Back to Journals » Clinical Ophthalmology » Volume 20
Association of Gonioscopy Scores with Changes in Intraocular Pressure after Phacoemulsification in a Predominantly Vietnamese Population: A Retrospective Study
Authors Nguyen KC, Chansangpetch S, Truong D, Tran BG, Nguyen L, Nguyen N ![]() , Iwach A, Lin SC
, Iwach A, Lin SC ![]()
Received 31 January 2026
Accepted for publication 12 May 2026
Published 18 May 2026 Volume 2026:20 600343
DOI https://doi.org/10.2147/OPTH.S600343
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Kelly C Nguyen,1 Sunee Chansangpetch,2– 4 Dzuy Truong,5 Brittney G Tran,6 Lauren Nguyen,6 Ngoc Nguyen,7 Andrew Iwach,8,9 Shan C Lin7,8
1University of California, San Francisco School of Medicine, San Francisco, CA, USA; 2Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Center of Excellence in Glaucoma, Chulalongkorn University, Bangkok, Thailand; 4Department of Ophthalmology, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand; 5Saint Louis University School of Medicine, Saint Louis, MO, USA; 6University of California, Davis, CA, USA; 7Glaucoma Research and Education Group, San Francisco, CA, USA; 8Glaucoma Center of San Francisco, San Francisco, CA, USA; 9Department of Ophthalmology, University of California, San Francisco, CA, USA
Correspondence: Shan C Lin, Glaucoma Center of San Francisco, 55 Stevenson St # 2-4, San Francisco, CA, 94105, USA, Email [email protected]
Purpose: To evaluate the effectiveness of cataract extraction in reducing intraocular pressure (IOP) between high gonioscore and low gonioscore groups in a predominantly Vietnamese population.
Patients and Methods: In this retrospective cohort study, we reviewed the records of patients who had cataract surgeries between Aug 2016-Sep 2019 at an ophthalmology clinic with a high volume of Vietnamese patients. The relationship between postoperative IOP and gonioscopy score (low [≤ 10] and high gonioscore [> 10]) was evaluated.
Results: There was a significant difference between the low and high gonioscore groups by age (low, 73.26 ± 8.34, high, 67.74 ± 9.10; p < 0.001), eyes with laser peripheral iridotomy (LPI) (low, n = 64 (42.1%), high, n = 5 (6.8%), p < 0.001), and anterior chamber depth (low, 2.89 ± 0.36, high, 3.18 ± 0.34; p < 0.001). The majority of eyes were from Vietnamese patients (n = 193, 85.4%). In an unadjusted model, there was a significant difference in absolute IOP at 6 months between the high and low gonioscore groups (low, 12.57 ± 2.85, high, 13.64 ± 3.20; p = 0.034). After adjustment, both gonioscore groups showed significant IOP reduction at 6-month follow-up, with higher IOP reduction in the low gonioscore group (p = 0.034). In the group-time interaction, there was a significant difference between low and high gonioscore groups at 6 months (Model 1, p = 0.033, Model 2, p = 0.044).
Conclusion: We found a significant difference in IOP reduction at 6 months after cataract surgery between low and high gonioscore groups within a predominantly Vietnamese cohort. Given that IOP reduction can be achieved with cataract surgery to help minimize vision loss in glaucoma, gonioscopy can be a useful measure to predict post-surgical IOP in this population.
Keywords: cataract extraction, gonioscopy score, anterior chamber depth
Introduction
Glaucoma is a progressive optic neuropathy that is characterized by irreversible visual field loss.1 Elevated intraocular pressure (IOP) due to impaired aqueous humor outflow is the single most important modifiable risk factor.1 Therapies that lower IOP remain the primary means of preventing further vision loss.1 Glaucoma can be clinically classified by the configuration of the anterior chamber angle (ACA). In open angle glaucoma (OAG), the angle is anatomically open, but outflow through the trabecular meshwork is impaired.2 By contrast, in narrow angle glaucoma (NAG), the peripheral iris apposes or occludes the trabecular meshwork.2
Cataract refers to the opacification of the lens, leading to progressive visual impairment and, if untreated, potential blindness.3 It is the most common cause of reversible blindness worldwide and a major cause of visual disability in aging populations.2 The only definitive treatment is surgical removal of the opacified lens, typically replaced with a clear intraocular lens implant.4 In the case of NAG, cataract extraction removes a relatively bulky cataract and deepens the ACA, which can help alleviate the physical blockage of aqueous humor outflow.5 Several studies have shown that cataract extraction may play a role in concurrently treating cataracts and NAG.5–8 Moreover, prior literature has supported the use of preoperative predictors for IOP change after cataract surgery.9,10 For instance, studies have found an inverse relationship between IOP reduction and anterior chamber depth (ACD).9,10 Perez et al found that gonioscopy score was a more significant predictor compared to preoperative ACD for IOP reduction after cataract surgery, thus supporting its clinical relevance.11 Though the use of anterior segment optical coherence tomography (AS-OCT) has provided insight into clinical outcomes after phacoemulsification, few studies have explored the association between gonioscopy scores, iridocorneal angle widening, and IOP reduction after cataract surgery. Since gonioscopy is a more readily available test, it may have more practical relevance to the busy clinician.
This study aims to evaluate the effectiveness of cataract extraction in reducing IOP among predominantly Vietnamese patients, a population with a relatively high prevalence of narrow angle eyes. In particular, our comparison between high and low gonioscore groups examines whether IOP reduction after cataract surgery can be predicted using gonioscopy. We hypothesize that there will be a significant reduction in IOP after cataract surgery in both groups, with the low gonioscore group having a greater IOP reduction than that of the high gonioscore group. The Vietnamese population has been reported to exhibit a higher prevalence of primary angle closure glaucoma (PACG) and a narrower ACA compared with other ethnic groups, making it a particularly relevant cohort for assessing the IOP-lowering effect of lens extraction.12 However, no studies have investigated using gonioscopy as a clinically accessible predictor of cataract surgery outcomes in patients with narrow angles predominant in Southeast Asian populations. In particular, there is a paucity of data on surgical outcomes in the Vietnamese population. Clinically, these findings could support the use of lens extraction as an effective first-line or adjunctive therapy for narrow angle disease states in Vietnamese patients as well as reduce dependence on topical glaucoma medications following cataract extraction.
Methods
Data Collection
Patient charts were reviewed from the clinic of a single glaucoma specialist (N.N.) and included patients who had cataract surgeries between August 2016 and September 2019. Institutional review board approval was obtained from Advarra, Columbia, MD, and the study was conducted in accordance with the tenants of the Declaration of Helsinki. Informed consent was exempted by the IRB due to the retrospective study design, where subjects were not available to provide informed consent. The study subjects were selected from an existing clinic population, and patient confidentiality was maintained by following secure protocols for handling protected health information. Gonioscopy scores were obtained by taking the sum of the Shaffer gonioscopy grading in all four quadrants (0 to 16).11 High gonioscore was defined as a gonioscore of >10. Low gonioscore was defined as a gonioscore of ≤10 that indicates a narrower angle. The cut-off value of 10 used to categorize patients into high and low gonioscore groups was selected based off the sample’s median (10, IQR 8 to 12). Patients were excluded based on the following criteria: (1) had previous penetrating surgery or (2) had complications related to cataract surgery (eg, posterior capsular rupture and vitreous loss, primary or secondary glaucoma, or peripheral anterior synechiae). Additionally, none of the patients had a diagnosis of glaucoma or used glaucoma medications during the study time frame.
Preoperative and Postoperative Evaluation
Basic demographic characteristics were obtained from medical chart review. Preoperative data collection included slit lamp examination, visual acuity testing, gonioscopy, and IOP assessment. IOP and gonioscopy were measured using Goldmann applanation tonometry and Zeiss-style 4-mirror gonioscopy lens (model OPDSG; Ocular Instruments Inc., Bellevue, Washington), respectively. Angles were graded using the Shaffer method in all 4 quadrants (superior, nasal, temporal, and inferior). BCVA, cup-to-disc (C:D) ratio, gonioscopy, and IOP were recorded before surgery. Central corneal thickness (CCT) was obtained using optical coherence tomography (OCT) (Cirrus OCT, CarlZeiss, Meditec, Dublin, CA, USA) before surgery. Anterior chamber depth (ACD), axial length (AL) and keratometry (K) values were also obtained using an optical biometer (ARGOS®, Alcon Inc., Fort Worth, TX, USA) before surgery. When multiple measurements were recorded, the average was utilized. BCVA and gonioscopy were then recorded after surgery. IOP was recorded at day 1; week 1; and months 1, 3, and 6.
Patient and Public Involvement
Due to the retrospective design of the study, there was no direct involvement of patients or the public. However, aims of the study were created with the intent to better inform gonioscopy scores as a predictive aid for post-operative outcomes and lens extraction as first-line therapy for narrow angle disease.
Surgical Technique
All patients had monitored anesthesia care (MAC) and were given preservative-free 0.5% Xylocaine for local anesthesia. Viscoat (Alcon Laboratories, Fort Worth, TX) was injected into the anterior chamber after a paracentesis site was made and anesthetic was injected. A 2.4 mm keratome blade was used to create a temporal clear corneal incision. An anterior capsulorrhexis was performed. Hydrodissection and hydrodelineation were performed with balanced salt solution through a blunt cannula. The phacoemulsification tip and irrigation-aspiration tip were used to remove the nuclear material and residual cortical material, respectively. Viscoelastic was placed in the anterior chamber and the intact and clear capsular bag. The lens (Alcon SN60WF series) was inspected, irrigated with a balanced salt solution, loaded into the injector, inserted in the capsular bag and then rotated into position using the Sinskey hook. Residual viscoelastic was removed with the irrigation-aspiration tip. Subconjunctival injections of Ancef (cefazolin) and dexamethasone were given. Maxitrol (combination neomycin, polymyxin, and dexamethasone) ointment and timolol 0.5% drops were placed in the affected eye. For postoperative care, all patients were instructed to use 1% prednisone acetate and 0.3% nepafenac drops for 5 weeks following surgery as well as a fluroquinolone antibiotic drop for 2 weeks following surgery. Patients came in for follow-up appointments with the ophthalmologist at day 1, week 1, and months 1, 3, and 6.
Statistical Analysis
Baseline characteristics between the two study groups were compared using independent t tests for continuous variables and Chi-square or Fisher’s exact tests for categorical variables. Longitudinal changes in IOP were analyzed using a linear mixed-effects model with fixed effects for group, time, and their interaction (group × time), and a random intercept for each eye to account for within-subject correlation. The interaction term assessed whether the temporal pattern of IOP change differed between groups. A second model additionally included covariates that represented baseline characteristics showing significant differences between groups in the univariable analyses. Adjusted marginal means were estimated and plotted against time from the adjusted model. Statistical significance was defined as P < 0.05. Assuming a two-sided α of 0.05, 80% power, an allocation ratio of 2, and an effect size of Cohen’s d = 0.4, the required sample size was 149 and 75 participants in low and high gonioscore groups, respectively. All analyses were performed using Stata Software, version 16.0 (StataCorp, College Station, TX, USA).
Results
There were a total of 226 eyes from 200 patients included in the study, with 152 (67.2%) comprising the low gonioscore group and 74 (32.7%) comprising the high gonioscore group. Baseline characteristics are described in Table 1. There was a significant difference in age between low and high gonioscore groups (low, 73.26 ± 8.34; high, 67.74 ± 9.10; p < 0.001). There was a greater number of eyes with laser peripheral iridotomy (LPI) in the low gonioscore group compared to the high gonioscore group (low, n = 64 (42.1%), high, n = 5 (6.8%), p < 0.001). There was greater anterior chamber depth in the high gonioscore group compared to the low gonioscore group (high, 3.18 ± 0.34; low, 2.89 ± 0.36; p < 0.001). Although we did not find a significant difference across race/ethnicity between the two groups, the majority of eyes included in the study were from patients of Vietnamese descent (n = 193, 85.4%).
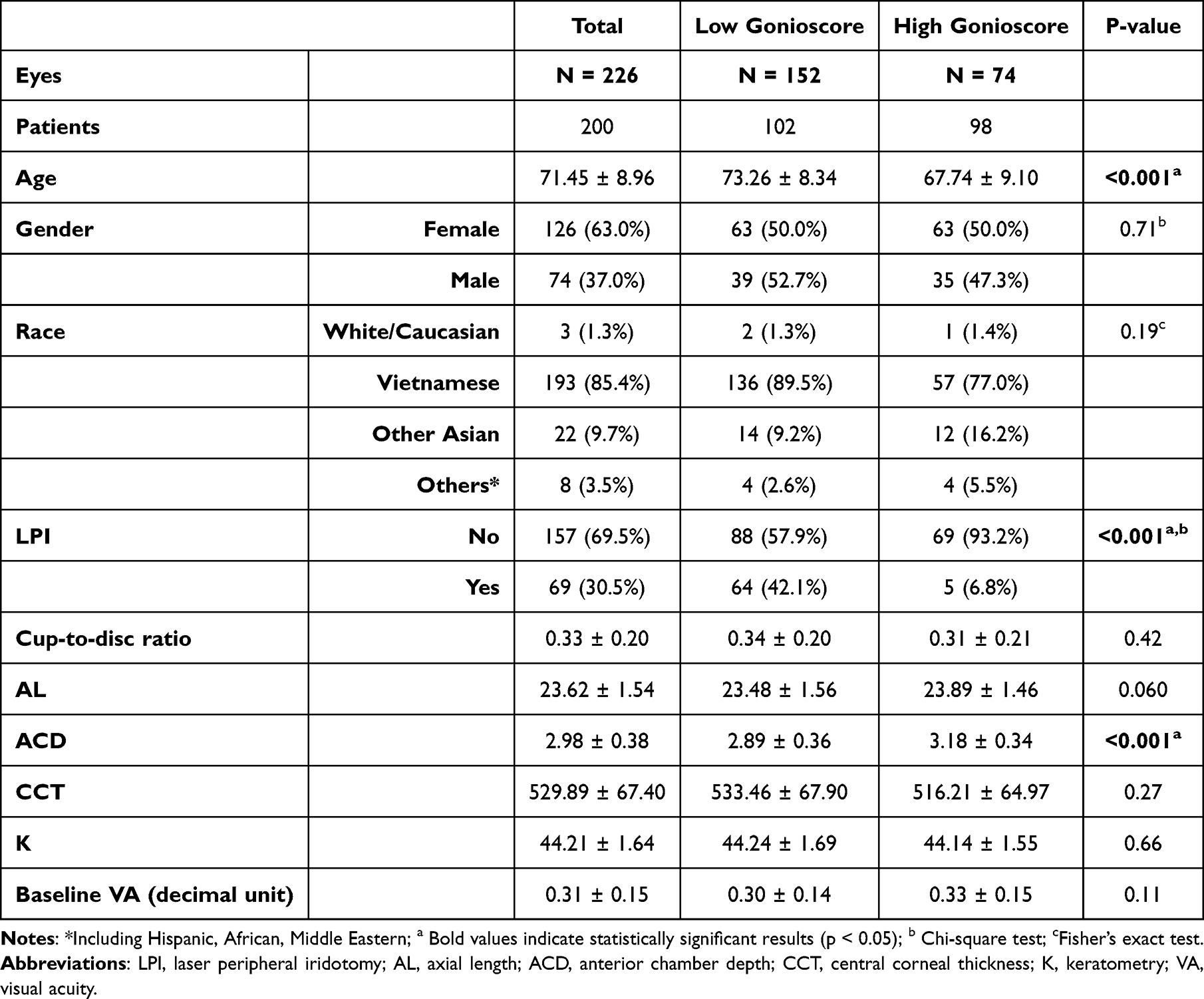 |
Table 1 Baseline Characteristics of the Study Population |
Table 2 shows the change in IOP over 6-month follow-up in an unadjusted model. At 6 months, there was a significant difference in absolute IOP between the high and low gonioscore groups (high, 13.64 ± 3.20, low, 12.57 ± 2.85, p = 0.034). No other significant differences were noted between the two groups at other time points. In a regression model adjusting for significant baseline characteristics, including age, anterior chamber depth, and presence of iridotomy between groups, low and high gonioscore groups showed significant IOP reduction over 6-months follow-up (p-value < 0.003) (Figure 1). In a subgroup analysis of eyes with LPI and without LPI in the low gonioscore group, there was no significant difference in the overall IOP change between eyes with and without LPI after adjusting for age and anterior chamber depth (Figure 2). With regard to group-time interaction, the LPI subgroup had additional lower IOP by 1.3 mmHg relative to eyes without LPI at 30 days. There were no significant differences at other time points.
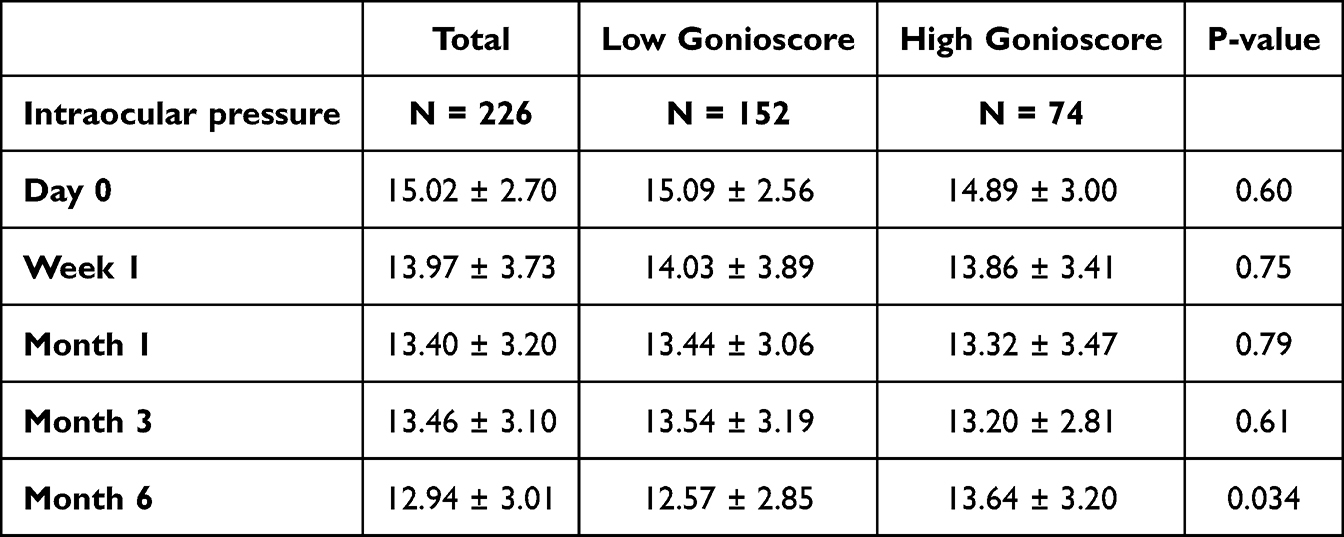 |
Table 2 Change in Intraocular Pressure Over 6 Months |
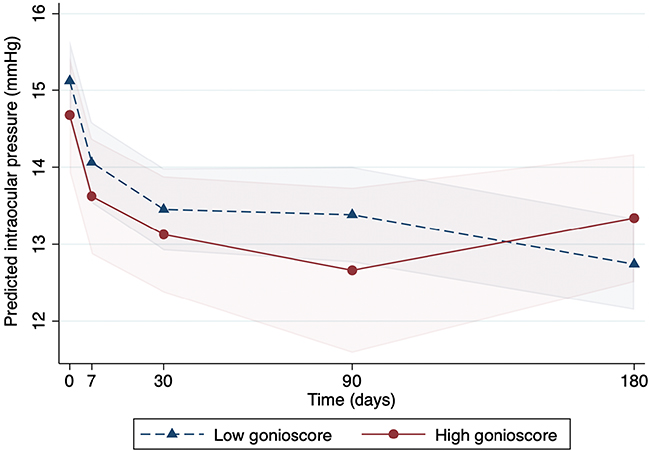 |
Figure 1 Predicted intraocular pressure over time, adjusted for age, anterior chamber depth, and presence of iridotomy using mixed-effects model with fixed effects for group, time, and their interaction. |
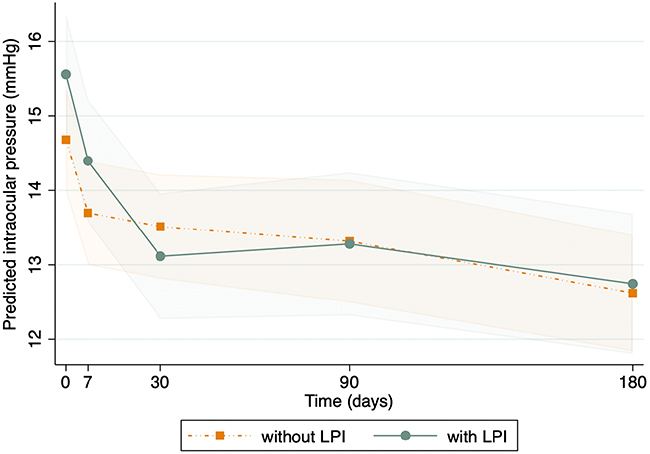 |
Figure 2 Predicted intraocular pressure with and without laser peripheral iridotomy, adjusted for age and anterior chamber depth. |
There was a statistically significant IOP reduction from baseline at all time points (all p < 0.003) (Table 3). In Table 3, Model 2 adjusted for age, anterior chamber depth, and presence of iridotomy between groups, while Model 1 had no adjustments. There was no significant difference between the two groups in terms of overall IOP change (Model 1, p = 0.65, Model 2, p = 0.34). However, in the group-time interaction, there was a significant difference between low and high gonioscore groups at 6 months (Model 1, p = 0.033, Model 2, p = 0.044). Additionally, at 6 months, the IOP of the low gonioscore group was lower by 1.1 mmHg relative to the high gonioscore group. There were no other significant differences in relation to group-time interactions between the groups at the other time points.
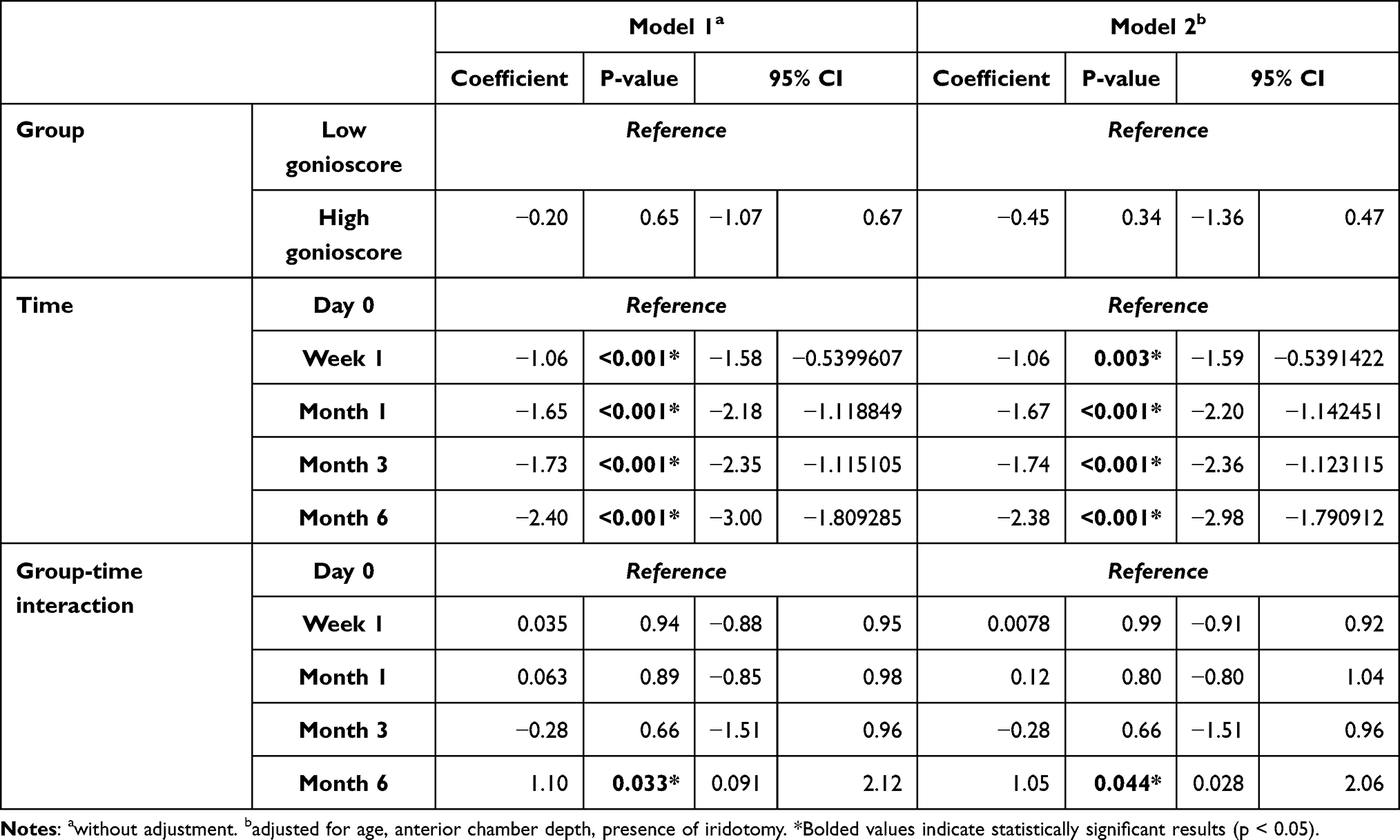 |
Table 3 Association Between Low Gonioscore and High Gonioscore Groups, Time, and Their Interaction on Intraocular Pressure Change |
Discussion
Overall, our study found that there was a significant difference between low and high gonioscore groups across age, LPI, and ACD. When adjusting for these variables, we saw a significant difference between low and high gonioscore groups at 6 months in relation to group-time interaction, with a higher IOP reduction seen in the low gonioscore group.
Existing literature has shown there is a high proportion of angle closure and mixed mechanism glaucoma among Vietnamese patients.13 Prior studies have supported that Vietnamese eyes have smaller angle and anterior chamber parameters compared to Chinese and White eyes.14 Several studies have explored mechanisms for angle closure in the Vietnamese population. Do et al found that 86.6% of primary angle closure suspect eyes had pupillary block and 31.3% had mixed pupillary block and plateau iris.15 Moreover, they also showed a higher proportion of pupillary block in Vietnamese eyes compared to Chinese eyes, which is consistent with previous studies that showed a higher iris curvature in Vietnamese eyes.14,15
Importantly, one study demonstrated that there is an inverse relationship between preoperative ACD and postoperative IOP reduction in non-glaucomatous eyes.9 Another study found that a shallower anterior chamber was associated with greater IOP reduction after surgery for eyes with PACG and cataract.16 Moreover, our study showed that there was a greater ACD in the high gonioscore group but lower IOP reduction at 6 months when compared to the low gonioscore group in the group-time interaction model. Altogether, these findings are consistent with previous literature that suggests a greater association between postoperative IOP reduction and Asian ethnicity compared to non-Asian ethnicity.11 Given a higher prevalence of angle closure disease in East Asia due to shallow ACD, greater lens thickness and shorter AL,16 further investigation of parameters to predict IOP reduction after cataract surgery is needed to inform disease management. Additionally, both groups had similar baseline IOPs, but the low gonioscore group reached a lower IOP at 6 months. This suggests that angle width may be an independent predictor of surgical success rather than baseline pressure alone. To our knowledge, this is the first study that explored the association between narrower angles using gonioscopy scores and IOP reduction after cataract surgery in a predominantly Vietnamese population.
Our study showed a significant difference between gonioscore groups in IOP reduction at 6 months when examining the interactions between group and time, which is consistent with studies that have found an association between gonioscopy score and IOP reduction at 6 months.11 One study assessed various formulas used to predict IOP change at 6 months post cataract surgery and found that preoperative IOP and gonioscopy score were most frequently associated.11 There may be possible explanations for these phenomena. Lower gonioscopy scores indicate narrower angles, which have been shown in prior studies to be associated with a greater IOP reduction after cataract surgery.11,17 Although the mechanism is not fully understood, one study hypothesized that cataract surgery widens the drainage angle and improves the aqueous outflow through the trabecular meshwork.18 Ultimately, this mechanism helps to understand greater IOP reduction in narrower angles. However, one study showed there is high variability in gonioscopy as a predictor for IOP reduction, thus it may not be appropriate as a standalone predictor for post-cataract surgery outcomes.11 For instance, prior studies have explored other preoperative markers that can predict IOP reduction after cataract surgery. One study found that higher preoperative and changes in iridotrabecular contact (ITC) index and area using anterior segment OCT (AS-OCT) were associated with greater postoperative IOP reduction in primary angle closure disease (PACD).19 Although gonioscopy is typically used as the standard for diagnosis of ITC in PACD, these studies have suggested that AS-OCT may provide more anatomical data of ACAs with higher accuracy and reproducibility. In addition, prior studies have shown that higher preoperative baseline IOP is associated with greater sustained IOP reduction after cataract surgery.20,21 Therefore, future studies can investigate the ability of various methods, using gonioscopy as the reference, to predict postoperative outcomes in the same patient sample.
Moreover, other mechanisms have contributed to the lowering of IOP after cataract surgery. One study found that phacoemulsification ultrasound activates the interleukin 1α/nuclear factor kappa B/endothelial leukocyte adhesion molecule 1 pathway in trabecular meshwork cells, which increases the expression of IL-1alpha leading to enhanced aqueous outflow and subsequent IOP reduction.22 Another possible mechanism is increased diameter and area of the Schlemm canal (SC) after cataract surgery, which has been shown to reduce IOP and sustain these changes for 6 months.23 Moreover, Zhao et al found that SC expansion following cataract surgery improves the SC valves and facilitates outflow leading to IOP reduction. That study also showed the ACD deepened and the ACA widened after surgery, which is consistent with prior studies.23 However, these changes had no association with those found in the SC after cataract surgery, so it remains unclear whether structural changes improving IOP are tied to the SC.
The study cohort included patients of predominantly Vietnamese heritage at a single ophthalmology clinic, so we may be unable to generalize findings to broader populations. Moreover, the study cohort was relatively small, so our findings may also not be generalizable to the larger Vietnamese population as a whole. The retrospective nature of the study may contribute to selection bias and missing or inconsistent reporting of data, thus not fully representative of the population. The study cohort was followed for 6 months, which may be a short follow-up period. However, prior studies have shown that the effect of IOP reduction remains relatively stable at 6 months compared to other time points, such as 1 year follow-up.5 Further investigation can determine whether the association between IOP reduction and gonioscopy scores (narrower angles) persists and would be clinically relevant for an extended time period. Although there was a significant difference between gonioscore groups in IOP reduction at 6 months, the magnitude was relatively small. Additionally, the mean IOP at baseline and 6 months for both groups was within the normal IOP range, which contributes to the relatively low IOP reduction. Future studies can investigate glaucoma patients with angle closure versus open angle using gonioscopy as a post-surgical predictor, which may yield more clinically relevant results. Additionally, given that few studies have used the sum of gonioscopy grading in all four quadrants as a clinical measure, using a cut off gonioscore of 10 based on the sample’s median can be expanded on in future studies to reinforce its clinical relevance. Moreover, the sum of the quadrants does not disclose the specific grading in each of the four quadrants. Therefore, this method does not indicate the total closure in specific quadrants, and whether this may have impacted the IOP reduction compared to the cumulative sum.
Conclusion
In our population of mainly Vietnamese patients, we found a significant difference in IOP reduction at 6 months after cataract surgery between low and high gonioscore groups. These findings support the efficacy of lens extraction as first-line or adjunctive therapy for narrow angle conditions prevalent in the Vietnamese population. These findings suggest the use of gonioscopy scores as a potential predictive aid for postoperative outcomes but future studies should investigate longitudinal follow up including in glaucoma patients undergoing cataract surgery.
Acknowledgments
There is no funding to disclose. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Disclosure
Shan C. Lin is a consultant for Santen, IRIDEX, Bausch & Lomb, and iSTAR and a speaker for Santen and Bausch & Lomb. Andrew G. Iwach is a consultant and advisor for Alcon Laboratories, Inc., public equity and stockholder for Eyenovia, public equity and stockholder for Eli Lilly & Company, and board member for Ophthalmic Mutual Insurance Company. The authors report no other conflicts of interest in this work.
References
1. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–9. doi:10.1001/jama.2014.3192
2. Dave SD, Zeppieri M, Meyer JJ. Chronic Closed Angle Glaucoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 January 25.
3. Nizami AA, Gurnani B, Gulani AC. Cataract. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024 February 27.
4. Vision Loss Expert Group of the Global Burden of Disease Study; GBD 2019 Blindness and Vision Impairment Collaborators. Global estimates on the number of people blind or visually impaired by cataract: a meta-analysis from 2000 to 2020. Eye. 2024;38(11):2156–2172. doi:10.1038/s41433-024-02961-1.
5. Pasquali A, Varano L, Ungaro N, et al. Does cataract extraction significantly affect intraocular pressure of glaucomatous/hypertensive eyes? Meta-analysis of literature. J Clin Med. 2024;13(2):508. doi:10.3390/jcm13020508
6. Tham CC, Kwong YY, Leung DY, et al. Phacoemulsification versus combined phacotrabeculectomy in medically uncontrolled chronic angle closure glaucoma with cataracts. Ophthalmology. 2009;116(4):725–731.e7313. doi:10.1016/j.ophtha.2008.12.054
7. Tham CC, Kwong YY, Leung DY, et al. Phacoemulsification versus combined phacotrabeculectomy in medically controlled chronic angle closure glaucoma with cataract. Ophthalmology. 2008;115(12):2167–2173.e2. doi:10.1016/j.ophtha.2008.06.016
8. Tham CC, Leung DY, Kwong YY, Li FC, Lai JS, Lam DS. Effects of phacoemulsification versus combined phaco-trabeculectomy on drainage angle status in primary angle closure glaucoma (PACG). J Glaucoma. 2010;19(2):119–123. doi:10.1097/IJG.0b013e31819d5d0c
9. Issa SA. A novel index for predicting intraocular pressure reduction following cataract surgery. Br J Ophthalmol. 2005;89(5):543–546. doi:10.1136/bjo.2004.047662
10. Kashiwagi K, Kashiwagi F, Tsukahara S. Effects of small-incision phacoemulsification and intraocular lens implantation on anterior chamber depth and intraocular pressure. J Glaucoma. 2006;15(2):103–109. doi:10.1097/00061198-200604000-00005
11. Perez CI, Chansangpetch S, Nguyen A, et al. How to predict intraocular pressure reduction after cataract surgery? A prospective study. Curr Eye Res. 2019;44(6):623–631. doi:10.1080/02713683.2019.1580375
12. Nguyen N, Mora JS, Gaffney MM, et al. A high prevalence of occludable angles in a Vietnamese population. Ophthalmology. 1996;103(9):1426–1431. doi:10.1016/s0161-6420(96)30488-0
13. Peng PH, Manivanh R, Nguyen N, Weinreb RN, Lin SC. Glaucoma and clinical characteristics in Vietnamese Americans. Curr Eye Res. 2011;36(8):733–738. doi:10.3109/02713683.2011.584009
14. Chansangpetch S, Tran B, Perez CI, et al. Comparison of anterior segment optical coherence tomography parameters among vietnamese, chinese, and whites. Am J Ophthalmol. 2018;195:72–82. doi:10.1016/j.ajo.2018.07.034
15. Do T, Nguyen Xuan H, Dao Lam H, et al. Ultrasound biomicroscopic diagnosis of angle-closure mechanisms in vietnamese subjects with unilateral angle-closure glaucoma. J Glaucoma. 2018;27(2):115–120. doi:10.1097/IJG.0000000000000856
16. Mitchell WG, Azuara-Blanco A, Foster PJ, et al. Predictors of long-term intraocular pressure control after lens extraction in primary angle closure glaucoma: results from the EAGLE trial. Br J Ophthalmol. 2023;107(8):1072–1078. doi:10.1136/bjophthalmol-2021-319765
17. Chen PP, Lin SC, Junk AK, Radhakrishnan S, Singh K, Chen TC. The effect of phacoemulsification on intraocular pressure in glaucoma patients. Ophthalmology. 2015;122(7):1294–1307. doi:10.1016/j.ophtha.2015.03.021
18. Huang G. Anterior chamber depth, iridocorneal angle width, and intraocular pressure changes after phacoemulsification. Arch Ophthalmol. 2011;129(10):1283. doi:10.1001/archophthalmol.2011.272
19. Song W, Sung K, Kim K. Assessment of iridotrabecular contact and its association with intraocular pressure after phacoemulsification in primary angle closure. Am J Ophthalmol. 2022;249:1–11.
20. Wang SY, Azad AD, Lin SC, Hernandez-Boussard T, Pershing S. Intraocular pressure changes after cataract surgery in patients with and without glaucoma: an informatics-based approach. Ophthalmol Glaucoma. 2020;3(5):343–349. doi:10.1016/j.ogla.2020.06.002
21. Rothman AL, Chang TC, Lum F, et al. Predictors of intraocular pressure response and survival after phacoemulsification for glaucomatous eyes in the IRIS registry (Intelligent Research in Sight). Sci Rep. 2024;14:19050. doi:10.1038/s41598-024-70148-5
22. Wang N, Chintala SK, Fini ME, Schuman JS. Ultrasound Activates the TM ELAM-1/IL-1/NF-κB response: a potential mechanism for intraocular pressure reduction after phacoemulsification. Investigat Opthalmol Vis Sci. 2003;44(5):1977. doi:10.1167/iovs.02-0631
23. Zhao Z, Zhu X, He W, Jiang C, Lu Y. Schlemm’s canal expansion after uncomplicated phacoemulsification surgery: an optical coherence tomography study. Investigat Opthalmol Vis Sci. 2016;57(15):6507. doi:10.1167/iovs.16-20583
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.