Back to Journals » Nature and Science of Sleep » Volume 18

Association Between Work Stress and Sleep Disorders in Law Enforcement: A Systematic Review and Meta-Analysis
Received 16 February 2026
Accepted for publication 28 April 2026
Published 15 May 2026 Volume 2026:18 601666
DOI https://doi.org/10.2147/NSS.S601666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Huaihan Yang, Shuchen Tang
People’s Public Security University of China, Beijing, People’s Republic of China
Correspondence: Shuchen Tang, Email [email protected]
Background: Law enforcement personnel face diverse occupational stressors, including shift work, organizational pressure, operational demands, and traumatic incidents. Previous systematic reviews have primarily focused on prevalence estimates of sleep disturbances, whereas the strength of the association with occupational stress and the relative contribution of distinct stressor domains remain to be systematically quantified.
Methods: This systematic review and meta-analysis followed PRISMA 2020 guidelines and was registered with PROSPERO (CRD420261284369). Four databases (PubMed, Cochrane Library, Web of Science, and SpringerLink) were searched from inception to January 2026. Observational studies using validated instruments to assess occupational stress and sleep outcomes were included. A random-effects model was used to pool odds ratios (ORs). Subgroup analyses distinguished three stressor domains: shift work, work and organizational stress, and dual stress exposure.
Results: Seventeen studies were included in the qualitative synthesis, of which ten (N = 5124) provided data for meta-analysis. Occupational stress was significantly associated with sleep disorders (pooled OR = 3.51, 95% CI: 2.54– 4.84), with moderate to substantial heterogeneity (I2 = 69%). Subgroup analyses showed that shift work (OR = 3.02), work and organizational stress (OR = 5.94), and dual stress exposure (OR = 3.66) were each associated with elevated sleep risk, with no significant subgroup difference (P = 0.19). The dual stress exposure subgroup exhibited high heterogeneity (I2 = 87%), possibly attributable to differences in measurement tools, study populations, and confounder adjustment.
Conclusion: This study provides a quantitative estimate of the association between occupational stress and sleep disorders in law enforcement personnel. Differentiating occupational stress into distinct stressor domains may help clarify its relationship with sleep, with different stressors potentially operating through distinct pathways (eg, circadian disruption, cognitive rumination, hyperarousal). Methodologically, the study highlights issues in measurement standardization and confounder adjustment. From an intervention perspective, organizational-level strategies—such as enhancing decision-making autonomy and supportive leadership—may warrant further exploration alongside individual-level approaches. Safeguarding sleep health in this population is important for both individual well-being and public safety.
Keywords: police officers, work stress, sleep disorders, occupational health, meta-analysis, shift work
Introduction
Occupational stress is a pervasive determinant of psychological and physical morbidity in contemporary work settings, and law enforcement officers represent a particularly high-risk occupational group.1 The role of law enforcement officers entails a distinctive constellation of demands: officers must sustain high-intensity operational workloads (eg, rotating shifts, night duty, and prolonged on-call periods) while repeatedly confronting critical and potentially traumatic incidents, such as exposure to severe injury, death, or violent crime scenes.2 These occupational characteristics make law enforcement officers uniquely susceptible to the cumulative adverse consequences of work-related stressors.
Sleep is a fundamental homeostatic process that supports physiological recovery, emotional regulation, and cognitive performance. Growing evidence indicates that occupational stressors are strongly linked to sleep disturbance and that sleep disorders are more prevalent among law enforcement officers than in the general population. For example, the Buffalo Cardio-Metabolic Occupational Police Stress (BCOPS) study reported that officers working night shifts had significantly poorer sleep quality, as assessed by the Pittsburgh Sleep Quality Index (PSQI), and more than a threefold higher risk of excessive daytime sleepiness, measured by the Epworth Sleepiness Scale (ESS), compared with day-shift officers.3 Moreover, perceived stress has been consistently associated with poorer sleep outcomes, suggesting a dose–response pattern in which higher stress levels correspond to a greater likelihood of sleep pathology.
In recent decades, the conceptualization of occupational stress has undergone substantial development, with theoretical frameworks becoming increasingly refined. The Job Demands–Resources (JD-R) model4 and the Conservation of Resources (COR) theory5 represent two of the most influential perspectives in occupational health psychology, offering critical insights into the relationship between work-related stress and health outcomes. The JD-R model posits that any occupation encompasses two fundamental dimensions: job demands and job resources. Job demands—such as workload, emotional demands, and time pressure—consume individuals’ physical and psychological energy, whereas job resources—including autonomy, social support, and feedback—help buffer the impact of demands and foster work engagement. When job demands persistently exceed available resources, stress responses and adverse health outcomes may ensue. The COR theory further emphasizes that individuals are inherently motivated to acquire, maintain, and protect resources they value; stress arises from actual or threatened resource loss, and chronic resource depletion constitutes a core mechanism underlying exhaustion, depression, and physical illness. Collectively, these two theoretical frameworks indicate that occupational stress is not a unidimensional construct but rather a dynamic process involving the interplay between multiple job demands and resources, the effects of which depend on the nature of stressors, their duration, and the availability of coping resources.
In the context of law enforcement, occupational stress exhibits a distinctly multidimensional character that defies conceptualization as a homogeneous construct. Existing research has identified at least four categories of stressors that are particularly salient among police officers: organizational stressors (eg, rigid hierarchical structures, administrative burden, lack of supervisory support, limited promotion opportunities), operational stressors (eg, high-stakes decision-making, shift duties, exposure to violence), trauma-related stressors (eg, direct exposure to or witnessing of death, severe injury, violent crimes), and scheduling-related stressors (eg, night shifts, rotating shifts, extended duty hours). Different stressor domains may influence sleep through distinct psychobiological pathways: scheduling-related stress operates primarily via circadian disruption that disturbs the sleep–wake cycle; trauma exposure exerts its effects mainly through hyperarousal and intrusive re-experiencing that interfere with sleep initiation and maintenance; and organizational stress may contribute to chronic insomnia via cognitive rumination and sustained vigilance. Failure to differentiate among these stressor domains risks obscuring important mechanistic differences and constrains the development of targeted interventions. Previous systematic reviews on sleep problems in police officers6 have largely focused on prevalence estimates without systematically distinguishing stressor types or examining whether the strength of association with sleep disorders varies across stressor domains. Consequently, the relative contribution of each stressor domain to sleep disturbances remains poorly quantified, hindering the formulation of mechanism-informed occupational health strategies and limiting the precision of interventions aimed at specific sources of occupational stress.
To address this gap, a systematic integration and quantitative synthesis of existing data are needed. Meta-analysis can increase statistical power, reconcile inconsistencies across studies, and provide more precise estimates of association. Therefore, the present study systematically reviews and meta-analyzes the association between law enforcement work stressors—including workload and scheduling demands, traumatic exposure,7 and perceived stress—and sleep disorders. Drawing on the Conservation of Resources Theory, which posits that stress arises from actual or threatened resource loss across multiple domains, we propose that different stressor types may converge on sleep disturbances through distinct resource depletion pathways. In this meta-analysis, we categorize the included studies into three stressor domains: (1) shift work, representing primarily circadian disruption and physiological resource depletion; (2) work and organizational stress, capturing organizational and operational pressures that predominantly deplete psychological and social resources; and (3) dual stress exposure, encompassing studies that explicitly combined traumatic exposure with occupational stress, reflecting a compounded resource loss across multiple domains. This categorization allows us to quantify the association for each domain while acknowledging their conceptual distinctness within a unified theoretical framework.
Materials and Methods
Protocol and Registration
This systematic review and meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement.8 The protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration No. CRD420261284369).
Search Strategy
A comprehensive literature search was conducted in four electronic databases: PubMed, the Cochrane Library, Web of Science and SpringerLink. Searches were performed from database inception to January 2026. No language restrictions were applied.
The search strategy combined controlled vocabulary terms (eg, MeSH/Emtree) and free-text keywords covering three core domains: (1) the target population (eg, “police”, “policeman”, “law enforcement”, “correctional officer”), (2) work-related stressors/exposures (eg, “occupational stress”, “work stress”, “burnout”, “organizational stress”, “operational stress”, “trauma exposure”, “shift work”, “night shift”, “rotating shift”), and (3) sleep outcomes (eg, “sleep disorder”, “sleep disturbance”, “sleep quality”, “insomnia”, “excessive daytime sleepiness”, “obstructive sleep apnea”, “shift work disorder”). Boolean operators (AND/OR) were used to combine terms. The detailed search strategies for each database are provided in Supplementary Material 1.
Eligibility Criteria
Population
Adult (≥18 years) active-duty law enforcement personnel, including police officers, patrol officers, traffic police, criminal investigators, SWAT personnel, and correctional/prison officers. For studies with mixed occupational samples, eligibility was restricted to: (a) studies comprising 100% law enforcement participants; (b) studies in which law enforcement personnel constituted ≥50% of the sample; or (c) studies reporting extractable subgroup data specifically for law enforcement participants.
Exposure
Quantitative assessment of law enforcement work-related stressors, including (i) perceived/organizational/operational stress assessed using validated scales (eg, Operational Police Stress Questionnaire [PSQ-Op], Perceived Stress Scale [PSS]); and/or (ii) objective job characteristics reflecting occupational strain (eg, night shift/rotating shift exposure, shift frequency, on-call duty, or quantified traumatic/critical incident exposure). In addition to validated psychometric questionnaires, objective exposure measures—particularly shift work—are recognized as well-validated occupational stressors in their own right. From an occupational health perspective, shift work disrupts circadian rhythms and triggers a sustained physiological stress response (eg, elevated cortisol and sympathetic activation) that operates independently of subjective perception.9,10 Studies using such objective measures (eg, Charles et al, 2007) were therefore included to capture a broader spectrum of occupational stress beyond self-report, thereby enhancing the comprehensiveness of our synthesis.
Comparator
Comparisons between higher versus lower exposure to work stressors (eg, high vs. low perceived stress categories) or, for scheduling-related exposures, night/rotating shift versus day/fixed shift, as defined in the original studies.
Outcome
Sleep-related outcomes assessed using validated subjective instruments with established thresholds (eg, PSQI > 5, ISI ≥ 15, ESS ≥ 10, Berlin Questionnaire, Athens Insomnia Scale ≥ 6) and/or objective assessments (eg, polysomnography [PSG], actigraphy). Outcomes could include insomnia, poor sleep quality, excessive daytime sleepiness, obstructive sleep apnea (OSA), or other clinically relevant sleep disturbances.
Study Design
Observational studies, including cross-sectional, cohort (prospective or retrospective), and case-control designs.
Exclusion Criteria
Studies were excluded if they: (1) had a total sample size <20; (2) did not focus on occupational/work-related stressors (eg, exclusively domestic or non-work stress); (3) reported sleep outcomes only qualitatively or without extractable quantitative data; (4) were non-original publications (reviews, editorials, case reports) or conference abstracts without full data; or (5) lacked sufficient data for effect size calculation and could not be derived from the reported information.
Study Selection
All records retrieved from the databases were imported into a reference management system, and duplicates were removed. Two investigators independently screened titles and abstracts, followed by full-text assessment of potentially eligible articles.
To quantify inter-reviewer agreement, we employed Cohen’s kappa coefficient for statistical evaluation. Specifically, during the title/abstract screening phase, the kappa value between the two reviewers was 0.74 (95% CI: 0.70–0.78), indicating a “high level of agreement”. In the full-text screening phase, the kappa value reached 0.76 (95% CI: 0.68–0.88), demonstrating similarly high consistency. During the data extraction phase, the assessment of key variables (such as sample size information) yielded a kappa of 0.79 (95% CI: 0.75–0.83), further validating the reliability of the data extraction process. All discrepancies were resolved through consensus discussions or adjudicated by a third reviewer.
Data Extraction and Effect Size Handling
Two investigators independently extracted data using a standardized form. Extracted variables included: first author, publication year, country/region, study design, sample size, participant characteristics, exposure definition and measurement tool, sleep outcome definition and measurement instrument, effect estimates, and covariates included in adjusted models (if available).
The primary effect measure was the odds ratio (OR). When studies reported ORs (crude or adjusted), these were extracted directly. When ORs were not provided but sufficient raw data were available (eg, 2×2 tables or event counts by exposure category), unadjusted ORs and 95% confidence intervals (CIs) were calculated. If a study reported only continuous sleep outcomes (eg, mean PSQI without a dichotomized threshold) and the information was insufficient to derive an OR, the study was not included in the OR-based quantitative synthesis and was summarized narratively.
For each included study, the primary effect estimate was extracted according to a predefined hierarchical selection rule to ensure transparency and consistency. When multiple eligible estimates were available (eg, different stress measures, different sleep outcomes, or models with varying degrees of covariate adjustment), the following prioritization was applied: (1) the estimate that most closely aligned with the prespecified exposure–outcome definition; (2) the most fully adjusted model; (3) for studies reporting multiple stress measures, the estimate based on the most comprehensive stress construct; (4) for studies reporting multiple sleep outcomes, the estimate for poor sleep quality (PSQI > 5) was prioritized. In the present meta-analysis, all ten included studies provided only a single eligible effect estimate that met the prespecified criteria; therefore, no additional selection was required. Nevertheless, to assess the robustness of the pooled estimate against potential selection bias, sensitivity analyses were conducted as described below.
Risk of Bias Assessment
The methodological quality of the included studies was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional Studies.11 This instrument comprises eight items that evaluate the following aspects: (1) clarity of inclusion criteria; (2) description of study participants and setting; (3) measurement of exposure; (4) measurement of outcomes; (5) use of objective criteria for measurement; (6) identification of confounding factors; (7) strategies employed to address confounding; and (8) appropriateness of statistical analysis. For each item, the study was rated as “Yes” (criterion met), “No” (criterion not met), or “Unclear” (insufficient information). A total score was calculated for each study based on the number of items meeting the criteria, with higher scores indicating superior methodological quality. The quality assessment was conducted independently by two reviewers; any discrepancies were resolved through discussion or consultation with a third reviewer.
Statistical Analysis
Meta-analyses were conducted using Review Manager (RevMan) version 5.4 and Stata version 18.0. Effect estimates were pooled as ORs with corresponding 95% CIs. For pooling, ORs were analyzed on the logarithmic scale and combined using the inverse-variance method.
Statistical heterogeneity was assessed using Cochran’s Q (χ2) test and the I2 statistic. Significant heterogeneity was defined as a Q-test P value <0.10 and/or I2 >50%. Given anticipated clinical and methodological diversity (eg, differences in occupational settings, stress measures, and outcome definitions), a random-effects model (DerSimonian–Laird method)12 was used as the primary approach.
Preplanned subgroup analyses were performed to explore potential sources of heterogeneity by categorizing studies into: (1) Shift work–related stressors, focusing primarily on rotating shifts, night shifts, or shift schedule exposure; (2) Work and Organizational Stressors, capturing combined organizational and operational stress. (3) Dual stress exposure stressors, focusing on the combined impact of traumatic exposure and occupational/organizational stress. Between-subgroup differences were examined using a χ2-test for subgroup differences where applicable.
The categorization of studies into three stressor domains was guided by the Conservation of Resources Theory and the Job Demands–Control Model, with the aim of distinguishing stressor types that may operate through different resource depletion pathways.
Sensitivity analyses were conducted using a leave-one-out approach to evaluate the robustness of pooled estimates and identify influential studies. Publication bias was assessed by visual inspection of funnel plots and by Begg’s rank correlation test13 and Egger’s linear regression test14 (performed when ≥10 studies were available). A two-tailed P value <0.05 was considered statistically significant for all analyses except the heterogeneity Q test.
Evidence Assessment
We employed the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework15 to assess the quality of evidence for each primary outcome. All included cross-sectional studies were initially assigned a baseline rating of “low” evidence. Subsequently, we performed downgrading across five domains: risk of bias, indirectness, inconsistency, imprecision, and publication bias. Given that our analysis primarily relied on self-reported data and exhibited moderate to substantial heterogeneity, the final GRADE assessment results are presented in Table 1.
 |
Table 1 GRADE Assessment of the Evidence Quality |
Results
Study Selection
The initial systematic search across the four electronic databases yielded a total of 1762 records. After removing duplicates, 899 unique records remained for title and abstract screening. Of these, 620 were excluded as they did not meet the inclusion criteria, leaving 279 full-text articles for detailed eligibility assessment. After retrieval, 238 reports could not be obtained, and the remaining 41 full-text articles were assessed for eligibility. Following a rigorous review, 17 studies were included for qualitative synthesis.3,6,16–30 Among these, 10 independent studies provided sufficient quantitative data to be included in the final meta-analysis (Figure 1).
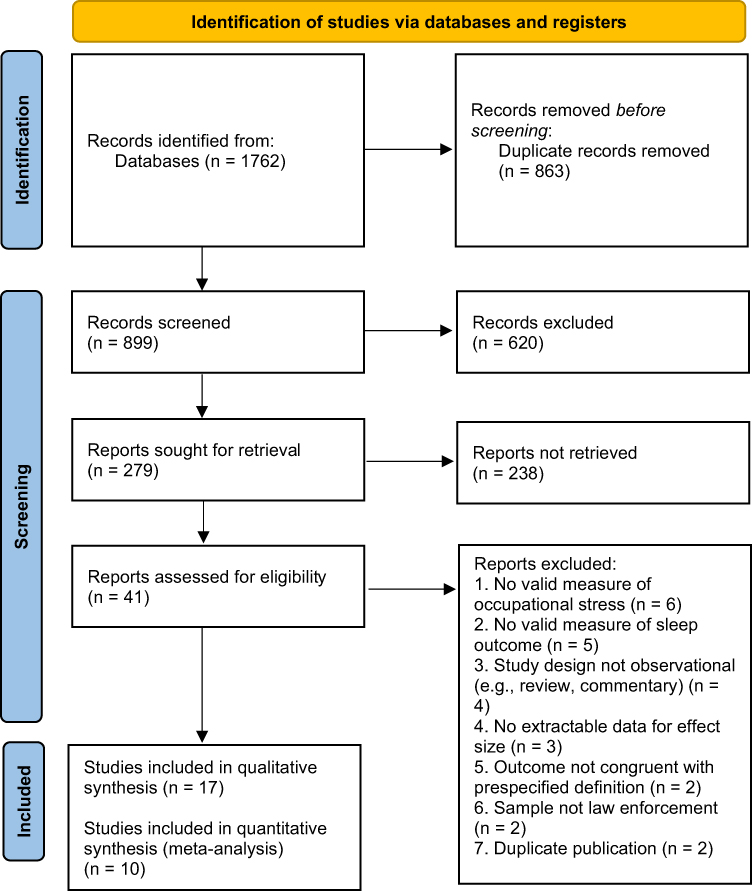 |
Figure 1 PRISMA 2020 flow diagram of the literature search and study selection process. Records were identified from four databases (PubMed, Cochrane Library, Web of Science, and SpringerLink). After duplicate removal and screening, 17 studies were included in the qualitative synthesis, of which 10 provided sufficient data for meta-analysis. Reasons for full-text exclusion are listed. |
Characteristics of Included Studies
Table 2 summarizes the main characteristics of the included studies. Sample sizes ranged from 20 to 733 participants. The studies were conducted predominantly in the United States (n = 9), followed by Italy (n = 2), Brazil (n = 2), China (n = 1), and other countries (n = 3). Most studies adopted a cross-sectional design, and one study used a prospective cohort design. Work stress was assessed using validated questionnaires and/or job-related indicators (eg, shift schedules or exposure to operational/traumatic events). Overall methodological quality is evaluated with the Joanna Briggs Institute Critical Appraisal Checklist for Analytical Cross-Sectional Studies (JBI) (Table 3).
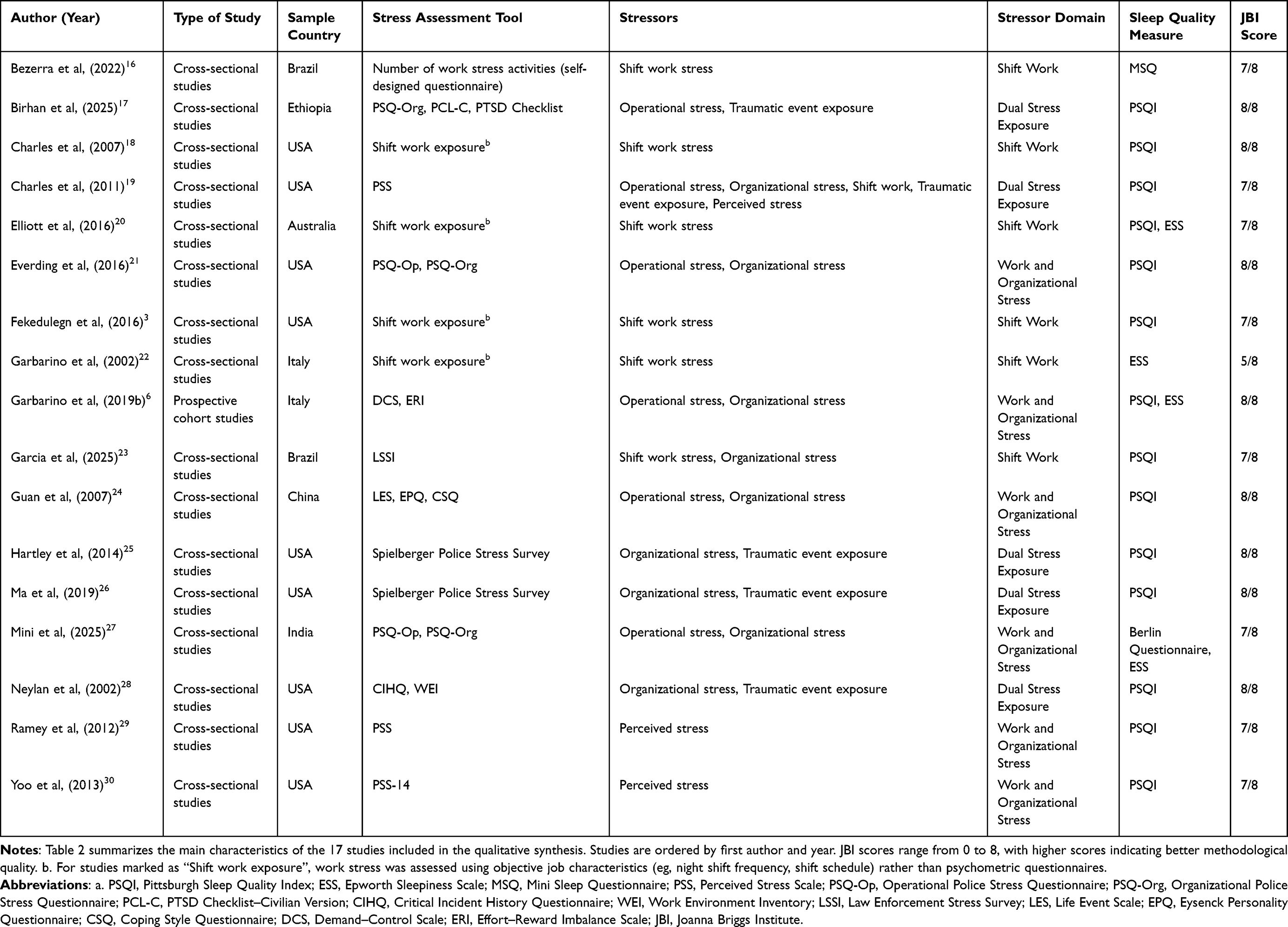 |
Table 2 Characteristics of the Included Studies |
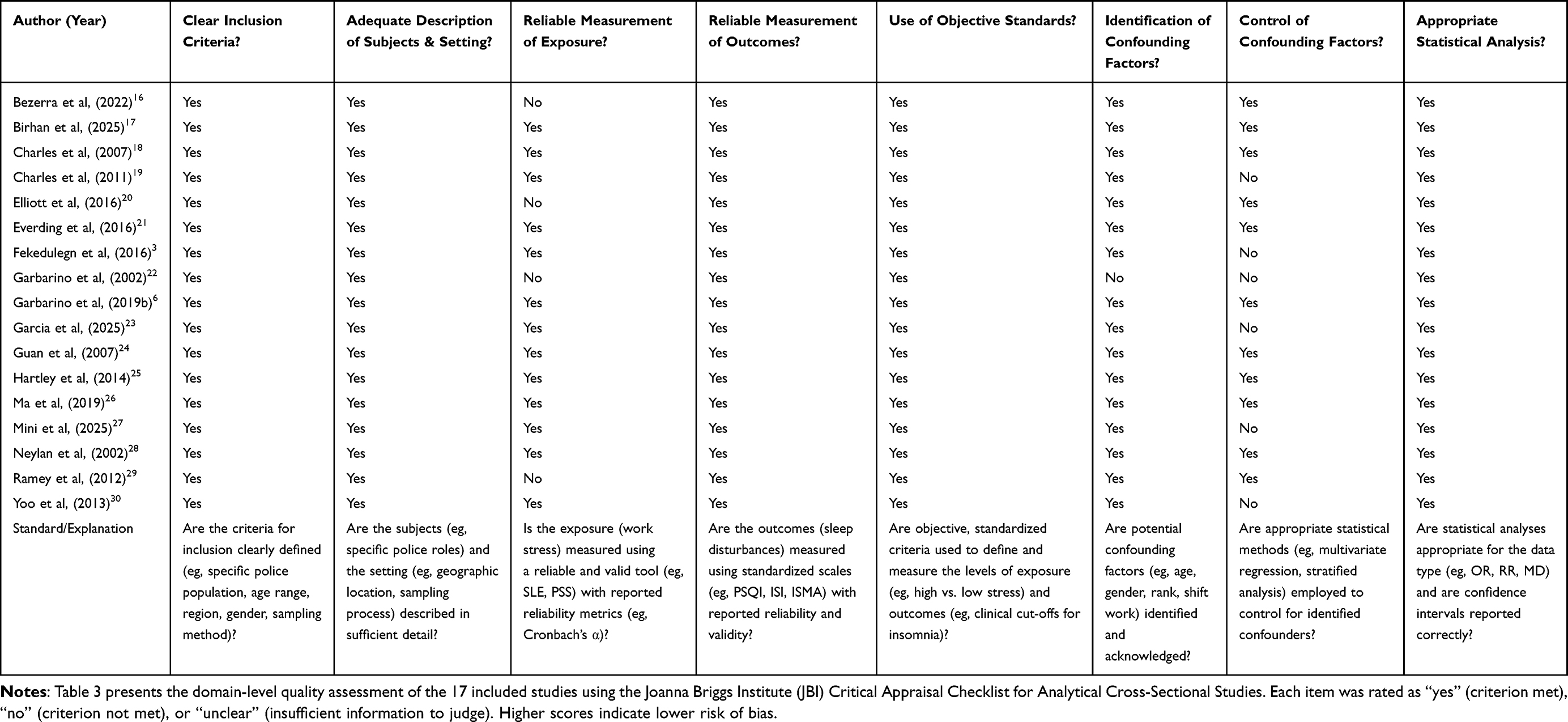 |
Table 3 JBI Critical Appraisal Checklist for Analytical Cross-Sectional Studies |
Association Between Work Stress and Sleep Disorders
Although 17 studies were included in the qualitative synthesis, 7 were excluded from the meta-analysis (Table 4) because the effect estimates could not be expressed as odds ratios (ORs) or could not be derived from the reported data (eg, continuous outcomes without dichotomous thresholds, insufficient extractable data, or reporting only P values). Therefore, 10 studies were included in the quantitative synthesis.
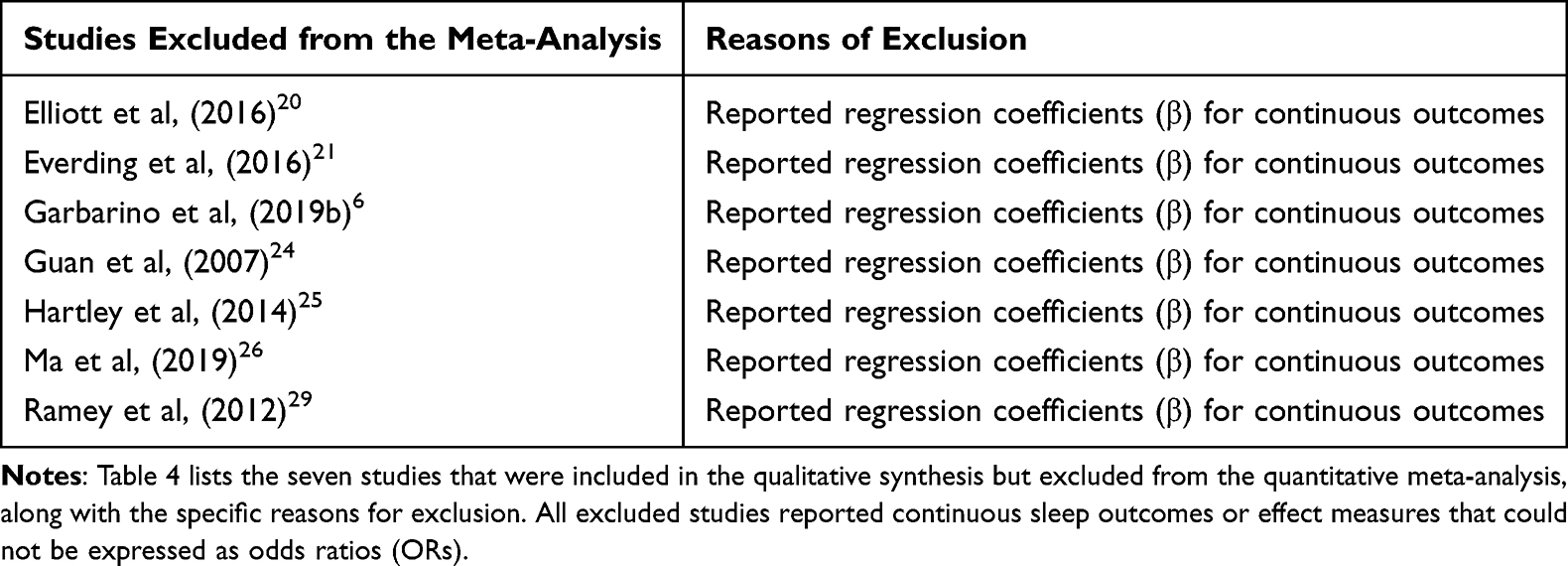 |
Table 4 Studies Excluded from the Meta-Analysis with Reasons for Exclusion |
Significant heterogeneity was observed (χ2 = 29.15, df = 9, P = 0.0006; I2 = 69%). Accordingly, a random-effects model was used to pool effect estimates. The meta-analysis showed a statistically significant association between higher work stress and sleep disorders among officers (pooled OR = 3.51, 95% CI: 2.54–4.84; Z = 7.66, P < 0.00001) (Figure 2). Individual study estimates ranged from OR = 1.86 to OR = 6.69, and all studies indicated an association in the same direction.
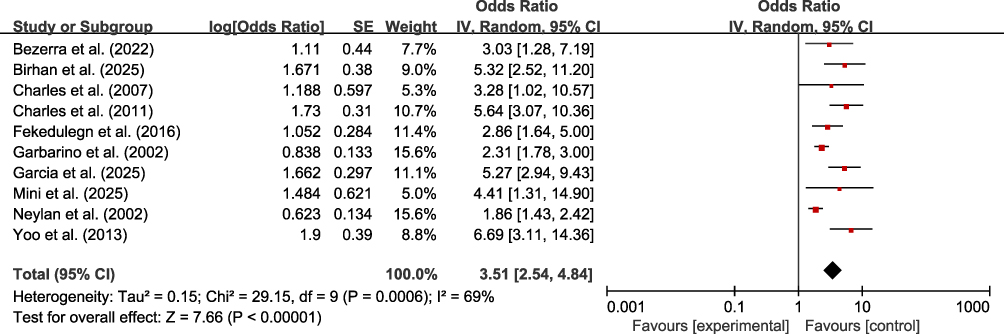 |
Figure 2 Forest plot of the association between occupational stress and sleep disorders. Squares represent study-specific odds ratios (ORs); horizontal lines represent 95% confidence intervals (CIs); the size of each square is proportional to the study weight. The diamond represents the pooled OR with its 95% CI. Heterogeneity: I2 = 69%. |
Among the studies excluded from the meta-analysis, seven primarily employed linear regression models, mean-difference analyses, or reported effect sizes without providing direct odds ratios (OR). A systematic review and appraisal of these works revealed a high degree of concordance with the directionality of the outcomes reported in the studies incorporated into the quantitative synthesis. Specifically, these excluded studies uniformly indicated a significant positive association between law enforcement occupational stress and deteriorating sleep quality, and they suggested that heightened occupational stress levels may lead to prolonged sleep latency and impaired daytime functioning. This observation further substantiates the robustness of our pooled estimate (OR = 3.51, 95% CI: 2.54–4.84, P < 0.00001), underscoring that it reflects a conservative and authentic synthesis of the extant evidence rather than a selective bias introduced by the exclusion criteria.
Sensitivity Analysis
A leave-one-out sensitivity analysis was performed to assess the robustness of the pooled estimate (Table 5). The pooled ORs ranged from 3.26 (excluding Yoo et al30) to 3.91 (excluding Neylan et al28). Notably, all leave-one-out pooled estimates remained within the 95% CI of the primary analysis, and all corresponding confidence intervals remained above 1.0, indicating that the overall association was stable.
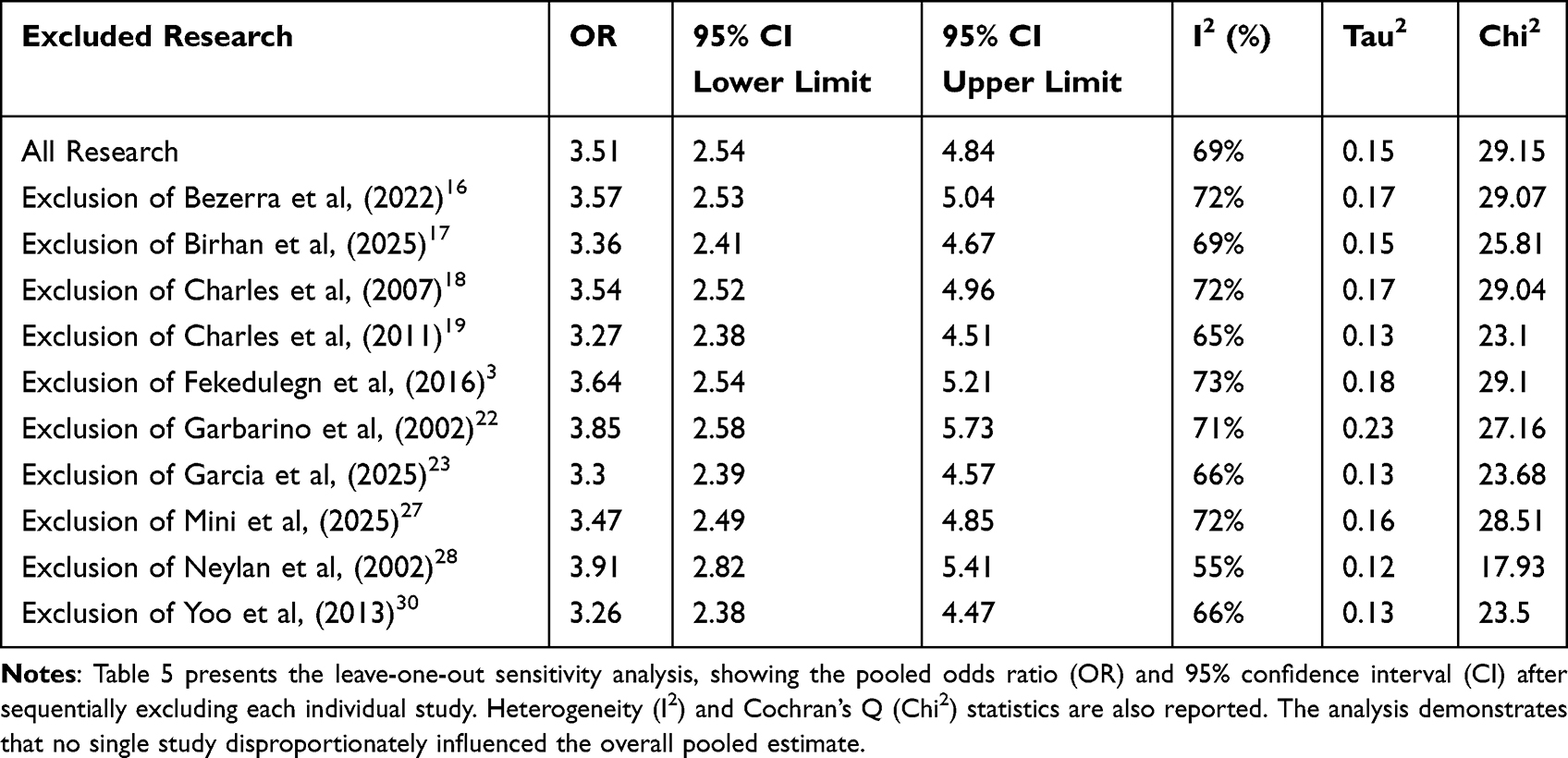 |
Table 5 Leave-One-Out Sensitivity Analysis |
Excluding Neylan et al28 and Yoo et al30 reduced heterogeneity (I2 to 55% and 66%, respectively), suggesting partial influence on between-study variability; however, heterogeneity remained moderate-to-high, and the direction of the association was unchanged.
To assess the impact of confounding factor adjustment on our findings, a secondary sensitivity analysis was performed. Specifically, four of the included studies had already accounted for at least one confounding factor (depression, anxiety, or PTSD). We systematically excluded each of the remaining six studies that did not adjust for these confounders, recalculating the pooled OR for each iteration (Table 6). The final analysis, after completely removing the non-adjusted studies, yielded a pooled OR of 2.91 (95% CI: 1.66–5.11). This OR is lower than the overall pooled OR derived from all ten studies (OR = 3.51), yet the confidence interval remains entirely above the null value of 1.
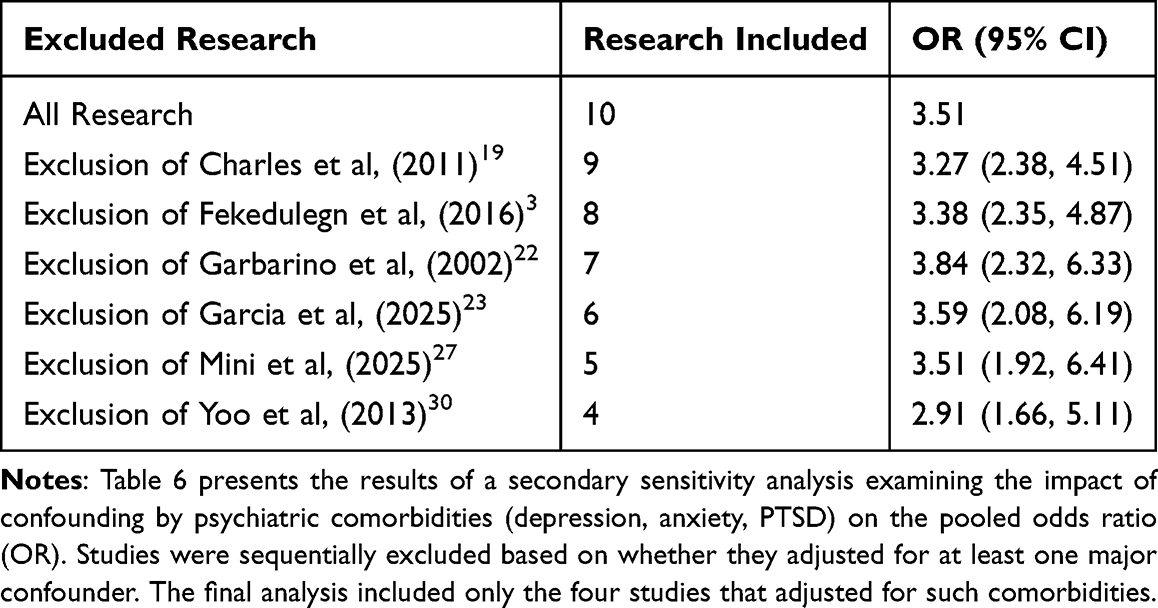 |
Table 6 Sensitivity Analysis by Adjustment for Psychiatric Comorbidities |
Publication Bias
Visual inspection of the funnel plot did not reveal obvious asymmetry (Figure 3). Begg’s rank correlation test did not provide evidence of publication bias (z = 1.17, P = 0.243), and Egger’s linear regression test did not reach statistical significance (P = 0.18). However, given the limited number of studies included in the meta-analysis (k = 10), the statistical power of these tests is inherently low; therefore, the findings of these tests should be interpreted with caution, and the possibility of publication bias cannot be entirely excluded.
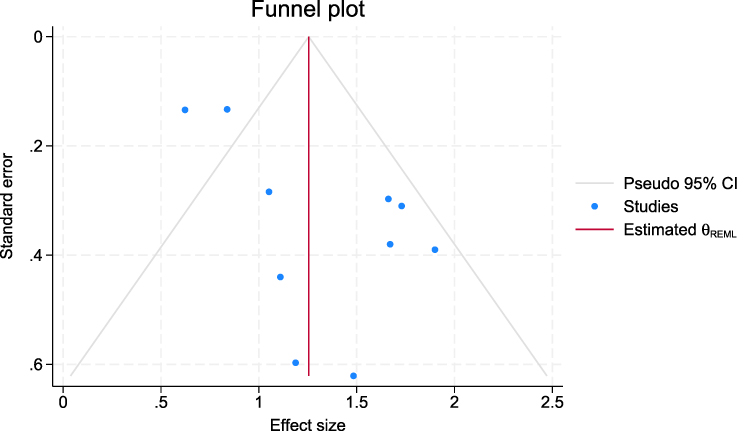 |
Figure 3 Funnel plot for publication bias assessment. Each point represents an individual study. The vertical line represents the pooled effect estimate from the random-effects model. Pseudo 95% confidence limits are shown as dashed curves. |
Subgroup Analysis
Based on the literature included in our review, we performed a dedicated subgroup analysis focusing on seven studies that specifically reported poor sleep quality (PSQI > 5) as the outcome. The results of this analysis are illustrated in Figure 4.
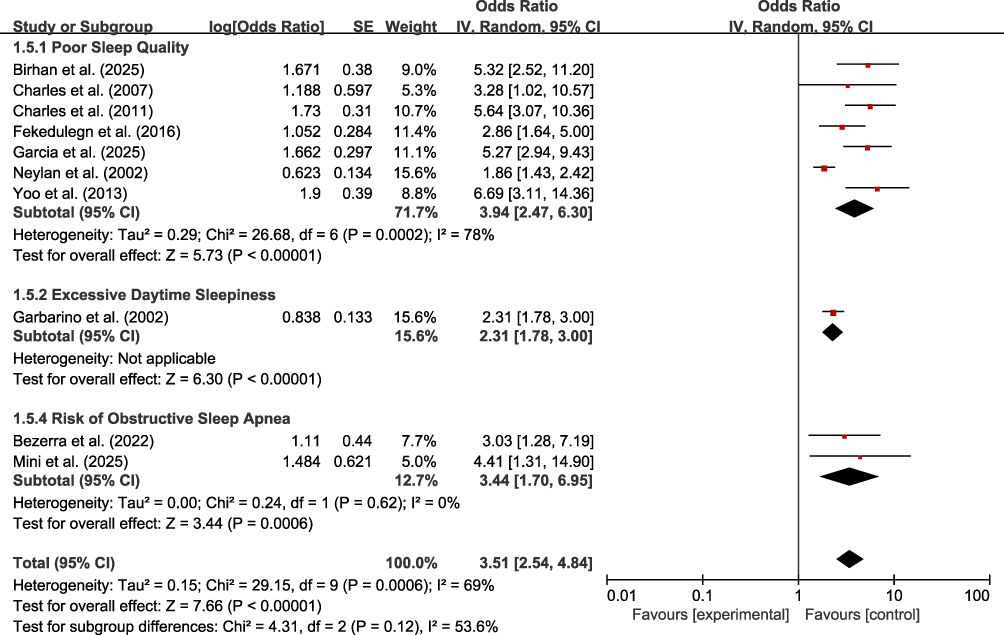 |
Figure 4 Subgroup analysis of sleep outcomes. Forest plot showing the association between occupational stress and specific sleep outcomes across three subgroups: poor sleep quality (PSQI > 5, 7 studies), excessive daytime sleepiness (ESS ≥ 10, 1 study), and risk of obstructive sleep apnea (Berlin Questionnaire, 2 studies). Squares represent study-specific ORs; horizontal lines represent 95% CIs; diamonds represent pooled estimates. |
Based on the forest plot, the pooled odds ratio for the seven studies that employed poor sleep quality (PSQI > 5) as the primary outcome was 3.94 (95% CI: 2.47–6.30; I2 = 78%).
However, due to the insufficient number of studies in the remaining subgroups, it was not feasible to conduct reliable subgroup analyses for those outcomes; consequently, only the effect estimates for these categories are reported. The pooled odds ratio for the excessive daytime sleepiness subgroup was 2.31, whereas the pooled odds ratio for the risk of obstructive sleep apnea subgroup was 3.44.
To explore whether associations differed by stressor type, subgroup analyses were conducted by classifying studies as three subgroups— “Shift Work”, “Work and Organizational Stress”, and “Dual Stress Exposure” (Figure 5).
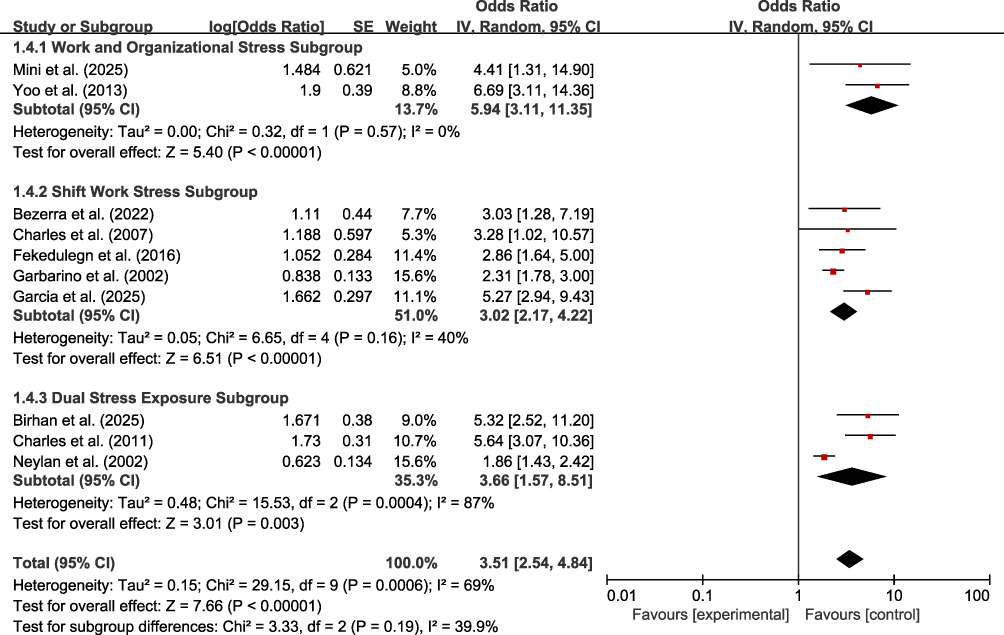 |
Figure 5 Subgroup analysis by stressor type. Forest plot showing three stressor domains: work and organizational stress, shift work stress, and dual stress exposure. Squares represent study-specific ORs; horizontal lines represent 95% CIs; diamonds represent pooled estimates. Heterogeneity (I2) is shown for each subgroup. Test for subgroup differences: χ2 = 3.33, df = 2, P = 0.19. |
The results of the random-effects model showed that the pooled effect size for the work and organizational stress subgroup (n = 2) yielded a pooled OR of 5.94 (95% CI: 3.11–11.35) with no evidence of heterogeneity (I2=0%, P=0.57). For the shift work stress subgroup (n = 5) yielded a pooled OR of 3.02 (95% CI: 2.17–4.22; I2 = 40%). For the dual stress exposure subgroup (n = 3) yielded a pooled OR of 3.66 (95% CI: 1.57–8.51; I2 = 87%). The test for subgroup differences was not statistically significant (χ2 = 3.33, P = 0.19), suggesting no clear statistical evidence that the magnitude of association differed between stressor types.
GRADE Assessment
We performed a GRADE assessment of the evidence quality for the primary outcomes of this study (Table 1). Overall, the evidence included in the meta-analysis is primarily derived from cross-sectional studies, which start at a low level of certainty. Adjustments were then made to the evidence rating for the association between occupational stress and sleep disorders. Specifically, the evidence quality was further downgraded due to substantial information bias (both stress and sleep quality were self-reported) and statistically significant heterogeneity (I2 = 69%). Consequently, the certainty of evidence for this outcome remains at a very low level. Although a statistically significant association was observed between law enforcement occupational stress and sleep disorders (OR = 3.51, 95% CI 2.54–4.84), the conclusions should be interpreted with caution given the limitations of the underlying evidence.
Discussion
Principal Findings
This systematic review and meta-analysis synthesizes evidence from 17 observational studies and provides quantitative confirmation of a strong association between occupational stress and sleep disorders among law enforcement officers.31 Officers reporting higher work stress had more than threefold higher odds of sleep disorders compared with those reporting lower stress (pooled OR = 3.51; 95% CI: 2.54–4.84). From an occupational health and public-safety perspective, this effect size is clinically meaningful, given the central role of adequate sleep in maintaining vigilance, decision-making, and emotional regulation in high-stakes law-enforcement settings.
In our sensitivity analysis, we sought to delineate the potential influence of confounding variables on the pooled effect estimate (OR). Specifically, among the ten included studies, only four had accounted for at least one major confounder (depression, anxiety, or PTSD). To more comprehensively assess the impact of unadjusted confounders, we systematically excluded the remaining six studies that lacked such adjustments. The subsequent analysis revealed that, after the complete removal of the unadjusted studies, the pooled OR decreased from the initial 3.51 to 2.91 (95% CI: 1.66–5.11). Nevertheless, the confidence interval remained entirely above the null value, indicating that the association between occupational stress and sleep disturbances remained statistically significant.
This finding offers a nuanced perspective on the relationship between occupational stress and sleep disturbances. The reduction in OR (approximately 83% of the original estimate) suggests that unadjusted confounders—particularly depression, anxiety, and PTSD—may have contributed to an upward bias in the initial OR, implying that a portion of the observed risk could be attributed to the comorbidity of these affective disorders. However, even after more stringent adjustment for these confounders, occupational stress continued to significantly elevate the risk of sleep disturbances (OR = 2.91). This suggests that the detrimental impact of occupational stress on sleep may not be solely mediated through the induction of affective disorders but may also involve other independent physiological or behavioral mechanisms.
Nevertheless, we acknowledge that the contribution of this meta-analysis is primarily confirmatory in nature. The findings reinforce what has long been suspected—that occupational stress is a major determinant of sleep health in policing—while providing more precise estimates and a clearer delineation of stressor domains. The conceptual advancement lies not in discovering a novel association, but in refining the specificity of that association and in underscoring the need for mechanism-informed, domain-sensitive interventions. We hope that this synthesis serves as a foundation for future research that moves beyond prevalence estimates and toward a deeper understanding of the causal pathways linking distinct stressor types to sleep pathology.
Comparison with Prior Literature
The overall magnitude of association observed in this meta-analysis (pooled OR = 3.51) is largely consistent with, yet extends, the extant body of research on sleep disturbances among law enforcement personnel. A systematic review and meta-analysis conducted by Garbarino et al32 reported a pooled prevalence of poor sleep quality among police officers at approximately 51%; however, this prior work did not directly quantify the strength of the relationship between occupational stress and sleep disorders. In contrast, the present study offers a direct estimate of this relationship, indicating that police officers exposed to higher levels of occupational stress have a more than threefold increased risk of developing sleep disorders compared to those experiencing lower stress.
Our subgroup analyses revealed numerical differences in pooled effect sizes across stress types; however, the between-group differences did not reach statistical significance (P = 0.19). The work and organizational stress subgroup (comprising two studies) yielded a pooled OR of 5.94, which is numerically the highest among the three subgroups. Nevertheless, due to the limited number of studies included in this subgroup, the stability of this estimate warrants further verification through additional research. The shift work subgroup (encompassing five studies) produced a pooled OR of 3.02, aligning with previous findings regarding the detrimental impact of circadian rhythm disruption on sleep. The dual stress exposure subgroup (comprising three studies) yielded a pooled OR of 3.66; however, this subgroup exhibited substantial heterogeneity (I2 = 87%), suggesting considerable variability in how “dual stress” was defined and measured across different studies.
Plausible Mechanisms: Circadian Misalignment and Sleep–Wake Dysregulation
Shift work is an inherent operational feature of law enforcement duties. Our subgroup analysis indicates that exposure to non-standard work schedules significantly increases the risk of sleep disorders (OR = 3.02; 95% CI: 2.17–4.22). The prevailing mechanistic explanation for this phenomenon is circadian misalignment: nocturnal and rotating shift work disrupts the temporal coordination between the sleep–wake cycle and endogenous biological rhythms, including melatonin secretion patterns and the homeostatic regulation of sleep pressure.33 This misalignment can manifest as prolonged sleep latency, fragmented sleep, reduced total sleep time, and a lack of restorative sleep, all of which can be captured by validated sleep scales such as the Pittsburgh Sleep Quality Index (PSQI).
Additionally, shift work in law enforcement often involves extended duty periods, unpredictable overtime, and insufficient recovery time between shifts. These factors may exacerbate the accumulation of sleep debt and impair the ability to achieve sustained sleep. Moreover, when officers attempt to revert to a daytime schedule on days off, they may experience “social jetlag”—a mismatch between biological and social time—further aggravating chronic sleep insufficiency. The aforementioned mechanisms provide biological plausibility for the association observed in the shift work subgroup and suggest that optimizing shift schedules is a potential intervention target.
Plausible Mechanisms: Cumulative Occupational Burden, Hyperarousal, and Organizational Context
The work and organizational stress subgroup (OR = 5.94; 95% CI: 3.11–11.35) and the dual stress exposure subgroup (OR = 3.66; 95% CI: 1.57–8.51) point to pathways that transcend mere circadian misalignment, aligning with cumulative or additive stress models. It is important to emphasize that, although the work and organizational stress subgroup showed a numerically higher effect size (5.94 vs. 3.66), the test for subgroup differences was not statistically significant (χ2=3.33, df=2, P=0.19), and the confidence intervals across subgroups exhibited considerable overlap. This numerical difference should be interpreted with caution, as it may reflect insufficient statistical power due to the limited number of studies within each subgroup, rather than a genuine difference in the effect of distinct stressor types on sleep disturbances. Indeed, when the number of studies in a subgroup is small, the pooled estimate may be disproportionately influenced by individual studies, and numerical fluctuations may represent sampling variation rather than true effect heterogeneity. Accordingly, the subgroup analyses presented here should be regarded as exploratory. Their value lies in suggesting directional patterns across stressor domains, rather than providing definitive conclusions regarding the relative magnitude of effects across stress types. Any inferences drawn from numerical differences between subgroups should be made with caution and await validation in future studies with larger sample sizes.
In the dual stress exposure subgroup, trauma-related hyperarousal may be particularly salient.34 Repeated exposure to traumatic events (eg, violence, fatalities, severe injuries) can induce sustained physiological arousal and intrusive cognitive–emotional processing, both of which are detrimental to sleep initiation and maintenance. Dysregulation of stress response systems—including persistent activation of the hypothalamic–pituitary–adrenal axis and hyperactivity of sympathetic pathways—may contribute to insomnia symptoms, nightmares, and fragmented sleep.35
The organizational and operational stressors captured within the work and organizational stress subgroup also warrant consideration. Stressors such as perceived lack of supervisory support, rigid hierarchical structures, excessive administrative burden, staffing shortages, and limited decision latitude may generate persistent low-level stress that extends beyond the immediate impact of acute incidents. This chronic stress may sustain cognitive rumination and anticipatory anxiety,36 creating a vicious cycle: diminished sleep quality further impairs coping capacity and stress tolerance, which in turn exacerbates sleep disturbances. Collectively, these mechanisms provide both biological and psychological plausibility for the observed associations across stress types and underscore the necessity of intervention strategies that extend beyond merely adjusting work schedules.
Theoretical Perspectives
The mechanisms discussed above provide biological and psychological explanations for the observed associations between distinct stressor types and sleep disturbances. However, situating the findings of the present study within broader theoretical frameworks in occupational stress and organizational research can further deepen our understanding of their academic significance and reveal the deeper structural determinants underlying sleep problems in law enforcement populations.
Within the field of occupational health psychology, the Job Demands–Control Model stands37 as one of the most influential theoretical frameworks. This model posits that occupational stress arises from the interaction between job demands and job control: the combination of high demands and low control—termed “high-strain jobs”—is most likely to result in psychological strain and adverse health outcomes. This framework has direct applicability to law enforcement contexts. Law enforcement officers routinely face exceptionally high operational demands, including rapid decision-making under pressure, exposure to violence, and management of unpredictable critical incidents. Concurrently, however, they often possess limited control over organizational aspects of their work, such as shift scheduling, task allocation, and resource deployment. This mismatch—high demands coupled with low control—may represent a core mechanism through which organizational stressors exert a particularly potent influence on sleep. The elevated effect size observed in the work and organizational stress subgroup (OR = 5.94) may, in part, reflect the operation of this theoretical mechanism. For a comprehensive review of the JD-R model’s evolution and applications, see Bakker and Demerouti.38
Another closely related and highly relevant framework is the Effort–Reward Imbalance Model.39 This model emphasizes that sustained stress responses arise when individuals perceive a chronic imbalance between the effort they expend and the rewards they receive—rewards that encompass not only financial compensation but also esteem, recognition, and career opportunities. In policing, such imbalances are particularly salient. Officers endure high-intensity, high-risk workloads, yet frequently encounter limited promotion opportunities, inadequate organizational recognition, and insufficient supervisory support.40 This perceived inequity may persistently activate stress response systems, thereby disrupting sleep initiation and maintenance. The strong association observed between organizational stressors and sleep disturbances in the present study can be meaningfully interpreted through the lens of this model.
Furthermore, the more recent Conservation of Resources Theory5 originally proposed by Hobfoll41 offers valuable insights for interpreting the current findings. This theory posits that individuals are inherently motivated to acquire, protect, and sustain resources they value, and that stress results from actual or threatened resource loss. Chronic resource depletion—whether of physical resources (eg, energy), psychological resources (eg, self-efficacy), or social resources (eg, organizational support)—constitutes a core mechanism underlying mental and physical health deterioration. Among law enforcement officers, organizational stressors (such as lack of supervisory support and excessive administrative burden) may persistently deplete coping resources, while trauma exposure may simultaneously erode both psychological and social resources. As resource depletion accumulates, sleep—a fundamental physiological process for recovery—may be among the first functions to be compromised.
In summary, interpreting the results of this meta-analysis through these established theoretical frameworks not only deepens our understanding of the mechanisms linking occupational stress to sleep disturbances but, more importantly, illuminates the deeper structural roots of sleep problems in law enforcement populations. These theoretical perspectives suggest that interventions aimed at improving sleep health among officers should extend beyond individual-level approaches (eg, stress management training) or simple schedule modifications. Rather, they point to the necessity of systematic organizational-level changes—including enhancing decision-making autonomy, fostering supportive leadership, ensuring fairness in effort–reward balance, and cultivating an organizational culture that prioritizes resource preservation. Such structural interventions hold the potential to address the root causes of occupational stress, shifting the focus from symptom management toward root-cause mitigation.
Heterogeneity, Subgroup Findings, and Methodological Considerations
The overall analysis of this meta-analysis revealed moderate to high heterogeneity (I2 = 69%), which was anticipated given the variability across studies on multiple dimensions. Firstly, the definitions and measurement tools for stress differed, encompassing perceived stress scales, operational law enforcement stress scales, objective shift exposure data, and trauma-stress composite measurements. Secondly, there were discrepancies in sleep outcomes and diagnostic thresholds, including poor sleep quality (PSQI > 5), excessive daytime sleepiness (ESS ≥ 10), and obstructive sleep apnea screening (Berlin Questionnaire). Thirdly, the background of law enforcement work—encompassing organizational structures, shift systems, and trauma exposure—varied significantly across different countries and agencies. Fourthly, strategies for adjusting confounders were inconsistent; some studies only controlled for demographic and lifestyle factors, while others did not account for potential confounders such as depression and PTSD.
It is noteworthy that the degree of heterogeneity varied markedly across subgroups. The work and organizational stress subgroup exhibited zero heterogeneity (I2 = 0%). The absence of heterogeneity in this subgroup is primarily attributable to the limited number of studies (n=2) rather than a high degree of concordance between studies; therefore, interpretations of this subgroup’s results should be approached with caution. The shift work stress subgroup displayed moderate heterogeneity (I2 = 40%), suggesting that shift work, as an objectively defined stress exposure, yields relatively consistent effect estimates across studies.
In contrast, the dual stress exposure subgroup exhibited high heterogeneity (I2 = 87%) and the sources of this residual heterogeneity warrant further exploration. First, differences in stress measurement tools represent an important source of heterogeneity. The three studies included in this subgroup demonstrated considerable variability in the operationalization of “dual stress”. Neylan et al28 used the Critical Incident History Questionnaire (CIHQ) and the Work Environment Inventory (WEI) to measure traumatic exposure and routine work stress, respectively. Birhan et al17 employed the PTSD Checklist–Civilian Version (PCL-C) in combination with the Organizational Police Stress Questionnaire (PSQ-Org) for a composite assessment. Charles et al19 while exploring the modifying role of depressive symptoms in stratified analyses did not include traumatic exposure as an independent exposure variable. Such heterogeneity in measurement instruments and conceptual frameworks may contribute to genuine differences in effect sizes across studies. Second, differences in study populations and contexts cannot be overlooked: Neylan et al28 studied urban police officers in the United States and Canada, whereas Birhan et al17 focused on law enforcement personnel in Ethiopia. The nature, frequency, and intensity of traumatic events and organizational stressors may vary systematically across cultural contexts. Third, inconsistencies in confounder adjustment also merit attention: although all three studies adjusted for mental health variables to some extent, the specific variables and methods of adjustment differed (eg, some adjusted only for depression, while others adjusted for both PTSD and depression), which may also contribute to variation in effect estimates. This heterogeneity may also reflect the absence of a widely accepted theoretical operationalization of “dual stress” within the framework of resource depletion, underscoring the need for future research to develop standardized, theory-driven measures that capture the compounded resource loss associated with combined trauma and occupational stress.
Given the high heterogeneity in this subgroup and the diversity of its sources, the interpretation of the pooled effect size for this subgroup should be approached with caution. Although the pooled OR of 3.66 (95% CI: 1.57–8.51) was statistically significant, its confidence interval was wide, and the point estimate may be substantially influenced by the aforementioned sources of heterogeneity. From a methodological perspective, quantitatively synthesizing studies with considerable differences in study design, measurement instruments, and population characteristics into a single subgroup yields limited robustness of the findings. Therefore, the present subgroup analysis should be regarded as exploratory rather than confirmatory. Its primary value lies in suggesting that “dual exposure to trauma and occupational stress” may represent a distinct risk domain warranting further attention, rather than in providing a precise effect estimate. Future research should strive to standardize the operational definition of dual stress, adopt validated measurement tools, and examine its association with sleep disturbances across diverse cultural contexts.
Sensitivity analyses indicated that the overall effect size remained robust regardless of the analytical approach—whether through a leave-one-out analysis that sequentially removed individual studies or by excluding studies that did not adjust for mental health comorbidities. When studies lacking such adjustments were excluded, the pooled OR decreased from 3.51 to 2.91, suggesting that insufficient control for comorbid mental health conditions such as depression, anxiety, or PTSD may lead to an overestimation of the effect size. Nonetheless, even after excluding these studies, the confidence interval of the pooled OR remained entirely above 1, affirming the persistent association between occupational stress and sleep disorders.
Directionality of Causality and the Necessity for Longitudinal Studies
The studies included in this meta-analysis were predominantly cross-sectional in design, fundamentally limiting the reliability of causal inferences. The conceptual model underlying this research typically assumes occupational stress as a precursor to sleep disorders; however, the possibility of reverse causality is equally plausible: chronic sleep deprivation may impair emotional regulation, exacerbate threat perception, and intensify stress perception, thereby establishing a bidirectional relationship. Moreover, cross-sectional designs cannot ascertain the temporal sequence between exposure and outcome, nor do they rule out the influence of unmeasured common causes (eg, genetic susceptibility, pre-existing mental health conditions) that may simultaneously affect stress perception and sleep disorders.
Importantly, the relationship between occupational stress and sleep is likely dynamic and reciprocal rather than unidirectional. Longitudinal evidence supports this bidirectional perspective.42 Sleep disturbances may reduce an individual’s capacity to cope with workplace demands, leading to heightened stress perception and further sleep deterioration. This bidirectional perspective aligns with transactional models of stress,43 which emphasize the continuous interplay between environmental demands and individual coping resources. From this vantage point, interventions targeting either stress or sleep may have cascading effects on the other, suggesting that integrated approaches addressing both domains simultaneously may be more effective than single-domain interventions.
Nonetheless, some of the included literature provided prospective evidence, offering limited support for the temporal directionality wherein stress leads to sleep deterioration. For instance, the prospective cohort study by Garbarino and Magnavita6 found that sleep problems could predict stress-related metabolic changes in law enforcement personnel, suggesting a dynamic interaction between stress and sleep rather than a unidirectional causality.
Future research should prioritize adequately powered prospective cohort studies that repeatedly measure occupational stress (including objective indicators such as shift systems and trauma exposure) and sleep outcomes (including actigraphy or polysomnography). Such study designs would facilitate the elucidation of causal directionality, the identification of critical temporal windows (eg, early versus late career stages), and the evaluation of potential mediators (eg, PTSD symptoms, rumination, coping strategies, metabolic dysregulation). Additionally, given that the sensitivity analyses in this study indicated a significant impact of controlling for mental health comorbidities on effect size, future research should systematically adjust for depression, PTSD, and related confounding factors to more accurately isolate the direct effect of occupational stress on sleep.
Strengths and Limitations
Strengths of this study include protocol registration, PRISMA-concordant methods, comprehensive multi-database searching, explicit eligibility criteria, quality assessment, and extensive robustness checks (subgroup and sensitivity analyses, publication bias assessment). The analysis also offers practical value by distinguishing, albeit imperfectly, between scheduling-related and broader occupational stressor domains.
Limitations should be acknowledged. First, the predominance of cross-sectional designs constrains causal inference and may be affected by reverse causality. Second, many studies relied on self-reported measures for both exposure and outcome, which may introduce common-method variance and reporting biases. Third, residual confounding remains likely; not all studies adjusted for key factors such as depressive symptoms, PTSD-related symptoms, alcohol/caffeine use, body mass index, or comorbid medical conditions that may influence sleep. Fourth, the operationalization of “work stress” varied widely, and our three-category subgrouping (shift work, work and organizational stress, and dual stress exposure) may mask more specific stressor effects. Fifth, the present sensitivity analysis, which aimed to exclude the influence of confounding factors, is inherently limited by the heterogeneity in confounding adjustment across the included literature. Specifically, while the ten cross-sectional studies incorporated in this meta-analysis offer valuable cross-sectional insights into the field, there is an evident imbalance in the control of confounders: only four studies adjusted for at least one major confounder (depression, anxiety, or PTSD), and these adjustments were predominantly limited to single variables. Consequently, the pooled odds ratio (OR = 3.51) derived from the full set of studies may not have fully accounted for the independent effects of depression, anxiety, and PTSD on sleep disturbances, thereby introducing a potential upward bias. The pooled OR of 2.91 obtained after excluding studies that did not adjust for these confounders should therefore be interpreted with caution. Finally, a “healthy worker effect”44,45 may lead to underestimation if officers with severe stress and sleep disturbances leave active duty and are therefore underrepresented in study samples.
Certainty of Evidence
According to the GRADE assessment, the overall certainty of evidence in this study is deemed very low. This rating is primarily constrained by several critical limitations. First, both the exposure (occupational stress) and the outcome (sleep disorder) were measured using self-reported questionnaires, which may introduce information bias. Second, there is substantial heterogeneity among the included studies (I2 = 69%), potentially arising from variations in geographic locations, law enforcement subpopulations, or measurement instruments. Moreover, several studies provided insufficient adjustment for confounding variables such as age and gender. Despite these limitations, the observed association (OR = 3.51) remains epidemiologically suggestive, indicating that occupational stress may be an important risk factor for sleep disorders among law enforcement officers. Future research should focus on prospective cohort studies and interventional trials to validate these findings.
Conclusion
This systematic review and meta-analysis of 17 observational studies provides the first quantitative synthesis of the association between occupational stress and sleep disorders in law enforcement populations. Officers exposed to higher work-related stress had more than threefold higher odds of sleep disturbances (pooled OR = 3.51; 95% CI: 2.54–4.84). Subgroup analyses revealed that shift work, work and organizational stress, and dual stress exposure were each independently associated with elevated sleep risk, suggesting that sleep disturbances in policing may reflect a multi-domain occupational burden.
Conceptually, the study advances the field by deconstructing occupational stress into distinguishable domains—each potentially operating through distinct mechanisms (circadian disruption, cognitive rumination, hyperarousal)—thereby aligning with established frameworks such as the Job Demands–Control Model and the Effort–Reward Imbalance Model. This differentiation suggests that targeted, domain-sensitive interventions may hold greater promise than one-size-fits-all approaches.
Methodologically, substantial heterogeneity—particularly within the dual stress exposure subgroup (I2 = 87%)—highlights current gaps in measurement standardization. Future research may benefit from validated, uniform measures across stress domains and sleep outcomes to enhance comparability.
Regarding causal inference, the predominance of cross-sectional designs limits conclusions about directionality. A bidirectional relationship is plausible, as sleep loss may impair stress tolerance, potentially perpetuating a vicious cycle. Prospective cohort studies with repeated measures and objective assessments (eg, actigraphy, cortisol) could help disentangle these pathways.
From an intervention perspective, individual-level stress management or schedule modifications alone may not fully address observed sleep disturbances. Organizational-level structural interventions—such as enhancing decision-making autonomy, fostering supportive leadership, and ensuring effort–reward fairness—warrant consideration as complementary strategies. Law enforcement personnel shoulder the important responsibility of maintaining social order and protecting public safety, and their sleep health, which is closely related to their work efficiency, physical and mental state and public security service quality, has become more crucial with the increasing number of new types of crimes putting higher demands on their work intensity.
Data Sharing Statement
The datasets generated and analyzed in the present study are available from the corresponding author upon reasonable request.
Author Contributions
H.-Y. (Huaihan Yang): Conceptualization, Methodology, Software, Validation, Investigation, Formal Analysis, Data Curation, Writing – Original Draft, Visualization. S.-T. (Shuchen Tang): Validation, Project Administration, Data Curation, Writing – Review & Editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The paper is supported by the Fundamental Research Funds for the Central Universities for “Research on New Types of Crimes and Their Investigation Theories”(2026JKF02SK21). The funders did not play any role in study design, data collection and analysis, decision to publish, or paper preparation.
Disclosure
The authors declare no potential conflicts of interest regarding the research, authorship, or publication of this article.
References
1. Violanti JM, Fekedulegn D, Andrew ME, et al. Shift work and the incidence of injury among police officers. Am J Ind Med. 2012;55:217–21. doi:10.1002/ajim.22007
2. Bond J, Hartley TA, Sarkisian K, et al. Association of traumatic police event exposure with sleep quality and quantity in the BCOPS study cohort. Int J Emerg Ment Health. 2013;15(4):255–265.
3. Fekedulegn D, Burchfiel CM, Charles LE, Hartley TA, Andrew ME, Violanti JM. Shift work and sleep quality among urban police officers: the BCOPS study. J Occup Environ Med. 2016;58(3):e66–e71. doi:10.1097/JOM.0000000000000620
4. Demerouti E, Bakker AB, Nachreiner F, Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. 2001;86(3):499–512. doi:10.1037/0021-9010.86.3.499
5. Hobfoll SE. The influence of culture, community, and the nested-self in the stress process: advancing conservation of resources theory. Appl Psychol. 2001;50:337–421. doi:10.1111/1464-0597.00062
6. Garbarino S, Magnavita N. Sleep problems are a strong predictor of stress-related metabolic changes in police officers. A prospective study. PLoS One. 2019b;14(10):e0224259. doi:10.1371/journal.pone.0224259
7. Chopko BA, Palmieri PA, Adams RE. Trauma-related sleep problems and associated health outcomes in police officers: a path analysis. J Interpers Violence. 2021;36(5–6):NP2725–NP2748. doi:10.1177/0886260518767912
8. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:372. doi:10.1186/s13643-021-01626-4.
9. Åkerstedt T. Shift work and disturbed sleep/wakefulness. Occup Med. 2003;53(2):89–94. doi:10.1093/occmed/kqg046
10. Puttonen S, Härmä M, Hublin C. Shift work and cardiovascular disease: pathways from circadian stress to morbidity. Scand J Work Environ Health. 2010;36(2):96–108. doi:10.5271/sjweh.2894
11. Joanna Briggs Institute. Critical appraisal tools: checklist for analytical cross sectional studies. 2017. Available from: http://joannabriggs.org/research/critical-appraisal-tools.html.
12. DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled Clin Trials. 1986;7(3):177–188. doi:10.1016/0197-2456(86)90046-2
13. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50:1088–1101. doi:10.2307/2533446
14. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
15. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
16. Bezerra GL, Carvalho FM, Fernandes RDC, Santos KOB. Sleep disorders in correctional officers: cross-sectional study. Sleep Sci. 2022;15(1):34–40. doi:10.5935/1984-0063.20210027
17. Birhan Z, Addisu F, Ergetie T, et al. Sleep quality and associated factors among police officers in Northwest Ethiopia: a cross-sectional study. Sleep Sci Pract. 2025;9(1):8. doi:10.1186/s41606-025-00126-x
18. Charles LE, Burchfiel CM, Fekedulegn D, et al. Shift work and sleep: the Buffalo Police health study. Policing. 2007;30(2):215–227. doi:10.1108/13639510710753225
19. Charles LE, Slaven JE, Mnatsakanova A, et al. Association of perceived stress with sleep duration and sleep quality in police officers. Int J Emerg Ment Health. 2011;13(4):229–224.
20. Elliott JL, Lal S. Blood pressure, sleep quality and fatigue in shift working police officers: effects of a twelve hour roster system on cardiovascular and sleep health. Int J Environ Res Public Health. 2016;13(2):172. doi:10.3390/ijerph13020172
21. Everding B, Hallam JE, Kohut ML, Lee DC, Anderson AA, Franke WD. Association of sleep quality with cardiovascular disease risk and mental health in law enforcement officers. J Occup Environ Med. 2016;58(8):e281–e286. doi:10.1097/JOM.0000000000000814
22. Garbarino S, Nobili L, Beelke M, Balestra V, Cordelli A, Ferrillo F. Sleep disorders and daytime sleepiness in state police shiftworkers. Arch Environ Health. 2002;57(2):167–173. doi:10.1080/00039890209602932
23. Garcia LOR, Moreira R, Silva MRG. Occupational stress and sleep of military police officers from Rio de Janeiro, Brazil. Am J Hum Biol. 2025;37(1):e24184. doi:10.1002/ajhb.24184
24. Guan N, Zhang J, Wang X, Gan Z, Chen M. The relationship between sleep quality and psychosocial factors among prison police officers. Chin J Clin Psychol. 2007;15(2):93–98. doi:10.16128/j.cnki.1005-3611.2007.04.029
25. Hartley TA, Violanti JM, Sarkisian K, et al. Association between police-specific stressors and sleep quality: influence of coping and depressive symptoms. J Law Enforce Leadership Ethics. 2014;1(1):31–48.
26. Ma CC, Hartley TA, Sarkisian K, et al. Influence of work characteristics on the association between police stress and sleep quality. Saf Health Work. 2019;10(1):30–38. doi:10.1016/j.shaw.2018.07.004
27. Mini GK, Sangeeth KS, Gopika GB, et al. Sleep apnea and daytime sleepiness in police officers from Kerala, India. BMC Public Health. 2025;25(1):2119. doi:10.1186/s12889-025-23292-0
28. Neylan TC, Metzler TJ, Best SR, et al. Critical incident exposure and sleep quality in police officers. Psychosom Med. 2002;64(2):345–352. doi:10.1097/00006842-200203000-00019
29. Ramey SL, Perkhounkova Y, Moon M, Budde L, Tseng HC, Clark MK. The effect of work shift and sleep duration on various aspects of police officers’ health. Workplace Health Saf. 2012;60(5):215–222. doi:10.1177/216507991206000505
30. Yoo H, Franke WD. Sleep habits, mental health, and the metabolic syndrome in law enforcement officers. J Occup Environ Med. 2013;55(1):99–103. doi:10.1097/JOM.0b013e31826e294c
31. Mao Y, Raju G, Zabidi MA. Association between occupational stress and sleep quality: a systematic review. Nat Sci Sleep. 2023;15:931–947. doi:10.2147/NSS.S431442
32. Garbarino S, Guglielmi O, Puntoni M, Bragazzi NL, Magnavita N. Sleep quality among police officers: implications and insights from a systematic review and meta-analysis of the literature. Int J Environ Res Public Health. 2019a;16(5):885. doi:10.3390/ijerph16050885
33. Boivin DB, Boudreau P. Impacts of shift work on sleep and circadian rhythms. Pathol Biol. 2014;62(5):292–301. doi:10.1016/j.patbio.2014.08.001
34. Lavie P. Sleep disturbances in the wake of traumatic events. N Engl J Med. 2001;345(25):1825–1832. doi:10.1056/NEJMra012893
35. Germain A. Sleep disturbances as the hallmark of PTSD: where are we now? Am J Psychiatry. 2013;170(4):372–382. doi:10.1176/appi.ajp.2012.12040432
36. Brosschot JF, Gerin W, Thayer JF. The perseverative cognition hypothesis: a review of worry, prolonged stress-related physiological activation, and health. J Psychosom Res. 2006;60(2):113–124. doi:10.1016/j.jpsychores.2005.06.074
37. Karasek RA. Job demands, job decision latitude, and mental strain: implications for job redesign. Adm Sci Q. 1979;24(2):285–308. doi:10.2307/2392498
38. Bakker AB, Demerouti E. Job demands–resources theory: taking stock and looking forward. J Occup Health Psychol. 2017;22(3):273–285. doi:10.1037/ocp0000056
39. Siegrist J. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol. 1996;1(1):27–41. doi:10.1037/1076-8998.1.1.27
40. Acquadro Maran D, Magnavita N, Garbarino S. Identifying organizational stressors that could be a source of discomfort in police officers: a thematic review. Int J Environ Res Public Health. 2022;19(6):3720. doi:10.3390/ijerph19063720
41. Hobfoll SE. Conservation of resources: a new attempt at conceptualizing stress. Am Psychol. 1989;44(3):513–524. doi:10.1037/0003-066X.44.3.513
42. Akerstedt T, Kecklund G, Axelsson J. Impaired sleep after bedtime stress and worries. Biol Psychol. 2007;76(3):170–173. doi:10.1016/j.biopsycho.2007.07.010
43. Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York: Springer; 1984.
44. McMichael AJ. Standardized mortality ratios and the “healthy worker effect”: scratching beneath the surface. J Occup Med. 1976;18(3):165–168.
45. Shah D. Healthy worker effect phenomenon. Indian J Occup Environ Med. 2009;13(2):77–79. doi:10.4103/0019-5278.55123
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.