Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Association of Simulation-Based Team Training Implementation with Treatment Process Optimization and Clinical Outcomes in a Chest Pain Center: A Retrospective Pre-Post Analysis of Real-World Data
Authors Liu S, Wang P, Song S, Zhang F, Chen Y, Liu P, Jiang X
Received 15 December 2025
Accepted for publication 5 May 2026
Published 5 June 2026 Volume 2026:19 586570
DOI https://doi.org/10.2147/JMDH.S586570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Sha Liu,1 Pengyu Wang,2 Shaohua Song,3 Fan Zhang,4 Ying Chen,5 Pujuan Liu,6 Xinyan Jiang7
1Pharmacy Intravenous Admixture Services, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 2Office of Academic Affairs, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 3Department of Critical Care Medicine, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 4Department of Nursing, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 5Department of Emergency, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 6Department of Cardiac Surgery, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China; 7Department of Nephrology, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China
Correspondence: Xinyan Jiang, Department of Nephrology, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China, Tel +86-18633889399, Email [email protected] Pujuan Liu, Department of Cardiac Surgery, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, People’s Republic of China, Tel +86-18633889399, Email [email protected]
Background: Efficient multidisciplinary teams in chest pain centers are critical for ST-segment elevation myocardial infarction (STEMI) outcomes. Simulation-based team training (SBTT) may enhance team performance, but real-world clinical impacts remain under-documented. This study evaluated the association between a systematic SBTT program and treatment processes and clinical outcomes in STEMI patients.
Methods: We conducted a retrospective pre-post analysis at a tertiary center in China. Consecutive STEMI patients undergoing primary percutaneous coronary intervention (May 2020–June 2023) were included. Patients were divided into pre-intervention (May 2020–Dec 2021) and post-intervention (Jan 2022–June 2023) groups, separated by the implementation of a multidisciplinary SBTT program. Primary outcomes were door-to-balloon (D2B) and first-medical-contact-to-balloon (FMC-to-B) times. Interrupted time series (ITS) analysis assessed D2B time changes.
Results: We included 260 patients (125 pre-intervention, 135 post-intervention). Post-SBTT, median D2B time decreased from 92 to 68 minutes (p < 0.001), and FMC-to-B time from 125 to 95 minutes (p < 0.001). Patients achieving D2B ≤ 90 min increased from 44.8% to 85.2% (p < 0.001). ITS analysis showed an immediate D2B time drop of 23.5 minutes (p < 0.001). In-hospital MACE rates decreased from 12.8% to 5.2% (p = 0.031).
Conclusion: These findings suggest that SBTT could be a valuable quality improvement tool in chest pain centers for optimizing the timeliness of reperfusion therapy and clinical outcomes. However, further prospective, multicenter studies are needed to confirm these findings and establish definitive causality before universal adoption can be firmly recommended.
Keywords: simulation training, chest pain center, myocardial infarction, quality improvement, teamwork, clinical outcomes
Introduction
Acute myocardial infarction (AMI), particularly ST-segment elevation myocardial infarction (STEMI), remains a leading cause of morbidity and mortality worldwide.1,2 The cornerstone of STEMI management is timely reperfusion, typically through primary percutaneous coronary intervention (PCI), where every minute of delay is associated with increased mortality.3,4 To minimize these critical time delays, the concept of the chest pain center (CPC) has been globally adopted. CPCs are integrated systems of care designed to streamline the diagnosis and treatment of patients with acute coronary syndromes (ACS) through standardized protocols, multidisciplinary collaboration, and continuous quality improvement.5,6 Indeed, managing acute and chronic cardiovascular conditions increasingly requires addressing complex comorbidities, such as the frequent coexistence of heart failure and chronic obstructive pulmonary disease, which severely complicates disease trajectories.7 Furthermore, optimizing patient outcomes relies heavily on effective continuous medical education and innovative care models. For instance, structured education and feedback on cardiovascular management have been shown to influence clinical practice patterns,8 while novel alternative rehabilitation strategies, such as yoga-based programs, have shown benefits in improving post-myocardial infarction quality of life when conventional methods fall short.9
The success of a CPC is profoundly dependent on the seamless coordination and communication of its multidisciplinary team, which includes emergency medical services (EMS) personnel, emergency physicians, nurses, cardiologists, and catheterization laboratory staff.10–12 However, the high-stakes, time-sensitive nature of STEMI care creates a complex environment fraught with potential for error, communication breakdown, and process inefficiencies.11,13 Traditional didactic training methods are often insufficient to prepare teams for the dynamic and unpredictable realities of clinical emergencies, as they fail to address non-technical skills such as leadership, situational awareness, and closed-loop communication, which are paramount to effective teamwork.13–15
Simulation-based team training (SBTT) has emerged as a powerful educational modality in healthcare to bridge this gap. By creating realistic, high-fidelity clinical scenarios in a safe environment, SBTT allows teams to practice and refine both technical skills and non-technical skills without posing any risk to patients.16–18 This methodology facilitates experiential learning, structured debriefing, and the identification of latent safety threats—system-based issues that may otherwise go unnoticed until a real adverse event occurs.19,20 While the benefits of simulation in improving individual and team performance in controlled settings are well-established, there is a need for more robust evidence from real-world clinical settings linking the implementation of SBTT programs to tangible improvements in system-level process metrics and patient clinical outcomes.17,21,22
Several smaller-scale studies have shown promising results. For instance, in-situ simulation drills have been shown to reduce door-to-needle times for stroke thrombolysis and improve teamwork in trauma resuscitation.23,24 However, large-scale, longitudinal data on the sustained impact of implementing a comprehensive SBTT program within a CPC, particularly focusing on the critical door-to-balloon (D2B) and first-medical-contact-to-balloon (FMC-to-B) times, are scarce. Quantifying the effect of such an educational intervention is crucial for justifying the requisite investment in resources, personnel, and time, and for promoting its wider adoption as a standard quality improvement tool.25
Therefore, this study was designed to address this evidence gap by retrospectively analyzing real-world data from our institution. We aimed to evaluate the association between the implementation of a structured, ongoing SBTT program and the performance of our CPC. We hypothesized that the introduction of SBTT would be associated with a significant reduction in reperfusion times, improved adherence to guideline-directed process-of-care metrics, and ultimately, better in-hospital clinical outcomes for patients with STEMI.
Methods
Study Design and Setting
We conducted a retrospective, pre-post, single-center observational study at The First Hospital of Hebei Medical University, a tertiary academic medical center in Shijiazhuang, China, which operates a certified CPC. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Institutional Review Board of The First Hospital of Hebei Medical University, which waived the need for individual informed consent due to the retrospective nature of the analysis and the use of de-identified data. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines26 for reporting this study.
Study Population
We retrospectively identified all consecutive patients aged 18 years or older who were diagnosed with STEMI and underwent primary PCI at our institution between May 1, 2020, and June 30, 2023. The diagnosis of STEMI was based on the universal definition of myocardial infarction, requiring characteristic clinical symptoms, electrocardiographic changes (new ST-segment elevation at the J-point in two contiguous leads), and a rise and/or fall of cardiac troponin values.27 Patients were excluded if they were transferred from another facility for primary PCI (as FMC and D2B times could not be accurately determined), if they received fibrinolytic therapy before PCI, or if they had incomplete data regarding the primary outcome time metrics (Figure 1).
 |
Figure 1 STROBE Flow Diagram for patient inclusion. The diagram illustrates the process of patient selection, from the initial assessment of 305 patients with ST-Segment Elevation Myocardial Infarction (STEMI) undergoing primary Percutaneous Coronary Intervention (PCI) to the final cohort included in the analysis. After applying exclusion criteria, 260 patients were divided into two study groups: a pre-intervention group (n = 125) and a post-intervention group (n = 135) for comparison. Abbreviations: PCI, Percutaneous Coronary Intervention; STEMI, ST-Segment Elevation Myocardial Infarction; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology. |
Intervention: Simulation-Based Team Training (SBTT) Program
Our institution formally implemented a structured, multidisciplinary SBTT program for the CPC team on January 1, 2022. This date served as the cutoff to define the two study periods. The SBTT program consisted of monthly in-situ simulation sessions conducted in the emergency department and the catheterization laboratory. Each session involved a multidisciplinary team (emergency physicians, cardiologists, nurses, and technicians) managing a high-fidelity mannequin simulating a common or challenging STEMI scenario (eg., cardiogenic shock, cardiac arrest, difficult vascular access). The scenarios were designed to test and reinforce the entire chain of care, from patient arrival and initial assessment to catheterization lab activation and reperfusion. Each simulation was followed by a structured debriefing session led by trained facilitators using the “promoting excellence and reflective learning in simulation” (PEARLS) framework.28 The debriefing focused on both clinical management and non-technical skills, including communication, role clarity, resource utilization, and situational awareness. To maintain implementation fidelity over the 18-month post-intervention period, the core facilitator team remained consistent. While the standardized PEARLS debriefing framework was consistently applied, the specific clinical scenarios were rotated and updated monthly to prevent predictability and maintain engagement. Refresher sessions for core concepts were integrated into the debriefings rather than held as separate events.
Data Collection and Variables
The study period was divided into a pre-intervention period (May 1, 2020, to December 31, 2021) and a post-intervention period (January 1, 2022, to June 30, 2023). Data for all eligible patients were extracted from the CPC database and the hospital’s electronic medical record system by two trained research coordinators. Data extraction was performed retrospectively in a single phase after the conclusion of the study period. The extractors were blinded to the study hypothesis and the specific cut-off date defining the pre- and post-intervention periods to minimize detection bias. Any discrepancies were resolved by a third reviewer.
We collected data on patient demographics (age, sex), comorbidities (hypertension, diabetes mellitus, hyperlipidemia, prior MI, prior PCI), clinical presentation (Killip class, systolic blood pressure on admission), and procedural characteristics.
The primary outcomes were two key time-to-reperfusion metrics: 1) Door-to-balloon (D2B) time: defined as the time from the patient’s arrival at the hospital emergency department to the first device inflation in the culprit coronary artery. 2) First-medical-contact-to-balloon (FMC-to-B) time: defined as the time from the first contact with the medical system (eg., EMS arrival at the scene) to the first device inflation.
Secondary outcomes included process-of-care metrics and in-hospital clinical outcomes. Process-of-care metrics were proxies for team efficiency and protocol adherence: 1) Proportion of patients meeting the guideline-recommended D2B time of ≤ 90 minutes. 2) Proportion of patients with an ECG performed and interpreted within 10 minutes of hospital arrival. 3) Proportion of patients bypassing the emergency department and taken directly to the catheterization laboratory. 4) Administration rates of guideline-recommended medications (aspirin, P2Y12 inhibitor) prior to PCI. In-hospital clinical outcomes included: 1) In-hospital mortality. 2) Major adverse cardiovascular events (MACE), a composite of all-cause mortality, non-fatal re-infarction, and stroke. 3) Length of hospital stay.
Statistical Analysis
All statistical analyses were performed using R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided p-value of < 0.05 was considered statistically significant. Continuous variables were reported as mean ± standard deviation (SD) or median with interquartile range (IQR) based on their distribution, which was assessed using the Shapiro–Wilk test. Categorical variables were reported as counts and percentages. To compare baseline characteristics and outcomes between the pre- and post-intervention groups, we used the independent t-test or Mann–Whitney U-test for continuous variables and the chi-squared test or Fisher’s exact test for categorical variables.
To analyze the impact of the SBTT intervention while accounting for underlying temporal trends, we performed a segmented regression analysis of interrupted time series (ITS) for the monthly median D2B time.29 The ITS model was specified as: Yt = β0 + β1(time) + β2(intervention) + β3(time_after_intervention) + εt. In this model, Yt is the median D2B time for month t; “time” is a continuous variable for time in months from the start of the study period; “intervention” is an indicator for the pre- (0) or post-intervention (1) period; and “time_after_intervention” is a continuous variable counting the months after the intervention started. The coefficient β2 represents the immediate change in the level of D2B time after the intervention, and β3 represents the change in the slope (trend) of D2B time after the intervention. The monthly median D2B time was chosen as the dependent variable for the ITS analysis to minimize the influence of extreme outliers typical in emergency time metrics. The distribution of these monthly medians was assessed and found to approximate normality, satisfying model assumptions. Autocorrelation was assessed using the Durbin-Watson test, and no significant first-order autocorrelation was detected; thus, standard errors were not adjusted for autocorrelation. Visual inspection of the data did not reveal significant seasonal patterns, so seasonality was not included in the model.
Subgroup analyses were performed to explore the consistency of the intervention’s effect on D2B time reduction across different patient populations (eg., age, sex, presentation during on- vs. off-hours). A Kaplan-Meier survival analysis with a Log rank test was used to compare the MACE-free survival between the two groups. A multivariable logistic regression model was constructed to assess the independent association of the SBTT intervention with the composite MACE outcome, adjusting for potential confounders identified from baseline characteristics.
Results
Patient Characteristics
During the study period, a total of 305 patients with STEMI underwent primary PCI. After applying the exclusion criteria, 260 patients were included in the final analysis. Of these, 125 patients were treated in the pre-intervention period and 135 in the post-intervention period (Figure 1). The baseline demographic and clinical characteristics of the two groups were well-balanced, as shown in Table 1. The mean age was 62.1 ± 11.5 years in the pre-intervention group and 63.3 ± 10.9 years in the post-intervention group (p = 0.358). There were no significant differences in sex, prevalence of comorbidities such as hypertension and diabetes, or clinical presentation factors like Killip class at admission between the two periods.
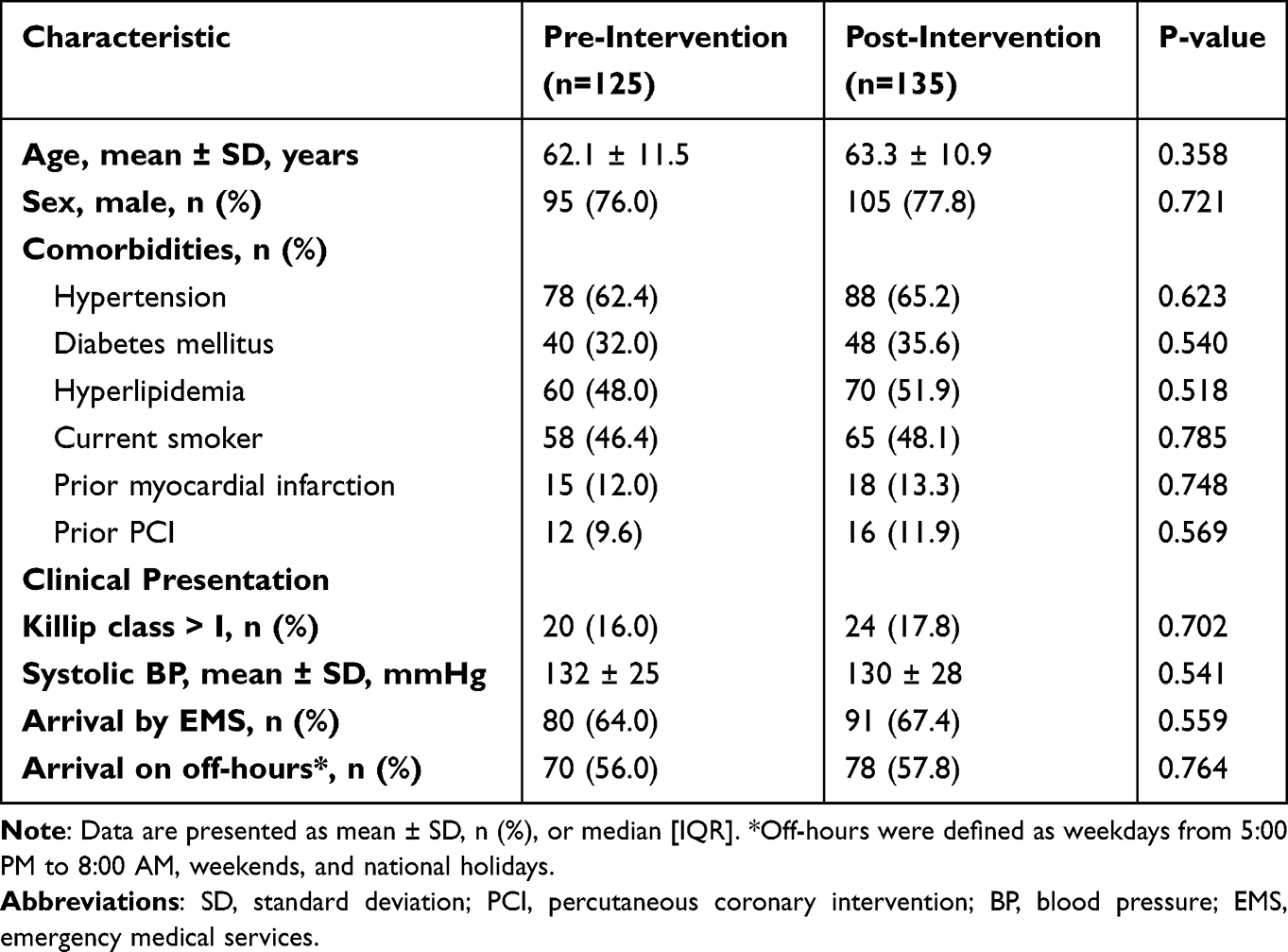 |
Table 1 Baseline Characteristics of STEMI Patients in the Pre- and Post-Intervention Periods |
Primary Outcomes: Time-to-Reperfusion Metrics
The implementation of the SBTT program was associated with a statistically significant and clinically meaningful reduction in both primary time-to-reperfusion metrics (Table 2 and Figure 2). The median D2B time decreased by 26.1%, from 92 minutes (IQR 78–105) in the pre-intervention period to 68 minutes (IQR 59–81) in the post-intervention period (p < 0.001). Similarly, the median FMC-to-B time was reduced by 24.0%, from 125 minutes (IQR 108–142) to 95 minutes (IQR 83–110) (p < 0.001). The proportion of patients who achieved the guideline-recommended D2B time of ≤ 90 minutes dramatically increased from 44.8% (56/125) pre-intervention to 85.2% (115/135) post-intervention (p < 0.001).
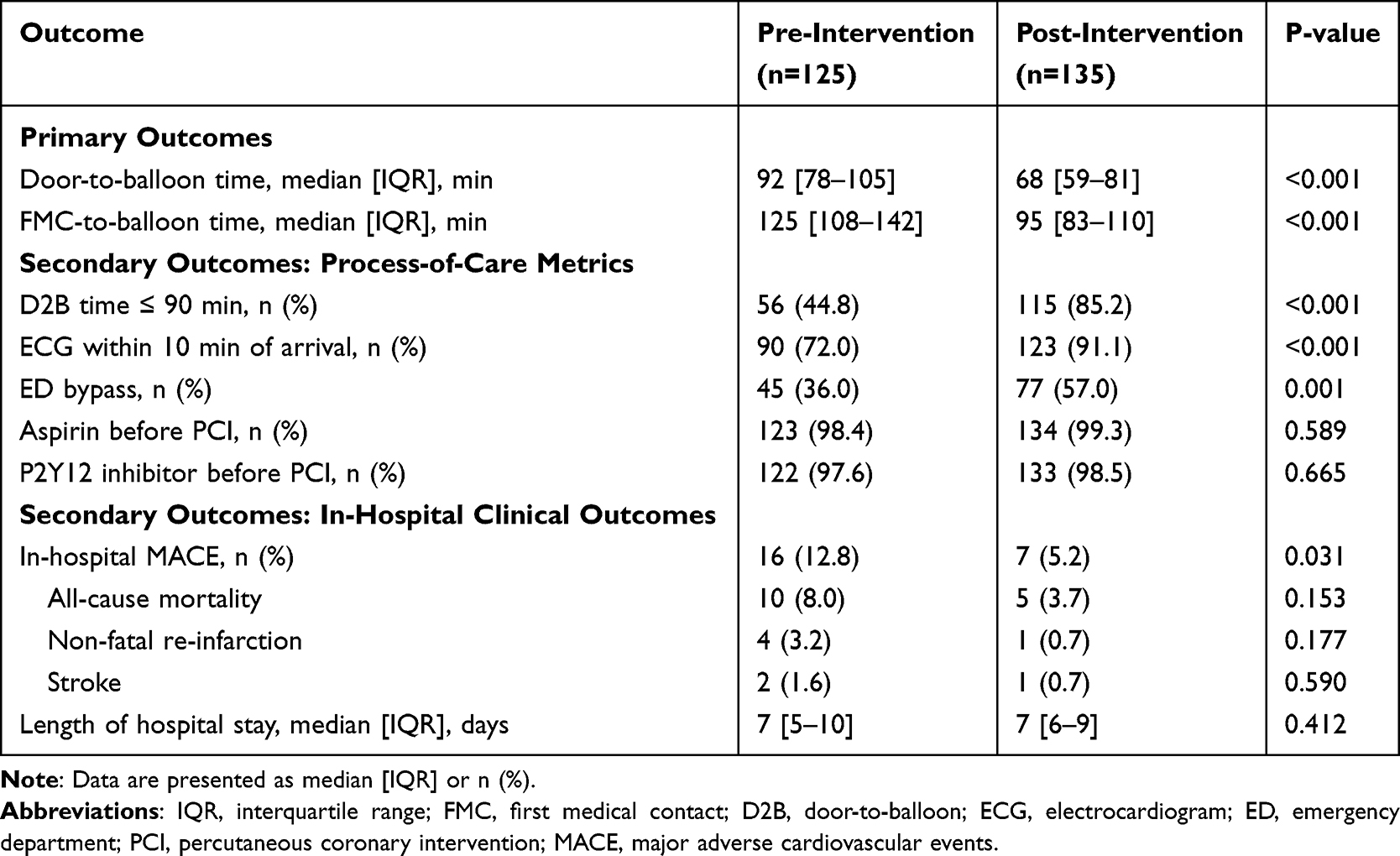 |
Table 2 Comparison of Process-of-Care Metrics and Clinical Outcomes |
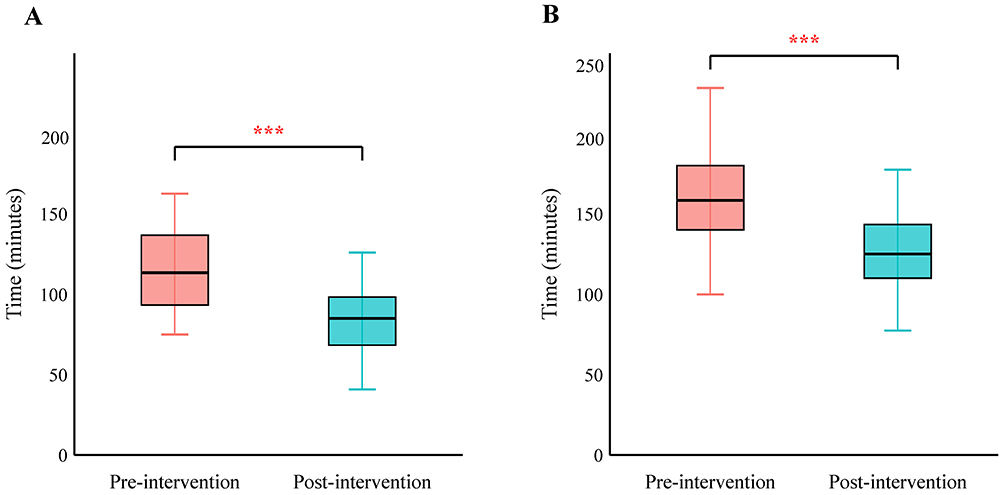 |
Figure 2 Comparison of Primary Temporal Outcomes Before and After Intervention. Box plots showing (A) Door-to-Balloon (D2B) time and (B) First Medical Contact-to-Balloon (FMC-to-B) time for the pre-intervention (n = 125) and post-intervention (n = 135) groups. The central line in each box represents the median value, the box boundaries represent the interquartile range (IQR), and the whiskers extend to 1.5 times the IQR. Statistical significance between the groups was assessed using the Mann–Whitney U-test. Abbreviations: D2B, Door-to-Balloon; FMC-to-B, First Medical Contact-to-Balloon. Note: ***p < 0.001. |
Secondary Outcomes: Process-of-Care and Clinical Outcomes
Significant improvements were also observed in key process-of-care metrics, which serve as proxies for improved team coordination and system efficiency (Table 2 and Figure 3). The rate of ECG completion within 10 minutes of hospital arrival increased from 72.0% to 91.1% (p < 0.001). The proportion of patients who bypassed the emergency department and were transported directly to the catheterization laboratory also rose significantly from 36.0% to 57.0% (p = 0.001). Guideline-directed medical therapy administration rates were high at baseline and remained so, with no significant differences between the groups.
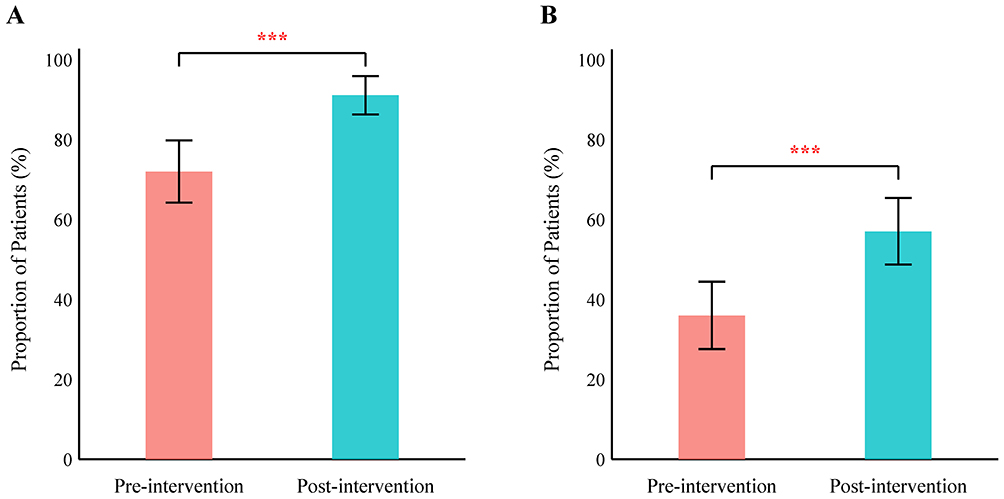 |
Figure 3 Comparison of Key Process-of-Care Metrics. Bar charts displaying the proportion of patients who achieved (A) an electrocardiogram (ECG) performed within 10 minutes of hospital arrival and (B) direct catheterization laboratory access, bypassing the Emergency Department (ED). Comparisons are shown for the pre-intervention (n = 125) and post-intervention (n = 135) groups. Error bars represent 95% confidence intervals (CIs). Statistical analysis was performed using the Chi-square test. Abbreviations: ECG, Electrocardiogram; ED, Emergency Department. Note: *** indicates p < 0.001 between the pre-intervention and post-intervention groups. |
Regarding in-hospital clinical outcomes, the post-intervention group had a significantly lower incidence of MACE (5.2% vs. 12.8%, p = 0.031). This reduction in the composite MACE outcome was driven by numerical decreases across its individual components (pre-intervention vs. post-intervention), including all-cause mortality (8.0% vs. 3.7%, p = 0.153), non-fatal re-infarction (3.2% vs. 0.7%, p = 0.177), and stroke (1.6% vs. 0.7%, p = 0.590), although the differences for these individual components did not reach statistical significance. There was no significant difference in the median length of hospital stay between the two groups (Table 2).
Interrupted Time Series Analysis
The results of the ITS analysis for the monthly median D2B time are presented in Figure 4. Before the SBTT program, there was a slight, non-significant downward trend in D2B time (slope β1 = −0.25 min/month, p = 0.312), indicating minimal change over time. At the point of intervention (January 2022), there was an immediate and statistically significant level drop of 23.5 minutes (β2 = −23.5, 95% CI: −28.9 to −18.1, p < 0.001). Following the intervention, the trend in D2B time showed a continued, significant decline (slope change β3 = −0.65 min/month, p = 0.041), suggesting that the effects of the training were not only immediate but also sustained and potentially enhanced over time.
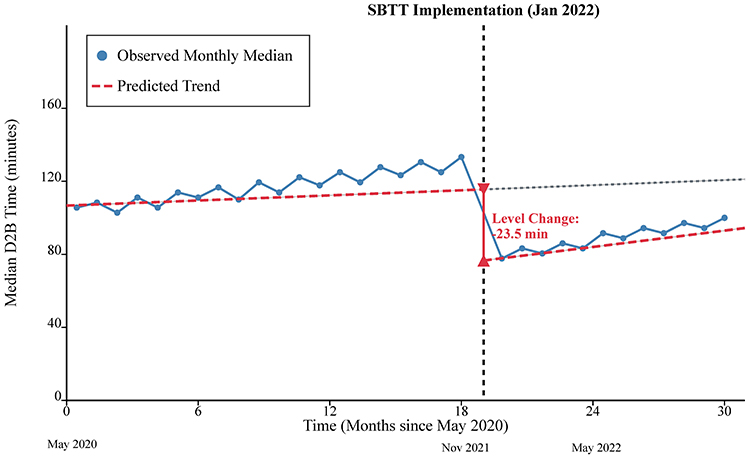 |
Figure 4 Interrupted Time Series (ITS) Analysis of Monthly Median Door-to-Balloon (D2B) Time. The plot displays the monthly median D2B time from May 2020 to June 2023. The vertical dashed line indicates the implementation of the new team-based protocol in January 2022. Blue circles represent the observed monthly median values. The red dashed lines show the predicted trend based on the ITS model for the pre- and post-intervention periods. The analysis revealed a significant immediate level change (a drop of 23.5 minutes, p < 0.001) and a significant change in slope post-intervention (p = 0.01). |
Subgroup and Survival Analysis
The beneficial effect of the SBTT program on reducing D2B time was consistent across various predefined subgroups, including age, sex, and arrival time (on-hours vs. off-hours), with no significant interaction observed (Figure 5). Kaplan-Meier analysis demonstrated that patients in the post-intervention group had a significantly higher rate of MACE-free survival during hospitalization compared to the pre-intervention group (log-rank p = 0.028) (Figure 6). After adjusting for potential confounders in a multivariable logistic regression model, the implementation of SBTT remained independently associated with a lower risk of in-hospital MACE (Adjusted Odds Ratio: 0.38, 95% CI: 0.15–0.94, p = 0.036).
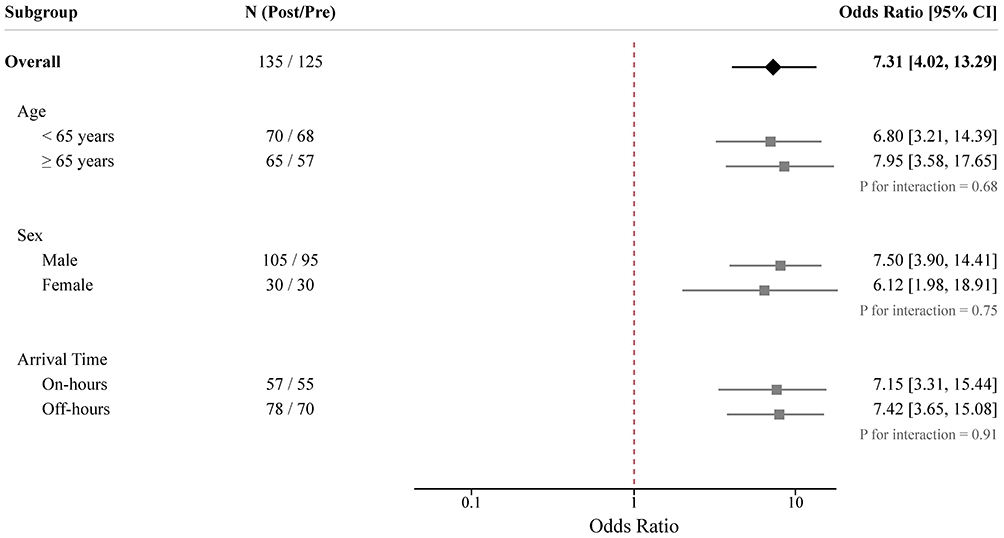 |
Figure 5 Forest Plot of Subgroup Analyses for the Primary Outcome. The plot shows the odds ratios (ORs) and 95% confidence intervals (CIs) for achieving a Door-to-Balloon (D2B) time of ≤ 90 minutes, comparing the post-intervention group to the pre-intervention group (reference). Squares represent the point estimate for each subgroup, with the size of the square proportional to the weight of the subgroup in the analysis. Horizontal lines indicate the 95% CI. The diamond represents the overall pooled OR. Values to the right of the vertical line at 1.0 favor the post-intervention group. P-int denotes the p-value for interaction. |
 |
Figure 6 Kaplan-Meier Curves for In-Hospital MACE-Free Survival. Kaplan-Meier analysis illustrating the probability of in-hospital MACE-free survival for the pre-intervention (n = 125) and post-intervention (n = 135) groups. The shaded areas represent the 95% confidence intervals for each curve. Small vertical ticks on the curves indicate censored data points. The table below the plot shows the number of patients at risk at specific time intervals. The p-value was calculated using the Log rank test. Abbreviations: MACE, Major Adverse Cardiac Events. |
Discussion
In this large, retrospective analysis of real-world data, we found that the implementation of a structured, multidisciplinary simulation-based team training (SBTT) program was significantly associated with substantial and sustained improvements in the performance of a certified chest pain center. The primary findings of our study are threefold: first, SBTT was associated with a dramatic reduction in critical time-to-reperfusion metrics, including both D2B and FMC-to-B times. Second, this improvement was accompanied by enhanced adherence to key process-of-care protocols, suggesting a positive transformation in system efficiency. Third, these process improvements were associated with better in-hospital clinical outcomes, including a significant reduction in major adverse cardiovascular events.
The magnitude of the reduction in D2B time observed in our study — a median decrease of 24 minutes — is both statistically significant and highly clinically relevant. This level of improvement is comparable to or even exceeds that reported for major system-level interventions such as catheterization lab pre-activation by paramedics or direct transport to the cath lab, bypassing the emergency department.30,31 Our findings strongly suggest that optimizing the “human factor” through enhanced teamwork and communication is a powerful lever for quality improvement, complementary to technological and logistical advancements. The traditional model of medical education, which often focuses on individual competence, may be insufficient for complex, team-based emergencies like STEMI care. SBTT addresses this gap by creating a space for the entire care team to rehearse their roles, clarify communication pathways, and identify system vulnerabilities in a coordinated fashion.32,33
A key strength of our study is the use of interrupted time series (ITS) analysis. This quasi-experimental method allowed us to move beyond a simple pre-post comparison and rigorously assess the changes in both the level and trend of D2B time, while accounting for pre-existing temporal trends.34,35 The ITS results provided compelling evidence: a sharp, immediate drop in D2B time coincided precisely with the rollout of the SBTT program, followed by a sustained downward trend. This pattern strongly supports a potential link between the intervention and the observed improvements, reducing the likelihood that the changes were due to mere coincidence or other unmeasured quality improvement initiatives occurring simultaneously.36
The observed improvements in process-of-care metrics, such as higher rates of rapid ECG acquisition and ED bypass, serve as objective evidence of improved team function. These are not isolated tasks but complex workflows requiring seamless coordination among triage nurses, physicians, and cath lab staff. For example, achieving a higher ED bypass rate necessitates reliable pre-hospital notification, rapid in-hospital confirmation by a physician, and swift activation and preparation of the cath lab team. The improvements in these metrics suggest that SBTT likely enhanced the team’s shared mental model, role clarity, and closed-loop communication, enabling them to execute complex protocols more efficiently and reliably.37,38 These metrics act as valuable surrogate markers for the non-technical skills that are notoriously difficult to measure retrospectively.
Ultimately, the goal of any quality improvement initiative is to improve patient outcomes. Our finding of a significant reduction in the composite MACE outcome in the post-intervention period is particularly noteworthy. However, it is important to note that while the overall MACE rate decreased, the study was not sufficiently powered to detect a statistically significant difference in the individual outcome of in-hospital mortality. The reduction in mortality (8.0% to 3.7%) was numerically encouraging but warrants cautious interpretation. The reduction in MACE, which remained significant after multivariable adjustment, suggests that the benefits of faster reperfusion and more efficient care translate into tangible clinical advantages for patients. This aligns with the well-established “time is muscle” paradigm and reinforces the clinical importance of the process improvements driven by the SBTT program.39,40 The Kaplan-Meier analysis further visualized this survival benefit, lending more credence to the positive impact of the intervention.
Our study should be interpreted within the context of its limitations. First, as a single-center, retrospective observational study, it is susceptible to unmeasured confounding variables, despite our use of ITS analysis and multivariable adjustment. Furthermore, during the study period, there were no major changes in the overall EMS coordination system or broad hospital protocols for STEMI care outside of the SBTT implementation. However, we cannot entirely rule out the influence of gradual refinements in staffing experience or minor local protocol adjustments over time. Second, our study design did not allow for the direct measurement of non-technical skills using validated teamwork assessment tools (such as the Clinical Teamwork Scale). Instead, we relied on process metrics as surrogates for team performance. Future prospective studies could incorporate direct teamwork assessment tools to elucidate the mechanisms of improvement more clearly. Third, the findings from a single academic center may not be generalizable to all settings, such as community hospitals or centers with different resource levels. However, the principles of team training are universal, and the framework of our SBTT program could be adapted to various contexts.
In conclusion, our study provides strong real-world evidence that the systematic implementation of a multidisciplinary SBTT program is associated with significant and sustained improvements in STEMI care. The intervention was associated with faster reperfusion times, optimized care processes, and better patient outcomes. These findings suggest that SBTT could be a valuable quality improvement tool in chest pain centers. However, further prospective, multicenter studies are needed to confirm these findings and establish definitive causality before universal adoption can be firmly recommended.
Abbreviations
AMI, Acute myocardial infarction; CPC, Chest pain center; D2B, Door-to-balloon; ECG, Electrocardiogram; ED, Emergency department; EMS, Emergency medical services; FMC-to-B, First-medical-contact-to-balloon; ITS, Interrupted time series; MACE, Major adverse cardiovascular events; PCI, Percutaneous coronary intervention; SBTT, Simulation-based team training; STEMI, ST-segment elevation myocardial infarction; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to hospital privacy policies regarding patient data but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of The First Hospital of Hebei Medical University. The requirement for individual informed consent was waived by the Institutional Review Board of The First Hospital of Hebei Medical University due to the retrospective nature of the analysis and the use of de-identified data.
Acknowledgments
We would like to thank all the staff of the Chest Pain Center at The First Hospital of Hebei Medical University for their participation in the training program and their dedication to patient care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Medical Science Research Project of Hebei (Grant No. 20211428). The funding body had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93–12. doi:10.1161/CIR.0000000000001123
2. Steg PG, James SK, Atar D, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33(20):2569–2619.
3. Scholz KH, Maier SKG, Maier LS, et al. Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial. Eur Heart J. 2018;39(13):1065–1074.
4. Reddy A, Ganti L, Banerjee A, Banerjee P. Continuous quality improvement for prehospital STEMI improved triage rates and achievement of gold standard < 90-min EMS-to-balloon time. Int. J. Emerg. Med. 2025;18(1):53. doi:10.1186/s12245-025-00863-x
5. Amsterdam EA, Wenger NK, Brindis RG, et al. AHA/ACC guideline for the management of patients with non-st-elevation acute coronary syndromes: a report of the American College Of Cardiology/American Heart association task force on practice guidelines. J. Am. Coll. Cardiol. 2014;64(24):e139–e228. doi:10.1016/j.jacc.2014.09.017
6. Abrahim C, Capatina A, Kalyan-Sundaram A, Lotfi A. Reducing door-to-balloon time using ems-initiated app-based communication. J Soc Cardiovasc Angiogr Interv. 2024;3(9):102199. doi:10.1016/j.jscai.2024.102199
7. Wu Z, Wang D, Tang C. Comorbid management of chronic obstructive pulmonary disease and heart failure. Respir Med. 2026;251:108575. doi:10.1016/j.rmed.2025.108575
8. Brunström M, Ng N, Dahlström J, et al. Association of education and feedback on hypertension management with risk for stroke and cardiovascular disease. Blood Press. 2022;31(1):31–39. doi:10.1080/08037051.2022.2041393
9. Prabhakaran D, Chandrasekaran AM, Singh K, et al. Yoga-based cardiac rehabilitation after acute myocardial infarction: a randomized trial. J. Am. Coll. Cardiol. 2020;75(13):1551–1561. doi:10.1016/j.jacc.2020.01.050
10. Anderson HVS, Masri SC, Abdallah MS, et al. ACC/AHA key data elements and definitions for chest pain and acute myocardial infarction: a report of the American Heart Association/American College of Cardiology joint committee on clinical data standards. Circ Cardiovasc Qual Outcomes. 2022;15(10):e000112. doi:10.1161/HCQ.0000000000000112
11. Hsiao SH, Wang PY, Tsia CC. Cross-team collaboration shortens percutaneous coronary intervention time for stemi patients transferred via emergency medical services. Hu li za zhi j nurs. 2025;72(3):68–76. doi:10.6224/JN.202506_72(3).09
12. Sanz M, Smalling RW, Brewer DL, et al. Development of systems of care for ST-elevation myocardial infarction patients: the physician perspective. Circulation. 2007;116(2):e39–42. doi:10.1161/CIRCULATIONAHA.107.184046
13. Habib H, Ginanjar E, Mansjoer A, Sulistio S, Albar IA, Mulyana RM. ST-elevation myocardial infarction: a simulation case for evaluation of interprofessional performance in a hospital. Emerg. Med. Int. 2019;2019:7562637. doi:10.1155/2019/7562637
14. Rosen MA, DiazGranados D, Dietz AS, Benishek LE. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. 2018;73(4):433–450. doi:10.1037/amp0000298
15. Shapiro MJ, Morey JC, Small SD, et al. Simulation based teamwork training for emergency department staff: does it improve clinical team performance when added to an existing didactic teamwork curriculum? Qual Saf Health Care. 2004;13(6):417–421.
16. Cheng A, Kessler D, Mackinnon R, et al. Reporting guidelines for health care simulation research: extensions to the consort and strobe statements. Simul Healthc. 2016;11(4):238–248. doi:10.1097/SIH.0000000000000150
17. Abildgren L, Lebahn-Hadidi M, Mogensen CB, et al. The effectiveness of improving healthcare teams’ human factor skills using simulation-based training: a systematic review. Adv simul. 2022;7(1):12. doi:10.1186/s41077-022-00207-2
18. Escher C, Rystedt H, Creutzfeldt J, et al. All professions can benefit - a mixed-methods study on simulation-based teamwork training for operating room teams. Adv simul. 2023;8(1):18. doi:10.1186/s41077-023-00257-0
19. Uttley E, Suggitt D, Baxter D, Jafar W. Multiprofessional in situ simulation is an effective method of identifying latent patient safety threats on the gastroenterology ward. Frontline Gastroenterol. 2020;11(5):351–357. doi:10.1136/flgastro-2019-101307
20. Kotagal M, Falcone RA Jr, Daugherty M, et al. Making a move: using simulation to identify latent safety threats before the care of injured patients in a new physical space. J Trauma Acute Care Surg. 2023;95(3):426–431. doi:10.1097/TA.0000000000003865
21. Cook DA, Hatala R, Brydges R, et al. Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA. 2011;306(9):978–988. doi:10.1001/jama.2011.1234
22. Zendejas B, Wang AT, Brydges R, Hamstra SJ, Cook DA. Cost: the missing outcome in simulation-based medical education research: a systematic review. Surgery. 2013;153(2):160–176. doi:10.1016/j.surg.2012.06.025
23. Svobodová V, Maršálková H, Volevach E, Mikulík R. Simulation-based team training improves door-to-needle time for intravenous thrombolysis. BMJ Open Quality. 2023;12(1):e002107. doi:10.1136/bmjoq-2022-002107
24. Lapierre A, Bouferguene S, Gauvin-Lepage J, Lavoie P, Arbour C. Effectiveness of interprofessional manikin-based simulation training on teamwork among real teams during trauma resuscitation in adult emergency departments: a systematic review. Simul healthc. 2020;15(6):409–421. doi:10.1097/SIH.0000000000000443
25. Ajmi SC, Kurz MW, Ersdal H, et al. Cost-effectiveness of a quality improvement project, including simulation-based training, on reducing door-to-needle times in stroke thrombolysis. BMJ Qual Saf. 2022;31(8):569–578.
26. von El E, Altman DG, Egger M. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2007;60(6):344–349.
27. Thygesen K, Alpert JS, Jaffe AS. Fourth universal definition of myocardial infarction (2018). Rev Esp Cardiol. 2019;72(1):72. doi:10.1016/j.rec.2018.11.011
28. Eppich W, Cheng A. Promoting Excellence and Reflective Learning in Simulation (PEARLS): development and rationale for a blended approach to health care simulation debriefing. Simul healthc. 2015;10(2):106–115. doi:10.1097/SIH.0000000000000072
29. Xiao H, Augusto O, Wagenaar BH. Reflection on modern methods: a common error in the segmented regression parameterization of interrupted time-series analyses. Int J Epidemiol. 2021;50(3):1011–1015. doi:10.1093/ije/dyaa148
30. Miedema MD, Newell MC, Henry TD. Delays in the treatment of STEMI: remarkable progress, room for improvement. Interv. Cardiol. 2012;4(1):1–4. doi:10.2217/ica.11.100
31. Kini AS, Garcia H, Springer B, et al. A mobile application for STEMI care optimization: pilot implementation project report. Int J Cardiol. 2024;415:132447. doi:10.1016/j.ijcard.2024.132447
32. Schoenborn S, Steratore AF, Hoffman A, Marshall TC, Shaver EB, Kiefer CS. Managing stemis without a catheterization lab: a simulated scenario to improve emergency clinician recognition and execution of thrombolysis in the setting of rural stemi management. J. Educ. Teach. Emerg. Med. 2024;9(2):S55–s77.
33. Dunkerton S, Fang R, Sng N, et al. Simulation-based quality improvement and training to improve door to puncture time for mechanical thrombectomy. J. Med. Imaging Radiat. Oncol. 2025;69(4):479–483. doi:10.1111/1754-9485.13845
34. Crowder R, Nakasendwa S, Kityamuwesi A, et al. Scale-up of 99DOTS for TB treatment supervision: an interrupted time series analysis. Int J Tuberc Lung Dis. 2025;29(7):306–311. doi:10.5588/ijtld.24.0587
35. Staples JA, Liu G, Brubacher JR, Karimuddin A, Sutherland JM. Physician financial incentives to reduce unplanned hospital readmissions: an interrupted time series analysis. J Gen Intern Med. 2021;36(11):3431–3440.
36. Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. 2017;46(1):348–355. doi:10.1093/ije/dyw098
37. Nelson BD, McLaughlin CJ, Rivera OE, et al. Implementation of a novel prehospital clinical decision tool and ecg transmission for stemi significantly reduces door-to-balloon time and sex-based disparities. Prehosp Emerg Care. 2025;29(2):170–176. doi:10.1080/10903127.2024.2357595
38. Im J, Evans JM, Grudniewicz A, Boeckxstaens P, Upshur R, Steele Gray C. On the same page? A qualitative study of shared mental models in an interprofessional, inter-organizational team implementing goal-oriented care. J. Interprof. Care. 2023;37(4):549–557. doi:10.1080/13561820.2022.2113048
39. Lu Q, Wang JL, Chen ZN, Fu WB, Liu HJ, Ding SF. The impact of COVID-19 on short-term prognosis of ST-segment elevation myocardial infarction patients receiving primary percutaneous coronary intervention in Wuhan China. Rev cardiovasc med. 2021;22(1):247–256. doi:10.31083/j.rcm.2021.01.243
40. Castillo Costa Y, Delfino F, Palacio S, et al. ARGEN-IAM-ST Registry: older adults with infarction: are they all the same? Medicina. 2024;84(4):682–688.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.