care system similarly delivers coordinated services through multidisciplinary teams, emphasizing accessibility and individualized management for older adults.38 These frameworks illustrate the feasibility and efficacy of integrated policies in improving oral and nutritional health. Given the compounded challenges of cognitive impairment, frailty, and limited mobility in LTC residents, self-management of oral care is often impractical.39,40 Korean LTCFs also face environmental and workforce constraints that limit consistent caregiver engagement in oral health practices.41 Therefore, Korea should consider implementing a multidisciplinary, integrated care model that includes regular oral assessments, caregiver training programs, and tailored nutritional interventions based on oral function.
Despite the meaningful implications, this study has limitations. The sample was limited to 180 older adults from two municipal LTCFs, which may not be representative of all institutionalized older adults in Korea. Therefore, generalizability should be approached with caution. Nonetheless, a key strength of this research lies in its comprehensive, clinically guided oral assessments conducted by trained dental professionals, based on internationally recognized protocols adapted for the LTCF context. In contrast to many previous studies relying on self-reported oral health indicators or broad survey tools, this study incorporated objective measures, such as plaque accumulation, oral dryness, and chewing ability, allowing for a nuanced understanding of how specific oral health domains interact with nutritional status. This approach offers valuable evidence that can inform more targeted and integrated care strategies within long-term care settings.
Therefore, to effectively address these unmet needs, Korea should move toward implementing a multidisciplinary care model that reflects both oral and nutritional health considerations. Drawing from international examples such as Japan’s community-based integrated care system, efforts should include routine oral assessments, structured caregiver training, and customized dietary strategies aligned with oral function.
In particular, the government introduced a new “oral care” indicator in the 2025 evaluation framework for LTCFs, allowing assessment of how systematically each facility strives to maintain the oral cleanliness and oral health of its residents. This signifies a policy shift that strengthens the institutional foundation for oral health management within LTCFs. In addition, a phased approach is recommended, commencing with the establishment of implementation bases through local government-led pilot programmes and interprofessional training within facilities in the short term, and culminating in the integration of these efforts into the national LTC evaluation system in the long term. In addition to oral care, integrated nutritional management is also essential, highlighting the importance of staff education and coordinated care between dental and nutrition professionals. Such a coordinated approach would help mitigate health disparities and support the well-being of institutionalized older adults in Korea.42
Conclusion
This study demonstrates that oral health is a pivotal determinant of nutritional status among older adults residing in long-term care facilities. The findings highlight the pressing need to move beyond fragmented care systems and adopt a multidisciplinary approach that integrates oral health and nutrition. To address the unmet needs in oral and nutritional care among older adults in Korean LTCFs, national policy should prioritize routine oral health assessments, systematic caregiver training, and personalized nutrition planning based on oral function. Such an integrated approach has the potential to enhance health equity and improve the quality of life for institutionalized older adults.
Abbreviations
LTCI, Long-Term Care Insurance; LTCFs, Long-Term Care Facilities; LT, Long-Term Care; NHIS, National Health Insurance Service; MNA, Mini Nutritional Assessment.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board of Kyung Hee University, and written informed consent was obtained from all participants prior to data collection. This study was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the BK21 plus program “AgeTech-Service Convergence Major” through the National Research Foundation (NRF) funded by the Ministry of Education of Korea[5120200313836].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Han E-J, Han Z-A, Kim H, Jung TR. Monitoring healthy ageing for the next decade: South Korea’s perspective. Age Ageing. 2023;52(Supplement_4):iv10–12. doi:10.1093/ageing/afad102
2. Statistics Korea. Senior citizen statistics. Statistics Korea; 2024. Available from: https://kostat.go.kr/board.es?mid=a20111030000&bid=11759&act=view&list_no=433631.
3. Kang I-O, Park CY, Lee Y. Role of healthcare in Korean long-term care insurance. J Korean Med Sci. 2012;27(Suppl):S41–S46. doi:10.3346/jkms.2012.27.S.S41
4. Ga H. Long-term care system in Korea. Anna Geriatric Med Res. 2020;24(3):181. doi:10.4235/agmr.20.0036
5. Yoon MN, Ickert C, Slaughter SE, Lengyel C, Carrier N, Keller H. Oral health status of long-term care residents in Canada: results of a national cross-sectional study. Gerodontology. 2018;35(4):359–364. doi:10.1111/ger.12356
6. Sallam A, McCorry NK, Harvey M, et al. The impact of dietary intake and nutritional status on the oral health of older adults living in care homes: a scoping review. Gerodontology. 2025;42(4):444–472. doi:10.1111/ger.12821
7. Huang X, Kang L, Bi J. Epidemiology of oral health in older adults aged 65 or over: prevalence, risk factors and prevention. Aging Clin Exp Res. 2025;37(1):193. doi:10.1007/s40520-025-03110-8
8. Park M, Song J-A, Lee M, et al. National study of the nutritional status of Korean older adults with dementia who are living in long-term care settings. Japan J Nurs Sci. 2018;15(4):318–329. doi:10.1111/jjns.12203
9. Borkent J, Manders M, Nijhof A, et al. Too low protein and energy intake in nursing home residents. Nutrition. 2023;110:112005. doi:10.1016/j.nut.2023.112005
10. Do KY, Moon S. Relationship between subjective oral discomfort and health-related quality of life in the South Korean elderly population. Int J Environ Res Public Health. 2020;17(6):1906. doi:10.3390/ijerph17061906
11. Torma J, Winblad U, Cederholm T, Saletti A. Does undernutrition still prevail among nursing home residents? Clin Nutr. 2013;32(4):562–568. doi:10.1016/j.clnu.2012.10.007
12. Lindmark U, Ernsth Bravell M, Johansson L, Finkel D. Oral health is essential for quality of life in older adults: a Swedish national quality register study. Gerodontology. 2021;38(2):191–198. doi:10.1111/ger.12514
13. Khoury C, Samot J, Helmer C, et al. The association between oral health and nutritional status in older adults: a cross-sectional study. BMC Geriatr. 2022;22(1):499. doi:10.1186/s12877-022-03133-0
14. Althaiban MA, Aljefree NM, Almoraie NM, Shatwan IM. Malnutrition is associated with increased disease risk in older people in the Makkah region of Saudi Arabia: a cross-sectional study. Front Public Health. 2023;11:1149739. doi:10.3389/fpubh.2023.1149739
15. Wu X, Xu Y, Liu Y, et al. Relationships between oral function, dietary intake and nutritional status in older adults aged 75 years and above: a cross-sectional study. BMC Public Health. 2024;24(1):1465. doi:10.1186/s12889-024-18906-y
16. Izumi M, Sonoki K, Ohta Y, Fukuhara M, Nagata M, Akifusa S. Impact of tongue pressure and peak expiratory flow rate on nutritional status of older residents of nursing homes in Japan: a cross-sectional study. J Nutr Health Aging. 2020;24(5):512–517. doi:10.1007/s12603-020-1347-y
17. Bakker MH, Vissink A, Spoorenberg SLW, Jager-Wittenaar H, Wynia K, Visser A. Are edentulousness, oral health problems and poor health-related quality of life associated with malnutrition in community-dwelling elderly (aged 75 years and over)? A cross-sectional study. Nutrients. 2018;10(12):1965. doi:10.3390/nu10121965
18. Lindmark U, Jansson H, Lannering C, Johansson L. Oral health matters for the nutritional status of older persons—A population-based study. J Clin Nurs. 2018;27(5–6):1143–1152. doi:10.1111/jocn.14146
19. Fukuyama Y, Komiyama T, Ohi T, Hattori Y. Association between oral health and nutritional status among older patients requiring long-term care who received home-visit dental care. J Oral Sci. 2024;66(2):130–133. doi:10.2334/josnusd.23-0344
20. Chou K-R, Huang M-S, Chiu W-C, et al. A comprehensive assessment of oral health, swallowing difficulty, and nutritional status in older nursing home residents. Sci Rep. 2023;13(1):19914. doi:10.1038/s41598-023-47336-w
21. Lowenstein A, Singh ML, Papas AS. Addressing disparities in oral health access and outcomes for aging adults in the United States. Front Dental Med. 2025;6:1522892. doi:10.3389/fdmed.2025.1522892
22. Janto M, Iurcov R, Daina CM, et al. Oral health among elderly, impact on life quality, access of elderly patients to oral health services and methods to improve oral health: a narrative review. J Pers Med. 2022;12(3):372. doi:10.3390/jpm12030372
23. Organization WH. Oral Health Surveys: Basic Methods. World Health Organization; 2013.
24. Japanese Society of Gerodontology. Oral hygiene management manual for residents of long-term care insurance facilities, 2019 edition. Tokyo, Japan: Japanese Society of Gerodontology; 2019. Available from: https://www.gerodontology.jp/publishing/manual.shtml.
25. Vellas B, Guigoz Y, Garry PJ, et al. The mini nutritional assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition. 1999;15(2):116–122. doi:10.1016/S0899-9007(98)00171-3
26. Kang JH, Ko MJ. Developing Korean version of diagnostic criteria and management method for oral frailty. National Evidence-based Healthcare Collaborating Agency. 2023. Available from: https://www.neca.re.kr/lay1/program/S1T11C145/report/view.do?seq=366.
27. Kwon SH, Park HR, Lee YM, et al. Difference in food and nutrient intakes in Korean elderly people according to chewing difficulty: using data from the Korea National health and nutrition examination survey 2013 (6th). Nutr Res Pract. 2017;11(2):139–146. doi:10.4162/nrp.2017.11.2.139
28. Chan AKY, Tsang YC, Jiang CM, Leung KCM, Ecm L, Chu CH. Diet, nutrition, and oral health in older adults: a review of the literature. Dent J. 2023;11(9). doi:10.3390/dj11090222
29. Lu T-Y, Chen J-H, Du J-K, et al. Dysphagia and masticatory performance as a mediator of the xerostomia to quality of life relation in the older population. BMC Geriatr. 2020;20(1):521. doi:10.1186/s12877-020-01901-4
30. Liu S, Guo Y, Hu Z, Zhou F, Li S, Xu H. Association of oral status with frailty among older adults in nursing homes: a cross-sectional study. BMC Oral Health. 2023;23(1):368. doi:10.1186/s12903-023-03009-8
31. World Health Organization. Achieving better oral health as part of the universal health coverage and noncommunicable disease agendas towards 2030. Geneva, Switzerland: World Health Organization; 2021. Available from: https://apps.who.int/gb/ebwha/pdf_files/eb148/b148_8-en.pdf.
32. 2025 Dietary Guidelines Advisory Committee. Scientific report of the 2025 dietary guidelines advisory committee: advisory report to the secretary of health and human services and secretary of agriculture. U.S. Department of Health and Human Services; 2024. 10.52570/DGAC2025.
33. Wong FMF, YTY N, Leung WK. Oral health and its associated factors among older institutionalized residents-a systematic review. Int J Environ Res Public Health. 2019;16(21):4132. doi:10.3390/ijerph16214132
34. Saarela RKT, Hiltunen K, Kautiainen H, Roitto H-M, Mantyla P, Pitkala KH. Oral hygiene and health-related quality of life in institutionalized older people. Eur Geriatr Med. 2022;13(1):213–220. doi:10.1007/s41999-021-00547-8
35. Weintraub JA, Zimmerman S, Ward K, et al. Improving nursing home residents’ oral hygiene: results of a cluster randomized intervention trial. J Am Med Dir Assoc. 2018;19(12):1086–1091. doi:10.1016/j.jamda.2018.09.036
36. Public Health England. Commissioning better oral health for vulnerable older people: a guide for commissioners. London, UK: Public Health England; 2018. Available from: https://www.gov.uk/government/publications/commissioning-better-oral-health-for-vulnerable-older-people.
37. Hatano Y, Matsumoto M, Okita M, et al. The vanguard of community-based integrated care in Japan: the effect of a rural town on national policy. Int J Integrated Care. 2017;17(2). doi:10.5334/ijic.2451
38. Tsutsui T. Implementation process and challenges for the community-based integrated care system in Japan. Int J Integrated Care. 2014;14(1). doi:10.5334/ijic.988
39. Chiesi F, Grazzini M, Innocenti M, et al. Older people living in nursing homes: an oral health screening survey in florence, Italy. Int J Environ Res Public Health. 2019;16(18):3492. doi:10.3390/ijerph16183492
40. Liu W, Galik E, Boltz M, Nahm E-S, Lerner N, Resnick B. Factors associated with eating performance for long-term care residents with moderate-to-severe cognitive impairment. J Adv Nurs. 2016;72(2):348–360. doi:10.1111/jan.12846
41. Park J-A, Han S, Jin B-H. Exploration of the experience of caregivers for oral health care for the elderly in long-term care facilities: based on the grounded theory. J Korean Acad Oral Health. 2022;46(4):228–235. doi:10.11149/jkaoh.2022.46.4.228
42. National Health Insurance Service. 2025 Evaluation manual for institution-based benefits. Available from: https://www.longtermcare.or.kr/npbs/d/m/000/moveBoardView?menuId=npe0000002602&bKey=B0153&prevPath=/npbs/d/m/000/moveBoardView.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Feeding and Nutrition for People with Dementia in Gerontological Services: A Focus Group Study
Moreno-Fergusson ME, Caez-Ramírez GR, Sotelo-Diaz LI, Sarmiento-González P, Sánchez-Herrera B
Journal of Multidisciplinary Healthcare 2024, 17:3957-3970
Published Date: 13 August 2024
Prevention and Care of Pressure Ulcers in Long-Term Bedridden Adult and Older Adult Patients in the Community: A Systematic Review
Meng L, Banharak S, Sommana C, Ransinyo K, Cheumnok W, Tian J
Therapeutics and Clinical Risk Management 2026, 22:592581
Published Date: 4 May 2026