Back to Journals » OncoTargets and Therapy » Volume 10
Association between TP53 gene Arg72Pro polymorphism and Wilms’ tumor risk in a Chinese population
Authors Fu W, Zhuo Z, Jia W, Zhu J ![]() , Zhu S, Lin Z, Wang F, Xia H
, Zhu S, Lin Z, Wang F, Xia H ![]() , He J
, He J ![]() , Liu G
, Liu G
Received 23 December 2016
Accepted for publication 3 February 2017
Published 23 February 2017 Volume 2017:10 Pages 1149—1154
DOI https://doi.org/10.2147/OTT.S131014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Yao Dai
Wen Fu,1,2,* Zhen-Jian Zhuo,3,* Wei Jia,1,2 Jinhong Zhu,4 Shi-Bo Zhu,1,2 Ze-Feng Lin,1,2 Feng-Hua Wang,1,2 Huimin Xia,1,2 Jing He,1,2 Guo-Chang Liu1,2
1Department of Pediatric Urology, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, Guangzhou, Guangdong, 2Department of Pediatric Surgery, Guangzhou Institute of Pediatrics, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, Guangzhou, Guangdong, 3Faculty of Medicine, School of Chinese Medicine, The Chinese University of Hong Kong, Hong Kong, 4Molecular Epidemiology Laboratory, Department of Laboratory Medicine, Harbin Medical University Cancer Hospital, Harbin, Heilongjiang, People’s Republic of China
*These authors contributed equally to this work
Abstract: Wilms’ tumor is one of the most prevalent pediatric malignancies, ranking fourth in childhood cancer worldwide. TP53 is a critical tumor suppressor gene, which encodes a 53 kDa protein, p53. The p53 functions to protect against cancer by regulating cell cycle and apoptosis and maintaining DNA integrity. TP53 gene is highly polymorphic. Several TP53 gene polymorphisms have been considered to be associated with cancer risk. Of them, a nonsynonymous polymorphism, Arg72Pro (rs1042522 C>G), has been most extensively studied for the association with cancer risk; however, few studies have investigated its effect on Wilms’ tumor. Because of the central role of p53 in cell cycle control, the TP53 gene Arg72Pro polymorphism is also a good potential candidate predisposition locus for this pediatric cancer. We genotyped this polymorphism in 145 patients and 531 cancer-free controls recruited from Chinese children by Taqman methodology. Overall, our result suggested a lack of association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor. In the stratified analysis, we found that carriers of CG/GG genotypes had a significantly increased Wilms’ tumor risk in children not older than 18 months (adjusted odds ratio =2.04, 95% confidence interval =1.003–4.13, P=0.049) compared with CC genotype carriers. Our study indicated that the TP53 gene Arg72Pro polymorphism may have a weak, age-related effect on Wilms’ tumor risk in Chinese children. These findings need further validations in other populations with larger sample size.
Keywords: TP53, polymorphism, Wilms’ tumor, susceptibility
Introduction
Wilms’ tumor, also known as nephroblastoma, is the fourth most frequently diagnosed childhood cancer worldwide. It constitutes ~6% of all cancers detected among children younger than 15 years. The incidence rate of Wilms’ tumor varies geographically. The occurrence rate of Wilms’ tumor is ~1/8,000 children, with 400–650 new cases annually, in the USA1,2 and ~1/10,000 children in Western populations.3 Wilms’ tumor is also one of the most common renal tumors in children in China but less prevalent than that in Western countries, with an incidence rate of ~3.3 per million.4 Up to 2% of Wilms’ tumor cases are familial, with a known causal genetic lesion.5 No more than 5% of cases can be attributed to known causes, and the genetic basis underlying most Wilms’ tumors remains largely unknown.6,7
The human TP53 gene, encoding a 53 kDa protein (p53), is located on chromosome 17p13.1. TP53 gene is one of the most commonly mutated genes in human cancers.8 The TP53 gene is a tumor suppressor gene, playing an important role in the maintenance of DNA integrity, cell cycle control, and apoptosis.9–11 According to dbSNP database (http://www.ncbi.nlm.nih.gov/projects/SNP), at least 1,462 single-nucleotide polymorphisms (SNPs) have been identified in the TP53 gene so far, supporting its highly polymorphic nature. Among them, the most commonly reported SNP is a nonsynonymous Arg72Pro (rs1042522 C>G) polymorphism. This polymorphism is located in the exon 4 of the TP53 gene and can lead to the replacement of arginine (Arg) with proline (Pro) at codon 72. This polymorphism is able to alter the primary structures as well as biochemical functions of the p53 protein.12–14 It has been reported that the Arg72 form of p53 is more effective in inducing apoptosis and protecting cells from malignant transformation than the Pro72 variant.12,15 Numerous studies have been carried out to investigate the association between this polymorphism and cancer susceptibility.16–20 However, very few studies have investigated its association with Wilms’ tumor susceptibility and clinical outcomes until now.21,22 In light of the important tumor-suppressing role of TP53 gene, we investigated the association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor susceptibility in the current hospital-based case–control study with 145 cases and 531 cancer-free controls.
Subjects and methods
Subjects
This study consisted of 145 newly diagnosed and histopathologically confirmed Wilms’ tumor patients from the Department of Pediatric Urology, Guangzhou Women and Children’s Medical Center.23 Patients were enrolled between March 2001 and June 2016. Controls were chosen from children who visited for routine physical examination, as we described previously.24–29 A total of 531 ethnicity-, age-, and gender-matched cancer-free controls were included in the study. Written informed consent was obtained from all subjects or their legal guardians in accordance with the principles of the Declaration of Helsinki. This study was approved by the Institutional Review Board of Guangzhou Women and Children’s Medical Center.
DNA extraction and genotyping of TP53 gene Arg72Pro polymorphism
Total genomic DNA was mainly isolated from the peripheral blood leukocytes using the TIANamp Blood DNA Kit (TianGen Biotech Co., Ltd., Beijing, China) as described previously.26 The TP53 gene Arg72Pro polymorphism was genotyped using the TaqMan real-time PCR method.26,30 Genotyping was performed blindly to the status of the case or control. Moreover, 10% of the samples were randomly selected to perform repeated assays, and the results were 100% concordant.
Statistical analysis
χ2 test was adopted to compare demographic characteristics and the frequency distributions of genotypes between cases and controls. Deviation from Hardy–Weinberg equilibrium (HWE) was tested using the χ2 goodness-of-fit test for the control subjects. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to assess the association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor susceptibility. Adjusted ORs and corresponding 95% CIs adjusting for age and gender were calculated by unconditional multiple logistic regression model. Stratified analyses were performed by age, gender, and clinical stages. All the statistical tests were two sided, and P-values <0.05 were considered as statistically significant. Statistical analysis was performed using the SAS software (Version 9.4; SAS Institute, Cary, NC, USA).
Results
Subject characteristics
Epidemiological characteristics of Wilms’ tumor patients and cancer-free controls are listed in Table S1. The mean age was 26.17 months (±21.48, range =1–132 months) for Wilms’ tumor patients and 29.73 months (±24.86, range =0.07–156 months) for controls. No significant differences were observed between the patients and controls in the distribution of age (P=0.725) and gender (P=0.956). According to the classification of childhood renal tumors defined by NWTS-5 criteria,31 4 (2.76%), 49 (33.79%), 50 (34.48%), and 33 (22.76%) patients had clinical stages I, II, III, and IV Wilms’ tumor, respectively. Unfortunately, tumor specimens were not available for nine (6.21%) patients.
Association between TP53 gene Arg72Pro polymorphism and Wilms’ tumor risk
The genotype frequencies of the TP53 gene Arg72Pro polymorphism in the Wilms’ tumor patients and controls are listed in Table 1. Genotype analysis for the TP53 gene Arg72Pro polymorphism revealed that there was no significant deviation from the HWE in the control group (P=0.440). We did not observe any significant association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor susceptibility (CG vs CC: adjusted OR =1.48, 95% CI =0.95–2.32, P=0.086; GG vs CC: adjusted OR =1.02, 95% CI =0.58–1.78, P=0.948; CG/GG vs CC: adjusted OR =1.33, 95% CI =0.87–2.04, P=0.191; and GG vs CC/CG: adjusted OR =0.78, 95% CI =0.49–1.25, P=0.307).
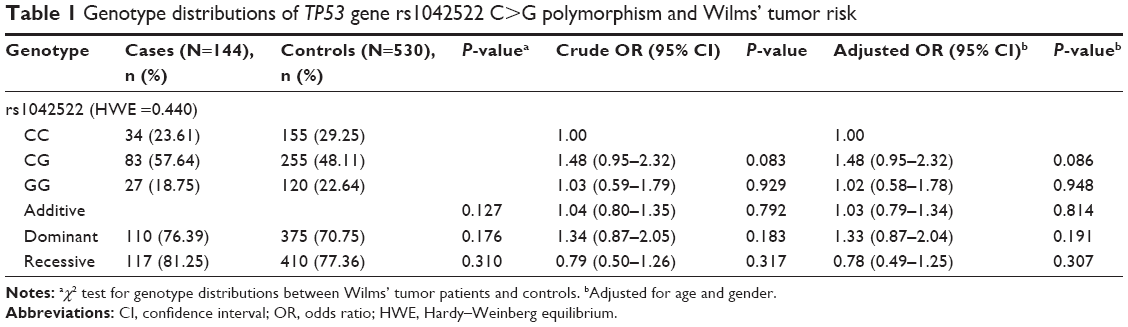 | Table 1 Genotype distributions of TP53 gene rs1042522 C>G polymorphism and Wilms’ tumor risk |
We further explored the association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor susceptibility in the stratified analysis by age, gender, and clinical stages (Table 2). Significant association was observed in children aged 18 months or younger (OR =2.06, 95% CI =1.02–4.18, P=0.045, and adjusted OR =2.04, 95% CI =1.003–4.13, P=0.049). It was suggested that younger children (≤18 months old) with CG/GG genotypes were at significantly higher risk of Wilms’ tumor than those with CC genotypes. However, no significant associations were observed in other stratified analyses.
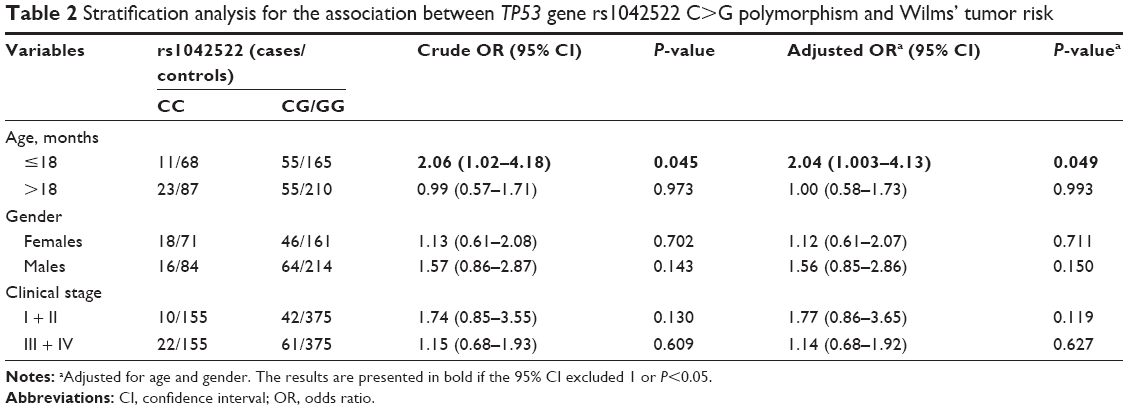 | Table 2 Stratification analysis for the association between TP53 gene rs1042522 C>G polymorphism and Wilms’ tumor risk |
Discussion
In the current hospital-based case–control study with 145 cases and 531 unrelated cancer-free controls, we did not observe any significant association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor susceptibility among Southern Chinese children. Interestingly, we found that the carriers of CG/GG genotypes, if 18 months old or younger, had a significantly increased Wilms’ tumor risk compared with counterparts carrying wild-type CC genotypes.
The TP53 gene (gene ID: 7157) is also known as P53 gene. It encodes a p53 tumor suppressor protein that contains DNA binding, transcriptional activation, and oligomerization domains.32,33 The p53 protein can regulate the expression of target genes in response to diverse cellular stresses, thereby inducing DNA repair, cell cycle arrest, metabolism changes, apoptosis, and cellular senescence accordingly.9–11,34 The p53 protein has been recognized as the guardian of human cells against cancer.9,35 However, this gene is highly mutated, and mutations in the TP53 gene have been implicated in the various types of cancer in human beings.36 Apart from the predisposition to mutations, TP53 is also highly polymorphic. A great number of SNPs has been identified in the TP53 gene. Several TP53 gene SNPs have been shown to confer cancer susceptibility, such as the rs78378222 A>C polymorphism discovered by whole-genome sequencing in 2011. We recently performed a meta-analysis to investigate the association between TP53 gene rs78378222 A>C and overall cancer risk.37 Evidence from 34 studies including 36,599 cases and 91,272 controls confirmed that this polymorphism was significantly associated with an increased overall cancer risk.37 The TP53 gene Arg72Pro polymorphism is the most extensively investigated variant among the known TP53 gene susceptibility loci, which was first reported by Matlashewski et al.38 Intriguingly, the two alleles of this nonsynonymous polymorphism differ in the capacity of inducing target gene transcription, consequentially modifying cancer susceptibility differentially.13,39,40
As so far, numerous studies have been conducted to investigate the association between this polymorphism and cancer susceptibility.16–20 Klug et al16 carried out a meta-analysis by including a total of 49 studies with 7,946 cases and 7,888 controls. They found that the TP53 gene Arg72Pro polymorphism was not associated with cervical cancer risk when the analyses were restricted to methodologically sound studies. Dahabreh et al17 did not find any significant association between TP53 gene Arg72Pro polymorphism and colorectal cancer with evidence from 23 studies including 6,514 cases and 9,334 controls. Xu et al18 combined 15 publications and found that the TP53 gene Arg72Pro polymorphism was associated with a significantly increased bladder cancer risk among Asians but not among Caucasians. Dahabreh et al19 carried out a meta-analysis involving breast cancer (68 studies), lung cancer (42), colorectal cancer (26), ovarian cancer (16), and endometrial cancer (8). They found that the association with the TP53 gene Arg72Pro polymorphism only existed among studies using tumor tissue as the source of genotyping material for cases (22 studies) but not among studies using other sources of genotyping material (eg, blood). However, it should be noted that the use of tumor tissue as the source of genotyping material for cases can lead to bias in the association studies. In the study by Tian et al20 with 14 investigations, including 2,506 cases and 4,386 controls, no association was observed between the TP53 gene Arg72Pro polymorphism and leukemia risk.
However, there is lack of evidence of the association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor risk to date. Only one case–control study has been performed to examine the association of this polymorphism with Wilms’ tumor risk22 using controls from other studies. In the study with 46 cases and 300 controls, Andrade et al22 found that carriers of the rs1042522 C allele may associate with an increased Wilms’ tumor risk. In our present study, we failed to find any significant association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor risk, which was similar to most previous investigations in other types of cancer.16,17,20 Failure to find any significant association between the TP53 gene Arg72Pro polymorphism and Wilms’ tumor risk may be ascribed to the weak effect of low-penetrant SNPs, ethnicity difference, as well as the limited sample size in the current study. We found that the TP53 gene Arg72Pro polymorphism may contribute to a weak effect for Wilms’ tumor risk in Chinese children aged 18 months and younger, which may be ascribed to the fact that young children may be more genetic susceptible to Wilms’ tumor risk; besides, it may be a chance finding for the sample size, which is relatively small.
Although this is the first investigation to assess the association between TP53 gene Arg72Pro polymorphism and Wilms’ tumor risk in Chinese children, our results should be interpreted with cautious for several limitations should be addressed. First, due to the low occurrence rate of Wilms’ tumor, only 145 cases were included in this study, which may have limited statistical power. Second, because of the nature of retrospective study design, we were only able to collect age, gender, ethnicity, and geographical factors for cases and controls. Other factors, such as dietary intake and parental environment exposures, were not available. Third, we just performed a case–control designed study to investigate the association between TP53 Arg72Pro polymorphism and Wilms’ tumor risk and we did not explore the potential mechanisms in cell lines for this polymorphism, which need to be investigated in future. Finally, we included only the most frequently investigated Arg72Pro polymorphism, and other TP53 gene polymorphisms (such as rs78378222 A>C) were not examined in this study.
Conclusion
This study indicated that the TP53 gene Arg72Pro polymorphism may contribute to a weak effect for Wilms’ tumor risk in Chinese children aged 18 months and younger. However, further prospective studies with larger sample size, different ethnicities, and more polymorphisms are required to confirm our findings.
Acknowledgments
This study was supported by the grant of State Clinical Key Specialty Construction Project (Pediatric Surgery) 2013 (no GJLCZD1301) and the grant of Clinical Medicine Research and Transformation Center of Brain Injury in Premature Infant in Guangzhou (no 520101-2150092). We thank Hongjiao Chen, Yanlu Tong, and Hezhen Wang for their assistance in DNA extraction and Zhang Zhao and Jin-Hua Hu for their assistance in sample collection and medical histories information collection.
Disclosure
The authors report no conflicts of interest in this work.
References
Rivera MN, Haber DA. Wilms’ tumour: connecting tumorigenesis and organ development in the kidney. Nat Rev Cancer. 2005;5(9):699–712. | ||
Chu A, Heck JE, Ribeiro KB, et al. Wilms’ tumour: a systematic review of risk factors and meta-analysis. Paediatr Perinat Epidemiol. 2010;24(5):449–469. | ||
Stiller CA, Parkin DM. International variations in the incidence of childhood renal tumours. Br J Cancer. 1990;62(6):1026–1030. | ||
Bao PP, Li K, Wu CX, et al. [Recent incidences and trends of childhood malignant solid tumors in Shanghai, 2002–2010]. Zhonghua Er Ke Za Zhi. 2013;51(4):288–294. | ||
Scott RH, Stiller CA, Walker L, Rahman N. Syndromes and constitutional chromosomal abnormalities associated with Wilms tumour. J Med Genet. 2006;43(9):705–715. | ||
Scott RH, Douglas J, Baskcomb L, et al. Constitutional 11p15 abnormalities, including heritable imprinting center mutations, cause nonsyndromic Wilms tumor. Nat Genet. 2008;40(11):1329–1334. | ||
Little SE, Hanks SP, King-Underwood L, et al. Frequency and heritability of WT1 mutations in nonsyndromic Wilms’ tumor patients: a UK Children’s Cancer Study Group Study. J Clin Oncol. 2004;22(20):4140–4146. | ||
Harris CC, Hollstein M. Clinical implications of the p53 tumor-suppressor gene. N Engl J Med. 1993;329(18):1318–1327. | ||
Levine AJ. p53, the cellular gatekeeper for growth and division. Cell. 1997;88(3):323–331. | ||
Sager R. Tumor suppressor genes: the puzzle and the promise. Science. 1989;246(4936):1406–1412. | ||
Xu H, el-Gewely MR. P53-responsive genes and the potential for cancer diagnostics and therapeutics development. Biotechnol Annu Rev. 2001;7:131–164. | ||
Dumont P, Leu JI, Della Pietra AC 3rd, George DL, Murphy M. The codon 72 polymorphic variants of p53 have markedly different apoptotic potential. Nat Genet. 2003;33(3):357–365. | ||
Thomas M, Kalita A, Labrecque S, Pim D, Banks L, Matlashewski G. Two polymorphic variants of wild-type p53 differ biochemically and biologically. Mol Cell Biol. 1999;19(2):1092–1100. | ||
Siddique M, Sabapathy K. Trp53-dependent DNA-repair is affected by the codon 72 polymorphism. Oncogene. 2006;25(25):3489–3500. | ||
Whibley C, Pharoah PD, Hollstein M. p53 polymorphisms: cancer implications. Nat Rev Cancer. 2009;9(2):95–107. | ||
Klug SJ, Ressing M, Koenig J, et al. TP53 codon 72 polymorphism and cervical cancer: a pooled analysis of individual data from 49 studies. Lancet Oncol. 2009;10(8):772–784. | ||
Dahabreh IJ, Linardou H, Bouzika P, Varvarigou V, Murray S. TP53 Arg72Pro polymorphism and colorectal cancer risk: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2010;19(7):1840–1847. | ||
Xu T, Xu ZC, Zou Q, Yu B, Huang XE. P53 Arg72Pro polymorphism and bladder cancer risk – meta-analysis evidence for a link in Asians but not Caucasians. Asian Pac J Cancer Prev. 2012;13(5):2349–2354. | ||
Dahabreh IJ, Schmid CH, Lau J, Varvarigou V, Murray S, Trikalinos TA. Genotype misclassification in genetic association studies of the rs1042522 TP53 (Arg72Pro) polymorphism: a systematic review of studies of breast, lung, colorectal, ovarian, and endometrial cancer. Am J Epidemiol. 2013;177(12):1317–1325. | ||
Tian X, Dai S, Sun J, Jiang S, Jiang Y. Association between TP53 Arg72Pro polymorphism and leukemia risk: a meta-analysis of 14 case-control studies. Sci Rep. 2016;6:24097. | ||
Cost NG, Mitui M, Khokhar S, Wickiser JE, Baker LA, Rakheja D. TP53 codon 72 polymorphisms in favorable histology Wilms tumors. Pediatr Blood Cancer. 2012;59(2):326–328. | ||
Andrade RC, Cardoso LC, Ferman SE, et al. Association of TP53 polymorphisms on the risk of Wilms tumor. Pediatr Blood Cancer. 2014;61(3):436–441. | ||
Fu W, Zhu J, Xiong SW, et al. BARD1 gene polymorphisms confer nephroblastoma susceptibility. EBioMedicine. Epub 2017 Jan 31. doi: 10.1016/j.ebiom.2017.01.038. | ||
He J, Wang F, Zhu J, et al. Association of potentially functional variants in the XPG gene with neuroblastoma risk in a Chinese population. J Cell Mol Med. 2016;20(8):1481–1490. | ||
He J, Yang T, Zhang R, et al. Potentially functional polymorphisms in the LIN28B gene contribute to neuroblastoma susceptibility in Chinese children. J Cell Mol Med. 2016;20(8):1534–1541. | ||
He J, Zhang R, Zou Y, et al. Evaluation of GWAS-identified SNPs at 6p22 with neuroblastoma susceptibility in a Chinese population. Tumour Biol. 2016;37(2):1635–1639. | ||
He J, Zhong W, Zeng J, et al. LMO1 gene polymorphisms contribute to decreased neuroblastoma susceptibility in a Southern Chinese population. Oncotarget. 2016;7(16):22770–22778. | ||
Zhang R, Zou Y, Zhu J, et al. The association between GWAS-identified BARD1 gene SNPs and neuroblastoma susceptibility in a Southern Chinese population. Int J Med Sci. 2016;13(2):133–138. | ||
Zheng J, Zhang R, Zhu J, et al. Lack of associations between XPC gene polymorphisms and neuroblastoma susceptibility in a Chinese population. Biomed Res Int. 2016;2016:2932049. | ||
He J, Qiu LX, Wang MY, et al. Polymorphisms in the XPG gene and risk of gastric cancer in Chinese populations. Hum Genet. 2012;131(7):1235–1244. | ||
Beckwith JB. National Wilms Tumor Study: an update for pathologists. Pediatr Dev Pathol. 1998;1(1):79–84. | ||
Isobe M, Emanuel BS, Givol D, Oren M, Croce CM. Localization of gene for human p53 tumour antigen to band 17p13. Nature. 1986;320(6057):84–85. | ||
Finlay CA, Hinds PW, Levine AJ. The p53 proto-oncogene can act as a suppressor of transformation. Cell. 1989;57(7):1083–1093. | ||
Scopinaro MJ, Casak SJ. Paediatric oncology in Argentina: medical and ethical issues. Lancet Oncol. 2002;3(2):111–117. | ||
Petitjean A, Achatz MI, Borresen-Dale AL, Hainaut P, Olivier M. TP53 mutations in human cancers: functional selection and impact on cancer prognosis and outcomes. Oncogene. 2007;26(15):2157–2165. | ||
Frebourg T, Friend SH. Cancer risks from germline p53 mutations. J Clin Invest. 1992;90(5):1637–1641. | ||
Wang Y, Wu XS, He J, Ma T, Lei W, Shen ZY. A novel TP53 variant (rs78378222 A > C) in the polyadenylation signal is associated with increased cancer susceptibility: evidence from a meta-analysis. Oncotarget. 2016;7(22):32854–32865. | ||
Matlashewski GJ, Tuck S, Pim D, Lamb P, Schneider J, Crawford LV. Primary structure polymorphism at amino acid residue 72 of human p53. Mol Cell Biol. 1987;7(2):961–963. | ||
Marin MC, Jost CA, Brooks LA, et al. A common polymorphism acts as an intragenic modifier of mutant p53 behaviour. Nat Genet. 2000;25(1):47–54. | ||
Storey A, Thomas M, Kalita A, et al. Role of a p53 polymorphism in the development of human papillomavirus-associated cancer. Nature. 1998;393(6682):229–234. |
Supplementary material
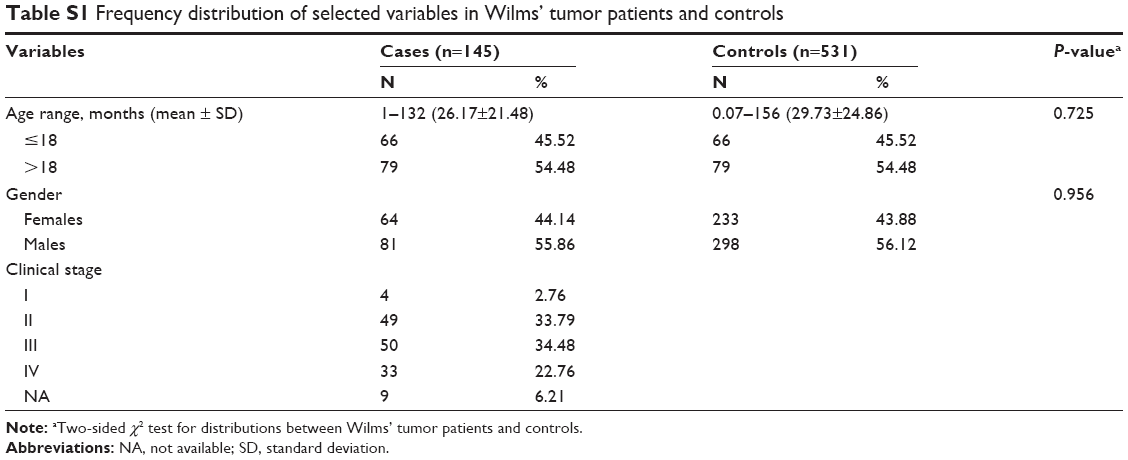 | Table S1 Frequency distribution of selected variables in Wilms’ tumor patients and controls |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.