Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Association Between the Non-High-Density Lipoprotein Cholesterol-to-High-Density Lipoprotein Cholesterol Ratio (NHHR) and Mortality in Patients with COPD: Evidence From the NHANES 1999–2018
Authors Zhong Y, Zhou K, Li S, Zhang R, Wang D ![]()
Received 25 November 2024
Accepted for publication 21 March 2025
Published 28 March 2025 Volume 2025:20 Pages 857—868
DOI https://doi.org/10.2147/COPD.S508481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Yuhua Zhong,1 Kesi Zhou,2 Sheng Li,1 Renzi Zhang,1 Daoxin Wang1
1Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Anesthesiology, Sichuan Second Hospital of T.C.M, Chengdu, People’s Republic of China
Correspondence: Renzi Zhang; Daoxin Wang, Email [email protected]; [email protected]
Purpose: The non-high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio (NHHR) is a new composite blood lipid index. We aimed to investigate the relationships of the NHHR with mortality from all-causes, cardiovascular disease (CVD), and chronic lower respiratory disease (CLRD) in US patients with COPD.
Methods: We assessed the association between the NHHR and mortality via weighted multivariate Cox proportional hazards regression models with restricted cubic splines (RCSs). Between-group survival rates at specific time points were compared via Kaplan‒Meier (KM) curves and Log rank tests. Receiver operating characteristic (ROC) curves were constructed to evaluate the efficiency of the NHHR for predicting mortality risk in COPD patients.
Results: After adjusting for confounding factors, weighted multivariate Cox proportional hazards regression model showed that higher NHHR was not significantly associated with all-cause mortality (HRs = 1.74), CVD mortality (HRs = 1.19), and CLRD-related mortality (HRs = 0.65), but HRs tended to increase as NHHR increased. RCS revealed U-shaped associations between the NHHR and all-cause mortality. KM survival analysis revealed a significantly lower survival rate for patients in the high-NHHR group (Log rank test P< 0.001). In addition, the NHHR had superior performance in predicting mortality, with AUC values of 0.85 and 0.883 for all-cause mortality, 0.769 and 0.815 for CVD mortality, and 0.765 and 0.815 for CLRD-related mortality at 5 and 10 years, respectively.
Conclusion: The higher the NHHR is, the greater the risk of all-cause mortality in COPD patients. The NHHR was significantly superior to other haematological biomarkers in predicting mortality.
Keywords: COPD, NHHR, all-cause mortality, CVD mortality, CLRD-related mortality
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung condition that impedes airflow in the lungs. Specifically, COPD is characterized by a progressive decline in lung function, accompanied by persistent respiratory symptoms such as cough, sputum production, and dyspnoea.1 Moreover, chronic respiratory disease ranks as the third leading cause of mortality, following cardiovascular diseases (CVDs) and cancer. With the ageing of the population, chronic respiratory disease remains a significant cause of mortality, with COPD being the leading contributor.2–5 Additionally, COPD patients often experience physical frailty, which primarily manifests as lower limb skeletal muscle dysfunction, further diminishing their quality of life.6,7 Studies have shown that COPD is prevalent among long-term smokers, but smoking cessation can delay the decline in lung function, and is considered an effective treatment for COPD in all stages.8–10 However, the high prevalence and mortality of COPD pose a great challenge to both human beings and health care systems, and there is an urgent need to comprehensively understand the contributing factors to improve the quality of life and clinical outcomes of patients.
Several studies have shown that obesity has an important effect on lung function: obesity-related indicators are negatively correlated with lung function, and obesity markedly increases susceptibility to lung diseases. The accumulation or abnormal distribution of lipids due to obesity is believed to be a crucial factor in the development of respiratory diseases.11–15 Moreover, increasing evidence indicates that lipoproteins may be associated with the onset and progression of COPD. Elevated serum triglycerides (TGs) may lead to increased airway resistance and, consequently, airway obstruction.16–18 For example, Unay et al measured TG and cholesterol levels in both a COPD group and a control group. The results indicated that the TG level in the stable COPD group was significantly greater than that in the control group, whereas the high-density lipoprotein (HDL) level was significantly lower than that in the control group.19 In another study, researchers conducted a subgroup analysis of patients who did not receive lipid-lowering therapy and reported that TG levels were higher in patients with stable COPD than in healthy individuals.20 Additionally, Zafirova-Ivanovska et al reported that low-density lipoprotein (LDL) and HDL levels were significant independent factors affecting patients with very severe COPD. Furthermore, patients with severe and very severe COPD presented higher blood cholesterol and LDL levels and lower blood HDL levels. Lipid imbalance exists in patients with COPD, and the lipid profile may change with the progression of the disease.21 For example, studies have shown that HDL may also be involved in the inflammatory process and may play a role in the pathogenesis of COPD.22 Consequently, investigating the relationship between lipoproteins and COPD patients is highly important for the prevention and treatment of COPD.
In this study, we used a novel composite lipid measure, the NHHR, (non-HDL cholesterol-to-HDL cholesterol ratio), which is a lipid parameter used to assess cardiovascular risk by quantifying the balance between atherogenic and protective lipoproteins. The NHHR has demonstrated significant predictive value in assessing the risk of developing a variety of diseases, including coronary heart disease, diabetes, abdominal aortic aneurysm, and carotid atherosclerosis.23–26 However, the prognostic value of the NHHR in patients with pulmonary diseases, particularly COPD, remains unclear. To address this gap, we conducted a study using the National Health and Nutrition Examination Survey (NHANES) database. The aim of the present study was to investigate the association of the NHHR with all-cause, CVD and respiratory disease mortality in COPD patients and its associations across different population characteristics to provide valuable insights into disease management and prevention strategies.
Methods
Study Population and Design
In the present study, we utilized data from the NHANES database spanning from 1999–2018 and included 3122 participants. The NHANES is a survey conducted by the National Center for Health Statistics (NCHS) to evaluate the nutritional and health status of a representative United States (US) population.27 The study protocol was formally approved by the Research Ethics Review Board of the NCHS, and informed consent was obtained from all participants.28 Publicly available data for analysis can be downloaded from https://www.cdc.gov/nchs/nhanes/index.htm.
To focus on adult health, participants under 18 years of age were excluded from the study. COPD diagnosis was determined through responses to specific questions in the NHANES questionnaire, a method validated by prior studies.29,30 Participants were classified as having COPD if they responded “yes” to any of the following questions: “Have you ever been told by a doctor that you have COPD?”, “Have you ever been told by a doctor that you have chronic bronchitis?”, or “Have you ever been told by a doctor that you have emphysema?”. After excluding those with incomplete NHHR and mortality data, 3,122 COPD patients were included in the final analysis. This meticulous approach ensured that the core information from participants with comprehensive health data was included in the analysis. The detailed screening process is depicted in Figure 1.
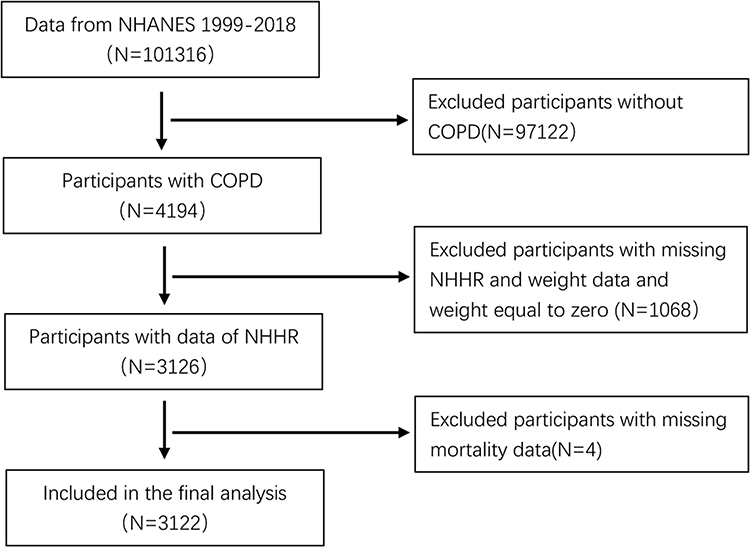 |
Figure 1 Flowchart of participants selection. Abbreviations: COPD, chronic obstructive pulmonary disease; NHHR, the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio. |
Calculation and Definition of the NHHR
The NHHR is calculated by first subtracting the HDL-C level from the total cholesterol (TC) level to obtain the non-HDL-C level. The NHHR was subsequently computed, with the following equation. NHHR = (TC - HDL-C) / HDL-C.31 The NHANES investigators collect blood lipid data through a rigorous, systematic process. Participants undergo a medical examination during which trained healthcare professionals draw blood samples. These serum samples are carefully processed and stored before being sent to the University of Minnesota for comprehensive analysis. In the laboratory, blood cells are separated from the serum through centrifugation. Next, the concentrations of TC, HDL-C, and other lipid parameters are measured via precise enzymatic or chemical assays. Each measurement result is meticulously documented and stored in a secure database for in-depth subsequent analysis.
Definition of COPD and Outcomes
Our study outcomes included all-cause mortality, cardiovascular mortality (CVD mortality), and chronic lower respiratory disease (CLRD)-related mortality. Specifically, all-cause mortality encompasses deaths from any cause, including diseases, accidents, and suicides, thus serving as a comprehensive measure of overall mortality risk in epidemiological studies. Similarly, CVD mortality is defined as death attributable to CVDs, such as coronary artery disease, heart failure, stroke, and hypertension. Finally, CLRD-related mortality refers to deaths caused by CLRDs, including COPD, asthma, emphysema, and chronic bronchitis. Consequently, this multifaceted approach allows for a detailed assessment of the impact of the NHHR on mortality. The mortality data were analysed on the basis of publicly available mortality data provided by the NCHS. NHANES data were integrated with death certificate records from the National Death Index (NDI). Follow-up mortality data were updated through December 31, 2019.
Covariates
Demographic characteristics, including age, sex (female or male), race, education level, and the family income‒poverty ratio, were collected. Age was categorized into groups of ≤65 years and >65 years. Races included Mexican American, other Hispanic, non-Hispanic white, non-Hispanic black, and other. Education attainment was categorized as <9th grade, 9–11th grade, high school diploma/ general educational development (GED), some college or associate degree, college graduate, or graduate degree or above. For the definition and classification of smoking and drinking status, we referenced established criteria from relevant literature.32 Alcohol intake was categorized into 4 groups: non-drinker, 1–5 times/month, 5–10 times/month, and more than 10 times/month. Smoking status was categorized into three groups: never smokers, former smokers and current smokers. Physical activity was categorized into three groups: Light activity, Moderate activity, Vigorous activity. Medications use was categorized as Use of statins, Use of cholesterol absorption inhibitor drugs, Use of statins and cholesterol absorption inhibitor drugs, Use of non-lipid-lowering drugs, no medication used. Diabetes was defined on the basis of a physician’s diagnosis, the use of antidiabetic medications or insulin, or laboratory criteria such as a fasting plasma glucose (FPG) level of ≥7.0 mmol/L or a glycosylated haemoglobin (HbA1c) level of ≥6.5%. Hypertension was defined as having a mean systolic blood pressure of ≥130 mmHg and/or diastolic blood pressure of ≥80 mmHg on the basis of three consecutive measurements, a physician’s diagnosis on two or more occasions, or the use of antihypertensive medication. Further details regarding these covariates are available on the NHANES social networking site.
Statistical Analysis
All analyses adhered to the NHANES analysis guide, accounting for sample weights, stratification, and clustering inherent to its complex sampling design. Normally distributed continuous variables are expressed as weighted means ± SDs, whereas categorical variables are presented as frequencies and weighted percentages. Using the continuous NHHR values, participants were divided into quartiles (Q1-Q4) via weighted analysis. The baseline characteristics of these quartiles were compared via analysis of variance (ANOVA) for continuous variables and the χ2 test for categorical variables.
To control for confounding factors, we developed three models and employed multivariate Cox regression models to determine hazard ratios (HRs) and 95% confidence intervals (CIs) for mortality. Model 1 was unadjusted. Model 2 was adjusted for age, sex, race, educational attainment, and the family income‒poverty ratio. Model 3 was further adjusted for alcohol intake, smoking status, physical activity, medications use, diabetes status, hypertension status, BMI, WC, FPG, HbA1c%, SBP, DBP, and TG.
Additionally, the Cox proportional hazards regression model, combined with restricted cubic splines (RCSs), was used for smooth curve fitting to explore the dose‒response relationship between the NHHR and mortality. Kaplan‒Meier (KM) curves, coupled with the Log rank test, were used to compare survival probabilities at specific time points between different groups. The Log rank test was used to assess whether survival differences between groups were statistically significant. Moreover, to evaluate the efficacy and reliability of the NHHR in predicting mortality risk in patients with COPD, we used receiver operating characteristic (ROC) curves. The performance of the model was assessed by the area under the curve (AUC), where an AUC closer to 1 indicated stronger discriminative ability, and an AUC closer to 0.5 suggested no discriminative power beyond random guessing.
All analyses were performed with R software, version 4.3.2, and a two-sided P value of less than 0.05 was considered to indicate statistical significance.
Results
Baseline Characteristics of the Participants
A total of 3122 participants were included in this study, with an average age of 57±16.03 years, and 61% of the cohort was female. Among participants with COPD, the prevalence rates of all-cause mortality, CVD mortality, and CLRD-related mortality were 20%, 6%, and 9%, respectively. The mean NHHR was 2.75±1.62. The baseline characteristics of the participants grouped by NHHR quartile are presented in Table 1. The participants in the higher-NHHR quartiles were generally younger, male, and non-Hispanic White, and presented higher BMI, FPG, and HbA1c levels than did those in the lowest quartile. Additionally, a higher prevalence of participants with 1–5 alcoholic drinks per month and current smokers was observed in the higher NHHR quartiles. As shown in Table 1, we present a realistic picture of higher mortality in the lower NHHR group, which may be due to potential confounders, such as differences in baseline characteristics, coexisting conditions, or treatment patterns between groups. Similarly, in Model 1 of Table 2, we also showed higher mortality in the lower NHHR group without controlling for covariates, but in model 3 after controlling for covariates, the HR showed an upward trend, suggesting that higher NHHR had higher mortality after controlling for covariates. And these relationships require further investigation in the future.
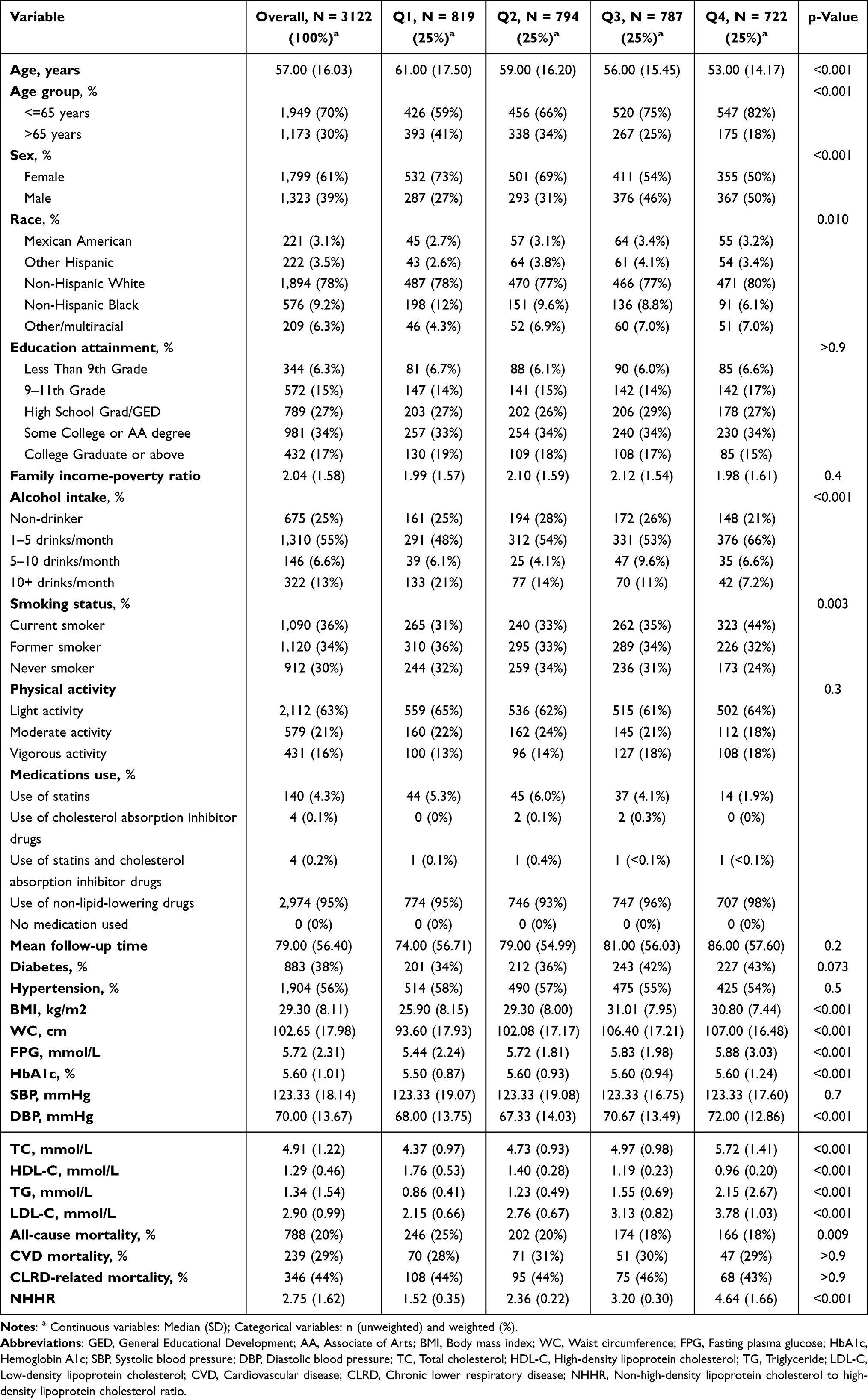 |
Table 1 Baseline Characteristics: Overall and Stratified by NHHR Quartiles |
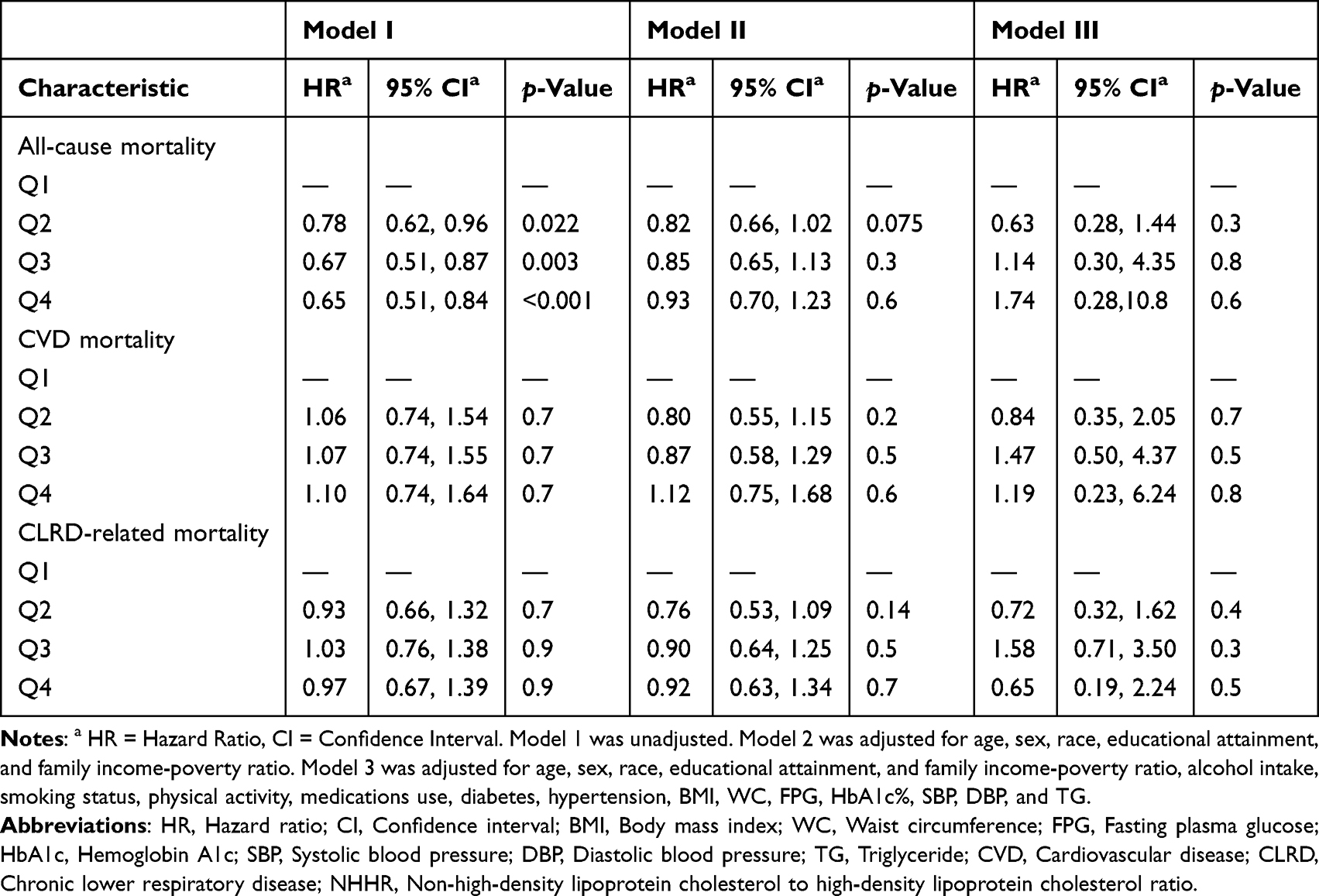 |
Table 2 HRs (95% CIs) for Mortality According to NHHR Quartiles |
Relationships Between the NHHR and Mortality
During the follow-up period, 788 deaths were recorded, including 239 attributable to cardiovascular causes and 346 attributable to CLRD. The relationship between the NHHR and mortality is detailed in Table 2. A weighted multivariate Cox proportional hazards regression model was used to assess the independent association of the NHHR with the risk of death. After adjusting for multiple variables (Model 3), the HRs and 95% CIs for all-cause mortality from the lowest to highest quartiles of the NHHRS (Q1-Q4) were 1.00 (reference), 0.63 (95% CI: 0.28, 1.44), 1.14 (95% CI: 0.30, 4.35), and 1.74 (95% CI: 0.28, 10.8), respectively; 1.00 (reference), 0.84 (95% CI: 0.35, 2.05), 1.47 (95% CI: 0.50, 4.37), and 1.19 (95% CI: 0.23, 6.24), respectively, for CVD mortality; and 1.00 (reference interval), 0.72 (95% CI: 0.32, 1.62), 1.58 (95% CI: 0.71, 3.50), and 0.65 (95% CI: 0.19, 2.24), respectively, for CLRD-related mortality. Although the HRs did not reach statistical significance, the trend in adjusted model 3 is consistent with our hypothesis that the risk of all-cause death in COPD patients tended to increase with increasing NHHR. Using an RCS model and smooth curve analysis adjusted for age, sex, race, educational attainment, the family income‒poverty ratio, alcohol intake, smoking status, physical activity, medications use, diabetes status, hypertension status, BMI, WC, FPG, HbA1c%, SBP, DBP, and TG, we observed a U-shaped association between the NHHR and all-cause mortality among COPD participants (P overall <0.001, P nonlinear <0.001) (Figure 2A). The inflection point for the NHHR 3.57 for all-cause mortality. No significant trend was observed between CVD mortality and CLRD-related mortality and an increased NHHR levels (Figure 2B and 2C). The KM survival curve demonstrated that patients in the high-NHHR group had a lower survival rate than those in the low-NHHR group did over the follow-up period (Figure 3A, Log rank test P<0.001). However, no significant associations were observed between the NHHR and CVD-related mortality or CLRD-related mortality (Figure 3B and 3C).
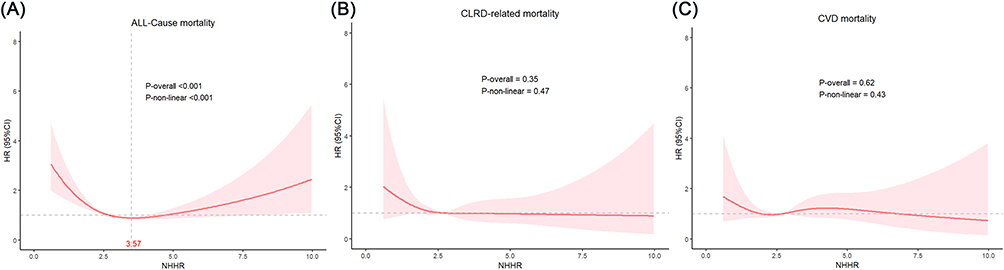 |
Figure 2 Restricted cubic spline analyses the association of NHHR with (A) all-cause mortality, (B) CVD mortality, and (C) CLRD-related mortality. Adjusted for age, sex, race, educational attainment, and family income-poverty ratio, alcohol intake, smoking status, physical activity, medications use, diabetes, hypertension, BMI, WC, FPG, HbA1c%, SBP, DBP, and TG. Abbreviations: NHHR, the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio; HR, hazard ratio; CI, confidence interval; CVD, cardiovascular diseases; CLRD, chronic lower respiratory disease; BMI Body mass index; WC Waist circumference; FPG Fasting plasma glucose; HbA1c Hemoglobin A1c, SBP Systolic blood pressure; DBP Diastolic blood pressure; TG Triglyceride. |
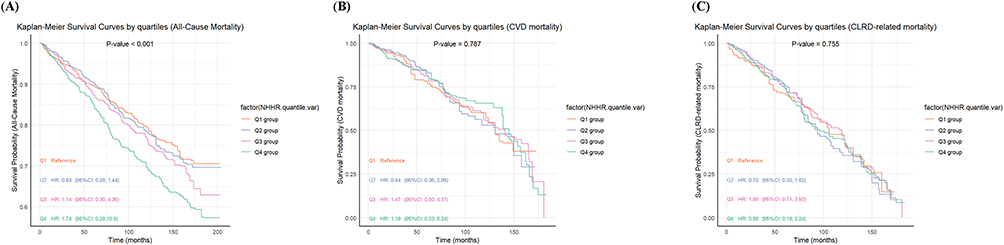 |
Figure 3 Kaplan–Meier survival curve of NHHR with (A) all-cause mortality, (B) CVD mortality, and (C) CLRD-related mortality. Abbreviations: NHHR, the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio; CVD, cardiovascular diseases; CLRD, chronic lower respiratory disease; HR, hazard ratio; CI, confidence interval. |
ROC Analysis of the Predictive Role of the NHHR for Mortality
A time-dependent adjusted ROC curve was used to assess the predictive value of the NHHR for all-cause mortality, CVD mortality, and CLRD-related mortality. The AUC values for the NHHR in predicting all-cause mortality at 1, 3, 5, and 10 years were 0.845 (95% CI = 78.41, 90.64), 0.843(95% CI = 80.43, 88.17), 0.85(95% CI = 81.74, 88.33), and 0.883(95% CI = 85.61, 90.92), respectively. For CVD mortality, the AUC values were 0.742(95% CI = 66.55, 81.84), 0.757(95% CI = 71.00, 80.39), 0.769(95% CI = 72.80, 80.92), and 0.815(95% CI = 77.98, 84.97), respectively, whereas for CLRD-related mortality, the AUC values were 0.76(95% CI = 67.63, 84.34), 0.771(95% CI = 72.57, 81.58), 0.765(95% CI = 72.53, 80.48), and 0.815(95% CI = 77.97, 85.08), respectively. These results, illustrated in Figure 4A–4C highlight the significant predictive value of the NHHR for all-cause, CVD, and CLRD-related mortality.
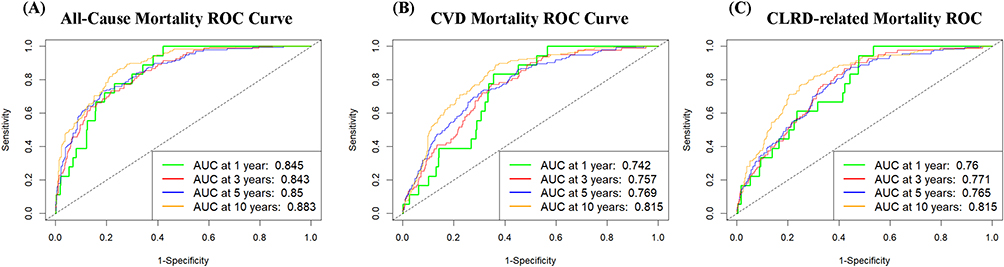 |
Figure 4 A Time-dependent ROC curves of NHHR for predicting (A) all-cause mortality, (B) CVD mortality, and (C) CLRD-related mortality. Abbreviations: AUC, area under the curve; ROC, receiver-operating characteristic; NHHR, the non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio; CVD, cardiovascular diseases; CLRD, chronic lower respiratory disease. |
Discussion
This study is the first to examine the associations between the NHHR and all-cause, CVD, and CLRD-related mortality in COPD patients. Our findings revealed a U-shaped association between the NHHR and all-cause mortality. Lipid metabolism disorder is a factor in the pathogenesis and development of COPD patients. Too low or too high NHHR suggests that the patients have lipid metabolism disorder, which may explain why there is a U-shaped correlation between NHHR and all-cause mortality in COPD patients.33 Since microvascular disease is highly prevalent in heavy smokers and may contribute to COPD and cardiovascular outcomes, this may mask the true relationship between NHHR and mortality.34 These results underscore the value of the NHHR as a prognostic indicator for all-cause mortality in COPD patients, emphasizing its importance in disease risk stratification and prognosis. By establishing the NHHR as a significant predictor of mortality outcomes, this research has important implications for enhancing clinical management and providing targeted interventions for COPD patients. The potential of the NHHR in guiding clinical decision-making could lead to more personalized and effective treatment strategies, ultimately improving patient outcomes.
These refined insights underscore the pivotal role of the NHHR in advancing the understanding and management of mortality risks associated with COPD. The NHHR, a novel indicator for assessing lipid balance, is both cost-effective and clinically valuable in predicting various diseases. For example, Hou et al reported a positive association between the NHHR and the prevalence of periodontitis, with a 7% increase per one-unit increase in the NHHR.35 Similarly, in a study of 6763 participants, Pan et al reported a 9% increase in obstructive sleep apnoea (OSA) incidence per one-unit increase in the NHHR, with a U-shaped association and an inflection point at 4.12.36 Other studies have also indicated a positive correlation between the NHHR and the risk of developing hypertension, suggesting its potential utility in the prevention and diagnosis of this condition.37 Collectively, these studies underscore the prognostic value of lipid metabolism for inflammatory, respiratory, and cardiovascular diseases. In the present study, we screened 3122 COPD patients aged 40 years or older from the US NHANES database from 1999–2018. After adjusting for multiple covariates, we observed a strong linear association between the NHHR and all-cause mortality in COPD patients.
Pulmonary dysfunction in COPD is characterized by irreversible progressive airflow obstruction, chronic airway inflammation, and systemic effects or comorbidities. The pathophysiological basis of COPD involves chronic airway inflammation due to long-term exposure to harmful gases, smoke, dust, and other particles.38,39 Inflammation status is significantly associated with the risk of developing lipid metabolism disorders.40 In addition, several studies suggest that the presence of COPD is associated with the risk of developing lipid disorders. The outcome and prognosis of obese patients with COPD are worse, which manifests as more severe dyspnoea, worse quality of life, etc., and are dose dependent with obesity. Obesity may aggravate the progression of COPD.41 Furthermore, animal studies have shown that caloric restriction leads to “emphysema-like” changes in lung morphology and mechanics, implicating lipids in lung disease pathogenesis.42–44 Apolipoprotein A1 (ApoA1), the primary protein in HDL, facilitates the extraction of cholesterol and phospholipids from lung cells for transport to the liver, playing a crucial role in reverse cholesterol transport. In COPD patients, ApoA1 levels are significantly decreased in lung tissues. The overexpression of ApoA1 can mitigate cigarette smoke-induced lung tissue inflammation, oxidative stress, metalloproteinase activation, and cell apoptosis in mice.45 Mechanistically, ApoA1 prevents cigarette exposure-induced fatty acid synthesis (FAS) and the translocation of downstream death signalling complexes to lipid rafts, thereby inhibiting FAS-mediated apoptosis.46
Previous studies have highlighted the predictive role of lipid-related indicators in COPD patients. For example, HDL-C has been identified as a marker of muscle volume, function, and total energy expenditure in COPD patients.47 The LDL-to-lymphocyte ratio (LLR), a composite index, has been widely used to predict cerebral infarction prognosis. Huang et al reported a positive correlation between the LLR and COPD severity, with higher LLR values associated with more severe airway obstruction and dyspnoea.48 We compared articles on the prediction of mortality in COPD patients by numerous haematology-related indicators, and reported that the NHHR was more effective in predicting disease. The AUCs of red blood cell distribution width (RDW) for predicting all-cause and CVD mortality in COPD patients at 5 and 10 years were 0.707, and 0.714 and 0.686, and 0.698, respectively. The AUCs of the Hb-to- RDW ratio (HRR) for the prediction of 5-year and 10-year all-cause mortality were 0.661 and 0.653, respectively, and those for the prediction of CVD mortality were 0.654 and 0.66, respectively. The AUCs of the neutrophil-to-albumin ratio (NPAR) and neutrophil-to-lymphocyte ratio (NLR) for the prediction of 5-year all-cause mortality in COPD patients are 0.808 and 0.799, respectively.27 The Prognostic Nutritional Index (PNI) and the Geriatric Nutritional Risk Index (GNRI) had AUCs of 0.706 and 0.710 for predicting all-cause mortality in COPD patients, respectively.49 The predictive power of these indicators for mortality in COPD patients was significantly lower than that of our study results. In addition, compared with previous studies, we provided a clearer definition of drinking status and adopted the latest numerical definition of hypertension diagnosis, which made our study more scientific and led to more convincing conclusions. An elevated NHHR indicates an increased risk of these mortality outcomes, suggesting that early detection and intervention targeting lipid levels could improve COPD prognosis. In addition, our results also provide clinicians with more prognosis and individualized treatment guidance. Higher NHHR values can alert clinicians to a higher risk of death and enable them to adjust treatment accordingly. Since different COPD patients may have different NHHR levels, treatment strategies can be tailored based on this biomarker. For example, for patients with high NHHR who are predicted to be at high risk for death, more intensive treatment, such as novel agents targeting the underlying pathophysiological mechanisms associated with NHHR, or more frequent pulmonary rehabilitation programs, could be considered. Future studies should be validated in larger, more centers and more diverse patient populations, and studies with a wider range of patients will improve the generalizations of the results and strengthen the reliability of NHHR as a predictive marker.
Despite these findings, our study has several limitations. We did not observe a clear association between the NHHR and CVD mortality and CLRD-related mortality in COPD patients, which may be related to the small size of our sample. We adjusted for several covariates, but unknown risk factors not included in the NHANES dataset may exist. Additionally, parts of the NHANES survey data were self-reported, which may introduce reporting or recall bias, potentially affecting the results. Future research could incorporate strategies such as cross-referencing self-reported data with clinical records, using more objective measures like laboratory tests, longitudinal data collection, and enhanced training for data collectors. Nevertheless, the results of the present study confirm the importance of monitoring lipid levels in COPD patients and highlights the potential of the NHHR as a prognostic marker. Future research should further explore the role of lipid metabolism in COPD prognosis and address these limitations to validate and extend our findings.
Conclusions
The results of this study confirm that the NHHR is a valuable predictor of all-cause mortality in COPD patients, and is superior to other haematological-related measures. In a nationally representative sample of US adults with COPD, we observed U-shaped relationships between the NHHR and all-cause mortality. Routine monitoring of the NHHR can significantly improve the assessment of COPD prognosis and the associated mortality risk, and provide the basis for more precise and effective clinical intervention. Our study adds to the growing body of evidence that lipid-related measures predict mortality and provides valuable insights for future research and clinical applications.
Abbreviations
NHHR, the non-high-density lipoprotein cholesterol-to-high-density lipoprotein cholesterol ratio; CVD, cardiovascular disease; CLRD, chronic lower respiratory disease; COPD, chronic obstructive pulmonary disease; RCS, restricted cubic spline; KM, Kaplan‒Meier; ROC, receiver operating characteristic; HR, hazard ratio; TG, triglyceride; HDL, high-density lipoprotein; LDL, low-density lipoprotein; NHANES, National Health and Nutrition Examination Survey; NCHS, National Center for Health Statistics; US, United States; NDI, National Death Index; GED, general educational development; FPG, fasting plasma glucose; HbA1c, hemoglobin A1c; CI, confidence interval; BMI, body mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; TC, total cholesterol; AUC, area under the curve; OSA, obstructive sleep apnoea; ApoA1, apolipoprotein A1; FAS, fatty acid synthesis; LLR, LDL-to-lymphocyte ratio; RDW, red blood cell distribution width; HRR, Hb-to- RDW ratio; NPAR, the neutrophil-to-albumin ratio; NLR, neutrophil-to-lymphocyte ratio; PNI, the Prognostic Nutritional Index; GNRI, the Geriatric Nutritional Risk Index.
Data Sharing Statement
The datasets used and/or analysed during the current study was publicly available datasets. This data can be found here: https://www.cdc.gov/nchs/nhanes/index.htm.
Ethics Approval and Informed Consent
The database used in this study was a publicly available data source, and all data were anonymized and did not contain personal information that could identify the participants. According to item 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects: research using legally obtained public data, or conducting research through observation, data generated without interfering with public behavior, and research using anonymous information data are exempt from ethical review. The data use protocol and ethical guidelines were strictly followed, and the study was conducted for scientific research analysis only. The study adhered to the ethical principles of the Declaration of Helsinki and respected the privacy and data confidentiality of the participants.
Consent for Publication
All participants in the study provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Key Laboratory of Respiratory Inflammatory Injury and Precision Diagnosis and Treatment, Chongqing Municipal Health And Health Committee, Chongqing 400010, China and the National Natural Science Foundation of China (Grant no. 82270091).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hogg JC. Pathophysiology of airflow limitation in chronic obstructive pulmonary disease. Lancet. 2004;364(9435):709–721. doi:10.1016/s0140-6736(04)16900-6
2. JB Soriano, PJ Kendrick, KR Paulson. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/s2213-2600(20)30105-3
3. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/s2213-2600(21)00511-7
4. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/s0140-6736(22)00470-6
5. García Castillo E, Alonso Pérez T, Ancochea J, et al. Mortality prediction in chronic obstructive pulmonary disease comparing the GOLD 2015 and GOLD 2019 staging: a pooled analysis of individual patient data. ERJ Open Res. 2020;6(4). doi:10.1183/23120541.00253-2020
6. Gephine S, Mucci P, Grosbois JM, Maltais F, Saey D. Physical Frailty in COPD Patients with Chronic Respiratory Failure. Int J Chron Obstruct Pulmon Dis. 2021;16:1381–1392. doi:10.2147/copd.S295885
7. Bernard S, LeBlanc P, Whittom F, et al. Peripheral muscle weakness in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;158(2):629–634. doi:10.1164/ajrccm.158.2.9711023
8. Marsh S, Aldington S, Shirtcliffe P, Weatherall M, Beasley R. Smoking and COPD: what really are the risks? Eur Respir J. 2006;28(4):883–884. doi:10.1183/09031936.06.00074806
9. Leem AY, Park B, Kim YS, Chang J, Won S, Jung JY. Longitudinal decline in lung function: a community-based cohort study in Korea. Sci Rep. 2019;9(1):13614. doi:10.1038/s41598-019-49598-9
10. Franciosi L, Postma DS, van den Berge M, et al. Susceptibility to COPD: differential proteomic profiling after acute smoking. PLoS One. 2014;9(7):e102037. doi:10.1371/journal.pone.0102037
11. Kim HJ, Park JH, Min JY, et al. Abdominal adiposity intensifies the negative effects of ambient air pollution on lung function in Korean men. Int J Obes Lond. 2017;41(8):1218–1223. doi:10.1038/ijo.2017.97
12. Sorlí-Aguilar M, Martín-Luján F, Flores-Mateo G, et al. Adiposity markers and lung function in smokers: a cross-sectional study in a Mediterranean population. BMC Pulm Med. 2016;16(1):178. doi:10.1186/s12890-016-0341-y
13. Robinson PD. Obesity and its impact on the respiratory system. Paediatr Respir Rev. 2014;15(3):219–226. doi:10.1016/j.prrv.2014.06.003
14. Lin CK, Lin CC. Work of breathing and respiratory drive in obesity. Respirology. 2012;17(3):402–411. doi:10.1111/j.1440-1843.2011.02124.x
15. Brazzale DJ, Pretto JJ, Schachter LM. Optimizing respiratory function assessments to elucidate the impact of obesity on respiratory health. Respirology. 2015;20(5):715–721. doi:10.1111/resp.12563
16. Rafie S, Moitra S, Brashier BB. Association between the Serum Metabolic Profile and Lung Function in Chronic Obstructive Pulmonary Disease. Turk Thorac J. 2018;19(1):13–18. doi:10.5152/TurkThoracJ.2017.17043
17. Zafirova-Ivanovska B, Stojkovikj J, Dokikj D, et al. The Level of Cholesterol in COPD Patients with Severe and Very Severe Stage of the Disease. Open Access Maced J Med Sci. 2016;4(2):277–282. doi:10.3889/oamjms.2016.063
18. Burkart KM, Manichaikul A, Wilk JB, et al. APOM and high-density lipoprotein cholesterol are associated with lung function and per cent emphysema. European Respiratory Journal. 2014;43(4):1003–1017. doi:10.1183/09031936.00147612
19. Gunay S, Sariaydin M, Acay A. New Predictor of Atherosclerosis in Subjects With COPD: atherogenic Indices. Respir Care. 2016;61(11):1481–1487. doi:10.4187/respcare.04796
20. Xuan L, Han F, Gong L, et al. Association between chronic obstructive pulmonary disease and serum lipid levels: a meta-analysis. Lipids Health Dis. 2018;17(1):263. doi:10.1186/s12944-018-0904-4
21. Markelić I, Hlapčić I, Rogić D, et al. Lipid profile and atherogenic indices in patients with stable chronic obstructive pulmonary disease. Nutr Metab Cardiovasc Dis. 2021;31(1):153–161. doi:10.1016/j.numecd.2020.07.039
22. Kotlyarov S. High-Density Lipoproteins: a Role in Inflammation in COPD. Int J mol Sci. 2022;23(15):8128. doi:10.3390/ijms23158128
23. Sheng G, Liu D, Kuang M, Zhong Y, Zhang S, Zou Y. Utility of Non-High-Density Lipoprotein Cholesterol to High-Density Lipoprotein Cholesterol Ratio in Evaluating Incident Diabetes Risk. Diabetes Metab Syndr Obes. 2022;15:1677–1686. doi:10.2147/dmso.S355980
24. Qin G, Tu J, Zhang C, et al. The value of the apoB/apoAΙ ratio and the non-HDL-C/HDL-C ratio in predicting carotid atherosclerosis among Chinese individuals with metabolic syndrome: a cross-sectional study. Lipids Health Dis. 2015;14(1):24. doi:10.1186/s12944-015-0023-4
25. Lin W, Luo S, Li W, et al. Association between the non-HDL-cholesterol to HDL- cholesterol ratio and abdominal aortic aneurysm from a Chinese screening program. Lipids Health Dis. 2023;22(1):187. doi:10.1186/s12944-023-01939-4
26. Mao Q, Zhao J, Zhao X. Association of non-HDL-C-to-HDL-C ratio with coronary lesions and its prognostic performance in first-onset NSTEMI. Biomarker Med. 2023;17(1):29–39. doi:10.2217/bmm-2022-0548
27. Lan CC, Su WL, Yang MC, Chen SY, Wu YK. Predictive role of neutrophil-percentage-to-albumin, neutrophil-to-lymphocyte and eosinophil-to-lymphocyte ratios for mortality in patients with COPD: evidence from NHANES 2011-2018. Respirology. 2023;28(12):1136–1146. doi:10.1111/resp.14589
28. Yu B, Li M, Yu Z, et al. The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) as a predictor of all-cause and cardiovascular mortality in US adults with diabetes or prediabetes: NHANES 1999-2018. BMC Med. 2024;22(1):317. doi:10.1186/s12916-024-03536-3
29. Ibrahimou B, Azim SI, Sun N. Interaction between blood lead level and chronic obstructive pulmonary disease (COPD) on risk of heart attack or stroke: USA NHANES, 2013-2014. Pulm Pharmacol Ther. 2019;58:101805. doi:10.1016/j.pupt.2019.101805
30. Liu S, Zhang H, Zhu P, Chen S, Lan Z. Predictive role of red blood cell distribution width and hemoglobin-to-red blood cell distribution width ratio for mortality in patients with COPD: evidence from NHANES 1999-2018. BMC Pulm Med. 2024;24(1):413. doi:10.1186/s12890-024-03229-w
31. Qing G, Deng W, Zhou Y, Zheng L, Wang Y, Wei B. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and suicidal ideation in adults: a population-based study in the United States. Lipids Health Dis. 2024;23(1):17. doi:10.1186/s12944-024-02012-4
32. Zhao D, Chen P, Chen M, Chen L, Wang L. Association of Magnesium Depletion Score with Congestive Heart Failure: results from the NHANES 2007-2016. Biol Trace Elem Res. 2024;202(2):454–465. doi:10.1007/s12011-023-03697-x
33. Kotlyarov S, Kotlyarova A. Molecular Mechanisms of Lipid Metabolism Disorders in Infectious Exacerbations of Chronic Obstructive Pulmonary Disease. Int J mol Sci. 2021;22(14):7634. doi:10.3390/ijms22147634
34. Freund O, Shetrit A, Bar-Shai A, et al. Smoking and Respiratory Diseases in Patients with Coronary Microvascular Dysfunction. Am J Med. 2024;137(6):538–544.e1. doi:10.1016/j.amjmed.2024.02.034
35. Hou K, Song W, He J, Ma Z. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and prevalence of periodontitis among US adults: a cross-sectional NHANES study. Sci Rep. 2024;14(1):5558. doi:10.1038/s41598-024-56276-y
36. Pan X, Zhang X, Wu X, et al. Association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and obstructive sleep apnea: a cross-sectional study from NHANES. Lipids Health Dis. 2024;23(1):209. doi:10.1186/s12944-024-02195-w
37. Wu J, Guo J. Non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and hypertension in American adults: a NHANES cross-sectional study. Front Physiol. 2024;15:1398793. doi:10.3389/fphys.2024.1398793
38. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
39. Sutherland ER, Martin RJ. Airway inflammation in chronic obstructive pulmonary disease: comparisons with asthma. J Allergy Clin Immunol. 2003;112(5):819–827. doi:10.1016/s0091
40. Kotlyarov S, Bulgakov A. Lipid Metabolism Disorders in the Comorbid Course of Nonalcoholic Fatty Liver Disease and Chronic Obstructive Pulmonary Disease. Cells. 2021;10(11):2978. doi:10.3390/cells10112978
41. Lambert AA, Putcha N, Drummond MB, et al. Obesity Is Associated With Increased Morbidity in Moderate to Severe COPD. Chest. 2017;151(1):68–77. doi:10.1016/j.chest.2016.08.1432
42. Kerr JS, Riley DJ, Lanza-Jacoby S, et al. Nutritional emphysema in the rat. Influence of protein depletion and impaired lung growth. Am Rev Respir Dis. 1985;131(4):644–650. doi:10.1164/arrd.1985.131.4.644
43. Sahebjami H, Wirman JA. Emphysema-like changes in the lungs of starved rats. Am Rev Respir Dis. 1981;124(5):619–624. doi:10.1164/arrd.1981.124.5.619
44. Sahebjami H, MacGee J. Effects of starvation on lung mechanics and biochemistry in young and old rats. J Appl Physiol. 1985;58(3):778–784. doi:10.1152/jappl.1985.58.3.778
45. Chen H, Li Z, Dong L, Wu Y, Shen H, Chen Z. Lipid metabolism in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2019;14:1009–1018. doi:10.2147/copd.S196210
46. Kim C, Lee JM, Park SW, et al. Attenuation of Cigarette Smoke-Induced Emphysema in Mice by Apolipoprotein A-1 Overexpression. Am J Respir Cell mol Biol. 2016;54(1):91–102. doi:10.1165/rcmb.2014-0305OC
47. Shirahata T, Sato H, Yogi S, et al. Possible association of high-density lipoprotein cholesterol levels with trunk muscle deficits and decrease in energy expenditure in patients with or at risk for COPD: a pilot study. Respir Investig. 2022;60(5):720–724. doi:10.1016/j.resinv.2022.06.005
48. Huang Y, Ding K, Dai Z, et al. The Relationship of Low-Density-Lipoprotein to Lymphocyte Ratio with Chronic Obstructive Pulmonary Disease. Int J Chron Obstruct Pulmon Dis. 2022;17:2175–2185. doi:10.2147/copd.S369161
49. Xu Y, Yan Z, Li K, Liu L, Xu L. Association between nutrition-related indicators with the risk of chronic obstructive pulmonary disease and all-cause mortality in the elderly population: evidence from NHANES. Front Nutr. 2024;11:1380791. doi:10.3389/fnut.2024.1380791
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.