Back to Journals » International Journal of General Medicine » Volume 18
Association Between the Aggregate Index of Systemic Inflammation and Slow Coronary Flow Phenomenon in Patients with Ischemia and No Obstructive Coronary Arteries
Authors Wang HY, Guo J, Hong MY, Li JJ, Jin XQ
Received 14 January 2025
Accepted for publication 5 March 2025
Published 12 March 2025 Volume 2025:18 Pages 1431—1438
DOI https://doi.org/10.2147/IJGM.S515822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Hong-Yang Wang,1 Jiang Guo,2 Min-Yan Hong,3 Jia-Jia Li,4 Xue-Qiang Jin3
1Department of Cardiovascular Medicine, The First People’s Hospital of Linhai, Taizhou, Zhejiang, 317000, People’s Republic of China; 2Department of Cardiovascular Medicine, Longquan People’s Hospital Affiliated to Lishui University, LiShui, Zhejiang, 323700, People’s Republic of China; 3Department of General Surgery, The First People’s Hospital of Linhai, Taizhou, Zhejiang, 317000, People’s Republic of China; 4Department of Emergency Medicine, The First People’s Hospital of Linhai, Taizhou, Zhejiang, 317000, People’s Republic of China
Correspondence: Xue-Qiang Jin, Email [email protected]
Background: Inflammation has been proposed as a potential pathogenic mechanism underlying the slow coronary flow phenomenon (SCFP). The aggregate index of systemic inflammation (AISI), a novel biomarker for evaluating inflammation, has been linked to various cardiovascular diseases. However, the relationship between AISI and the occurrence of SCFP in patients with ischemia and non - obstructive coronary arteries (INOCA) remains unclear.
Methods: In this study, 1328 consecutive patients with INOCA were recruited. Among them, 90 patients had SCFP (SCFP group). A total of 180 age - and sex - matched individuals with INOCA and normal blood flow were selected as controls at a ratio of 1:2. Clinical manifestations, laboratory parameters, and angiographic features were recorded to identify potential predictors of SCFP in INOCA patients.
Results: Compared with the control group, patients in the SCFP group had a higher prevalence of current smoking, as well as elevated white blood cell (WBC), neutrophil, monocyte, and platelet counts, and a higher AISI. The AISI value increased with the number of vessels affected by SCFP. Multivariate logistic regression analysis demonstrated that the WBC count and AISI were independent predictors of SCFP in INOCA patients. Additionally, when the AISI was > 264.1, the sensitivity and specificity were 64.4% and 64.4% respectively, and the area under the receiver operating characteristic curve (AUC) was 0.657 (95% CI: 0.590– 0.723, P < 0.001). The AISI had a more favorable predictive value for the presence of SCFP than WBC, neutrophils, lymphocytes, monocytes, and platelets alone (P < 0.05).
Conclusion: Higher AISI scores are associated with an increased risk of SCFP in INOCA patients. As an easily - obtained biomarker for assessing the degree of inflammation, the AISI can serve as a promising tool for risk stratification and appropriate management in INOCA patients.
Keywords: aggregate index of systemic inflammation, slow coronary flow phenomenon, ischemia and no obstructive coronary arteries, predictors
Introduction
Slow coronary flow (SCFP) was first reported by Tambe et al in 1972, which is characterized by delayed coronary blood flow in the absence of obstructive coronary artery disease (CAD).1 Initially, SCFP was considered to be a benign angiographic finding. With the deepening of understanding and research, SCFP has been suggested as an ominous phenomenon that predisposes individuals to atherosclerosis and obstructive CAD.2 Moreover, in some case reports, SCFP is associated with sudden cardiac death due to ventricular arrhythmias3 and ST-segment elevation myocardial infarction (STEMI).4 As a subtype of ischemia and no obstructive coronary arteries (INOCA), SCFP had quite a complex pathogenesis. Although the pathogenic mechanism of SCFP is not fully elucidated, accumulating evidence has confirmed that early atherosclerosis,2 microvascular disorder,5 endothelial function,6,7 oxidative stress,7 and inflammation8–12 are recognized as important pathogenesis in the initiation and development of SCFP.
Inflammation plays a pivotal role in the development of atherosclerosis and CAD,13 the monocytes, neutrophils, and lymphocytes are intricately involved in this process.14 Consequently, in recent years, a growing body of research has centered on routine blood tests and their derived indicators, which are easily acquired and calculated. The aggregate index of systemic inflammation (AISI), which represents the degree of immunity and inflammation through multiple blood cells, such as neutrophils, lymphocytes, monocytes, and platelets, was initially shown to be associated with prolonged hospital stay in open elective thoracic surgery.15 Recently, AISI has been increasingly investigated in the context of CAD.16–21
Given the complex pathogenesis of SCFP, the diverse clinical manifestations, and the significant association between inflammation and SCFP, we aimed to investigate the potential role of the AISI in the occurrence of SCFP. We hypothesized that high AISI is associated with an increased risk of SCFP in patients with INOCA.
Methods
Study Population
We consecutively recruited 1328 patients with INOCA in the present study between March 2019 and February 2024. The flowchart of the study is presented in Figure 1. 90 patients had SCFP (SCFP group), accounting for 6.8% of individuals with INOCA. A total of 180 age - and sex - matched individuals with INOCA and normal blood flow were selected as controls at a ratio of 1:2 using a simple random sampling method (n=180). In total, 270 individuals were included in the study. The exclusion criteria are shown in Figure 1. This study was conducted in accordance with the ethical standards of the Helsinki Declaration. Informed consent was obtained before participation.
 |
Figure 1 The study flowchart. |
Coronary Angiography
Coronary angiography was performed by experienced cardiologists using the standard Judkins technique, and the Thrombolysis in Myocardial Infarction (TIMI) frame count (TFC) was used to quantitatively evaluate the coronary blood flow.22 The first frame was defined as antegrade contrast filling in 70% of the ostium of left anterior descending artery (LAD), left circumflex (LCX) and right coronary artery (RCA). The last frame was defined as the contrast filling the mustache area for the LAD, bifurcation segment with the farthest distance for the LCX, and first branch of the posterolateral artery for the RCA.22 TFC was calculated as the last frame count minus the first frame count.22 Considering the longer distance of the LAD, the corrected TFC (TFC divided by 1.7) was calculated to assess the coronary blood flow of the LAD.22 The cut off value of TFC for SCFP were 36.2±2.6 for the LAD (21.1±1.5 cTFC), 22.2±4.1 for the LCX, and 20.4±3.1 for the RCA.16 If the TFC of any of the three main coronary vessels exceeded the diagnostic criteria, SCFP was diagnosed. The mean TFC (mTFC) was calculated by dividing the sum of the TFC of the three main vessels by three.8–11
Laboratory Measurements
Routine blood biochemical examinations were conducted prior to the procedure. Laboratory parameters, including routine blood testing, were performed at the core laboratory of our hospital. AISI was calculated as follows: neutrophil count × platelet count × monocyte count platelet/lymphocyte count.15
Statistical Analysis
SPSS software (version 20.0) was used for data processing. Categorical variables are shown as rates or percentages and were analyzed using chi-square or Fisher’s exact test. Continuous variables were displayed as mean±standard deviation or median and 25th-75th percentile values, which were compared using the t-test or Mann–Whitney U-test, as applicable. Univariate logistic regression analysis was used to investigate indicators associated with the presence of SCFP. Factors with a p value <0.1 were added in the multivariate logistic regression analysis to determine the independent predictors for the presence of SCFP in patients with INOCA. Smoking status, WBC count, AISI, hypertension, and diabetes mellitus were included in the univariate analysis. The receiver operating characteristic (ROC) curve was used to determine the predictive value of the factors associated with CSFP. The 2-sided P<0.05 was considered statistical significance.
Results
Baseline and Clinical Characteristics
The baseline characteristics and medication histories are displayed in Table 1. Variables including age, sex, body mass index (BMI), heart rate, comorbidities (hypertension and diabetes mellitus), and medication history did not show significant difference between the two groups (p>0.05) (Table 1). However, compared to controls, patients with SCFP had a higher proportion of current smokers (p < 0.05) (Table 1).
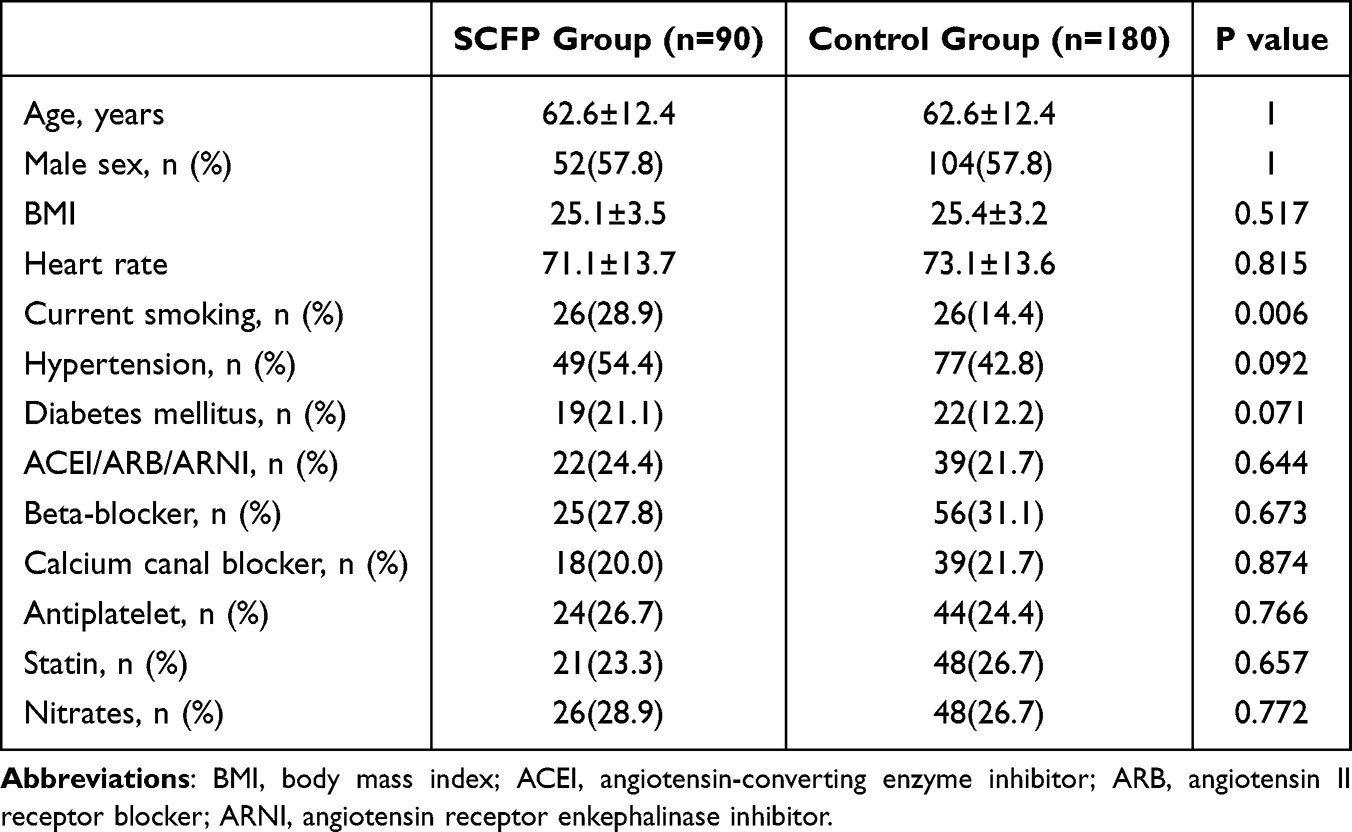 |
Table 1 Baseline Characteristics and Medication of the Two Groups |
Laboratory Parameters of the Two Groups
The laboratory indicators are listed in Table 2. An increased white blood cell (WBC) count, neutrophil count, monocyte count, platelets count, and AISI were observed in patients with CSFP compared to controls (p< 0.05) (Table 2). For the remaining parameters, including lymphocyte count, fasting blood glucose (FBG), creatinine (Cr), albumin (ALB), and lipid indicators, there were no significant differences between the two groups (p>0.05) (Table 2).
 |
Table 2 Laboratory Parameters of the Two Groups |
Angiographic Findings of the Two Groups
The angiographic findings are shown in Table 3. We found that 90 individuals developed SCFP in at least one main coronary vessel. The TFCs in patients with SCFP were significantly higher than those in controls (p < 0.001) (Table 3). A total of 29 individuals (32.2%) were affected by SCFP in one coronary arteries, 28 (3.1%) in two coronary arteries, and 33 (36.7) in three coronary arteries. In terms of the vessels involved, the RCA was the most frequently affected, followed by LAD and LCX (Table 3).
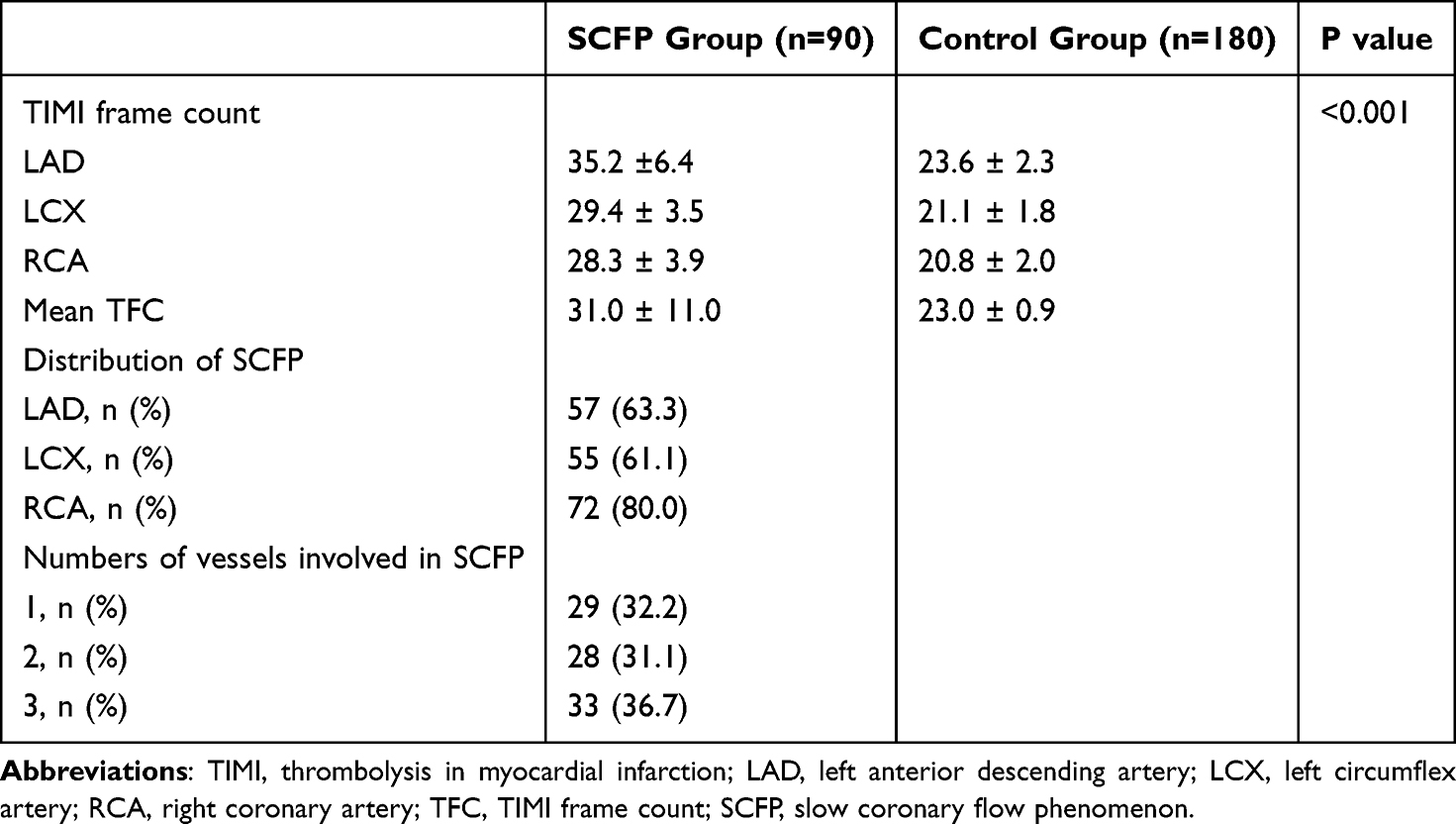 |
Table 3 Angiographic Findings of the Two Groups |
Predictors of SCFP
Smoking, WBC count, AISI, hypertension, and diabetes mellitus were included in the univariate analysis to investigate the potential risk factors for the presence of SCFP. As shown in Table 4, the WBC count and AISI were associated with SCFP. Multivariate logistic analysis showed that WBC count and AISI were independent predictors of SCFP in patients with INOCA (Table 4). In addition, we found that the AISI increased as the number of vessels affected by SCFP increased (Figure 2). The ROC curve was used to assess the predictive value of indicators for the presence of SCFP. When the AISI was > 264.1, the sensitivity and specificity were 64.4% and 64.4%, respectively, and the area under the ROC curve (AUC) was 0.657 (95% CI: 0.590–0.723, P < 0.001). AISI had a better predictive value for the presence of SCFP than WBC, neutrophils, lymphocytes, monocytes, and platelets alone (Table 5 and Figure 3).
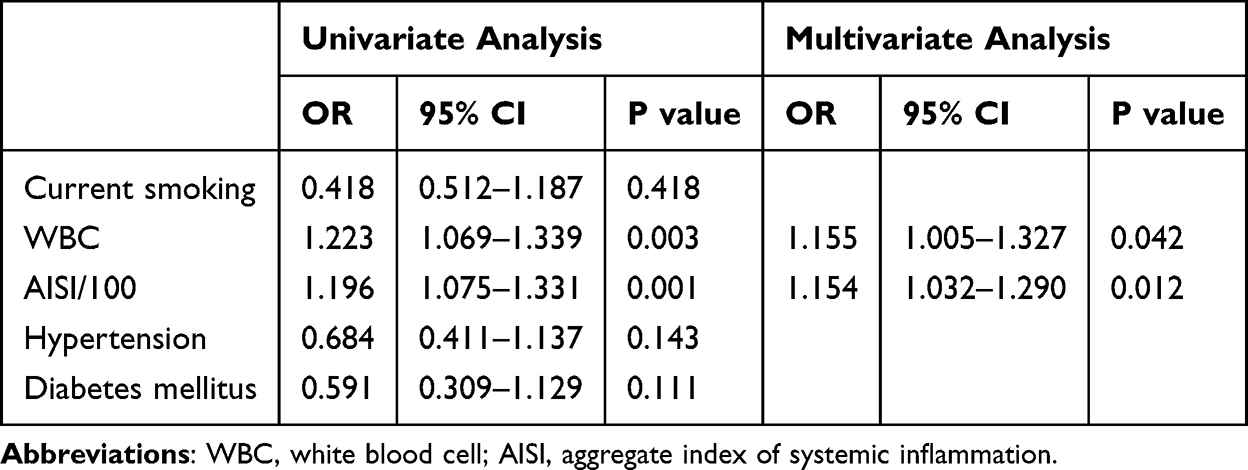 |
Table 4 Univariate and Multivariate Logistic Regression Analysis for Presence of SCFP |
 |
Table 5 ROC Analysis of the Related Parameters |
 |
Figure 2 Correlation between the number of vessels affected by SCFP and AISI. |
 |
Figure 3 ROC curve showing the predicting value of risk factors for the presence of SCFP. |
Discussion
In the current study, we first explored the relationship between the AISI and the presence of SCFP in patients with INOCA. We found that a higher AISI score was associated with an increased risk of SCFP among INOCA patients. Additionally, the AISI increased with the number of vessels affected by SCFP. AISI could serve as a promising indicator for risk assessment as well as for the appropriate management of INOCA.
As a matter of fact, SCFP is not merely an angiographic finding. This study had several important clinical implications. Unlike cardiac X syndrome (CXS), patients with SCFP are more prone to suffer angina attacks at rest rather than exertional angina in CXS.6,9–11 Moreover, nearly 20% of SCFP patients had repeated emergency visits or admissions to the CCU due to recurrent angina attacks resembling ACS.5,6,9–11 Some patients may even experience sudden cardiac death3 and STEMI.4 Therefore, precise prediction of SCFP in INOCA is important for the optimal management of these specific populations. However, the available indicators for the predicting SCFP in patients with INOCA are still limited. Hence, in the present study, we aimed to explore the easily acquired and calculated indicators for the presence of SCFP in patients with INOCA to improve the management of these patients.
However, the relationship between the traditional CVD risk factors and SCFP remains unclear. Some studies have suggested that hypertension and diabetes are the risk factors for SCFP.23,24 In other studies, no significant associations were found.6,8–11,25 In the present study, there was no significant difference in the incidence of hypertension and diabetes between the groups. However, the p-value was less than 0.1. Therefore, hypertension and diabetes were included in univariate analysis. We found that hypertension and diabetes were not associated with SCFP. We speculate that SCFP is a unique clinical entity with complex pathogenesis and diverse clinical manifestations. Different studies had different comorbidities, medications, sample sizes, and races; therefore, different results.9–11 Nonetheless, optimal management of these risk factors is still important.
Although the pathogenesis of SCFP is not fully understood, substantial evidence supports the relationship between inflammation and SCFP.8–12 As a newly developed indicator for assessing inflammation, the AISI integrates various blood cells, including neutrophils, lymphocytes, monocytes, and platelets.15 It is well established that an increased inflammatory reaction is a significant pathological change during the initiation and development of CAD.13 Systemic inflammation can increase platelet reactivity, resulting in localized ischemia, hypoxia, and microthrombus formation, ultimately causing tissue necrosis.26 A decreased lymphocyte count suggests increased cell death and subsequent immune system dysfunction.20 Lymphocyte apoptosis, along with an increase in monocytes and neutrophils, collectively aggravates the development of atherosclerosis,20 resulting in a higher risk of SCFP. A high AISI indicates an increased inflammatory response and disrupted immune function, which contribute to the initiation and development of SCFP in patients with INOCA. A recent study demonstrated that patients with SCFP had higher neutrophil counts and that the neutrophil percentage to albumin ratio was an independent predictor of the presence of SCFP.9 Moreover, in recent years, indicators derived from blood cells, including pan-immune-inflammation,12 systemic immune-inflammation index (SII),8 and systemic inflammation response index (SIRI),10 have been proven to be associated with the presence of SCFP in patients with INOCA. Nonetheless, the relationship between the AISI and SCFP remains undetermined. Therefore, we aimed to investigate the potential role of the AISI in the presence of SCFP in patients with INOCA. We discovered that patients with SCFP had increased AISI, which could serve as a valuable predictor of SCFP occurrence in INOCA. Initially, AISI was demonstrated as a predictor of an increased risk of prolonged hospital stay in patients who underwent open chest surgery.15 Recently, the AISI has been widely discussed in CAD. AISI is associated with in-stent restenosis after PCI,16 major adverse cardiovascular events (MACE) in patients with acute coronary syndrome,17 myocardial infarction with non-obstructive coronary arteries,18 cardiovascular death in acute myocardial infarction,20 and in-hospital mortality in patients with aortic stenosis after mechanical aortic valve replacement.21 It is speculated that this association between AISI and CVD may be caused by the combined effects of different inflammatory blood cells. Considering the contributions of these inflammatory blood cells to the pathogenesis of SCFP, the combined indicator of AISI has a biological rationale and a reliable clinical indication.
Limitations
This study had some limitations. First, it was a single-center study with a relatively small sample size, which may have limited the analysis. Second, although we tried to include all the indicators associated with SCFP, some may have escaped from this study, which may have affected prediction efficiency. Third, the gold standard index of inflammation, C-reactive protein (CRP), was not included in the present study. Finally, large-scale multicenter studies are required to validate our conclusions.
Conclusion
We discovered that increased AISI may provide a valuable and reliable method for distinguishing SCFP from INOCA. AISI provided a better predictive value for the presence of SCFP than indicators alone.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available because of further study in this area but are available from the corresponding author upon reasonable request.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Tambe AA, Demany MA, Zimmerman HA, et al. Angina pectoris and slow flow velocity of dye in coronary arteries--a new angiographic finding. Am Heart J. 1972;84(1):66–71. doi:10.1016/0002-8703(72)90307-9
2. Sadr-Ameli MA, Saedi S, Saedi T, et al. Coronary slow flow: benign or ominous? Anatol J Cardiol. 2015;15(7):531–535. doi:10.5152/akd.2014.5578
3. Saya S, Hennebry TA, Lozano P, et al. Coronary slow flow phenomenon and risk for sudden cardiac death due to ventricular arrhythmias: a case report and review of literature. Clin Cardiol. 2008;31(8):352–355. doi:10.1002/clc.20266
4. Sen T. Coronary slow flow phenomenon leads to ST elevation myocardial infarction. Korean Circ J. 2013;43(3):196–198. doi:10.4070/kcj.2013.43.3.196
5. Beltrame JF, Limaye SB, Horowitz JD. The coronary slow flow phenomenon--a new coronary microvascular disorder. Cardiology. 2002;97(4):197–202. doi:10.1159/000063121
6. Wang Y, Jia PY, Chen BJ, et al. Evaluation of plasma thrombomodulin in patients with coronary slow flow. Cardiology. 2017;138(3):141–146. doi:10.1159/000460239
7. Kopetz V, Kennedy J, Heresztyn T, et al. Endothelial function, oxidative stress and inflammatory studies in chronic coronary slow flow phenomenon patients. Cardiology. 2012;121(3):197–203. doi:10.1159/000336948
8. Dai XT, Kong TZ, Zhang XJ, et al. Relationship between increased systemic immune-inflammation index and coronary slow flow phenomenon. BMC Cardiovasc Disord. 2022;22(1):362. doi:10.1186/s12872-022-02798-0
9. Zang SW, Long JJ, Wang Y. Neutrophil percentage to albumin ratio as a predictor for coronary slow flow phenomenon in patients with myocardial ischemia with no obstructive coronary arteries. Int J Gen Med. 2024;17:3511–3519. doi:10.2147/IJGM.S477431
10. Chen YD, Wen ZG, Long JJ, et al. Association between systemic inflammation response index and slow coronary flow phenomenon in patients with ischemia and no obstructive coronary arteries. Int J Gen Med. 2024;17:4045–4053. doi:10.2147/IJGM.S481538
11. Yang SB, Cui Y, Hou JJ, et al. Assessment of the relationship between plasma fibrinogen-to-albumin ratio and slow coronary flow phenomenon in patients without obstructive coronary artery disease. BMC Cardiovasc Disord. 2023;23(1):540. doi:10.1186/s12872-023-03579-z
12. Akkaya S, Cakmak U. Association between pan-immune-inflammation value and coronary slow flow phenomenon in patients with angiographically normal coronary arteries. Int J Cardiol. 2024;398:131631. doi:10.1016/j.ijcard.2023.131631
13. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685–1695. doi:10.1056/NEJMra043430
14. Wei C, Fan W, Zhang Y, et al. Nomograms based on the albumin/neutrophil-to-lymphocyte ratio score for predicting coronary artery disease or subclinical coronary artery disease. J Inflamm Res. 2023;16:169–182. doi:10.2147/JIR.S392482
15. Paliogiannis P, Ginesu GC, Tanda C, et al. Inflammatory cell indexes as preoperative predictors of hospital stay in open elective thoracic surgery. ANZ J Surg. 2018;88(6):616–620. doi:10.1111/ans.14557
16. Hou L, Zhao J, He T, et al. Machine learning-based prediction of in-stent restenosis risk using systemic inflammation aggregation index following coronary stent placement. Risk Manag Healthc Policy. 2024;17:1779–1786. doi:10.2147/RMHP.S468235
17. Fan W, Wei C, Liu Y, et al. The prognostic value of hematologic inflammatory markers in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Clin Appl Thromb Hemost. 2022;28:10760296221146183. doi:10.1177/10760296221146183
18. Zhou H, Li X, Wang W, et al. Immune-inflammatory biomarkers for the occurrence of MACE in patients with myocardial infarction with non-obstructive coronary arteries. Front Cardiovasc Med. 2024;11:1367919. doi:10.3389/fcvm.2024.1367919
19. Xiu J, Lin X, Chen Q, et al. The aggregate index of systemic inflammation (AISI): a novel predictor for hypertension. Front Cardiovasc Med. 2023;10:1163900. doi:10.3389/fcvm.2023.1163900
20. Jiang Y, Luo B, Lu W, et al. Association between the aggregate index of systemic inflammation and clinical outcomes in patients with acute myocardial infarction: a retrospective study. J Inflamm Res. 2024;17:7057–7067. doi:10.2147/JIR.S481515
21. Shvartz V, Sokolskaya M, Ispiryan A, et al. The role of novel biomarkers of systemic inflammation in the development of early hospital events after aortic valve replacement in patients with aortic stenosis. Life. 2023;13(6):1395. doi:10.3390/life13061395
22. Gibson CM, Cannon CP, Daley WL, et al. TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation. 1996;93(5):879–888. doi:10.1161/01.CIR.93.5.879
23. Sanghvi S, Mathur R, Baroopal A, et al. Clinical, demographic, risk factor and angiographic profile of coronary slow flow phenomenon: a single centre experience. Indian Heart J. 2018;70 Suppl 3(Suppl 3):S290–S294. doi:10.1016/j.ihj.2018.06.001
24. Sanati H, Kiani R, Shakerian F, et al. Coronary slow flow phenomenon clinical findings and predictors. Res Cardiovasc Med. 2016;5(1):e30296. doi:10.5812/cardiovascmed.30296
25. Wang Y, Liu MJ, Yang HM, et al. Association between increased serum alkaline phosphatase and the coronary slow flow phenomenon. BMC Cardiovasc Disord. 2018;18(1):138. doi:10.1186/s12872-018-0873-6
26. Kim KH, Barazia A, Cho J. Real-time imaging of heterotypic platelet-neutrophil interactions on the activated endothelium during vascular inflammation and thrombus Formation in live mice. J Vis Exp. 2013;74:50329. doi:10.3791/50329
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.