")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 11
Association of tumor location with economic outcomes and air leak complications in thoracic lobectomies: results from a national hospital billing dataset
Authors Bhora F, Ghosh SK, Kassis E, Yoo A, Ramisetti S, Johnston SS, Rehmani S, Kalsekar I
Received 12 October 2018
Accepted for publication 26 March 2019
Published 6 June 2019 Volume 2019:11 Pages 373—383
DOI https://doi.org/10.2147/CEOR.S190644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Samer Hamidi
Faiz Bhora,1 Sudip K Ghosh,2 Edmund Kassis,3 Andrew Yoo,4 Sushama Ramisetti,4 Stephen S Johnston,4 Sadiq Rehmani,5 Iftekhar Kalsekar4
1Health Quest Health System, Poughkeepsie, NY 12601, USA; 2Global Health Economics and Market Access, Ethicon, Inc., Cincinnati, OH, USA; 3Medical Affairs, Ethicon, Inc., Cincinnati, OH, USA; 4Medical Devices - Epidemiology, Johnson and Johnson, New Brunswick, NJ, USA; 5Department of Thoracic Surgery, Mount Sinai St. Luke‘s Hospital, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Purpose: To assess whether tumor location during thoracic lobectomies affects economic outcomes or air leak complications.
Patients and methods: Retrospective, observational study using Premier Healthcare Database. The study included patients aged ≥18 years who underwent elective inpatient thoracic lobectomy for lung cancer between 2012 and 2014 (first qualifying=index admission). Three mutually exclusive tumor location groups were formed: upper lobe, middle lobe, and lower lobe. Primary outcomes were index admission’s length of stay (LOS), total hospital costs, and operating room time; in-hospital air leak complications (composite of air leak/pneumothorax) served as an exploratory outcome. Multivariable models were used to examine the association between tumor location and the study outcomes, accounting for covariates and hospital-level clustering.
Results: 8,750 thoracic lobectomies were identified: upper lobe (n=5,284), middle lobe (n=512), and lower lobe (n=2,954). Compared with the upper lobe, the middle and lower lobe groups had statistically significant (p<0.05): shorter adjusted LOS (7.0 days upper vs 5.8 days middle, 6.6 days lower), lower adjusted mean total hospital costs ($26,177 upper vs $23,109 middle, $24,557 lower), and lower adjusted odds of air leak complications (odds ratio middle vs upper=0.81, 95% CI=0.74–0.89; odds ratio lower vs upper=0.60, 95% CI=0.46–0.78). Findings were similar but varied in statistical significance when stratified by open and video-assisted thoracoscopic surgery approach.
Conclusion: Among patients undergoing elective thoracic lobectomy for lung cancer in real-world clinical practice, upper lobe tumors were significantly associated with increased in-hospital resource use and air leak complications as compared with lower or middle lobe tumors.
Keywords: thoracic lobectomy, costs, length of stay, cancer
Introduction
According to the American Cancer Society, an estimated 212,584 individuals were newly diagnosed with lung cancer in the US in 2017.1 Lung cancer is the second most prevalent cancer in the US and is the leading cause of cancer death globally.2 Among the available treatment options, surgical resection is still the gold standard for patients with stage 1 and 2 lung cancers. Types of surgical resection include diagnostic and therapeutic wedge resection, segmentectomy, lobectomy, and pneumonectomy. Surgical resections can be performed via open or video-assisted thoracoscopic surgical (VATS) approach. The VATS approach has been associated with improvements in a variety of clinical and economic outcomes relative to the open approach;3 however, the adoption of VATS lobectomy has been found to vary widely in US hospitals and is used less frequently than the open approach.4,5
While there have been multiple studies looking at factors affecting clinical and economic outcomes associated with lung resection, one variable that has been identified but not extensively studied is the location of the lobe on which the resection is performed. Studies have shown that upper lobe resections are associated with an increased risk of prolonged air leaks.6–9 To date, however, little is known regarding whether location of lobe resection affects economic outcomes. The study described herein addresses this gap by using a large hospital billing database to assess the association between tumor location and outcomes, including operating room time (ORT), hospital length of stay (LOS), total hospital costs, and air leak complications (ALC).
Material and methods
Data and patient selection
This retrospective, observational study used the Premier Healthcare Database®, which comprises hospital administrative and billing information for all hospital discharges occurring within more than 700 hospitals throughout the US. The database contains discharge-level information on all International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnoses and procedures recorded during each admission, a date-stamped log and cost of all billed items by cost-accounting department, administrative records on LOS and discharge status, and selected information on patient, provider, hospital, and insurance characteristics. Although the database excludes federally funded hospitals (eg, Veterans Affairs), the hospitals included therein are nationally representative based on bed size, geographic region, location (urban/rural), and teaching status.
Patients included for study had elective thoracic lobectomy (ICD-9-CM 32.41 for VATS lobectomy; 32.49 for open lobectomy) with a primary diagnosis of lung cancer associated with a specified tumor location (ICD-9-CM 162.3 for upper lobe, 162.4 for middle lobe, or 162.5 for lower lobe) between January 1, 2012 and December 31, 2014 (first observed admission=index admission). Patients were classified into three mutually exclusive groups according to their tumor location based on the primary diagnosis of lung cancer during the index admission: those who had tumor(s) in the upper lobe (upper lobe group); those who had tumor(s) in the (middle lobe group); those who had tumor(s) in the (lower lobe group).
Measurement of patient, hospital, provider, and procedure characteristics
Patient demographics measured included age, sex, race, marital status, and payer type. Patient clinical characteristics measured during the index admission included the Charlson Comorbidity Index Score, which is a risk adjustment score calculated based on ICD-9-CM diagnosis codes for various comorbidities,10 as well as selected individual comorbidities (diabetes, hypertension, obesity, depression, and chronic obstructive pulmonary disorder [COPD]). All comorbidities were adjusted to exclude instances wherein they were indicated as specifically not being “Present on Admission”. Hospital and provider characteristics measured during index admission included urban vs rural hospital, hospital teaching status, hospital geographic region, hospital bed size, hospital annual thoracic surgery volume, and procedural physician specialty. Procedure characteristics measured included year of surgery and VATS vs open approach.
Measurement of economic and clinical outcomes
Primary outcomes measured during theindex admission included the index admission’s total ORT, hospital LOS, and total hospital costs (ie, the costs of the index admission from the hospital’s perspective, as opposed to charges [ie, the amount of money a hospital charges to an insurance company/patient for a given discharge] or reimbursement [ie, the amount of money the hospital is actually paid by the insurance company/patient for a given discharge]). Total hospital costs included both direct and indirect costs, and based on the Premier Healthcare Database taxonomy of costs included those related to room and board, supply, operating room, laboratory, pharmacy, radiology, therapy, respiratory, cardiology, labor and delivery (when applicable), and other. Total hospital costs were inflation adjusted to 2014 US dollars using the Medical Care component of the US Bureau of Labor Statistics Consumer Price Index. The study’s exploratory outcome, which was designated as such due to uncertainty regarding the diagnostic coding used for its definition, was ALC. ALC were ascertained from diagnosis codes recorded during the index admission. Patients were flagged as having an ALC if any of the following ICD-9-CM diagnosis codes were recorded during the index admission: “512.1 Iatrogenic pneumothorax”, “512.2 Postoperative air leak”, “512.84 Other air leak”, or “512.89 Other pneumothorax”. As there is no specific date or duration for diagnosis codes, it was not possible to ascertain if the ALC was present for a prolonged or shorter duration. Instances in which the diagnosis of the exploratory outcomes was designated as being Present on Admission were ignored.
Statistical analyses
Descriptive statistics were used to characterize all study variables. Multivariable regressions – survey logistic for binary outcomes and generalized estimating equations (GEE) for continuous outcomes – were used to compare the outcomes across the tumor location groups, accounting for hospital-level clustering and adjusting for patient characteristics (age, sex, race, marital status, payer, year of index admission, the Charlson Comorbidity Index, and specific comorbid conditions [diabetes, hypertension, depression, obesity, and COPD]), and hospital/provider/procedure characteristics (rural vs urban hospital, teaching vs non-teaching hospital, geographic region, hospital bed size, hospital volume, procedural physician specialty, and hospital costing type); see Tables 1 and 2 for specific categorizations of these variables. These GEE models used an exchangeable working correlation structure, which was chosen based on a qualitative understanding of the potential nature of clustering within hospitals. Each model used a link function and error distribution which was tailored to the empirical distribution of the outcome variable, based on the Box–Cox and modified Park tests:11,12 total ORT – log link/gamma error; hospital LOS – log link/negative binomial error; total hospital cost – log link/gamma error; exploratory outcomes – logit link/binomial error. All models were checked for potential multicollinearity and interaction effects.
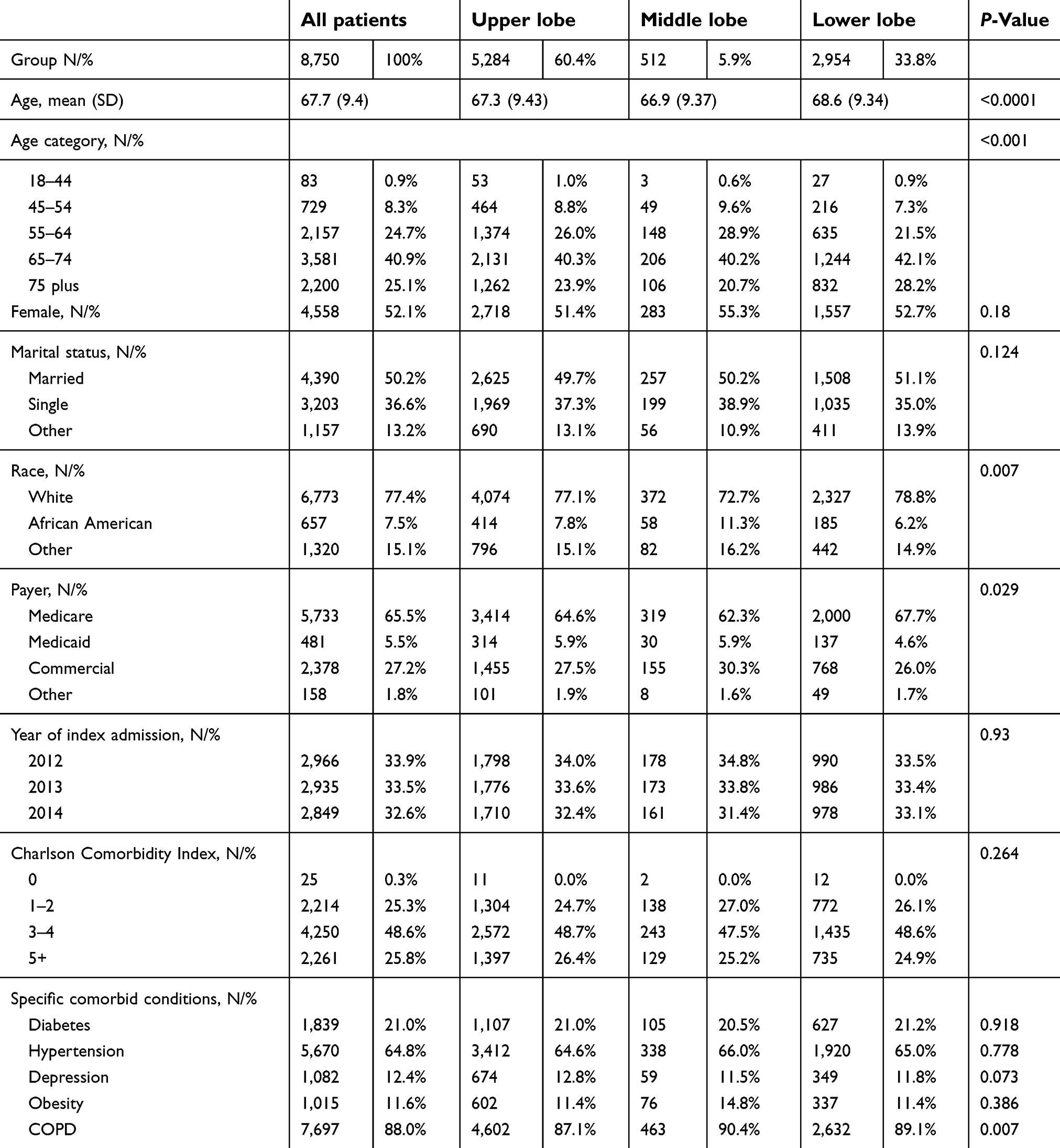 | Table 1 Patient demographics and clinical characteristics, all patients |
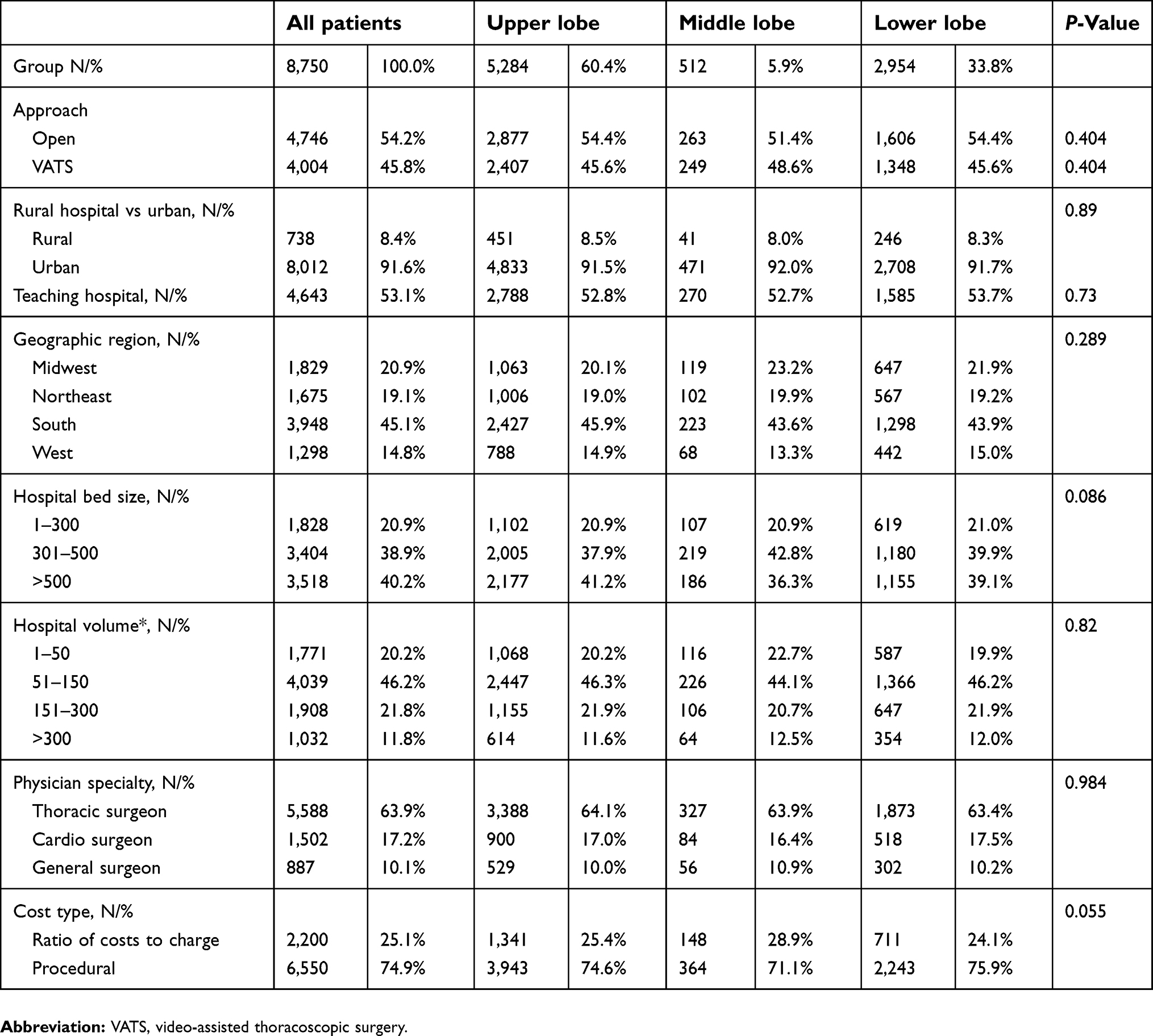 | Table 2 Hospital, provider, and procedure characteristics, all patients |
Adjusted outcomes were generated for each of the study groups using the least squares means approach with observed margins. In the GEE models, inference was based on empirical (robust) standard error estimates. A two-sided critical value of 0.05 was used to determine statistical significance. All statistical analyses were performed using SAS version 9.3. All analyses were completed for all patients combined, as well as stratified by VATS vs open approach.
External validation analysis
To externally validate the study results in a different population and data source, an analysis was performed in which the study was replicated within an administrative insurance claims database; specifically, the Truven Health MarketScan® Commercial and Medicare databases. These databases comprise inpatient and outpatient medical claims data and outpatient pharmacy data for individuals with employer-sponsored primary or Medicare supplemental health insurance. Patients selected from these databases underwent thoracic lobectomy between January 1, 2012 and September 30, 2015. This external validation analysis examined the association between the tumor location and all study outcomes except for ORT and total hospital costs from the hospital perspective, which are not available in the MarketScan databases.
Post-hoc sub-analyses
To explore whether the association of tumor location with LOS was affected by key provider characteristics, a post-hoc sub-analyses was conducted in which the multivariable analyses were repeated among urban vs rural hospitals and by procedural physician specialty (thoracic surgeon, cardiovascular surgeon, general surgeon, or other surgeon). We examined whether the direction of the associations found in these sub-analyses would be consistent with that in the primary analyses, while expecting that the ability to detect statistical significance for such associations may be eliminated due to the relatively smaller sample sizes of the sub-analysis groups.
Results
Patient demographic and clinical characteristics
A total of 8,750 patients undergoing elective thoracic lobectomy for lung cancer between January 1, 2012 and December 31, 2014 met the study inclusion criteria: 5,284 in the upper lobe group, 512 in the middle lobe group, and 2,954 in the lower lobe group. Descriptive statistics on patient demographics and clinical characteristics for the overall cohort, stratified by tumor location group, are shown in Table 1. The mean patient age ranged from 67.3 years (SD =9.4 years) in the upper lobe group to 68.6 years (SD =9.3 years) in the lower lobe group, just over half of each group was female, and approximately three quarters of each group were of white race. Of the selected comorbidities examined for the study, COPD was the most common, with prevalence ranging from 87.1% in the upper lobe group to 90.4% in the middle lobe group. Descriptive statistics on patient demographics and clinical characteristics, presented separately by approach (open vs VATS), are shown in
Hospital, provider, and procedure characteristics
Descriptive statistics on hospital, provider, and procedure characteristics for the overall cohort, stratified by tumor location group, are shown in Table 2. The proportion of patients undergoing open surgeries ranged from 51.4% in the middle lobe group to 54.4% in both the upper and lower lobe groups. The other hospital, provider, and procedure characteristics were generally similar across the tumor location groups: thoracic surgeons performed 63.4–64.1% of operations and 44.1–46.3% of operations were performed in hospitals in the South region of the US, which has predominant representation in the Premier Healthcare Database. Descriptive statistics on hospital, provider, and procedure characteristics, presented separately by approach (open vs VATS), are shown in
Unadjusted outcomes
Descriptive statistics on unadjusted outcomes, presented for all patients and separately by approach (open vs VATS), are shown in Table 3. Among all patients, the upper lobe group had the longest hospital LOS, highest total hospital costs, longest total ORT, and the highest rates of ALC. These relationships held when the analyses were stratified by approach.
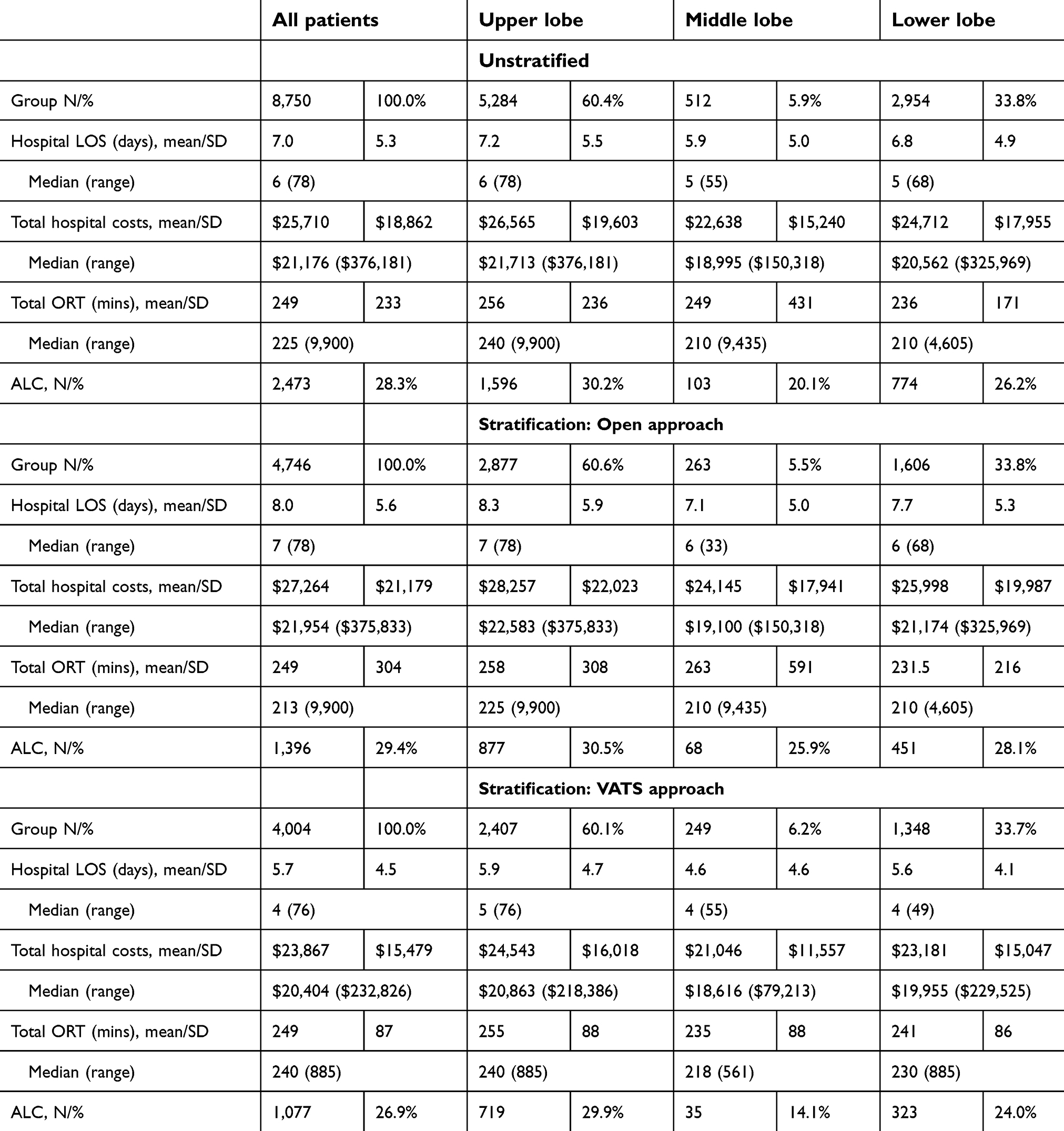 | Table 3 Unadjusted outcomes, all patients and stratified by the approach |
Multivariable-adjusted outcomes
Multivariable-adjusted results for the analysis of primary outcomes, presented for all patients and separately by approach (open vs VATS), are shown in Table 4. Among all patients, compared with the upper lobe, the middle and lower lobe groups had statistically significant (all p<0.05): shorter adjusted hospital LOS (7.0 days upper lobe group vs 5.8 days middle lobe group, 6.6 days lower lobe group) and lower adjusted mean total hospital costs ($26,177 upper lobe group vs $23,109 middle lobe group, $24,557 lower lobe group). Adjusted total ORT differed significantly between the upper and lower lobe groups (254 mins upper lobe group vs 244 mins middle lobe group, 235 mins lower lobe group).
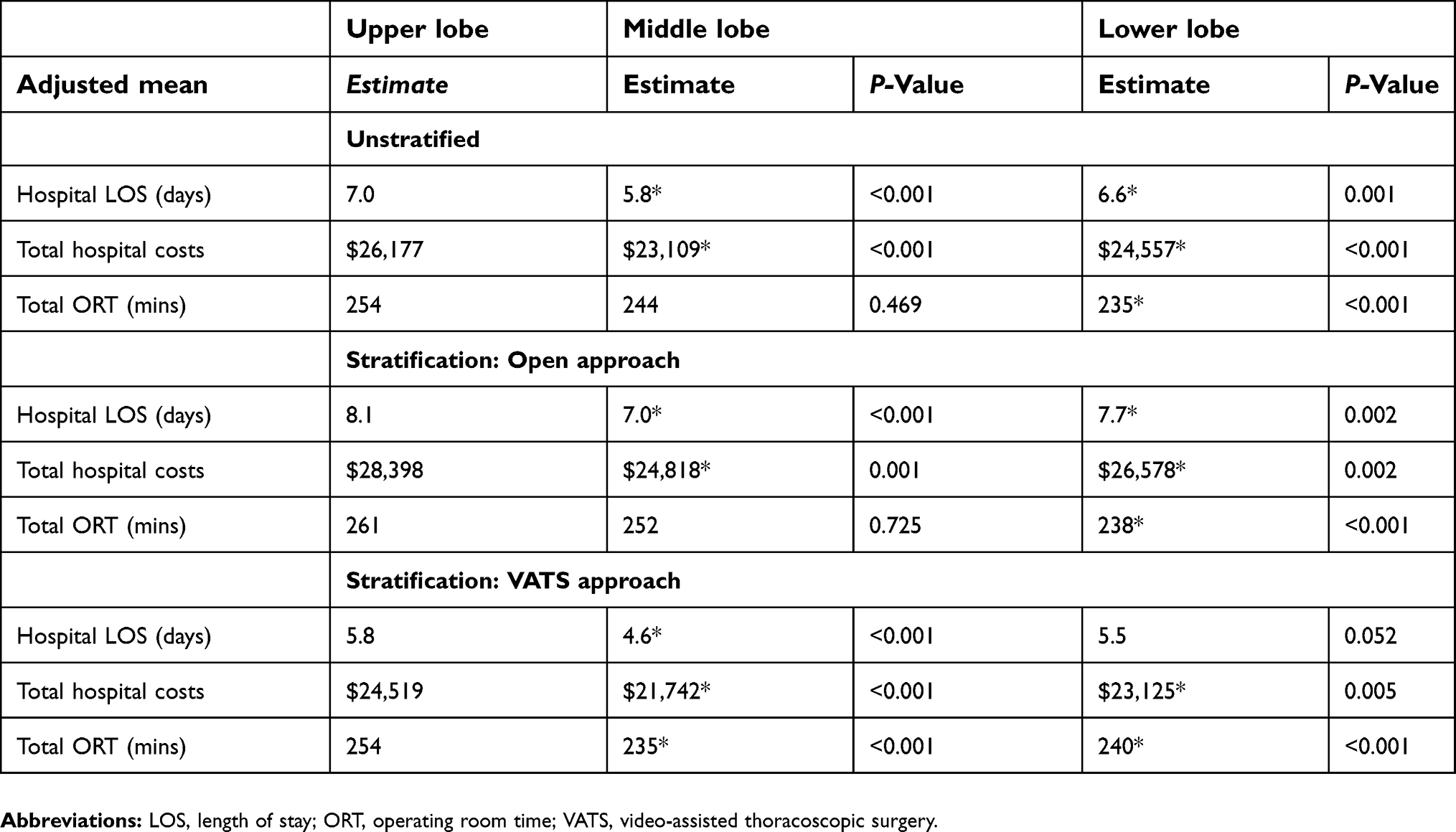 | Table 4 Multivariable-adjusted primary outcomes, all patients and stratified by the approach |
When stratified by the approach, the directions of associations between the primary outcomes and the tumor location groups were consistent. Among patients undergoing lobectomy through the open approach, the difference in adjusted total ORT was not statistically significant between the lower and upper lobe groups, in contrast to being statistically significant in the overall analysis. Among patients undergoing lobectomy through the VATS approach, the difference in adjusted hospital LOS was not statistically significant between the lower and upper lobe groups, in contrast to being statistically significant in the overall analysis.
Multivariable-adjusted results for the analysis of the exploratory ALC outcome, presented for all patients and separately by approach (open vs VATS), are shown in Table 5. Among all patients, compared with the upper lobe, the middle and lower lobe groups had statistically significant (all p<0.05) lower adjusted odds of ALC (OR middle lobe group vs upper lobe group=0.81, 95% CI=0.74–0.89; OR lower lobe group vs upper lobe group=0.60, 95% CI=0.46–0.78). When stratified by the approach, the directions of associations between ALC and the tumor location groups were consistent; however, among patients undergoing lobectomy through the open approach, the difference in ALC rates was not statistically significant between the middle and upper lobe groups, in contrast to being statistically significant in the overall analysis.
 | Table 5 Multivariable-adjusted exploratory outcome, all patients and stratified by the approach |
External validation analysis
In the external validation analysis replicating the study results in the Truven Health MarketScan Commercial and Medicare Supplemental administrative insurance claims databases, a total of 5,824 patients undergoing elective thoracic lobectomy for lung cancer between January 1, 2012 and September 30, 2015 met the study inclusion criteria; 3,564 in the upper group, 340 in the middle group, and 1,920 in the lower group.
Multivariable-adjusted outcomes of the external validation analysis are shown in Table 6. Consistent with the primary analyses, compared with the upper lobe, the middle and lower lobe groups had statistically significant: shorter adjusted LOS (6.4 days upper lobe group vs 5.5 days middle lobe group, p<0.001; 6.2 days lower lobe group, p=0.035) and lower adjusted odds of ALC (middle lobe group vs upper lobe group OR=0.57, 95% CI=0.37–0.86, p=0.007; lower lobe group vs upper lobe group OR=0.82, 95% CI=0.68–0.97, p=0.0238).
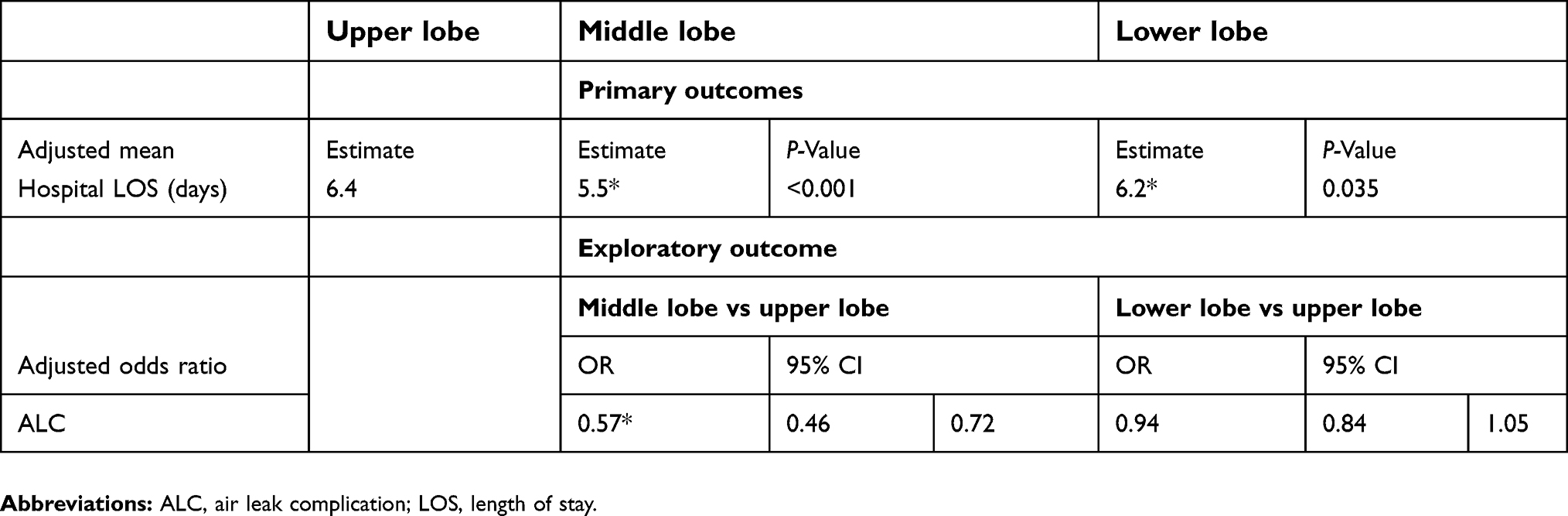 | Table 6 Adjusted outcomes, external validation analysis in administrative insurance claims data |
Post-hoc sub-analyses
Appendix Table 3 displays the results of the post-hoc sub-analyses examining whether the direction of the associations found in selected sub-groups (urban vs rural hospitals; thoracic surgeon, cardiovascular surgeon, general surgeon, or other surgeon) would be consistent with that in the primary analyses. In these analyses, findings were consistent with the primary analyses: the upper lobe group was always associated with the highest adjusted values of LOS, and the association remained statistically significant in most cases; as expected, for some of the smaller sub-group samples the results did not reach statistical significance.
Discussion
To our knowledge, this study is the first to compare economic and clinical outcomes by tumor location among patients undergoing elective thoracic lobectomies for lung cancer using a real-world database. This study found that patients who had upper lobe tumors had significantly longer hospital LOS, higher total hospital costs, and higher odds of ALC as compared with middle and lower lobe tumors.
There are no other studies that have attempted to specifically address the impact of tumor location on economic outcomes; however, several studies have been published in which tumor location of the upper lobe has been reported as being significantly associated with the risk of ALC.6–9 As noted above, Brunelli et al (2004) performed a retrospective analysis of 588 patients to identify the predictors of prolonged air leak in patients undergoing lung lobectomy.7 They reported that among other factors, patients undergoing an upper lobectomy were at a significantly increased risk of air leak lasting ≥7 days. Ciccone et al (2003) performed a retrospective analysis of 2,000 patients to identify predictors of postoperative air leaks in patients undergoing lung resections.13 They also reported that among other factors, patients undergoing an upper lobe lobectomy were at a significantly increased risk for developing prolonged postoperative air leak. Similar findings to those of Ciccone (2003) and Brunelli (2004) regarding upper lobectomies and air leaks were also reported by DeCamp et al (2006) in the context of the NETT trial.14
One plausible explanation for a higher PALs rate after upper lobe resection is the residual apical pleural spaces often leading to a poor visceral–parietal pleura apposition.7 In upper lobe resections procedures, the rarefied or poorly compliant remaining lobes are not able to fill the remaining space in the hemithorax regularly. This may allow persistent large undrained postresection fluid collections, which will lead to trapping of the remaining lobe thus preventing adequate re-expansion. Even when drainage will be ultimately attempted, this will result in a fixed space.6 Other potential explanations include more variability in upper lobe anatomy, exposure, and extent of tissue dissection.
Upper lobe tumors had significantly longer hospital LOS and higher total hospital costs as compared with middle and lower lobe tumors. This can be partially explained by increased risk of ALC associated with upper lobe tumors: in a post-hoc multivariable analysis comparing patients with vs without ALC (not adjusting for cancer location), those with air leak complications had significantly longer hospital LOS (8.6 vs 6.1 days, p<0.001) and higher total hospital costs $28,865 vs $24,081) as compared with those without ALC. Furthermore, when including ALC as an explanatory variable in the models of cancer location’s impact on hospital LOS and total hospital costs, the overall impact of cancer location was attenuated (specifically: the differences between the upper lobe and middle lobe reduced from 1.13 to 0.96 for LOS days and from $3,068 to $2,757 for total hospital costs; the differences between the upper lobe and lower lobe reduced from 0.36 to 0.27 for LOS days and from $1,620 to $1,464 for total hospital costs); however, upper lobe tumors still had significantly longer hospital LOS and higher total hospital costs as compared with middle and lower lobe tumors, suggesting that the impact of cancer location on these outcomes is not entirely explained by ALC. Thus, future research investigating whether cancer location affects other important clinical outcomes is warranted to explain the differences observed in the present study.
Although no formal statistical comparisons were made between patients undergoing lobectomy via the open vs the VATS approach, the latter group had numerically lower costs, LOS, and rates of ALC (particularly in the middle and lower lob groups). This finding is consistent with prior analyses in which the VATS approach was found to be associated with improvements in a variety of clinical and economic outcomes relative to the open approach.3 Future analyses formally comparing these approaches in a large real-world database such as the one used for the present study would be useful.
Studies such as the present one are also valuable to informing “feature engineering” (more specifically, developing a list of candidate variables) in the context of predictive analytics and machine learning algorithms aimed at identifying patients who are at elevated risk for undesirable outcomes. As predictive models become disseminated into clinical practice (eg, for hospitals to prioritize and target resources in real time), hypothesis-generating studies such as the present study will play a key role in informing the development and refinement of the list of variables which may be considered important to making predictions. In the case of the present study, tumor location may play an important role in future predictive models of ALC or identification of surgical cases which may be associated with elevated intensity of resource use.
The present study is subject to some limitations. First, the non-randomized, observational nature of this study does not allow for causal inference regarding the effect of tumor location on the study outcomes. All findings of the present study must be interpreted as associations. Whereas, the Premier Healthcare Database is one of the largest and most generalizable databases in which information on hospital costs are available, it lacks information on potentially important clinical variables such as certain elements of operative approach (eg, fissureless, anterior, posterior), FEV1, diffusing capacity of the lungs for carbon monoxide, tumor/node/metastasis status/cancer stage and tumor size, smoking history/current smoking status, and pulmonary function tests; it also lacks information on other factors such as use of valves (eg, Heimlich valves), reinforcements (eg, sealants, buttresses), or the performance of the procedural physician and supporting operating room staff. If these factors vary substantially by cancer location, the adjusted estimates of LOS, total hospital costs, and risk of ALC may be subject to residual confounding. To our knowledge, no database exists in which both hospital costs and clinical/surgical factors are both comprehensively captured.
Second, administrative data are subject to measurement error arising from non-specific coding and miscoding. Air leaks and pneumothorax were identified using ICD-9-CM diagnosis coding, which does not incorporate the ideal level of granularity to identify severity (eg, prolonged air leak). The diagnosis codes for thoracic cancer include “other” and “unspecified” locations which were excluded in the present analysis due to an inability to assign location. Future studies using data from the ICD-10 Procedure Coding System era (October 1, 2015 and onward) may be able to better elucidate the specific location in which lobectomies are performed because of greater specificity identifying right from left, and upper from middle and lower lung lobes.
Third, the cross-sectional nature of the data (information recorded during inpatient admissions only) limits the ability to examine patient characteristics prior to admission (eg, receipt of neoadjuvant chemotherapy) and outcomes after discharge. Future studies employing longitudinal data sources may be able to examine the impact of tumor location on outcomes, such as long-term health care costs, morbidity, and survival.
Finally, the Premier Healthcare Database is a non-probability sample and thus this study’s results may not be generalizable to all hospitals, patients, or thoracic lobectomies performed in the US. However, this study is perhaps the largest of its kind to date, spanning multiple institutions and years, and thus can be viewed as being more reflective of real-world clinical practice than single-center or small randomized trials. Furthermore, the external validation of the study results within an administrative claims database yielded similar findings, suggesting that the findings from the primary analyses generalized to other settings.
Conclusions
Among patients undergoing elective thoracic lobectomy for lung cancer in real-world clinical practice, upper lobe tumors were significantly associated with increased in-hospital resource use and ALC as compared with lower or middle lobe tumors. Given the higher possibility of ALC for upper lobectomies, surgeons may adapt their surgical and intra-procedural approach to reduce the likelihood of post-operative complications.
Abbreviation list
CCI, Charlson Comorbidity Index; COPD, chronic obstructive pulmonary disorder; GEE, generalized estimating equations; ICD-9-CM; international classification of diseases, 9th revision, clinical modification; LOS, length of stay; ORT, operating room time; SAS, statistical analysis system; VAT, video-assisted thoracoscopic surgical approach.
Ethics statement
The study databases are commercially available for purchase from Premier Inc. and IBM Watson Health (Truven). The Premier Healthcare Database and the Truven Health MarketScan® Commercial and Medicare databases consist of de-identified health care records. In the US, retrospective analyses of these databases are considered exempt from informed consent and institutional review board approval as dictated by Title 45 Code of Federal Regulations, Part 46 of the United States, specifically 45 CFR 46.101(b)(4) (
Acknowledgment
We would like to thank Dr Wissam Raad for the clinical input.
Disclosure
Iftekhar Kalsekar, Sudip Ghosh, Edmund Kassis, Stephen Johnston, and Andrew Yoo are employees of Johnson & Johnson. Sushama Ramisetti was a contract employee of Johnson & Johnson at the time this study was conducted. This study was funded by Johnson & Johnson. Dr Faiz Bhora reports being a consultant for Ethicon and serving as a surgical thought leader on new device development, especially the new surgical robot. The authors report no other conflicts of interest in this work.
References
1.
2.
3. Whitson BA, Groth SS, Duval SJ, Swanson SJ, Maddaus MA. Surgery for early-stage non-small cell lung cancer: a systematic review of the video-assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann Thorac Surg. 2008;86(6):
4. Abdelsattar ZM, Allen MS, Shen KR, et al. Variation in hospital adoption rates of video-assisted thoracoscopic lobectomy for lung cancer and the effect on outcomes. Ann Thorac Surg. 2017;103(2):454–460. doi:10.1016/j.athoracsur.2016.08.091
5. Blasberg JD, Seder CW, Leverson G, Shan Y, Maloney JD, Macke RA. Video-assisted thoracoscopic lobectomy for lung cancer: current practice patterns and predictors of adoption. Ann Thorac Surg. 2016;102(6):1854–1862. doi:10.1016/j.athoracsur.2016.06.030
6. Mueller MR, Marzluf BA. The anticipation and management of air leaks and residual spaces post lung resection. Journal of Thoracic Disease. 2014;6(3):271–284. doi:10.3978/j.issn.2072-1439.2013.11.29
7. Brunelli A, Monteverde M, Borri A, Salati M, Marasco RD, Fianchini A. Predictors of prolonged air leak after pulmonary lobectomy. Ann Thorac Surg. 2004;77(4):
8. Elsayed H, McShane J, Shackcloth M. Air leaks following pulmonary resection for lung cancer: is it a patient or surgeon related problem? Annals of the Royal College of Surgeons of England. 2012;94(6):422–427. doi:10.1308/003588412X13171221592258
9. Pompili C, Miserocchi G. Air leak after lung resection: pathophysiology and patients’ implications. Journal of Thoracic Disease. 2016;8(Suppl 1):S46–S54. doi:10.3978/j.issn.2072-1439.2015.11.08
10. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139.
11. Manning WG, Mullahy J. Estimating log models: to transform or not to transform? J Health Econ. 2001;20:461–494. doi:10.1016/S0167-6296(01)00086-8
12. Park RE. Estimation with heteroscedastic error terms. Econometrica. 1996;34:888. doi:10.2307/1910108
13. Ciccone AM, Meyers BF, Guthrie TJ, et al. Long-term outcome of bilateral lung volume reduction in 250 consecutive patients with emphysema. J Thorac Cardiovasc Surg. 2003;125:513–525. doi:10.1067/mtc.2003.147
14. DeCamp MM, Blackstone EH, Naunheim KS, et al. Patient and surgical factors influencing air leak after lung volume reduction surgery: lessons learned from the national emphysema treatment trial. Ann Thorac Surg. 2006;82:
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.