Back to Journals » Nature and Science of Sleep » Volume 14
Association of Obstructive Apnea with Thoracic Fluid Shift and Small Airways Narrowing in Asthma During Sleep
Authors Cao X, de Oliveira Francisco C, Bradley TD, Montazeri Ghahjaverestan N, Tarlo SM, Stanbrook MB, Chapman KR, Inman M, Yadollahi A ![]()
Received 19 January 2022
Accepted for publication 20 April 2022
Published 6 May 2022 Volume 2022:14 Pages 891—899
DOI https://doi.org/10.2147/NSS.S359021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Xiaoshu Cao,1,2 Cristina de Oliveira Francisco,2 T Douglas Bradley,2– 4 Nasim Montazeri Ghahjaverestan,1,2 Susan M Tarlo,3,5,6 Matthew B Stanbrook,3,5 Kenneth R Chapman,3,5 Mark Inman,7 Azadeh Yadollahi1,2
1Institute of Biomedical Engineering, University of Toronto, Toronto, ON, Canada; 2KITE, Toronto Rehabilitation Institute - University Health Network, Toronto, ON, Canada; 3Department of Medicine, University of Toronto, Toronto, ON, Canada; 4Department of Medicine, University Health Network Toronto General Hospital, Toronto, ON, Canada; 5Department of Medicine, University Health Network Toronto Western Hospital, Toronto, ON, Canada; 6Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada; 7Faculty of Medicine (Respirology), McMaster University, Hamilton, ON, Canada
Correspondence: Azadeh Yadollahi, KITE, Toronto Rehabilitation Institute - University Health Network, Room 12-106, 550 University Avenue, Toronto, ON, M5G 2A2, Canada, Email [email protected]
Rationale: Obstructive sleep apnea (OSA) is highly prevalent among patients with asthma, suggesting a pathophysiological link between the two, but a mechanism for this has not been identified.
Hypothesis: Among patients with asthma, those with OSA will have greater overnight increases in thoracic fluid volume and small airways narrowing than those without OSA.
Methods: We enrolled 19 participants with asthma: 9 with OSA (apnea-hypopnea index (AHI) ≥ 10) and 10 without OSA (AHI < 10). All participants underwent overnight polysomnography. Before and after sleep, thoracic fluid volume was measured by bioelectrical impedance and small airways narrowing was primarily assessed by respiratory system reactance at 5Hz using oscillometry.
Results: Patients with asthma and OSA (OSA group) had a greater overnight increase in thoracic fluid volume by 120.5 mL than patients without OSA (non-OSA group) (164.4 ± 44.0 vs 43.9 ± 47.3 mL, p=0.006). Compared to the non-OSA group, the OSA group had greater overnight decrease in reactance at 5Hz (− 1.08 ± 0.75 vs 0.21 ± 0.27 cmH2O/L/s, p=0.02), and overnight increase in reactance area (14.81 ± 11.09 vs − 1.20 ± 2.46 cmH2O/L, p=0.04), frequency dependence of resistance (1.02 ± 0.68 vs 0.05 ± 0.18 cmH2O/L/s, p=0.04), and resonance frequency (2.80 ± 4.14 vs − 1.42 ± 2.13 cmH2O/L/s, p=0.04).
Conclusion: Patients with asthma and co-existing OSA had greater overnight accumulation of fluid in the thorax in association with greater small airways narrowing than those without OSA. This suggests OSA could contribute to worsening of asthma at night by increasing fluid accumulation in the thorax.
Keywords: asthma, obstructive sleep apnea, small airway narrowing, thoracic fluid volume
Introduction
Both asthma and obstructive sleep apnea (OSA) are highly prevalent chronic respiratory disorders.1,2 They cause disability, morbidity, and poor quality of life.1,2 OSA affects approximately 10% of adult Americans,3 and is caused by recurrent collapse of the pharynx during sleep.4 Obstructive apneas cause hypoxia, surges in sympathetic nervous system activity and blood pressure, and sleep fragmentation. Asthma affects approximately 8–15% of adult Canadians and 3.5–5.1% of adults globally.5,6 Asthma is characterized by reversible bronchoconstriction and airways inflammation accompanied by exacerbations of wheezing, shortness of breath, and cough.7,8 The prevalence of OSA in patients with asthma ranges between 19–60% and 50–95% in those with severe asthma.9–12 OSA is also associated with double the incidence of asthma symptoms during the day and worsening of asthma at night,9,11–13 as well as a more rapid decline in forced expiratory volume in 1 second (FEV1) over 5 years.14 OSA remains undiagnosed in approximately 80% of the general population15,16 and is likely overlooked in people with asthma as well.17 The above evidence suggests a pathophysiological link between asthma and OSA. However, few studies have investigated why OSA could predispose to, or worsen asthma.
A pathophysiological link between OSA and asthma could include intermittent hypoxia, local and systemic inflammation,18 circadian alteration in autonomic function,19 obesity,20 and sleep-induced reduction in lung volume.4,21 However, these mechanisms do not explain for increases in nocturnal asthma symptoms. For example, in people with asthma, airways resistance increases overnight whether awake or asleep, but increases more during sleep.22 This indicates an independent contribution of sleep beyond any potential circadian effect.
We have previously shown that induction of fluid shifts out of the legs into the thorax by inflating anti-shock trousers induces small airways narrowing in people with asthma.23,24 Also, performing Mueller maneuvers to simulate the exaggerated negative pleural pressure generated during obstructive apneas, draws fluid into the thorax in those with asthma and induces increased small airways narrowing probably by increasing airways mucosal fluid content.25 These studies suggest that in people with asthma, some fluid shifting out of the legs overnight23–25 can accumulate in the thorax and around small airways, causing them to narrow. In view of the above, we hypothesized that patients with asthma and co-existing OSA will have a larger increase in thoracic fluid volume and greater small airways narrowing, than those without OSA, due to a larger degree of negative intrathoracic pressure generated by obstructive apneas.
Methods
Participants
We included adults ≥ 18 years of age, with a body mass index ≤ 35 kg/m2, with clinical diagnosis of asthma, who were never-smokers or ex-smokers with a smoking history < 10 pack-years. Exclusion criteria were any cardiovascular or renal disorders, or the use of any medication for these conditions, or the use of medication that might influence fluid retention (eg diuretics). Participants with asthma were recruited consecutively from pulmonary clinics at the University Health Network (UHN), Toronto, with the diagnosis based on Global Initiative for Asthma guidelines.27 The experimental protocol was approved by the Research Ethics Board of UHN, and all participants were informed about the purpose of the study, in accordance with the Declaration of Helsinki, and provided written consent prior to participation.
Questionnaires
Participants’ level of asthma control was assessed by the Asthma Control Test28 and Asthma Control Questionnaire29 (ACT and ACQ, respectively).
Oscillometry
The primary outcome was reactance at 5 Hz (X5) as assessed by oscillometry (TremoFlo C-100). X5 becomes more negative with narrowing of small airways and increased airways stiffness.30 Other factors assessed by oscillometry included reactance area (AX), the difference between resistance at 5 and 19 Hz (R5-19), and resonance frequency (Fres), and respiratory system resistance at 5 Hz (R5).31 Specifically, X5 reflects elastance of the lung and is mostly determined by functionally communicating peripheral lung volume; AX is a measurement of ventilatory heterogeneity; R5-19 reflects mechanical heterogeneity due to uneven obstruction in the small airways; Fres increases with airways obstruction and indicates pulmonary function abnormalities; and R5 reflects narrowing in both large and small airways.31,32
Fluid Volumes
Thoracic and leg fluid volumes (TFV and LFV, respectively) were measured continuously by bioelectrical impedance (Biopac Systems), as previously described.2,3
Polysomnography
All participants underwent overnight polysomnography (PSG). PSG was performed using standard techniques and scoring criteria.33 Nasal airflow was monitored by a nasal pressure cannula. Thoraco-abdominal motion was monitored by respiratory inductance plethysmography and arterial oxyhemoglobin saturation (SaO2) was monitored by oximetry. Obstructive apneas were defined as a >90% reduction of tidal volume for ≥ 10s with out-of-phase thoraco-abdominal motion and obstructive hypopneas were defined as a 30–90% reduction in tidal volume from baseline for ≥ 10s with out-of-phase thoraco-abdominal motion or airflow limitation on nasal pressure. Apneas were classified as central in the absence of thoraco-abdominal motion, and hypopneas were classified as central in the presence of in-phase thoraco-abdominal motion and without airflow limitation on nasal pressure. The AHI was calculated as the number of apneas and hypopneas per hour of sleep. As another index of OSA severity, we took into account differences in duration of apneas and hypopneas, in addition to their frequency, by calculating total apnea–hypopnea time (mean duration of apneas and hypopneas in minutes × total number of apneas and hypopneas). Total sleep time (TST), sleep efficiency % (sleep time /TST×100%), rapid eye movement (REM) sleep % (REM time /TST×100%), and arousal index (total number of arousals/number of hours of sleep), were extracted from the sleep report. Participants were divided into a non-OSA group (AHI<10) and an OSA group (AHI≥10).
Lung Function
Standardized spirometry (Vmax Encore 229) was performed in the seated position in accordance with American Thoracic Society/European Respiratory Society guidelines.34 Forced vital capacity (FVC), FEV1, and FEV1/FVC were measured.
Protocol
Participants visited the sleep laboratory for one overnight sleep study. Participants’ current asthma medications were not withheld. After being instrumented for PSG, participants first performed spirometry while seated and then moved to the supine position for sleep. Before and after sleep, oscillometry was performed while remaining supine. During sleep, fluid volumes were measured continuously.
Statistical Analyses
Data are reported as means ± standard deviation (SD) unless indicated otherwise. Differences in baseline measures between the non-OSA and OSA groups were assessed with an unpaired t-test. Chi square test was used in assessing sex differences between the groups. Within-group changes in respiratory impedance and fluid volumes were compared with a paired t-test or Wilcoxon signed-rank test. Between-group changes in the measures were compared using analysis of covariance (ANCOVA), adjusted for age, BMI and sex. Statistical significance was accepted at p ≤ 0.05 (SAS 7.1, SAS Institute, Cary, USA).
Results
Characteristics of Participants
Nineteen individuals with asthma consented to participate. There were no significant differences between the OSA and non-OSA group in lengths of the leg and thorax. However, compared to the non-OSA group, the OSA group was significantly older with a higher BMI (Table 1).
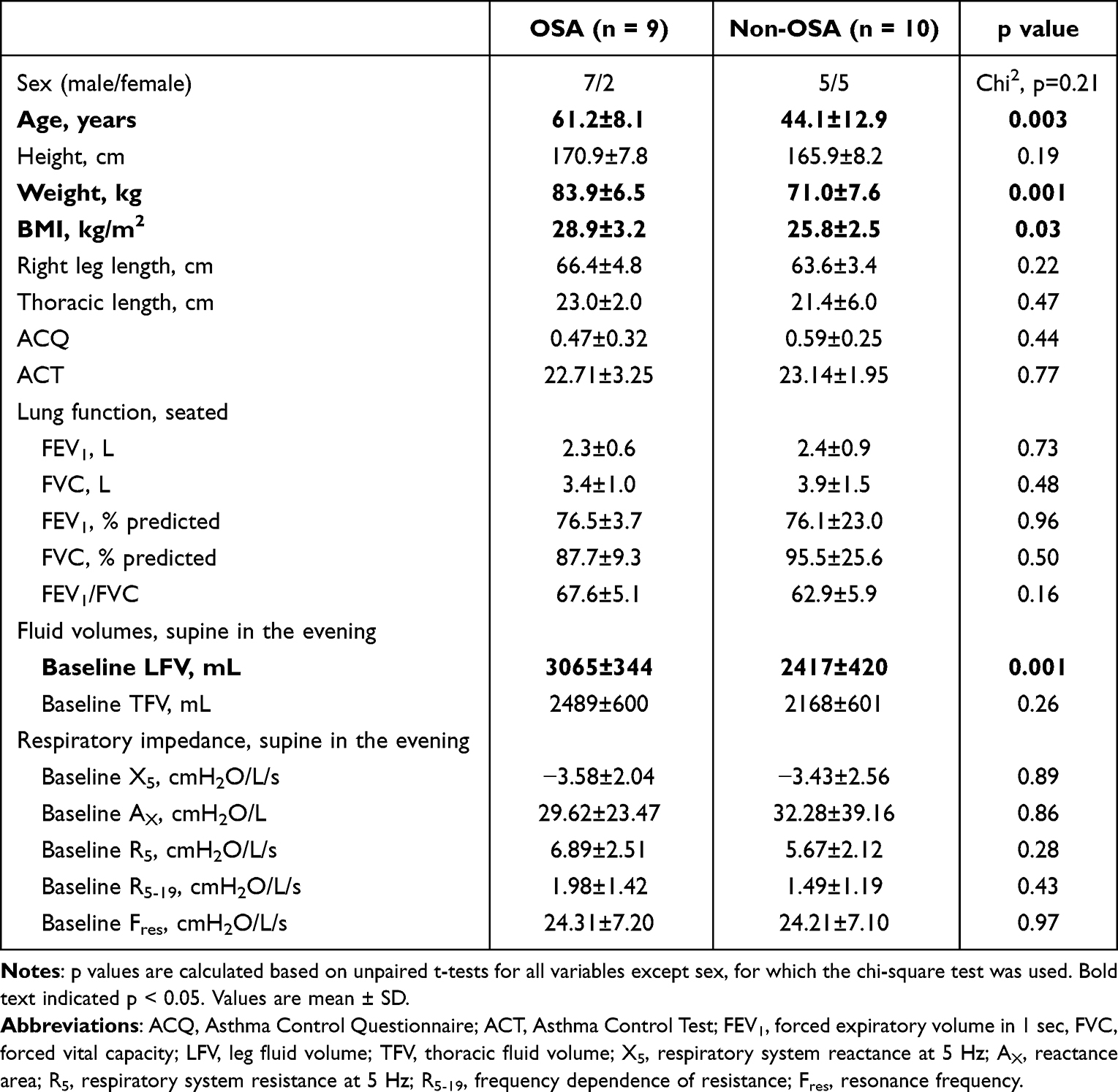 |
Table 1 Participant Demographics and Lung Function |
Pulmonary Function
There was no significant difference in ACQ and ACT scores between the two groups. Furthermore, there were no significant differences between the two groups in FEV1, FVC, FEV1% predicted, and FEV1/FVC % predicted values. Taken together, these data suggest that baseline asthma control was similar in the two groups. (Table 1).
Sleep Characteristics
PSG data are summarized in Table 2. By definition, the OSA group had a higher AHI than the non-OSA group (p = 0.001). Both the OSA and non-OSA groups had similar sleep efficiency, and percentage of rapid-eye-movement (REM) sleep. However, the OSA group had less total sleep time (TST, p = 0.052, Table 2), higher oxygen desaturation index (p < 0.001, Table 2) and total apnea-hypopnea time (p = 0.01, Table 2). There were no significant differences between the two groups in arousal index.
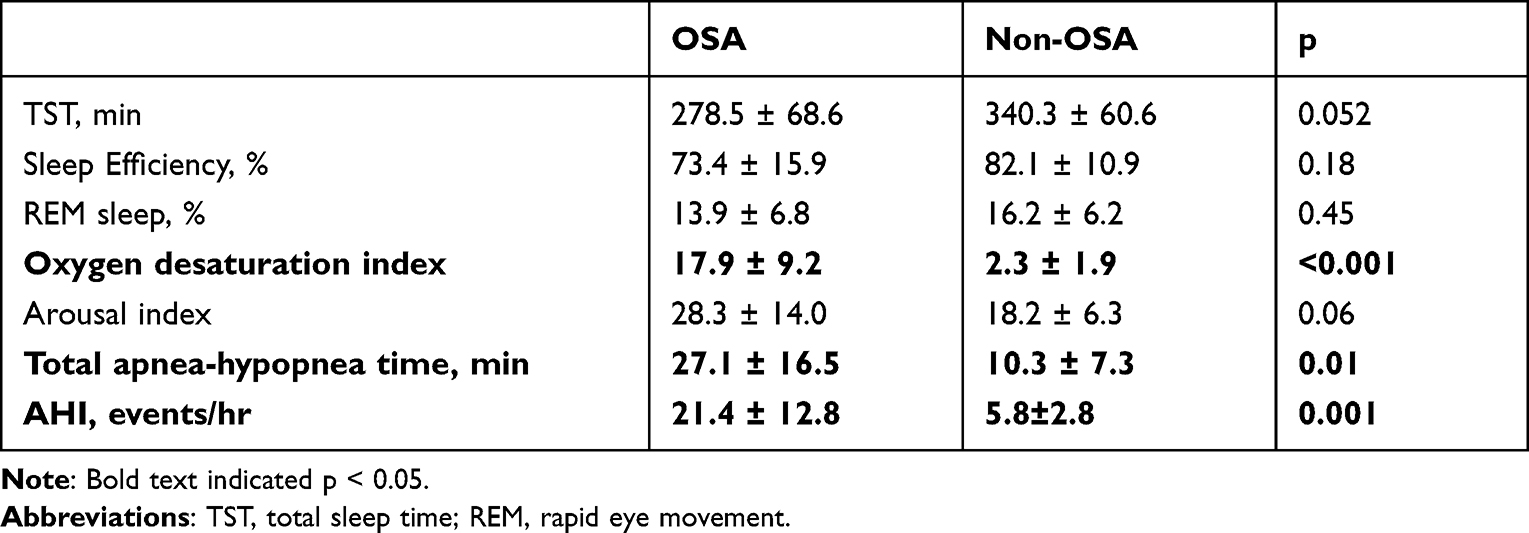 |
Table 2 Sleep Characteristics |
Fluid Volumes
At baseline before sleep, the LFV was significantly larger in the OSA group compared to the non-OSA group. However, baseline TFV was similar in the two groups (Table 1). LFV decreased significantly overnight in both the OSA and non-OSA group (p < 0.001 for both groups, Figure 1A), but the decrease was not different between the two groups (p = 0.17, Figure 1A). Both the OSA and non-OSA groups had significant overnight increases in TFV (p < 0.001 and p = 0.02, respectively, Figure 1B), but the increase was greater in the OSA group (p = 0.006, Figure 1B).
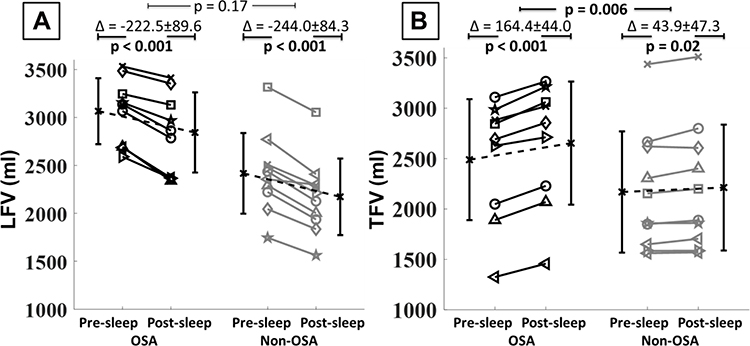 |
Figure 1 Changes in leg fluid volumes (ΔLFV) and thoracic fluid volumes (ΔTFV) in the OSA group (black lines) and non-OSA group (grey lines) ((A and B), respectively) from pre-sleep to post-sleep measurements. Each line represents an individual participant. P values for comparisons between groups are based on analysis of covariance, adjusted for age, BMI and sex. Bars on either side of data lines represent group mean value with SD. |
Oscillometry
Baseline X5, AX, R5, R5-19, and Fres were similar between the two groups (Table 1). A significant overnight decrease in X5 was seen in the OSA group (p = 0.003, Figure 2A, left), while in the non-OSA group, it increased significantly (p = 0.03, Figure 2A, right). The overnight decrease in X5 in the OSA group was greater than in the non-OSA group (p = 0.02, Figure 2A). In the non-OSA group, there was no significant overnight change in AX (Figure 2B), R5-19 (Figure 2C), and Fres (Figure 2D). In contrast, the OSA group experienced significant overnight increases in AX (p = 0.004, Figure 2B), R5-19 (p = 0.002, Figure 2C), and Fres (p = 0.05, Figure 2D) that were significantly greater than in the non-OSA group (p = 0.04, Figure 2B, p = 0.04, Figure 2C, and p = 0.04, Figure 2D, respectively). No significant overnight change in R5 was seen in either the OSA or non-OSA groups (p = 0.13 and p = 0.32, respectively, Figure 2E) and there was no significant differences between the two groups (p = 0.82, Figure 2E).
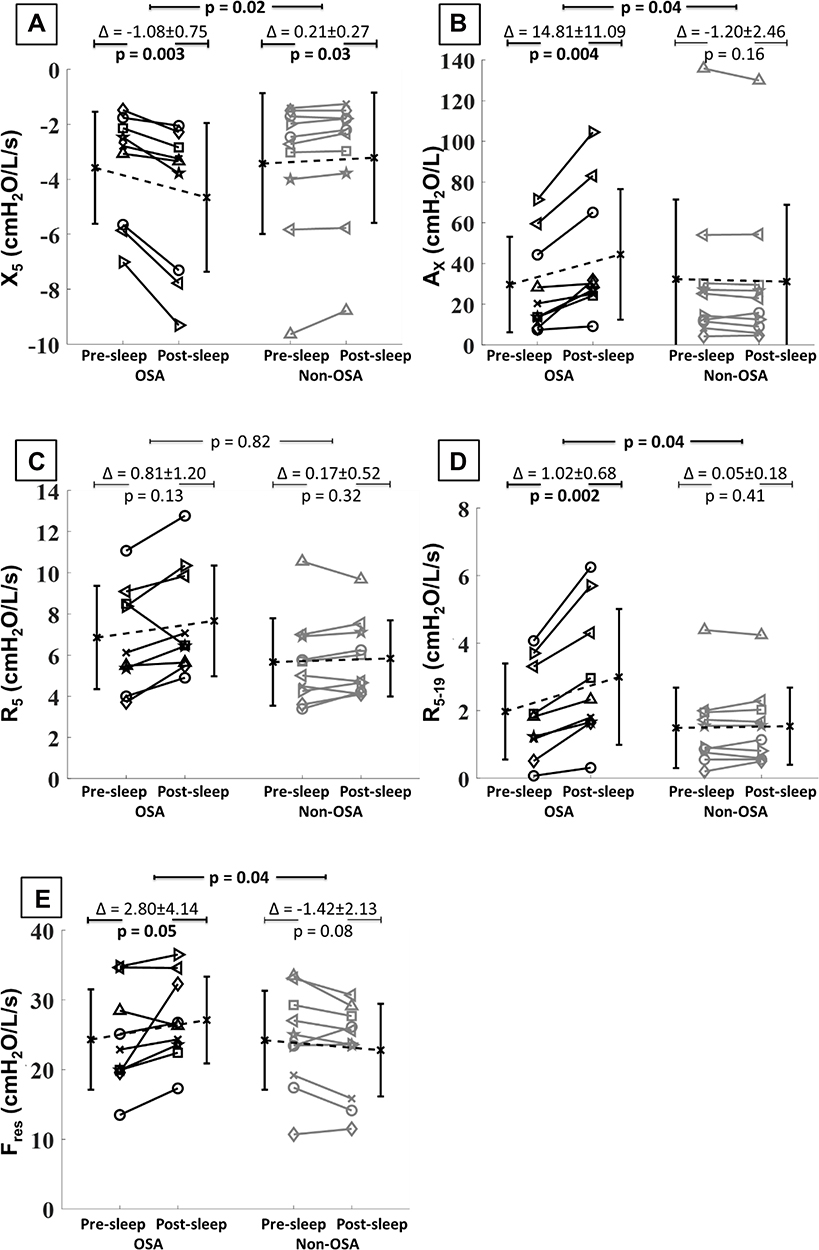 |
Figure 2 Changes in respiratory system reactance at 5 Hz (X5), reactance area (AX), total respiratory system resistance at 5 Hz (R5), frequency dependence of resistance (R5-19), and resonant frequency (Fres) in the OSA group (black lines) and non-OSA group (grey lines) (A–E, respectively) from pre-sleep to post-sleep measurements. Each line represents an individual participant. P values for comparisons between groups are based on analysis of covariance, adjusted for age, BMI and sex. Bars on either side of data lines represent group mean value with SD. More negative X5 indicates greater small airways resistance. |
Discussion
In this study, we observed two novel and important findings. First, patients with asthma and co-existing OSA had significantly greater overnight fluid accumulation in the thorax compared to those with asthma and without OSA. Second, compared to the non-OSA group, the OSA group experienced significantly greater overnight narrowing of the small airways as indicated by a significant reduction in X5 and increases in AX, R5-19, and Fres. Taken together our findings provide insights into a potential pathophysiological link between OSA and asthma. Specifically, they support the concept that in patients with asthma, co-existing OSA can draw fluid into the thorax, likely due to generation of exaggerated negative pleural pressure during obstructive events. If some of this increase in thoracic fluid accumulated around small airways, it could narrow them, and increase their airflow resistance and ventilatory heterogeneity. Such effects imply that, when present in patients with asthma, OSA could contribute to small airways narrowing and nocturnal asthma worsening due to rostral fluid shift.
The greater increase in TFV in the OSA group than in the non-OSA group is consistent with our previous finding, which showed simulation of the exaggerated negative pleural pressure generated during obstructive apneas by performing Mueller maneuvers increased TFV by approximately 50 mL. This was sufficient to induce small airways narrowing in patients with asthma.25 Although we did not measure pleural pressure in this study, it is likely that this was the major factor drawing fluid into the thorax among those with OSA. Interestingly, the overnight increase in TFV in the OSA group was more than three times that observed in response to Mueller maneuvers mentioned above,23,25 and therefore was probably a contributor to the overnight small airways narrowing observed in the OSA group. The source of the fluid drawn into the thorax of participants with OSA, however, remains uncertain. Fluid shift out of the legs was similar between the two groups, suggesting overnight change in leg fluid volume was a result of the change in gravitational direction and the resulting redistribution of fluid out of the legs. Therefore, the extra fluid drawn into the thorax was not likely a result of gravitational fluid shifts, but possibly a direct effect of the obstructive events on the lower intrathoracic pressure and consequently on the splanchnic circulation and/or the superior vena cava.
The increase in small airways narrowing overnight was greater among participants with asthma and co-existing OSA than in those without OSA, despite similar baseline X5, AX, R5, R5-19, and Fres before sleep. If some of the overnight increase in TFV accumulated around already narrowed small airways, this could induce further narrowing as we observed. Specifically, the greater overnight reduction in X5 and increases in AX, R5-19 and Fres indicate a greater degree of overnight small airways narrowing and ventilator heterogeneity in patients with OSA than among those without OSA. All four variables measure somewhat different aspects of respiratory system mechanics, and therefore provide a more comprehensive understanding of the effects of OSA and overnight changes in thoracic fluid volume on small airways function than any one variable alone. Our findings are in keeping with a recent study, that in children hospitalized with acute asthma exacerbations, generation of highly negative inspiratory pleural pressure was accompanied by an increase in extravascular lung water and associated with worse respiratory clinical outcomes.35
Neither group experienced any significant change in R5. R5 reflects the resistance of the entire respiratory system including both small and large airways (≥ 2 mm in diameter), but is dominated by the latter.8 This observation suggests that large airways were either not affected or were minimally affected by the overnight increase in TFV in those with OSA. It is likely that a larger increase in TFV would be needed to cause narrowing of the large airways.
Previous studies have shown that rostral fluid shift into the neck, narrows the pharyngeal airway and increases its airflow resistance, thereby contributing to the pathogenesis of OSA.36,37 Similarly, fluid shift from the legs into the thorax induced by application of lower body positive pressure or Mueller maneuvers increases both TFV and the degree of small airways narrowing in patients with asthma.23–25 In addition, as demonstrated in the present study, patients with asthma and OSA had a greater increase in TFV and greater narrowing of small airways overnight than asthma patients without OSA. This observation suggests a unifying link among overnight fluid shifts, OSA and asthma such that while rostral fluid shift into the neck predisposes to OSA, fluid shift into the thorax induced by OSA in people with asthma may worsen asthma at night by narrowing the small airways and increasing airways resistance.
OSA is becoming recognized as a modifiable risk factor for difficult to control asthma, and more specifically, nocturnal asthma.9,11,12 In addition, in patients with asthma, treating co-existing OSA with continuous positive airway pressure (CPAP), which would eliminate apnea-associated swings in negative pleural pressure, improves symptoms of asthma and quality of life.5,38–40 However, current asthma management guidelines do not include OSA as a factor that could worsen asthma and whose treatment could improve it, likely because potential mechanisms linking the two diseases remain unclear. The importance of our findings, therefore, is that they provide proof-of–principle that OSA can cause an increase in TFV overnight, most likely due to generation of exaggerated negative pleural pressure, and that this is associated with narrowing of the small airways in individuals with asthma, probably by increasing extravascular lung water and airway edema.
The present study has some limitations. Firstly, compared to the non-OSA group, the OSA group was older and had higher BMI, which are also risk factors for OSA. However, we adjusted for these differences statistically using ANCOVA. It may also show that in asthma, older individuals or those with higher BMI are at higher risk due to overnight fluid accumulation in the thorax;24 this could be investigated in future studies. Secondly, pleural pressure of participants was not measured during the sleep, so we could not quantify the degree of the negative pressure generated during obstructive events. However, it is likely that greater overnight increases in TFV and small airways narrowing in patients with asthma who have OSA than in those who do not could also be attributed to the exaggerated negative inspiratory pleural pressure during obstructive events. Thirdly, the sample size of 19 was rather small. However, since the difference between the two groups in primary outcome (X5) was significant, this sample size was sufficient to detect this difference and avoid a type 2 error. Lastly, although we did not measure clinical outcomes, our findings have potential clinical implications. They raise the issue of whether patients whose asthma is difficult to control or who have nocturnal symptoms should be screened or diagnose for OSA, and if present, treated in an attempt to better control asthma and prevent exacerbations. More efforts could be done in this population to enhance adherence to CPAP treatment, or alternative treatments such as exercise or reducing overall body fluid with diet.
In conclusion, the present study provides strong evidence that in patients with asthma, OSA induced fluid accumulation in the thorax that, in turn, provoked small airways narrowing, a reduction in functionally communicating peripheral airspaces, and an increase in ventilatory heterogeneity overnight. These observations support a mechanism by which OSA could worsen asthma and could help to explain the high prevalence of nocturnal symptoms in individuals with asthma and OSA. Randomized trials will be needed to determine whether management of co-existing OSA in patients with asthma will reduce overnight thoracic fluid accumulation, and improve respiratory mechanics and symptoms of asthma. Our findings also raise the possibility that other means of reducing nocturnal thoracic fluid accumulation in patients with asthma and co-existing OSA such as exercise,41 wearing compression stockings during the day,42 taking diuretics,43 or raising head would reduce overnight increases in small airways narrowing and nocturnal asthma symptoms.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Ontario Lung Association and the Canadian Respiratory Research Network. XC was supported by a scholarship from Ontario Graduate Scholarship (OGS) program from Province of Ontario and the University of Toronto, and the Asthma Canada-Canadian Allergy, Asthma and Immunology Foundation Graduate Student Research Award-Bastable-Potts from Asthma Canada. TDB was supported by the Godfrey S. Pettit Chair in Respiratory Medicine.
Disclosure
The authors report no conflicts of interest for this work. The abstract of this paper was presented at the European Respiratory Society Conference as a conference talk with interim findings. The presentation’s abstract was published in “ERS International Congress Abstract” in European Respiratory Journal: https://erj.ersjournals.com/content/58/suppl_65/OA3013.26
References
1. Ioachimescu OC, Teodorescu M. Integrating the overlap of obstructive lung disease and obstructive sleep apnea: OLDOSA syndrome. Respirology. 2013;18:421–431.
2. Owens RL, Macrea MM, Teodorescu M. The overlaps of asthma or COPD with OSA: a focused review. Respirology. 2017;22(6):1073–1083.
3. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased Prevalence of Sleep-Disordered Breathing in Adults. Am J Epidemiol. 2013;1:243.
4. Dempsey JA, Veasey SC, Morgan BJ, O’Donnell CP. Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47–112.
5. Mattiuzzi C, Lippi G. Worldwide asthma epidemiology: insights from the Global Health Data Exchange database. Int Forum Allergy Rhinol. 2020;10(1):75–80.
6. Rehman A, Amin F, Sadeeqa S. Prevalence of asthma and its management: a review. J Pak Med Assoc. 2018;68(12):1823–1827.
7. Brown RH. Groundhog day: airway narrowing, deep inspirations, and asthma. Am J Respir Crit Care Med. 2014;190(8):847–848.
8. Macklem PT, Mead J. Resistance of central and peripheral airways measured by a retrograde catheter. J Appl Physiol. 1967;22(3):395–401.
9. Prasad B, Nyenhuis SM, Imayama I, Siddiqi A, Teodorescu M. Asthma and Obstructive Sleep Apnea Overlap: what Has the Evidence Taught Us? Am J Respir Crit Care Med. 2020;201(11):1345–1357.
10. Kong D-L, Qin Z, Shen H, Jin H-Y, Wang W, Wang Z-F. Association of Obstructive Sleep Apnea with Asthma: a Meta-Analysis. Sci Rep. 2017;7(1):4088.
11. Davies SE, Bishopp A, Wharton S, Turner AM, Mansur AH. The association between asthma and obstructive sleep apnea (OSA): a systematic review. J Asthma. 2019;56(2):118–129.
12. Senaratna CV, Walters EH, Hamilton G, et al. Nocturnal symptoms perceived as asthma are associated with obstructive sleep apnoea risk, but not bronchial hyper-reactivity. Respirology. 2019;24(12):1176–1182.
13. Özden Mat D, Firat S, Aksu K, Aksu F, Duyar SŞ. Obstructive sleep apnea is a determinant of asthma control independent of smoking, reflux, and rhinitis. Allergy Asthma Proce. 2021;42(1):e25–e9.
14. Wang TY, Lo YL, Lin SM, et al. Obstructive sleep apnoea accelerates FEV1 decline in asthmatic patients. BMC Pulm Med. 2017;17(1):55.
15. Watson NF. Health Care Savings: the Economic Value of Diagnostic and Therapeutic Care for Obstructive Sleep Apnea. J Clin Sleep Med. 2016;12(8):1075–1077.
16. Frost & Sullivan. Hidden health crisis costing America billions. Underdiagnosing and undertreating obstructive sleep apnea draining healthcare system Darien, IL2016; 2016; Available from: http://www.aasmnet.org/sleep-apnea-economic-impact.aspx.
17. Sato S, Saito J, Fukuhara A, et al. Association Between Sleep Characteristics and Asthma Control in Middle-Aged and Older Adults: a Prospective Cohort Study. J Asthma Allergy. 2021;14:325–334.
18. Kraft M, Djukanovic R, Wilson S, Holgate ST, Martin RJ. Alveolar tissue inflammation in asthma. Am J Respir Crit Care Med. 1996;154(5):1505–1510.
19. Prasad B, Nyenhuis SM, Weaver TE. Obstructive sleep apnea and asthma: associations and treatment implications. Sleep Med Rev. 2014;18(2):165–171.
20. Al-Alwan A, Bates JHT, Chapman DG, et al. The nonallergic asthma of obesity. Am j Respir Critical Care Med. 2014;189(12):1494–1502.
21. Eastwood PR, Malhotra A, Palmer LJ, et al. Obstructive Sleep Apnoea: from pathogenesis to treatment: current controversies and future directions. Respirology. 2010;15(4):587–595.
22. Ballard RD. Sleep, respiratory physiology, and nocturnal asthma. Chronobiol Int. 1999;16(5):565–580.
23. Bhatawadekar SA, Inman MD, Fredberg JJ, et al. Contribution of rostral fluid shift to intrathoracic airway narrowing in asthma. J Appl Physiol. 2017;122(4):809–816.
24. Bhatawadekar SA, Keller G, Francisco CO, et al. Reduced Baseline Airway Caliber Relates to Larger Airway Sensitivity to Rostral Fluid Shift in Asthma. Front Physiol. 2017;8:1012.
25. Cao X, Bradley TD, Bhatawadekar SA, et al. Effect of Simulated Obstructive Apnea on Thoracic Fluid Volume and Airway Narrowing in Asthma. Am J Respir Crit Care Med. 2021;203(7):908–910.
26. Cao X, Francisco CO, Montazeri Ghahjaverestan N, et al. Association of obstructive sleep apnea with thoracic fluid volume and small airways narrowing in asthma during sleep. Eur Respir Soc Int Congress. 2021;1:56.
27. Bateman ED, Hurd SS, Barnes PJ, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31(1):143–178.
28. Thomas M, Kay S, Pike J, et al. The Asthma Control Test (ACT) as a predictor of GINA guideline-defined asthma control: analysis of a multinational cross-sectional survey. Prim Care Respir J. 2009;18(1):41–49.
29. Juniper EF, Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14(4):902.
30. Bates JHT, Irvin CG, Farré R, Hantos Z. Oscillation Mechanics of the Respiratory System. Compr Physiol. 2011;1:1233–1272.
31. Eddy RL, Westcott A, Maksym GN, Parraga G, Dandurand RJ. Oscillometry and pulmonary magnetic resonance imaging in asthma and COPD. Physiol Rep. 2019;7(1):e13955–e.
32. Young HM, Guo F, Eddy RL, Maksym G, Parraga G. Oscillometry and pulmonary MRI measurements of ventilation heterogeneity in obstructive lung disease: relationship to quality of life and disease control. J Appl Physiol. 2018;125(1):73–85.
33. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications. 2020.
34. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–338.
35. Kantor DB, Hirshberg EL, McDonald MC, et al. Fluid Balance Is Associated with Clinical Outcomes and Extravascular Lung Water in Children with Acute Asthma Exacerbation. Am J Respir Crit Care Med. 2018;197(9):1128–1135.
36. Redolfi S, Yumino D, Ruttanaumpawan P, et al. Relationship between overnight rostral fluid shift and obstructive sleep apnea in nonobese men. Am J Respir Crit Care Med. 2009;179:241–246.
37. Chiu K-L, Ryan CM, Shiota S, et al. Fluid Shift by Lower Body Positive Pressure Increases Pharyngeal Resistance in Healthy Subjects. Am J Respir Crit Care Med. 2006;174(12):1378–1383.
38. Busk M, Busk N, Puntenney P, et al. Use of continuous positive airway pressure reduces airway reactivity in adults with asthma. Eur Respir J. 2013;41(2):317.
39. Davies SE, Bishopp A, Wharton S, Turner AM, Mansur AH. Does Continuous Positive Airway Pressure (CPAP) treatment of obstructive sleep apnoea (OSA) improve asthma-related clinical outcomes in patients with co-existing conditions?- A systematic review. Respir Med. 2018;143:18–30.
40. Serrano-Pariente J, Plaza V, Soriano JB, et al. Asthma outcomes improve with continuous positive airway pressure for obstructive sleep apnea. Allergy. 2017;72(5):802–812.
41. Mendelson M, Lyons OD, Yadollahi A, Inami T, Oh P, Bradley TD. Effects of exercise training on sleep apnoea in patients with coronary artery disease: a randomised trial. Eur Respir J. 2016;48(1):142.
42. White LH, Lyons OD, Yadollahi A, Ryan CM, Bradley TD. Effect of below-the-knee compression stockings on severity of obstructive sleep apnea. Sleep Med. 2015;16(2):258–264.
43. Kasai T, Bradley TD, Friedman O, Logan AG. Effect of intensified diuretic therapy on overnight rostral fluid shift and obstructive sleep apnoea in patients with uncontrolled hypertension. J Hypertens. 2014;32(3):443.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.