")
Back to Journals » Open Access Emergency Medicine » Volume 15
Association Between the Emergency Department Length of Stay and in-Hospital Mortality: A Retrospective Cohort Study
Authors Habib H , Sudaryo MK
Received 5 April 2023
Accepted for publication 30 August 2023
Published 13 September 2023 Volume 2023:15 Pages 313—323
DOI https://doi.org/10.2147/OAEM.S415971
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Hadiki Habib,1– 3,* Mondastri Korib Sudaryo4,*
1Doctoral Program of Epidemiology, Epidemiology Department, Faculty of Public Health, Universitas Indonesia, Depok, Indonesia; 2Emergency Unit, Dr. Cipto Mangunkusumo Hospital/Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 3Division of Respirology and Critical Illness, Department of Internal Medicine, Dr. Cipto Mangunkusumo Hospital/Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 4Epidemiology Department, Faculty of Public Health, Universitas Indonesia, Depok, Indonesia
*These authors contributed equally to this work
Correspondence: Mondastri Korib Sudaryo, Epidemiology Department, Faculty of Public Health, Universitas Indonesia, Depok, 10430, Indonesia, Tel +62 81263488115, Email [email protected]
Purpose: The number of emergency department (ED) visits and prolonged ED length of stay (LOS) are increasing worldwide. Prolonged ED LOS may be associated with a higher risk of in-hospital mortality. Here, we analysed the association between of ED LOS and the risk of in-hospital mortality in a hospital in Jakarta, Indonesia.
Patients and methods: This was a single-centre retrospective cohort study performed in a referral academic hospital in Jakarta, Indonesia. Data on ED visits in 2019 were obtained from the electronic medical records. ED patient was used as the unit of the analysis. The dependent variable was all-cause in-hospital mortality during one’s visit. The main independent variable was ED LOS with respect to approval (< 8 h) and prolonged (≥ 8 h). Potential confounders were sex, age, triage categories, trauma-related case, malignancy-related case, labour-related case, and referral patients from other healthcare facilities. Multivariate logistic regression analysis was performed to evaluate the association of ED LOS and in-hospital mortality after adjusting for other confounders.
Results: There were 18,553 participants included in the analysis. The in-hospital mortality was 13.5% among all participants, and 63.5% participants had an ED LOS ≥ 8 h. Multivariate analysis showed that a prolonged ED LOS was associated with an increased risk of in-hospital mortality (adjusted relative risk, 2.69; 95% confidence interval, 2.40– 3.03; P< 0.001).
Conclusion: Prolonged ED LOS was associated with risk an increased of in-hospital mortality after adjusting for several confounders. In future, hospital service plans should aim to reduce ED LOS and increase patient flow from the ED to in-patient wards.
Plain Language Summary: Prolonged emergency department length of stay (ED LOS) was associated with risk of in-hospital mortality in an Indonesia referral hospital; this is the first such reported association.
Therefore, reduced ED LOS and increased patient flow to the inpatient ward should be a target for quality improvement in hospital service plans.
Keywords: emergency department, mortality, length of stay, overcrowding, patient flow, triage
Introduction
In many countries, the emergency department (ED) functions as a safety net for the health system1 and plays a pivotal role in achieving sustainable development goals related to the health domain.2 On a global scale, implementing universal health coverage and improving the accessibility of the ED further increase the use of emergency services.1 However, an increase in ED visits raises concerns regarding prolonged length of stay (LOS) in the ED,3,4 which can lead to ED overcrowding. In such cases, the ED cannot respond appropriately to emergency cases because the number of patients exceeds the patient-handling capacity of standard ED services and personnel.5,6 Overcrowding lowers ED performance in managing new emergency cases and increases the risk of delayed treatment, mortality, morbidity, and patient complaints.7–9
Several studies investigating the association between ED LOS and mortality risk have shown inconsistent results.7–9 However, a meta-analysis by Boudi et al indicated that mortality tends to increase in patients who have a longer stay in the ED prior to admission.10 A large-scale study by Singer et al revealed that ED LOS among boarding patients in the ED (patients who stay in the ED after the decision to admit has been made), the mortality rate increased from 2.5% in patients boarded for <2 h to 4.5% among patients boarded for >12 h (P<0.001).11
A survey of 118 emergency departments in Jakarta, Indonesia, revealed that there were approximately 2 million ED visits per year and that >60% of these visits continued to receive inpatient services.12 Most the ED cases in Indonesia are self-admitted because the pre-hospital ambulance service systems are under developed. Nevertheless, prolonged ED LOS in Indonesia poses similar risks to those reported elsewhere, which could lead to ED overcrowding.
To date, no researchers have reported the condition of ED LOS in Indonesia and its impact on patient condition. Therefore, in this study, we measured the effect of ED LOS on in-hospital mortality in a referral hospital in Jakarta, Indonesia. We hypothesized that a prolonged ED LOS is associated with an increased risk of in-hospital mortality.
Methods
This was a retrospective cohort study conducted in mid-June 2020 at Dr. Cipto Mangunkusumo Hospital, an academic referral hospital in Jakarta, Indonesia. The hospital has 73 beds in the ED and a total of 927 beds for inpatient care; an annual census of the ED revealed that there are approximately 30,000 ED visits per year.13,14 This study was approved by the institutional ethics board of the hospital (The Ethics Committee of the Faculty of Medicine, University of Indonesia-Cipto Mangunkusumo Hospital protocol number 20–10-1256). All patient data were treated with confidentiality in accordance with the Declaration of Helsinki. This observational study conformed to the STROBE statement (Supplementary File 1).15 Informed consent was not obtained due to the retrospective nature of the study; the ethics committee specifically waived the requirement of informed consent.
The independent variable was ED LOS, defined as the time at first triage to the end of the ED service (the time when the patient leaves the ED due to discharge or inpatient admission; alternatively, time of death in the ED).16,17 The standard ED LOS in our hospital is <8 h.18 The dependent variable was in-hospital mortality, defined as all-cause mortality in the hospital (including mortality in the ED) during each patient visit. Mortality was determined by confirming the mortality report in the medical records.
The following variables were considered as potential confounders: triage category, age, sex, trauma-related case, labour-related case, and malignancy-related case.10 The month and shift of ED visit and episodes of weekend visit were also recorded as baseline characteristics of the study participants but were not included as confounding variables. The potential confounders were selected based on regular ED registries and previous studies that were in accordance with the conceptual framework of this study.
Triage was performed upon initial admission to the ED and was used as a clinical proxy of the severity of illness and urgency of medical condition. The ED in our hospital implements a three-tier triage system.13 The resuscitation category includes patients with the most severe clinical conditions who need immediate intervention. The urgent category includes patients with very disturbing symptoms or those who have medical conditions that may potentially deteriorate if not urgently assessed; the maximum physician response time for this category is 30 minutes. The non-urgent category includes patients predicted to have minor clinical conditions and those with relatively mild symptoms; the physician response time for this category is a maximum of 60 minutes.
Patient age was determined in years, and sex was defined as male or female. Trauma cases were defined as all trauma-related cases in the ED, including trauma ranging from minor injury to major trauma or polytrauma. Labour-related cases were defined as all medical conditions associated with pregnancy cases with a labour indication that arrived at the ED with or without comorbid conditions. Malignancy-related cases were defined as all active malignancies—including solid tumours and blood malignancies—that were identified and documented in the medical record. The month of ED visit was defined as the month of patient visit based on the 2019 calendar, weekend visit was defined as ED attendance on Saturdays and Mondays throughout 2019, and daily shift visit was defined as ED visit at specified hours during the day. To categorize the daily shift, we divided a day into four shifts: shift 1 (06:00–11:59), shift 2 (12:00–17:59), shift 3 (18:00–23:59), and shift 4 (00:00–05:59).
Data regarding the dependent, independent, and potential confounding variables were retrieved from the electronic health records of the hospital. During data collection, blinding to exposure and outcome was not required.
Study Population and Sampling
The unit of analysis was the ED patient. The target population included all patients who visited the ED and needed inpatient admission. The source population included all patients who visited the ED of Dr. Cipto Mangunkusumo Hospital in 2019.
The eligible population included ED visits that fulfilled the following inclusion criterion: clinical ED attendance (all age) that was assessed through triage. ED visits were excluded if they met the following exclusion criteria: death on arrival, intrauterine foetal death, visit for visum et repertum examination, and clinical cases that should have been managed in the outpatient clinic (patients with no specific clinical complaints who were managed in the ED because their routine medications were used up or they needed routine minor wound care). If a patient had frequent ED visits (>1 visit) during the study period, we only included the final ED visit for analysis. The data of all eligible participants were retrospectively assessed by the researcher and included in this study (total sampling).
Study participants were identified after excluding patients with missing data (incomplete information for dependent and independent variables) and patients lost to follow-up (cancelled treatment in the ED or left without being checked-up; Figure 1). The requirement for informed consent was waived owing to the retrospective nature of the study.
 |
Figure 1 Flow chart of the study participants’ selection process. Abbreviations: ED; emergency department, h, hours; n, number of participants, DOA; death on arrival, IUFD; intra-uterine foetal death. |
Data Analysis
Categorical data are presented as frequency and proportion, and quantitative data are summarized using measures of central tendency. A causal model was developed using Cox regression analysis to measure the relative risk (RR) between ED LOS and in-hospital mortality. First, a crude association model was developed between the main independent variable (ED LOS) and dependent variable (in-hospital mortality). Second, all potential confounders (sex, age, triage category, trauma-related visits, labour-related visits, malignancy-related visits, and patient referral) were included in the analysis to build a hierarchically well-formulated model.
ED LOS was further stratified into ordinal categories (<8 h, 8–24 h, and >24 h) to assess the dose-response relationship. Sub-group analyses of the paediatric and adult patients’ data were performed to assess the consistency of the associations among different age groups. Interaction terms were not considered in the exploratory model. Data were analysed using SPSS version 22 (IBM Corp., Armonk, NY, USA).
Results
Data from 18,553 participants were included in the analysis (Figure 1). The baseline characteristics of the participants were as follows (Table 1): 51.1% were males, the median age was 38 years, and 60.8% were in the age interval of >18 years to 59 years. The proportion of ED visits was relatively similar across months. Most ED visits were in shift 2 (12:00–17:59), followed by shift 3 (18:00–23.59). Following triage, most participants (81.3%) were placed in the urgent category.
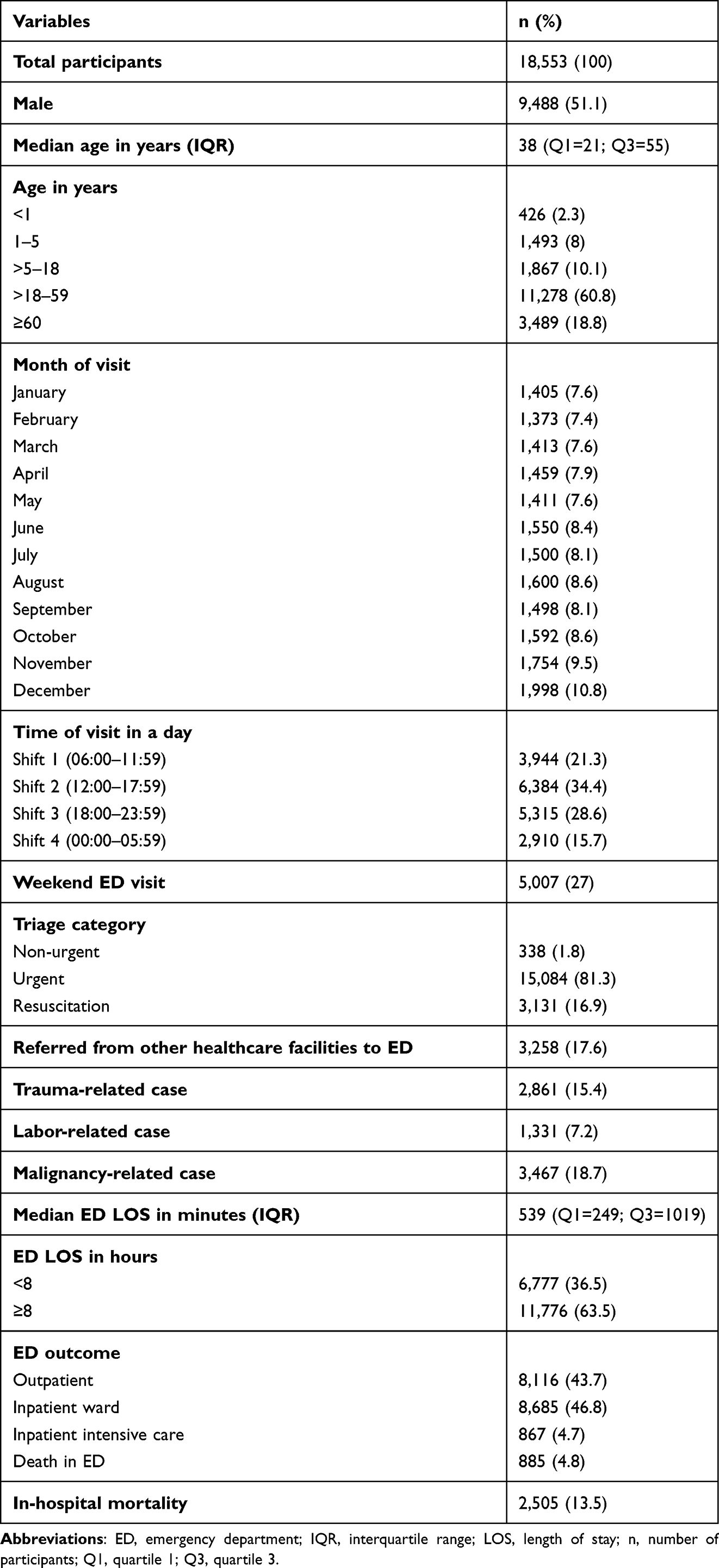 |
Table 1 Characteristics of Study Participants |
Of all cases, 17.6% had been referred from other healthcare facilities. Overall, 15.4% were trauma-related cases, 7.2% were labour-related cases, and 18.7% were malignancy-related cases. The median ED LOS was 539 minutes, and 63.5% of the participants had an ED LOS of ≥8 h. Admission to the inpatient ward was the most common ED outcome (46.8%), and a lower proportion of patients was admitted to the intensive care (4.7%). Moreover, 43.7% of participants were managed as outpatients after treatment and consultation in the ED. The overall in-hospital mortality was 13.5%.
Table 2 shows the 2×2 cross-tabulation matrix between exposure (ED LOS) and outcome (in-hospital mortality). Patients with prolonged ED LOS (≥8 h) showed higher mortality (18.3%) than those with an ED LOS <8 h (5.2%). The attributable risk was 13.1%, and the attributable risk proportion was 71.6%.
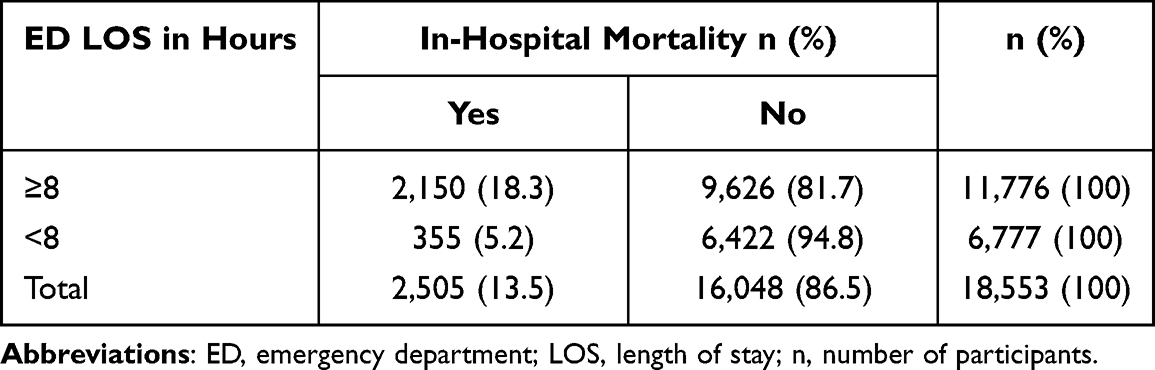 |
Table 2 A 2×2 Cross-Tabulation Matrix Between ED LOS (Exposure) and in-Hospital Mortality (Outcome) |
Based on Table 3, Model 1 showed a crude association that among ED patients that needed inpatient admission, a prolonged ED LOS was associated with risk of in-hospital mortality (RR, 3.48; 95% confidence interval [95% CI], 3.11–3.90). Model 2 was the hierarchical well formulated model and showed consistent association even after adjusting for all potential confounders, but there was slight reduction in the risk of in-hospital mortality (adjusted RR, 2.69; 95% CI, 2.40–3.02). To measure the dose-response relationship and consistency of the effect of ED LOS on mortality risk, we stratified the ED LOS into three categories (model 3). Table 4 showed that model 3 revealed a higher risk of in-hospital mortality among participants who stayed in the ED for >24 h (adjusted RR, 3.13; 95% CI, 2.76–3.53) than among those who stayed for 8–24 h (adjusted RR, 2.36; 95% CI, 2.08–2.66). Triage acuity and malignancies were associated with increase risk of mortality, trauma and labour-related cases were associated with decrease risk of mortality.
 |
Table 3 Results of Bivariate and Multivariate Cox-Regression Analysis to Examine the Association Between ED LOS and in-Hospital Mortality |
 |
Table 4 Multivariate Cox-Regression Analysis to Examine the Association Between ED LOS (Three Categories) and in-Hospital Mortality and Subgroup Analysis Based on Age (Pediatric =0–18 Years Old and Adult ≥18 Years Old) |
We also performed sub-group analysis to examine the association between prolonged ED LOS and in-hospital mortality among pediatric (age, 0–18 years) and adult (age, >18 years) participants. In the pediatric group, a prolonged ED LOS was associated with an increased risk of in-hospital mortality; however, there were no differences in risk between the groups with an ED-LOS of 8–24 h vs >24 h (adjusted RR, 1.58; 95% CI, 1.20–2.11 vs adjusted RR, 1.57; 95% CI, 1.21–2.04, respectively). Among adult participants, an ED LOS of >24 h was associated with a higher risk of in-hospital mortality than was ED LOS 8–24 h (adjusted RR, 3.68; 95% CI, 3.21–4.22 vs adjusted RR, 2.60; 95% CI, 2.26–2.97).
Table 5 describes the participant’s ED outcome stratified by to ED LOS. Most ED deaths occurred after an ED stay of ≥8 h (63.5%). Most of the patients who were admitted to the inpatient ward (85.1%) or intensive care unit (78%) waited for ≥8 h in the ED.
 |
Table 5 Participant Outcome in the ED Stratified by ED LOS |
Discussion
Model 1 revealed that a prolonged ED LOS was significantly associated with risk of in-hospital mortality. This result is clinically relevant because it indicates that ED LOS is an important determinant of in-hospital patient outcomes. Bivariate analysis between ED LOS and in-hospital mortality (Table 2) indicated that given the association of prolonged ED LOS on in-hospital mortality, 71.6% of the mortality among patients who stayed in the ED for ≥8 h may be attributable to the prolonged ED LOS (before adjusted with other confounders).
After adjustment for several confounders, there was a slight decrease in the effect of ED LOS on risk of in-hospital mortality (model 2). However, the trend and interpretation of the results remained consistent. Model 2 also showed that severity conditions (triage acuity) and malignancies-related conditions were associated with the increase risk of in-hospital mortality. The stratification of ED LOS into three categories (model 3) revealed similar results, indicating that participants with a prolonged ED LOS were associated with a higher risk of in-hospital mortality.
In the sub-group analysis, prolonged ED LOS was associated with an increased risk of in-hospital mortality in both paediatric (age ≤18 years) and adult (age >18 years) groups. In the paediatric group (model 4), there was no difference in adjusted RR between participants who stayed in the ED for >24 h and those who stayed for 8–24 h. However, the risk of in-hospital mortality was the highest in the adult group who stayed in the ED for >24 h (model 5).
Our findings are consistent with those of other large-scale studies on the association between ED LOS and mortality. Prolonged ED boarding (waiting time in the ED after the decision to admit has been made) has been shown to increase the risk of mortality in general ED patients,11 specific populations including trauma patients,19 and medical patients who need admission to the intensive care ward.8,20 However, several previous studies have not shown any consistent association between ED LOS and risk of mortality.10 Nevertheless, other negative outcomes of prolonged ED LOS have been reported, including prolonged hospital LOS,7,21 increased risk of missed treatment,22 and increased risk of adverse perioperative outcomes.23 One plausible explanation for this is that a longer ED LOS increases the risk of delayed treatment in the ED, nosocomial infections, and delays in appropriate supportive care in the inpatient setting.24
In a study that showed no negative effect of prolonged ED LOS on patient mortality, the ED had sufficient capability (including facility operations and human resources) to perform appropriate resuscitation protocols and had fewer incidences of overcrowding.25 Thus, reducing the standard ED LOS and waiting time can help increase the total quality of care26 and prevent overcrowding due to the simultaneous influx of new cases.5
The analysis of ED outcomes based on ED LOS showed that the ED had a serious problem in accessing the inpatient ward and intensive care unit (Table 5). Among patients admitted to the ward (n=8685), only 14.9% had the appropriate ED LOS of <8 h; among patients admitted to the intensive care unit (including the adult intensive care, adult high care, intensive cardiovascular care, paediatric intensive care, and neonatal intensive care units), only 22% had the target ED LOS of <8 h. ED mortality was the highest among participants who stayed in the ED for ≥8 h (63.5%), suggesting that the ED had limited ability to provide critical care to seriously ill patients for >8 h. This highlights the need for immediate access to the intensive care unit from the ED.
When selecting the eligible patients, we found that some ED visits were more appropriate for outpatient clinics (n=2,896). These included visits for procedures such as intravenous administration of antibiotics and nutrients, elective placement of a nasogastric tube, and postoperative wound management. Owing to the increasing need to reduce non-urgent visits to the ED, these types of visits should be minimised because they can put more pressure on the ED.6,27
This study had a large sample size and therefore had a good statistical power (power estimation based on the likelihood ratio test: >0.95). Moreover, the cohort retrospective nature of this study guaranteed a temporal relationship between the exposure (prolonged ED LOS) and outcome (mortality). Electronic health records represent valid sources of data regarding patient outcomes and provide valid measurements of ED attendance time and ED discharge time, which minimises the risk of information bias. The samples selected for analysis had a relatively low number of losses to follow-up and small amount of missing data (<1%). Therefore, the results of this study may be generalisable for patients who experience a prolonged ED LOS in similar hospitals—including referral and academic hospitals—in the study location.28 However, the results may differ for non-academic and private hospitals.
Our study also had some limitations. This was a single-centre study, and our results may not be generalisable to other institutions. Data from a dying patient may result in a shorter ED LOS due to early death; therefore, we stratified the severity of illness based on the triage system and adjusted the causal model accordingly. However, the triage system has limited accuracy as a surrogate for the severity of illness or as a tool for predicting the need for admission. As such, this method may have introduced some selection bias. We did not account for the time of the physician’s decision to admit the patient, which may have introduced unmeasured confounding. The decision to admit is an important factor for patients who have already received decisions related to admission. In addition, some patients were in a severe condition, were critically ill with haemodynamically unstable conditions requiring complex resuscitation (surgery or haemodialysis), or had conditions that made them non-transportable for admission to the intensive care unit. These patients had a prolonged ED LOS and had to stay in the ED until death.29,30 Also, this study did not consider other potential confounders that could have affected the primary outcome, such as terminal disease, common comorbidities such as cardiac disease or renal disease, and admission to an isolation ward. Further studies should be performed to break down the total ED LOS into several business processes (ED wait time, ED treatment time, ED disposition time, and ED boarding time), addressed various comorbidities as confounders and to evaluate several patient outcomes such as hospital LOS, rate of intensive care unit admission, and rate of intubation in ED.
Conclusion
In conclusion, we found that prolonged ED was associated with an increased risk of in-hospital mortality at Dr. Cipto Mangunkusumo Hospital in Jakarta, Indonesia after adjusted with several confounders. In future, hospital service plans should aim to reduce the ED LOS and increase patient flow to the inpatient ward, which can help improve the quality of patient care.
Acknowledgments
We acknowledge the Head of the Emergency Department, Dr. Yogi Prabowo, SpOT(K); the Emergency Medical Managers (Dr. Radi Muharris Mulyana, SpOT(K); Dr. Septo Sulistio, SpAn; and Dr. Imamul Aziz Albar, SpOT(K)); and the staff of the Emergency Department at Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia. We also acknowledge the Data management team made of Friska Putri Amalia, Swasti Despriningtyas, Indah, and Rasmawati. Proofreading services were provided by Editage (www.editage.com).
Funding
This study was supported by a PUTI grant of Universitas Indonesia (contract number KB-613/UN2.RST/HKP.05.00/2020).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Taylor TB. Threats to the health care safety net. Acad Emerg Med. 2001;8(11):1080–1087. doi:10.1111/j.1553-2712.2001.tb01119.x
2. World Health Organization. Monitoring health for the SDGs. Available from: https://www.who.int/data/gho/data/themes/world-health-statistics.
3. Moore BJ, Stocks C, Owens PL. Trends in Emergency Department Visits 2006–2014. HCUP Statistical Brief #227. Rockville, MD: Agency for Healthcare Research and Quality; 2017.
4. National Center for Health Statistics. Emergency Department visits 2018. Available from: https://www.cdc.gov/nchs/fastats/emergency-department.htm.
5. Canadian Association of Emergency Physicians and National Emergency Nurses Affiliation. Joint position statement on emergency department overcrowding. CJEM. 2001;3(2):82–88. doi:10.1017/S1481803500005285
6. American College of Emergency Physicians policy statement. Crowding. Available from: https://www.acep.org/patient-care/policy-statements/crowding/.
7. Chong CP, Haywood C, Barker A, et al. Is emergency department length of stay associated with inpatient mortality? Aust J Ageing. 2013;32(2):122–124. doi:10.1111/j.1741-6612.2012.00651.x
8. Al-Qahtani S, Alsultan A, Haddad S, et al. The association of duration of boarding in the emergency room and the outcome of patients admitted to the intensive care unit. BMC Emerg Med. 2017;17(1):34. doi:10.1186/s12873-017-0143-4
9. Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard medical practice study I. N Engl J Med. 1991;324(6):370–376. doi:10.1056/NEJM199102073240604
10. Boudi Z, Lauque D, Alsabri M, et al. Association between boarding in the emergency department and in-hospital mortality: a systematic review. PLoS One. 2020;15(4):e0231253. doi:10.1371/journal.pone.0231253
11. Singer AJ, Thode HC, Viccellio P, et al. The association between length of emergency department boarding and mortality. Acad Emerg Med. 2011;18(12):1324–1329. doi:10.1111/j.1553-2712.2011.01236.x
12. Yusvirazi L, Sulistio S, Ramlan AAW, et al. Snapshot of emergency departments in Jakarta, Indonesia. Emerg Med Aust. 2020;32(4):830–839. doi:10.1111/1742-6723.13570
13. Habib H, Sulistio S, Albar IA, et al. Validation of the Cipto triage method: a single-centre study from Indonesia. Open Access Emerg Med. 2020;12:137–143. doi:10.2147/OAEM.S246598
14. Cipto Mangunkusumo Hospital.Keputusan Direktur Utama RSUP Nasional dr. Cipto Mangunkusumo No: HK.01.07/3.3/12068/2019 tentang kapasitas tempat tidur RSUPN dr Cipto Mangunkusumo [Regulation of Chief Director of dr. Cipto Mangunkusumo Hospital Regarding Hospital Bed Capacity No: HK.01.07/3.3/12068/2019]; 2019.
15. von Elm E, Altman DG, Egger M, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
16. Affleck A, Parks P, Drummond A, et al. Emergency department overcrowding and access block. CJEM. 2013;15(6):359–384. doi:10.1017/S1481803500002451
17. Derose SF, Gabayan GZ, Chiu VY, et al. Emergency department crowding predict admission length-of-stay but not mortality in a large health system. Med Care. 2014;52(7):602–611. doi:10.1097/MLR.0000000000000141
18. Emergency Department. Emergency department service guideline of RSCM. RS dr Cipto Mangunkusumo; 2018.
19. Mowery NT, Dougherty SD, Hildreth AN, et al. Emergency department length of stay is an independent predictor of hospital mortality in trauma activation patients. J Trauma. 2011;70(6):1317–1325. doi:10.1097/TA.0b013e3182175199
20. Chalfin DB, Trzeciak S, Likourezos A, et al. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35(6):1477–1483. doi:10.1097/01.CCM.0000266585.74905.5A
21. Lord K, Parwani V, Ulrich A, et al. Emergency department boarding and adverse hospitalization outcomes among patients admitted to a general medical service. Am J Emerg Med. 2018;36(7):1246–1248. doi:10.1016/j.ajem.2018.03.043
22. Liu SW, Thomas SH, Gordon JA, et al. A pilot study examining undesirable events among emergency department-boarded patients awaiting inpatient beds. Ann Emerg Med. 2009;54(3):381–385. doi:10.1016/j.annemergmed.2009.02.001
23. Montes FR, Vásquez SM, Camargo-Rojas CM, et al. Association between emergency department length of stay and adverse perioperative outcomes in emergency surgery: a cohort study in two Colombian University hospitals. BMC Emerg Med. 2019;19(1):27. doi:10.1186/s12873-019-0241-6
24. Junhasavasdikul D, Theerawit P, Kiatboonsri S. Association between admission delay and adverse outcome of emergency medical patients. Emerg Med J. 2013;30(4):320–323. doi:10.1136/emermed-2011-200788
25. Agustin M, Price LL, Andoh-Duku A, et al. Impact of delayed admission to the intensive care unit from the emergency department upon sepsis outcomes and sepsis protocol compliance. Crit Care Res Pract. 2017;2017:9616545. doi:10.1155/2017/9616545
26. Vermeulen MJ, Guttmann A, Stukel TA, et al. Are reductions in emergency department length of stay associated with improvements in quality of care? A difference-in-differences analysis. BMJ Qual Saf. 2016;25(7):489–498. doi:10.1136/bmjqs-2015-004189
27. Wang Z, Xiong X, Wang S, et al. Causes of emergency department overcrowding and blockage of access to critical services in Beijing: a 2-year study. J Emerg Med. 2018;54(5):665–673. doi:10.1016/j.jemermed.2018.02.009
28. Oktaviani AS, Hakim DDL, Suwarman S. Response time, decision time, and delivery time in pediatric emergency unit of West Java top referral hospital. AMJ. 2017;4(3):33–38.
29. Chaou CH, Chiu TF, Yen AM, et al. Analyzing factors affecting emergency department length of stay-using a competing risk-accelerated failure time model. Medicine. 2016;95(14):e3263. doi:10.1097/MD.0000000000003263
30. Rose L, Scales DC, Atzema C, et al. Emergency department length of stay for critical care admissions. A population-based study. Ann Am Thorac Soc. 2016;13(8):1324–1332. doi:10.1513/AnnalsATS.201511-773OC
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.