Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 17
Association of the Reduced Function Met420del Polymorphism of SLC22A1 with Metformin-Induced Gastrointestinal Intolerance in Ethiopian Patients with Type 2 Diabetes Mellitus
Authors Degaga A ![]() , Sirgu S, Huri HZ
, Sirgu S, Huri HZ ![]() , Sim MS, Loganadan NK
, Sim MS, Loganadan NK ![]() , Kebede T
, Kebede T ![]() , Tegene B
, Tegene B ![]() , Engidawork E
, Engidawork E ![]() , Shibeshi W
, Shibeshi W ![]()
Received 31 December 2023
Accepted for publication 27 April 2024
Published 3 May 2024 Volume 2024:17 Pages 183—191
DOI https://doi.org/10.2147/PGPM.S457374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Martin H Bluth
Abraham Degaga,1,2 Sisay Sirgu,3 Hasniza Zaman Huri,2 Maw Shin Sim,4 Navin Kumar Loganadan,5 Tedla Kebede,6 Birhanemeskel Tegene,7 Ephrem Engidawork,1 Workineh Shibeshi1
1Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Clinical Pharmacy & Pharmacy Practice, Faculty of Pharmacy, Universiti Malaya, Kuala Lumpur, Malaysia; 3Department of Internal Medicine, Diabetes and endocrinology unit, Saint Paul Hospital Millennium Medical College, Addis Ababa, Ethiopia; 4Department of Pharmaceutical Life Sciences, Faculty of Pharmacy, Universiti Malaya, Kuala Lumpur, Malaysia; 5Department of Pharmacy, Putrajaya Hospital, Putrajaya, Malaysia; 6Department of Internal Medicine, Diabetes and endocrinology unit, Addis Ababa University, Addis Ababa, Ethiopia; 7Department of Microbiology, Saint Paul Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Workineh Shibeshi, Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, P.O.Box 9086, Addis Ababa, Ethiopia, Tel +251 927361143, Email [email protected]
Background: Despite its widespread use and favored profile, there are extensive variations in the treatment outcome of metformin therapy. Furthermore, studies reported that the inter-individual variability in the occurrence of metformin treatment associated side effects were related to the differences in individual genetic profiles. Thus, this study aimed to evaluate whether the reduced function methionine deletion at codon 420 (Met420del) variant of SLC22A1 (rs72552763) is associated with metformin induced gastrointestinal intolerance in Ethiopian patients with type 2 diabetes mellitus (T2DM).
Patients and Methods: A retrospective observational study was conducted on 47 T2DM patients on metformin treatment for < 3 years to assess the association of SLC22A1 (rs72552763) polymorphism with metformin induced gastrointestinal intolerance. Accordingly, 24 metformin tolerant and 23 metformin intolerant individuals with T2DM were recruited. Genotyping of rs72552763 was performed using TaqMan® Drug Metabolism Enzyme Genotyping Assay and its association to metformin induced gastrointestinal intolerance was assessed based on switching to a new class of glucose lowering agents or failure to up titrate dose due to metformin induced gastrointestinal intolerance. Chi-square, logistic regression and Mann–Whitney statistical tests were used as appropriate. Statistical significance was set at p < 0.05.
Results: In our study, no significant association was observed between rs72552763 and metformin induced gastrointestinal intolerance. We found that the female gender and physical inactivity were risk factors for metformin gastrointestinal intolerance.
Conclusion: Our study found that the Met420del variant of SLC22A1 (rs72552763) was not associated with metformin induced gastrointestinal intolerance in Ethiopian patients with T2DM. This is the study first to investigate the association of rs72552763 with metformin intolerance in the Ethiopian population with T2DM. However, the findings need to be cautiously interpreted given the relatively small sample size. In addition, a more complete investigation of SLC22A1 variants would be required to fully assess the effect of the gene on metformin induced gastrointestinal intolerance as several variants with a more severe loss of function have been described.
Keywords: metformin intolerance, SLC22A1 gene, rs72552763, Ethiopia
Introduction
Metformin is indicated as a first-line glucose lowering agent for patients with type 2 diabetes mellitus (T2DM),1 though it has been frequently associated with gastrointestinal symptoms than most other oral glucose lowering agents.2,3 Moreover, although metformin is still recommended as a drug of choice for patients with T2DM,4–6 there are increasing reports demanding a more personalized approaches in its use.7,8 Previous studies reported that the variability to metformin treatment associated incidence of side effects is related to differences in individual genetic profile.9,10
Metformin diffuses poorly across biological membranes as it is a hydrophilic molecule at physiological pH.11 Variations in the gene encoding for one of its main transporters (the organic cation transporter-1(OCT1)),12,13 SLC22A1, could thus potentially affect metformin associated gastrointestinal adverse effects.14 Furthermore, several studies postulated that decreased metformin transport through OCT1 that is expressed in enterocytes might raise local metformin concentration in the intestine, leading to metformin’s gastrointestinal side effects.15–17
In addition, in recent years, the alteration in the gut microbiome composition is increasingly recognized as a potential mediator of metformin-associated gastrointestinal adverse effects.18 To this effect, a comparative study on the gut microbiota profile of metformin-tolerant and metformin-intolerant patients with T2DM revealed that metformin-induced shift in the composition and function of the gut microbiota potentially mediate the drug intolerance.19 Moreover, recent studies showed that the common metformin induced gastrointestinal adverse effects have been attributed to gases (such as CO2 and H2S) produced by the gut microbiota, seemingly through metformin-induced selection and metabolic modelling of Escherichia spp. and Akkermansia muciniphila.20–22 Thus, the decreased metformin transport through OCT1 associated with the reduced functional variants of SLC22A1 might increase metformin concentration in the gut, inducing selective alteration in the metabolic profile of the human gut microbiota and a subsequent shift to potentially mediate metformin associated gastrointestinal adverse effect.
However, there are inconsistent reports on the association between the role of individual SLC22A1 variants and gastrointestinal side effects.14 To address this issue, the reduced function methionine deletion at codon 420 (Met420del) variant of SLC22A1 (rs72552763) was selected for this study since its allele frequency is higher in Ethiopian population as compared to other African population.23–25 Furthermore, Met420del is the most studied functional variant of SLC22A1 gene for its influence on metformin pharmacokinetics though there were inconsistent reports based an extensive survey of recent literature. In addition, this variant is generally observed in combination with a rare loss of function polymorphism, Cys88Arg (rs55918055), that causes improper membrane localization of OCT1, resulting in metformin gastrointestinal intolerance.15 Thus, in this study, we investigated the association of an individual Met420del polymorphism of SLC22A1 with metformin induced gastrointestinal intolerance in Ethiopian patients with T2DM.
Materials and Method
Study Design and Setting
The study setting was described in our recent study, which reported the association of Met420del polymorphism of SLC22A1 with metformin response.23 In this study, a retrospective observational study was conducted on T2DM patients on metformin treatment for <3 years to assess the association of SLC22A1 (rs72552763) polymorphism with metformin induced gastrointestinal intolerance.
Selection of the Study Participants
All patients were diagnosed according to the WHO criteria26 and information on comorbidities, medication use, clinical data, biochemical test parameters, and metformin gastrointestinal intolerance were obtained from clinical records. Socio-demographic data, metformin gastrointestinal intolerance, life style, and medication adherence were obtained from questionnaire interview. Information on gastrointestinal intolerance was obtained both from medical charts and through interview as the information was not available in the charts for some participants and also to confirm for those available.
Eligibility Criteria
Inclusion Criteria
Age 18–65, recently diagnosed (less than 3 years) unrelated T2DM patients on metformin monotherapy within the first 6 months of treatment (for intolerant group) and on metformin treatment for more than 6 months (tolerant group), and willing to give consent to participate in the study were included in the study.
Exclusion Criteria
Pregnant or lactating women, patients with renal or hepatic insufficiency (serum creatinine >1.2mg/dl for renal insufficiency; serum glutamic-pyruvic transaminase or serum glutamic-oxaloacetic transaminase >40IU/L for hepatic insufficiency), active smokers (an adult who smoked even one puff during the past seven days), patients with malignancies or thyroid disorders or depression depending on the documented medical history, patients not adherent to medications, patients with chronic gastrointestinal diseases (including chronic liver disease, cholelithiasis, chronic pancreatitis, inflammatory bowel disease and gastroduodenal ulcer), and patients unable to recall being on metformin or having the gastrointestinal adverse effects were excluded.
Sample Size Estimation and sampling
Comparison of two proportion formula27 was used to determine whether the rs72552763 polymorphism of SLC22A1 exists between metformin intolerant and metformin tolerant groups, considering the following assumptions: p1 = 0.30,28 95% CI, 5% margin of error and a power of 80%. Accordingly, the calculated sample size was set at 21 for each group in the present study. Adding a 10% to account for potential dropouts, the final sample size was 47 (24 for tolerant and 23 for the intolerant group). Purposive sampling technique was used to enroll study subjects.
Collection of Data
In this study, initial preliminary identification of potentially eligible study participants was done based on the attending physician’s review of the medical chart and/or active patient compliant to the attending physician working at the diabetic follow-up clinic. Subsequently, a written consent was obtained from each potential study participant before collection of data. In order to reduce potential source of bias, data were collected by trained nurses working on diabetic follow-up clinic after the participants agreed to written informed consent. An interviewer administered questionnaire and a chart review were used for data collection.
Thus, relevant information was collected from their medical charts and confirmed through oral interview whether gastrointestinal intolerance was a reason for discontinuation and/or not increasing metformin dose over the first 6 months of therapy. However, for those participants who did not have a recorded metformin-associated gastrointestinal adverse effects in their medical charts but actively complaining about the adverse effects to their attending physician, we confirmed through oral interview whether gastrointestinal intolerance was a reason for discontinuation and/or not increasing metformin dose. Accordingly, patients were categorized as metformin tolerant and intolerant groups. Patients meeting the following were taken as intolerant: i) Patients who were on metformin monotherapy and stopped receiving metformin immediate release (IR) formulation within the first 6 months of treatment and switched to another oral hypoglycemic agent (including metformin slow-release formulations) within 6 months of the last metformin IR prescription and reported gastrointestinal adverse effects as the reason for switching;15,29 ii) Patients who were on metformin monotherapy and could not increase their metformin IR dose >500 mg daily despite an HbA1c >7.0% because of the reported gastrointestinal adverse effects.30
Metformin-tolerant individuals were defined as those treated with >2000 mg of metformin daily for more than 6 months (excluding modified-release formulations of metformin) and reported no adverse effects.15 A daily dose of metformin was defined as the last prescribed dose for intolerant patients and as an average dose in the first 6 months (after satisfying tolerance definition) of metformin treatment for tolerant patients.
A four-item Self-Reported Measure of Adherence scale were used to assess medication adherence and individuals who responded “NO’ for all the four questions were considered adherent to medication.31 Furthermore, individuals who modified their lifestyle as recommended for greater than 3 days in the last seven successive days were considered adherent to diet.32 Likewise, study participants who accomplished at least 150 min per week (3 days) of moderate-intensity physical exercise were considered as active or inactive if perform any lesser.33
Genotyping
Blood collection, DNA extraction and genotyping of the rs72552763 polymorphism were described in our recent study.23 Briefly, genotyping of the rs72552763 polymorphism was performed using the TaqMan® Drug Metabolism Enzyme Genotyping Assay (Assay ID: C__34211613_10) from Applied Biosystems (Carlsbad, CA, USA) and ChamQ Geno-SNP Probe Master Mix (Vazyme Biotechnology, Singapore). The qPCR was conducted using the StepOnePlus™ Real-Time PCR System. The genotyping quality was assessed by looking at the allelic discrimination plots for the color and number of discrete clusters as the software makes genotyping call based on VIC/FAM dye ratios and cluster orientation (Figure 1). The quality value was assigned manually in each well for each genotype call to be 100%. Furthermore, a no template control sample was also run in each assay to confirm whether proper genotype call was made or not.
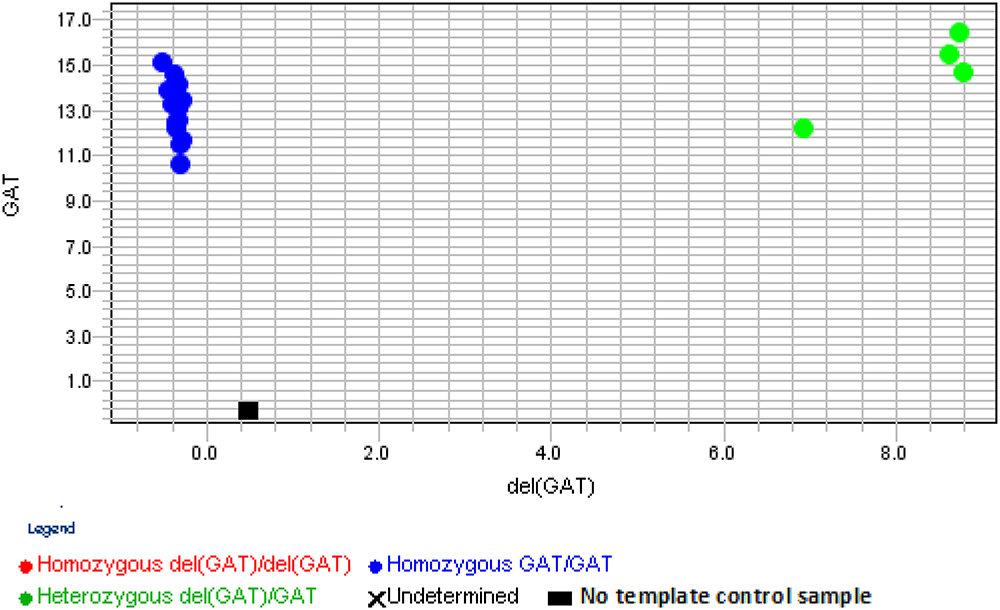 |
Figure 1 Allelic discrimination plot for the delGAT/GAT polymorphic SNP rs72552763. |
Statistical Analysis
Statistical Package for Social Sciences (SPSS) Version 26 for Windows (IBM Corps, Armonk, New York, NY, USA) was utilized for statistical analyses. Categorical variables were described as percentages. Continuous variables were described as medians and interquartile range (IQR). The normality of continuous variables was determined by Kolmogorov–Smirnov and Shapiro–Wilk tests and all the data were not normally distributed. For continuous dependent variables, associations were assessed by Independent-Samples Mann–Whitney U-test. The associations between categorical variables were assessed by a Chi-square test and 95% confidence interval. Logistic regression model analysis was also performed for categorical dependent variables. The Hosmer–Lemeshow goodness-of-fit test was done to assess the model fit (Hosmer–Lemeshow statistic > 0.05). A p-value less than 0.05 was considered statistically significant. In order to evaluate the association of rs72552763 polymorphism with metformin induced gastrointestinal adverse effects, the number of metformin-intolerant patients was assessed. In this study, the Hardy–Weinberg equilibrium (HWE) test was performed using Gene-Calc software, which uses the Chi-square test to determine whether or not observed genotype frequencies are consistent with Hardy-Weinberg expectations.34
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of the College of Health Science, Addis Ababa University (protocol number:118/20/SoP) and IRB of St. Paul’s Hospital Millennium Medical College (RN: DM23/576). National Ethical approval was granted by the National Research Ethics Review Committee, Ministry of Education (MOE), Ethiopia (RN:02/246/572/22). All participants received information about the process and purpose of the study in their local language (Amharic) and provided with a written informed consent. All collected data were anonymized and held confidential.
Results
Characteristics of the Study Participants
In this study, 24 metformin tolerant and 23 metformin intolerant individuals with T2DM were recruited. The Independent-Samples Mann–Whitney U-test showed no significant difference in the median values of BMI and age at diagnosis between the two groups. Obviously, there was a significant difference in the median metformin daily doses between the metformin tolerant and intolerant groups. The median daily dose of metformin was 1000 mg in metformin intolerant group while it was 2000 mg in the tolerant group. Furthermore, the Independent-Samples Mann–Whitney U-Test showed no significant difference in the median values of baseline HbA1c and FBG between metformin tolerant and intolerant study participants (Figure 2). However, there were significant differences in sex and level of physical activity between metformin tolerant and intolerant groups in a chi-square test analysis (Table 1).
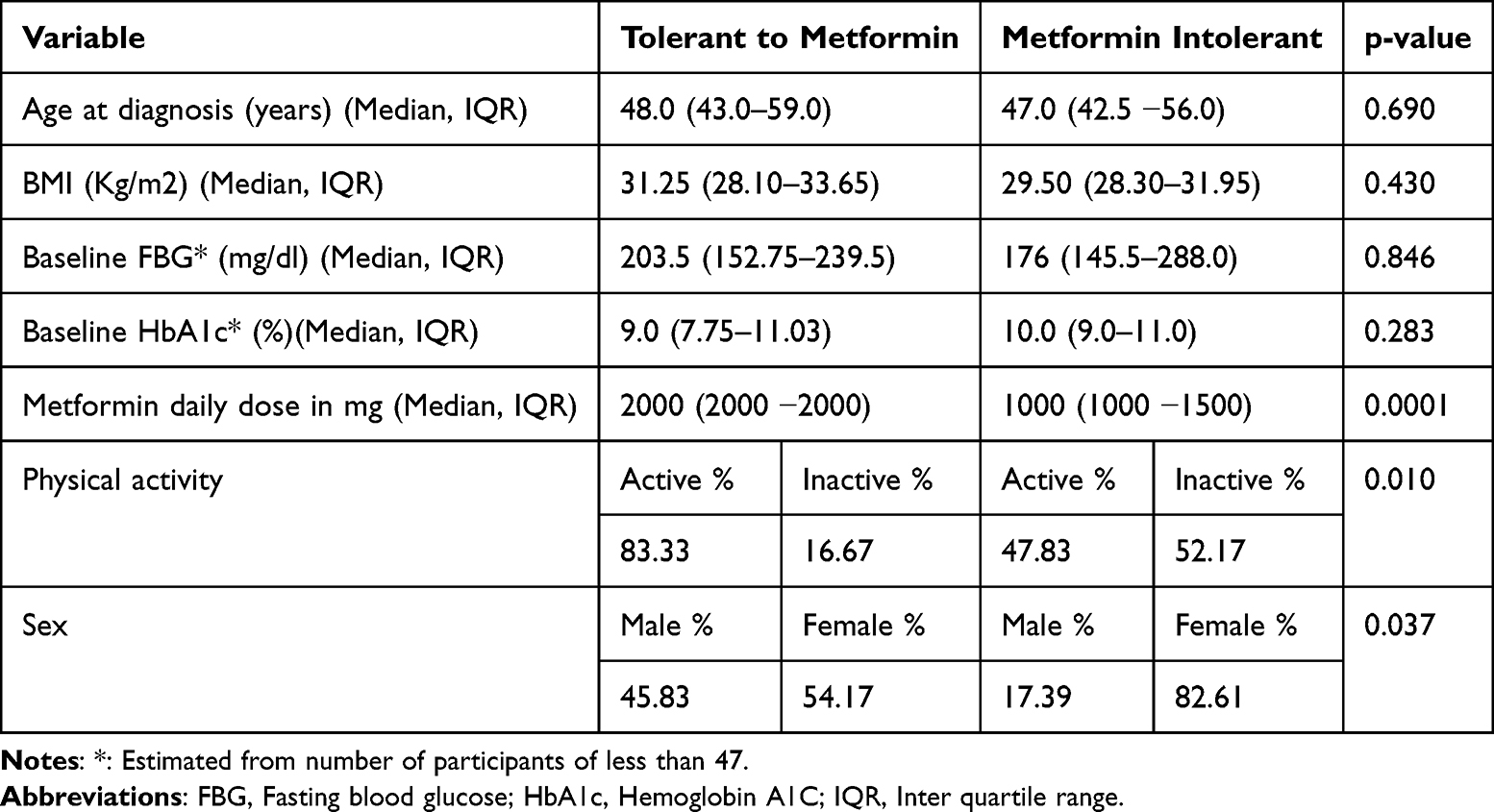 |
Table 1 General Characteristics of the Metformin Intolerance Study Participants (n = 47) |
 |
Figure 2 Independent-Samples Mann–Whitney U-test between metformin tolerant and intolerant groups on their baseline FBG (panel (A) and HbA1c levels (panel (B). |
Genotype Frequency
The minimum allele frequency (MAF) of the 3-base pair (GAT) deletion mutation at rs72552763 was 9.6%, whereas that of the wild-type GAT (G) allele was 90.4% in the current study. No patient was homozygous for the rs72552763 deletion (del) allele in this study (Table 2). The SNP rs72552763 was in line with the principles of the HWE with p-value of 0.984.
 |
Table 2 Genotype and Allele Frequency Distribution of the rs72552763 Polymorphism Across Intolerance Study Participants (n = 47) |
Association of rs72552763 with Metformin Intolerance
In the logistic regression analyses, our study found that there was no significant association between metformin intolerance and genotypes of the SNP rs72552763 (Table 3). In the chi-square test analyses, the alleles of rs72552763 polymorphism were also not significantly associated with metformin intolerance (Table 4). Furthermore, no significant intergroup difference in age were observed between the study participants who were metformin tolerant and intolerant in a logistic regression analysis (Table 3). By contrast, the female gender (OR=4.019, 95% CI (1.048–15.416), p<0.05) and physical inactivity (OR=5.455, 95% CI (1.414–21.035), p<0.05) were found to be significantly associated with increased metformin intolerance (Table 3).
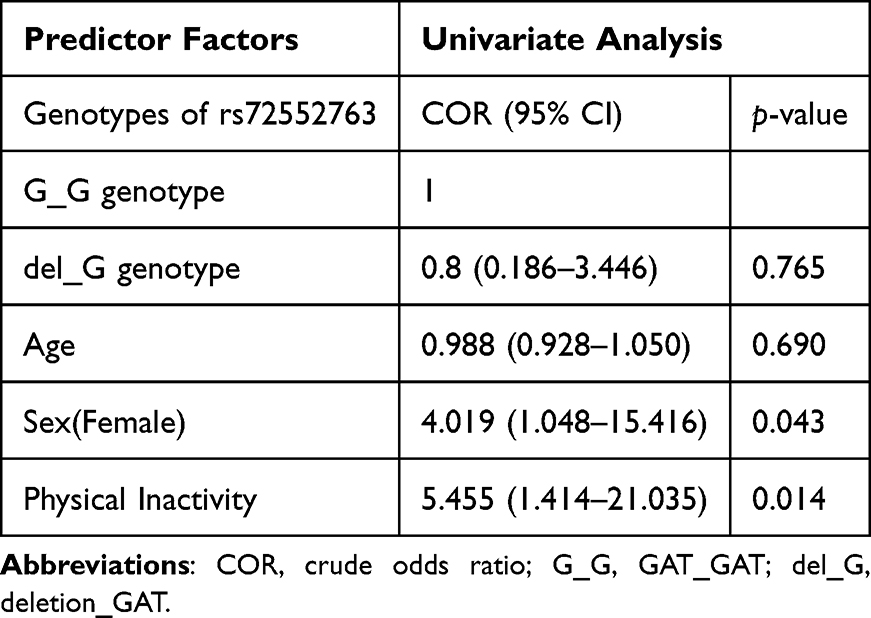 |
Table 3 Logistic Regression Analysis on the Predictors of Metformin Intolerance Among Study Participants (n = 47) |
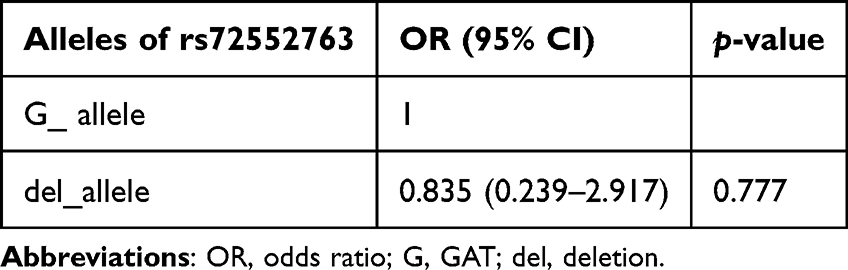 |
Table 4 Chi-Square Test Analysis on the Effect of the Alleles of the rs72552763 Polymorphism on Metformin Intolerance Among Study Participants (n = 47) |
Discussion
In this study, metformin gastrointestinal intolerance was defined in 47 patients with T2DM. Since we involved an individual variant of SLC22A1, the Met420del polymorphism (rs72552763), to associate with metformin gastrointestinal intolerance in our study, intolerance phenotype was defined to include common and/or severe gastrointestinal intolerance, as both share a common underlying mechanism despite the difference in the intensity and duration of the symptoms.29 Moreover, as no study participant was homozygous for the deletion allele in this study, comparison was made between the patient homozygous for the wild-type GAT allele (G_G genotype) and the patient heterozygous for the deletion allele in the association study.
In our study, no significant association was observed between the Met420del variant of SLC22A1 (rs72552763) and metformin intolerance. Indeed, this result is in accordance with earlier finding, which showed that Met420del variant had no association with metformin side-effects, although the same study reported the association of common gastrointestinal side effects of metformin therapy in an individual with reduced function variants of SLC22A1 (rs628031 and rs36056065).14 The findings from two previous studies also showed that individual variants (including rs72552763) were not associated with the occurrence of side effects, though the number of SLC22A1 reduced-function alleles was associated with common gastrointestinal adverse effects to metformin29 and individuals carrying two reduced function SLC22A1 alleles had higher chances of severe intolerance compared with individuals with one or no reduced function alleles.15 In addition, in the same study15 individuals with two SLC22A1 reduced-function alleles receiving treatment with known OCT1 inhibitors exhibited a nearly four times more gastrointestinal intolerance. Collectively, these findings indicate that inadequate SLC22A1 transport appears to be a major contributor to the metformin gastrointestinal intolerance, although there is lack of consistency in the association between individual reduced function SLC22A1 variants and metformin gastrointestinal intolerance. Thus, it is plausible to assume that the combined effect of the reduced function variants of SLC22A1 is valuable to predict metformin induced gastrointestinal adverse effects rather than the individual variants. However, as our study involved only a single reduced functional variant of SLC22A1, Met420del variant, this assumption needs to be confirmed by further studies involving more than one reduced functional variants of the gene. Besides, we assume that the absence of association between Met420del polymorphism and metformin induced gastrointestinal intolerance in our study might be related to the absence of participant who is homozygous for the deletion allele and, most importantly, due to the smaller sample size. Thus, a more complete investigation of SLC22A1 variants would be required to fully assess the effect of the gene on metformin induced gastrointestinal intolerance as several variants with a more severe loss of function have been described.
Furthermore, our study found that the female gender was associated with more than 4 times greater chance of being intolerant to metformin. This finding adds to the previous knowledge that indicated sex-related differences in metformin intolerance.14,15,29 However, further studies are needed to assess the underlying factors for the potential sex differences in metformin intolerance. Moreover, there was a significant difference in the level of physical activity between metformin tolerant and intolerant groups. It is not clear why physical inactivity is related to metformin gastrointestinal intolerance. Further prospective studies are required to confirm this observation. Age appeared to have influence on the occurrence of side effects depending on the time of T2DM diagnosis. Evidence for this assertion comes from the observation that whilst age had significant effect on the occurrence of side effects in patients with a longer duration of T2DM,14,15 it was found to have no association in patients with newly diagnosed T2DM,29 which is concordant with our findings. This might have to do with the fact that both metformin tolerant and intolerant patients had similar age in the current study, as all the study participants were recently diagnosed T2DM individuals.
One of the major limitations of this study is the relatively small sample size. We used the minimum sample size estimated by comparison of two proportion formula. However, more reliable results could have been obtained if we expanded the sample size. Thus, the findings of this study need to be cautiously interpreted and require validation in larger cohort studies involving multiple variants of SLC22A1 gene reported to affect metformin induced gastrointestinal intolerance. We excluded patients on medications, such as proton pump inhibitors and cimetidine that could potentially affect OCT1 in the present study. As a result, how such medications affect the outcome is lacking. Future studies including such factors into account may help to fully establish the effect of the gene on metformin induced gastrointestinal intolerance.
Conclusions
In this study, rs72552763 polymorphism was not significantly associated with metformin induced gastrointestinal intolerance in Ethiopian patients with T2DM. The present study is the first to investigate the association of rs72552763 with metformin intolerance in the Ethiopian population with T2DM. Thus, the finding of this study might provide additional important data that contributes to knowledge synthesis for the Ethiopian and African genetic diversity in terms of metformin associated adverse effects. In our study, we also found that the female gender and physical inactivity were risk factors for metformin induced gastrointestinal intolerance.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We acknowledge Haramaya University, Addis Ababa University (RN: PV 475613/11), CDT-Africa (RN: CDT/2028/22), and the European and Developing Countries Clinical Trials Partnership (EDCTP, Grant No: 2016-1778) for their support for AD in terms of the stipend and/or procurement of study supplies. We would like to thank the University of Malaya, Kuala Lumpur, for granting access to AD to its laboratory and generously providing all materials and reagents needed to conduct DNA isolation and PCR analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35(6):1364–1379. doi:10.2337/dc12-0413
2. Haupt E, Knick B, Koschinsky T, Liebermeister H, Schneider J, Hirche H. Oral antidiabetic combination therapy with sulphonylureas and metformin. Diabete Metab. 1991;17(1 Pt 2):224–231.
3. DeFronzo RA. Pharmacologic therapy for type 2 diabetes mellitus. Ann Intern Med. 1999;131(4):281–303. doi:10.7326/0003-4819-131-4-199908170-00008
4. Overbeek JA, Heintjes EM, Prieto-Alhambra D, et al. Type 2 diabetes mellitus treatment patterns across Europe: a population-based multi-database study. Clin Ther. 2017;39(4):759–770. doi:10.1016/j.clinthera.2017.02.008
5. Lukas L, Andreas M, Willi O, et al. Prescription of oral antidiabetic drugs in Tyrol - Data from the Tyrol diabetes registry 2012–2015. Wien Klin Wochenschr. 2017;129(1–2). doi:10.1007/s00508-016-1135-1
6. Tanabe M, Motonaga R, Terawaki Y, Nomiyama T, Yanase T. Prescription of oral hypoglycemic agents for patients with type 2 diabetes mellitus: a retrospective cohort study using a Japanese hospital database. J Diabetes Investig. 2017;8(2):227–234. doi:10.1111/jdi.12567
7. Holt R. Personalized medicine for diabetes: a special issue. Diabet Med. 2016;33:711. doi:10.1111/dme.13144
8. Pearson ER. Personalized medicine in diabetes: the role of “omics” and biomarkers. Diabet Med J Br Diabet Assoc. 2016;33(6):712–717. doi:10.1111/dme.13075
9. Pawlyk AC, Giacomini KM, McKeon C, Shuldiner AR, Florez JC. Metformin pharmacogenomics: current status and future directions. Diabetes. 2014;63(8):2590–2599. doi:10.2337/db13-1367
10. Todd JN, Florez JC. An update on the pharmacogenomics of metformin: progress, problems and potential. Pharmacogenomics. 2014;15(4):529–539. doi:10.2217/pgs.14.21
11. Dujic T, Zhou K, Yee SW, et al. Variants in pharmacokinetic transporters and glycemic response to metformin: a metgen meta-analysis. Clin Pharmacol Ther. 2017;101(6):763–772. doi:10.1002/cpt.567
12. Hiroshi T, Eriko S, Kenji O, Shun H, Ichiro I. Polymorphism in human organic cation transporters and metformin action. Pharmacogenomics. 2008;9(4). doi:10.2217/14622416.9.4.415
13. Becker ML, Visser LE, van Schaik RHN, Hofman A, Uitterlinden AG, Stricker BHC. Genetic variation in the organic cation transporter 1 is associated with metformin response in patients with diabetes mellitus. Pharmacogenomics J. 2009;9(4):242–247. doi:10.1038/tpj.2009.15
14. Tarasova L, Kalnina I, Geldnere K, et al. Association of genetic variation in the organic cation transporters OCT1, OCT2 and multidrug and toxin extrusion 1 transporter protein genes with the gastrointestinal side effects and lower BMI in metformin-treated type 2 diabetes patients. Pharmacogenet Genomics. 2012;22(9):659–666. doi:10.1097/FPC.0b013e3283561666
15. Dujic T, Zhou K, Donnelly LA, Tavendale R, Palmer CNA, Pearson ER. Association of organic cation transporter 1 with intolerance to metformin in type 2 diabetes: a GoDARTS study. Diabetes. 2015;64(5):1786–1793. doi:10.2337/db14-1388
16. Wilcock C, Bailey CJ. Accumulation of metformin by tissues of the normal and diabetic mouse. Xenobiotica Fate Foreign Compd Biol Syst. 1994;24(1):49–57. doi:10.3109/00498259409043220
17. Khatami F, Mohajeri-Tehrani MR, Tavangar SM. The importance of precision medicine in type 2 diabetes mellitus (T2DM): from pharmacogenetic and pharmacoepigenetic aspects. Endocr Metab Immune Disord Drug Targets. 2019;19(6):719–731. doi:10.2174/1871530319666190228102212
18. Bonnet F, Scheen A. Understanding and overcoming metformin gastrointestinal intolerance. Diabetes Obes Metab. 2017;19(4):473–481. doi:10.1111/dom.12854
19. Díaz-Perdigones CM, Muñoz-Garach A, Álvarez-Bermúdez MD, Moreno-Indias I, Tinahones FJ. Gut microbiota of patients with type 2 diabetes and gastrointestinal intolerance to metformin differs in composition and functionality from tolerant patients. Biomed Pharmacother. 2022;145:112448. doi:10.1016/j.biopha.2021.112448
20. Forslund K, Hildebrand F, Nielsen T, et al. Disentangling type 2 diabetes and metformin treatment signatures in the human gut microbiota. Nature. 2015;528(7581):262–266. doi:10.1038/nature15766
21. Bryrup T, Thomsen CW, Kern T, et al. Metformin-induced changes of the gut microbiota in healthy young men: results of a non-blinded, one-armed intervention study. Diabetologia. 2019;62(6):1024–1035. doi:10.1007/s00125-019-4848-7
22. Rosario D, Benfeitas R, Bidkhori G, et al. Understanding the representative gut microbiota dysbiosis in metformin-treated type 2 diabetes patients using genome-scale metabolic modeling. Front Physiol. 2018;9:775. doi:10.3389/fphys.2018.00775
23. Degaga A, Sirgu S, Huri HZ, et al. Association of Met420del variant of metformin transporter gene SLC22A1 with metformin treatment response in Ethiopian patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2023;16:2523–2535. doi:10.2147/DMSO.S426632
24. Du Plessis M, Pearce B, Jacobs C, Hoosain N, Benjeddou M. Genetic polymorphisms of the organic cation transporter 1 gene (SLC22A1) within the Cape Admixed population of South Africa. Mol Biol Rep. 2015;42(3):665–672. doi:10.1007/s11033-014-3813-2
25. Jacobs C, Pearce B, Du Plessis M, Hoosain N, Benjeddou M. Genetic polymorphisms and haplotypes of the organic cation transporter 1 gene (SLC22A1) in the Xhosa population of South Africa. Genet Mol Biol. 2014;37(2):350–359.
26. Bennett PH. Impact of the new WHO classification and diagnostic criteria. Diabetes Obes Metab. 1999;1(Suppl 2):S1–6. doi:10.1046/j.1463-1326.1999.0010s2001.x
27. Wang H, Chow SC. Sample size calculation for comparing proportions. In: Wiley Encyclopedia of Clinical Trials. John Wiley & Sons, Ltd; 2007. doi10.1002/9780471462422.eoct005
28. Kirpichnikov D, McFarlane SI, Sowers JR. Metformin: an update. Ann Intern Med. 2002;137(1):25–33. doi:10.7326/0003-4819-137-1-200207020-00009
29. Dujic T, Causevic A, Bego T, et al. Organic cation transporter 1 variants and gastrointestinal side effects of metformin in patients with Type 2 diabetes. Diabet Med J Br Diabet Assoc. 2016;33(4):511–514. doi:10.1111/dme.13040
30. Dawed AY, Zhou K, van Leeuwen N, et al. Variation in the Plasma Membrane Monoamine Transporter (PMAT) (Encoded by SLC29A4) and Organic Cation Transporter 1 (OCT1) (Encoded by SLC22A1) and gastrointestinal intolerance to metformin in type 2 diabetes: an IMI direct study. Diabetes Care. 2019;42(6):1027–1033. doi:10.2337/dc18-2182
31. Lim MT, Ab Rahman N, Teh XR, et al. Optimal cut-off points for adherence measure among patients with type 2 diabetes in primary care clinics: a retrospective analysis. Ther Adv Chronic Dis. 2021;12:2040622321990264. doi:10.1177/2040622321990264
32. Seid MA, Akalu Y, Gela YY, et al. Microvascular complications and its predictors among type 2 diabetes mellitus patients at Dessie town hospitals, Ethiopia. Diabetol Metab Syndr. 2021;13:86. doi:10.1186/s13098-021-00704-w
33. Colberg SR, Sigal RJ, Fernhall B, et al. Exercise and Type 2 Diabetes. Diabetes Care. 2010;33(12):e147–e167. doi:10.2337/dc10-9990
34. Miks SBJ Gene-Calc [Computer software]; 2018. Available from: www.gene-calc.pl.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.