Back to Journals » International Journal of General Medicine » Volume 19
Association of the National Database Code “General Anesthesia” and Mechanical Ventilation with New-Onset Neuro-Psychiatric Medication Use in Sepsis Survivors Aged ≥90 Years: A Nationwide Retrospective Cohort Study
Authors Shimoyama Y, Kadono N, Umegaki O
Received 17 March 2026
Accepted for publication 15 May 2026
Published 19 May 2026 Volume 2026:19 609863
DOI https://doi.org/10.2147/IJGM.S609863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Woon-Man Kung
Yuichiro Shimoyama,1,2 Noriko Kadono,1,2 Osamu Umegaki1,2
1Department of Anesthesiology, Osaka Medical and Pharmaceutical University, Takatsuki, Osaka, Japan; 2Intensive Care Unit, Osaka Medical and Pharmaceutical University Hospital, Takatsuki, Osaka, Japan
Correspondence: Yuichiro Shimoyama, Intensive Care Unit, Osaka Medical and Pharmaceutical University Hospital, 2-7 Daigaku-machi, Takatsuki, Osaka, 569-8686, Japan, Tel +81-72-683-1221, Fax +81-72-684-6547, Email [email protected]
Purpose: As the global population ages, Post-Intensive Care Syndrome (PICS) has emerged as a critical public health concern. However, in sepsis survivors aged 90 years or older, the etiology of cognitive and mental decline remains obscured by the natural aging process. A pivotal unresolved debate in critical care is distinguishing whether this neuro-psychiatric decline is driven by “mechanical ventilation” (associated with sedation and immobilization) or “general anesthesia” (representing surgical stress and systemic inflammation). This study aimed to evaluate the association of the National Database (NDB) codes for general anesthesia and mechanical ventilation with the new-onset neuro-psychiatric medication use in sepsis survivors aged ≥ 90 years.
Patients and Methods: In this retrospective cohort study using the National Database of Japan, we identified a previously independent cohort of sepsis survivors aged ≥ 90 years without prior psychotropic use or home care. The primary outcome was new CNS-active medication initiation within 6 months. We performed multivariate logistic regression, utilizing Variance Inflation Factor (VIF) analysis to mathematically rule out multicollinearity between anesthesia and ventilation.
Results: Among 269 strictly selected independent survivors, 83 (30.9%) initiated new CNS-active medications. VIF analysis confirmed the complete statistical independence of the two factors (VIF < 1.02). General anesthesia independently predicted the outcome (Odds Ratio [OR] 1.85; 95% CI 1.05– 3.25; P = 0.032), whereas mechanical ventilation did not (OR 0.82; P = 0.502). Phenotypic analysis revealed general anesthesia shifted risks toward sleep-wake (50.0%) and sensory dysregulation (43.8%) rather than frank dementia (27.3%). Furthermore, general anesthesia was associated with a significant concurrent loss of physical and mental autonomy (P = 0.036).
Conclusion: Supported by VIF analysis, the general anesthesia code was independently associated with systemic neuro-vulnerability in nonagenarians. Surgical stress is specifically associated with a phenotypic shift toward sleep and sensory dysregulation and concurrent loss of autonomy, necessitating a paradigm shift in surgical decision-making.
Plain Language Summary: Sepsis is a severe, life-threatening condition. In very old patients (aged 90 or older), surviving sepsis often comes with a decline in mental health or cognitive function. It has been unclear whether this decline is caused by the surgical stress of “general anesthesia” or the “mechanical ventilation” used during intensive care. In this study, we looked at a nationwide database in Japan to examine 269 sepsis survivors aged 90 or older who were completely independent before their illness. We found that receiving general anesthesia significantly increased the risk of needing new psychiatric medications—specifically for sleep and sensory issues like pain—after recovery. Mechanical ventilation did not show this effect. Our findings suggest that surgery itself is a significant physiological stressor associated with a devastating loss of autonomy in extremely old patients, highlighting the need for careful decision-making before surgery.
Keywords: post-intensive care syndrome, PICS, nonagenarians, sepsis, general anesthesia, sleep disorders
Introduction
The “Hidden” PICS and the Challenge of the Oldest-Old
Driven by rapid global population aging, the number of patients aged 90 and older admitted to Intensive Care Units (ICUs) is increasing globally.1 For these survivors, Post-Intensive Care Syndrome (PICS) poses a devastating threat to their remaining quality of life.2 While physical impairments (PICS-Physical) are often visibly apparent, cognitive and mental health impairments (PICS-CI/MH) frequently remain “hidden”. In this oldest-old population, new-onset cognitive decline or depressive symptoms are often dismissed by clinicians and families as inevitable consequences of aging (“senescence”) rather than recognized as iatrogenic sequelae of acute care.3 However, for previously independent and medication-free patients—those who have maintained complete independence without medication until the age of 90—losing their mental autonomy due to medical intervention is a preventable tragedy that warrants urgent investigation.
General Anesthesia vs Mechanical Ventilation: A Statistical Dilemma
A critical unresolved question in critical care medicine is the etiology of this decline.4,5 Conventionally, the primary culprit for post-ICU cognitive dysfunction has been attributed to “sedation and immobilization” associated with mechanical ventilation, as emphasized by the ABCDEF bundle initiatives.6 However, in the management of sepsis, mechanical ventilation (medical care) and general anesthesia (surgical intervention) often coexist, making it notoriously difficult to disentangle their independent effects. Previous studies have often treated “ICU admission” as a monolithic exposure,4,5 failing to distinguish the distinct neurocognitive effects of surgical trauma (systemic inflammation, oxidative stress) versus critical care management per se. Specifically, does the aging brain suffer more from the prolonged sedation required for the ventilator, or from the acute neuroinflammatory insult caused by surgical intervention?
Beyond Dementia: Defining the Spectrum of “Neuro-Vulnerability”
Surgical stress does not solely cause dementia. Emerging evidence suggests it induces systemic neuro-inflammation and blood-brain barrier disruption that can manifest as a broader spectrum of “Neuro-Vulnerability”, including disrupted sleep architecture (insomnia) and sensitized pain pathways (neuropathic pain or sensory dysregulation).7–9 Crucially, for the nonagenarian brain, the inability to maintain sleep-wake rhythms or regulate sensory input signifies a critical breakdown of neural homeostasis.10 Therefore, focusing research solely on anti-dementia drugs might underestimate the true burden of surgical stress, as it would overlook these valid manifestations of neuro-homeostatic collapse. Conversely, simply labeling all psychotropic use as “bad” ignores the nuance of appropriate symptom management in modern geriatrics.11
This study aims to address these gaps with two specific objectives: (1) To statistically separate the association of General Anesthesia vs Mechanical Ventilation using a composite endpoint strictly verified by VIF analysis, and (2) To perform detailed phenotyping to determine whether surgical stress drives frank dementia or specific functional disorders like insomnia and pain, providing a comprehensive map of post-surgical sequelae in patients aged ≥ 90 years. While general anesthesia and mechanical ventilation often clinically co-occur, making their independent effects notoriously difficult to separate, we strictly isolated them in this study using Variance Inflation Factor (VIF) analysis to rule out multicollinearity.
Methods
Study Population and Strict Selection of an Independent Cohort
This study was conducted and reported in accordance with the STROBE statement. This study employed a retrospective cohort design utilizing the National Database of Health Insurance Claims and Specific Health Checkups of Japan (NDB). The NDB is a comprehensive administrative database managed by the Ministry of Health, Labour and Welfare (MHLW), which aggregates more than 98% of all medical claims data issued by medical institutions nationwide under Japan’s universal health insurance system.12,13
The analysis period covered medical claims from October 2015 to March 2020. To ensure the accuracy of baseline characteristic assessment and the rigorous application of exclusion criteria, we obtained data starting from April 2015. The period from April 2015 to September 2015 served as a designated 6-month washout period, allowing us to identify and exclude patients with pre-existing conditions or treatments.
This study protocol was reviewed and approved by the Institutional Review Board of Osaka Medical and Pharmaceutical University (Approval No. 2871–2). Given the retrospective nature of the study and the use of anonymized administrative data, the requirement for individual informed consent was waived in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan.
To ensure high data quality and diagnostic accuracy, we restricted our analysis to patients aged ≥ 90 admitted to ICUs claiming the “Specific Intensive Care Unit Management Fee” (Tokutei Shuchu Chiryo Shitsu Kanriryou). In the Japanese medical fee schedule, facilities eligible to claim this fee must meet stringent structural and staffing criteria, including a nurse-to-patient ratio of 1:2 or higher and the mandatory placement of board-certified intensive care specialists. This criterion effectively serves as a quality filter, ensuring that the diagnosis of sepsis and the subsequent critical care management were conducted according to standard clinical guidelines. All cases included in this cohort were identified based on the index admission codes for sepsis management upon ICU entry.
Sepsis was defined based on ICD-10 codes recorded in the claims data, consistent with the definition (Sepsis-3)14 and the methodology of our previous report.15 We operationally defined individuals who have successfully aged without any medical dependency as the previously independent and medication-free cohort. To establish this rigorous baseline, we applied strict exclusion criteria. We rigorously excluded any patients who had claims for home medical care, rehabilitation, or any psychiatric medications (including antipsychotics, antidepressants, anxiolytics, and anti-dementia drugs) in the 6 months prior to ICU admission. This procedure was essential to eliminate confounding by pre-existing frailty or cognitive decline, ensuring that the observed outcomes were truly new-onset sequelae.
Composite Outcome and Variable Selection Logic
Due to the nature of administrative claims data lacking direct cognitive or functional testing scores, the primary outcome was defined as the “New Initiation of CNS-Active Medications” (including antipsychotics, antidepressants, anxiolytics, anti-dementia drugs, hypnotics, and neuropathic pain modulators acting as a validated surrogate for significant neuro-psychiatric sequelae requiring clinical intervention, within 6 months after ICU admission. We performed multivariate logistic regression analysis to identify independent predictors.
Rationale for Variable Selection: The selection of independent variables was strictly predetermined based on the following two criteria to ensure scientific rigor and comparability:
- Consistency with our First Report: We intentionally utilized the exact same set of variables as in our previous study on physical outcomes.15 This methodological consistency allows for a direct and robust comparison of risk factors between “PICS-Physical” (Body) and “PICS-Mental” (Brain) within the same cohort aged ≥ 90 years, facilitating a holistic understanding of PICS.
- Clinical Plausibility: We included General Anesthesia and Mechanical Ventilation to statistically disentangle the effects of surgical stress from medical critical care. In the Japanese NDB claims system, there is no single, universal code for “surgery” that effectively captures the highest level of surgical stress; therefore, we utilized the “General Anesthesia” code as a robust surrogate to identify major surgical procedures requiring systemic management. Dyslipidemia and Liver Dysfunction were retained to evaluate the contribution of “Vascular Vulnerability” and the “Liver Paradox”, respectively, based on our prior hypotheses.15 Age was included as a fundamental demographic adjuster.
This parsimonious model (5 variables for 83 events) satisfied the widely accepted “10 Events Per Variable” (EPV) rule,16 safeguarding against model overfitting and ensuring the reliability of the calculated Odds Ratios.
Statistical Validation: The Role of VIF
A major methodological challenge in separating surgical and medical effects is multicollinearity (eg, surgical patients frequently require postoperative ventilation). To address this, we explicitly calculated the Variance Inflation Factor (VIF) for all independent variables.17 A VIF value < 2.0 (ideally near 1.0) indicates the absence of problematic multicollinearity. This step was crucial to mathematically confirm that General Anesthesia and Mechanical Ventilation could be treated as statistically independent risk factors in our model.
For sub-group comparisons (Phenotype Shift and Double Hit analysis), we utilized Fisher’s exact test to assess statistical significance between the General Anesthesia and non-General Anesthesia groups.
Phenotypic Subgroup Analysis
To clarify the clinical nature of the outcome, we categorized the “Cognitive/Neuro-modulating” subgroup into three mutually exclusive groups. To handle potential overlap, we applied a strict hierarchical classification rule based on clinical severity:
- Group 1 (True PICS): Patients initiating anti-dementia drugs (eg, donepezil), representing cognitive failure (classified regardless of concurrent hypnotics or pain modulators).
- Group 2 (Isolated Sleep Dysfunction): Patients initiating hypnotics (specifically orexin antagonists) without anti-dementia drugs, representing isolated sleep-wake rhythm disorders.
- Group 3 (Neuropathic Pain Phenotype): Patients initiating neuropathic pain modulators (eg, pregabalin, mirogabalin) without anti-dementia drugs or hypnotics. Note: To capture a broader spectrum of central sensory/neural dysregulation, this category also included a very small number of patients prescribed neuroprotective agents (edaravone) or central antipruritic agents (nalfurafine). However, the vast majority of this group consisted of patients treated for neuropathic pain.
We visualized the prevalence of general anesthesia in each group to identify phenotype-specific risks. Furthermore, to assess the systemic consequences of surgery, we categorized patients into those maintaining baseline autonomy (neither), those with a partial decline (drug or home care), and those with a concurrent decline in physical and mental autonomy (both), visualizing the collapse of autonomy.
Statistical significance was defined as a two-sided P-value < 0.05. Data reporting adhered to NDB privacy regulations; counts less than 10 were suppressed or aggregated, and age was categorized into 5-year increments. All statistical analyses were performed using JMP software version 11.0.0 (SAS Institute Inc, Cary, NC).
Results
Study Population and Screening Process
From the comprehensive NDB dataset covering the specified period, we initially screened approximately 14.1 billion records, identifying 860 candidates aged ≥ 90 with sepsis. Following the rigorous application of exclusion criteria to identify the previously independent and medication-free phenotype (no prior home medical care, rehabilitation, or psychotropic or anti-dementia medications), 269 patients were included in the final analysis (Figure 1). The baseline characteristics of the overall cohort are presented in Table 1. This rigorous selection process highlights the rarity of truly independent individuals in this age group. Among these 269 previously independent patients, 83 (30.9%) met the definition for the composite outcome (Figure 1). As shown in Table 2, the baseline demographic and clinical characteristics were well-balanced between the General Anesthesia group and the Mechanical Ventilation group, with no significant differences in comorbidities (all P > 0.05).
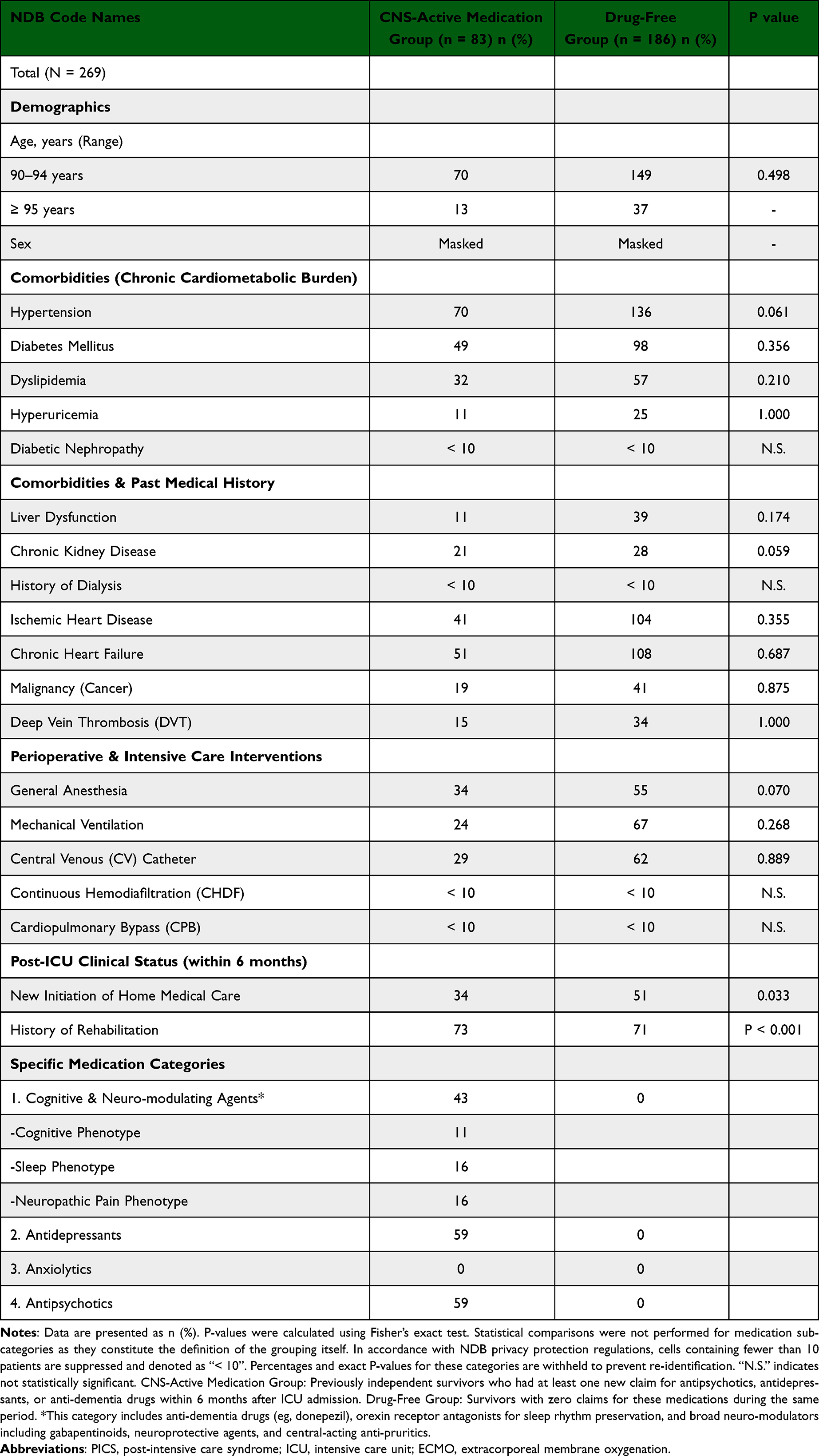 |
Table 1 Baseline Characteristics and Post-ICU Outcomes |
 |
Table 2 Baseline Demographic and Clinical Characteristics of Sepsis Survivors Aged ≥90 Years, Stratified by Exposure to General Anesthesia or Mechanical Ventilation |
 |
Figure 1 Study Flow Diagram. Flowchart illustrating the selection process of the previously independent cohort from the National Database of Japan (NDB). From an initial screening of approximately 14.1 billion records, 860 sepsis patients aged ≥ 90 were identified. After applying strict exclusion criteria to eliminate pre-existing medical dependency (home medical care, rehabilitation, psychotropic medications), 269 patients were included in the final analysis. The composite outcome occurred in 83 patients (30.9%). Abbreviation: PICS-CI/MH, post-intensive care syndrome-cognitive impairment/mental health. |
Multivariate Analysis: General Anesthesia vs Mechanical Ventilation
Among 269 survivors, 83 (30.9%) initiated new CNS-active medications. Multivariate analysis revealed that General Anesthesia was a significant independent risk factor (OR 1.85; 95% CI 1.05–3.25; P = 0.032). In stark contrast, Mechanical Ventilation showed no significant association with the outcome (OR 0.82; 95% CI 0.46–1.47; P = 0.502) (Table 3).
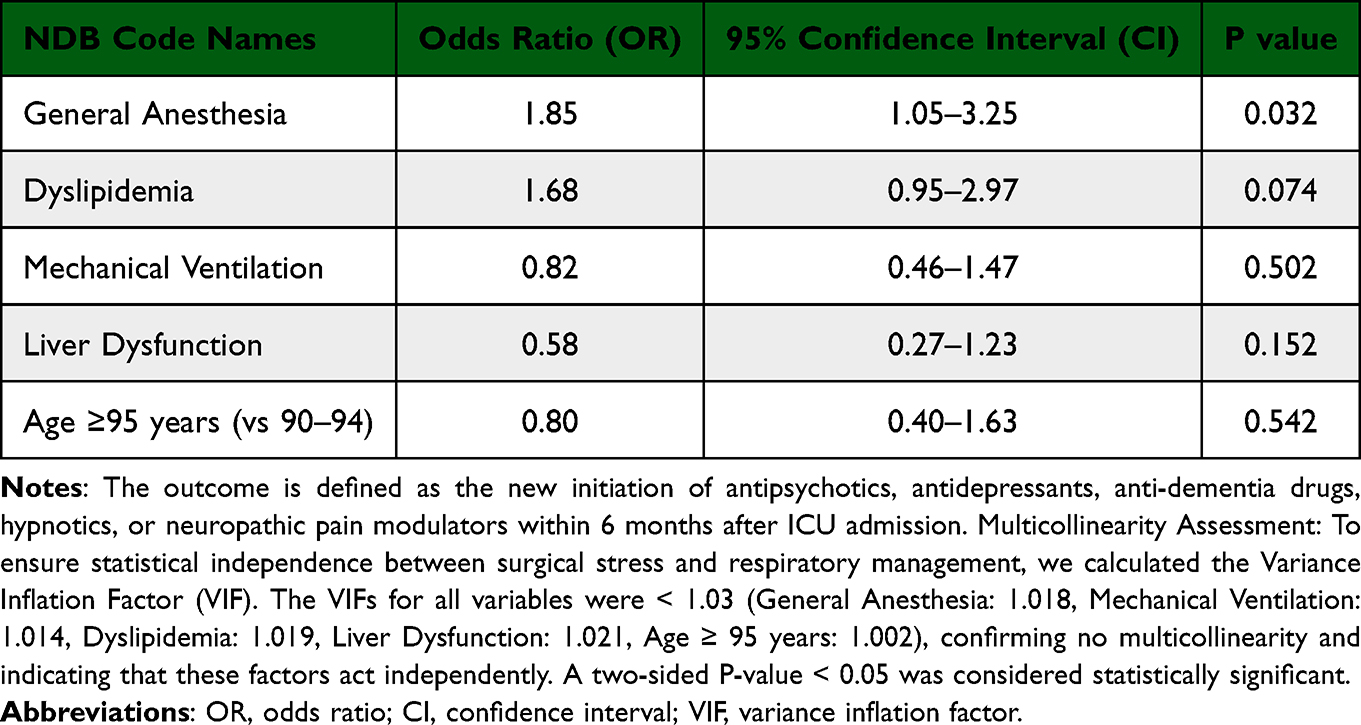 |
Table 3 Multivariate Logistic Regression Analysis for Predictors of New-Onset CNS-Active Medication Initiation |
Multicollinearity Assessment
A critical finding of this study is the result of the VIF analysis. The VIF values for General Anesthesia and Mechanical Ventilation were 1.018 and 1.014, respectively. These extremely low values (far below the threshold of 2.0 or 5.0) mathematically prove that the statistical contribution of surgical stress was distinct from that of respiratory support in our cohort. This validates that the observed risk is attributable to the surgery itself, not the concurrent ICU care.
Metabolic Factors
Dyslipidemia showed a strong trend toward increased risk (OR 1.68; 95% CI 0.95–2.97; P = 0.074), while Liver Dysfunction showed a protective trend (OR 0.58; 95% CI 0.27–1.23; P = 0.152) (Table 3). These findings perfectly mirror the “Liver Paradox” pattern observed in our first report on physical outcomes.15
The Phenotype Shift
Analysis of the “Cognitive/Neuro-modulating” category (n = 43) revealed a striking disparity in general anesthesia prevalence across phenotypes. Phenotypic analysis revealed a specific phenotypic shift:
General anesthesia prevalence was numerically higher in the Insomnia phenotype (50.0%; P = 0.099 vs Control) and Neuropathic Pain phenotype (43.8%; P = 0.26), suggesting a trend toward sleep-sensory dysregulation. Notably, in the Insomnia phenotype (n = 16), all patients were prescribed orexin receptor antagonists, with a zero incidence of new benzodiazepine initiation. In stark contrast, in the Dementia phenotype (27.3%), the prevalence was statistically identical to the drug-free control group (29.6%; P = 1.00). All comparisons were performed using Fisher’s exact test.
This data suggests that while general anesthesia is associated with the overall composite outcome, it is specifically linked to sleep and sensory dysregulation rather than frank dementia in this cohort.
Concurrent Decline in Physical and Mental Autonomy
The analysis of systemic autonomy revealed devastating systemic consequences associated with surgery. Patients who underwent general anesthesia (n = 89) had a significantly lower rate of maintaining their baseline independent status (38.2% vs 56.1%; P = 0.023) compared to those who did not (n = 180). Conversely, the rate of concurrent decline in physical and mental autonomy (requiring both new CNS drugs and home medical care) was significantly higher in the anesthesia group (16.9% vs 10.6%; P = 0.036). This indicates that surgical stress is associated with a simultaneous loss of mental and physical autonomy.
Discussion
General Anesthesia as a Significant Systemic Stressor (Validated by VIF)
Our findings fundamentally refine the understanding of PICS in patients aged ≥ 90 years. General anesthesia predicted new CNS medication needs, independent of mechanical ventilation. Crucially, the true negative association of General Anesthesia, which might have been obscured in unadjusted comparisons, was likely unmasked by adjusting for Liver Dysfunction (which acted as a protective factor) and other confounders. The extraordinarily low VIF values (< 1.02) critically validate this finding, confirming that the observed risk is not a statistical artifact or a confounding product of ICU sedation. This robustness allows us to conclude that for the nonagenarian brain, the acute insult of surgery—likely via systemic inflammation and oxidative stress18—is a distinct and more potent stressor than the prolonged immobilization of critical care. It is crucial to clarify that we utilized “General Anesthesia” as a surrogate marker for the “composite burden” of surgical intervention. The observed risk likely reflects the systemic burden of surgical stress (tissue injury, inflammation) rather than the direct pharmacological toxicity of anesthetic agents alone.19 Furthermore, while some anesthetic agents such as propofol or volatile anesthetics may possess anti-inflammatory and neuroprotective properties that could partially mitigate ischemic or inflammatory injury, our findings indicate that the overwhelming systemic burden of the surgical procedure itself outweighs these potential protective pharmacological effects.
Association of General Anesthesia with a “Phenotype Shift” Toward Homeostatic Breakdown
Phenotypic analysis revealed a nuanced landscape. The risk of psychotropic initiation was predominantly observed in Insomnia (Group 2; 50% GA rate) and Neuropathic Pain (Group 3; 44% GA rate), whereas the risk for True Dementia (Group 1; 27% GA rate) was indistinguishable from baseline aging. This implies that surgical stress triggers a phenotypic shift toward neuro-functional dysregulation (sleep-wake cycles, sensory processing) rather than immediate neurodegeneration. Critics might argue that insomnia or sensory disorders are less severe than dementia. However, in this age group, the inability to maintain sleep-wake rhythms implies a breakdown of neural homeostasis.10,20 Furthermore, the use of neuropathic pain modulators (eg, pregabalin) in the post-acute phase (new initiation) suggests the development of central sensitization or chronic post-surgical pain, distinct from acute nociceptive pain.21 Clinically, this is vital: many patients labeled as “demented” post-surgery may actually be suffering from treatable, surgically-induced functional disorders.
The “High Quality Care” Paradox
Group 2 (n = 16) represents a critical finding. These patients, suffering from surgically induced insomnia, were managed with orexin antagonists (avoiding benzodiazepines). The zero prescription rate of benzodiazepines in our cohort reflects “High Quality Care” and adherence to safety guidelines.22 However, the necessity for this care is a direct sequela of the surgery. This creates a paradox: while clinicians are successfully preventing the transition to delirium or frank dementia through appropriate medication, the underlying “Sleep Vulnerability” remains an iatrogenic sequela of surgical intervention.
Concurrent Decline in Physical and Mental Autonomy
As shown in Figure 2, the association of general anesthesia extends beyond the brain. Over 60% of patients exposed to surgery lost some form of autonomy (Single or Double Hit). Specifically, the 1.6-fold increase in the concurrent decline of physical and mental autonomy challenges the notion that surgery is a localized treatment. For these patients, surgical stress is significantly associated with a concurrent decline in mental independence (drug dependency) and physical independence (home care). This systemic decline cuts deeper than mechanical ventilation, which showed no such association.
 |
Figure 2 Concurrent Decline in Physical and Mental Autonomy after General Anesthesia Stacked bar chart illustrating the systemic loss of autonomy in sepsis survivors aged ≥ 90 years (N = 269), stratified by exposure to general anesthesia. Patients were categorized into three mutually exclusive outcomes based on their post-discharge status relative to the baseline independent status: Follow-up Independent (Green): Maintained complete Independence (no new medications, no home care). Partial Decline (Orange): Lost partial autonomy, requiring either new psychotropic medications or new home medical care. Concurrent Decline (Red): Experienced a concurrent decline, requiring both new psychotropic medications and new home medical care. Statistical Analysis: Fisher’s exact test revealed a statistically significant shift away from the baseline independent status in the general anesthesia group. The risk of transitioning to both a partial decline (P = 0.023) and a concurrent decline (P = 0.036) was significantly higher compared to the no-anesthesia group. Specifically, general anesthesia was associated with a 1.6-fold increase in the concurrent decline rate (16.9% vs 10.6%) and a marked reduction in the likelihood of maintaining independence (38.2% vs 56.1%). |
Brain-Body Link: Vascular Vulnerability and the Liver Paradox
The metabolic findings reinforce our “Brain-Body Link” hypothesis. Dyslipidemia tended to increase risk (OR 1.68), likely reflecting systemic “Vascular Vulnerability” and endothelial dysfunction that extends to the neurovascular unit.23,24 Conversely, Liver Dysfunction showed a protective trend (OR 0.58), consistent with the “Liver Paradox” (deprescribing bias) observed in our first report.15 This “protective” trend likely reflects “Deprescribing Bias”, where clinicians avoid CNS-active drugs in hepatically impaired patients due to concerns about reduced clearance, rather than a true biological advantage.25,26 These consistent patterns across both physical and mental outcomes suggest that physiological reserve (Liver) and vascular health (Lipid) are universal determinants of post-ICU trajectories. Furthermore, as these metabolic correlations mirror our previous unpublished report,15 these specific findings should be considered preliminary.
Strengths and Limitations
While this study utilizes a unique, nationwide previously independent cohort to minimize baseline confounding, several limitations must be acknowledged. First, as a retrospective observational study using administrative claims data (NDB), we could not access granular clinical data such as SOFA scores or specific laboratory values (eg, albumin, bilirubin levels). However, we mitigated this by strictly selecting baseline independent patients, effectively homogenizing the baseline physiological reserve. Second, although VIF analysis confirmed statistical independence, “General Anesthesia” serves as a surrogate for the comprehensive burden of surgery (tissue injury, inflammation) rather than isolating the effect of anesthetic agents per se. Third, the causality between surgery and the concurrent decline outcome remains associative; unmeasured confounders such as intraoperative hypotension or specific surgical complications could not be fully adjusted.
Fourth, regarding the phenotypic sub-analysis, the sample sizes of the subgroups were limited (eg, Dementia: n=11). Although statistical significance was limited by the small sample size (Type II error), the distinct contrast in P-values (Insomnia P=0.099 vs Dementia P=1.00) supports a specific phenotypic shift. Therefore, these phenotypic findings should be interpreted as exploratory and hypothesis-generating, requiring confirmation in larger cohorts.
Finally, the competing risk of death must be considered. Patients who died shortly after discharge might have been misclassified into the “Drug-Free” group due to a lack of opportunity for prescription. However, if surgical stress correlates with higher mortality, this attrition would bias the results toward the null, effectively underestimating the true negative association of general anesthesia. Thus, the observed significant association represents a conservative and robust estimate. As the study is limited to the Japanese population, generalizability to other healthcare systems requires validation. Due to strict NDB regulations to prevent re-identification of this extremely rare cohort (≥ 90 years), sex data was masked.
Conclusion
In previously independent sepsis survivors aged ≥ 90, general anesthesia is associated with a specific phenotypic shift toward sleep-wake and sensory dysregulation (“Isolated Sleep/Pain Dysfunction”) rather than frank dementia (“True PICS”). This conclusion is statistically robust, as VIF analysis rigorously ruled out multicollinearity with mechanical ventilation. Furthermore, surgical stress is often associated with a devastating concurrent loss of both mental and physical autonomy. Prevention strategies must shift from simply minimizing sedation to strictly scrutinizing surgical indications, weighing the benefit of survival against the significant risk of losing total autonomy.
Abbreviations
PICS, Post-intensive care syndrome; ICU, Intensive care unit; NDB, National Database of Health Insurance Claims and Specific Health Checkups of Japan; MHLW, Ministry of Health, Labour and Welfare; CNS, Central nervous system; VIF, Variance Inflation Factor; OR, Odds ratio; CI, Confidence interval; ECMO, Extracorporeal membrane oxygenation; GA, General anesthesia; PICS-CI/MH, Post-intensive care syndrome-cognitive impairment/mental health.
Data Sharing Statement
The data that support the findings of this study are available from the Ministry of Health, Labour and Welfare (MHLW) of Japan, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are strictly controlled under the “Act on Assurance of Medical Care for Elderly People” to protect personal information and cannot be shared by the authors. Researchers who meet the criteria for data access may apply directly to the MHLW for access to the NDB data.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of Osaka Medical College (currently Osaka Medical and Pharmaceutical University; Osaka, Japan). Given the retrospective nature of the study and the use of anonymized administrative data, the requirement for individual informed consent was waived in accordance with the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan. The study was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki). All methods were carried out in accordance with relevant guidelines and regulations.
Acknowledgments
We would like to express our deepest gratitude to Lecturer Sayuri Shimizu (Department of Health Data Science, Yokohama City University) for her invaluable advice regarding the study design and the application process for the National Database of Japan (NDB), and fcuro Co., Ltd. (Japan) for technical assistance with the extraction and processing of the NDB data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by JSPS KAKENHI Grant Number JP21K09088.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Guidet B, de Lange DW, Boumendil A, et al. The “Silver Tsunami”: sepsis in the oldest old. Intensive Care Med. 2019;45(1):110–12. doi:10.1007/s00134-018-5462-8
2. Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med. 2012;40(2):502–509. doi:10.1097/CCM.0b013e318232da75
3. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911–922. doi:10.1016/S0140-6736(13)60688-1
4. Ehlenbach WJ, Hough CL, Crane PK, et al. Association between acute care and dementia in older adults. JAMA. 2010;303(16):1632–1640. doi:10.1001/jama.2010.167
5. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med. 2013;369(14):1306–1316. doi:10.1056/NEJMoa1301372
6. Pun BT, Balas MC, Barnes-Daly MA, et al. Caring for critically Ill patients with the ABCDEF bundle: results of the ICU liberation collaborative in over 15,000 adults. Crit Care Med. 2019;47(1):3–14. doi:10.1097/CCM.0000000000003482
7. Evered L, Silbert B, Knopman DS, et al. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery-2018. Br J Anaesth. 2018;121(5):1005–1012. doi:10.1016/j.bja.2017.11.087
8. Terrando N, Eriksson LI, Ryu JK, et al. Resolving postoperative neuroinflammation and cognitive decline. Ann Neurol. 2011;70(6):986–995. doi:10.1002/ana.22664
9. Alam A, Hana Z, Jin Z, Suen KC, Ma D. Surgery, neuroinflammation and cognitive impairment. EBioMedicine. 2018;37:547–556. doi:10.1016/j.ebiom.2018.10.021
10. Suen J, Cholico GN, Isho NF, et al. Circadian rhythms, sleep, and cognitive decline in the elderly. Front Aging Neurosci. 2020;12:256. doi:10.3389/fnagi.2020.00256
11. Page AT, Potter K, Clifford R, Etherton-Beer C. Deprescribing in older people. Maturitas. 2016;91:115–128. doi:10.1016/j.maturitas.2016.06.006
12. Ministry of Health, Labour and Welfare (MHLW). National database of health insurance claims and specific health checkups of Japan (NDB). Available from: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/kenkou_iryou/iryouhoken/zenseido/ndb/index_00001.html.
13. Kubo S, Nishioka Y, Noda T, et al. The national database of health insurance claims and specific health checkups of Japan (NDB): a comprehensive review. J Epidemiol. 2018;28(Suppl_III):S1–S28. doi:10.2188/jea.JE20170242
14. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
15. Shimoyama Y, Kadono N, Umegaki O. Iatrogenic and metabolic factors associated with new-onset home medical care in “Super-Normal” sepsis patients aged ≥ 90: a nationwide study. [Submitted].
16. Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol. 2007;165(6):710–718. doi:10.1093/aje/kwk052
17. O’brien RM. A caution regarding rules of thumb for variance inflation factors. Qual Quant. 2007;41(5):673–690. doi:10.1007/s11135-006-9018-6
18. Vutskits L, Xie Z. Lasting impact of general anaesthesia on the brain: mechanisms and relevance. Nat Rev Neurosci. 2016;17(11):705–717. doi:10.1038/nrn.2016.128
19. Brown EN, Pavone KJ, Naranjo M. Multimodal general anesthesia: theory and practice. Anesth Analg. 2018;127(5):1246–1258. doi:10.1213/ANE.0000000000003668
20. Pisani MA, Friese RS, Gehlbach BK, Schwab RJ, Weinhouse GL, Jones SF. Sleep in the intensive care unit. Am J Respir Crit Care Med. 2015;191(7):731–738. doi:10.1164/rccm.201411-2099CI
21. Colloca L, Ludman T, Bouhassira D, et al. Neuropathic pain. Nat Rev Dis Primers. 2017;3(1):17002. doi:10.1038/nrdp.2017.2
22. American Geriatrics Society Beers Criteria Update Expert Panel. 2019 updated AGS beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
23. Iadecola C. The pathobiology of vascular dementia. Neuron. 2013;80(4):844–866. doi:10.1016/j.neuron.2013.10.008
24. Choutka J, Jansky P, Dvorak J, et al. Endothelial dysfunction in sepsis: a narrative review. Front Immunol. 2018;9:1063. doi:10.3389/fimmu.2018.01063
25. Strasser F, Blum D, von Moos R, et al. The effect of liver dysfunction on drug metabolism in the elderly. Expert Opin Drug Metab Toxicol. 2012;8(5):567–578.
26. Page AT, Clifford RM, Potter K, Schwartz D, Etherton-Beer CD. The feasibility and effect of deprescribing in older adults on mortality and health: a systematic review. Br J Clin Pharmacol. 2016;82(3):583–623. doi:10.1111/bcp.12975
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.