Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Association of Euthyroid Thyroid Hormone Levels with Hepatic Steatosis in Patients with Nonalcoholic Fatty Liver Disease
Authors Oral A ![]() , Çavuşoğlu Türker B, Anılır E
, Çavuşoğlu Türker B, Anılır E ![]() , Şahin T
, Şahin T ![]() , Koçak E, Türker F
, Koçak E, Türker F ![]()
Received 16 September 2025
Accepted for publication 27 November 2025
Published 23 May 2026 Volume 2026:19 555563
DOI https://doi.org/10.2147/DMSO.S555563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Alihan Oral,1 Betül Çavuşoğlu Türker,2 Ender Anılır,3 Tolga Şahin,4 Erdem Koçak,5 Fatih Türker2
1Department of Internal Medicine, Biruni University, İstanbul, Turkey; 2Department of Internal Medicine, Haseki Health Training and Research Hospital, University of Health Sciences Turkey, İstanbul, Turkey; 3Department of General Surgery, Ödemis State Hospital, İzmir, Turkey; 4Department of Gastroenterology, Bayındır Içerenköy Hospital, İstanbul, Turkey; 5Department of Internal Medicine, Istınye University, İstanbul, Turkey
Correspondence: Fatih Türker, Department of Internal Medicine, Haseki Health Training and Research Hospital, University of Health Sciences Turkey, Aksaray, Dr. Adnan Adıvar Cd. No: 9, 34130 Fatih, İstanbul, Turkey, Tel +905364721656, Fax +90212 453 20 00, Email [email protected]
Purpose: The frequency of nonalcolic fatty liver disease (NAFLD), a major health issue that affects people all over the world, has been rising recently. Numerous studies have demonstrated the tight connection between NAFLD and thyroid function. In this study, we aimed to evaluate the relationship between thyroid function tests and the degree of liver steatosis in patients with biopsy proven NAFLD.
Patients and Methods: We retrospectively evaluated data of living donor applicants who received liver biopsies. Three hundred sixty seven patients were included in the study. According to the liver biopsy results, the patients were divided into two groups; 227 patients biopsy-proven NAFLD and 145 control subjects without NAFLD. Demographic, anthropometric and laboratory parameters were compared between two groups.
Results: All groups thyroid function tests fall within the normal range. However, in patients with NAFLD, serum FT3 and FT4 levels were significantly higher than control group. In addition negative relationship was found between the levels of FT3, FT4, and the stage of NAFLD. In patients with NAFLD, alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, triglyceride, total cholesterol levels, homeostasis model assessment of insulin resistance (HOMA-IR), body mass index were significantly high.
Conclusion: In this retrospective study, we showed that in patients with NAFLD, serum FT3 and FT4 levels were significantly lower than the control group. Our findings support that low levels of serum FT3 and FT4 might be a risk factor for liver steatosis in euthyroid patients with NAFLD.
Keywords: nonalcolic fatty liver disease, thyroid function, hepatic steatosis
Introduction
An urgent public health issue called nonalcolic fatty liver disease (NAFLD) can result in cirrhosis, hepatocellular cancer, and chronic liver disease, affects around 30% of the population and is continuously becoming more prevalent.1,2 NAFLD is the primary contributor of abnormal liver tests, according to population-based research.3 The rising prevalence of diabetes, obesity, and other metabolic risk factors are the main causes of nonalcolic steatohepatitis (NASH).4 Some studies have shown that the prevalence of NAFLD in patients with diabetes and obesity reaches 80%.5,6 According to the American Association for the Study of Liver Diseases, numerous conditions, including hypothyroidism, have been reported to increase the risk of NAFLD/NASH.7 The thyroid and NAFLD have a close relationship, according to numerous clinical investigations.8 The regulation of hepatic lipid, cholesterol, and glucose metabolism is greatly influenced by thyroid hormones. Ampirde thyroid hormone signaling decreases the liver’s ability to use fatty acids, which causes the fatty acids to be esterified and build up as triglycerides.9,10 As a result, abnormal thyroid hormone levels predispose to NAFLD/NASH.11 However, the role of FT3 and FT4 levels within the normal range in NAFLD patients remains unclear. Our study’s objective was to assess how thyroid hormone levels affected the emergence of NAFLD.
Materials and Method
In this study, we retrospectively assessed the data of living liver donor candidates who underwent liver biopsies between January 2010 and January 2019. Donor candidates who underwent biopsy due to the finding of moderate to severe liver steatosis on imaging and whose steatosis was histopathologically verified were included in the study. The study was approved by the Ethics Committee of Demiroglu Bilim University (No: 20191603) and performed in accordance with National Institute of Health guidelines and conducted in accordance with good clinical practice principles and the Declaration of Helsinki. Since the patients had given systematic consent upon applying to the physician, it was deemed unnecessary to obtain written consent with an ethics committee decision. All of the patients had imaging procedures, such as abdominal ultrasonography, computed tomography, and magnetic resonance, prior to liver biopsy. A liver biopsy was done when imaging techniques revealed moderate to severe fatty liver disease. The same expert liver pathologist assessed each liver biopsy sample and categorized them all using the NASH Clinical Research Network.12 Three hundred and seventy two patients with liver biopsy-proven NAFLD or those without NAFLD based on histopathological investigations made up the study population (Figure 1).
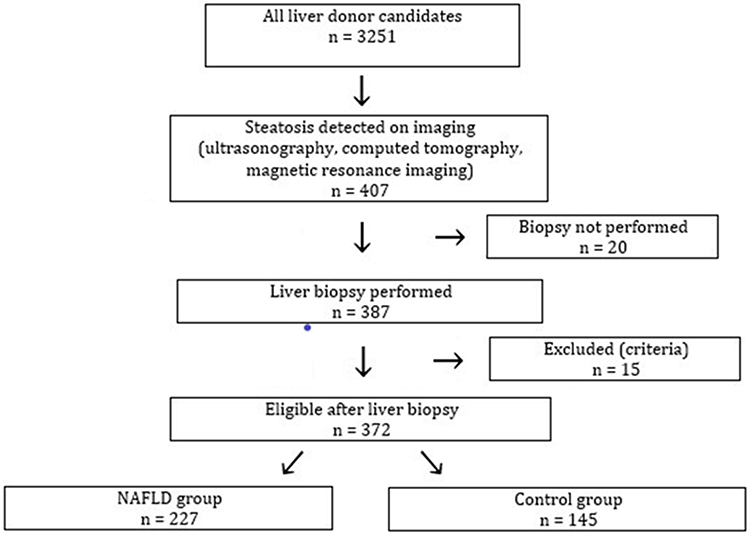 |
Figure 1 Flowchart of the number of patients included in the study. |
Male or female participants between the ages of 18 and 65 were required to meet the following criteria: normal thyroid function, non-obesity (body mass index (BMI) <30), lack of history of binge drinking (ethyl alcohol consumption is greater than 30 grams for men and 20 grams for women per day), and the hepatitis B surface antigen and hepatitis C virus antibody have been tested negative. Patients with any thyroid diseases or using drug for these diseases, any other chronic liver diseases, diabetes mellitus, heart failure, asthma, hemathologic problems, acute or chronic infections, a history of malignancy, drug-associated fatty liver, or refusal to participate in the study were the exclusion criteria. Data on anthropometric traits (such as age, gender, and BMI) and biochemistry were gathered. Total cholesterol (TC), triglycerides (TG), alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma glutamyl transferase (GGT), alkaline phosphatase (ALP), total bilirubin (TB), albumin, free triiodothyronine (FT4), free thyroxine (FT3), thyroid-stimulating hormone (TSH), glucose, and insulin were all included as biochemical parameters. Formula: (22.5 fasting insulin [mU/mL] glucose [mmol/L]) was used to calculate the insulin resistance score (HOMA-IR). Insulin resistance was identified using HOMA-IR 2.5.13 Age, gender, BMI, the levels of ALT (IU/L), AST (IU/L), ALP (U/L), GGT (U/L), total biluribin (mg/dl), albumin (g/dl), triglyceride (mg/dL), and total cholesterol (mg/dl) were compared statistically between the NAFLD and control groups. Additionally, HOMA-IR, FT3, and FT4 levels were compared statistically between the NAFLD and control groups.
The study used SPSS 21.0 for statistical analysis, examining mean values, standard deviations, ranges, and percentages. Normality was assessed using Kolmogorov–Smirnov test, Mann Whitney U-test, and χ2 test for categorical parameters. Spearman coefficient was used for bivariate correlation.
Results
There were 372 patients overall (145 in the control group and 227 in the NAFLD group). The patients median (IQR) ages were 34.00 (26.00–46.00) years for NAFLD and 34.00 (27.00–46.00) years for controls. In both the NAFLD and control groups, each patient had a BMI below 30. The median body mass index was 27.10 (24.50–30.00) in the NAFLD group and 24.1 (22.50–27.00) in the control group, and it was statistically higher in the NAFLD group (p < 0.001). HOMA-IR, ALT, AST, ALP, triglyceride, and total cholesterol levels were significantly higher in the NAFLD group compared to the control group (p < 0.05). However, there were no statistically significant differences in GGT, total biluribin, and albumin levels between the two groups (p > 0.05) (Table 1).
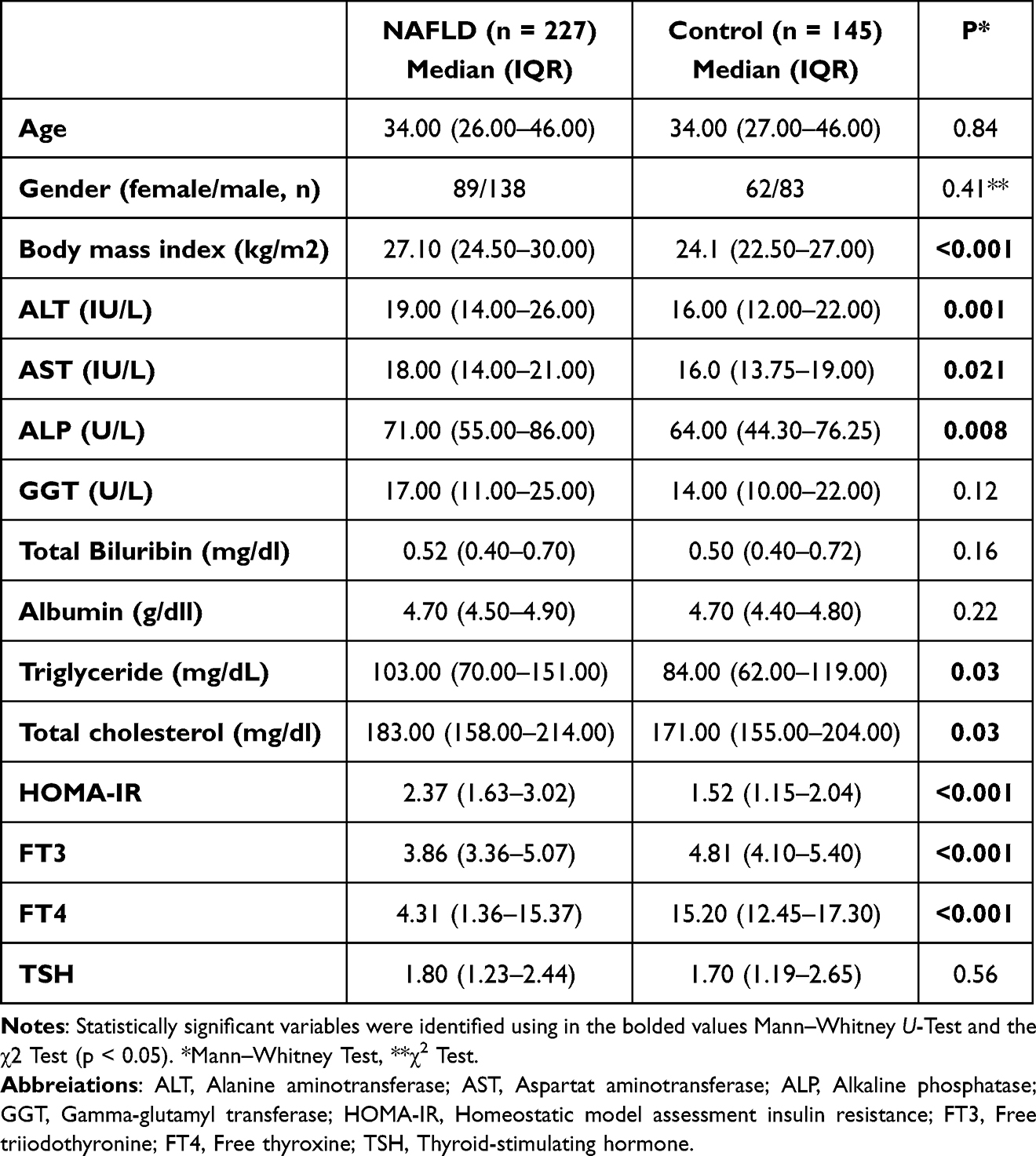 |
Table 1 Clinical, Laboratory, and Demographic Data of NAFLD Patients Compared to Controls |
Additionally, FT3, and FT4 levels were significantly lower in the NAFLD group compared to the control group (p < 0.001), while there was no statistically significant difference in TSH levels between the two groups (p > 0.05) (Table 1).
NAFLD stage was observed to have negative relationship between the values of serum FT3, and FT4 (FT3: r = −0.276, P 0.001; FT4: r = −0.207, P 0.001). TSH levels and NAFLD stage did not correlate (TSH: r = 0.072, P = 0.350) (Table 2).
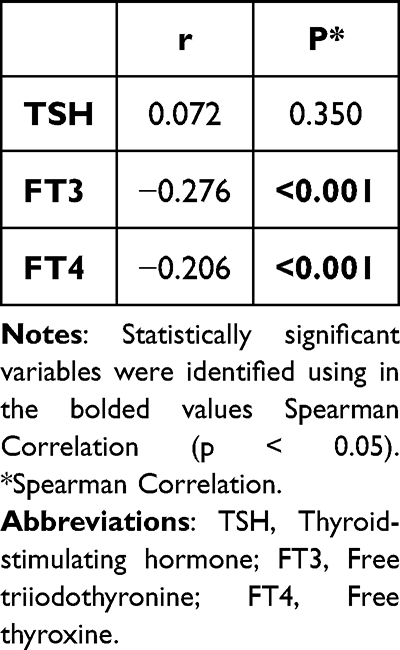 |
Table 2 Correlation Analysis Between Thyroid Hormones and NAFLD Stage |
The ROC curve for FT4 and FT3 in estimating NAFLD was constructed, and the area under the curve of FT4 0.681 (95% CI = 0.624 to 0.737, P < 0.001) and FT3 0.645 (95% CI = 0.625 to 0.739, P < 0.001) were found. The cut-off values of FT4 were 13.92 mg/dl with sensitivity of 65.6% and specificity of 65.8%. The cut-off values of FT3 were 4.58 mg/dl with sensitivity of 63.6% and specificity of 62.0% (Figure 2).
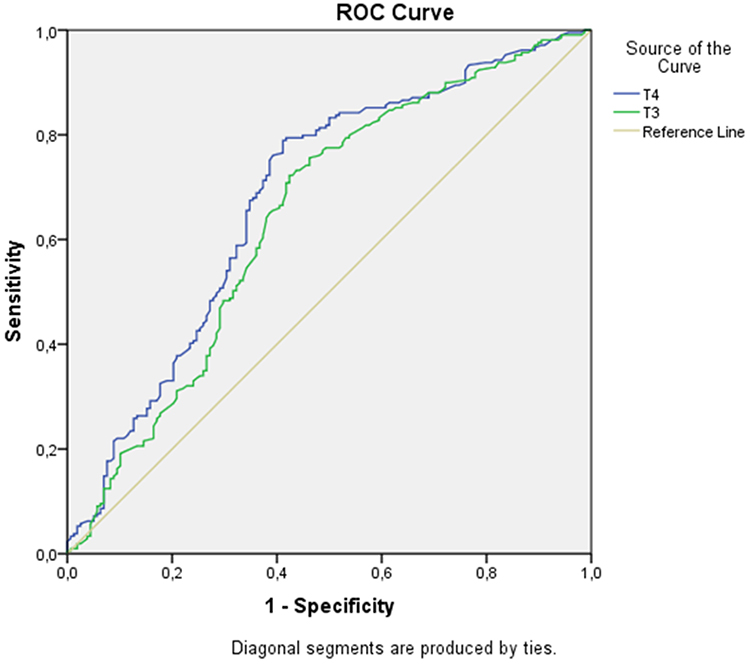 |
Figure 2 Curve for the prediction of NAFLD by FT4 and FT3. The ROC curve for FT4 and FT3 in estimating NAFLD was constructed, and the area under the curve of FT4 0.681 (95% CI = 0.624 to 0.737, P < 0.001) and FT3 0.645 (95% CI = 0.625 to 0.739, P < 0.001) were found. The cut-off values of FT4 were 13.92 mg/dl with sensitivity of 65.6% and specificity of 65.8%. The cut-off values of FT3 were 4.58 mg/dl with sensitivity of 63.6% and specificity of 62.0%. |
Discussion
In our study, we found that in patients with NAFLD, serum FT3 and FT4 levels were significantly lower than the control group. Moreover, stage of NAFLD was negatively correlated with serum FT3 and FT4 levels. In addition, serum triglyceride, total cholesterol levels and HOMA-IR were both higher in patients with NAFLD. However, serum TSH levels were not statistically different between NAFLD and control group.
It is suggested that Non-Alcoholic Fatty Liver Disease (NAFLD), which underlies diseases such as increasing obesity and insulin resistance, may be associated with thyroid dysfunction.14–17 Despite the physiological mechanism that appears to underlie NAFLD development, it is still unknown how thyroid dysfunction and the metabolic syndrome are related to NAFLD. Thyroid hormones play a critical role in regulating metabolism, particularly lipid metabolism in the liver. The patients with subclinical and clinical hypothyroidism have a considerably increased chance of developing NAFLD than people with euthyroidism. Patients with hypothyroidism have elevated triglyceride and LDL cholesterol levels due to decreased plasma lipoprotein lipase activity. According to these mechanism, fatty accumulation and cellular oxidative stress might be associated with the development of NAFLD.18 In another study, it was discovered that people with euthyroidism had considerably greater FT3 and lower FT4 levels, which increased their chance of developing NAFLD.19 Liu et al was showed that the development of NAFLD and FT3, TSH levels were found to be correlated, whereas FT4 levels were not20 Also in the other studies showed that the FT3/FT4 ratio, HOMA-IR, uric acid and waist circumference width are both as risk factors for the onset of NAFLD.21,22 Significantly different from these studies, in our study NASH was diagnosed histopathologically. Moreover, we investigated only euthyroid patients with NASH. Therefore, patient selection is one of the strongest aspect of our study and provided a more accurate interpretation of the results.
Some researchers have shown that TH and THR agonist therapies effectively lowered serum levels of triglycerides and free fatty acids and decreased the stage of hepatic stetaosis.23–25 Levothyroxine treatment is effective in terms of lowering liver enzymes and hepatic fat content by thyroid receptor in individuals with hypothyroidism and NAFLD.26 It is interesting to note that this effect was also seen in people who were euthyroid in a study on animals.27 This study differs from other studies by demonstrating that NAFLD is a treatable and reversible condition with a specific therapeutic intervention.28,29 Even while TSH and TH levels were within the normal range in NAFLD patients with the disease verified by biopsy, the NAFLD group in our study had considerably lower FT4 and FT3 values. The most significant finding of our study is that, despite normal TSH levels, lower FT3 and FT4 may be related with fatty liver. In addition, it may be inferred that TH and TRH agonists can be utilized to treat hepatic steatosis, and it would be beneficial to check not just TSH but also FT3 and FT4 levels when monitoring people with NAFLD and hypothyroidism.
Our study has some limitations. This study includes only living donor candidates who had moderate-severe steatosis on who underwent liver biopsies. This might not be representative of the general population with NAFLD. Secondly, it is a retrospective study.
Conclusion
Low levels of serum FT3 and FT4 might be a risk factor for liver steatosis in euthyroid patients with NAFLD. Clinicians may concentrate on the involvement of thyroid functions in the development of liver fibrosis from fatty liver disease. In the future, the relationship between thyroid disease and fatty liver can be more clearly revealed with prospective studies involving a larger number of patients.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
We would like to thank the Department of Internal Medicine at Demiroğlu Science University, our former institution, for its contributions.
Author Contributions
AO: Methodology, Validation, Funding acquisition, Writing – review and editing
BCT: Resources, Supervision, Project Administration, Methodology
EA: Methodology
TS: Investigation, Writing – original draft
EK: Software
FT: Conceptualization, Formal analysis, Project Administration, Writing – original draft. All authors took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that there is no conflicts of interest in this study.
References
1. Buzzetti E, Pinzani M, Tsochatzis EA. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism. 2016;65(8):1038–7. doi:10.1016/j.metabol.2015.12.012
2. Contos MJ, Choudhury J, Mills AS, et al. The histologic spectrum of nonalcoholic fatty liver disease. Clin Liver Dis. 2004;8(3):481–500. doi:10.1016/j.cld.2004.04.013
3. Angulo P. GI epidemiology: nonalcoholic fatty liver disease. Aliment Pharmacol Ther. 2007;25(8):883–889. doi:10.1111/j.1365-2036.2007.03246.x
4. Day CP. Non-alcoholic fatty liver disease: a massive problem. Clin Med. 2011;2:176–178.
5. Oral A, Solmaz I, Koca N, et al. Obesity-related disorders in türkiye: a multi center, retrospective, cross-sectional analysis from the OBREDI-TR study. J Clin Med. 2025;14(8):2680. doi:10.3390/jcm14082680
6. Şahintürk Y, Köker G, Koca N, et al. Metabolic dysfunction-associated fatty liver disease and fibrosis status in patients with type 2 diabetes treated at internal medicine clinics: türkiye DAHUDER Awareness of Fatty Liver Disease (TR-DAFLD) Study. Turk J Gastroenterol. 2024;35(8):643–650. doi:10.5152/tjg.2024.24045
7. Asrih M, Jornayvaz FR. Metabolic syndrome and nonalcoholic fatty liver disease: is insulin resistance the link? Mol Cell Endocrinol. 2015;418:55–65. doi:10.1016/j.mce.2015.02.018
8. Mullur R, Liu YY, Brent GA. Thyroid hormone regulation of metabolism. Physiol Rev. 2014;94(2):355–382. doi:10.1152/physrev.00030.2013
9. Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010;304(12):1365–1374. doi:10.1001/jama.2010.1361
10. Amarapurkar D, Kamani P, Patel N, et al. Prevalence of non-alcoholic fatty liver disease: population based study. Ann Hepatol. 2007;6(3):161–163. doi:10.1016/S1665-2681(19)31922-2
11. Ghamari-Langroudi M, Vella KR, Srisai D, et al. Regulation of thyrotropin-releasing hormone-expressing neurons in paraventricular nucleus of the hypothalamus by signals of adiposity. Mol Endocrinol. 2010;24(12):2366–2381. doi:10.1210/me.2010-0203
12. Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313–1321. doi:10.1002/hep.20701
13. Vasques AC, Rosado LE, Alfenas RD, Geloneze B. Análise crítica do uso dos índices do Homeostasis Model Assessment (HOMA) na avaliação da resistência à insulina e capacidade funcional das células-beta pancreáticas [Critical analysis on the use of the homeostasis model assessment (HOMA) indexes in the evaluation of the insulin resistance and the pancreatic beta cells functional capacity]. Arq Bras Endocrinol Metabol. 2008;1:32–39. Portuguese.
14. White DL, Kanwal F, El-Serag HB. Association between nonalcoholic fatty liver disease and risk for hepatocellular cancer, based on systematic review. Clin Gastroenterol Hepatol. 2012;10(12):1342–1359. doi:10.1016/j.cgh.2012.10.001
15. Fabbrini E, Sullivan S, Klein S. Obesity and nonalcoholic fatty liver disease: biochemical, metabolic, and clinical implications. Hepatology. 2010;51(2):679–689. doi:10.1002/hep.23280
16. Baffy G, Brunt EM, Caldwell SH. Hepatocellular carcinoma in non-alcoholic fatty liver disease: an emerging menace. J Hepatol. 2012;56(6):1384–1391. doi:10.1016/j.jhep.2011.10.027
17. Chung GE, Kim D, Kim W, et al. Non-alcoholic fatty liver disease across the spectrum of hypothyroidism. J Hepatol. 2012;57(1):150–156. doi:10.1016/j.jhep.2012.02.027
18. Bano A, Chaker L, Plompen EP, et al. Thyroid function and the risk of nonalcoholic fatty liver disease: the rotterdam study. J Clin Endocrinol Metab. 2016;101(8):3204–3211. doi:10.1210/jc.2016-1300
19. Van den Berg EH, van Tienhoven-Wind LJ, Amini M, et al. Higher free triiodothyronine is associated with non-alcoholic fatty liver disease in euthyroid subjects: the Lifelines Cohort Study. Metabolism. 2017;67:62–71. doi:10.1016/j.metabol.2016.11.002
20. Liu Y, Wang W, Yu X, et al. Thyroid function and risk of non-alcoholic fatty liver disease in euthyroid subjects. Ann Hepatol. 2018;17(5):779–788. doi:10.5604/01.3001.0012.3136
21. Gökmen FY, Ahbab S, Ataoğlu, et al. FT3/FT4 ratio predicts non-alcoholic fatty liver disease independent of metabolic parameters in patients with euthyroidism and hypothyroidism. Clinics. 2016;71(4):221–225. doi:10.6061/clinics/2016(04)08
22. Huang YY, Gusdon AM, Qu S. Cross-talk between the thyroid and liver: a new target for nonalcoholic fatty liver disease treatment. World J Gastroenterol. 2013;19(45):8238–8246. doi:10.3748/wjg.v19.i45.8238
23. Motomura K, Brent GA. Mechanisms of thyroid hormone action. Implications for the clinical manifestation of thyrotoxicosis. Endocrinol Metab Clin North Am. 1998;27(1):1–23. doi:10.1016/S0889-8529(05)70294-2
24. Perra A, Simbula G, Simbula M, et al. Thyroid hormone (T3) and TRbeta agonist GC-1 inhibit/reverse nonalcoholic fatty liver in rats. FASEB J. 2008;22(8):2981–2989. doi:10.1096/fj.08-108464
25. Cable EE, Finn PD, Stebbins JW, et al. Reduction of hepatic steatosis in rats and mice after treatment with a liver-targeted thyroid hormone receptor agonist. Hepatology. 2009;49(2):407–417. doi:10.1002/hep.22572
26. Liu L, Yu Y, Zhao M, et al. Benefits of levothyroxine replacement therapy on nonalcoholic fatty liver disease in subclinical hypothyroidism patients. Int J Endocrinol. 2017;2017:5753039. doi:10.1155/2017/5753039
27. Bruinstroop E, Dalan R, Cao Y, et al. Low-dose levothyroxine reduces intrahepatic lipid content in patients with type 2 diabetes mellitus and NAFLD. J Clin Endocrinol Metab. 2018;103(7):2698–2706. doi:10.1210/jc.2018-00475
28. Türker F, Oral A, Şahin T, et al. Does the FT3-to-FT4 ratio easily predict the progression of NAFLD and NASH cirrhosis? J Int Med Res. 2021;49(11):03000605211056841. doi:10.1177/03000605211056841
29. Oral A, Sahin T, Turker F, et al. Relationship between serum uric acid levels and nonalcoholic fatty liver disease in non-obese patients. Medicina. 2019;55(9):
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pro-Neurotensin as a Potential Novel Diagnostic Biomarker for Detection of Nonalcoholic Fatty Liver Disease
Mohamed AA, Abo-Elmatty DM, Ezzat O, Mesbah NM, Ali NS, Abd El Fatah AS, Alsayed E, Hamada M, Hassnine AA, Abd-Elsalam S, Abdelghani A, Hassan MB, Fattah SA
Diabetes, Metabolic Syndrome and Obesity 2022, 15:1935-1943
Published Date: 22 June 2022