Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Association Between Visceral Adipose Tissue and Chronic Respiratory Diseases: A Two-Sample Multivariable Mendelian Randomization Study in European Population
Authors Huang JX, Xiao BJ, Yan YX, Xie W, Feng LY, Liu XM ![]()
Received 21 December 2024
Accepted for publication 22 March 2025
Published 2 April 2025 Volume 2025:20 Pages 919—928
DOI https://doi.org/10.2147/COPD.S510828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Jin-Xian Huang,1 Bing-Jie Xiao,2 Yu-Xin Yan,1 Wei Xie,1 Le-Yi Feng,1 Xue-Mei Liu3
1The Fourth Clinical Medicine College, Guangzhou University of Chinese Medicine, Shenzhen, People’s Republic of China; 2The Second Clinical Medicine College, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 3Department of Endocrinology, Shenzhen Traditional Chinese Medicine Hospital, Shenzhen, People’s Republic of China
Correspondence: Xue-Mei Liu, Email [email protected]
Background: The relationship between obesity and some respiratory diseases has been well documented. However there have been few studies on the association between visceral adipose tissue (VAT) and chronic respiratory diseases (CRDs), it remains unclear whether VAT is causally associated with CRDs.
Methods: We used two-sample Mendelian randomization (MR) to illuminate the effects of VAT on four CRDs: chronic obstructive pulmonary disease (COPD), allergic asthma, interstitial lung disease (ILD), and sarcoidosis. Inverse variance weighted (IVW) served as the primary assessment method. MR Egger, weighted median, Simple mode and Weighted mode were the supplementary methods for MR analysis. We used multivariate MR analysis to adjust for the effect of body mass index (BMI) on outcomes, Egger intercept, MR-pleiotropy residual sum and outlier, and leave-one-out analysis to confirm the MR results’ consistency.
Results: Genetically-predicted VAT was associated with an increased risk of COPD (OR = 1.56; 95% CI: 1.34– 1.82; P = 1.16× 10− 8), allergic asthma (OR = 1.44; 95% CI: 1.20– 1.73; P = 8.63× 10− 5), and ILD (OR = 1.15; 95% CI: 1.04– 1.26; P = 4.62× 10− 3). However, there was limited evidence to support an association between VAT and sarcoidosis. In multivariate MR analysis, VAT’s associations with COPD, allergic asthma, and ILD persisted after adjusting for BMI.
Conclusion: This study provides evidence for a potential causal relationship between VAT and COPD, allergic asthma, and ILD; these relationships were independent of the effect of BMI.
Keywords: visceral adipose tissue, chronic respiratory diseases, chronic obstructive pulmonary disease, allergic asthma, interstitial lung disease, Mendelian randomization
Introduction
Obesity is a risk factor for many chronic diseases,1 and is now a global health problem.2,3 Since 1990, the global prevalence of obesity has nearly tripled in men, and more than doubled in women.4 Traditionally, the definition of obesity is a body mass index (BMI) greater than or equal to 30 kg/m2.5 However, the harmful effects of abdominal obesity are becoming increasingly recognized. BMI is not an independent tool for identifying obesity-related complications, as fat distribution is a better predictor of obesity-related complications.6 Visceral adipose tissue (VAT) is a type of fat deposited around the abdominal organs.7 Excess VAT is probably more harmful than the accumulation of adipose tissue in other areas.8 Many clinical studies have shown that VAT is associated with diabetes, metabolic syndrome, hypertension, inflammatory bowel disease, cardiometabolic diseases, and other chronic diseases.9–12
Chronic respiratory disease (CRD) encompass a spectrum of pulmonary conditions affecting the airways and other structures of the lung, including chronic obstructive pulmonary disease (COPD), asthma, interstitial lung disease (ILD), sarcoidosis and pneumoconiosis. CRD has become a principal contributor to global morbidity and mortality, burdening the world’s health sustainability.13,14 In 2019, CRDs were the third leading cause of death responsible for 4 million deaths with a prevalence of 454.6 million cases globally and 77.6 million new global cases, marking a 49.0% increase in new cases since 1990.14 Studies have shown that CRD is associated with many risk factors, including environmental, occupational, behavioral and metabolic risks.14 Therefore, understanding the risk factors of CRD can help policymakers in developing and efficiently targeting risk modification interventions, which can result in reduced disability and premature mortality. For example, obesity has long been recognized as a risk factor for many respiratory diseases, such as bronchitis, COPD, asthma, and pneumonia.15,16 A recent large Mendelian randomization (MR) study has also validated the relationship between obesity and various respiratory diseases.17 In addition, VAT has been recognized as an important metabolic tissue associated with energy storage, immunity, chronic inflammation and metabolic disorders, as well as an endocrine organ that secretes a variety of biologically active substances.18,19 These released inflammatory mediators may be closely related to the development of CRDs. However, there have been few studies on the association between VAT and CRDs. A cross-sectional study has shown that a COPD group had a larger area of visceral fat than a control group, despite there being no difference in BMI or waist circumference between the two groups.20 Another study showed that VAT is associated with a narrowed lumen in the bronchial tubes of patients with asthma.21 Furthermore, a meta-analysis combining 43 observational studies revealed an association between higher VAT and asthma.22 Additionally, a cohort study showed that every doubling of the area of visceral adipose tissue was associated with a 30% increase in ILD incidence.23 Most studies that have explored the relationship between VAT and CRDs have been observational. However, it is well known that observational studies are characterized by uncontrollable confounding factors that may affect their results’ accuracy.
MR is a method that uses genome-wide association study (GWAS) databases to investigate the potential causal association between specific exposure and outcomes. Specifically, this method uses genetic variants as instrumental variables (IVs) to analyse the effect of modifiable exposures on various health, social and economic outcomes. The genetic variation is randomly inherited from parents to offspring at conception, similar to the random assignment of treatment in an randomized controlled trial, hence reducing the risk of confounding. Compared with observational studies, the MR-based approach is less susceptible to reverse causation or the influence of potentially confounding variables.24–26 Meanwhile with the rapid expansion of publicly available GWAS summary statistics over the past decade, especially the data on European population, the method’s flexibility and applicability have increased significantly.27 Besides, the causal relationship between VAT and CRDs in European population is still unclear. There is no relevant MR study to explore the relationship.
The present study utilizes MR analysis to explore the potential causal association between VAT and CRDs in European population, providing more evidence for CRDs prevention and treatment strategies.
Methods
Study Design
We used two-sample MR analysis to explore the association between VAT and several CRDs. Figure 1 shows an overview of the study design. The MR analysis was based on three critical assumptions: (i) genetically IVs are strongly correlated with exposure factors; (ii) genetically IVs are not affected by any confounders; (iii) single nucleotide polymorphisms (SNPs) do not influence the results through any pathways other than the exposure pathway (VAT).
 |
Figure 1 Schematic representation of our Mendelian randomization study of the associations between visceral adipose tissue and chronic respiratory diseases. BMI: body mass index. |
Data Sources
Data Sources for Exposures
The predicted genes for the instrumental variable were derived from a large-scale UK Biobank cohort. In the study, Researchers measured the VAT of 4198 White British ancestors from the UK Biobank by dual-energy X-ray absorptiometry, and established a VAT training dataset. They also constructed an application dataset of the VAT including 325,153 White British individuals.28,29 Both the training dataset and the application dataset shared similar characteristics. Compared to previous GWAS for VAT or VAT adjusted for BMI, this GWAS identified more VAT-associated loci. We obtained publicly available summary data from the GWAS Catalog (https://www.ebi.ac.uk/gwas/). Detailed characteristics of the IVs are shown in Table 1.
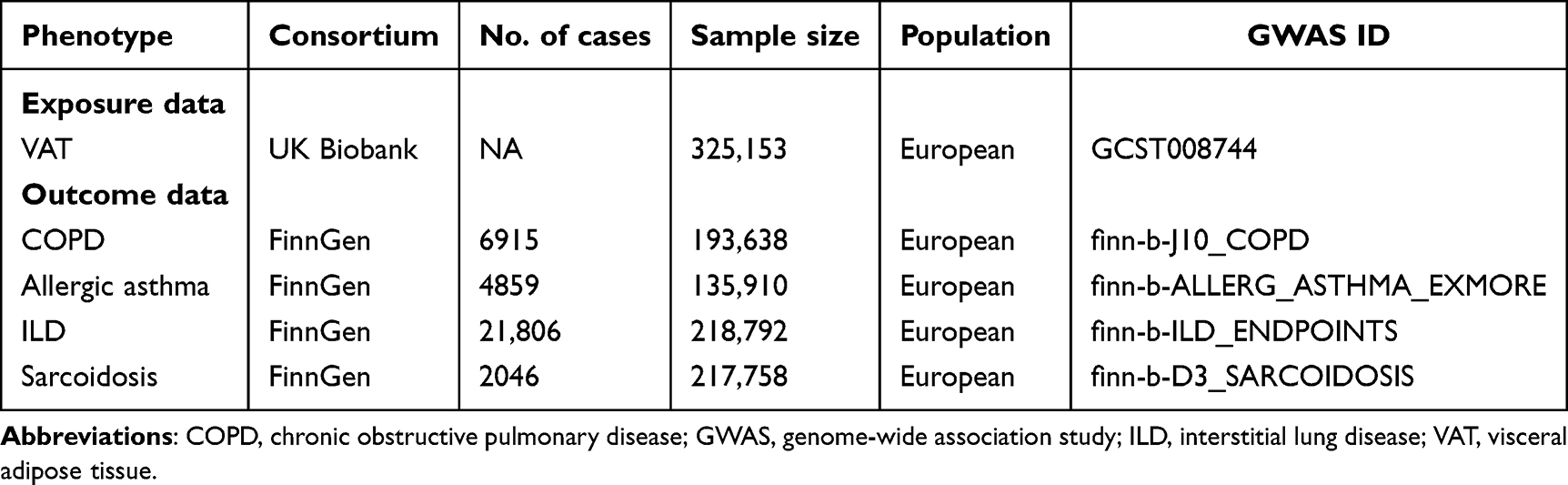 |
Table 1 Data Sources for Exposure and Outcomes |
Data Sources for Outcomes
COPD, allergic asthma, ILD, and sarcoidosis served as endpoints in this study. To minimize potential bias due to sample overlap, all data for these four outcomes were derived from the FinnGen study (https://www.finngen.fi/). We obtained the GWAS summary statistics for these outcomes through the IEU Open GWAS database (https://gwas.mrcieu.ac.uk/). Detailed characteristics of the four outcomes are presented in Table 1.
Instrumental Variable Selection
We screened SNPs strongly associated with VAT from the GWAS database as IVs with a threshold of P < 5×10−8. Linkage disequilibrium was excluded based on r2 = 0.001 and clump distance > 10,000 kb to ensure that the IVs selected for VAT were independent of each other.30 F-statistics (F = β2/SE2) were calculated for each SNP to assess the IVs’ strength. Generally, SNPs with F-statistics > 10 are recommended for MR analyses, as they are unlikely to be weak IVs, whereas those with F-statistics < 10 were excluded to prevent the effect of weak IVs’ bias on results.30–32
Statistical Analysis
MR analysis was performed using the “TwoSampleMR” (Version 0.5.7) software package in R (Version 4.3.1). We used inverse-variance weighted (IVW) as the primary assessment method to examine the role of genetic susceptibility to VAT on the outcome of four CRDs, which can provides a robust causal estimate in the presence of heterogeneity.33 MR Egger, weighted median, Simple mode and Weighted mode were considered complementary MR analysis methods to improve the robustness of the results.34,35 MR results were reported as odds ratios. Given that our study included four outcomes, the significance threshold was adjusted for multiple testing using the Bonferroni correction, with a two-sided P < 1.25×10⁻² (0.05/4) considered statistically significant to control for type I errors. Egger intercept and MR-pleiotropy residual sum and outlier (MR-PRESSO) were used to test the results’ horizontal pleiotropy.36 Where P > 0.05, no horizontal pleiotropy was considered. MR-PRESSO was used not only to identify pleiotropy but also to identify outliers. If there were any outliers, we performed a new MR analysis after removing the outliers. Leave-one-out was also used for sensitivity testing to investigate whether the association was affected by any particular SNP. Cochran’s Q was employed to estimate the heterogeneity of the results. Heterogeneity was indicated by P < 0.05.
Considering that VAT is strongly associated with BMI, which in turn is associated with respiratory disease, we performed regression-based multivariate MR (MVMR) analysis,37 which adjusted for BMI to exclude the confounding results of BMI.
Results
Genetic Instruments
We identified 21,727 strongly associated SNPs from a GWAS including 325,153 individuals of European ancestry. Next, we obtained 221 SNPs strongly associated with VAT as IVs after excluding linkage disequilibrium (specific SNP characteristics are shown in Table S1). The F-statistics of these 221 SNPs were all greater than 10, implying that there were no weak variables. We extracted 219 SNPs from the genomes of COPD, allergic asthma, ILD, and sarcoidosis. After removing 11 SNPs for being palindromic, our final sample included 208 SNPs for MR analysis (see Table S1).
Estimating the Causal Effects of VAT on Chronic Respiratory Diseases
In two-sample MR analysis, the IVW method suggested a positive correlation between VAT and COPD (OR = 1.56; 95% CI: 1.34–1.82; P = 1.16×10⁻8), allergic asthma (OR = 1.44; 95% CI: 1.20–1.73; P = 8.63×10⁻5), and ILD (OR = 1.15; 95% CI: 1.04–1.26; P = 4.62×10−3), but not with sarcoidosis (OR = 1.02; 95% CI: 0.78–1.34; P = 8.76×10−1). Weighted median also confirmed the correlation of VAT with COPD (OR = 1.49; 95% CI: 1.19–1.85; P = 4.44×10-4) and allergic asthma (OR = 1.55; 95% CI: 1.19–2.02; P = 1.06×10−3). More detailed results are shown in Table 2, Figures 2 and S1.
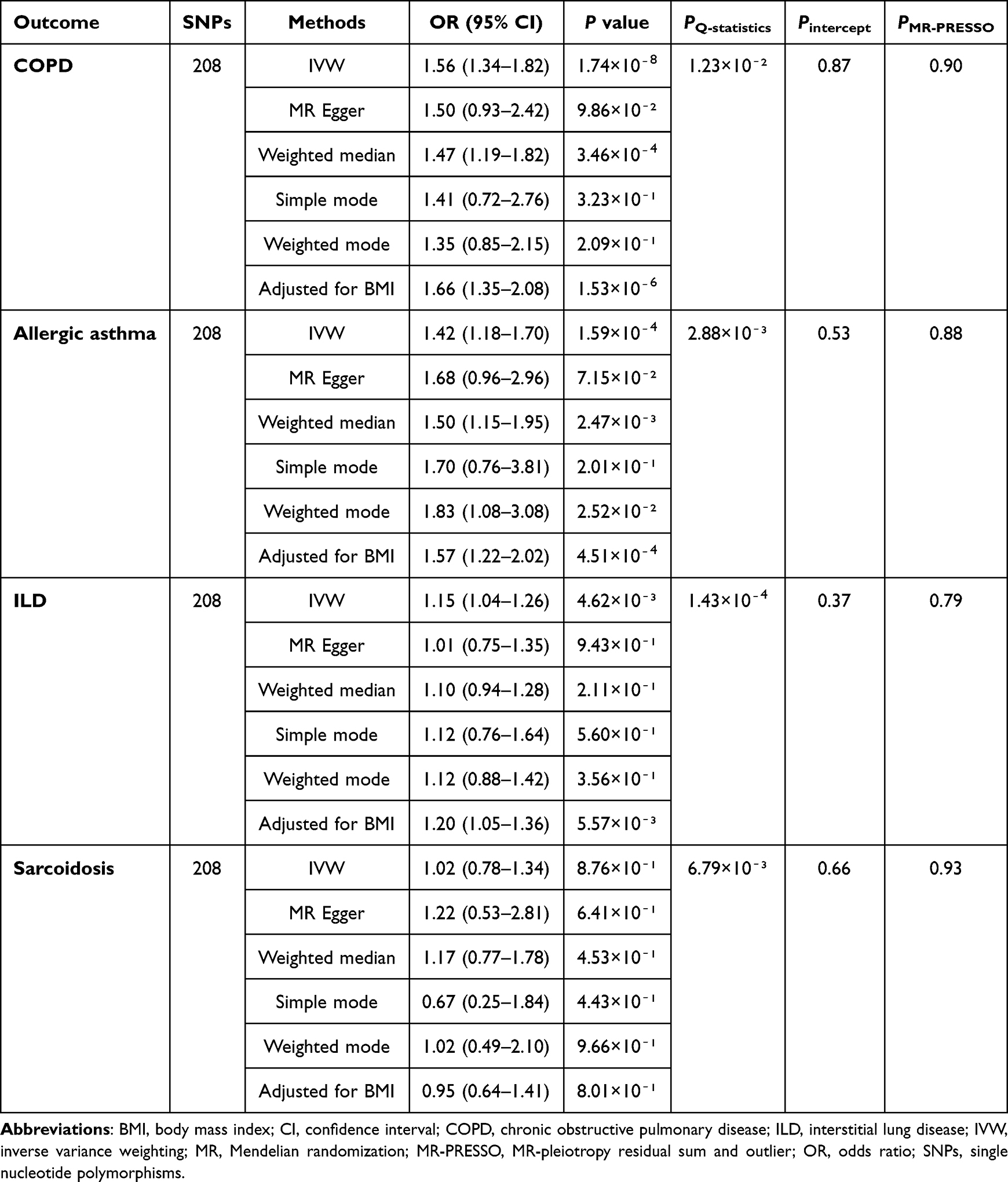 |
Table 2 Mendelian Randomization Analysis Results for the Associations Between Visceral Adipose Tissue and the Risk of Four Chronic Respiratory Diseases |
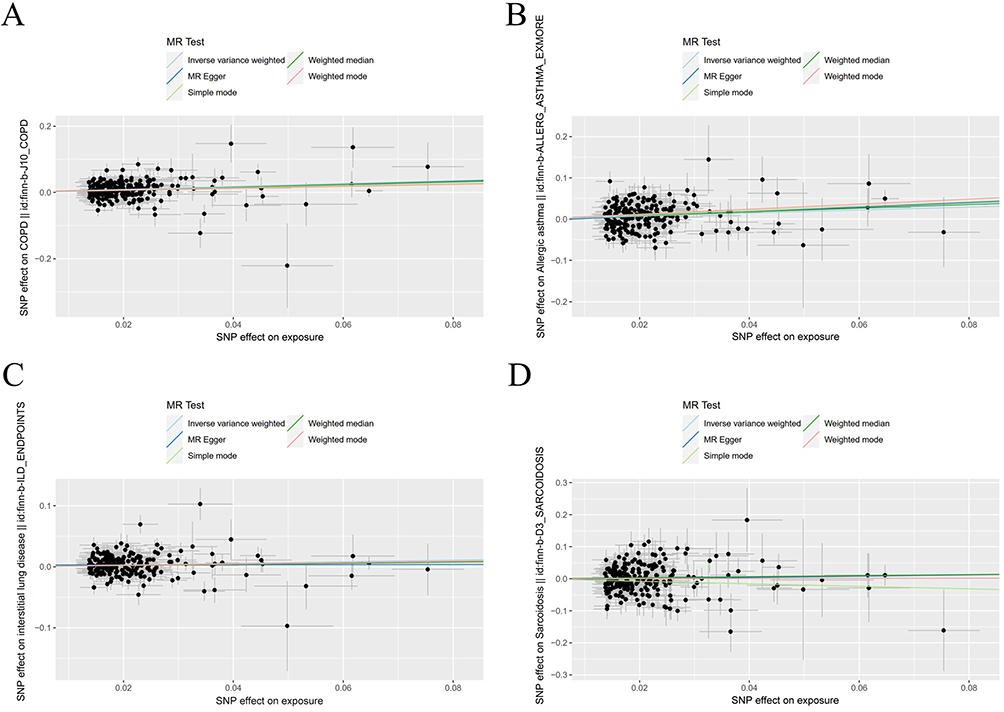 |
Figure 2 Scatter plots of Mendelian randomization analysis for the associations between visceral adipose tissue and the risk of (A) chronic obstructive pulmonary disease, (B) allergic asthma, (C) interstitial lung disease, and (D) sarcoidosis. |
We further performed MVMR analysis to obtain MR estimates independent of the effect of BMI. In MVMR analysis adjusted for BMI, VAT was independently associated with the risk of COPD (OR = 1.66; 95% CI: 1.35–2.08; P = 1.53×10−6), allergic asthma (OR = 1.57; 95% CI: 1.22–2.02; P = 4.51×10−4), and ILD (OR = 1.20; 95% CI: 1.05–1.36; P = 5.57×10−3), but not with sarcoidosis (OR = 0.95; 95% CI: 0.64–1.41; P = 8.01×10−1).
Sensitivity Analysis
The leave-one-out method results were similar to those obtained with the standard IVW (Figure S2). We observed modest heterogeneity in the analysis for COPD, allergic asthma, ILD and sarcoidosis using Cochran’s Q statistic (Table 2). The intercept from the MR Egger method did not reveal the presence of horizontal pleiotropy (COPD: P = 0.88; allergic asthma: P = 0.49; or ILD: P = 0.37; sarcoidosis: P = 0.66). In addition, MR-PRESSO did not identify any abnormal SNPs, with all P values > 0.05 (COPD: P = 0.90; allergic asthma: P = 0.87; ILD: P = 0.79; sarcoidosis: P = 0.93).
Discussion
A growing body of research is addressing the adverse effects of VAT on human health. In this study, we performed an MR analysis to assess the relationship between VAT and the risk of four CRDs. We found that VAT was associated with increased risk of COPD, allergic asthma, and ILD at the genetic level. In addition, the associations for VAT and COPD, allergic asthma, and ILD were independent of BMI. Our results were consistent with the previous observational findings, further confirming that VAT is an independent genetic risk factor for COPD, allergic asthma, and ILD.
Even though VAT has become a more concerning indicator than obesity, more studies have focused on the association between respiratory diseases and obesity.6 Though several previous observational studies have focused on VAT’s associations with COPD, asthma, and ILD,38,39 which were confirmed by our research, the biological mechanisms associated with the increased risk of chronic respiratory diseases due to VAT have yet to be clarified. Perhaps we could draw inspiration from the mechanism of obesity and some respiratory diseases.
VAT is considered an active endocrine organ with metabolic activity. In obesity, hypertrophic adipose tissue produces many pro-inflammatory mediators, including leptin, resistin, interleukin 6 (IL-6), and tumor necrosis factor-alpha,38,39 all of which are associated with not only local inflammation, but also systemic inflammatory responses.22,40,41 It has been shown that these pro-inflammatory mediators may promote the NLR family pyrin domain containing 3 (NLRP3) inflammasome activation and IL-1β secretion. Activation of IL-1β signalling in the lung further increases the expression of pro-inflammatory cytokines (eg, IL-23, IL-5, IL-13), promoting the activity of immune cells (eg, T-helper cells, eosinophils, macrophages), leading to lung inflammation and dysfunction, and promoting development of lung diseases.42 Adiponectin acts as both an insulin sensitizer and an anti-inflammatory factor, playing an essential role in the regulation of glucolipid metabolism.43 In contrast to leptin and other pro-inflammatory mediators, researchers have discovered that adiponectin is significantly lower in individuals with obesity.44–46
Existing high-quality studies exploring the relationship between VAT and COPD are limited. Based on previous studies, we hypothesized that inflammation-induced airway hyperresponsiveness may play an essential role in the relationship between VAT and COPD. van den Borst et al revealed a significant increase in VAT in elderly patients with COPD, which was associated with elevated IL-6 in plasma.47 IL-6 has also been shown to be a strong predictor of death in respiratory and cardiovascular diseases.47,48 Bruzzaniti et al discovered that leptin inhibited COPD patients’ regulatory T cells’ proliferation and activity, and adversely affected the progression of COPD.49 Moreover, a cross-sectional study demonstrated a significant negative correlation between adiponectin and FEV1%, suggesting that adiponectin may serve as a biomarker of the severity and progression of disease in patients with COPD.50
Allergic asthma is the most common asthma phenotype.51 It is now recognized as a complex chronic inflammatory disease related to airway hyperresponsiveness and tissue remodeling in airway structures.52 A study has shown that elevated leptin levels in obese mice exacerbate allergic asthma and increase airway hyperresponsiveness.53,54 Another study indicated that leptin promoted the survival and proliferation of Th2 cells, leading to increased expression of IL-4, IL-5, and IL-13, which collectively promoted the allergic response.55 Sideleva et al showed an increased infiltration of VAT macrophages and leptin expression, but decreased adiponectin in obese asthmatics, compared to the control group. They also found that respiratory epithelial cells expressed leptin and adiponectin receptors, while leptin might be directly involved in airway remodeling.56 Adiponectin has previously been shown to alleviate allergic airway inflammation and airway hyperresponsiveness in ovalbumin-sensitized mice.57
ILD is a disease involving the pulmonary interstitium and alveoli.58 Most ILD is characterized by inflammation or fibrosis within the interstitial spaces. However, the molecular mechanisms of ILD pathogenesis remain unknown, and the mechanism of how VAT works to increase the risk of ILD has yet to be investigated. Previous studies have suggested that adipokines may be mediators of pro-inflammatory changes leading to interstitial lung abnormalities and fibrosis.59,60 In an animal study, researchers observed that mice with leptin receptor deficiency were resistant to bleomycin-induced fibrosis.61 Resistin is another adipokine that promotes the production of inflammatory factors such as IL-6, IL-1β, and tumor necrosis factor-alpha.62 A study has shown that resistin was significantly elevated in the serum of ILD patients with interstitial lung abnormalities, and this result remained significant after correction by Bonferroni.63 Adiponectin is an anti-inflammatory adipokine relevant to metabolic regulation, tissue remodeling and intravascular homeostasis.64 When adiponectin-deficient mice were exposed to a toxic environment, alveolar macrophages were spontaneously activated, accompanied by increased release of pro-inflammatory mediators (such as tumor necrosis factor-alpha and matrix metalloproteinase 12), resulting in structural lung alterations.65 These findings may provide inspiration for exploring the mechanism of action through which VAT increases the risk of ILD.
Currently, we found no studies that explored the relationship between VAT and sarcoidosis. However, several observational studies have illustrated the correlation between obesity and sarcoidosis, although the results have been different. For example, a study from the US Veterans Administration found no correlation between BMI and the incidence of sarcoidosis. Meanwhile, a cohort study conducted on 59,000 African American women between the ages of 21 and 69 showed that the prevalence of sarcoidosis increased with BMI and weight. Another case-control study demonstrated that the BMI (≥ 25 kg/m2) was significantly higher in patients with sarcoidosis than in healthy volunteers. In our study, we found no correlation between VAT and sarcoidosis. This may be due to differences in inflammatory pathways or etiologies between sarcoidosis and other CRDs (eg, COPD, allergic asthma and ILD), as well as insufficient statistical power to detect a weak association due to lower prevalence of sarcoidosis. Further relevant studies could be conducted to explore the relationship in the future.
As far as we know, our study is the first to comprehensively assess the relevance of VAT for multiple chronic respiratory diseases using MR analysis. This is important because MR analysis minimalizes the likelihood of residual confusion. We also used several sensitivity analysis methods to evaluate the assumptions of MR, and multivariate MR analysis to adjust for the effect of BMI to ensure higher reliability in our results.
However, we do recognize that there are several limitations in this study. Firstly, the training model for VAT prediction was built on a small subset of data, and this may have limited its statistical efficacy. Next, to ensure consistency in the genetic background of our sample, our MR analysis only included individuals from Europe, and therefore it does not represent VAT’s true genetic association with the general population. This may limit the generalizability of this finding to other races. Thirdly, despite our findings suggesting a association between VAT and the three CRDs, it is possible that this relationship is nonlinear. Future studies should further investigate the relationship between VAT and other CRDs. Finally, MR studies are helpful in determining whether the observed correlations is supported by genetic evidence. However, as with all MR studies, our conclusions depend on adherence to the MR method’s assumptions. Despite various sensitivity analyses to assess the reliability of our results, it still could not definitively exclude the potential impact of unmeasured confounders on our results. Meanwhile, more laboratory and clinical studies are often needed to reveal the underlying biological mechanisms.
Conclusion
This MR study indicated that genetically-predicted higher VAT was associated with an increased risk of COPD, allergic asthma, and IDL, and this association was independent of the effect of BMI.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Materials. Further inquiries can be directed to the corresponding author.
Ethics Statement
This study is exempt from ethics approval based on item 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China. The details are as follows:
Item 1 of Article 32: using legally obtained public data or conducting research through observation without interfering with public behavior. Item 2 of Article 32: using anonymized information data to conduct research.
Acknowledgments
The authors sincerely thank the GWAS database and the investigators involved for sharing the summary statistics used in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shenzhen Science and Technology Plan Project (JCYJ20170817094838619).
Disclosure
The authors report that there are no competing interests to declare.
References
1. Smith U. Abdominal obesity: a marker of ectopic fat accumulation. J Clin Invest. 2015;125(5):1790–1792. doi:10.1172/JCI81507
2. Schwartz MW, Seeley RJ, Zeltser LM, et al. Obesity pathogenesis: an endocrine society scientific statement. Endocr Rev. 2017;38(4):267–296. doi:10.1210/er.2017-00111
3. Lee SJ, Shin SW. Mechanisms, pathophysiology, and management of obesity. N Engl J Med. 2017;376(15):1491–1492. doi:10.1056/NEJMc1701944
4. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in underweight and obesity from 1990 to 2022: a pooled analysis of 3663 population-representative studies with 222 million children, adolescents, and adults. Lancet. 2024;403(10431):1027–1050. doi:10.1016/S0140-6736(23)02750-2
5. Reid TJ, Korner J. Medical and surgical treatment of obesity. Med Clin North Am. 2022;106(5):837–852. doi:10.1016/j.mcna.2022.03.002
6. Goossens GH. The metabolic phenotype in obesity: fat mass, body fat distribution, and adipose tissue function. Obes Facts. 2017;10(3):207–215. doi:10.1159/000471488
7. Ross R, Soni S, Houle SA. Negative Energy Balance Induced by Exercise or Diet: effects on Visceral Adipose Tissue and Liver Fat. Nutrients. 2020;12(4):891. doi:10.3390/nu12040891
8. Piché ME, Tchernof A, Després JP. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ Res. 2020;126(11):1477–1500. doi:10.1161/CIRCRESAHA.120.316101
9. Faria G, Gonçalves A, Cunha R, et al. Beyond central adiposity: liver fat and visceral fat area are associated with metabolic syndrome in morbidly obese patients. Int J Surg. 2015;14:75–79. doi:10.1016/j.ijsu.2014.12.028
10. Haberka M, Stolarz-Skrzypek K, Biedroń M, et al. Obesity, Visceral Fat, and Hypertension-Related Complications. Metab Syndr Relat Disord. 2018;16(10):521–529. doi:10.1089/met.2018.0062
11. Rowan CR, McManus J, Boland K, et al. Visceral adiposity and inflammatory bowel disease. Int J Colorectal Dis. 2021;36(11):2305–2319. doi:10.1007/s00384-021-03968-w
12. Agrawal S, Klarqvist MDR, Diamant N, et al. BMI-adjusted adipose tissue volumes exhibit depot-specific and divergent associations with cardiometabolic diseases. Nat Commun. 2023;14(1):266. doi:10.1038/s41467-022-35704-5
13. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
14. Momtazmanesh S, Moghaddam SS, Ghamari S-H; GBD 2019. Chronic respiratory diseases collaborators. global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the global burden of disease study 2019. EClinicalMedicine. 2023;59:101936. doi:10.1016/j.eclinm.2023.101936
15. Guerra S, Sherrill DL, Bobadilla A, et al. The relation of body mass index to asthma, chronic bronchitis, and emphysema. Chest. 2002;122(4):1256–1263. doi:10.1378/chest.122.4.1256
16. Murugan AT, Sharma G. Obesity and respiratory diseases. Chron Respir Dis. 2008;5(4):233–242. doi:10.1177/1479972308096978
17. Yang W, Yang Y, Guo Y, et al. Obesity and risk for respiratory diseases: a Mendelian randomization study. Front Endocrinol (Lausanne). 2023;14:1197730. doi:10.3389/fendo.2023.1197730
18. Matsuzawa Y. Adiponectin: a key player in obesity related disorders. Curr Pharm Des. 2010;16(17):1896–1901. doi:10.2174/138161210791208893
19. Doyle SL, Donohoe CL, Lysaght J, et al. Visceral obesity, metabolic syndrome, insulin resistance and cancer. Proc Nutr Soc. 2012;71(1):181–189. doi:10.1017/S002966511100320X
20. Furutate R, Ishii T, Wakabayashi R, et al. Excessive visceral fat accumulation in advanced chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2011;6:423–430. doi:10.2147/COPD.S22885
21. Yang MS, Choi S, Choi Y, et al. Association between airway parameters and abdominal fat measured via computed tomography in asthmatic patients. Allergy Asthma Immunol Res. 2018;10(5):503–515. doi:10.4168/aair.2018.10.5.503
22. Wu T, Jahangir MR, Mensink-Bout SM, et al. Visceral adiposity and respiratory outcomes in children and adults: a systematic review. Int J Obes Lond. 2022;46(6):1083–1100. doi:10.1038/s41366-022-01091-6
23. Anderson MR, Kim JS, Allison M, et al. Adiposity and interstitial lung abnormalities in community-dwelling adults: the mesa cohort study. Chest. 2021;160(2):582–594. doi:10.1016/j.chest.2021.03.058
24. Burgess S, Butterworth A, Thompson SG. Mendelian randomization analysis with multiple genetic variants using summarized data. Genet Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
25. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomisation (STROBE-MR): explanation and elaboration. BMJ. 2021;375:n2233.
26. Larsson SC, Butterworth AS, Burgess S. Mendelian randomization for cardiovascular diseases: principles and applications. Eur Heart J. 2023;44(47):4913–4924. doi:10.1093/eurheartj/ehad736
27. Emdin CA, Khera AV, Kathiresan S. Mendelian Randomization. JAMA. 2017;318(19):1925–1926. doi:10.1001/jama.2017.17219
28. Karlsson T, Rask-Andersen M, Pan G, et al. Contribution of genetics to visceral adiposity and its relation to cardiovascular and metabolic disease. Nat Med. 2019;25(9):1390–1395. doi:10.1038/s41591-019-0563-7
29. Sun X, Yuan Y, Chen L, et al. Genetically predicted visceral adipose tissue and risk of nine non-tumour gastrointestinal diseases: evidence from a Mendelian randomization study. Int J Obes Lond. 2023;47(5):406–412. doi:10.1038/s41366-023-01279-4
30. Sekula P, Greco M F D, Pattaro C, et al. Mendelian randomization as an approach to assess causality using observational data. J Am Soc Nephrol. 2016;27(11):3253–3265. doi:10.1681/ASN.2016010098
31. Pierce BL, Ahsan H, Vanderweele TJ. Power and instrument strength requirements for Mendelian randomization studies using multiple genetic variants. Int J Epidemiol. 2011;40(3):740–752. doi:10.1093/ije/dyq151
32. Burgess S, Thompson SG. CRP CHD Genetics Collaboration. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 2011;40(3):755–764. doi:10.1093/ije/dyr036
33. Bowden J, Greco M F D, Minelli C, et al. A framework for the investigation of pleiotropy in two-sample summary data Mendelian randomization. Stat Med. 2017;36(11):1783–1802. doi:10.1002/sim.7221
34. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
35. Bowden J, Davey Smith G, Haycock PC, et al. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
36. Verbanck M, Chen CY, Neale B, et al. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
37. Sanderson E, Davey Smith G, Windmeijer F, et al. An examination of multivariable Mendelian randomization in the single-sample and two-sample summary data settings. Int J Epidemiol. 2019;48(3):713–727. doi:10.1093/ije/dyy262
38. Dixon AE, Holguin F, Sood A, et al. An official American thoracic society workshop report: obesity and asthma. Proc Am Thorac Soc. 2010;7(5):325–335. doi:10.1513/pats.200903-013ST
39. Ibrahim MM. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev. 2010;11(1):11–18. doi:10.1111/j.1467-789X.2009.00623.x
40. Malli F, Papaioannou AI, Gourgoulianis KI, et al. The role of leptin in the respiratory system: an overview. Respir Res. 2010;11(1):152. doi:10.1186/1465-9921-11-152
41. Ren Y, Zhao H, Yin C, et al. Adipokines, hepatokines and myokines: focus on their role and molecular mechanisms in adipose tissue inflammation. Front Endocrinol (Lausanne). 2022;13:873699. doi:10.3389/fendo.2022.873699
42. Palma G, Sorice GP, Genchi VA, et al. Adipose tissue inflammation and pulmonary dysfunction in obesity. Int J mol Sci. 2022;23(13):7349. doi:10.3390/ijms23137349
43. Wang ZV, Scherer PE. Adiponectin, the past two decades. J mol Cell Biol. 2016;8(2):93–100. doi:10.1093/jmcb/mjw011
44. Hoffstedt J, Arvidsson E, Sjölin E, et al. Adipose tissue adiponectin production and adiponectin serum concentration in human obesity and insulin resistance. J Clin Endocrinol Metab. 2004;89(3):1391–1396. doi:10.1210/jc.2003-031458
45. Yang WS, Lee WJ, Funahashi T, et al. Weight reduction increases plasma levels of an adipose-derived anti-inflammatory protein, adiponectin. J Clin Endocrinol Metab. 2001;86(8):3815–3819. doi:10.1210/jcem.86.8.7741
46. Arita Y, Kihara S, Ouchi N, et al. Paradoxical decrease of an adipose-specific protein, adiponectin, in obesity. Biochem Biophys Res Commun. 1999;257(1):79–83. doi:10.1006/bbrc.1999.0255
47. van den Borst B, Gosker HR, Koster A, et al. The influence of abdominal visceral fat on inflammatory pathways and mortality risk in obstructive lung disease. Am J Clin Nutr. 2012;96(3):516–526. doi:10.3945/ajcn.112.040774
48. Celli BR, Locantore N, Yates J, et al. Inflammatory biomarkers improve clinical prediction of mortality in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;185(10):1065–1072. doi:10.1164/rccm.201110-1792OC
49. Bruzzaniti S, Bocchino M, Santopaolo M, et al. An immunometabolic pathomechanism for chronic obstructive pulmonary disease. Proc Natl Acad Sci U S A. 2019;116(31):15625–15634. doi:10.1073/pnas.1906303116
50. Jaswal S, Saini V, Kaur J, et al. Association of adiponectin with lung function impairment and disease severity in chronic obstructive pulmonary disease. Int J Appl Basic Med Res. 2018;8(1):14–18. doi:10.4103/ijabmr.IJABMR_65_17
51. Akar-Ghibril N, Casale T, Custovic A, et al. Allergic endotypes and phenotypes of asthma. J Allergy Clin Immunol Pract. 2020;8(2):429–440. doi:10.1016/j.jaip.2019.11.008
52. Murdoch JR, Lloyd CM. Chronic inflammation and asthma. Mutat Res. 2010;690(1–2):24–39. doi:10.1016/j.mrfmmm.2009.09.005
53. Shore SA, Schwartzman IN, Mellema MS, et al. Effect of leptin on allergic airway responses in mice. J Allergy Clin Immunol. 2005;115(1):103–109. doi:10.1016/j.jaci.2004.10.007
54. Zheng H, Wu D, Wu X, et al. Leptin promotes allergic airway inflammation through targeting the unfolded protein response pathway. Sci Rep. 2018;8(1):8905. doi:10.1038/s41598-018-27278-4
55. Zheng H, Zhang X, Castillo EF, et al. Leptin enhances TH2 and ILC2 responses in allergic airway disease. J Biol Chem. 2016;291(42):22043–22052. doi:10.1074/jbc.M116.743187
56. Sideleva O, Suratt BT, Black KE, et al. Obesity and asthma: an inflammatory disease of adipose tissue not the airway. Am J Respir Crit Care Med. 2012;186(7):598–605. doi:10.1164/rccm.201203-0573OC
57. Shore SA, Terry RD, Flynt L, et al. Adiponectin attenuates allergen-induced airway inflammation and hyperresponsiveness in mice. J Allergy Clin Immunol. 2006;118(2):389–395. doi:10.1016/j.jaci.2006.04.021
58. Wijsenbeek M, Suzuki A, Maher TM. Interstitial lung diseases. Lancet. 2022;400(10354):769–786. doi:10.1016/S0140-6736(22)01052-2
59. Zielinski M, Chwalba A, Jastrzebski D, et al. Adipokines in interstitial lung diseases. Respir Physiol Neurobiol. 2023;315:104109. doi:10.1016/j.resp.2023.104109
60. Kim JS, Anderson MR, Podolanczuk AJ, et al. Associations of serum adipokines with subclinical interstitial lung disease among community-dwelling adults: the multi-ethnic study of atherosclerosis (mesa). Chest. 2020;157(3):580–589. doi:10.1016/j.chest.2019.10.011
61. Jain M, Budinger GR, Lo A, et al. Leptin promotes fibroproliferative acute respiratory distress syndrome by inhibiting peroxisome proliferator-activated receptor-γ. Am J Respir Crit Care Med. 2011;183(11):1490–1498. doi:10.1164/rccm.201009-1409OC
62. Ye L, Zuo Y, Chen F, et al. Resistin expression is associated with interstitial lung disease in dermatomyositis. Front Med Lausanne. 2022;9:903887. doi:10.3389/fmed.2022.903887
63. Buendía-Roldán I, Fernandez R, Mejía M, et al. Risk factors associated with the development of interstitial lung abnormalities. Eur Respir J. 2021;58(2):2003005. doi:10.1183/13993003.03005-2020
64. Haley S, Shah D, Romero F, Summer R. Scleroderma-related lung disease: are adipokines involved pathogenically? Curr Rheumatol Rep. 2013;15(12):381. doi:10.1007/s11926-013-0381-8
65. Summer R, Little FF, Ouchi N, et al. Alveolar macrophage activation and an emphysema-like phenotype in adiponectin-deficient mice. Am J Physiol Lung Cell mol Physiol. 2008;294(6):L1035–L1042. doi:10.1152/ajplung.00397.2007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.