")
Back to Journals » Clinical Interventions in Aging » Volume 18
Association of Frailty with Adverse Outcomes in Patients with Critical Acute Myocardial Infarction: A Retrospective Cohort Study
Authors Bai W, Huang T, Li X, Gao W, Qin J, Bian Y , Xu W, Xu J, Qin L
Received 9 September 2023
Accepted for publication 14 December 2023
Published 18 December 2023 Volume 2023:18 Pages 2129—2139
DOI https://doi.org/10.2147/CIA.S439454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Weimin Bai,1,* Taoke Huang,2,* Xinying Li,3,* Weiyang Gao,2 Ji Qin,2 Yongxin Bian,4 Weihao Xu,5 Juan Xu,6 Lijie Qin1
1Department of Emergency, Henan Provincial People’s Hospital, People’s Hospital of Zhengzhou University, People’s Hospital of Henan University, Zhengzhou, 463599, People’s Republic of China; 2Medical School of Chinese PLA, Beijing, 100853, People’s Republic of China; 3Faculty of Postgraduate Education, Shandong Sport University, Jinan, 250102, People’s Republic of China; 4The First School of Clinical Medicine, Binzhou Medical University, Yantai, 264003, People’s Republic of China; 5Haikou Cadre’s Sanitarium of Hainan Military Region, Haikou, 570203, People’s Republic of China; 6Department of General Surgery, Affiliated Xiaoshan Hospital, Hangzhou Normal University, Hangzhou, 311202, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Juan Xu; Lijie Qin, Email [email protected]; [email protected]
Background: Frailty is a risk factor for acute myocardial infarction (AMI). This study examined the association between the modified frailty index (MFI) and adverse outcomes in patients with critical AMI.
Methods: Data were obtained from the Medical Information Mart for Intensive Care IV database. Logistic and Cox regression models and a competing risk model were applied.
Results: Of 5003 patients, 1496 were non-frail and 3507 were frail. Frailty was significantly associated with in-hospital mortality (per point, OR 1.13, 95% CI: 1.05– 1.21; frail vs non-frail, OR 1.31, 95% CI: 1.04– 1.65) and 1-year mortality (per point, HR 1.15, 95% CI: 1.11– 1.20; frail vs non-frail, HR 1.37, 95% CI: 1.20– 1.58). Frailty was significantly associated with post-discharge care needs (per point, OR 1.23, 95% CI: 1.14– 1.33; frail vs non-frail, OR 1.47, 95% CI: 1.22– 1.78). In the competing risk models, frailty was significantly associated with a lower probability of being discharged from the ICU (per point, HR 0.87, 95% CI: 0.85– 0.90; frail vs non-frail, HR 0.73, 95% CI: 0.68– 0.79) and hospital (per point, HR 0.82, 95% CI: 0.80– 0.85; frail vs non-frail, HR 0.62, 95% CI: 0.57– 0.68). Subgroup analyses showed the association of frailty with in-hospital and 1-year mortality was stronger in patients with a SOFA score ≤ 2 than in those with a SOFA score > 2 (both p< 0.05 for interaction).
Conclusion: Frailty assessed by the MFI was an independent predictor of adverse outcomes in patients with critical AMI and may be helpful for prognostic risk stratification.
Keywords: frailty, modified frailty index, acute myocardial infarction, critically ill patients, prognosis
Background
Frailty is an age-related biological syndrome that describes a state of increased vulnerability when maintaining homeostasis following an external stress due to decreased physiologic reserves. Frailty is characterized by poor mobility, weakness, reduced muscle mass, poor nutritional status, and cognitive decline and is associated with poor outcomes such as falls, hospitalization, and mortality.1 Frailty affects millions of older people worldwide, with a prevalence of 14.8% among people over 65 years of age.2 A population-based meta-analysis of 62 countries worldwide showed that the prevalence of frailty was as high as 12%, indicating that this issue has become a serious global public health burden.3
Cardiovascular disease (CVD), which affects most elderly people and is the second leading cause of mortality worldwide, triples the likelihood of frailty.4 The prevalence of frailty is high in patients with acute coronary syndrome (ACS), ranging from 20.8–48.5%, and the prevalence is related to the use of different frailty measures.5 There is substantial evidence that frailty is independently associated with adverse outcomes such as mortality and bleeding in patients with acute myocardial infarction (AMI), highlighting the importance of frailty assessment in the clinical management of AMI.5,6 The European Society of Cardiology clinical practice guidelines recommend conducting a frailty evaluation in patients with ACS for risk stratification and therapeutic decisions.7
With the exploration and development of frailty assessments in CVD, various frailty assessment tools have been used in patients with AMI, such as the Fried frailty phenotype (FFP),8 Edmonton Frail Scale,9 FRAIL Scale,10 and Canadian Study of Health and Aging Clinical Frailty Scale (CSHA-CFS).11,12 The modified frailty index (MFI) is a modification of the CSHA-Frailty Index that has been previously validated in other populations and can also be conveniently used in an intensive care unit (ICU) setting.13,14 The MFI may also predict adverse outcomes in patients undergoing aortic valve replacement with moderate predictive efficacy.15 The components of the MFI can be easily and objectively captured from inpatient information, eliminating the inter-operator variability and assessment burden of commonly used frailty tools. To our knowledge, no previous study has investigated the use of the MFI in patients with AMI, especially those with critical AMI.
In the present study, we analyzed data from the Medical Information Mart for Intensive Care (MIMIC)-IV database 2.0 to examine the association between frailty (as assessed by the MFI) and short- and long-term adverse outcomes in patients with critical AMI.
Methods
Database and Study Design
The data analyzed in this retrospective cohort study were extracted from the MIMIC-IV database 2.0, which is an openly accessible critical care database from which data are derived with pre-existing institutional review board approval.16,17 The MIMIC-IV database contains data for 76,943 ICU admissions from the Beth Israel Deaconess Medical Center (Boston, MA, USA) between 2008 and 2019. To gain access to the database, we completed the Collaborative Institutional Training Initiative examination (certification number: 10713670).
Inclusion and Exclusion Criteria
We considered all patients diagnosed with AMI during the analysis period, the same as in our previous study.18 We excluded patients with one or more of the following criteria: age <18 years; survival time <24 h or organ donors; pregnant patients or those with puerperal illness; and those missing key variables (demographic data, AMI type, Sequential Organ Failure Assessment [SOFA] score,19 items to construct the MFI, and vital status at hospital discharge and one year after ICU admission). For patients with more than one ICU stay, only the first ICU stay was included for analysis.
Data Collection
Two versions of the International Statistical Classification of Diseases and Related Health Problems (ICD) codes were used to record the diagnoses of specific diseases for patients in the MIMIC-IV database. All patients with AMI included in this study met the diagnostic criteria of the ICD-9 code 410 or ICD-10 code I21.
We extracted the following from the database as baseline patient data: demographic data (age, gender, ethnicity [Caucasian, African American, and other]); maximum SOFA scores within 24 h after ICU admission; medical history (cerebrovascular disease, chronic pulmonary disease, congestive heart failure, dementia, diabetes, malignant cancer, and renal disease); smoking history; AMI type (ST-segment elevation myocardial infarction [STEMI] and non-STEMI); systolic blood pressure (SBP); diastolic blood pressure (DBP); Body Mass Index (BMI) and laboratory parameters (hemoglobin, white blood cell [WBC] count, glucose, creatinine, and troponin T). ICU and hospital length of stay (LOS), discharge location, and vital status at hospital discharge and one year after ICU admission were extracted to define outcomes.
Modified Frailty Index (MFI)
The components of the MFI were available in the MIMIC database; therefore, the MFI was used to assess frailty for patients with AMI in this study. As previously described,13 the MFI was calculated as the sum of the number of confirmed items of the 11 items (one point per item) representing previous functional capacity (functional Status [Loss Function]) and comorbid conditions and previous complications (history of diabetes mellitus; congestive heart failure; hypertension requiring medication; either transient ischemic attack or cerebrovascular accident; myocardial infarction; either peripheral vascular disease or rest pain; cerebrovascular accident with neurological deficit; either chronic obstructive pulmonary disease or pneumonia; either prior percutaneous coronary intervention, coronary artery bypass grafting, or angina; impaired sensorium). The components of the MFI include a medical history of myocardial infarction; thus, the MFI for patients in this study was ≥1 point. Patients were categorized as non-frail (MFI = 1–2) or frail (MFI ≥3). The ICD codes used to extract the MFI components and the prevalence of each MFI component in the study population are shown in Table S1.
Outcomes
The primary outcomes were in-hospital and 1-year mortality. The secondary outcomes included subsequent care needs among discharge survivors (post-discharge care needs including hospice, home-care, and other healthcare facilities versus discharge home without a further need for nursing care)14 and prolonged ICU and hospital LOS. A prolonged LOS was defined as having an LOS longer than the 75th percentile (4.1 days for ICU LOS and 12.7 days for hospital LOS),20 and patients were censored at this time or at discharge.
Statistical Analyses
The normality of the data was tested using the Shapiro–Wilk test. Continuous variables are described as the mean ± standard deviation (SD) or median (interquartile range). Categorical variables are described as counts (percentages). Student’s t-test, Mann–Whitney U-test, and χ2 test were used for analyses, as appropriate. To investigate the relationship between frailty and adverse outcomes, frailty was assessed as a continuous and categorical variable. A logistic regression model was used to examine the association of frailty with in-hospital mortality and discharge with the need for nursing care. A Cox regression model was used to investigate the association between frailty and 1-year mortality. A competing risk model was applied to assess the association of frailty with prolonged ICU and hospital LOS, considering death as a competitor for both ICU and hospital discharge. Age, gender, ethnicity, smoking, SOFA scores, AMI type, SBP, DBP, BMI, hemoglobin, WBC count, glucose, creatinine, and troponin T were adjusted in the multivariable model. Restricted cubic spline curves with five knots were used to display the associations between the MFI and in-hospital mortality, 1-year mortality, and discharge with the need for nursing care. Subgroup analyses were conducted in multivariable models to examine the associations between the MFI (continuous variable) and primary outcomes in the following subgroups: age (<65 or ≥65 years), SOFA score (0–2 or >2), and AMI type (STEMI or non-STEMI). Interactions between the MFI and subgroups were also tested. All statistical analyses were performed in Stata, version 17.0 (StataCorp) and R (version 4.1.2) using a 2-tailed p-value <0.05 to define statistical significance.
Results
Baseline Characteristics
A total of 5237 patients with AMI were admitted to the ICU for the first time between 2008 and 2019. Of these, 5003 patients were eligible for the final analyses. Detailed selection procedures for the study population are shown in Figure S1. The baseline demographic and clinical characteristics of the included patients are presented in Table 1. The mean (± SD) age of the included patients was 69.8 ± 13.1 years, and 3169 patients (63.3%) were men. The mean MFI score was 3.3 ± 1.3 points, and the MFI score distribution for the study population is shown in Figure 1. There were 1496 (29.9%) non-frail and 3507 (70.1%) frail patients. Both frail and non-frail patients were predominantly male, and frail patients were older and with a higher proportion of women (38.6% vs 32.0%, p<0.001) as compared with non-frail patients. As expected, patients reporting frailty had a higher SOFA score and prevalence of smoking habits, cerebrovascular disease, chronic pulmonary disease, congestive heart failure, dementia, diabetes, and renal diseases compared to patients who did not. The non-frail group had a higher prevalence of STEMI (46.7% vs 32.6%, p<0.001) than the frail group. SBP, BMI, glucose, and creatinine were higher in the frail group than in the non-frail group, while DBP, hemoglobin, and troponin T were lower.
 |
Table 1 Characteristics of Included Patients According to Frailty Status as Assessed by the MFI (n=5003) |
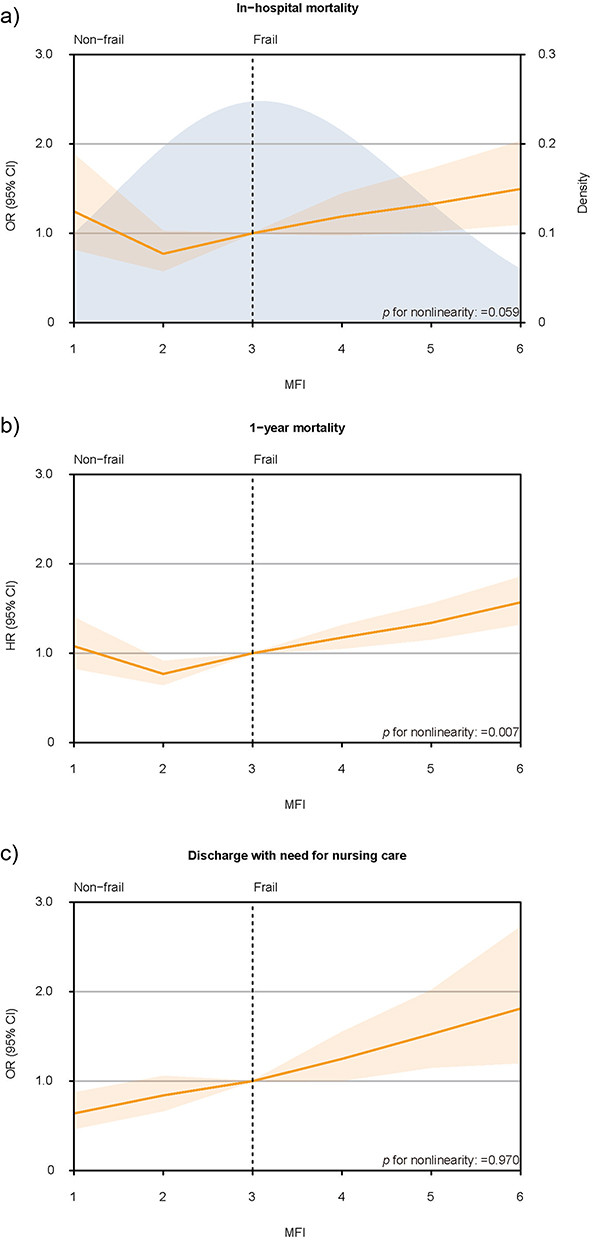 |
Figure 1 Distribution of MFI among study population and association of MFI with in-hospital mortality, 1-year mortality and discharge with need for nursing care. Spline curves showing the association of MFI with (a) in hospital mortality, (b) 1-year mortality and (c) discharge with need for nursing care. The density curve describes the distribution of MFI for more than 99% individuals in the study population. The dotted line indicates the cutoff score for non-frail and frail which is also the reference standard for association between frailty and outcomes (3 points for MFI). Spline curves were adjusted for age, gender, ethnicity, smoking, SOFA scores, AMI type (STEMI vs non-STEMI), SBP, DBP, BMI, hemoglobin, WBC, glucose, creatinine, and troponin T. |
Association of Frailty with In-Hospital Frailty and 1-Year Mortality
A total of 690 patients (13.8%) died during hospitalization. Frail patients had a higher rate of in-hospital mortality than non-frail patients (Table 2). In an unadjusted logistic regression model, the MFI was significantly associated with in-hospital mortality both as a continuous (per point increase, odds ratio [OR] 1.23, 95% confidence interval [CI]: 1.16–1.30) and categorical variable (frail vs non-frail, OR 1.82, 95% CI: 1.50–2.22). The association between the MFI score and in-hospital mortality persisted in the adjusted multivariable model (per point increase, OR 1.13, 95% CI: 1.05–1.21; frail vs non-frail, OR 1.31, 95% CI: 1.04–1.65; Table 2, Figure 1).
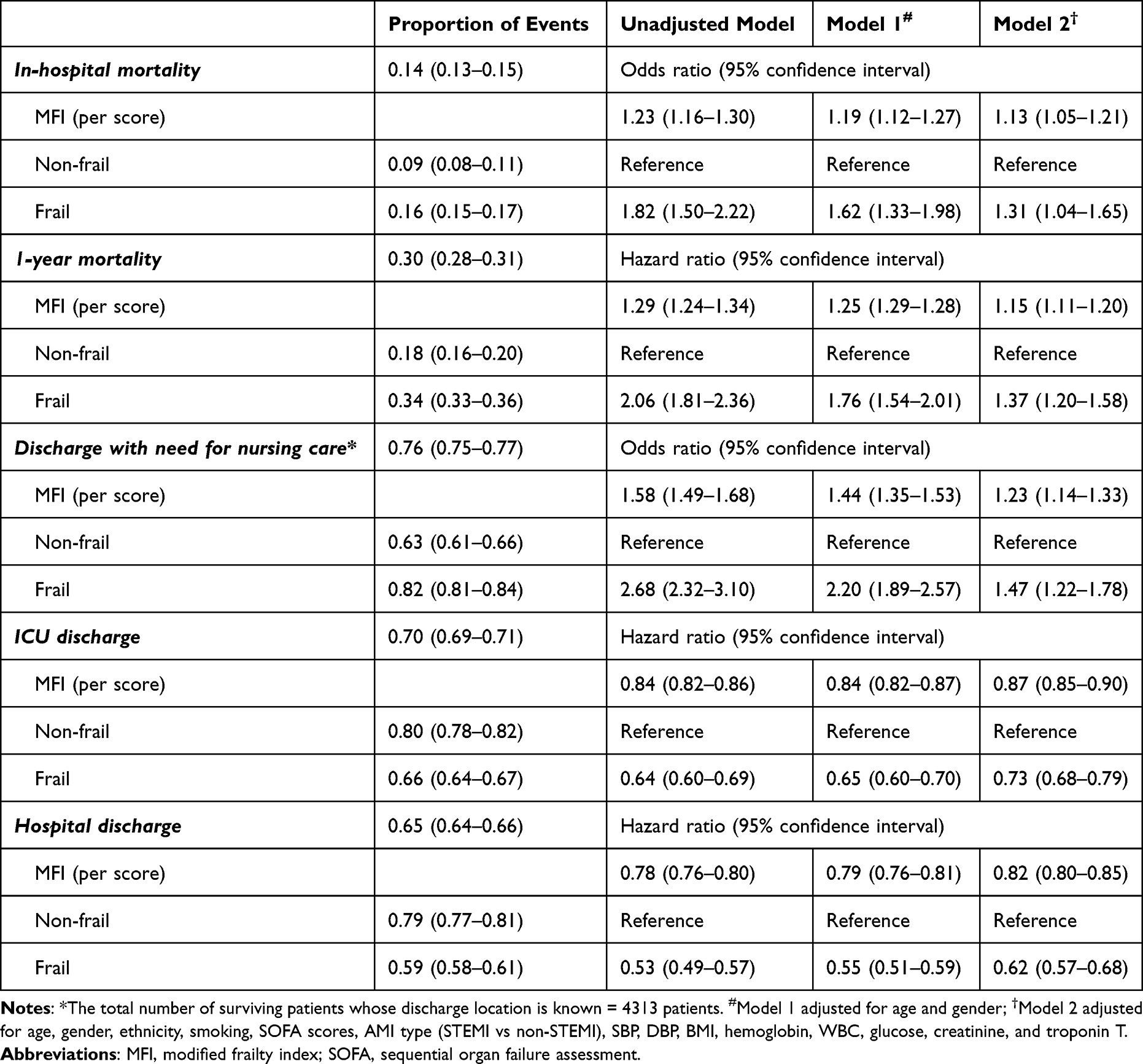 |
Table 2 Association Between Frailty and Outcomes |
A total of 1474 patients (29.5%) died within the 1-year follow-up period. One-year mortality was higher in frail than in non-frail patients (Table 2). In an unadjusted Cox model, the MFI score was significantly associated with 1-year mortality both as a continuous (per point increase, hazard ratio [HR] 1.29, 95% CI: 1.24–1.34) and categorical variable (frail vs non-frail, HR 2.06, 95% CI: 1.81–2.36). The MFI score was also significantly associated with 1-year mortality in the adjusted multivariable model (per point increase, HR 1.15, 95% CI: 1.11–1.20; frail vs non-frail, HR 1.37, 95% CI: 1.20–1.58; Table 2, Figure 1). There was a significant, nonlinear association between MFI (assessed as a continuous variable) and 1-year mortality (p = 0.007 for nonlinearity; Figure 1).
Association Between Frailty and Post-Discharge Care Needs
Among the 4313 survivors at discharge, 3285 patients (76.2%) needed subsequent nursing care. This percentage was higher for frail than for non-frail patients (82.1% vs 63.2%, Table 1). The MFI score was significantly associated with discharge with the need for nursing care in the adjusted multivariable model (per point increase, OR 1.23, 95% CI: 1.14–1.33; frail vs non-frail, OR 1.47, 95% CI: 1.22–1.78; Table 2). Figure 1 shows that the OR of discharge with the need for nursing care increased with an increasing MFI score.
Association Between Frailty and Prolonged ICU and Hospital LOS
Frail patients had longer ICU and hospital LOS than non-frail patients (Table 1). The results of a multivariable competing risks analysis, which considered death as a competitor for both ICU and hospital discharge, showed that an increasing MFI score was significantly associated with a progressively lower probability of being discharged from the ICU (per point increase, HR 0.87, 95% CI: 0.85–0.90) and hospital (per point increase, HR 0.82, 95% CI: 0.80–0.85). When assessed as a categorical variable, frailty was also significantly associated with a lower probability of being discharged from the ICU (frail vs non-frail, HR 0.73, 95% CI: 0.68–0.79) and hospital (frail vs non-frail, HR 0.62, 95% CI: 0.57–0.68; Table 2).
Subgroup Analyses
The results of subgroup analyses for the association between frailty and in-hospital mortality are shown in Figure 2. Patients aged ≥65 years had a higher risk of in-hospital mortality for each point increase in MFI (OR 1.14, 95% CI: 1.05–1.24). The MFI score was not significantly associated with in-hospital mortality in patients aged <65 years (OR 1.14, 95% CI: 0.99–1.32). There was a statistically significant (p = 0.025) interaction between frailty and the SOFA score: the association between frailty and in-hospital mortality in patients with a SOFA score ≤2 (OR 1.26, 95% CI: 1.02–1.56) was significantly stronger than that in patients with a SOFA score >2 (OR 1.09, 95% CI: 1.01–1.18).
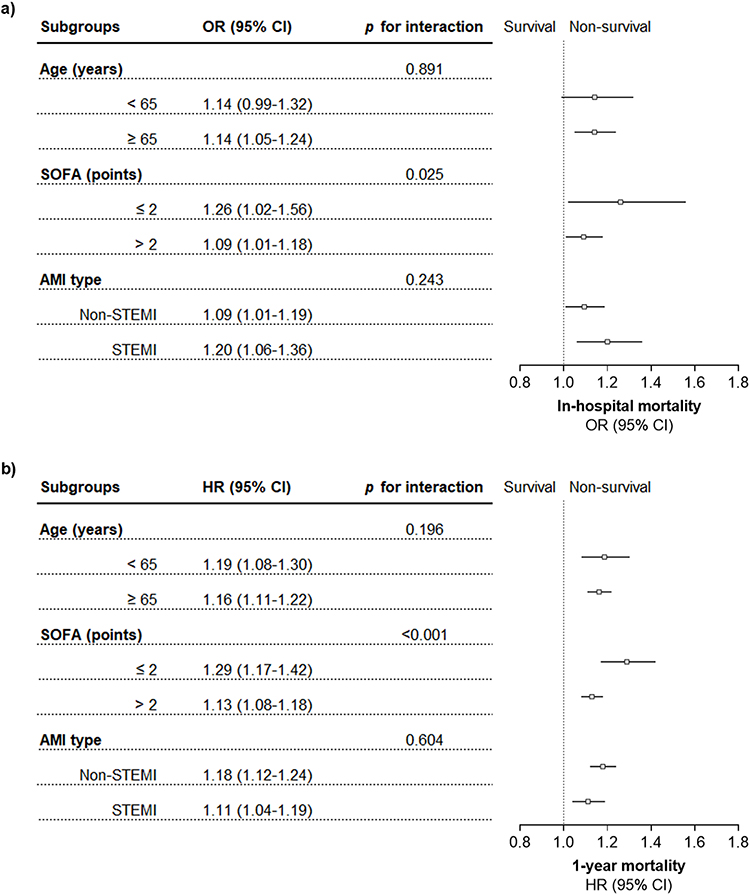 |
Figure 2 Forest plots of subgroup analyses of the association between frailty and primary outcomes. The association between frailty and (a) in-hospital and (b) 1-year mortality. Models were adjusted for age, gender, ethnicity, smoking, SOFA scores, AMI type, SBP, DBP, BMI, hemoglobin, WBC count, glucose, creatinine, and troponin T. Continuous variables for age and SOFA score were still adjusted in the age and SOFA score subgroups, while adjustment for AMI type was omitted in the AMI type subgroup. |
In the subgroup analysis for the association between frailty and 1-year mortality, frailty and 1-year mortality were significantly associated, regardless of whether patients were older than 65 years (Figure 2), and there was no significant interaction between age and frailty (p = 0.196 for interaction). Conversely, there was a statistically significant (p <0.001) interaction between frailty and the SOFA score: the association between frailty and 1-year mortality in patients with a SOFA score ≤2 (HR 1.29, 95% CI: 1.17–1.42) was significantly stronger than that in patients with a SOFA score >2 (HR 1.13, 95% CI: 1.08–1.18).
Frailty was significantly associated with both in-hospital and 1-year mortality in the AMI-type subgroup, but there was no significant interaction between AMI type and frailty (Figure 2).
Discussion
To our knowledge, this is the first study to examine the association between frailty as assessed by the MFI and short- and long-term adverse outcomes in patients with critical AMI. As expected, frail patients assessed by MFI were older, had a higher prevalence of common diseases, and had significant changes in physiological and laboratory parameters compared with non-frail patients. Our study demonstrated that frailty was not only significantly associated with in-hospital and 1-year mortality in ICU patients with AMI but was also an independent predictor of prolonged ICU and hospital LOS and post-discharge care needs.
More than a decade ago, the American Heart Association, Society of Geriatric Cardiology, and European Society of Cardiology called for an increased focus on frailty assessments in patients with CVD.21 At present, more than 30 frailty assessment tools have been developed and used in epidemiological research and clinical practice.22 The application of various frailty assessment tools in patients with ACS, especially in those with AMI, has been reported.5,6 Batty et al reported that frailty as assessed by the FFP was present in 27.5% of patients with non-STEMI undergoing revascularization and was associated with adverse short- and long-term outcomes.8 In another study, 48.5% of patients with non-STEMI were assessed as frail by the CSHA-CFS, and the predictive value of CSHA-CFS for all-cause mortality at five years was reported.11 The prevalence of frailty assessed by the FRAIL scale was 19.7% in patients with STEMI aged ≥75 years or older undergoing percutaneous coronary intervention and frailty was independently associated with in-hospital mortality.10 In our previous research,18 we reported on another frailty assessment method based on electronic medical record data called the Hospital Frailty Risk Score (HFRS),23 and its association with in-hospital and one-year mortality in the same population. The results showed that frailty, as assessed by the HFRS, was significantly associated with both in-hospital and one-year mortality in critical acute myocardial infarction (AMI) patients. The use of the HFRS improved the ability to predict short- and long-term mortality in these patients.
However, frailty assessment methods based on self-report and/or objective measures such as the FRAIL scale,24 Edmonton Frail Scale25 and FFP26 may not be feasible in the ICU setting, which are limited by patients’ state of consciousness and mobility. Conversely, frailty assessment methods based on electronic medical record data are easy to implement, which not only increase the objectivity of frailty assessments but also reduce the burden on physicians. Our study provides evidence for the use of MFI in patients with critical AMI. Notably, the MFI components incorporate various diagnoses related to cardiovascular and cerebrovascular diseases, which result in a high prevalence of frailty when using the MFI to assess frailty in patients with CVD or AMI. For the association with 1-year mortality in our study, HR was reduced at MFI=2. This may be due to the restriction of sample size (only 407 individuals with MFI=1), which could not conclude that MFI=1 was a protective factor for 1-year mortality compared with MFI = 3, so the HR at MFI = 2 showed an illusion of decreasing.
To our knowledge, few studies have focused on ICU and hospital LOS and post-discharge care needs in critically ill patients with AMI. Our study explored these two questions and focused on mortality outcomes. We defined a prolonged LOS as an ICU or a hospital LOS exceeding the highest quartile. However, this small group of patients with a prolonged LOS consumed the most ICU (62.0%) and hospital (53.3%) bed days of all patients. Our findings suggest that frail patients with critical AMI are at a greater risk of a prolonged LOS than non-frail patients, which requires substantial resource utilization and is associated with an increased economic burden. This is also a challenge for the allocation and orderly use of hospital medical resources. Strengthening the identification of this group could facilitate the development of individualized management to reduce the individual and societal burdens caused by the increased medical needs of critically ill patients with AMI.27,28 Critically ill patients may experience functional deterioration at the time of discharge and may require temporary or permanent support from community social care and rehabilitation services, which greatly affects patients’ quality of life. Thus, maintaining independence and preserving or improving functional status are important treatment goals. In our study, we demonstrated that the MFI used as a frailty screening tool can identify patients at risk of discharge to a non-home location after surviving a critical AMI. This can facilitate targeted implementation of multidisciplinary post-acute rehabilitation, such as comprehensive geriatric assessments to reduce post-acute, long-term functional dependence and mortality.29
Frailty is traditionally described in the elderly and emphasizes the functional decline seen with aging.30 However, recent literature describes that frailty also affects the health status of younger people (aged <65 years),31 and our findings showed that frailty was significantly associated with 1-year mortality in patients aged <65 years. Although there was no significant association between frailty and in-hospital mortality in patients aged <65 years, the statistical results indicated that a significant association may be expected if the sample size is increased further. The results of the interaction analyses indicated that the association between frailty and increased mortality was more evident in patients with SOFA score ≤2, and frailty was poorly predictive of adverse outcomes in patients with critical AMI with severe systemic organ damage (as assessed by the SOFA score) and even disappeared with the aggravation of systemic organ damage. However, MFI also provides additional information for prognostic risk stratification in patients with milder systemic organ damage, and this result has also been reported in a recent study.14 Further research is needed on the use of the MFI to further stratify the prognosis of critically ill patients with AMI.
The strength of this study is that our findings were derived from a high-quality database with a large sample size. We believe that this is the first study to demonstrate the prognostic value of frailty as assessed by the MFI for various adverse outcomes in patients with critical AMI. There are also some limitations in our study. First, use of the ICD-10 code “R26” (abnormalities of gait and mobility) and the ICD-9 codes “7197” (difficulty in walking) and “7812” (abnormality of gait) to assess the functional status of patients might have led to slight inaccuracy of the MFI. Second, because we could not obtain the currently recognized prognostic scores associated with adverse outcomes in patients with AMI, such as the Global Registry of Acute Coronary Events/Thrombolysis in Myocardial Infarction risk score, from the database, we did not consider the influence of these scores on the model in the multivariable analysis. Third, it was found in a previous study that frail subjects present physical and cognitive decline.32 In frail elderly STEMI patients, those with lower gait speed test scores had the worst Mini-Mental State Examination (MMSE) scores.33 However, data on the global cognitive scores (eg, the Montreal Cognitive Assessment and MMSE) and physical activity measurement (eg, the 5-m gait speed test) were not available in the MIMIC database. The role of cognitive and physical impairment in frailty in the ICU setting is an interesting and important topic that deserves further exploration.
Conclusions
Frailty as assessed by the MFI was an independent predictor of in-hospital mortality, 1-year mortality, need for nursing care after discharge, and prolonged ICU and hospital LOS in patients with critical AMI. The MFI is a convenient tool for frailty assessment in the ICU setting, which may be helpful for further prognostic risk stratification of critically ill patients with AMI.
Data Sharing Statement
The datasets presented in the current study are available in the MIMIC-IV database 2.0 (https://doi.org/10.13026/7vcr-e114).
Ethics Approval and Consent to Participate
The establishment of this de-identified database was approved by the Institutional Review Board at the Beth Israel Deaconess Medical Center. Written informed consent for participation was not required for this project in accordance with the national legislation and the institutional requirements. To gain access to the database, we completed the Collaborative Institutional Training Initiative examination (certification number: 10713670), and no additional ethical approval was required for this study.
Acknowledgments
We are extremely grateful to the Laboratory for Computational Physiology team from the Massachusetts Institute of Technology (LCP-MIT) who establish and maintain the MIMIC-IV databases.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–1375. doi:10.1016/S0140-6736(19)31786-6
2. Castellana F, Lampignano L, Bortone I, et al. Physical frailty, multimorbidity, and all-cause mortality in an older population from southern Italy: results from the Salus in Apulia Study. J Am Med Dir Assoc. 2021;22(3):598–605. doi:10.1016/j.jamda.2020.12.026
3. O’Caoimh R, Sezgin D, O’Donovan MR, et al. Prevalence of frailty in 62 countries across the world: a systematic review and meta-analysis of population-level studies. Age Ageing. 2021;50(1):96–104. doi:10.1093/ageing/afaa219
4. Newman AB, Gottdiener JS, McBurnie MA, et al. Associations of subclinical cardiovascular disease with frailty. J Gerontol a Biol Sci Med Sci. 2001;56(3):M158–M166. doi:10.1093/gerona/56.3.m158
5. Dou Q, Wang W, Wang H, et al. Prognostic value of frailty in elderly patients with acute coronary syndrome: a systematic review and meta-analysis. BMC Geriatr. 2019;19(1):222. doi:10.1186/s12877-019-1242-8
6. Putthapiban P, Vutthikraivit W, Rattanawong P, et al. Association of frailty with all-cause mortality and bleeding among elderly patients with acute myocardial infarction: a systematic review and meta-analysis. J Geriatr Cardiol. 2020;17(5):270–278. doi:10.11909/j.issn.1671-5411.2020.05.006
7. Collet JP, Thiele H, Barbato E, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–1367. doi:10.1093/eurheartj/ehaa575
8. Batty J, Qiu W, Gu S, et al. One-year clinical outcomes in older patients with non-ST elevation acute coronary syndrome undergoing coronary angiography: an analysis of the Icon1 Study. Int J Cardiol. 2019;274:45–51. doi:10.1016/j.ijcard.2018.09.086
9. Blanco S, Ferrieres J, Bongard V, et al. Prognosis impact of frailty assessed by the Edmonton Frail Scale in the setting of acute coronary syndrome in the elderly. Can J Cardiol. 2017;33(7):933–939. doi:10.1016/j.cjca.2017.03.026
10. Calvo E, Teruel L, Rosenfeld L, et al. Frailty in elderly patients undergoing primary percutaneous coronary intervention. Eur J Cardiovasc Nurs. 2019;18(2):132–139. doi:10.1177/1474515118796836
11. Ekerstad N, Pettersson S, Alexander K, et al. Frailty as an instrument for evaluation of elderly patients with Non-St-Segment elevation myocardial infarction: a follow-up after more than 5 years. Eur J Prev Cardiol. 2018;25(17):1813–1821. doi:10.1177/2047487318799438
12. Sujino Y, Tanno J, Nakano S, et al. Impact of hypoalbuminemia, frailty, and body mass index on early prognosis in older patients (>/=85 years) with ST-elevation myocardial infarction. J Cardiol. 2015;66(3):263–268. doi:10.1016/j.jjcc.2014.12.001
13. Farhat JS, Velanovich V, Falvo AJ, et al. Are the frail destined to fail? Frailty Index as predictor of surgical morbidity and mortality in the elderly. J Trauma Acute Care Surg. 2012;72(6):
14. Zampieri FG, Iwashyna TJ, Viglianti EM, et al. Association of frailty with short-term outcomes, organ support and resource use in critically ill patients. Intensive Care Med. 2018;44(9):1512–1520. doi:10.1007/s00134-018-5342-2
15. Esses G, Andreopoulos E, Lin HM, Arya S, Deiner S. A comparison of three frailty indices in predicting morbidity and mortality after on-pump aortic valve replacement. Anesth Analg. 2018;126(1):39–45. doi:10.1213/ANE.0000000000002411
16. Johnson A, Bulgarelli L, Pollard T, Horng S, Celi LA, Mark R. MIMIC-IV (version 2.0). PhysioNet. 2022. doi:10.13026/7vcr-e114
17. Goldberger AL, Amaral LA, Glass L, et al. Physiobank, physiotoolkit, and physionet: components of a new research resource for complex physiologic signals. Circulation. 2000;101(23):E215–E220. doi:10.1161/01.cir.101.23.e215
18. Bai W, Hao B, Meng W, Qin J, Xu W, Qin L. Association between frailty and short- and long-term mortality in patients with critical acute myocardial infarction: results from Mimic-Iv. Front Cardiovasc Med. 2022;9:1056037. doi:10.3389/fcvm.2022.1056037
19. Vincent JL, Moreno R, Takala J, et al. The Sofa (Sepsis-Related Organ Failure Assessment) Score to describe organ dysfunction/failure. On behalf of the working group on sepsis-related problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22(7):707–710. doi:10.1007/BF01709751
20. Agrawal S, Chen L, Tergas AI, et al. Characteristics associated with prolonged length of stay after hysterectomy for benign gynecologic conditions. Am J Obstet Gynecol. 2018;219(1):89 e1- e15. doi:10.1016/j.ajog.2018.05.001
21. Alexander KP, Newby LK, Cannon CP, et al. Acute coronary care in the elderly, part I: non-ST-segment-elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American heart association council on clinical cardiology: in collaboration with the society of geriatric cardiology. Circulation. 2007;115(19):2549–2569. doi:10.1161/CIRCULATIONAHA.107.182615
22. Rasiah J, Gruneir A, Oelke ND, Estabrooks C, Holroyd-Leduc J, Cummings GG. Instruments to assess frailty in community dwelling older adults: a systematic review. Int J Nurs Stud. 2022;134:104316. doi:10.1016/j.ijnurstu.2022.104316
23. Gilbert T, Neuburger J, Kraindler J, et al. Development and validation of a hospital frailty risk score focusing on older people in acute care settings using electronic hospital records: an observational study. Lancet. 2018;391(10132):1775–1782. doi:10.1016/S0140-6736(18)30668-8
24. Aprahamian I, Cezar NOC, Izbicki R, et al. Screening for frailty with the frail scale: a comparison with the phenotype criteria. J Am Med Dir Assoc. 2017;18(7):592–596. doi:10.1016/j.jamda.2017.01.009
25. Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale. Age Ageing. 2006;35(5):526–529. doi:10.1093/ageing/afl041
26. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.m146
27. Theou O, Campbell S, Malone ML, Rockwood K. Older adults in the emergency department with frailty. Clin Geriatr Med. 2018;34(3):369–386. doi:10.1016/j.cger.2018.04.003
28. Eamer GJ, Clement F, Holroyd-Leduc J, Wagg A, Padwal R, Khadaroo RG. Frailty predicts increased costs in emergent general surgery patients: a prospective cohort cost analysis. Surgery. 2019;166(1):82–87. doi:10.1016/j.surg.2019.01.033
29. Ellis G, Gardner M, Tsiachristas A, et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. 2017;9:CD006211. doi:10.1002/14651858.CD006211.pub3
30. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
31. Loecker C, Schmaderer M, Zimmerman L. Frailty in young and middle-aged adults: an integrative review. J Frailty Aging. 2021;10(4):327–333. doi:10.14283/jfa.2021.14
32. Katayama O, Lee S, Bae S, et al. Lifestyle activity patterns related to physical frailty and cognitive impairment in urban community-dwelling older adults in Japan. J Am Med Dir Assoc. 2021;22(3):583–589. doi:10.1016/j.jamda.2020.05.031
33. Mone P, Gambardella J, Pansini A, et al. Cognitive dysfunction correlates with physical impairment in frail patients with acute myocardial infarction. Aging Clin Exp Res. 2022;34(1):49–53. doi:10.1007/s40520-021-01897-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.