Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Association of Orthorexic Tendencies with Obsessive-Compulsive Symptoms, Eating Attitudes and Exercise
Authors Yılmaz H ![]() , Karakuş G, Tamam L
, Karakuş G, Tamam L ![]() , Demirkol ME
, Demirkol ME ![]() , Namlı Z
, Namlı Z ![]() , Yeşiloğlu C
, Yeşiloğlu C ![]()
Received 28 September 2020
Accepted for publication 26 November 2020
Published 14 December 2020 Volume 2020:16 Pages 3035—3044
DOI https://doi.org/10.2147/NDT.S280047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Hamdi Yılmaz, Gonca Karakuş, Lut Tamam, Mehmet Emin Demirkol, Zeynep Namlı, Caner Yeşiloğlu
Department of Psychiatry, Çukurova University School of Medicine, Adana, Turkey
Correspondence: Lut Tamam Mehmet Emin Demirkol
Department of Psychiatry, Çukurova University School of Medicine, Adana, Turkey
Tel + 90 533 6306006; +90 535 5849684
Fax +90 322 3386204
Email [email protected]; [email protected]
Purpose: The term orthorexia nervosa is used to describe the pathological fixation associated with consuming healthy food. It is assumed that orthorexia nervosa shares some phenomenological features with anorexia nervosa, obsessive-compulsive disorder (OCD), and other mental disorders. Individuals with orthorexic tendencies may have high physical activity as well as a healthy diet. This study aimed to investigate the relationship of orthorexia nervosa with obsessive-compulsive symptoms, eating attitudes, and several sociodemographic features.
Patients and Methods: We included 63 patients diagnosed with OCD, 63 healthy volunteers who perform physical exercises at least three days a week, at least 30 minutes a day, and 63 healthy volunteers who do not perform physical exercises regularly. Sociodemographic data form, Yale-Brown Obsessive Compulsive Scale, ORTO-11 Scale, Eating Attitude Test, Hamilton Anxiety Scale, and Structured Clinical Interview for DSM-5 Disorders (SCID-5 CV) were administered to all participants. OCD data form was also applied to patients with OCD diagnosis.
Results: We found a statistically significant relationship between current order-symmetry obsessions and orthorexic tendencies in patients with OCD (p< 0.05). There was no relationship between the severity of the disorder and orthorexia nervosa in patients with OCD (p> 0.05). Orthorexic tendencies were found to increase as impaired eating attitudes increased in participants who regularly performed physical exercises and patients with OCD (p< 0.05). The orthorexic tendencies of participants who regularly performed physical exercises were higher than those diagnosed with OCD and healthy individuals who did not perform physical exercises.
Conclusion: The absence of a significant relationship between disorder severity and orthorexia nervosa in patients diagnosed with OCD and the increase in orthorexic tendencies as the deterioration in eating attitudes increases in both patients with OCD and the participants who regularly perform physical exercises suggest that orthorexia nervosa may be closer to the eating disorders group than obsessive-compulsive spectrum. Studies with large samples and different diagnoses are needed to determine the place of orthorexia nervosa in diagnosis and classification systems.
Keywords: orthorexia nervosa, obsessive-compulsive disorder, eating attitudes, exercise
Introduction
Obsessive-compulsive disorder (OCD) is a time-consuming mental disorder characterized by chronic or episodic progress. OCD can cause a decrease in functionality by significantly affecting the usual routine, social life, and relationships of individuals.1 OCD can be comorbid with mental disorders such as anxiety disorders, mood disorders, impulse control disorders, substance use disorders.2 Besides, 10% of individuals diagnosed with OCD may show eating disorders symptoms in some part of their lives.3 OCD and eating disorders are listed under different categories within the psychiatric diagnosis and classification systems; however, studies have demonstrated that both disorder groups have some common cognitive, behavioral, and personality traits. The repetitive and persistent thoughts of patients diagnosed with anorexia nervosa (AN) about their body images and desires to lose weight have been associated with obsessions, and the excessive exercise and ritualized eating attitudes have been associated with compulsions.4
Bratman first described Orthorexia nervosa (ON) as referring to the pathological focus on healthy food consumption.5 ON has not yet been accepted as a separate diagnosis in the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5).6 Orthorexic tendencies usually begin with the goal of getting healthier, curing a disease, or losing weight.5 Efforts to reach optimum health through diet can sometimes lead to malnutrition or weight loss.7,8 Barthels et al suggested that ON may be associated with eating disorders and, in another study, orthorexic symptoms were found to be quite common in patients diagnosed with AN and bulimia nervosa (BN).9,10 On the other hand, individuals with orthorexic tendencies are overly concerned about consuming healthy and pure foods rather than the amount of food consumed, unlike AN and BN.8
Previous studies revealed that orthorexic individuals spend most of their time in strict rules and excessive efforts to choose, prepare, and eat healthy food, similar to the patients with OCD, which may cause deterioration in social functions over time.8,11 Studies in healthy populations have shown that obsessive-compulsive symptoms are associated with orthorexic tendencies.11,12 The catastrophization caused by not performing ritualistic behaviors in OCD can also present in orthorexic individuals. Orthorexic individuals may feel guilty when they do not follow healthy eating rules.10
Intense exercise is considered an important factor in the etiology and continuity of eating disorders, especially AN.13 Orthorexic individuals may experience intense physical activity as well as a healthy diet to achieve excellent physical health.14 Physical activity can turn into exercise addiction from time to time.15,16 It has also been claimed that orthorexic individuals’ motivation to exercise is not only to improve physical health but also to manage stress.17
The ON’s incidence is not precisely known since it is not considered a separate psychiatric diagnosis, and currently, there are no standardized diagnostic tools. Medical doctors, students, and dietitians may have a higher risk of developing ON than the general population.18,19 Individuals who exercise regularly may also have higher orthorexic tendencies.15,16 Previous studies have revealed conflicting results regarding the relationship of ON with the age, gender, education level, and body mass index.20,21 Besides, perfectionism, obsessive-compulsive personality traits, psychopathology, and irregular eating habits were associated with ON.22
In the present study, we aimed to investigate ON’s relationship with the obsessive-compulsive symptoms, eating attitudes, and sociodemographic characteristics in patients with OCD and healthy individuals who exercised regularly and did not exercise. Our first hypothesis was that ON could have a relationship with some clinical features, obsessions, and compulsions in OCD and eating attitudes. Our second hypothesis was that individuals who exercised regularly had higher orthorexic tendencies than those who did not exercise. We thought that this study’s results could contribute to the determination of ON’s significance in the diagnosis and classification systems.
Patients and Methods
Sample
The inclusion criteria for the first interview, according to DSM-5 criteria,6 were: being between 18–65 years of age, having a primary school degree at the minimum regarding the eligibility for completing the self-report tests.
The study included the 79 outpatients with OCD who applied to the Çukurova University Faculty of Medicine (CUFM), Department of Psychiatry between April 2019 and July 2019, 68 healthy controls, who exercised for a minimum of 30 minutes per day and three days per week throughout the last 12 months at the Çukurova University Fitness Center,23 and 69 healthy controls, who did not exercise. We excluded participants with comorbid mental disorders to prevent the confounding effects. Figure 1 presents the flow-chart for the enrolment of the participants.
 |
Figure 1 The flow-chart for enrolment of the participants. |
The final analysis included 63 patients with OCD, 63 healthy individuals who exercise regularly (E+ HC), and 63 healthy individuals who did not exercise (E- HC). We obtained informed written consent from all participants. The Non-Interventional Clinical Research Ethics Committee of CUFM approved the study (April 5, 2019 and decision number 87). The study was conducted in compliance with the Helsinki Declaration. Table 1 presents the sociodemographic features of participants.
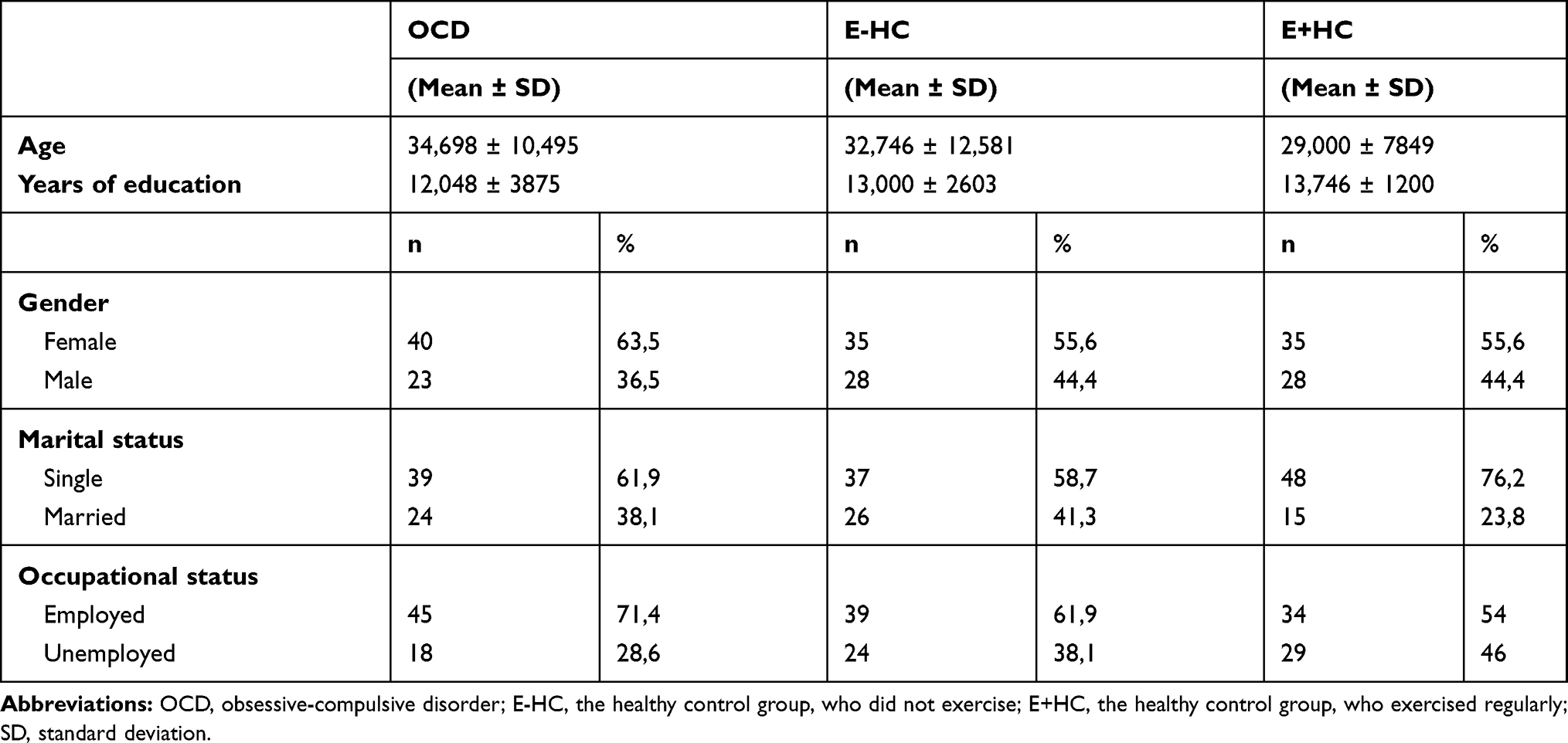 |
Table 1 Sociodemographic Features of Participants |
Power Analysis
We could not identify a similar study in the literature, so we performed a pilot study and tried to predict the sample size. In the power analysis, based on the pilot study’s findings, we calculated that a sample size of 159 subjects in total (for three groups) would be needed for 80% power and a 0.05 type I error rate on the G Power program (version 3.1).24 Therefore, a sample consisting of 189 individuals was determined to have sufficient power.
Procedure
The first author carried out interviews with all participants, which lasted approximately 45–75 minutes. The sociodemographic data form and the OCD data form, which questions the disorder’s clinical characteristics, were filled out during the interviews. We administered the Structured Clinical Interview for DSM-5 Disorders-Clinician Version (SCID-5/CV) to identify the comorbid mental diagnoses, the Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) to evaluate the obsessive-compulsive symptoms and the severity of OCD, the Eating Attitude Test-40 (EAT-40) and ORTO-11 tests to determine eating attitudes and orthorexic symptoms. Hamilton Anxiety Scale (HAS) was used to identify the accompanying anxiety symptoms.
Measures
The Sociodemographic Data Form
The form included information about participants regarding their age, gender, educational level, marital status, occupational status, lifestyle, socio-cultural level, physical disease, family history of mental disorders, and alcohol consumption.
The Obsessive Compulsive Disorder Data Form
The data form we had prepared to be filled out by the clinician inquired the age of onset for obsessive-compulsive symptoms, the age at first diagnosis of OCD, duration of the OCD, the age of onset for treatment, number of hospitalizations, presence of insight, and the suicide attempts. The course of the OCD was assessed by interviews and examination of clinical records.
The Structured Clinical Interview for DSM-5-Clinician Version (SCID-5/CV)
This structured interview contains 32 diagnostic categories with detailed diagnostic criteria and 17 diagnostic categories, including only the exploratory questions.25 In the validity and reliability study of the SCID-5/CV Turkish version, the kappa coefficients between the interviewers were between 0.65 and 1.00. The patient himself, the family and relatives, medical records/documents, and the healthcare team were accepted as information sources during the diagnostic interviews.26
The Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) and Symptom Checklist
The YBOCS is a clinician-rated scale developed by Goodman et al to measure the type and severity of obsessive-compulsive symptoms.27 In the validity and reliability study for the Turkish version, the Cronbach’s alpha value was 0.81.28
The YBOCS consists of 19 items in total, and the scores of the first ten items (except items 1b and 6b) are evaluated. Items 1–5 are about the severity of obsessions, and items 6–10 are about the severity of compulsions. Obsessions and compulsions are scored as 4 points per item. The total score is between 0 and 40.27
The Eating Attitude Test (EAT-40)
The EAT-40 was developed to screen eating disorders.29 In the validity and reliability study of Turkish version, the Cronbach’s alpha value was 0.70.30
It is used to screen potential disturbances in eating behavior, particularly in populations that constitute a high-risk group for AN. It is a self-report scale consisting of 40 questions in a 6-point Likert-type. For items 1, 18, 19, 23, 27, 39, “sometimes” is scored 1 point, “rarely” is scored 2 points and “never” is scored 3 points, while other options are scored as 0 points. For the other items of the scale, “always” is scored 3 points, “very often” is scored 2 points, “often” is scored 1 point, and other options are scored 0 points. The total score of the scale is obtained by adding the scores from each item. Participants with a score of thirty and above are considered to be in the high-risk group for eating disorders, particularly AN.29
The ORTO-11 Test
The ORTO-15 test, the original version, is a self-report tool that consists of 15 items developed by Donini et al and designed to assess the orthorexic tendencies.12 The items question individuals’ behaviors regarding choosing, purchasing, preparing, and consuming the foods they consider healthy. Each item is scored in a 4-point Likert-type from “always” to “never.” Low scores indicate higher orthorexic tendencies.12
In the Turkish version’s validity and reliability study, Arusoğlu et al offered to exclude items 1 (paying attention to the calories of food), 2 (feeling confused in a food shop), 9 (affected eating behavior by mood), 15 (being alone when having meals) and, only the items with a factor loading of 0.50 and above were selected.11 A total of 11 items were determined in this method, and the scale was called ORTO-11. The Cronbach’s alpha coefficient was 0.62 for ORTO-11. The final version of the scale included items 3, 4, 5, 6, 7, 8, 10, 11, 12, 13, and 14. Only item 8 was reversely scored. A three-factor solution explained 40.62% of the variance in ORTO-11. No cut-off value was determined.11
The Hamilton Anxiety Scale (HAS)
This clinician-rated, Likert-type scale determines the level of anxiety and measures the severity changes.31 The HAS consists of 14 items, inquiring both mental and physical symptoms. The increasing scores indicate increasing levels of anxiety. In the validity and reliability study for the Turkish version, the correlation coefficients of the items were found to be 0.72 separately, while the total was 0.94.32
Statistical Analysis
We encoded the data obtained in the study with the SPSS-20 software. Descriptive statistics were shown as mean ± standard deviation according to the distribution of data. The independent groups t-test and one-way ANOVA were used to examine the differences between groups, and the results of the comparison between the groups were obtained by Duncan posthoc analysis. When the number of participants per cell was insufficient for parametric tests, the Kruskal–Wallis H and Mann–Whitney U non-parametric tests were used. The relationships between continuous variables, total scale, and subscale scores were tested with the Pearson correlation analysis since they had a normal distribution.
Results
The Y-BOCS obsession, compulsion, total scores, and the scores of EAT-40, ORTO-11 test, and HAS presented in Table 2 were examined to determine any differences between groups.
 |
Table 2 Comparison of the Groups According to Scale Scores |
The Y-BOCS obsession, compulsion, and total scores differed between the OCD, E-HC and E+HC groups. The scores obtained by the patients with OCD were higher compared to the E-HC and E+HC groups (p<0.001). The control groups’ scores, who did not exercise and exercised regularly, did not differ (p>0.05).
The EAT-40 scores of the OCD group and the E+HC group, were similar (p>0.05); however, the EAT-40 scores of these two groups were significantly higher than the E-HC group (p<0.001).
When the groups were compared according to the ORTO-11 test scores, the orthorexic symptoms of the E+HC group, were higher than the OCD group and the E-HC group (p<0001). The scores of patients with OCD did not differ significantly from the scores of the E-HC group (p>0.05).
The HAS scores of the patients with OCD were higher than the E-HC group and E+HC group; and the E-HC group’s scores were higher than the E+HC group (p<0.001, for each).
There was a significant relationship in the OCD group between the ORTO-11 test and EAT-40 scores (p<0.01). There were no significant relationships between the ORTO-11 test, Y-BOCS obsession-compulsion, and HAS scores (p>0.05).
There were no significant relationships between the ORTO-11 test scores and the other scales in the E-HC group (p>0.05).
Table 3 revealed a significant relationship in the E+HC group, between the scores of the ORTO-11 test and EAT-40 (p<0.05). However, there were no significant relationships between the ORTO-11 test scores, Y-BOCS obsession-compulsion scores, and HAS scores (p>0.05).
 |
Table 3 The Correlation Between the ORTO-11 Test and Other Scales |
In Table 4, we investigated whether the ORTO-11 test scores in patients with OCD differed according to the Y-BOCS symptom checklist; orthorexic tendencies with current order-symmetry obsessions were higher compared to the patients with no such obsessions (p=0.03). However, ON had no statistically significant relationship with aggression, contamination, hoarding/hiding obsessions, sexual, religious, and somatic obsessions, cleaning/washing, checking, counting and hoarding/collecting compulsions, and repetitive ritual behaviors (p>0.05).
 |
Table 4 The Relationship Between Obsessive-Compulsive Symptoms and Orthorexic Tendencies in Patients with OCD |
When the ORTO-11 test scores of the patients with OCD were examined in terms of their correlation with the sociodemographic data, ON had no significant correlation with gender, marital status, employment status, place of residence, smoking, and alcohol consumption (p>0.05).
There were no significant relationships between ON and the level of insight, presence of a traumatic experience, stress factor at the onset of the OCD, history of suicide attempts, treatment compliance, the age at onset of obsessive-compulsive symptoms, the age at the onset of the first treatment, the period between the onset of the OCD and the first treatment, the age at first diagnosis of OCD and the number of hospitalizations.
Discussion
Researchers continue to discuss the place of ON among mental disorders. While certain researchers suggest that ON is a separate clinical diagnosis, some highlight the similarities between ON and eating disorders. Besides, some authors have classified ON as a manifestation of OCD.33 This study aimed to contribute to the literature by investigating the relationship between orthorexic tendencies and obsessive-compulsive symptoms, eating attitudes and, sociodemographic features in three different samples. Our results indicated that orthorexic tendencies were higher in individuals who perform physical exercises than other participants. Besides, we found that as the deterioration in eating attitude increases in individuals who regularly perform physical exercises and patients with OCD, orthorexic tendencies also increase.
Regular physical activities play an essential role in a healthy lifestyle, weight control, protecting heart health, and stress management. However, intense exercise is associated with different eating disorders.34 Kiss-Leizer et al also suggested that the increase in physical activity plays an important role in the development of orthorexic tendencies.34 Oberle et al reported that orthorexic individuals perform physical exercises and apply strict exercise programs to improve their health, but this situation may cause injury and diseases from time to time.17 It has also been suggested that these individuals may have obsessive tendencies towards exercise as well as eating behavior.35 Segura-Garcia et al compared the individuals who exercise regularly and the individuals who prefer a sedentary life and found that orthorexic tendencies and deterioration in eating attitudes were significantly higher in the group who exercised regularly.16 Dalle Grave et al investigated a group of patients with eating disorders and found that 45.5% of the participants were compulsive exercises, with the highest rate in the restricting type AN.36 Patients with eating disorders are more likely to do intense physical exercise to regulate negative emotional states rather than improving overall health. A recent study showed that the content of obsessive thinking in ON may be related to healthy eating and also to the sports activities. Kiss-Leizer et al suggested that individuals with orthorexic tendencies try to balance the weaknesses in their internal control and self-management skills through behavioral mechanisms in the form of physical activities.34 In the light of these data, an important outcome of this study is that the orthorexic symptoms in E+HC group, were significantly higher than the patients with OCD and the E-HC group, which is consistent with the previous studies.
Arusoglu et al investigated the relationship between eating attitudes and orthorexic tendencies and found that the group with eating disorders had higher orthorexic tendencies.11 In another study, Lucka et al found a significant relationship between eating disorders and the risk of ON.33 Both AN and ON are characterized by perfectionism, high anxiety levels, and a strong need for control. Both disorders’ common characteristics include keeping dietary restrictions as an indicator of self-discipline and perceiving each dietary violation as a failure. Lucka et al suggested that ON is not a separate clinical entity. It does not belong to the OCD spectrum but meets the criteria of the eating disorders spectrum.33 Our results that the orthorexic symptoms increased in the E+HC group, as the deterioration in eating attitude increased, supports the hypotheses that ON can be related to eating disorders in the diagnostic classification.
ON is characterized by obsessions (eg, overthinking about food preparation), compulsive behaviors (eg, food preparation rituals, weighing products), impaired social functions, and decreased quality of life like OCD.7 Previous studies have shown that obsessive-compulsive symptoms can be present in orthorexic individuals.37,38 Obsessive-compulsive symptoms have a significant effect on orthorexic tendencies, and as these symptoms increase, orthorexic tendencies increase.10,11 Barthels et al found a high prevalence of ON in a sample of patients with eating disorders; however, they found the prevalence of ON in patients with OCD similar to the general population.9 Our study results that there was no statistically significant relationship between the severity of OCD and ON, and that there were high orthorexic tendencies in patients with order-symmetry obsessions, which are also common in eating disorders, support the hypothesis that OCD and ON are two separate disorders. Our findings suggest that ON could be closer to eating disorders within the diagnostic and classification systems.
Another important outcome of the present study is to determine the relationship between current order-symmetry obsessions in patients with OCD and orthorexic tendencies. The cognitive interpretation of OCD involves the themes of perfectionism, impaired external observation, and anxiety. Another characteristic of OCD is the thought that harmful consequences would occur in proportion to the perceived threat when the rituals are not completed.39 This thought is similar to the anxiety experienced in ON when healthy eating rules are not followed sufficiently. Besides, the order-symmetry obsessions in OCD could represent the carefulness in the selection and preparation of food. Individuals with orthorexic tendencies spend a long time preparing their food; they may feel distressed when they think that this process is not entirely appropriate, and may repeat the same process.12,39 In a study comparing patients with the restricting type AN and patients with OCD, both groups were similar in terms of symmetry and somatic obsessions.40 Matsunaga et al found that order-symmetry obsessions and cleaning-washing compulsions were more common in patients with OCD accompanied by AN.41 Similarly, in another study evaluating the patients with OCD accompanied by BN; the order-symmetry obsessions and control and regulation compulsions were the most common symptoms.35 Our study shows that the high orthorexic symptoms in the group with current order-symmetry obsession are consistent with previous studies.
Advanced age is thought to be associated with healthy eating behavior;42 however, Arusoğlu et al showed that the age factor was not related to orthorexic tendencies in the Turkish population.11 Similarly, Lucka et al did not find any relationship between orthorexic symptoms and sociodemographic data such as gender, age, education level and place of residence.33 According to these data, it is not surprising that there was no relationship between ON and age in our study. There are conflicting results on the relationship between ON and gender. Several studies found that orthorexic tendencies were higher in the men compared to the women;12,43,44 however, some studies are indicating that there are no differences according to the genders.18 There may be differences in the approach to nutrition and health in societies, so orthorexic tendencies and behaviors may vary between cultures.21 We found no difference in orthorexic tendencies between male and female patients with OCD in the Turkish population; this could be explained with the hypothesis33 that there may be cross-cultural differences in the development of orthorexic tendencies.
Our study is one of the rare studies to examine ON in a clinical population. Besides, including healthy individuals who exercised regularly, expecting that their orthorexic symptoms could be high as in the patients with OCD could be listed among the strengths of our study. Our study has certain limitations. Since our cross-sectional design, we did not follow orthorexic symptoms longitudinally, so we could not determine whether these symptoms were related to the disorder’s course or the treatment change. Since all patients were under treatment in our study, the effect of drugs on orthorexic behavior remains unknown. The fact that we did not include other mental disorders among obsessive-compulsive spectrum disorders in DSM-5 could be considered another limitation.6 Although there are several better measures than ORTO-11 to assess orthorexic tendencies like the Eating Habits Questionnaire, the Orthorexia Nervosa Inventory, and the Düsseldorf Orthorexia Scale, we could not use them since they have not yet been validated in Turkish.45–47 We did not question whether the participants in our sample did intense exercises or why they did exercise. To generalize this study’s results, longitudinal studies involving participants from different cultures, investigating obsessive-compulsive personality traits, and examining personality traits’ effects on orthorexic behaviors would be useful. Revealing the cognitive processes underlying orthorexic tendencies would help to administer appropriate personalized cognitive therapies to these individuals. Identifying the risk factors associated with ON and the biological processes would ensure the administration of drug treatment more effectively.
Conclusion
ON is a phenomenon that has been the focus of attention in recent years, but its place in diagnosis and classification systems is still unclear. Our study results show that ON is associated with eating disorders rather than OCD, and people who exercise regularly have more orthorexic tendencies than those who do not. Future studies evaluating orthorexic tendencies in different disorder groups will help the diagnostic classification of ON.
Ethics
This study was approved by the Ethics Committee for Non-Invasive Clinical Research at Çukurova University School of Medicine.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors declare that they did not receive any financial support for this study.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Rasmussen SA, Tsuang MT. Clinical characteristics and family history in DSM-III obsessive-compulsive disorder. Am J Psychiatry. 1986;143(3):317–322. doi:10.1176/ajp.143.3.317
2. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the national comorbidity survey replication. Mol Psychiatry. 2010;15(1):53–63. doi:10.1038/mp.2008.94
3. Meier M, Kossakowski JJ, Jones PJ, Kay B, Riemann BC, McNally RJ. Obsessive–compulsive symptoms in eating disorders: A network investigation. Int J Eat Disord. 2020;53(3):362–371. doi:10.1002/eat.23196
4. Kaye WH, Weltzin T, Hsu LKG. Relationship between anorexia nervosa and obsessive and compulsive behaviors. Psychiatr Ann. 1993;23(7):365–373. doi:10.3928/0048-5713-19930701-07
5. Bratman S, Knight D. Health Food Junkies: Orthorexia Nervosa: Overcoming the Obsession with Healthful Eating.
6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
7. Brytek-Matera A, Fonte ML, Poggiogalle E, Donini LM, Cena H. Orthorexia nervosa: relationship with obsessive-compulsive symptoms, disordered eating patterns and body uneasiness among Italian university students. Eat Weight Disord. 2017;22(4):609–617. doi:10.1007/s40519-017-0427-4
8. Strand E. A new eating disorder? Psychol Today. 2004;37(5):1–3.
9. Barthels F, Meyer F, Huber T, Pietrowsky R. Orthorektisches ernährungsverhalten bei patienten mit essstörungen und mit zwangsstörungen [Analysis of orthorexic eating behavior in patients with eating disorder and obsessive-compulsive disorder]. Z Klin Psychol Psychother. 2017;(46):32–41. doi:10.1026/1616-3443/a000399
10. Poyraz CA, Tüfekçioğlu EY, Özdemir A, et al. Relationship between orthorexia and obsessive-compulsive symptoms in patients with generalised anxiety disorder, panic disorder and obsessive compulsive disorder. Yeni Symposium. 2016;53(4):22–26. doi:10.5455/NYS.20160324065040
11. Arusoğlu G, Kabakçi E, Köksal G, Merdol TK, Abstract Ö. Ortoreksiya nervoza ve orto- 11ʹ in türkçeye uyarlama çalışması. Turk Psikiyatri Derg. 2008;19(3):283–291.
12. Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C. Orthorexia nervosa: validation of a diagnosis questionnaire. Eat Weight Disord. 2005;10(2):28–32. doi:10.1007/BF03327537
13. Meyer C, Taranis L, Goodwin H, Haycraft E. Compulsive exercise and eating disorders. Eur Eat Disord Rev. 2011;19(3):174–189. doi:10.1002/erv.1122
14. Malmborg J, Bremander A, Olsson MC, Bergman S. Health status, physical activity, and orthorexia nervosa: A comparison between exercise science students and business students. Appetite. 2017;109:137–143. doi:10.1016/j.appet.2016.11.028
15. Varga M, Thege BK, Dukay-Szabó S, Túry F, van Furth EF. When eating healthy is not healthy: orthorexia nervosa and its measurement with the ORTO-15 in Hungary. BMC Psychiatry. 2014;14:59. doi:10.1186/1471-244X-14-59
16. Segura-García C, Papaianni MC, Caglioti F, et al. Orthorexia nervosa: A frequent eating disordered behavior in athletes. Eat Weight Disord. 2012;17(4):226–233. doi:10.3275/8272
17. Oberle CD, Watkins RS, Burkot AJ. Orthorexic eating behaviors related to exercise addiction and internal motivations in a sample of university students. Eat Weight Disord. 2018;23(1):67–74. doi:10.1007/s40519-017-0470-1
18. Baǧci Bosi AT, Çamur D, Güler Ç. Prevalence of orthorexia nervosa in resident medical doctors in the faculty of medicine (Ankara, Turkey). Appetite. 2007;49(3):661–666. doi:10.1016/j.appet.2007.04.007
19. Alvarenga MDS, Martins MCT, Sato KSCJ, Vargas SVA, Philippi ST, Scagliusi FB. Orthorexia nervosa behavior in a sample of Brazilian dietitians assessed by the Portuguese version of ORTO-15. Eat Weight Disord. 2012;17(1):29–35. doi:10.1007/BF03325325
20. Varga M, Dukay-szabo S, Tury F, Van Furth EF. Evidence and gaps in the literature on orthorexia nervosa. Eat Weight Disord. 2013;18(2):103–111. doi:10.1007/s40519-013-0026-y
21. Gramaglia C, Rogoza R, Zeppegno P. Orthorexia and anorexia nervosa: two distinct phenomena? A cross-cultural comparison of orthorexic behaviours in clinical and non-clinical samples. BMC Psychiatry. 2017;17(1):75. doi:10.1186/s12888-017-1241-2
22. McComb SE, Mills JS. Orthorexia nervosa: A review of psychosocial risk factors. Appetite. 2019;140:50–75. doi:10.1016/j.appet.2019.05.005
23. Kwak YS, Um SY, Son TG, Kim DJ. Effect of regular exercise on senile dementia patients. Int J Sports Med. 2008;29(6):471–474. doi:10.1055/s-2007-964853
24. Erdfelder E, FAul F, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
25. Osorio FL, Loureiro SR, Hallak JEC, et al. Clinical validity and intrarater and test–retest reliability of the structured clinical interview for DSM‐5 – clinician Version (SCID‐5‐CV). Psychiatry Clin Neurosci. 2019;73(12):754–760. doi:10.1111/pcn.12931
26. Elbi̇r M, Alp Topbaş Ö, Bayad S, et al. DSM-5 Bozuklukları için yapılandırılmış klinik görüşmenin klinisyen versiyonunun türkçeye uyarlanması ve güvenilirlik çalışması. Turk Psikiyatri Derg. 2019;30(1):51–56. doi:10.5080/u23431
27. Goodman WK, Price LH, Rasmussen SA, et al. The yale-brown obsessive compulsive scale: i. development, use, and reliability. Arch Gen Psychiatry. 1989;46(11):1006–1011. doi:10.1001/archpsyc.1989.01810110048007
28. Tek C, Ulug B, Rezaki BG, et al. Yale- brown obsessive compulsive scale and US national institute of mental health global obsessive compulsive scale in Turkish: reliability and validity. Acta Psychiatr Scand. 1995;91:410–413. doi:10.1111/j.1600-0447.1995.tb09801.x
29. Garner DM, Garfinkel PE. The eating attitudes test: an index of the symptoms of anorexia nervosa. Psychol Med. 1979;9(2):273–279. doi:10.1017/S0033291700030762
30. Savasir I, Erol N. Yeme tutum testi: anoreksia nervosa belirtiler indeksi. Psikol Derg. 1989;7(23):19–25.
31. Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. doi:10.1111/j.2044-8341.1959.tb00467.x
32. Yazıcı MK, Demir B, Tanrıverdi N, Karaağaoğlu E, Yolaç P. Hamilton Anksiyete Değerlendirme Ölçeği, değerlendiriciler arası güvenirlik ve geçerlik çalışması. Türk Psikiyatr Derg. 1998;9(2):114–117.
33. Łucka I, Janikowska-Hołoweńko D, Domarecki P, Plenikowska-Ślusarz T, Domarecka M. Orthorexia nervosa - A separate clinical entity, a part of eating disorder spectrum or another manifestation of obsessive-compulsive disorder? Psychiatr Pol. 2019;53(2):371–382. doi:10.12740/PP/OnlineFirst/85729
34. Kiss-Leizer M, Tóth-Király I, Rigó A. How the obsession to eat healthy food meets with the willingness to do sports: the motivational background of orthorexia nervosa. Eat Weight Disord - Stud Anorexia, Bulim Obes. 2019;24(3):465–472. doi:10.1007/s40519-019-00642-7
35. Matsunaga H, Kiriike N, Miyata A, et al. Prevalence and symptomatology of comorbid obsessive-compulsive disorder among bulimic patients. Psychiatry Clin Neurosci. 1999;53(6):661–666. doi:10.1046/j.1440-1819.1999.00622.x
36. Dalle Grave R, Calugi S, Marchesini G. Compulsive exercise to control shape or weight in eating disorders: prevalence, associated features, and treatment outcome. Compr Psychiatry. 2008;49(4):346–352. doi:10.1016/j.comppsych.2007.12.007
37. Koven NS, Wabry A. The clinical basis of orthorexia nervosa: emerging perspectives. Neuropsychiatr Dis Treat. 2015;11:385–394. doi:10.2147/NDT.S61665
38. Koven NS, Senbonmatsu N. A neuropsychological evaluation of orthorexia nervosa. Open J Psychiatr. 2013;3:214–222. doi:10.4236/ojpsych.2013.32019
39. Altman SE, Shankman SA. What is the association between obsessive-compulsive disorder and eating disorders? Clin Psychol Rev. 2009;29(7):638–646. doi:10.1016/j.cpr.2009.08.001
40. Halmi KA, Sunday SR, Klump KL, et al. Obsessions and compulsions in anorexia nervosa subtypes. Int J Eat Disord. 2003;33(3):308–319. doi:10.1002/eat.10138
41. Matsunaga H, Kiriike N, Iwasaki Y, Miyata A, Yamagami S, Kaye WH. Clinical characteristics in patients with anorexia nervosa and obsessive-compulsive disorder. Psychol Med. 1999;29(2):407–414. doi:10.1017/s003329179800796x
42. Shelton NJ. What not to eat: inequalities in healthy eating behaviour, evidence from the 1998 scottish health survey. J Public Health. 2005;27(1):36–44. doi:10.1093/pubmed/fdh191
43. Donini LM, Marsili D, Graziani MP, Imbriale M, Cannella C. Orthorexia nervosa: A preliminary study with a proposal for diagnosis and an attempt to measure the dimension of the phenomenon. Eat Weight Disord. 2004;9(2):151–157. doi:10.1007/BF03325060
44. Fidan T, Ertekin V, Işikay S, Kirpinar I. Prevalence of orthorexia among medical students in Erzurum, Turkey. Compr Psychiatry. 2010;51(1):49–54. doi:10.1016/j.comppsych.2009.03.001
45. Gleaves DH, Graham EC, Ambwani S. Measuring “orthorexia”: development of the eating habits questionnaire. Int J Educ Psychol Assess. 2013;12(2):1–18.
46. Oberle CD, De NAS, Madrid AL. Orthorexia Nervosa Inventory (ONI): development and validation of a new measure of orthorexic symptomatology. Eat Weight Disord. 2020. doi:10.1007/s40519-020-00896-6
47. Barthels F, Meyer F, Pietrowsky R. Die Düsseldorfer Orthorexie Skala—konstruktion und evaluation eines fragebogens zur erfassung orthorektischen ernährungsverhaltens. Z Klin Psychol Psychother. 2015;44:97–105. doi:10.1026/1616-3443/a000310
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.