Back to Journals » Risk Management and Healthcare Policy » Volume 16
Association of Systemic Immune-Inflammation Index with Non-Alcoholic Fatty Liver Disease: A Population-Based Cross-Sectional Study
Authors Zhao B ![]() , Liu Y, Yang Y, He J
, Liu Y, Yang Y, He J
Received 28 April 2023
Accepted for publication 18 July 2023
Published 16 August 2023 Volume 2023:16 Pages 1581—1592
DOI https://doi.org/10.2147/RMHP.S419183
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Bi Zhao,1 Yuee Liu,2 Yi Yang,3 Jihui He1
1Department of Gastroenterology, Jinshan Branch of Shanghai Sixth People’s Hospital, Shanghai, 201500, People’s Republic of China; 2Department of Emergency, Changhai Hospital, Shanghai, 200433, People’s Republic of China; 3Department of Emergency, Ruijin Hospital and Luwan Branch, School of Medicine, Shanghai Jiaotong University, Shanghai, 200020, People’s Republic of China
Correspondence: Bi Zhao, Department of Gastroenterology, Jinshan Branch of Shanghai Sixth People’s Hospital, Shanghai, 201500, People’s Republic of China, Email [email protected]
Background: The aim of this study was to explore the relationship between systemic immune-inflammation (SII) index with non-alcoholic fatty liver disease (NAFLD) in the general population of the United States (U.S.).
Methods: We conducted a cross-sectional study of subjects in the National Health and Nutrition Examination Survey 2017– 2018. For the analysis of the association between SII index and risk of NAFLD, the restricted cubic spline (RCS) plot, we performed multivariable logistic regression models and subgroup analysis. In addition, generalized additive models with smooth functions were conducted for the relationship between the SII index and the ZJU index, the BARD score, and the NAFLD fibrosis score.
Results: There were a total of 1197 individuals in our study. Taking into account known confounding variables, compared with the lowest quartiles, the odds ratios with 95% confidence intervals for NAFLD across the quartiles were 0.923 (0.585, 1.455), 0.563 (0.351, 0.901), and 1.061 (0.669, 1.682), respectively. As shown by the RCS plot, the SII index was linked with NAFLD risk in a U-shaped pattern. Based on the results of subgroup analysis, SII index and NAFLD risk were U-curve correlated among participants in all age groups, male or female, with or without hypertension, with diabetes mellitus, and with a BMI of < 30 or > 30 kg/m2. The SII index was linearly positive with the ZJU index but negative with the NAFLD fibrosis score. However, the SII index and BARD score showed a trend of first decreasing, then increasing, and then decreasing.
Conclusion: The U-shaped relationships exist between SII index and risk of NAFLD, which highlighted that we should focus on the dynamic change of SII index.
Keywords: cross-sectional study, non-alcoholic fatty liver disease, systemic immune-inflammation index, United States
Introduction
Non-alcoholic fatty liver disease (NAFLD) is a clinical syndrome characterized by steatosis of the liver cells and excessive accumulation of lipids without any previous history of excessive alcohol consumption.1 The incidence of NAFLD continues to increase year by year due to changes in lifestyle, diet structure, reduced physical activity, and an accelerated pace of life, which has become a global public health concern.2 The exact incidence of NAFLD is unknown. The prevalence of NAFLD in the general population in each country is 10–24%, which is significantly higher in women than in men.3 Among them, the prevalence of NAFLD in the United States (US) is estimated at 16%–23%.4 The pathogenesis of NAFLD is very complex and involves intracellular biochemical metabolism.5 More and more researchers believe that NAFLD is a manifestation of metabolic syndrome in the liver. It may be related to islet resistance and fat oxidation disorders.6 When left untreated, this disease may develop into liver cancer, which is difficult to treat and may even lead to death.7 As a result, we should pay great attention to the early detection and treatment of this disease.
NAFLD is associated with an increased burden of inflammation.8,9 Moreover, it is related to metabolic disturbance.10 Hu et al first developed the systemic immune-inflammation index (SII) in 2014, which integrated three types of inflammatory cells, including platelets, neutrophils, and lymphocytes, and was calculated by platelet count × neutrophil count lymphocyte count.11 The SII index is dependent on various cell counts in the hemogram, such as neutrophils, lymphocytes, and platelets. The markers based on these cell counts were also reported to be associated with inflammatory conditions such as thyroid conditions,12 gastrointestinal diseases,13 thyroiditis,14 diabetes mellitus,15 irritable bowel disease,16 and COVID-19 infection.17 On the other hand, the SII index is considered a good and stable index that reflects both local immune responses and systemic inflammation in the body as a whole.18,19 It has been identified to predict outcomes in patients with multiple cancers, heart failure, acute ischemic stroke, and acute kidney injury.20–24 However, the effect of the SII index on NAFLD has not been fully elucidated. In addition, epidemiological research has not been able to determine whether the SII index is associated with the ZJU index, BARD score, NAFLD fibrosis score, or the risk of NAFLD in the general US population. Considering the detrimental effects of NAFLD, recognizing risk factors and devising measures to avoid or control the consequences as soon as possible are highly beneficial. As a result, we examined the association between the SII index and the prevalence of NAFLD by analyzing data from the Nutrition and Health Examination Survey (NHANES) for the 2017–2018 years.
Materials and Methods
Study Population
The NHANES database is a population-based cross-sectional survey designed to gather information about the health and nutrition of representative American households. It combines demographics, dietary, examination, laboratory, questionnaire, and limited access data. For data users and researchers throughout the world, survey data are available on the internet.25 The NHANES data for the present study from 2017 to 2018 were used and analyzed. Among the 8897 participants in the total sample, we excluded participants with insufficient NAFLD data (n = 2949) and SII index (n = 257), respectively. Moreover, excluding participants who did not have data on the ZJU index, BARD score, or NAFLD fibrosis score (n = 3069) and participants with missing covariate data (n = 1425). Finally, a total of 1197 individuals were included in this research (Figure 1). The National Center for Health Statistics Ethical Review Board approved all protocols, and each participant provided written informed consent.26 Detailed study design proposals are publicly available online (https://www.cdc.gov/nchs/nhanes/).
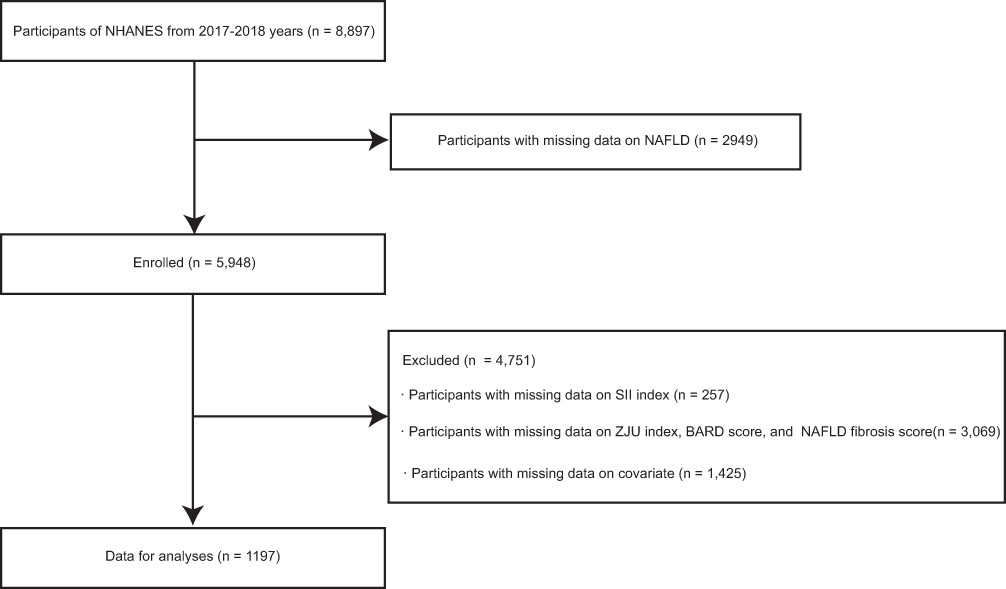 |
Figure 1 Study flow chart. Abbreviations: NHANES, National Health and Nutrition Examination Surveys; NAFLD, non-alcoholic fatty liver disease; SII index, systemic immune-inflammation index. |
Covariates
In the study, the covariates were as follows: age, sex (male, and female), race/ethnicity (Mexican American, Other Hispanic, Non-Hispanic White, Non-Hispanic Black, and Other Race), family poverty income ratio (PIR), education level (less than high school, high school, and more than high school), marital status (having a partner, no partner, unmarried), the complication of hypertension, and diabetes mellitus (DM), coronary heart disease (CHD), congestive heart failure (CHF), angina pectoris, heart attack, and stroke, smoker (no, former, now), drinker (never, mild, moderate, heavy), body mass index (BMI), waist circumference, fast glucose (FBG), glycosylated hemoglobin (HbA1c), hemoglobin (Hb), high-sensitivity C-reactive protein (hs CRP), alanine aminotransferase (ALT), aspartate amino transferase (AST), gamma-glutamyl transpeptidase (GGT), blood urea nitrogen (BUN), uric acid (UA), serum creatinine (Scr), estimated glomerular filtration rate (eGFR), high-density lipoprotein-cholesterol (HDL-C), total cholesterol (TC), triglyceride (TG), ZJU index, BARD score, and NAFLD fibrosis score.27–29 Participants self-reported data regarding their age, sex, race or ethnicity, educational level, marital status, smoking, and drinking habits during the home interview. These questions about the complications of CHD, CHF, angina pectoris, heart attack, and stroke were described in the NHANES dataset as 66 MCQ160b-e. In addition, data on FBG, HbA1c, Hb, hs CRP, ALT, AST, GGT, BUN, UA, Scr, eGFR, HDL-C, TC, and TG were obtained from laboratory examination. You can find more information about the variables in this study here https://www.cdc.gov/nchs/nhanes/.
Calculation of the SII Index, ZJU Index, BARD Score, and NAFLD Fibrosis Score
The blood samples were collected from fasting participants in the study. The automated hematology analyzing devices (Coulter® DxH 800 analyzer) was used to measure blood count (neutrophil, lymphocyte, and platelet counts). In this study, we calculated SII index for each participant as follows: SII index (×109/L) = neutrophil count (×109/L)/lymphocyte count (×109/L) × platelet count (×109/L).18,30 In addition, the ZJU index formula is expressed as follows: BMI (kg/m2) + FBG (mmol/L) + TG (mmol/L) + 3×ALT (IU/L)/AST (IU/L) ratio (+2, if female).27 The BARD score is calculated by weighted sum of three variables (BMI >28 = 1 point, AAR of >0.8 = 2 points, DM = 1 point).28 Finally, the NAFLD fibrosis score formula is expressed as follows: -1.675 + 0.037 × age (years) + 0.094 × BMI (kg/m2) + 1.13 × IFG/diabetes (yes=1, no=0) + 0.99 × AST (IU/L)/ALT (IU/L) ratio – 0.013 × platelet count (×109/L) – 0.66 × albumin (g/dl).29
NAFLD Measurement
NAFLD was defined using the US fatty liver index (FLI), a well-validated diagnostic index,31 which was employed utilizing NHANES III data and calculated as an equation according to a previous study32,33 that included information on BMI, GGT, TG, and waist circumference. All the information was collected concurrently with the status of iron metabolism. NAFLD was defined as an FLI score of ≥60. The FLI formula is expressed as follows:34

Statistical Analysis
The weighted NHANES sample was used to calculate all estimates. The sample size caused by the missing covariate was deleted in this study. All statistical analyses were calculated using R version 3.6.4 (R Foundation for Statistical Computing, Vienna, Austria) and SPSS version 24.0 (SPSS Inc., Chicago, IL, USA). A P-value < 0.05 was considered statistically significant. Continuous variables were reported as mean ± standard deviation (SD), while categorical variables were presented as numbers (%). Continuous variables were analyzed by the weighted Student’s t-test or one-way ANOVA, and categorical variables were analyzed by the weighted chi-square tests. The SII index was divided into quartiles (Q1: 50.000–292.000, Q2: 292.00–423.059, Q3: 423.060–602.735, and Q4: 602.736–3250.714), and the lowest quartile (Q1) served as the reference group (Q1). Firstly, we performed multivariable logistic regression models to explore the relationship between the independent variable SII index and the risk of NAFLD. Model 1 was adjusted for age and sex. Model 2 was adjusted for model 1 variables plus race/ethnicity, education level, marital status, family PIR, smoke status, drink status, the complication of hypertension, and DM. Model 3 was adjusted for model 2 variables plus the complication of CHD, CHF, angina pectoris, heart attack, and stroke, BMI, waist circumference, FBG, HbA1c, Hb, hs CRP, ALT, AST, GGT, UA, BUN, Scr, eGFR, TG, and HDL-C. Then, after adjusting all the covariates of Model 3 above, restricted cubic spline models (RCS) were analyzed to assess the association between SII index and risk of NAFLD, and generalized additive models and smooth curve fitting were used to explore SII index, ZJU index, BARD score, and NAFLD fibrosis score. Finally, subgroup analyses were stratified by age, sex, hypertension, DM, and BMI to evaluate the association between the SII index and the risk of NAFLD.
Results
Baseline Characteristics
The basic clinical characteristics and laboratory examinations are shown in Table 1. The 1197 subjects were divided into four groups (Q1, Q2, Q3, and Q4) based on their SII index levels. We computed that the number of participants in this research may be representative of the total population of 64,268,398 in the United States. The prevalence of NAFLD in this study was 28.1%. There were significant differences in sex, smoker, the complication of CHD, BMI, waist, hs CRP, Scr, ZJU score, BARD score, and NAFLD fibrosis score among the different uric acid groups.
 |
Table 1 Characteristics of the Study Population Based on SII Index Quartiles |
Association Between SII Index and ZJU Index, BARD Score, and NAFLD Fibrosis Score
We conducted generalized additive models with smooth functions to assess the association between the SII index and the ZJU index, the BARD score, and the NAFLD fibrosis score. The SII index was linearly positive with the ZJU index but negative with the NAFLD fibrosis score (Figure 2A and C). However, there is first a decrease in correlations between the SII index and BARD score, then an increase, and finally another decrease (Figure 2B).
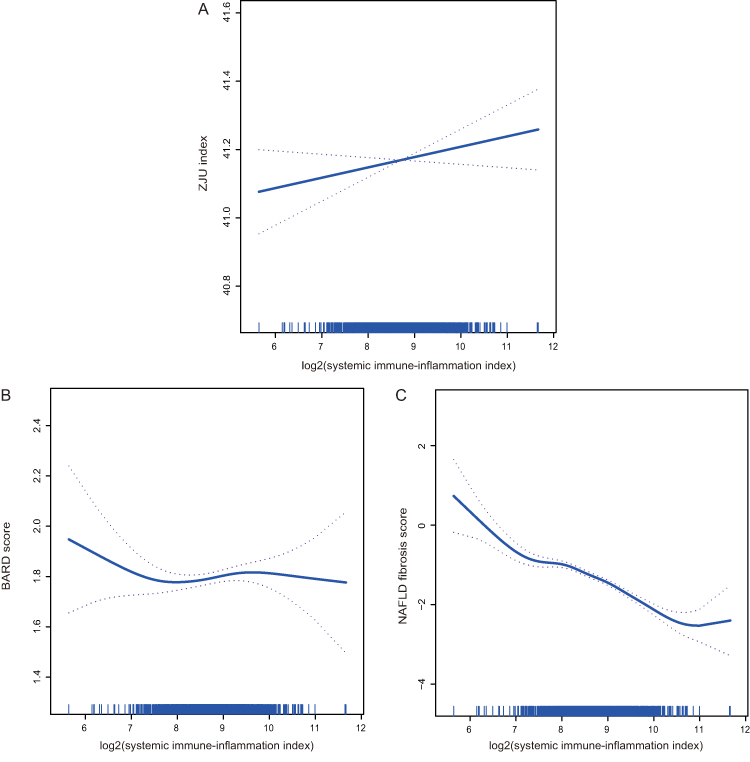 |
Figure 2 Associations of SII index with ZJU index, BARD score, and NAFLD fibrosis score. (A) Association between SII index and ZJU index. (B) Association between SII index and BARD score. (C) Association between SII index and NAFLD fibrosis score. Abbreviations: SII index, systemic immune-inflammation index; NAFLD, non-alcoholic fatty liver disease. |
Association Between SII Index and NAFLD
In the restricted cubic spline (RCS) plot, we can see the SII index is associated with a U-shaped association with the prevalence of NAFLD (P for nonlinearity <0.05, Figure 3). As the SII index increased, the risk of NAFLD decreased significantly. When the SII index reached 422.40, the risk of NAFLD was at its lowest, and then the curve showed an upward trend. Three multivariate logistic regression models (Model 1, Model 2, and Model 3) were constructed to investigate the relationship between the SII index and the prevalence of NAFLD (Table 2). After adjusting for interfering factors, compared with the lowest quartiles (Q1), the odds ratios (ORs) with 95% confidence intervals (CIs) for NAFLD across the quartiles were 0.923 (0.585, 1.455), 0.563 (0.351, 0.901), and 1.061 (0.669, 1.682).
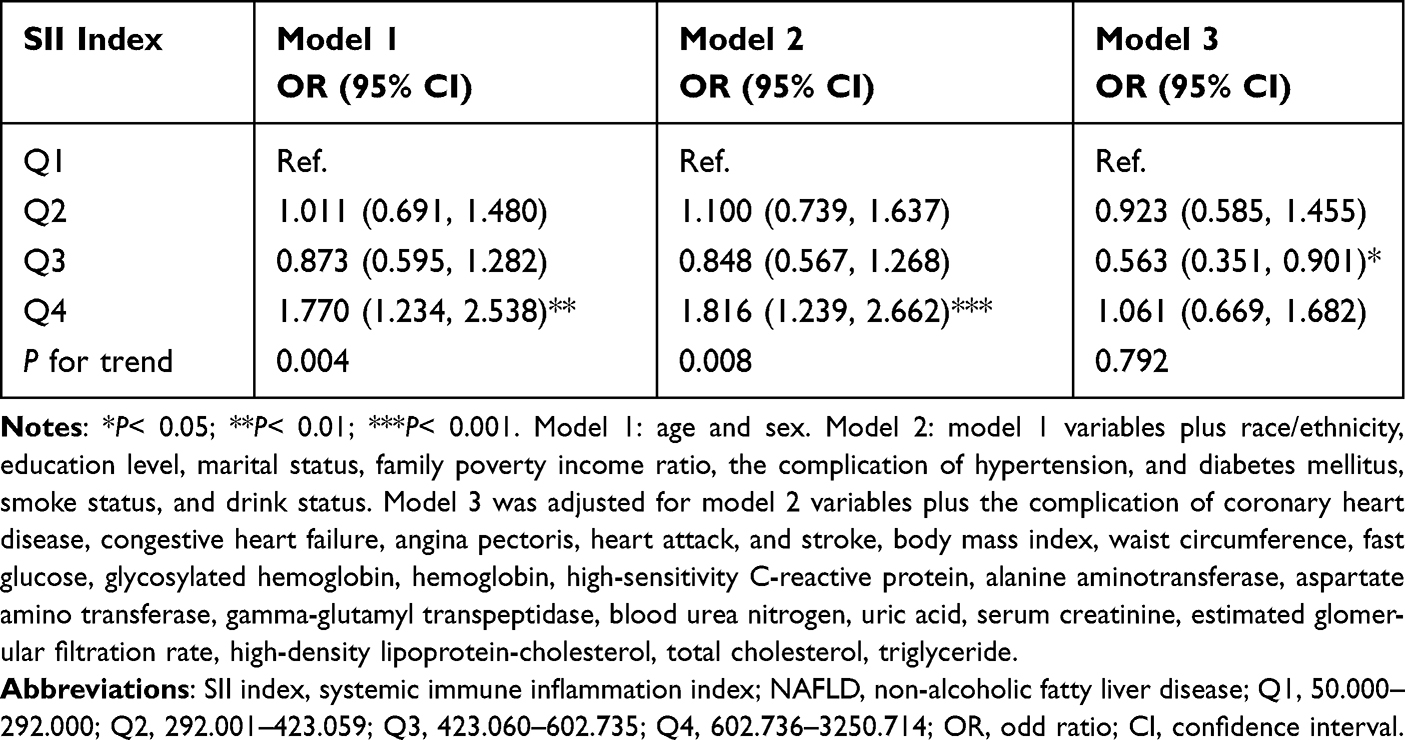 |
Table 2 Adjusted ORs for Associations Between SII Index and the Prevalence of NAFLD |
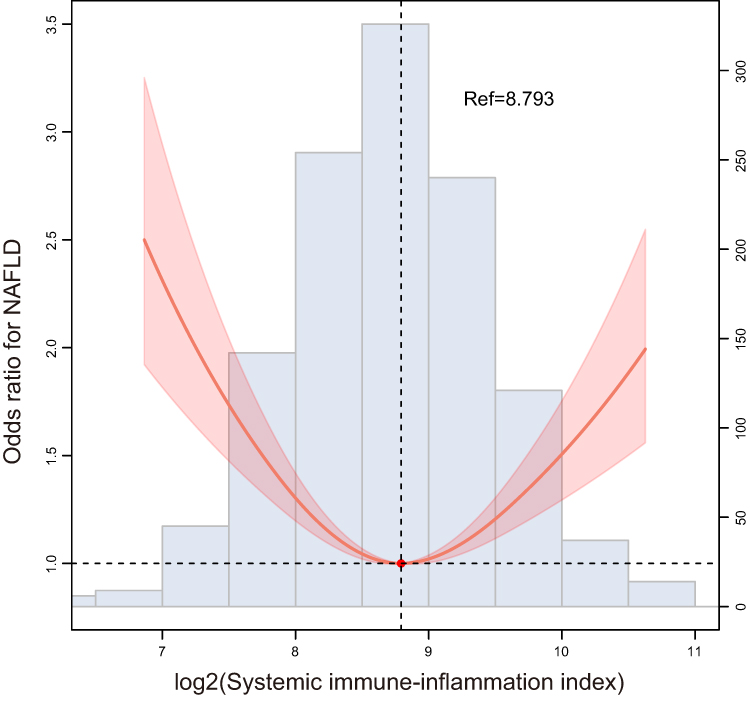 |
Figure 3 Restricted cubic spline curve for the relationship between SII index with the prevalence of NAFLD. Abbreviations: SII index, systemic immune-inflammation index; NAFLD, non-alcoholic fatty liver disease; OR, odd ratio; CI, confidence interval. |
Subgroup Analyses
We performed subgroup analyses stratified by age, sex, hypertension, DM, and BMI, to determine the link between SII index and risk of NAFLD are shown in Table 3, and Figure 4. The stratified analysis revealed the U-shaped associations of SII index with NAFLD were found among participants in all age groups, male or female, with or without hypertension, with DM, and with BMI of <30 or BMI of > 30 kg/m2 (Figure 4A–E). We also observed that SII index positively associated with risk of NAFLD in participants without DM (Figure 4D). The test for interactions was not statistically significant for age, sex, hypertension, DM, and BMI (all P for interactions >0.05, Table 3).
 |
Table 3 Subgroup Analysis for Associations Between SII Index and the Prevalence of NAFLD |
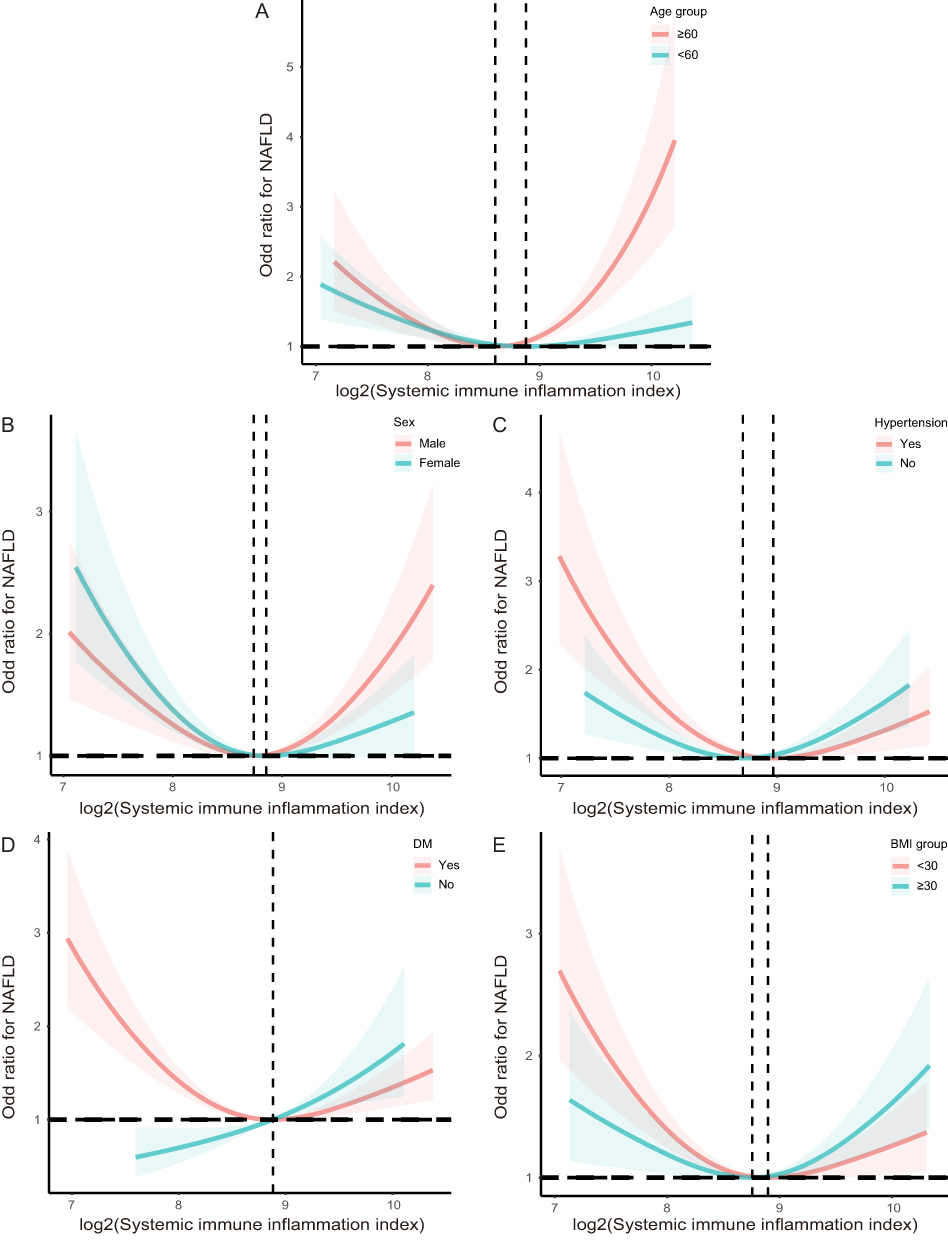 |
Figure 4 Restricted cubic spline curve for the relationship between SII index with the prevalence of NAFLD. (A) The association between SII index and NAFLD stratified by age; (B) The association between SII index and NAFLD stratified by sex; (C) The association between SII index and NAFLD stratified by hypertension; (D) The association between SII index and NAFLD stratified by DM; (E) The association between SII index and NAFLD stratified by BMI. Abbreviations: SII index, systemic immune-inflammation index; NAFLD, non-alcoholic fatty liver disease; DM, diabetes mellitus; BMI, body mass index. |
Discussion
NAFLD is the most common cause of elevated liver enzyme levels in U.S. adults and the most common cause of cryptogenic cirrhosis.35 NAFLD has attracted increasing attention and research because it can progress to cirrhosis and even liver cancer.36 Inflammation is a feature of non-alcoholic fatty liver disease progression and plays an important role in hepatic steatosis and fibrosis.37 In addition, the pathogenesis and disease progression of NAFLD are closely related to the activation of innate immunity.38 However, its pathogenesis is still not fully understood.
In the study, firstly, we found that the SII index was linearly positive with the ZJU index but negative with the NAFLD fibrosis score. And the SII index and BARD score showed a trend of first decreasing, then increasing, and then decreasing. A correlation between the SII index and the ZJU index, the BARD score, and the NAFLD fibrosis score has not been studied to date. Secondly, we revealed that the SII index is associated with a U-shaped association with the prevalence of NAFLD in the RCS plot. Wang et al found that genes associated with immune infiltration may serve as potential markers for therapeutic targets for NAFLD.39 Xie et al. Revealed that a high SII index is associated with hepatic steatosis but not with liver fibrosis.40 In addition, Song Y and his team also found that U.S. adults with a high SII index had an increased risk of hepatic steatosis.41 However, the findings of Ioannou GN showed that the presence and severity of hepatic steatosis were associated with increased pan-immune inflammation value levels but not with the SII index in obese children and adolescents.36 Additionally, the acute phase of inflammation plays a significant role in liver graft injury. Hong BJ and his team reveal that hepatic transplant rejection is attenuated by inhibiting the inflammasome activation pathway.42 In summary, this is consistent with the conclusion of this study. Reasonable control of inflammation in vivo can effectively reduce the occurrence of NAFLD. Thirdly, the stratified analysis showed that the U-shaped associations of the SII index with NAFLD were found among participants in all age groups, male or female, with or without hypertension, with DM, and with a BMI of <30 or > 30 kg/m2. Additionally, we also observed that the SII index was positively associated with the risk of NAFLD in subjects without DM. Type 2 diabetes, obesity, and hyperlipidemia are considered to be important risk factors for NAFLD.43 Between 21% and 45% of patients with NAFLD have type 2 diabetes.44 Among them, patients with NAFLD combined with type 2 diabetes are more likely to progress to cirrhosis, have an increased risk of cardiovascular disease and kidney disease, and have a higher mortality rate.45,46 In addition, the prevalence of NAFLD is 4–6 times higher in obese patients than in those of normal weight.47 Shi et al also found that obese children have low-grade chronic inflammation.48 In contrast, patients with type 2 diabetes are significantly more likely to develop NAFLD, regardless of their BMI.49 Among hyperlipidemic patients, those with hypertriglyceridemia are at greater risk of NAFLD than those with hypercholesterolemia.50,51
NHANES database provides nationally representative estimates based on standardized protocols for data collection. Consequently, the current findings can be generalized widely. However, it is important to note that our study has several limitations. Firstly, the study only included the general population of the United States from of NHANES 2017–2018 years, due to year limitations. Secondly, self-reported confounders may be biased due to self-reporting questionnaire. Finally, as a cross-sectional study, conclusions were limited to associations rather than causality.
Conclusion
In conclusion, the relationship between the SII index and the risk of NAFLD presented a U-shaped curve in the American population. A turning point for the SII index was observed, and the prevalence of NAFLD was lowest when the SII index was 422.40. The potential mechanisms of the SII index in NAFLD need further exploration.
Data Sharing Statement
This study analyzed publicly available datasets; these can be found here: https://www.cdc.gov/nchs/nhanes/.
Acknowledgments
In recognition of the valuable contribution of the NHANES study staff and participants, the authors would like to thank them.
Funding
This work was supported by any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Sheka AC, Adeyi O, Thompson J, Hameed B, Crawford PA, Ikramuddin S. Nonalcoholic steatohepatitis: a review. JAMA. 2020;323(12):1175–1183. doi:10.1001/jama.2020.2298
2. Younossi ZM. Non-alcoholic fatty liver disease - A global public health perspective. J Hepatol. 2019;70(3):531–544. doi:10.1016/j.jhep.2018.10.033
3. Ruhl CE, Everhart JE. Determinants of the association of overweight with elevated serum alanine aminotransferase activity in the United States. Gastroenterology. 2003;124(1):71–79. doi:10.1053/gast.2003.50004
4. Estes C, Anstee QM, Arias-Loste MT, et al. Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016–2030. J Hepatol. 2018;69(4):896–904. doi:10.1016/j.jhep.2018.05.036
5. Newgard CB, McGarry JD. Metabolic coupling factors in pancreatic beta-cell signal transduction. Annu Rev Biochem. 1995;64(1):689–719. doi:10.1146/annurev.bi.64.070195.003353
6. Lebeaupin C, Vallée D, Hazari Y, Hetz C, Chevet E, Bailly-Maitre B. Endoplasmic reticulum stress signalling and the pathogenesis of non-alcoholic fatty liver disease. J Hepatol. 2018;69(4):927–947. doi:10.1016/j.jhep.2018.06.008
7. Zafrani ES. Non-alcoholic fatty liver disease: an emerging pathological spectrum. Virchows Arch. 2004;444(1):3–12. doi:10.1007/s00428-003-0943-7
8. Arrese M, Cabrera D, Kalergis AM, Feldstein AE. Innate immunity and inflammation in NAFLD/NASH. Dig Dis Sci. 2016;61(5):1294–1303. doi:10.1007/s10620-016-4049-x
9. Schuster S, Cabrera D, Arrese M, Feldstein AE. Triggering and resolution of inflammation in NASH. Nat Rev Gastroenterol Hepatol. 2018;15(6):349–364.
10. Kosekli MA, Kurtkulagii O, Kahveci G, et al. The association between serum uric acid to high density lipoprotein-cholesterol ratio and non-alcoholic fatty liver disease: the abund study. Rev Assoc Med Bras. 2021;67(4):549–554. doi:10.1590/1806-9282.20201005
11. Diao P, Wu Y, Li J, et al. Preoperative systemic immune-inflammation index predicts prognosis of patients with oral squamous cell carcinoma after curative resection. J Transl Med. 2018;16(1):365. doi:10.1186/s12967-018-1742-x
12. Afsin H, Aktas G. Platelet to lymphocyte and neutrophil to lymphocyte ratios are useful in differentiation of thyroid conditions with normal and increased uptake. Ethiop J Health Dev. 2021;35(3):1–5.
13. Buse Balci S, Aktas G. A comprehensive review of the role of hemogram derived inflammatory markers in gastrointestinal conditions. Iran J Colorectal Res. 2022;10(3):75–86.
14. Erge E, Kiziltunc C, Balci SB, et al. A novel inflammatory marker for the diagnosis of hashimoto’s thyroiditis: platelet-count-to-lymphocyte-count ratio. Diseases. 2023;11(1):15. doi:10.3390/diseases11010015
15. Atak B, Aktas G, Duman TT, Erkus E, Kocak MZ, Savli H. Diabetes control could through platelet-to-lymphocyte ratio in hemograms. Rev Assoc Med Bras. 2019;65(1):38–42. doi:10.1590/1806-9282.65.1.38
16. Aktas G, Duman T, Atak B, et al. Irritable bowel syndrome is associated with novel inflammatory markers derived from hemogram parameters. Fam Med Prim Care Rev. 2020;22(2):107–110. doi:10.5114/fmpcr.2020.95311
17. Aktas G. Hematological predictors of novel Coronavirus infection. Rev Assoc Med Bras. 2021;67(Suppl 1):1–2. doi:10.1590/1806-9282.67.suppl1.20200678
18. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
19. Tong YS, Tan J, Zhou XL, Song YQ, Song YJ. Systemic immune-inflammation index predicting chemoradiation resistance and poor outcome in patients with stage III non-small cell lung cancer. J Transl Med. 2017;15(1):221. doi:10.1186/s12967-017-1326-1
20. Yang R, Chang Q, Meng X, Gao N, Wang W. Prognostic value of Systemic immune-inflammation index in cancer: a meta-analysis. J Cancer. 2018;9(18):3295–3302. doi:10.7150/jca.25691
21. Xie Y, Zhuang T, Ping Y, et al. Elevated systemic immune inflammation index level is associated with disease activity in ulcerative colitis patients. Clin Chim Acta. 2021;517:122–126. doi:10.1016/j.cca.2021.02.016
22. Tang Y, Zeng X, Feng Y, et al. Association of systemic immune-inflammation index with short-term mortality of congestive heart failure: a retrospective cohort study. Front Cardiovasc Med. 2021;8:753133. doi:10.3389/fcvm.2021.753133
23. Zhou YX, Li WC, Xia SH, et al. Predictive value of the systemic immune inflammation index for adverse outcomes in patients with acute ischemic stroke. Front Neurol. 2022;13:836595. doi:10.3389/fneur.2022.836595
24. Jiang H, Li D, Xu T, et al. Systemic immune-inflammation index predicts contrast-induced acute kidney injury in patients undergoing coronary angiography: a cross-sectional study. Front Med. 2022;9:841601. doi:10.3389/fmed.2022.841601
25. Xiao S, Wang X, Zhang G, et al. Association of systemic immune inflammation index with estimated pulse wave velocity, atherogenic index of plasma, triglyceride-glucose index, and cardiovascular disease: a large cross-sectional study. Mediators Inflamm. 2023;2023:1966680. doi:10.1155/2023/1966680
26. Zipf G, Chiappa M, Porter KS, Ostchega Y, Lewis BG, Dostal J. National health and nutrition examination survey: plan and operations, 1999–2010. Vital Health Stat Ser 1. 2013;56:1–37.
27. Wang J, Xu C, Xun Y, et al. ZJU index: a novel model for predicting nonalcoholic fatty liver disease in a Chinese population. Sci Rep. 2015;5:16494. doi:10.1038/srep16494
28. Harrison SA, Oliver D, Arnold HL, Gogia S, Neuschwander-Tetri BA. Development and validation of a simple NAFLD clinical scoring system for identifying patients without advanced disease. Gut. 2008;57(10):1441–1447. doi:10.1136/gut.2007.146019
29. Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45(4):846–854. doi:10.1002/hep.21496
30. Xiao S, Wang Z, Zuo R, et al. Association of systemic immune inflammation index with all-cause, cardiovascular disease, and cancer-related mortality in patients with cardiovascular disease: a cross-sectional study. J Inflamm Res. 2023;16:941–961. doi:10.2147/JIR.S402227
31. Ruhl CE, Everhart JE. Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey. Aliment Pharmacol Ther. 2015;41(1):65–76. doi:10.1111/apt.13012
32. Bedogni G, Bellentani S, Miglioli L, et al. The fatty liver index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 2006;6(1):33. doi:10.1186/1471-230X-6-33
33. Kobyliak N, Abenavoli L, Mykhalchyshyn G, et al. A multi-strain probiotic reduces the fatty liver index, cytokines and aminotransferase levels in NAFLD patients: evidence from a randomized clinical trial. J Gastrointestin Liver Dis. 2018;27(1):41–49. doi:10.15403/jgld.2014.1121.271.kby
34. Zhang X, Zuo R, Xiao S, Wang L. Association between iron metabolism and non-alcoholic fatty liver disease: results from the National Health and Nutrition Examination Survey (NHANES 2017-2018) and a controlled animal study. Nutr Metab. 2022;19(1):81. doi:10.1186/s12986-022-00715-y
35. Huang TD, Behary J, Zekry A. Non-alcoholic fatty liver disease: a review of epidemiology, risk factors, diagnosis and management. Intern Med J. 2020;50(9):1038–1047. doi:10.1111/imj.14709
36. Ioannou GN. Epidemiology and risk-stratification of NAFLD-associated HCC. J Hepatol. 2021;75(6):1476–1484. doi:10.1016/j.jhep.2021.08.012
37. Wiering L, Tacke F. Treating inflammation to combat non-alcoholic fatty liver disease. J Endocrinol. 2023;256(1). doi:10.1530/JOE-22-0194
38. Tilg H, Adolph TE, Dudek M, Knolle P. Non-alcoholic fatty liver disease: the interplay between metabolism, microbes and immunity. Nat Metab. 2021;3(12):1596–1607. doi:10.1038/s42255-021-00501-9
39. Wang Z, Xia Y, Pan Y, et al. Weighted gene co-expression network analysis of immune infiltration in nonalcoholic fatty liver disease. Endocr Metab Immune Disord Drug Targets. 2022. doi:10.2174/1871530323666221208105720
40. Xie R, Xiao M, Li L, et al. Association between SII and hepatic steatosis and liver fibrosis: a population-based study. Front Immunol. 2022;13:925690. doi:10.3389/fimmu.2022.925690
41. Song Y, Guo W, Li Z, Guo D, Li Z, Li Y. Systemic immune-inflammation index is associated with hepatic steatosis: evidence from NHANES 2015–2018. Front Immunol. 2022;13:1058779. doi:10.3389/fimmu.2022.1058779
42. Hong BJ, Liu H, Wang ZH, et al. Inflammasome activation involved in early inflammation reaction after liver transplantation. Immunol Lett. 2017;190:265–271. doi:10.1016/j.imlet.2017.08.020
43. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64(1):73–84. doi:10.1002/hep.28431
44. Targher G, Corey KE, Byrne CD, Roden M. The complex link between NAFLD and type 2 diabetes mellitus - mechanisms and treatments. Nat Rev Gastroenterol Hepatol. 2021;18(9):599–612. doi:10.1038/s41575-021-00448-y
45. Stefan N, Cusi K. A global view of the interplay between non-alcoholic fatty liver disease and diabetes. Lancet Diabetes Endocrinol. 2022;10(4):284–296. doi:10.1016/S2213-8587(22)00003-1
46. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
47. Powell EE, Wong VW, Rinella M. Non-alcoholic fatty liver disease. Lancet. 2021;397(10290):2212–2224. doi:10.1016/S0140-6736(20)32511-3
48. Shi JQ, Shen WX, Wang XZ, Huang K, Zou CC. Relationship between immune parameters and non-alcoholic fatty liver disease in obese children. Indian Pediatr. 2017;54(10):825–829. doi:10.1007/s13312-017-1143-x
49. Parra-Landazury NM, Cordova-Gallardo J, Méndez-Sánchez N. Obesity and gallstones. Visc Med. 2021;37(5):394–402. doi:10.1159/000515545
50. Shen L, Fan JG, Shao Y, et al. Prevalence of nonalcoholic fatty liver among administrative officers in Shanghai: an epidemiological survey. World J Gastroenterol. 2003;9(5):1106–1110. doi:10.3748/wjg.v9.i5.1106
51. Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. Am J Gastroenterol. 2003;98(5):960–967. doi:10.1111/j.1572-0241.2003.07486.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Systemic Immune-Inflammation Index and Stress Urinary Incontinence in Adult Women: A Population-Based Study
Jiang M, Yao X, Jiang H
International Journal of Women's Health 2025, 17:417-427
Published Date: 18 February 2025