Back to Journals » OncoTargets and Therapy » Volume 9
Association of polymorphisms in interleukin-8 gene with cancer risk: a meta-analysis of 22 case–control studies
Authors Zhang M ![]() , Fang T, Wang K, Mei H, Lv Z, Wang F, Cai Z, Liang C
, Fang T, Wang K, Mei H, Lv Z, Wang F, Cai Z, Liang C
Received 25 December 2015
Accepted for publication 1 April 2016
Published 22 June 2016 Volume 2016:9 Pages 3727—3737
DOI https://doi.org/10.2147/OTT.S103159
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jianmin Xu
Meng Zhang,1–3,* Tingting Fang,1–3,* Kai Wang,1–3,* Hongbing Mei,3 Zhaojie Lv,3 Feng Wang,3 Zhiming Cai,3 Chaozhao Liang1,2
1Department of Urology, The First Affiliated Hospital of Anhui Medical University, 2Institute of Urology, Anhui Medical University, Hefei, Anhui, 3Department of Urology, Shenzhen Second People’s Hospital, The First Affiliated Hospital of Shenzhen University, Shenzhen, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Abstract: Interleukin-8 (IL-8) is a kind of chemokine that plays an important role in the development and progression of many human malignancies. Previous studies have uncovered that polymorphisms in IL-8 is associated with the risk of many cancer types, but the results were inconsistent and inconclusive. In the present study, we aimed to explore the roles of IL-8 polymorphisms (rs2227307, rs2227306, +678T/C, rs1126647, and +1633C/T) and cancer risk through a systematic review and meta-analysis. Potential source of heterogeneity was sought out through sensitivity analysis. Desirable data were extracted and registered into databases. Finally, a total of ten publications comprising of 22 case–control studies, including 4,259 cases and 7,006 controls were ultimately eligible for the meta-analysis. No significant association was uncovered for all the five polymorphisms and the overall cancer risk. However, in the stratification analysis by cancer type, a significantly decreased risk of hepatocellular carcinoma was identified for rs2227306 polymorphism (T vs C: odds ratio [OR] =0.721, 95% confidence interval [CI] =0.567–0.916, Pz=0.007; TT vs CC: OR =0.447, 95% CI =0.274–0.728, Pz=0.001; TT vs TC + CC: OR =0.480, 95% CI =0.304–0.760, Pz=0.002). In conclusion, our data shows that rs2227306 polymorphism plays a protective role in hepatocellular carcinoma risk. Future well-designed studies with a larger sample size are warranted to verify our findings.
Keywords: interleukin-8, polymorphisms, cancer
Introduction
Interleukin-8 (IL-8) is a member of the CXC chemokine superfamily, which can activate neutrophil and lymphocyte attraction and cause a wide range of proinflammatory chemical reactions, generally by initiating and amplifying the acute inflammatory effects and chronic inflammatory process.1,2 It is also reported that IL-8 is related to different malignancies due to the involvement of thrombophilia and angiogenesis.3–5 Increased secretion of IL-8 may contribute to the metastatic ability of hepatocellular carcinoma (HCC),6 gastric cancer,7 renal cell carcinoma,8 colorectal cancer,9 prostate cancer,10 melanoma,11 and bladder neoplasms.12 These observations indicated that IL-8 might act as a biomarker for monitoring the clinical course of many tumor types.
The interleukin production is regulated by the polymorphisms of cytokine genes in promoter regions.13 Thus, IL-8 is located on chromosome 4q13-21 and contains three introns, four exons, and a proximal promoter region.14 Five polymorphisms in IL-8, +781C/T (rs2227306), +678T/C, 276A/T (rs1126647), +1633C/T, and +396G/T (rs2227307), have been extensively studied.15 The +781C/T polymorphism is situated in an intron and acts as an important factor in the process of gene transcription and regulation.16 The +678T/C polymorphism is associated with Behcet’s disease and ulcerative colitis risk although it does not regulate the transcript of IL-8.17,18
A large number of investigations were conducted to explore the associations between IL-8 polymorphisms and risk of human cancers; however, the conclusions were inconsistent.19–28 Therefore, it is necessary to perform a systematic review and meta-analysis to summarize the current available studies in order to draw a more cohesive conclusion.
Materials and methods
Search strategy
A systematic retrieval was performed to identify all eligible studies regarding IL-8 polymorphisms and cancer risk in PubMed, Web of Science, and Embase databases up until August 1, 2015. The combination of search terms were presented as follows: (“IL8” OR “Interleukin 8” OR “IL-8”) AND (“polymorphism” OR “variant” OR “SNP” OR “mutation” OR “genotype”) AND (“tumor” OR “carcinoma” OR “cancer”). The language of the enrolled studies was restricted to English or Chinese. We also conducted a hand search of the reference lists of the enrolled studies or reviews to identify additional eligible studies.
Study selection
Studies concerning the association of IL-8 polymorphisms with cancer risk were included if the following conditions were met: 1) any study described the association between IL-8 polymorphisms and cancer risk; 2) studies were case–control or cohort type; 3) the genotype frequencies of the cases and controls were available; and 4) each enrolled study should comprise at least one of rs2227306, rs2227307, rs1126647, +678T/C, and +1633C/T polymorphisms. Studies were excluded if: 1) there were no data regarding the associations between IL-8 polymorphisms and cancer risk; 2) they were duplicate of previous publications (when the same cohort was used in several publications, only the most complete information was included after careful examination); and 3) they were reviews or abstracts.
Data extraction
The following data from each article were extracted by MZ and TF independently: name of first author, year of publication, ethnicity of the participants (categorized as Caucasians, Asians, etc), source of control, number of controls and cases, genotyping method, and so on. We extracted the data through the following ways: 1) from the articles directly; 2) from the supplementary materials; and 3) by requesting the author through email to send the data.
Statistical analysis
All the statistical analyses were performed using STATA 12.0 statistical software (StataCorp LP., College Station, TX, USA). A χ2-based Q-test assessed the heterogeneity in each research. If P<0.05, it indicated significant heterogeneity, the random-effects model was adopted to estimate the pooled odds ratio (OR);29 otherwise, the fixed-effects model was performed.30 Two-sided P<0.05 were considered statistically significant. The χ2 OR and 95% confidence interval (CI) were applied to evaluate the power of associations between IL-8 gene polymorphisms and cancer risk. Sensitivity analysis was also performed by removing one study at a time to calculate the overall homogeneity and effect size. Publication biases were calculated through Egger’s regression test and Begg’s funnel plot.31,32
Results
Identification and characteristics of the included studies
As presented in Figure 1, the systematic literature retrieval identified a total of 574 relevant publications on PubMed, Web of Science, and Embase databases. After the titles and abstracts were checked only 31 articles related to the association between IL-8 polymorphisms and cancer risk remained. An additional 21 publications were excluded due to the lack of sufficient data, or they were without control groups, or they were related to the survival or treatment. As a result, ten publications comprising of 22 case–control studies were included in the present meta-analysis.
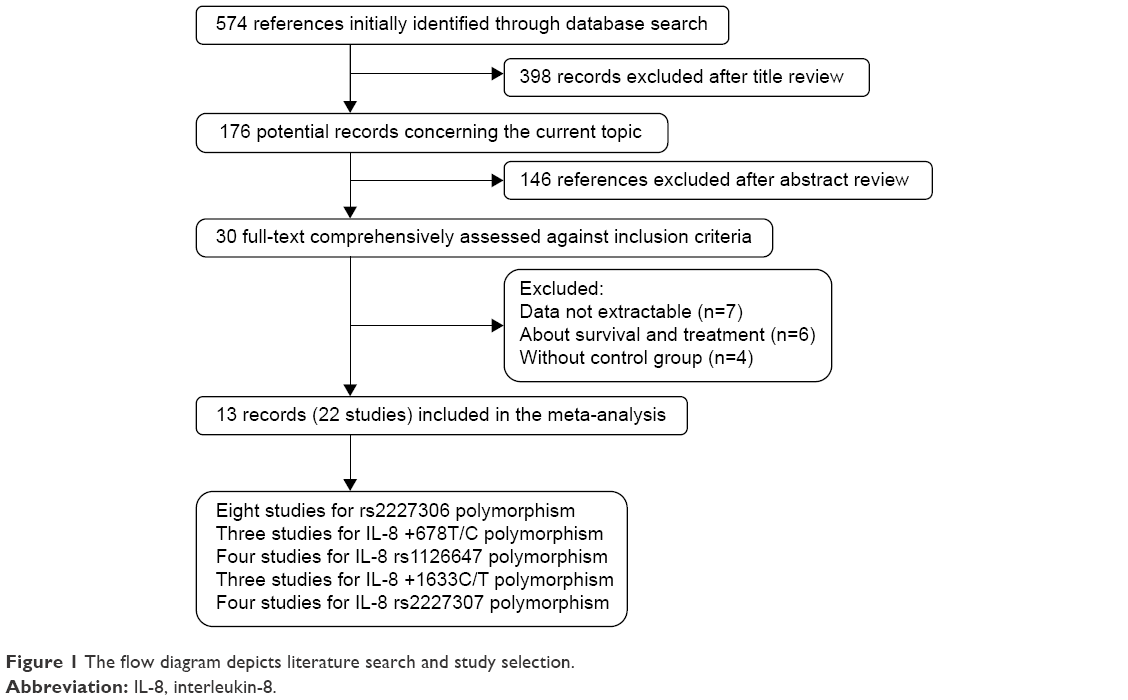 | Figure 1 The flow diagram depicts literature search and study selection. |
The characteristics of the enrolled studies were presented in Table 1. Approximately 14 studies were conducted among Asian descendants19,20,23–26 and eight studies among Caucasians.21,22,27,28 In addition, there were eleven studies conducted by polymerase chain reaction-restriction fragment length polymorphism,19–21,24 four performed by TaqMan,27,28 and only one used polymerase chain reaction-sequence-specific primer.25 The control groups were composed of ten population-based studies22,23,25,27,28 and twelve hospital-based studies.19–21,24,26 Approximately 19 of them were conformed with Hardy–Weinberg equilibrium,19,20,23–27 whereas three others were not.21,22,28 Furthermore, of these included studies, six studies23,27,28 reported about gastric cancer and five about HCC.19,24 Oral cancer20 and ovarian cancer21 were described by three studies.
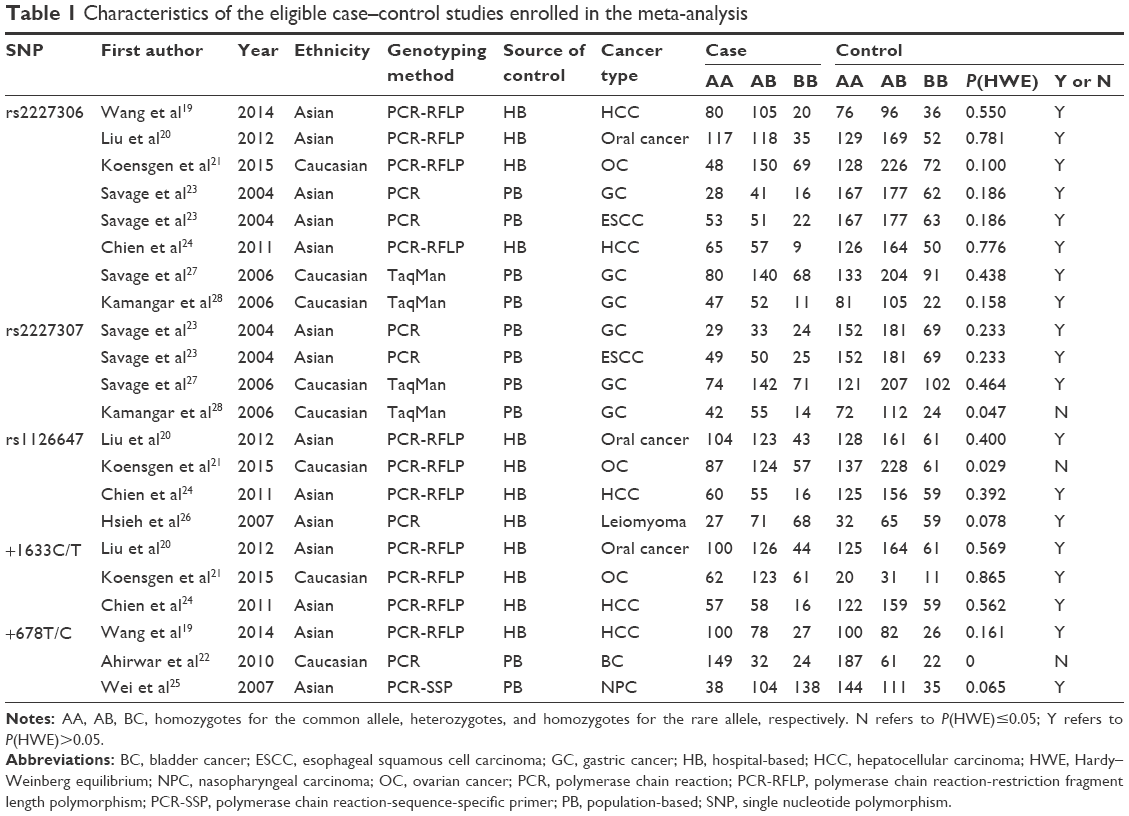 | Table 1 Characteristics of the eligible case–control studies enrolled in the meta-analysis |
Meta-analysis
Table 2 demonstrated the results of meta-analysis. No significant association was identified between the five polymorphisms in IL-8 (rs2227306, rs2227307, +678T/C, rs1126647, and +1633C/T) and the overall cancer risk. Table 2 also shows the results of subgroup analyses, and the data suggested that rs2227306 polymorphism in IL-8 had no significant association with cancer risk in the subgroup analyses sorted by either genotyping method or ethnicity. However, as for the subgroup analysis categorized by cancer type, it demonstrated a decreased risk of HCC (T vs C: OR =0.721, 95% CI =0.567–0.916, Pz=0.007, Figure 2A; TT vs CC: OR =0.447, 95% CI =0.274–0.728, Pz=0.001, Figure 2B; TT vs TC + CC: OR =0.480, 95% CI =0.304–0.760, Pz=0.002, Figure 2C), whereas no evidence showed significant relevance between the IL-8 rs2227306 polymorphism and gastric cancer (T vs C: OR =1.109, 95% CI =0.946–1.300, Pz=0.201; TT vs CC: OR =1.244, 95% CI =0.899–1.723, Pz=0.187; TC vs CC: OR =1.104, 95% CI =0.860–1.419, Pz=0.437; TT + TC vs CC: OR =1.135, 95% CI =0.890–1.447, Pz=0.308).
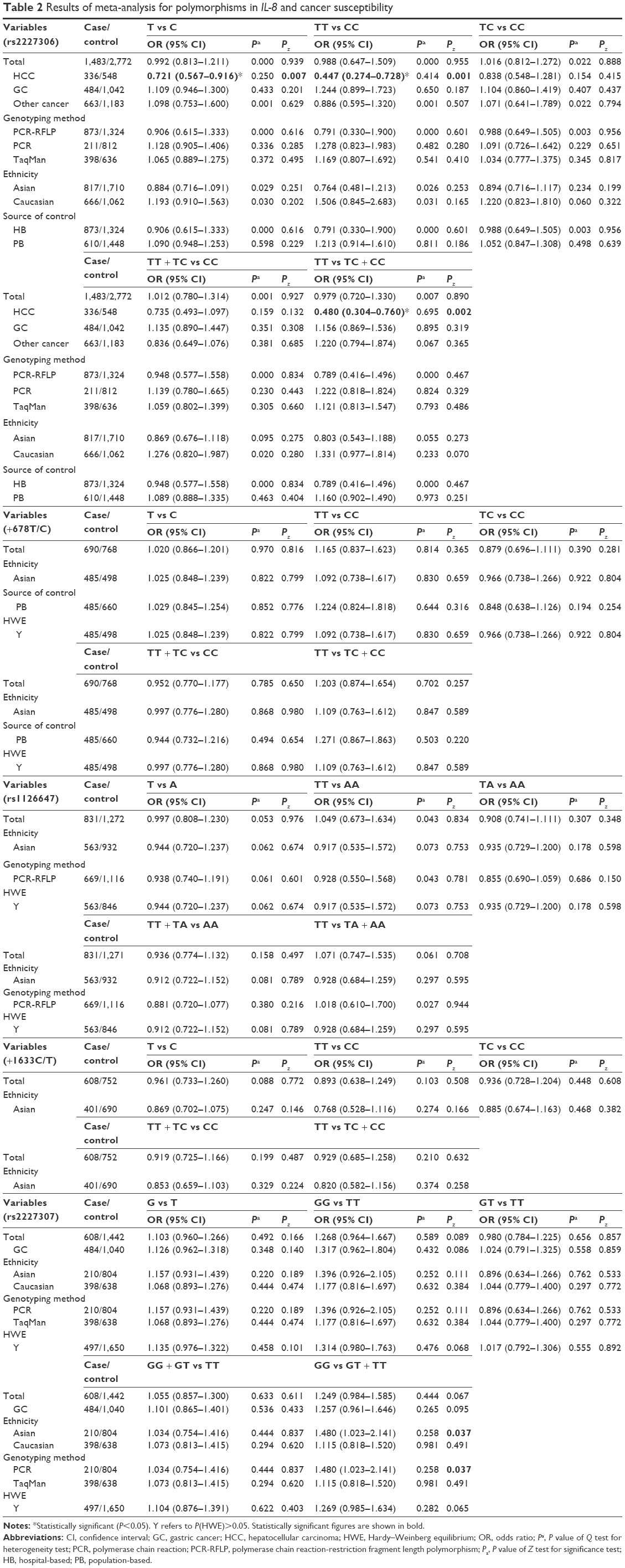 | Table 2 Results of meta-analysis for polymorphisms in IL-8 and cancer susceptibility |
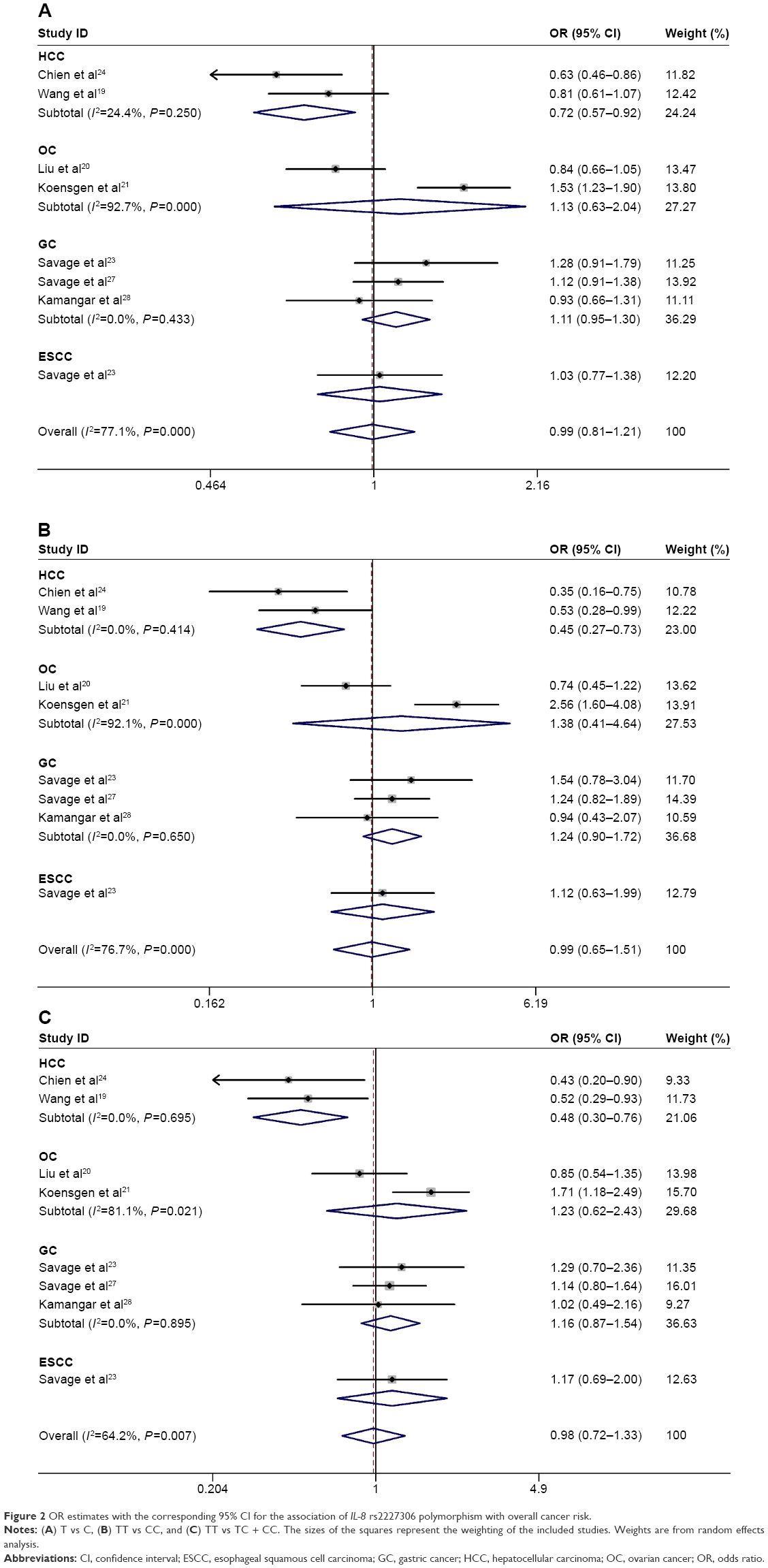 | Figure 2 OR estimates with the corresponding 95% CI for the association of IL-8 rs2227306 polymorphism with overall cancer risk. |
Sensitivity analysis and publication bias
By deleting one study at a time to evaluate the influence of an individual study on synthetic statistics, we referred this method as a sensitivity analysis. As presented in Figure 3, although each study was removed, the overall results did not alter obviously, which indicated the stability of our eligible statistics. In addition, all the enrolled articles were examined by using Begg’s funnel plot and Egger’s test in order to find whether publication bias existed, and as shown in Figure 4, no obvious biases were identified. In addition, the study quality was assessed by Newcastle–Ottawa Scale33 (Table 3).
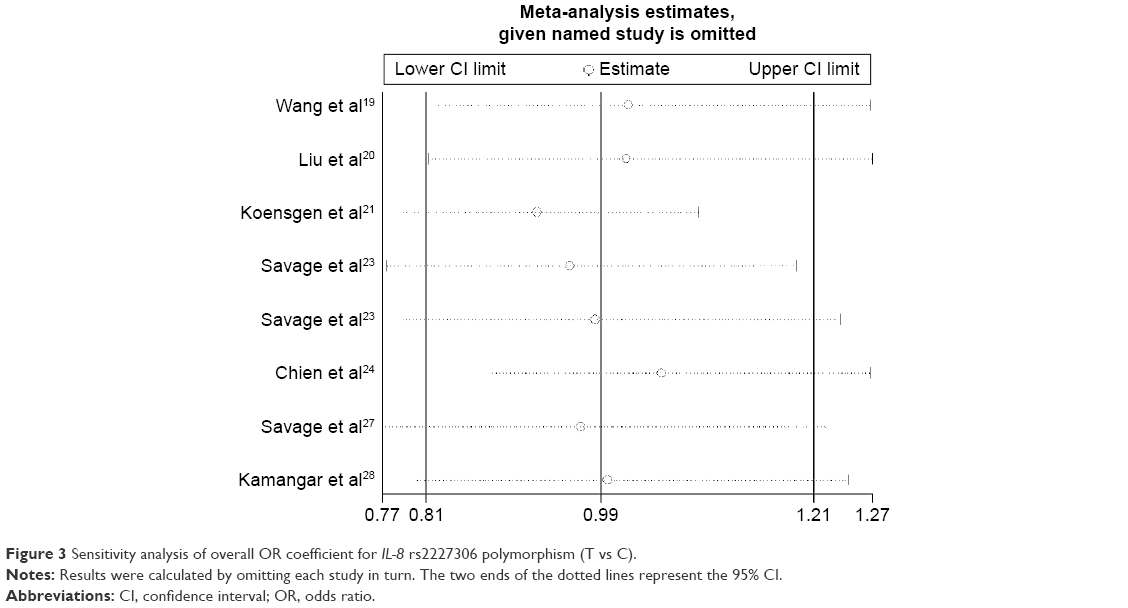 | Figure 3 Sensitivity analysis of overall OR coefficient for IL-8 rs2227306 polymorphism (T vs C). |
 | Figure 4 Publication bias in studies of the association between the IL-8 rs2227306 polymorphism and cancer susceptibility assessed by Begg’s funnel plot. |
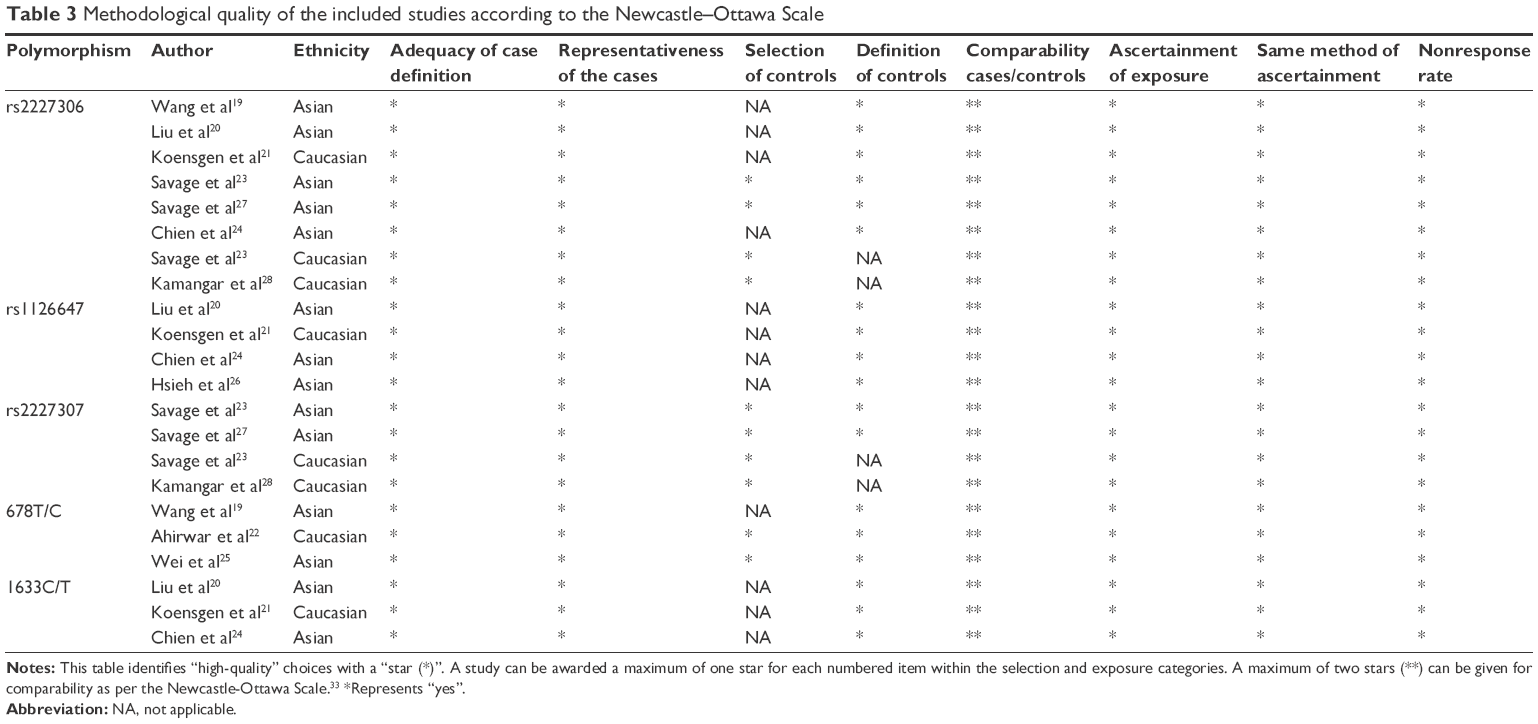 | Table 3 Methodological quality of the included studies according to the Newcastle–Ottawa Scale |
Discussion
IL-8 is a kind of chemokine, which has a significant role in tumorigenesis process, particularly for tumor growth, invasion, and angiogenesis.34 Growing evidence has suggested that abnormal expression of IL-8 may lead to several tumor types, including prostate, breast, lung, and liver cancers.6,10,11 To illustrate the complicated process of tumorigenesis and improve the theory for preventive interventions, main genes associated with cancer risk should be explored.35 Genotyping-related polymorphisms were regarded as eligible and valuable methods in predicting cancer risk and prognosis.
The IL-8 gene, located on chromosome 4q12-21, is 5.2-kb long and is made up of four exons and three introns. A total of five polymorphisms in IL-8 were reported, such as rs4073, rs2227307, rs2227306, +678T/C, rs1126647, and +1633C/T.19,20,22–27 However, only rs4073 and rs2227306 polymorphisms are related to the expression alteration of IL-8.36,37 Rs4073 polymorphism is located at the promoter region of IL-8, and a rare allele A of this polymorphism has been identified, which contributed to an increased level of IL-8.38 In addition, previous studies have confirmed that A allele is associated with an increased risk of many cancer types.19,20,39 Recently, several meta-analysis have been conducted and have identified that rs4073 polymorphism was related to an increased risk of overall cancers and potentially offered an evidence-based medical certificate to investigate cancer risk.35,40,41 Considering that a large number of meta-analyses concentrated on IL-8 rs4073 polymorphism and cancer risk were performed, we focus only on several other polymorphisms in IL-8 and cancer risk. Rs2227306 polymorphism is located at an intron region of IL-8 and is involved in the promotion of gene transcription and regulation,42 while the best strengthening influence on IL-8 expression was the common haplotype rs4073-rs2227306.36 Although several other polymorphisms do not influence the expression of IL-8, many studies have confirmed the association of those polymorphisms with cancer risk. Wang et al19 identified that no association of rs4073, rs2227306, −353A/T, and +678T/C polymorphisms in IL-8 gene and HCC risk was revealed in the Chinese population. Then, Wang et al39 performed a case–control study enrolling 474 breast cancer patients and 501 female nontumor controls and identified that TT genotype of IL-8 rs4073 polymorphism has a significantly reduced risk of breast cancer (TT: OR =0.48, 95% CI =0.33–0.72, P<0.001). In another study, Liu et al20 enrolled 270 patients with oral squamous cell carcinoma and 350 healthy controls, and their results demonstrated that four polymorphisms (rs4073, rs2227306, +1633C/T, and +276A/T) were not related to the risk of oral cancer or clinic pathological characteristics.
Currently, the relationship between IL-8 polymorphisms and cancer risk has been widely reported, but the conclusions remained controversial. Meta-analysis has been regarded as a crucial method to evaluate the influence of chosen genetic polymorphisms on cancer risk. To the very best of our knowledge, this is the first comprehensive meta-analysis of genetics studies on the relevance between IL-8 gene polymorphisms and cancer risk. We indicated a significantly decreased risk of HCC for rs2227306 polymorphism in allele contrast, recessive, and homozygous models.
Limitations
Although we have conducted a general retrieval for all eligible studies, there are several drawbacks that should be mentioned. First, the results may lack statistical power because of the limited sample size and limited number of studies enrolled. Second, only publications indexed in PubMed, Web of Science, and Embase databases were retrieved, while some relevant studies might have been ignored in other databases. Finally, unadjusted estimates were obtained in this work, and a more accurate analysis should be conducted on the basis of specific details such as sex, age, alcohol status, and environmental conditions.
Conclusion
Our meta-analysis suggests that there is no significant relationship between polymorphisms in IL-8 (rs2227307, rs2227306, +678T/C, rs1126647, and +1633C/T) and overall cancer risk. However, in the subgroup analysis by cancer type, a decreased risk of HCC was found for rs2227306 polymorphism. Well-designed studies are needed to further explicit the actual relevance between IL-8 polymorphisms and cancer risk.
Disclosure
The authors report no conflicts of interest in this work.
References
Matsushima K, Baldwin ET, Mukaida N. Interleukin-8 and MCAF: novel leukocyte recruitment and activating cytokines. Chem Immunol. 1992;51:236–265. | ||
Yuan A, Chen JJ, Yao PL, Yang PC. The role of interleukin-8 in cancer cells and microenvironment interaction. Frontiers Biosci. 2005;10:853–865. | ||
Gunter MJ, Canzian F, Landi S, Chanock SJ, Sinha R, Rothman N. Inflammation-related gene polymorphisms and colorectal adenoma. Cancer Epidemiol Biomarkers Prev. 2006;15:1126–1131. | ||
Lerebours F, Vacher S, Andrieu C, Espie M, Marty M, Lidereau R, Bieche I. NF-kappa B genes have a major role in inflammatory breast cancer. BMC Cancer. 2008;8:41. | ||
Zabaleta J, Su LJ, Lin HY, et al. Cytokine genetic polymorphisms and prostate cancer aggressiveness. Carcinogenesis. 2009;30:1358–1362. | ||
Ren Y, Poon RT, Tsui HT, et al. Interleukin-8 serum levels in patients with hepatocellular carcinoma correlations with clinic pathological features and prognosis. Clin Cancer Res. 2003;9:5996–6001. | ||
Zhang XY, Chan WY, Whitney BM, et al. Changes of interleukin expression correlate with Helicobacter pylori infection and lymph node metastases in gastric carcinoma. Diagn Mol Pathol. 2002;11:135–139. | ||
Slaton JW, Inoue K, Perrotte P, et al. Expression levels of genes that regulate metastasis and angiogenesis correlate with advanced pathological stage of renal cell carcinoma. Am J Pathol. 2001;158:735–743. | ||
Li A, Varney ML, Singh RK. Expression of interleukin 8 and its receptors in human colon carcinoma cells with different metastatic potentials. Clin Cancer Res. 2001;7:3298–3304. | ||
Kim SJ, Uehara H, Karashima T, Mccarty M, Shih N, Fidler IJ. Expression of interleukin-8 correlates with angiogenesis, tumorigenicity, and metastasis of human prostate cancer cells implanted orthotopically in nude mice. Neoplasia. 2001;3:33–42. | ||
Huang S, Mills L, Mian B, et al. Fully humanized neutralizing antibodies to interleukin-8 (ABX-IL8) inhibit angiogenesis, tumor growth, and metastasis of human melanoma. Am J Pathol. 2002;161:125–134. | ||
Sheryka E, Wheeler MA, Hausladen DA, Weiss RM. Urinary interleukin-8 levels are elevated in subjects with transitional cell carcinoma. Urology. 2003;62:162–166. | ||
Bidwell J, Keen L, Gallagher G, et al. Cytokine gene polymorphism in human disease: on-line databases, supplement 1. Genes Immun. 2001;2:61–70. | ||
Mukaida N, Shiroo M, Matsushima K. Genomic structure of the human monocyte-derived neutrophil chemotactic factor IL-8. J Immun. 1989;143:1366–1371. | ||
Hull J, Thomson A, Kwiatkowski D. Association of respiratory syncytial virus bronchiolitis with the interleukin 8 gene region in UK families. Thorax. 2000;55:1023–1027. | ||
Li K, Yao S, Liu S, Wang B, Mao D. Genetic polymorphisms of interleukin 8 and risk of ulcerative colitis in the Chinese population. Chinica Chimica Acta. 2009;405:30–34. | ||
Lee E, Kim J, Zhao J, Park M, Song Y. Haplotype association of IL-8 gene with Behcet’s disease. Tissue Antigens. 2007;69:128–132. | ||
Wigmore SJ, Maingay JP, Fearon KC, Ross JA. Endogenous production of IL-8 by human colorectal cancer cells and its regulation by cytokines. Int J Oncol. 2001;18:467–473. | ||
Wang JL, Nong LG, Wei YS, Tang YJ, Wang JC, Wang CF. Association of interleukin-8 gene polymorphisms with the risk of hepatocellular carcinoma. Mol Biol Reports. 2014;41:1483–1489. | ||
Liu CM, Yeh CJ, Yu CC, et al. Impact of interleukin-8 gene polymorphisms and environmental factors on oral cancer susceptibility in Taiwan. Oral Dis. 2012;18:307–314. | ||
Koensgen D, Bruennert D, Ungureanu S, et al. Polymorphism of the IL-8 gene and the risk of ovarian cancer. Cytokine. 2015;71:334–338. | ||
Ahirwar DK, Mandhani A, Mittal RD. IL-8-251 T > A polymorphism is associated with bladder cancer susceptibility and outcome after BCG immunotherapy in a northern Indian cohort. Arch Med Res. 2010;41:97–103. | ||
Savage SA, Abnet CC, Mark SD, et al. Variants of the IL8 and IL8RB genes and risk for gastric cardia adenocarcinoma and esophageal squamous cell carcinoma. Cancer Epidemiol Biomarkers Prev. 2004;13:2251–2257. | ||
Chien MH, Yeh CB, Li YC, et al. Relationship of interleukin-8 gene polymorphisms with hepatocellular carcinoma susceptibility and pathological development. J Surg Oncol. 2011;104:798–803. | ||
Wei YS, Lan Y, Tang RG, et al. Single nucleotide polymorphism and haplotype association of the interleukin-8 gene with nasopharyngeal carcinoma. Clin Immunol. 2007;125:309–317. | ||
Hsieh YY, Chang CC, Tsai CH, Lin CC, Tsai FJ. Interleukin (IL)-12 receptor beta1 codon 378 G homozygote and allele, but not IL-1 (beta-511 promoter, 3953 exon 5, receptor antagonist), IL-2 114, IL-4-590 intron 3, IL-8 3′-UTR 2767, and IL-18 105, are associated with higher susceptibility to leiomyoma. Fertil Steril. 2007;87:886–895. | ||
Savage SA, Hou L, Lissowska J, et al. Interleukin-8 polymorphisms are not associated with gastric cancer risk in a Polish population. Cancer Epidemiol Biomarkers Prev. 2006;15:589–591. | ||
Kamangar F, Abnet CC, Hutchinson AA, et al. Polymorphisms in inflammation-related genes and risk of gastric cancer (Finland). Cancer Causes Control. 2006;17:117–125. | ||
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22:719–748. | ||
DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–188. | ||
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–1101. | ||
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. | ||
Margulis AV, Pladevall M, Riera-Guardia N, et al. Quality assessment of observational studies in a drug-safety systematic review, comparison of two tools: the Newcastle-Ottawa Scale and the RTI item bank. Clin Epidemiol. 2014;6:359–368. | ||
Diekstra MH, Liu X, Swen JJ, et al. Association of single nucleotide polymorphisms in IL8 and IL13 with sunitinib-induced toxicity in patients with metastatic renal cell carcinoma. Eur J Clin Pharmacol. 2015;71:1477–1484. | ||
Xue H, Liu J, Lin B, Wang Z, Sun J, Huang G. A meta-analysis of interleukin-8-251 promoter polymorphism associated with gastric cancer risk. PLoS One. 2012;7:e28083. | ||
Hacking D, Knight JC, Rockett K, et al. Increased in vivo transcription of an IL-8 haplotype associated with respiratory syncytial virus disease-susceptibility. Genes Immun. 2004;5:274–282. | ||
Ross OA, O’Neil C, Rea IM, et al. Functional promoter region polymorphism of the proinflammatory chemokine IL-8 gene associates with Parkinson’s disease in the Irish. Human Immunol. 2004;65:340–346. | ||
Jin WJ, Xu JM, Xu WL, Gu DH, Li PW. Diagnostic value of interleukin-8 in colorectal cancer: a case-control study and meta-analysis. World J Gastroenterol. 2014;20:16334–16342. | ||
Wang Z, Liu QL, Sun W, et al. Genetic polymorphisms in inflammatory response genes and their associations with breast cancer risk. Croat Medical J. 2014;55:638–646. | ||
Wang N, Zhou R, Wang C, et al. -251 T/A polymorphism of the interleukin-8 gene and cancer risk: a huge review and meta-analysis based on 42 case-control studies. Mol Biol Rep. 2012;39:2831–2841. | ||
Gao P, Zhao H, You J, Jing F, Hu Y. Association between interleukin-8-251A/T polymorphism and risk of lung cancer: a meta-analysis. Cancer Investig. 2014;32:518–525. | ||
Li K, Yao S, Liu S, Wang B, Mao D. Genetic polymorphisms of interleukin 8 and risk of ulcerative colitis in the Chinese population. Clinica Chimica Acta. 2009;405:30–34. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.