Back to Journals » Clinical Interventions in Aging » Volume 21
Association of Urinary Equol Concentration with Frailty in Community-Dwelling Older Adults: The Itabashi Longitudinal Study on Aging
Authors Kojima N ![]() , Shida T, Ohta T, Motokawa K, Okamura T, Hirano H, Sasai H
, Shida T, Ohta T, Motokawa K, Okamura T, Hirano H, Sasai H
Received 7 May 2025
Accepted for publication 23 October 2025
Published 21 January 2026 Volume 2026:21 538853
DOI https://doi.org/10.2147/CIA.S538853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Narumi Kojima,1 Takashi Shida,1 Takahisa Ohta,1 Keiko Motokawa,2 Tsuyoshi Okamura,3 Hirohiko Hirano,2 Hiroyuki Sasai1
1Frailty and Musculoskeletal Health Research, Research Team for Promoting Independence and Mental Health, Tokyo Metropolitan Institute for Geriatrics and Gerontology, Tokyo, 173-0015, Japan; 2Oral Frailty and Nutrition Research, Research Team for Promoting Independence and Mental Health, Tokyo Metropolitan Institute for Geriatrics and Gerontology, Tokyo, 173-0015, Japan; 3Dementia and Mental Health Research, Research Team for Promoting Independence and Mental Health, Tokyo Metropolitan Institute for Geriatrics and Gerontology, Tokyo, 173-0015, Japan
Correspondence: Narumi Kojima, Frailty and Musculoskeletal Health Research, Research Team for Promoting Independence and Mental Health, Tokyo Metropolitan Institute for Geriatrics and Gerontology, 35-2 Sakae-cho, Itabashi-ku, Tokyo, 173-0015, Japan, Tel +81339643241, Email [email protected]
Background: Frailty is a common geriatric syndrome associated with adverse health outcomes. Equol, a metabolite of the soy isoflavone daidzein, has gained attention for its potential health benefits, particularly in bone, muscle, and cardiovascular health. This study examines the association between urinary equol concentration and frailty status in older adults, with participants further classified into equol producers and non-producers.
Methods: A cross-sectional analysis was conducted using data from 651 community-dwelling older adults (aged 70– 85) participating in the Itabashi Longitudinal Study on Aging in February 2023. Urinary equol concentration was measured using Enzyme-Linked Immunosorbent Assay, and participants were classified as equol producers (≥ 1,000 nmol/L) or non-producers (< 1,000 nmol/L). Frailty was assessed based on the revised Japanese Cardiovascular Health Study criteria. Binomial logistic regression was used to evaluate the association between equol production and frailty status or its components, adjusting for age and sex.
Results: Of the participants, 57.1% were equol producers. Fifty-five point eight percent were categorized as frail or prefrail. Equol producers had a significantly lower odds ratio (OR) for frailty or prefrailty (OR=0.71; 95% CI, 0.51– 0.97) compared to non-producers. Among the frailty components, low physical activity was associated with equol production (OR=0.60; 95% CI, 0.41– 0.88).
Conclusion: Equol production was inversely associated with the prevalence of frailty or prefrailty, particularly with respect to maintaining physical activity. This suggests a potential protective role of equol-producing capacity in healthy aging, warranting longitudinal studies to further explore this association.
Keywords: equol, frailty, aging, physical activity, soy isoflavones, community-dwelling older adults
Background
Frailty, a common geriatric syndrome characterized by decreased strength, endurance, and physiological function, increases vulnerability to adverse health outcomes, including disability, hospitalization, and mortality. Identifying factors that can mitigate frailty in older adults is crucial for improving their quality of life and extending healthy aging.1
Regardless of gender, the mechanism of physical and mental health functional decline including frailty have been partially explained by declining estrogen levels.2 In this context, preventive effects of intake of isoflavones, ie the phytoestrogens, against hormone-related diseases, including breast cancer, stroke, and myocardial infarction in women and prostate cancer in men have been reported.3,4
Especially, equol, a metabolite of the soy isoflavone daidzein, has recently gained attention for its potential health benefits. Notably, equol can exert estrogenic effects by binding to estrogen receptors, which may help support bone health, muscle maintenance, and cardiovascular function through the modulation of estrogen-like activity, potentially offsetting the effects of age-related estrogen decline.5 This phytoestrogenic action is thought to contribute to reduced inflammation and oxidative stress, mechanisms that further protect against frailty-related outcomes. However, not all individuals can produce equol; it can be produced in only 50–60% among East Asians, including Japanese.6 This capacity depends on specific gut bacteria to convert daidzein into equol, and this capacity varies based on an individual’s gut microbiota composition.7 This unique, microbiota-dependent process has positioned equol as a significant factor in personalized nutrition and health interventions, with implications for promoting healthy aging.
Previous studies have shown that equol producers may have better cognitive function8 and metabolic health,9 suggesting a potential protective role against age-related diseases. However, the relationship between equol production and frailty has not been well-studied. Given the biological plausibility of equol’s benefits and the need for modifiable factors to prevent frailty, this study aims to explore the association between equol-producing capacity as represented by urinary equol concentration and frailty status in community-dwelling older adults.
The Itabashi Longitudinal Study on Aging, which is a cohort study project on urban community-dwelling older adults starting in 2021,10 provides a unique opportunity to examine this association in a well-defined cohort. This study cross-sectionally investigates whether older adults who produce equol have a lower risk of frailty and its components, aiming to contribute to the understanding of dietary and microbial factors in healthy aging.
Methods
Participants
Community-dwelling older adults who underwent the health checkup as a part of “Itabashi Longitudinal Study on Aging” conducted in February 2023 participated in the study. Under an official agreement, Itabashi Ward provides researchers of Tokyo Metropolitan Institute for Geriatrics and Gerontology with personal details of residents aged 70+. The researchers conduct health checkups, use the data for research, and offer feedback and health advice. This project began in February 2021, while the health checkup of year 2023 took place February 1–14, 2023, to which those whose date of birth was between January 1938 and December 1952 were invited aiming to the potential age range of 70–85 years. Subjects without a urine sample or complete frailty status data (grip strength, walking speed, fatigue, physical activity, or weight loss) were excluded from the study. This study was approved by the Ethics Committee of the Tokyo Metropolitan Institute for Geriatrics and Gerontology (approval number: TMIG-R21-056) and was conducted in accordance with the ethical standards laid down in the Declaration of Helsinki.11 Written informed consent was obtained from all participants prior to their inclusion in the study.
Measurements
Urine samples were collected at the health examination site for the analysis of equol concentration. Each participant used a urine collection kit (urine collection SET-B, JESCO Corporation) to collect 5–10 cc of their first morning void at home, before breakfast. Participants were not given specific instructions to restrict or encourage soybean product consumption or medication use prior to collection. However, as the first morning void was used, this collection method inherently minimizes the influence of recent dietary intake or medication. Participants in this study were community-dwelling older adults who voluntarily attended health check-ups for this study, and thus were expected to have sufficient cognitive ability to comply with instructions. In addition, staff at the examination site confirmed the labeling and handling of the urine containers upon submission. Upon arrival at the health check-up site, the collected urine samples were transferred into vials, aliquoted, and stored at −80°C until analysis.
Urinary equol concentrations were analyzed using an equol ELISA kit (Healthcare Systems Co., Ltd).12 Measurements were performed in compliance with the protocol of the ELISA kit. The absorbance was measured at a wavelength of 450 nm with a reference wavelength of 570 nm.
A calibration curve (four-parameter logistic regression model) was constructed from the concentration and absorbance of the standard solution to calculate the concentration of equol. According to the manufacturer’s performance characteristics, the intra-assay coefficients of variation (CVs) were 10.8% at 10.0 μg/mL, 8.2% at 19.3 μg/mL, and 6.1% at 50.3 μg/mL (n=6 each), while the inter-assay CVs were 10.2% at 10.4 μg/mL, 10.1% at 17.8 μg/mL, and 12.9% at 39.6 μg/mL (n=6 each). According to the thresholds established in a previous study,13 urinary equol concentrations above 1,000 nmol/L were classified as equol producers, while those below 1,000 nmol/L were classified as non-producers.
Frailty was evaluated based on the revised Japanese version of Cardiovascular Health Study criteria.14 Participants were categorized as frail when three or more of the following (1)-(5) conditions were met, as prefrail when one or two were met, and robust when none of the conditions were met; (1) weight loss, (2) muscle weakness, (3) fatigue, (4) decreased walking speed, (5) decreased physical activity. “Weight loss” was defined as unintentional weight loss of 2 kg or more during past 6 months. “Muscle weakness” was assessed using a digital handgrip dynamometer (TKK5401, Takei Scientific Instruments Co., Ltd). Grip strength was measured twice with the dominant hand in a standing position when possible, with the maximum value recorded. For participants unable to stand, the test was conducted in a sitting position. Grip strength <28 kg for men and <18 kg for women was defined as weakness. “Fatigue” was evaluated with the question “Have you felt tired without reason during the past two weeks?” (yes/no), which has been adopted in previous studies. “Slowness” was defined as normal walking speed of <1.0 m/sec. “Physical inactivity” was assessed using two self-administered questions: (a) “Do you engage in light exercise or calisthenics? How many days per week?” and (b) “Do you engage in regular exercise or sports? How many days per week?” Participants who answered “none” to both questions were classified as physically inactive. Frailty assessment and urine sample collection were performed on the same day during the health checkup, with early-morning urine samples used for equol measurement.
In addition, covariates were assessed as follows. Dietary variety was evaluated using the dietary variety score developed by Kumagai et al (2003),15 which has been widely applied in Japan. Participants were asked whether they consumed each of the following 10 food groups almost daily: meat, fish/shellfish, eggs, milk, soybean products, green/yellow vegetables, potatoes, seaweeds, fruits, and fats/oils. One point was assigned for each group consumed almost daily, yielding a score ranging from 0 to 10. Weekly physical activity duration was assessed with a questionnaire based on the International Physical Activity Questionnaire (IPAQ),16 modified for feasibility in large-scale health checkups. Participants were asked (1) the number of days per week they engaged in walking or higher-intensity physical activity (none, 1–7 days), and (2) the average duration per day (open-ended). Weekly duration was calculated by multiplying frequency by duration. Social connections were measured using the validated Japanese version of the Lubben Social Network Scale-6 (LSNS-6).17 Smoking status was assessed by asking “Do you currently smoke tobacco products, including electronic cigarettes?” with three possible responses (current, former, never). For analysis, participants were dichotomized into current smokers and non-smokers (former and never smokers combined).
Statistical Analysis
Primary Analysis
Sex differences in baseline characteristics were assessed using Student’s t-test for continuous variables and χ2-test for categorical variables. Binomial logistic regression analyses with no adjustment, adjustment for age and sex, were conducted to analyze the association of equol-producing capacity as an independent variable with binomial frailty classification (robust vs prefrail or frail), and the each frailty component as dependent variables. We intentionally adjusted only for age and sex, considering these as fundamental and immutable factors. This approach aimed to broadly capture the association between equol-producing capacity and frailty, including potential mediating pathways through intermediate factors such as chronic disease or lifestyle. SPSS ver.27 (IBM Japan) was used for analysis and results were considered statistically significant when p value<0.05.
In a supplementary analysis, participants with undetectable urinary equol (n=164) were assigned a value of 0.0005 μg/mL, corresponding to half of the lowest detectable concentration. The values were then natural log-transformed, standardized, and entered into logistic regression models to estimate odds ratios per 1-SD increase in equol concentration for frailty status and its components.
Secondary Analysis
In addition to the primary analysis examining the association between equol-producing capacity and frailty risk, a secondary, exploratory analysis was conducted to investigate potential associations between modifiable lifestyle factors and frailty risk specifically among participants without equol-producing capacity. Binomial logistic regression analysis was performed with the presence of frailty as the dependent variable. The modifiable lifestyle factors considered in this analysis included:
- Dietary variety, assessed as the number of food groups (fish, meat, eggs, milk, soy products, colored vegetables, seaweed, potatoes, fruits, and oils/fats) consumed almost daily.
- Weekly total duration of physical activities equivalent to or greater than walking.
- Social connections, evaluated using the Japanese version of the Lubben Social Network Scale, short form (LSNS-6), with scores ranging from 0 to 30 points, with higher scores indicating better social connectedness.
- Current smoking status.
- Age and sex were included as adjustment variables in the model.
Results
Primary Analysis
Six hundred fifty-six people participated in this health checkup. Five of them were excluded from the analysis because of missing data necessary for measurement of urinary equol concentration or frailty classification. Thus, a total of 651 participants were included in the statistical analysis. A flow diagram depicting the number of participants at each stage, from invitation to final analysis, is provided in Figure 1. The cognitive status of participants, assessed by the Mini-Mental State Examination-Japanese (MMSE-J), indicated preserved function (median score 28; interquartile range 27–30), supporting that the cohort was cognitively intact and able to follow study instructions. Subjects ranged in age 70–85 years, with a mean of 75.6 (SD:4.0) years, 58.2% male, 57.1% equol-producing (ie 42.9% non-producing), and 55.8% “frail or prefrail” (ie robust 44.2%). The percentages of participants who fell into the categories of weight loss, muscle weakness, fatigue, decreased walking speed, and decreased physical activity were 12.0%, 25.9%, 12.0%, 13.1%, and 21.8%, respectively (Table 1).
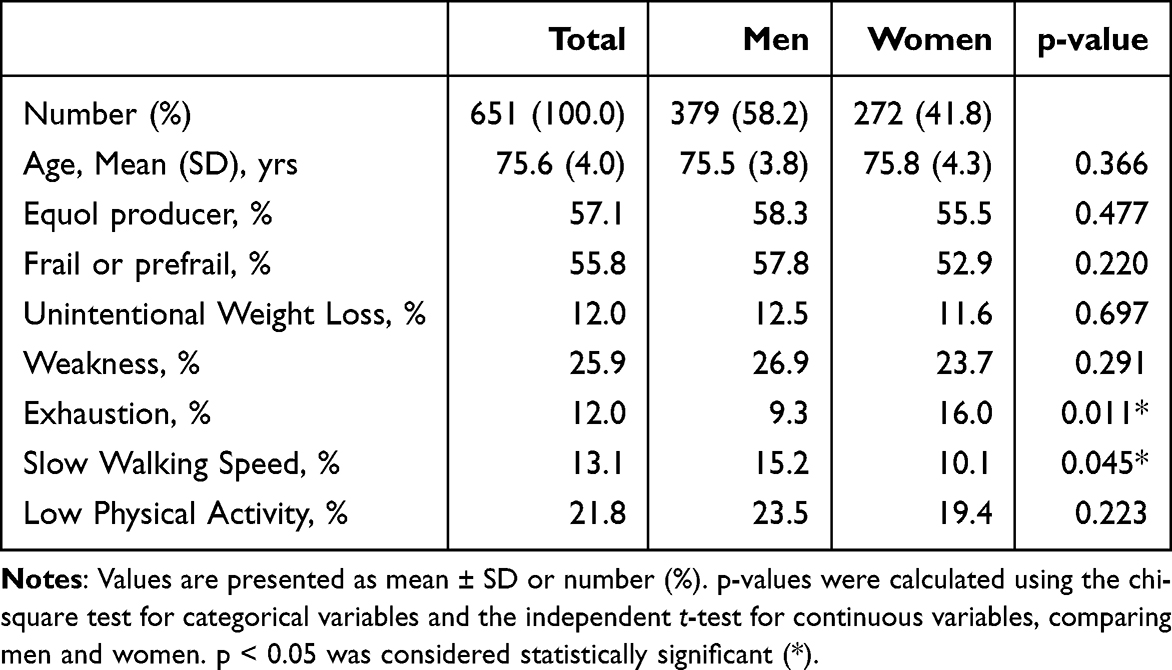 |
Table 1 Participant Characteristics |
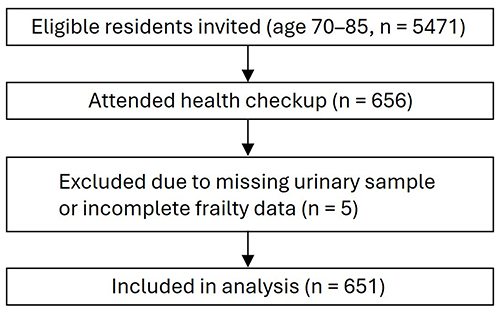 |
Figure 1 Participant flow diagram. |
As shown in Table 2, the unadjusted model indicated a non-significant association between equol-producing capacity and being frail or prefrail (OR = 0.77 [95% CI, 0.56–1.05]). After adjusting for sex and age, the association became statistically significant (OR = 0.71 [95% CI, 0.51–0.97]). In the sex-stratified analysis, a significant association was observed only in men (0.62 [0.40, 0.95]), whereas no significant association was found in women.
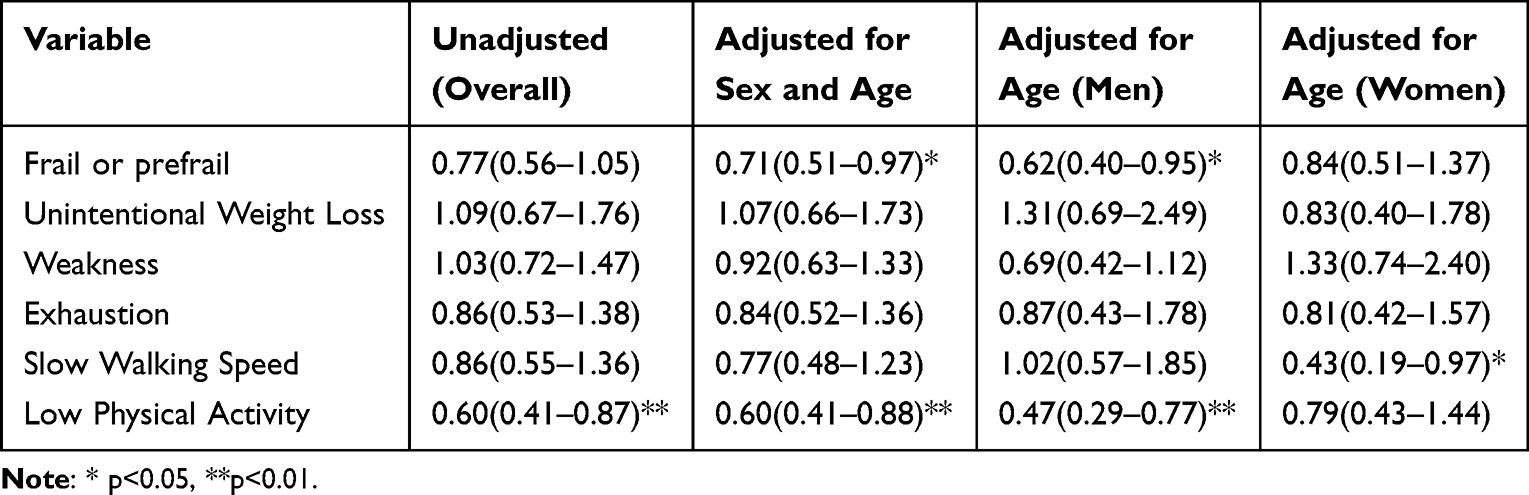 |
Table 2 Adjusted and Unadjusted Odds Ratios and 95% Confidence Intervals by Having Equol-Producing Capacity for Frail or Prefrail and for Each Frailty Component (Overall and by Sex) |
Regarding frailty components, the overall association was not significant for slow walking speed; however, in the sex-stratified analysis, a significant association was observed only in women (0.43 [0.19, 0.97]). In the overall analysis, equol producers had a significantly lower odds ratio for low physical activity (0.60 [95% confidence interval, 0.41, 0.88]). In the sex-stratified analysis, this association remained significant in men (0.47 [0.29, 0.77]) but not in women. No significant differences were found for the other frailty components (Table 2).
Supplementary analysis using log-transformed equol concentration as a continuous variable yielded consistent results, with higher equol levels associated with lower odds of frailty or prefrailty (adjusted OR=0.79; 95% CI, 0.67–0.93), and a significant association observed particularly for low physical activity (Supplementary Table S1). Similar associations were observed when frailty was treated as an ordinal outcome in supplementary analyses (Supplementary Table S2).
Secondary Analysis
Among the non-equol producers, none of the lifestyle-related variables—dietary variety, total duration of physical activity, social connectedness (LSNS-6), or smoking status—showed a significant association with the presence of frailty (Table 3).
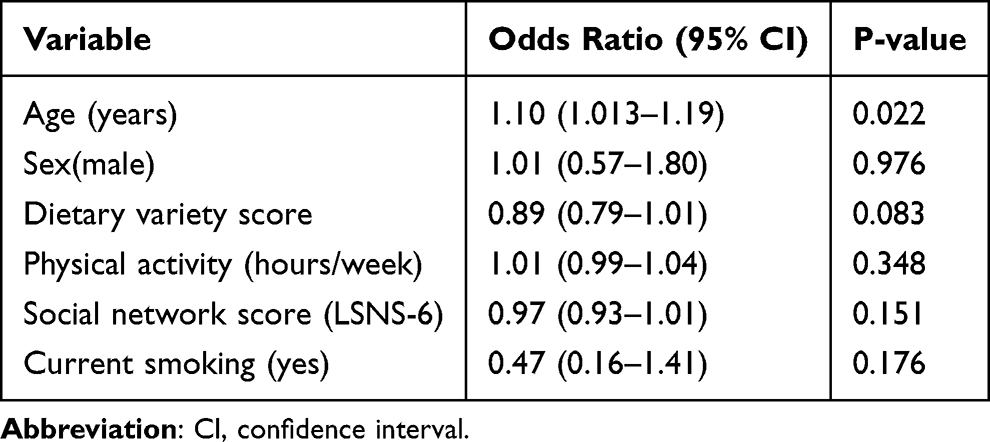 |
Table 3 Logistic Regression Analysis of Modifiable Lifestyle Factors Associated with Frailty in Non-Equol Producers |
Discussion
Our results cross-sectionally showed that equol producer status was associated with lower odds of being frail or prefrail. To the best of our knowledge, this is the first study on the association between equol-producing capacity and frailty.
The results of this study were similar to studies on the association of equol-producing capacity with cognitive function,13 non-alcoholic fatty liver disease18 or metabolic parameters19 in the context of health benefits by equol-producing capacity. According to a cross-sectional study on older adults,13 equol producers showed better cognitive function than non-producers after a standardized soy challenge test. Furthermore, equol production is significantly associated with a lower incidence of non-alcoholic fatty liver disease in Japanese women aged 50–69.14 Equol producer status is also linked to improved metabolic health and reduced atherosclerosis risk in Japanese women around menopause and early postmenopause.19
Estrogen-modulating and antiandrogenic functions of equol may help explain the observed associations with frailty status, with potential sex-specific effects being more pronounced in men.7 Equol has estrogen-modulating properties that may help prevent frailty in older adults by supporting bone health through estrogenic activity, maintaining muscle mass via estrogen receptors, and reducing inflammation. It also aids in hormonal balance, enhances endothelial function, and improves lipid metabolism, thereby promoting cardiovascular health. Additionally, equol has antiandrogenic effects by binding to dihydrotestosterone, which may contribute to prostate cancer prevention in men and indirectly reduce frailty risk.20 The observed stronger association in men may be attributed also to their inherently lower estrogen levels, making them more responsive to equol’s estrogen-like effects. In contrast, postmenopausal women, despite reduced estrogen levels, still retain a baseline estrogenic environment, potentially limiting the additional benefits conferred by equol.
Focusing on individual frailty components, the association between equol producer status (defined by urinary equol concentration) and a lower risk of walking speed decline in women may be attributable to equol’s role in preserving bone density, particularly after menopause. Women experience a rapid decline in bone density following menopause, which increases the risk of osteoporosis21 and may heighten the fear of falls and fractures, ultimately leading to a reduction in walking speed. However, equol has been shown to help maintain bone density, through its estrogen-like effects particularly in women, thereby potentially reducing fall risk and preserving walking speed among equol producers.22
The observed association between equol producer status and a lower risk of low physical activity, particularly in men, may be influenced by gender differences in lifestyle and social interactions. Compared to women, older men often have fewer opportunities for spontaneous physical activity, especially after retirement, partly because they tend to have fewer community-based social connections.23 Consequently, many men lack well-established exercise routines once they leave the workforce, leading to increased sedentary behavior and prolonged sitting time at home. This lack of physical activity may make them more susceptible to the influence of factors that promote movement and activity. In this context, equol’s potential benefits in improving vascular function and reducing inflammation could alleviate fatigue and enhance comfort during physical activity. While women generally maintain higher levels of daily physical activity, making any increase less pronounced, equol’s positive effects on physical activity levels may be more evident among men.
In contrast, other frailty components, such as weight loss, muscle strength, and fatigue, did not show significant associations with equol-producing capacity. Several potential reasons can be considered for this observation. First, the mechanisms by which equol exerts biological effects may not uniformly influence all aspects of frailty. For example, while equol’s anti-inflammatory and estrogen-like properties may directly support physical activity, their influence on parameters such as weight loss or fatigue might require longer periods to manifest or be secondary to changes in activity levels. Second, these components may be influenced more strongly by factors other than equol production, such as nutritional status, comorbidities, or genetic predispositions. Lastly, the lack of significant findings for these components could also be due to limitations in the study design, such as sample size or measurement sensitivity, which may have reduced the power to detect associations.
Implications
The potential involvement of equol-producing capacity in frailty development suggests the need to consider equol-producing status when formulating health maintenance strategies in older adults. While equol-producing capacity may be associated with a lower risk of frailty, maintaining adequate soy isoflavone intake remains essential to fully leverage its potential benefits. Unfortunately, for individuals who lack equol-producing capacity, the secondary analysis did not identify actionable lifestyle recommendations specific to frailty prevention. This suggests that personalized interventions tailored to the individual’s health status may be necessary.
Furthermore, emerging evidence indicates that equol-producing capacity is not necessarily fixed or innate, but may be influenced by lifestyle-related changes. Evidence suggests that it may be associated with improvements in gut microbiota composition.24 Lifestyle modifications, such as regular physical activity, sufficient sleep, and a balanced diet, could potentially enhance the gut environment, enabling equol production. Combining this with adequate soy product intake might represent a potential avenue for future research on strategies related to frailty in older adults including non-equol producers.
Strengths and Limitations
Although to the best of our knowledge, this is the first study to identify an association between equol-producing capacity and frailty, it cannot stand without several limitations. Firstly, there is a possibility that some individuals with the capacity to produce equol were misclassified as non-producers because they had not consumed isoflavones immediately prior to testing. In order to rigorously test for the equol- producing capacity itself, it may be better to standardize the intake of soy isoflavones, especially daidzein, the raw material of equol, immediately prior to the test, though such a control was difficult in this study because it used data from a multi-purpose population-based checkup. The second limitation stems from the cross-sectional nature of this study; the association between equol-producing capacity and frailty may be bidirectional. Older individuals with frailty may consume a restricted diet with a poor dietary variety, potentially leading to inadequate intake of soy isoflavones, the substrate for equol production. This may inhibit the growth of equol-producing bacteria in their gastrointestinal tract. Also, frailty-related inflammation and metabolic changes could negatively impact gut microbiota, further reducing equol production. The causal relationship of equol-producing capacity on an individual’s frailty status cannot be determined in this cross-sectional study. Thirdly, we could not fully account for several potential confounders that may influence equol production. Variations in habitual dietary intake, especially soy isoflavones, were not strictly controlled in this population-based study. In addition, we did not collect detailed information on the use of medications such as antibiotics, which can substantially alter the gut microbiota and thereby equol production. Furthermore, cognitive decline among some older participants may have affected the accuracy of self-reported dietary information or the collection of urine samples. These factors may have introduced measurement error or residual confounding into our findings.
Conclusion
This cross-sectional study showed that in the community-dwelling older adults, equol producer status was associated with a lower likelihood of being prefrail or frail. Longitudinal studies are warranted to test whether having the equol-producing capacity is protective against future incidence of frailty in older adults.
Acknowledgments
The authors would like to express their gratitude to all participants and collaborators involved in the study.
Funding
This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (Grant Number: 23K09708).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–8. doi:10.1016/S0140-6736(19)31786-6
2. Joseph C, Kenny AM, Taxel P, Lorenzo JA, Duque G, Kuchel GA. Role of endocrine-immune dysregulation in osteoporosis, sarcopenia, frailty and fracture risk. Mol Aspects Med. 2005;26(3):181–201. doi:10.1016/j.mam.2005.01.004
3. Steiner C, Arnould S, Scalbert A, Manach C. Isoflavones and the prevention of breast and prostate cancer: new perspectives opened by nutrigenomics. Br J Nutr. 2008;99(Suppl 1):S66–S73. doi:10.1017/S0007114508965788
4. Yamagata K. Soy isoflavones inhibit endothelial cell dysfunction and prevent cardiovascular disease. J Cardiovasc Pharmacol. 2019;74(3):201–209. doi:10.1097/FJC.0000000000000708
5. Setchell KDR, Brown NM, Lydeking-Olsen E. The clinical importance of the metabolite equol-a clue to the effectiveness of soy and its isoflavones. J Nutr. 2002;132(12):3577–3584. doi:10.1093/jn/132.12.3577
6. Lampe JW. Emerging research on equol and cancer. J Nutr. 2010;140(7):1369S–1372S. doi:10.3945/jn.109.118323
7. Mayo B, Vázquez L, Flórez AB. Equol: a bacterial metabolite from the daidzein isoflavone and its presumed beneficial health effects. Nutrients. 2019;11(9):2231. doi:10.3390/nu11092231
8. Sekikawa A, Wharton W, Butts B, et al. Potential protective mechanisms of S-equol, a metabolite of soy isoflavone by the gut microbiome, on cognitive decline and dementia. Int J Mol Sci. 2022;23(19):11921. doi:10.3390/ijms231911921
9. Takahashi A, Kokubun M, Anzai Y, et al. Association between equol production and metabolic syndrome in Japanese women in their 50s-60s. Menopause. 2022;29(10):1196–1199. doi:10.1097/GME.0000000000002052
10. Hatanaka S, Osuka Y, Kojima N, et al. Relationship between phase angle and lower-extremity function in older adults: itabashi longitudinal study on aging. Nutrition. 2024;119:112289. doi:10.1016/j.nut.2023.112289
11. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
12. Tabatabaei MS, Ahmed M. Enzyme-Linked Immunosorbent Assay (ELISA). Methods Mol Biol. 2022;2508:115–134.
13. Igase M, Igase K, Tabara Y, Ohyagi Y, Kohara K. Cross-sectional study of equol producer status and cognitive impairment in older adults. Geriatr Gerontol Int. 2017;17(11):2103–2108. doi:10.1111/ggi.13029
14. Satake S, Arai H. The revised Japanese version of the cardiovascular health study criteria (revised J-CHS criteria). Geriatr Gerontol Int. 2020;20(10):992–993. doi:10.1111/ggi.14005
15. Kumagai S, Watanabe S, Shibata H, et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a community. Nihon Koshu Eisei Zasshi. 2003;50(12):1117–1124.
16. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
17. Jang Y, Powers DA, Park NS, Chiriboga DA, Chi I, Lubben J. Performance of an abbreviated lubben social network scale (LSNS-6) in three ethnic groups of older Asian Americans. Gerontologist. 2022;62(2):e73–e81. doi:10.1093/geront/gnaa156
18. Takahashi A, Takahata Y, Kokubun M, et al. Association between equol and non-alcoholic fatty liver disease in Japanese women in their 50s and 60s. J Gastroenterol Hepatol. 2023;38(11):1958–1962. doi:10.1111/jgh.16315
19. Yoshikata R, Myint KZ, Ohta H. Relationship between equol producer status and metabolic parameters in 743 Japanese women: equol producer status is associated with antiatherosclerotic conditions in women around menopause and early postmenopause. Menopause. 2017;24(2):216–224. doi:10.1097/GME.0000000000000743
20. Lund TD, Blake C, Bu L, Hamaker AN, Lephart ED. Equol an isoflavonoid: potential for improved prostate health, in vitro and in vivo evidence. Reprod Biol Endocrinol. 2011;9(1):4. doi:10.1186/1477-7827-9-4
21. Blake J, Cosman FA, Lewiecki EM, et al. Management of osteoporosis in postmenopausal women: the 2021 position statement of The North American menopause society. Menopause. 2021;28(9):973–997. doi: 10.1097/GME.0000000000001831
22. Corbi G, Nobile V, Conti V, et al. Equol and resveratrol improve bone turnover biomarkers in postmenopausal women: a clinical trial. Int J Mol Sci. 2023;24(15):12063. doi:10.3390/ijms241512063
23. Seino S, Kitamura A, Nishi M, et al. Individual- and community-level neighbor relationships and physical activity among older Japanese adults living in a metropolitan area: a cross-sectional multilevel analysis. Int J Behav Nutr Phys Act. 2018;15(1):46. doi:10.1186/s12966-018-0679-z
24. Miyanaga N, Akaza H, Takashima N, et al. Higher consumption of green tea may enhance equol production. Asian Pac J Cancer Prev. 2003;4(4):297–301.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.