Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 11 » Issue 1
Association between TNF-α -308 G/A polymorphism and COPD susceptibility: a meta-analysis update
Authors Zhang L, Gu H, Gu Y, Zeng X
Received 30 January 2016
Accepted for publication 14 April 2016
Published 22 June 2016 Volume 2016:11(1) Pages 1367—1379
DOI https://doi.org/10.2147/COPD.S105394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Lu Zhang,1 Hao Gu,2 Yihang Gu,2 Xiaoning Zeng2
1Clinical Research Centre, 2Department of Respiratory & Critical Care Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China
Background and objective: The association between TNF-α -308 G/A polymorphism and COPD remains controversial due to insufficiently strict study designs and small group sizes among different studies. In the present study, a meta-analysis update which followed a stricter procedure was performed to obtain a clearer understanding of this association.
Methods: A comprehensive database search was conducted to identify the case–control studies published up to July 2015 which reported an association between the TNF-α -308 G/A polymorphism and COPD risk. Data were extracted to calculate pooled odds ratios with 95% confidence intervals under the most appropriate genetic and allelic models. Sensitivity was analyzed, and heterogeneity as well as publication bias was assessed.
Results: Thirty-eight eligible studies, comprising 3,951 COPD cases and 5,110 controls, were included in this study, among which 22 studies comprising 2,067 COPD cases and 2,167 controls were performed in Asians, and 16 studies comprising 1,884 COPD cases and 2,943 controls were in non-Asians. The overall result showed that TNF-α -308 G/A polymorphisms were significantly associated with increased COPD risk in both the codominant genetic and allelic models. Individuals with the GA or AA genotype were more susceptible to COPD development than those with the GG genotype. In addition, individuals with the AA genotype were more susceptible to developing COPD than those with the GA genotype. The subgroup analysis stratified by ethnicity supported the results in Asians but not in non-Asians. However, no association was found between TNF-α -308 G/A polymorphisms and COPD susceptibility either in Asians or in non-Asians in the meta-analysis conducted with restriction to former/current smokers.
Conclusion: The present meta-analysis suggested that the TNF-α -308 G/A polymorphism was associated with an increased risk of COPD among Asians but not in non-Asians. Furthermore, individuals with the AA genotype of TNF-α -308 were more susceptible to developing COPD.
Keywords: cytokine, genotype, ethnicity, COPD, smokers
Introduction
COPD is characterized by the progressive development of airflow limitation that is not fully reversible.1 COPD has been estimated to become the third leading cause of death in the world by 2020.2 According to statistics, COPD is ranked as the third and fourth leading cause of death in rural and urban areas of the People’s Republic of China, respectively.3 Cigarette smoking is considered to be a major environmental factor contributing to the development of COPD. However, only 25%–40% of cigarette smokers develop COPD,4 indicating that other components may be involved in COPD development.5–7
Accumulated evidence indicates that genetic factors influence COPD susceptibility. A number of studies have demonstrated that TNF-α is relevant to the pathogenesis of COPD, including involvement in neutrophil release from the bone marrow and neutrophil activation.8 Increased levels of TNF-α have been found in the sputum,9 bronchoalveolar lavage fluid, bronchial biopsies, and circulation10 of COPD patients. Genetic polymorphism analyses have identified several single-nucleotide polymorphisms in the TNF-α gene associated with COPD risk, including −238 G/A, −308 G/A, −376 G/A, −863 C/A, −857 T/C, −1031 T/C, and +489 G/A.11–14 Among these, the −308 G/A polymorphism is the best studied; however, a consistent association has not yet been found.15 Studies in Asians16,17 and non-Asians18 have demonstrated that the TNF-α −308 G/A polymorphism is associated with an increased risk of COPD. However, other studies in both Asians19,20 and non-Asians21–25 have showed opposite results.
A limited number of meta-analyses have been performed to further clarify the association between the TNF-α −308 polymorphisms and COPD risk;26–29 however, a firm conclusion has not been achieved because of several limitations in the previous meta-analyses including 1) failure to check the Hardy–Weinberg equilibrium (HWE), 2) lack of quality assessment, 3) inappropriate genetic model, and 4) a limited number of included studies. All these factors have led to considerable argument regarding the studies’ paradoxical conclusions. Additionally, only studies published up to 2010 were included in the most recent meta-analysis.29 In the present study, we conducted a meta-analysis update with studies published up to July 2015. Additionally, we followed a stricter procedure: 1) only studies in accordance with HWE were included, 2) all included studies had a quality score no less than 5 because studies with quality scores ≤4 are considered as low-quality studies,30 and 3) the most appropriate genetic model was employed. Thus, our report presented more detailed information which will not only help obtain a clearer understanding of the association between TNF-α −308 polymorphisms and COPD but also help pave the way for individualized treatment of COPD patients.
Materials and methods
The current meta-analysis was conducted according to the guidelines presented in the review by Sagoo et al.31
Search strategy for publication
A comprehensive search was conducted using the terms “TNF”, “tumor necrosis factor”, “polymorphism”, and “COPD” in several electronic databases (PubMed, EMBASE, ISI Web of Science, Cochrane Central Register of Controlled Trials, China National Knowledge Infrastructure, Database of Chinese Scientific and Technical Periodicals, China Biology Medicine disc database, and WANFANG databases) to identify studies that examined the association of TNF-α −308 (rs1800629) G/A polymorphisms with COPD published up to July 2015. Additional studies were identified by manually reviewing the bibliographies of relevant articles as well as relevant review articles. The search was performed without restriction regarding race, ethnicity, or geographic area. Only published studies with full text in English or Chinese were included. Concerning duplicate populations included in several publications, only the most recent or complete study was included in this meta-analysis.
Eligibility criteria
Eligible studies were required to meet the following inclusion criteria: 1) evaluation of the TNF-α −308 polymorphism and COPD risk, 2) employment of a case–control design, 3) inclusion of adult subjects within the case group or control group, 4) disclosure of the number of individual genotypes with COPD in cases and controls, and 5) congruency of the distribution of genotypes among controls with HWE. Studies were excluded if 1) they contained overlapping data with another study, 2) the number of wild-type genotypes or alleles was not stated, and 3) they reviewed only editorials, reviews, and abstracts. All articles were reviewed to determine eligibility by two independent investigators. A consensus with a third reviewer was needed if there was any disagreement between the two investigators.
Data extraction
Data were checked and extracted from each study by two independent investigators. Data inconsistencies or discrepancies were resolved by consensus of all investigators before being standardized into a unified dataset. The following information was extracted from each study: first author’s name, publication year, country/territory, numbers of cases and controls, ethnicity of the study population, source of control subjects, smoking status in cases and controls, and genotype and allele distribution.
Quality assessment
The Newcastle–Ottawa quality assessment scale32 was applied to assess the quality of each study by two investigators. The quality was evaluated with three major components: 1) selection of cases and controls, 2) comparability of cases and controls, and 3) ascertainment of exposure. Any disagreement was resolved by a third investigator. Only studies with a quality score ≥5 were included in the current study.
Statistical analysis
Statistical analysis was performed according to standard procedures.30 Pooled odds ratios (ORs) were calculated with the Mantel–Haenszel (M–H) mean of the logarithm with a 95% confidence interval (CI). First, an allele comparison was conducted to determine the allele risk. Second, OR1, OR2, and OR3 were explored for the genotypes (GG vs AA [OR1], GG vs GA [OR2], and GA vs AA [OR3]) to identify the most appropriate genetic model. When OR1 = OR3 ≠1 and OR2 =1, a recessive model was suggested. When OR1 = OR2 ≠1 and OR3 =1, then a dominant model was suggested. When OR1 > OR2 >1 and OR1 > OR3 >1 (or OR1 < OR2 <1 and OR1 < OR3 <1), then a codominant model was suggested.33 Lastly, the most appropriate genetic model was used to pool the results.
Heterogeneity was assessed by using the chi-square-based Cochran Q-test, which was considered significant if P<0.10, and the I2 statistic. If I2>50%, the random-effect model was adopted as the pooling method; otherwise, the fixed-effect model was used. To explore the source of the heterogeneity, subgroup analyses were performed with respect to ethnicity and smoking status.
A sensitivity analysis was conducted to assess the stability of the results. One study at a time was excluded to evaluate how robust the pooled estimator was. Publication bias was estimated by using Egger’s test.
All statistical analyses were performed with STATA version 11.0. A P-value <0.05 was considered statistically significant.
Results
Study characteristics
The flow diagram in Figure 1 summarizes the selection process carried out for this meta-analysis. A total of 38 eligible articles were included in the current meta-analysis, comprising 3,951 COPD cases and 5,110 controls.11–13,16,18,19,22,24,34–63 Twenty articles were published in English and 18 in Chinese. There were 16 studies performed in non-Asians which comprised 1,884 COPD cases and 2,943 controls and 22 studies in Asians which comprised 2,067 COPD cases and 2,167 controls. Fifteen studies contained sufficient information for subgroup analysis by smoking status. All of the cases were confirmed by the diagnostic criteria of COPD.64–68 The genotype distributions of the TNF-α −308 polymorphism were in accordance with HWE in the controls of all the studies. Based on the quality assessment scale for case–control studies, two studies scored 5 points, 22 studies scored 6 points, eleven studies scored 7 points, and the other three scored 8 points. The characteristics of these studies are shown in Table 1. The detailed genotype, allele information, and HWE results are listed in Table 2.
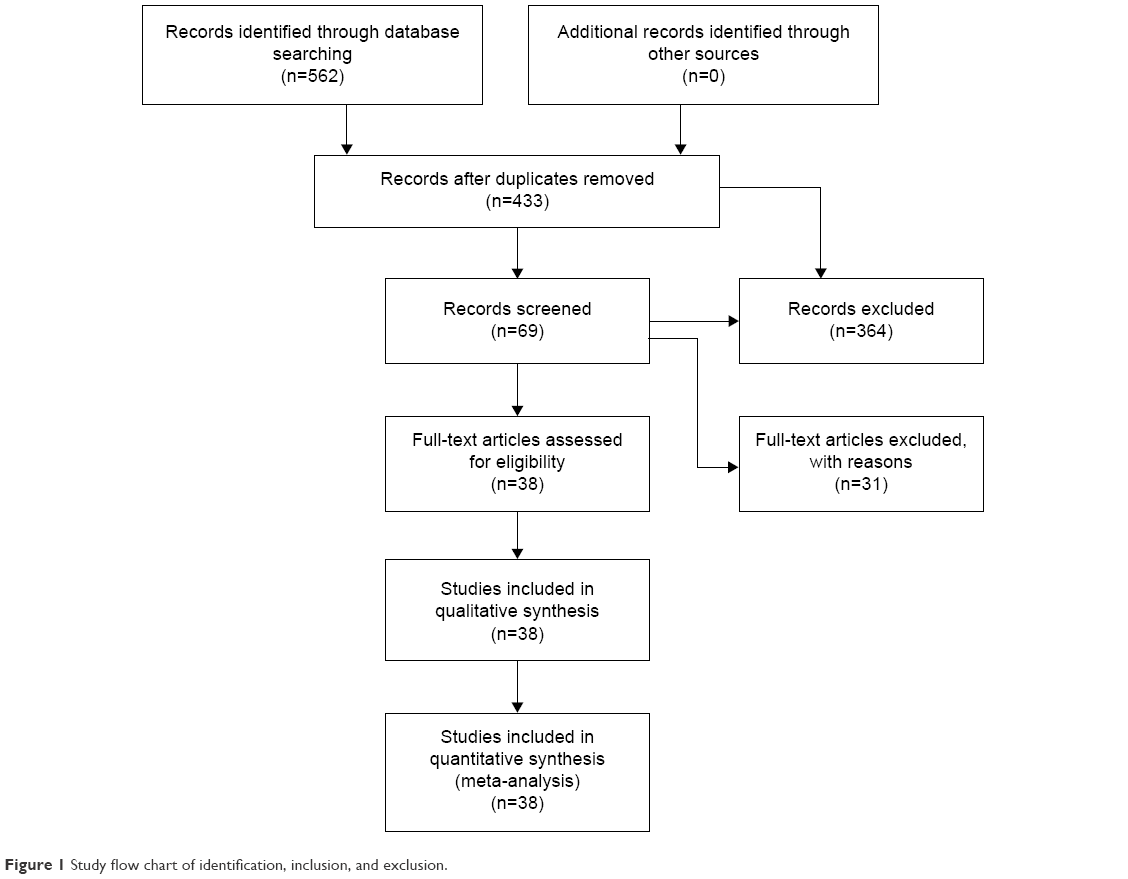 | Figure 1 Study flow chart of identification, inclusion, and exclusion. |
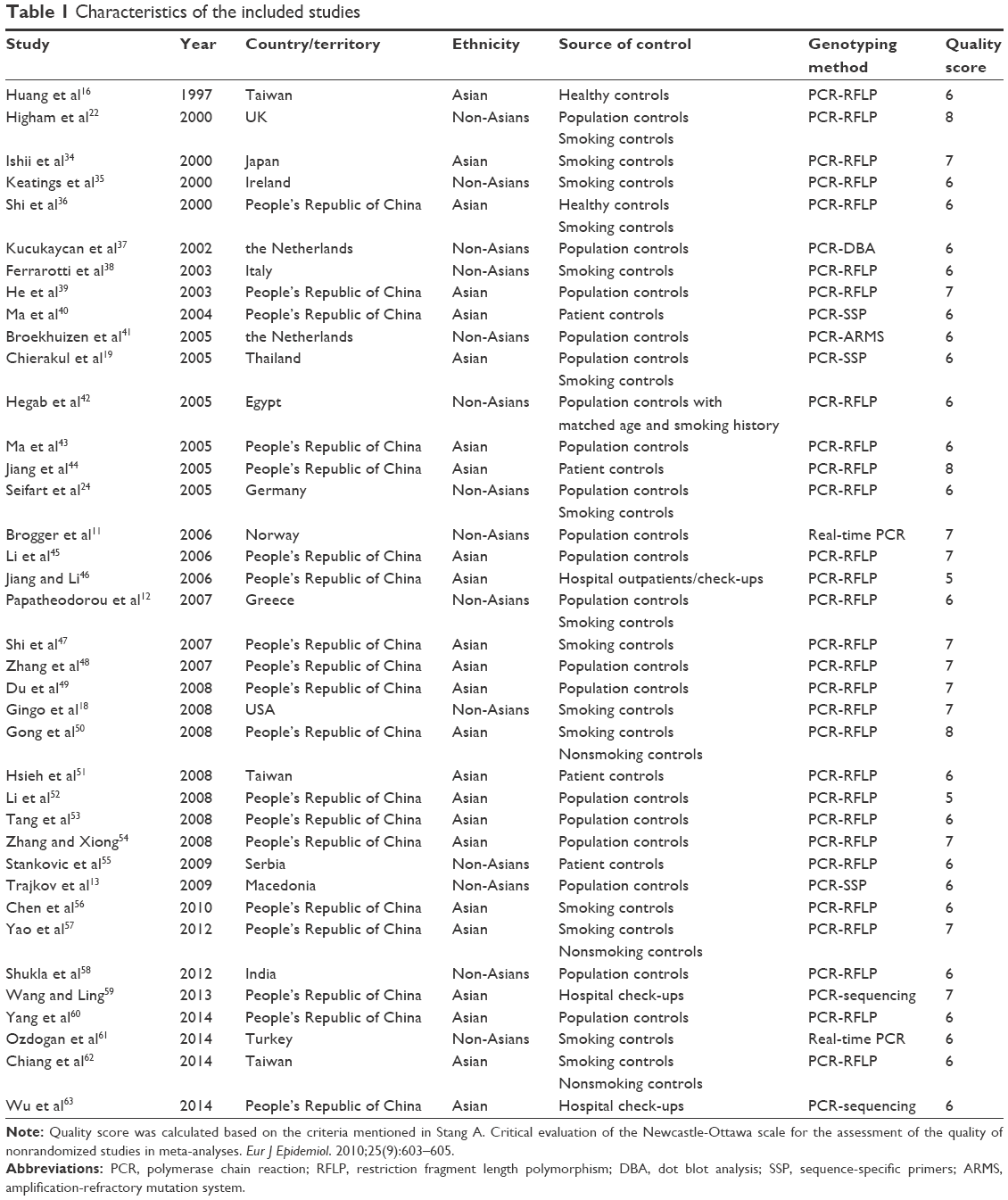 | Table 1 Characteristics of the included studies |
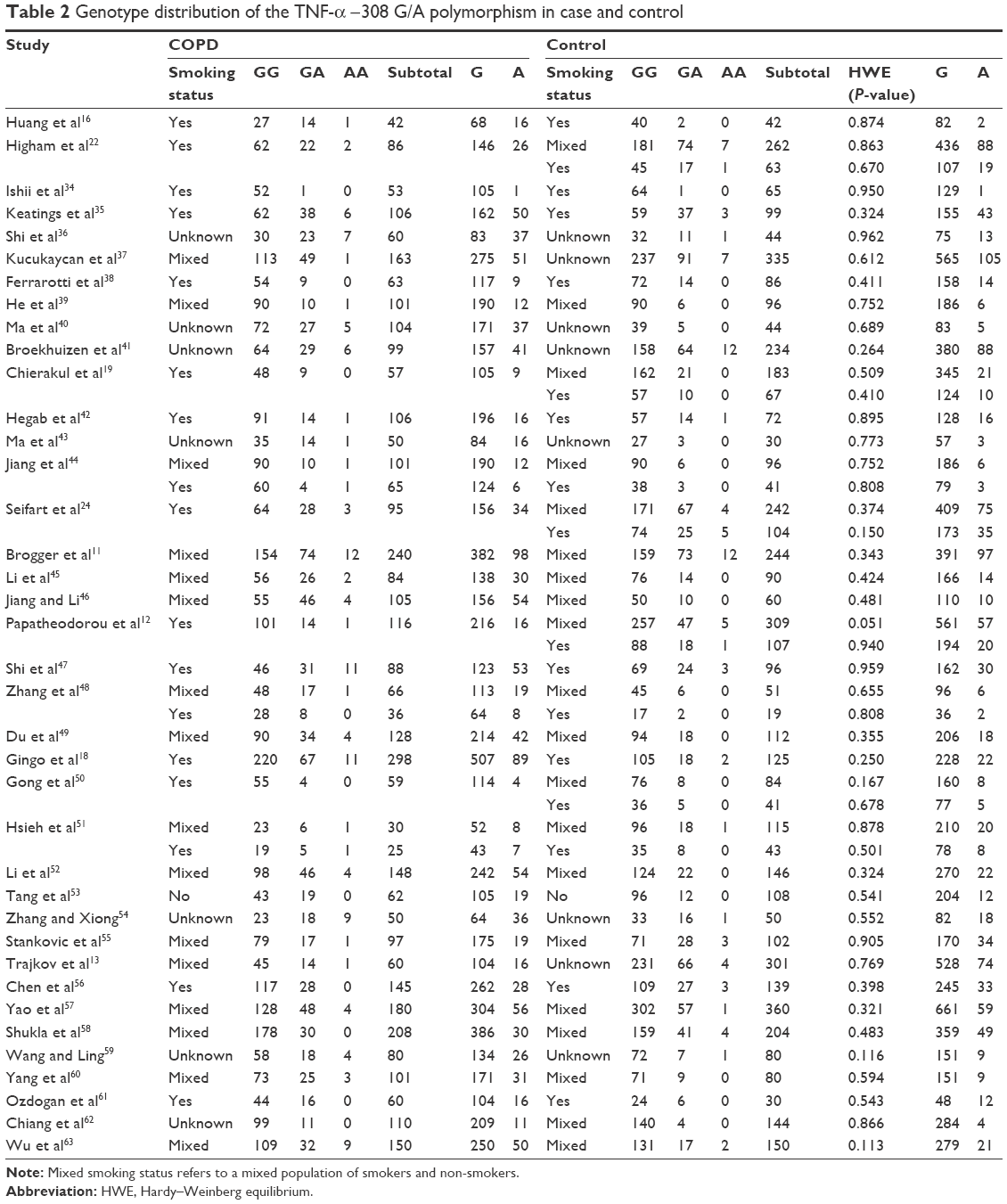 | Table 2 Genotype distribution of the TNF-α −308 G/A polymorphism in case and control |
Meta-analysis results
A summary of the meta-analysis results concerning association between TNF-α −308 polymorphism and COPD risk is provided in Table 3. The A allele was associated with an increased COPD risk in the overall population (OR =1.56, 95% CI 1.29–1.89, P=0.000 for heterogeneity, I2=70.8%) (Figure 2). The estimated OR1, OR2, and OR3 were 1.776 (P=0.000), 1.513 (P=0.211), and 1.216 (P=0.000), respectively, suggesting a codominant model as the most appropriate genetic model. Then, the pooled ORs were calculated under the codominant genetic model. OR was 1.78 for GG vs AA and 1.51 for GG vs GA (Figures 3 and 4), demonstrating a significant association between TNF-α −308 polymorphism and COPD in the overall population. Individuals with AA genotype were more susceptible to develop COPD than those with GA genotype. To identify the origin of heterogeneity, a subgroup analysis stratified by ethnicity was conducted. As shown in Figures 2–4, a stronger correlation of the polymorphism with COPD risk was found in Asians under the genetic model (OR =3.25 for GG vs AA and OR =2.22 for GG vs GA), and similar results were observed in the allelic model. Interestingly, the AA genotype carriers had a higher risk of developing COPD than GA carriers in Asian patients. Conversely, no association was found in non-Asians in the genetic model (OR =1.05 for GG vs AA and OR =1.00 for GG vs GA). Notably, heterogeneity was significantly decreased when stratified analysis was performed by ethnicity status in both models, indicating the ethnicity contributed partly to heterogeneity, and similar results were found in the allelic model.
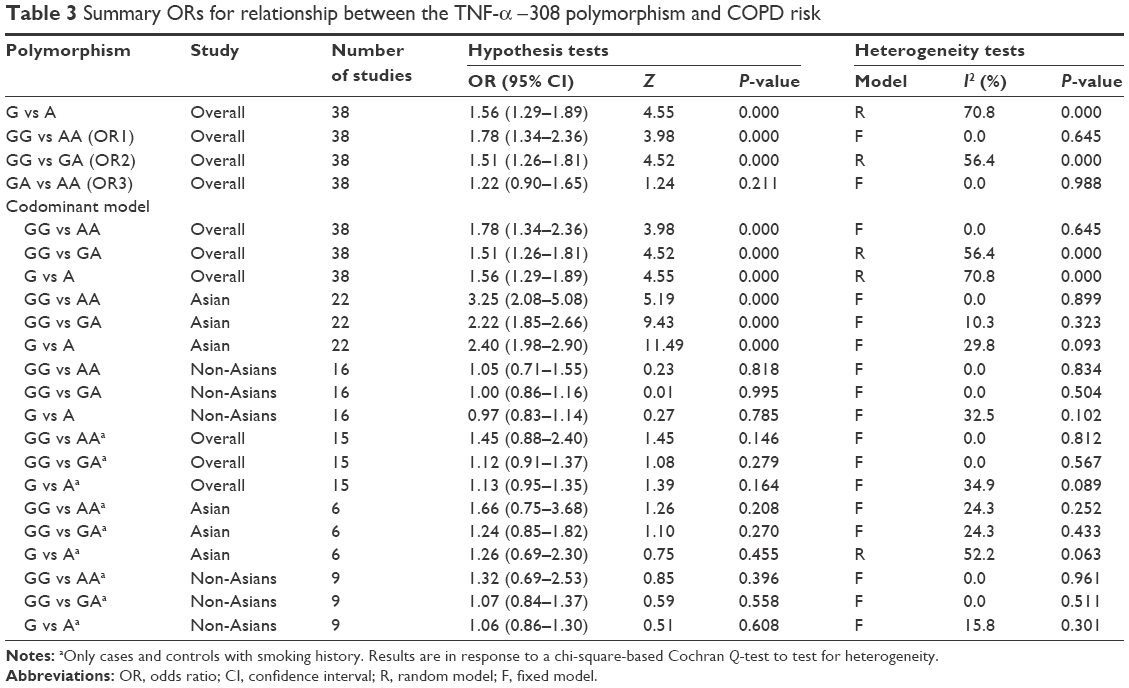 | Table 3 Summary ORs for relationship between the TNF-α −308 polymorphism and COPD risk |
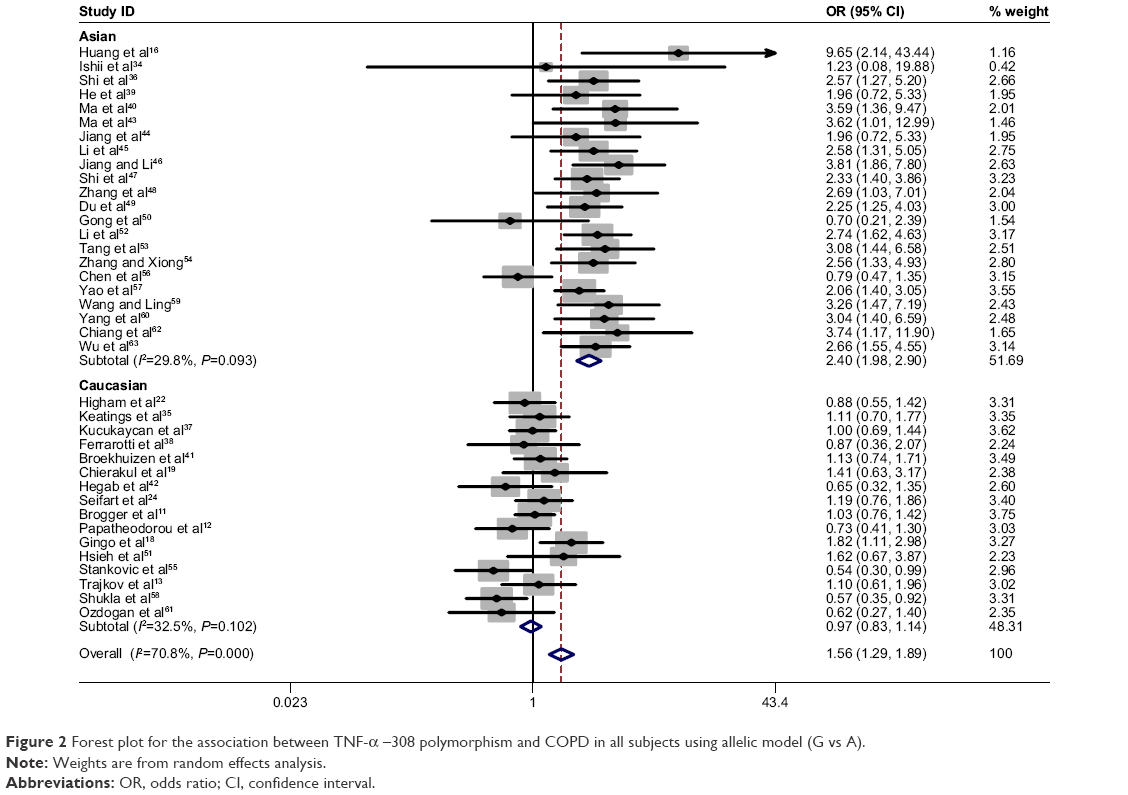 | Figure 2 Forest plot for the association between TNF-α –308 polymorphism and COPD in all subjects using allelic model (G vs A). |
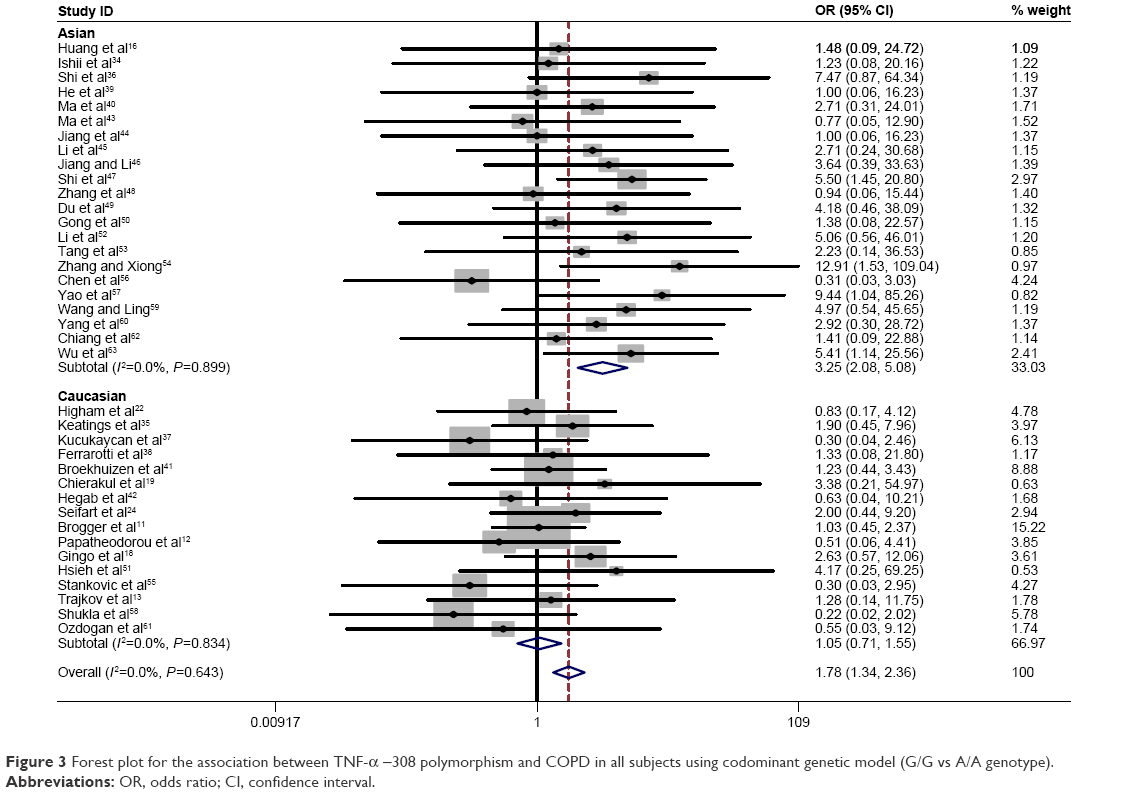 | Figure 3 Forest plot for the association between TNF-α −308 polymorphism and COPD in all subjects using codominant genetic model (G/G vs A/A genotype). |
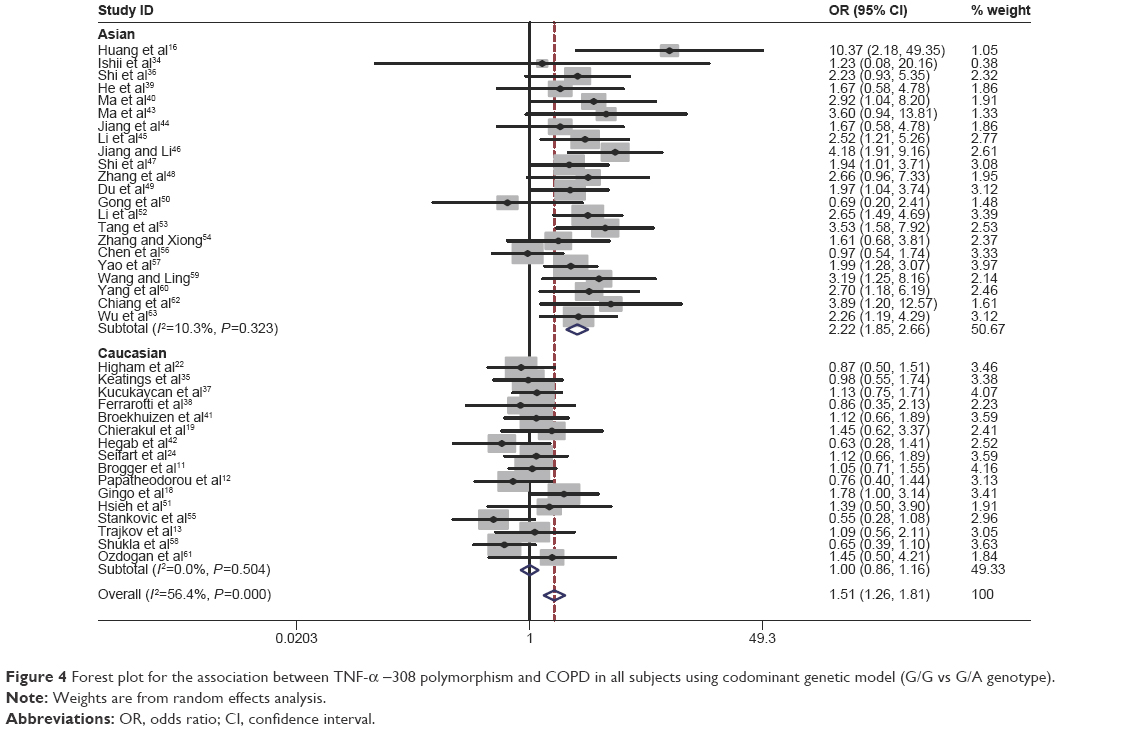 | Figure 4 Forest plot for the association between TNF-α −308 polymorphism and COPD in all subjects using codominant genetic model (G/G vs G/A genotype). |
Specific environmental factors, such as smoking, may contribute to the distribution of genetic polymorphisms.69 Moreover, there was a difference in the TNF-α −308 polymorphism between smoking and nonsmoking COPD patients.45 To minimize the effect of cigarette smoking on the association between the TNF-α −308 G/A polymorphism and COPD risk, a second meta-analysis was conducted with studies in which the COPD cases and the controls were current/former smokers. Interestingly, no significant association was found between the TNF-α −308 polymorphism and COPD risk either in Asian smokers or in non-Asian smokers. The statistics in non-Asians included OR =1.32 for GG vs AA and OR =1.07 for GG vs GA. The statistics in Asians included OR =1.66 for GG vs AA and OR =1.24 for GG vs GA (Figures 5 and 6). Our study indicated that the A allele was not a risk factor for the development of COPD in smoking populations.
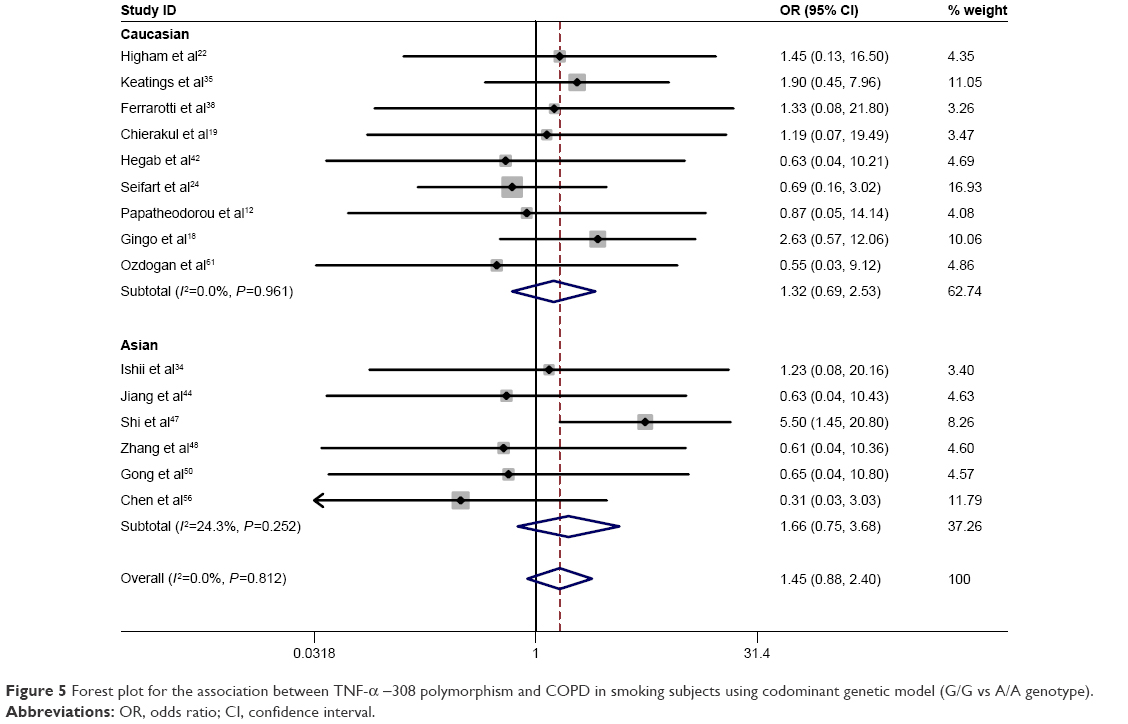 | Figure 5 Forest plot for the association between TNF-α −308 polymorphism and COPD in smoking subjects using codominant genetic model (G/G vs A/A genotype). |
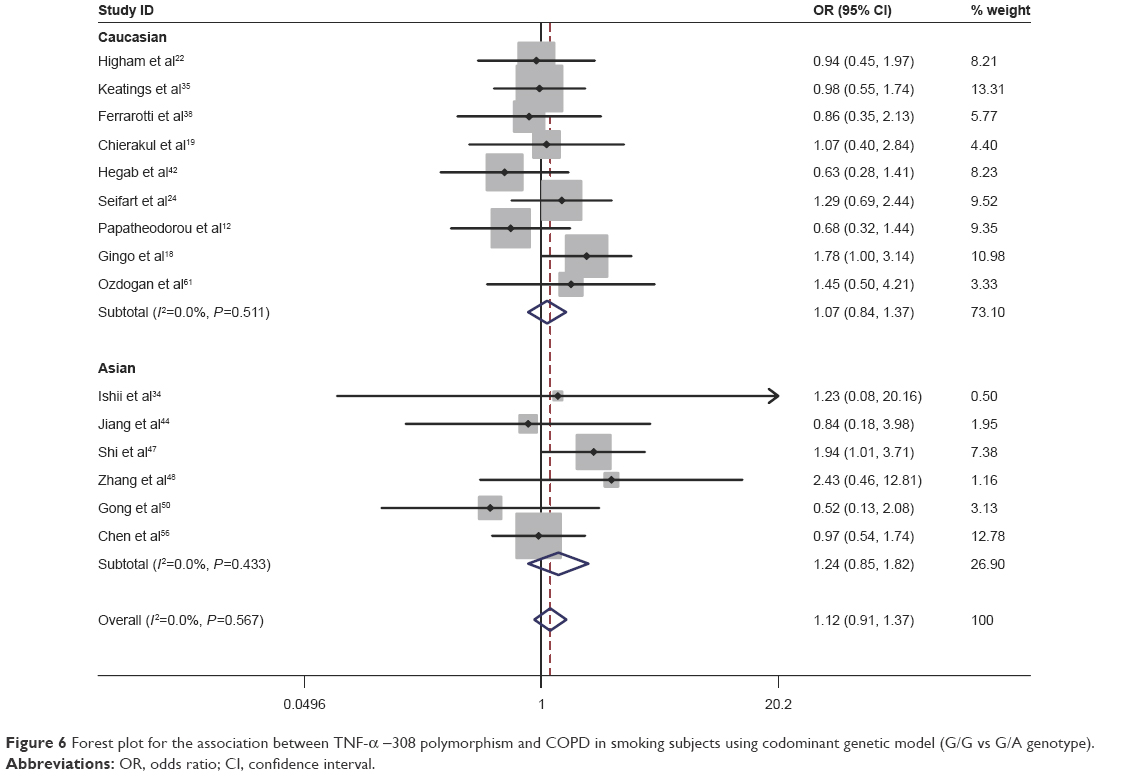 | Figure 6 Forest plot for the association between TNF-α −308 polymorphism and COPD in smoking subjects using codominant genetic model (G/G vs G/A genotype). |
Sensitivity analysis
Sensitivity analysis was performed by sequentially excluding each study to assess the stability of the results in this meta-analysis. The corresponding pooled ORs were not materially altered in the overall meta-analysis (Figure 7). In the meta-analysis with restriction to smokers, two studies18,47 were found to be the source of heterogeneity in Asian smokers (Figure 8). After excluding these two studies from the analysis, the pooled OR did not vary significantly, indicating that the results were relatively reliable (data not shown).
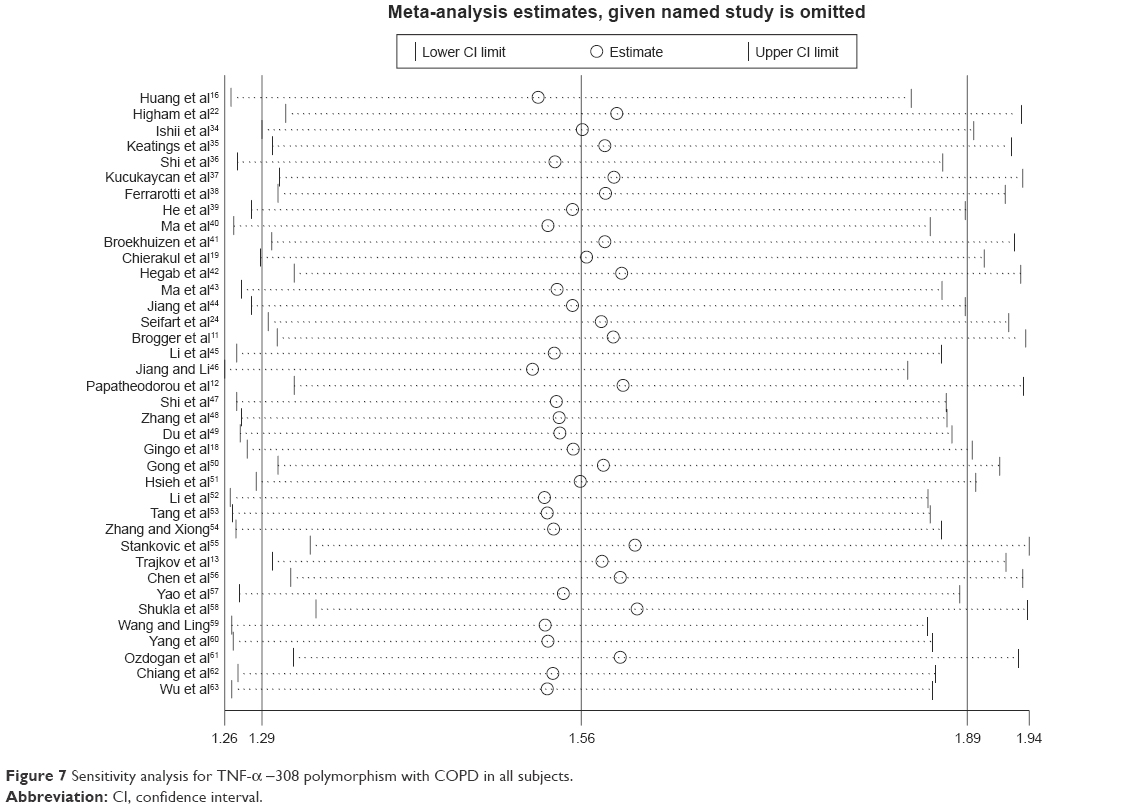 | Figure 7 Sensitivity analysis for TNF-α −308 polymorphism with COPD in all subjects. |
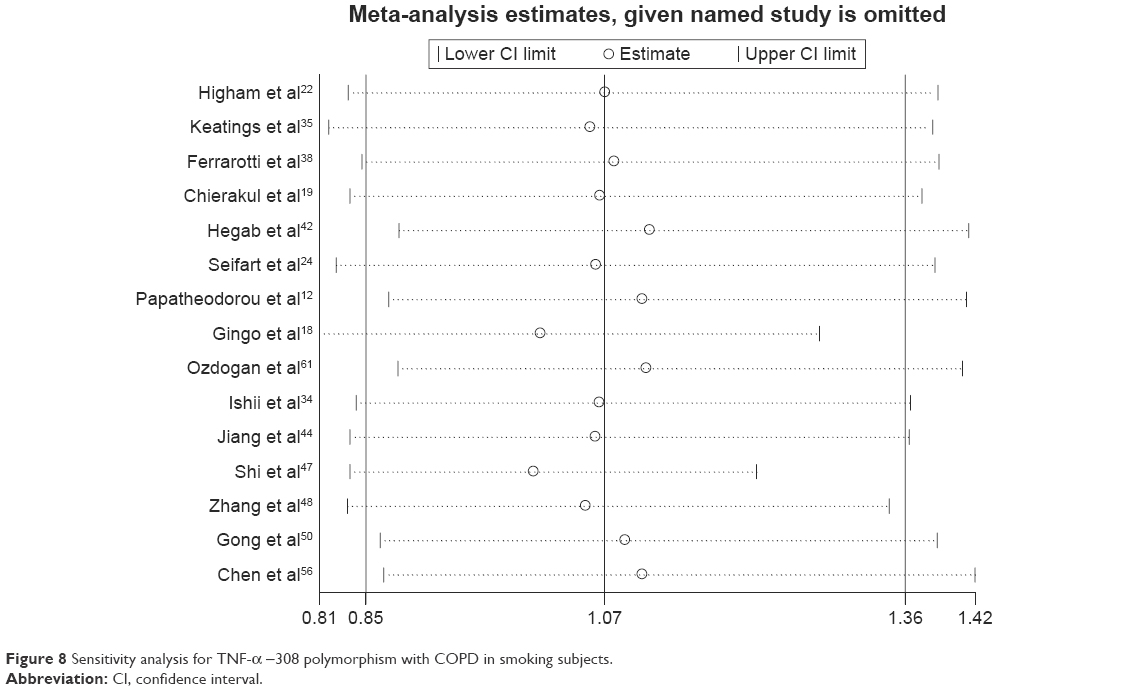 | Figure 8 Sensitivity analysis for TNF-α −308 polymorphism with COPD in smoking subjects. |
Publication bias
As shown in Figure 9, Egger’s test was performed to assess the publication bias of the literature. No publication bias was detected (P=0.726).
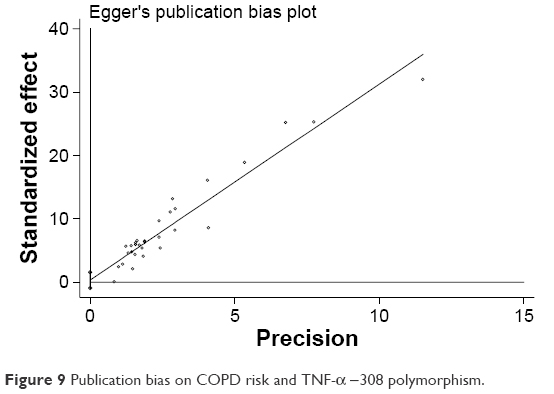 | Figure 9 Publication bias on COPD risk and TNF-α −308 polymorphism. |
Discussion
In the present meta-analysis update, we conducted a comprehensive database search for potential articles published up to July 2015 to evaluate the association between TNF-α −308 polymorphism and COPD risk, and several of the articles were not included in the previous meta-analysis. To our knowledge, this is the first report to analyze the association between TNF-α −308 polymorphism and COPD risk under the codominant genetic model. Thus, more detailed information can be achieved under this genetic model. Finally, a total of 38 studies with 3,951 patients and 5,110 controls were included in the meta-analysis. The results showed a significant association between the TNF-α −308 polymorphism and COPD susceptibility in the overall population. Individuals with the A allele (GA or AA) were more susceptible to developing COPD than those with the GG genotype. Additionally, we further clarified that individuals with the AA genotype had a higher risk of developing COPD than those with the GA genotype (77.6% vs 51.3%). The previous meta-analysis investigating the current question employed a dominant genetic model, and did not provide detailed information about the AA and GA genotypes separately. Here, for the first time, our report indicated that carriers of the AA genotype of TNF-α −308 were the most vulnerable to COPD development.
To identify the origin of heterogeneity, a subgroup analysis stratified by ethnicity was conducted. In our study, significant associations were shown in Asians but not in non-Asians, which is consistent with the previous meta-analysis.28,29 Our data reconfirmed that the TNF-α −308 G/A polymorphism was associated with COPD risk even under a stricter study design and procedure. Furthermore, our study further identified a stronger correlation between the TNF-α −308 G/A polymorphism and COPD risk in Asians with the AA genotype compared with those with the GA genotype. Notably, heterogeneity was significantly decreased when the analysis stratified by ethnicity was performed. We speculated that it may be because that the A allele is more important for COPD susceptibility in Asians than in non-Asians.
To minimize the effect of smoking status on the association, a second meta-analysis restricted to smokers was conducted. Interestingly, no correlation was found between the TNF-α −308 G/A polymorphism and the risk of COPD in either Asian smokers or non-Asian smokers. This result was contrary to the previous meta-analysis which showed an obvious correlation between the TNF-α –308 G/A polymorphism and the risk of COPD in smokers. Although moderate heterogeneity was observed in Asian smokers in the allelic model, which may distort the result, the pooled OR did not vary significantly after the removal of two studies that were considered the origin of the heterogeneity. This indicated that the results of this meta-analysis in the smokers were reliable. The opposite results may be attributed to the following: 1) the codominant model was adopted in the current study, which was different from the previous study (dominant model); and 2) due to stricter inclusion criteria, several studies were excluded from the current meta-analysis. Based on the results of our study, it seems that other factors may contribute to COPD development in smokers, and we speculated that the A allele may be a risk factor in nonsmokers; however, a firm conclusion should not be drawn until a larger number of studies with a sufficient number of nonsmokers can be included in the meta-analysis.
There are several limitations of the present meta-analysis that should be considered when explaining the results: 1) Even though we followed a strict procedure for data collection and data analysis to minimize the heterogeneity, several pooled ORs were obtained from heterogeneous studies. 2) There were not enough nonsmokers in the case and control groups to conduct a subgroup analysis to ascertain whether the A allele of TNF-α –308 was associated with the risk of COPD development in the nonsmoking population. 3) The numbers of studies were limited for this meta-analysis; some studies were excluded from the study. This selection bias may have an effect on the genotyping publication bias. What’s more, more studies are needed to further improve the power of the study. 4) The genotyping methods in the studies included are different, which may cause some bias on the result.
In conclusion, this meta-analysis update suggested that the A allele of TNF-α −308 is a risk factor for developing COPD. Additionally, individuals with the AA genotype appeared to be more susceptible to developing COPD than those with the GA genotype. Additionally, the subgroup analysis in Asians (but not in non-Asians) supported the results. The data presented in the current report may provide insight for COPD treatment based on patients’ genotype. In future, larger and more strictly controlled studies are needed to evaluate the relationship between gene polymorphisms and COPD. What’s more, relationship between gene polymorphisms and COPD in nonsmoking populations should be explored to further elucidate if gene polymorphism is an independent risk factor associated with the development of COPD, which will favor the development of effective prevention and treatment methods for COPD in nonsmokers.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No 81001428), the Jiangsu Province Scientific Research Innovation Project of University Graduate Students (KYLX15_0979), the Jiangsu Province Special Program of Medical Science (BL2012012), and a project funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD, JX10231802).
Disclosure
The authors declare no conflicts of interest in this work.
References
Rabe KF, Hurd S, Anzueto A, Barnes PJ, Buist SA, Calverley P. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176(6):532–555. | ||
Pauwels RA, Rabe KF. Burden and clinical features of chronic obstructive pulmonary disease (COPD). Lancet. 2004;364(9434):613–620. | ||
Fang X, Wang X, Bai C. COPD in China: the burden and importance of proper management. Chest. 2011;139(4):920–929. | ||
Lokke A, Lange P, Scharling H, Fabricius P, Vestbo J. Developing COPD: a 25 year follow up study of the general population. Thorax. 2006;61(11):935–939. | ||
Bascom R. Differential susceptibility to tobacco smoke: possible mechanisms. Pharmacogenetics. 1991;1(2):102–106. | ||
Silverman EK, Chapman HA, Drazen JM, et al. Genetic epidemiology of severe, early-onset chronic obstructive pulmonary disease. Risk to relatives for airflow obstruction and chronic bronchitis. Am J Respir Crit Care Med. 1998;157:1770–1778. | ||
Sandford AJ, Joos L, Pare PD. Genetic risk factors for chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2002;8(2):87–94. | ||
Keatings VM, Collins PD, Scott DM, Barnes PJ. Differences in interleukin-8 and tumor necrosis factor-alpha in induced sputum from patients with chronic obstructive pulmonary disease or asthma. Am J Respir Crit Care Med. 1996;153(2):530–534. | ||
Mueller R, Chanez P, Campbell AM, Bousquet J, Heusser C. Different cytokine patterns in bronchial biopsies in asthma and chronic bronchitis. Respir Med. 1996;90(2):79–85. | ||
Sun G, Stacey MA, Vittori E, Marini M, Bellini A, Kleimberg J. Cellular and molecular characteristics of inflammation in chronic bronchitis. Eur J Clin Invest. 1998;28(5):364–372. | ||
Brogger J, Steen VM, Eiken HG, Gulsvik A, Bakke P. Genetic association between COPD and polymorphisms in TNF, ADRB2 and EPHX1. Eur Respir J. 2006;27(4):682–688. | ||
Papatheodorou A, Latsi P, Vrettou C, Dimakou A, Chroneou A, Makrythanasis P. Development of a novel microarray methodology for the study of SNPs in the promoter region of the TNF-alpha gene: their association with obstructive pulmonary disease in Greek patients. Clin Biochem. 2007;40(12):843–850. | ||
Trajkov D, Mirkovska-Stojkovikj J, Petlichkovski A, Strezova A, Efinska-Mladenovska O, Sandevska E. Association of cytokine gene polymorphisms with chronic obstructive pulmonary disease in Macedonians. Iran J Allergy Asthma Immunol. 2009;8(1):31–42. | ||
Cordoba-Lanus E, Baz-Davila R, de-Torres JP, Rodriguez-Perez MC, Maca-Meyer N, Varo N. TNFA-863 polymorphism is associated with a reduced risk of chronic obstructive pulmonary disease: a replication study. BMC Med Genet. 2011;12:132. | ||
Wilson AG, di Giovine FS, Blakemore AI, Duff GW. Single base polymorphism in the human tumour necrosis factor alpha (TNF alpha) gene detectable by NcoI restriction of PCR product. Hum Mol Genet. 1992;1(5):353. | ||
Huang SL, Su CH, Chang SC. Tumor necrosis factor-alpha gene polymorphism in chronic bronchitis. Am J Respir Crit Care Med. 1997;156(5):1436–1439. | ||
Sakao S, Tatsumi K, Igari H, Shino Y, Shirasawa H, Kuriyama T. Association of tumor necrosis factor alpha gene promoter polymorphism with the presence of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;163(2):420–422. | ||
Gingo MR, Silveira LJ, Miller YE, Friedlander AL, Cosgrove SP, Chan ED. Tumour necrosis factor gene polymorphisms are associated with COPD. Eur Respir J. 2008;31(5):1005–1012. | ||
Chierakul N, Wongwisutikul P, Vejbaesya S, Chotvilaiwan K. Tumor necrosis factor-alpha gene promoter polymorphism is not associated with smoking-related COPD in Thailand. Respirology. 2005;10(1):36–39. | ||
Ezzeldin N, Shalaby A, Saad-Hussein A, Ezzeldin H, EI Lebedy D, Farouk H. Association of TNF-alpha -308G/A, SP-B 1580 C/T, IL-13 -1055 C/T gene polymorphisms and latent adenoviral infection with chronic obstructive pulmonary disease in an Egyptian population. Arch Med Sci. 2012;8(2):286–295. | ||
Teramoto S, Ishii T, Ishii M, Yamamoto H, Yamaguchi Y, Hibi S. Variation in the tumour necrosis factor-alpha gene is not associated with susceptibility to Asian COPD. Eur Respir J. 2008;31(3):682–683. | ||
Higham MA, Pride NB, Alikhan A, Morrell NW. Tumour necrosis factor-alpha gene promoter polymorphism in chronic obstructive pulmonary disease. Eur Respir J. 2000;15(2):281–284. | ||
Chappell S, Daly L, Morgan K, Baranes TG, Roca J, Rabinovich R. Variation in the tumour necrosis factor gene is not associated with susceptibility to COPD. Eur Respir J. 2007;30(4):810–812. | ||
Seifart C, Dempfle A, Plagens A, Seifart U, Clostermann U, Muller B. TNF-alpha-, TNF-beta-, IL-6-, and IL-10-promoter polymorphisms in patients with chronic obstructive pulmonary disease. Tissue Antigens. 2005;65(1):93–100. | ||
Tanaka G, Sandford AJ, Burkett K, Connett JE, Anthonisen NR, Pare PD. Tumour necrosis factor and lymphotoxin A polymorphisms and lung function in smokers. Eur Respir J. 2007;29(1):34–41. | ||
Castaldi PJ, Cho MH, Cohn M, Langerman F, Moran S, Tarragona N. The COPD genetic association compendium: a comprehensive online database of COPD genetic associations. Hum Mol Genet. 2010;19(3):526–534. | ||
Smolonska J, Wijmenga C, Postma DS, Boezen HM. Meta-analyses on suspected chronic obstructive pulmonary disease genes: a summary of 20 years’ research. Am J Respir Crit Care Med. 2009;180(7):618–631. | ||
Zhan P, Wang J, Wei SZ, Qian Q, Qiu X, Yu LK. TNF-308 gene polymorphism is associated with COPD risk among Asians: meta-analysis of data for 6,118 subjects. Mol Biol Rep. 2010;38(1):219–227. | ||
Zhang S, Wang C, Xi B, Li X. Association between the tumour necrosis factor-alpha-308G/A polymorphism and chronic obstructive pulmonary disease: an update. Respirology. 2011;16(1):107–115. | ||
Li Y, Guo B, Zhang L, Han J, Wu B, Xiong H. Association between C-589T polymorphisms of interleukin-4 gene promoter and asthma: a metaanalysis. Respir Med. 2008;102(7):984–992. | ||
Sagoo GS, Julian L, Higgins JPT. Systematic reviews of genetic association studies. PLoS Med. 2009;6(3):e1000028. | ||
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. | ||
Thakkinstian A, McElduff P, D’Este C, Duffy D, Attia J. A method for meta-analysis of molecular association studies. Stat Med. 2005;24(9):1291–1306. | ||
Ishii T, Matsuse T, Teramoto S, et al. Neither IL-1beta, IL-1 receptor antagonist, nor TNF-alpha polymorphisms are associated with susceptibility to COPD. Respir Med. 2000;94(9):847–851. | ||
Keatings VM, Cave SJ, Henry MJ, Morgan K, O’Connor CM, FitzGerald MX. A polymorphism in the tumor necrosis factor-alpha gene promoter region may predispose to a poor prognosis in COPD. Chest. 2000;118(4):971–975. | ||
Shi YZ, Wang XJ, Sun HM. Detection of TNF-a gene polymorphism in COPD patients. Basic Med Sci Clin. 2000;20:95. | ||
Kucukaycan M, Van Krugten M, Pennings HJ, et al. Tumor necrosis factor-alpha +489G/A gene polymorphism is associated with chronic obstructive pulmonary disease. Respir Res. 2002;3:29. | ||
Ferrarotti I, Zorzetto M, Beccaria M, et al. Tumour necrosis factor family genes in a phenotype of COPD associated with emphysema. Eur Respir J. 2003;21(3):444–449. | ||
He B, Jiang L, Ning L. Tumor necrosis factor-a gene 308 A allele can predispose to chronic obstructive pulmonary disease in smokers. Chin J Respir Crit Care Med. 2003;12:226–229. | ||
Ma Z, Zhang Z, Han Z. A study on relationship between tumor necrosis factor alpha gene promoter polymorphism and susceptibility to development of COPD. Pract Prev Med. 2004;11(5):417–419. | ||
Broekhuizen R, Grimble RF, Howell WM, et al. Pulmonary cachexia, systemic inflammatory profile, and the interleukin 1beta -511 single nucleotide polymorphism. Am J Clin Nutr. 2005;82(5):1059–1064. | ||
Hegab AE, Sakamoto T, Saitoh W, et al. Polymorphisms of TNFalpha, IL1beta, and IL1RN genes in chronic obstructive pulmonary disease. Biochem Biophys Res Commun. 2005;329(4):1246–1252. | ||
Ma Z, Zhang Z, Han Z. A study on the relationship between tumor necrosis factor a gene promoter polymorphism and the expressive levels of TNF-a protein. J Clin Intern Med. 2005;22(4):230–232. | ||
Jiang L, He B, Zhao MW, Ning LD, Li XY, Yao WZ. Association of gene polymorphisms of tumour necrosis factor-alpha and interleukin-13 with chronic obstructive pulmonary disease in Han nationality in Beijing. Chin Med J. 2005;118(7):541–547. | ||
Li Y, Zhai FZ, Du Y. Relationship of genetic polymorphisms of human betadefensin-1, tumor necrosis factor-alpha, mEH with chronic obstructive pulmonary disease. J Intern Med. 2006;45(3):225–226. | ||
Jiang P, Li Y. Association among genetic polymorphisms of HO-1, TNF-alpha and chronic obstructive pulmonary disease. J Shandong Univ (Health Sci). 2006;44(2):1253–1257. | ||
Shi YZ, Liu B, Zhang W; Study of the relationship between COPD and TNF-alpha gene polymorphism in Heilongjiang region. Chin J Tuberc Respir Dis. 2007;30:233–234. | ||
Zhang Y, Wang W, Xu SH. Association between polymorphism in the gene coding for tumor necrosis factor-alpha and chronic obstructive pulmonary disease. J Taishan Med Coll. 2007;28:106–109. | ||
Du Y, Sun HM, Li Y. The relationship between genetic polymorphism of tumor necrosis factor-alpha, human beta-defensin-1 and the development of chronic obstructive pulmonary disease. Clin Med J China. 2008;15:329–331. | ||
Gong Y, Jin ML, Ren T. Association of tumor necrosis factor gene promoter polymorphism with chronic obstructive pulmonary disease. Clin Med J China. 2008;15:166–169. | ||
Hsieh MH, Chong IW, Hwang JJ, Lee CH, Ho CK, Yu ML. Lack of associations between several polymorphisms in cytokine genes and the risk of chronic obstructive pulmonary diseases in Taiwan. Kaohsiung J Med Sci. 2008;24(3):126–137. | ||
Li Y, Du Y, Jiang P. Relationship of genetic polymorphisms of heme oxygenase-1, tumor necrosis factor-alpha, human betadefensin-1 with chronic obstructive pulmonary disease. Chin J Geriatr. 2008;27:333–336. | ||
Tang MQ, Mo HW, Cheng YQ. The relationship between the gene polymorphisms of TNF alpha and the genetic susceptibility to chronic obstructive pulmonary disease (COPD) with tuberculosis. J Qiqihar Med Coll. 2008;29:2949–2951. | ||
Zhang YQ, Xiong JL. Correlation of genetic polymorphisms of TNF-alpha and chronic obstructive pulmonary disease in North Chinese Han people. Clin Med China. 2008;24:129–130. | ||
Stankovic MM, Nestorovic AR, Tomovic AM, et al. TNF-alpha-308 promotor polymorphism in patients with chronic obstructive pulmonary disease and lung cancer. Neoplasma. 2009;56(4):348–352. | ||
Chen YC, Liu SF, Chin CH, et al. Association of tumor necrosis factor-alpha-863C/A gene polymorphism with chronic obstructive pulmonary disease. Lung. 2010;188(4):339–347. | ||
Yao ZG, Wang HY, Jia N; Study on the relationship between TNF-α+308,TNF-α+489 gene polymorphism and chronic obstructive pulmonary disease. Mod J Integr Trad Chin Western Med. 2012;21(22):2400–2405. | ||
Shukla RK, Kant S, Bhattacharya S, Mittal B. Association of cytokine gene polymorphisms in patients with chronic obstructive pulmonary disease. Oman Med J. 2012;27(4):285–290. | ||
Wang FE, Ling M. Relationship between tumor necrosis factor-α gene-308 promoter polymorphism and the susceptibility to chronic obstructive pulmonary disease in Xinjiang Uighur population. J Pract Med. 2013;29(22):3686–3689. | ||
Yang L, Li F, Yan M, Li X. Association of the CYP1A1 MspI and TNFα-308 polymorphisms with chronic obstructive pulmonary disease in Inner Mongolia. Genet Mol Res. 2014;13(2):3209–3217. | ||
Ozdogan N, Tutar N, Demir R, Saatci C, Kanbay A, Buyukoglan H. [Is TNF-alpha gene polymorphism related to pulmonary functions and prognosis as determined by FEV1, BMI, COPD exacerbation and hospitalization in patients with smoking-related COPD in a Turkish population?]. Rev Port Pneumol. 2014;20(6):305–310. Portuguese. | ||
Chiang CH, Chuang CH, Liu SL. Transforming growth factor-beta1 and tumor necrosis factor-alpha are associated with clinical severity and airflow limitation of COPD in an additive manner. Lung. 2014;192(1):95–102. | ||
Wu SM, Wang FE, Ling M. Relationship between tumor necrosis factor-α gene promoter polymorphism and susceptibility to development of COPD in Xinjiang Kazakh population. J Xi’an Jiao Tong Univ. 2014;35(6):820–823. | ||
Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summary. Am J Respir Crit Care Med. 2001;163(5):1256–1276. | ||
COPD Branch in Chinese Thoracic Society. The guideline of diagnosis and management for COPD. COPD Branch in Chinese Thoracic Society. Chin J Tuberc Respir Dis. 2002;25:453–460. | ||
American Thoracic Society. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. American Thoracic Society. Am J Respir Crit Care Med. 1995;152(5 Pt 2):S77–S121. | ||
The guideline of diagnosis and management for COPD. Chinese Thoracic Society. Chin J Tuberc Respir Dis. 1997;20:199–233. | ||
Chinese Thoracic Society. BTS guidelines for the management of chronic obstructive pulmonary disease. The COPD Guidelines Group of the Standards of Care Committee of the BTS. Thorax. 1997;52 Suppl 5:S1–S28. | ||
Tanni SE, Pelegrino NR, Angeleli AY, Correa C, Godoy I. Smoking status and tumor necrosis factor-alpha mediated systemic inflammation in COPD patients. J Inflamm (Lond). 2010;7:29. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.