Back to Journals » Journal of Inflammation Research » Volume 19
Association Between Systemic Inflammation Indices and Recurrence Risk in Primary Budd-Chiari Syndrome
Authors Shen Z, Ni M, Liu Y, Zhang H, Xing X, Zhang Q, Zu M ![]() , Li Y
, Li Y ![]() , Li S
, Li S
Received 7 November 2025
Accepted for publication 30 January 2026
Published 10 June 2026 Volume 2026:19 579101
DOI https://doi.org/10.2147/JIR.S579101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fatih Türker
Ziyuan Shen,1 Man Ni,1 Yang Liu,1 Huijie Zhang,1 Xing Xing,2 Qingqiao Zhang,3 Maoheng Zu,3 Yan Li,3 Shengli Li1
1Clinical Research Institute, Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, 221006, People’s Republic of China; 2Department of Biostatistics, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, 21205, USA; 3Department of Interventional Radiology, Affiliated Hospital of Xuzhou Medical University, Xuzhou, 221004, People’s Republic of China
Correspondence: Shengli Li, Email [email protected] Qingqiao Zhang, Email [email protected]
Background: Budd-Chiari syndrome (BCS) is a rare thrombotic liver disorder with a substantial risk of recurrence, even after treatment. Inflammation-based markers such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and lymphocyte-to-monocyte ratio (LMR) have been associated with thrombotic diseases, but their predictive value for BCS recurrence remains unclear.
Methods: This retrospective cohort study included 708 (median 51 y, male: 57.8%) patients diagnosed with primary BCS between January 2015 and July 2022. Nine systemic inflammatory indices were calculated from baseline and biochemical parameters. The primary outcome was recurrence, defined by clinical symptoms and imaging-confirmed re-obstruction or thrombosis. Associations were evaluated using logistic regression models, quartile-based logistic regression, and weighted quantile sum (WQS) regression. Subgroup and interaction analyses were also performed.
Results: During follow-up, 226 patients (31.9%) experienced post-treatment recurrence. Elevated NLR and PLR were associated with increased recurrence risk, while higher LMR was protective. WQS regression identified novel indices such as the neutrophil-to-albumin ratio (NAR) and monocyte-to-albumin ratio (MAR) as top contributors. Subgroup analyses showed consistent associations, especially in IVC-type BCS and cirrhotic patients.
Conclusion: Several inflammation-based indices were independently associated with recurrence risk in primary BCS. These findings highlight the potential utility of inflammatory markers in recurrence surveillance.
Keywords: Budd-Chiari syndrome, inflammatory indices, recurrence, weighted quantile sum
Introduction
Budd-Chiari syndrome (BCS) is a rare vascular liver disorder characterized by obstruction of hepatic venous outflow at the level of the hepatic veins, the inferior vena cava (IVC), or the right atrium.1,2 BCS presents with a spectrum of manifestations, from asymptomatic liver enzyme elevation to acute liver failure. The annual incidence of BCS ranges from 0.168 to 4.09 per million, and the prevalence from 2.40 to 33.10 per million.3 BCS is classified into primary and secondary types. Primary BCS, results from intrinsic venous lesions, and is frequently associated with prothrombotic conditions.4 Secondary BCS arises from extrinsic compression or invasion of the hepatic venous outflow tract by space-occupying lesions, including tumors or abscesses. Although diagnostic and therapeutic strategies have advanced in recent years, particularly with the use of anticoagulation, endovascular interventions such as stenting and transjugular intrahepatic portosystemic shunt (TIPS), and in selected cases, liver transplantation, primary BCS remains challenging to manage.5–8 The risk of recurrence after treatment is considerable and has a significant impact on long-term prognosis and clinical outcomes.
Previous studies have identified several clinical predictors of recurrence in BCS, including history of thrombosis, incomplete recanalization, and anatomical involvement of the IVC or multiple hepatic veins.9,10 However, these indicators often require imaging or invasive assessment and are not routinely used in long-term follow-up. Systemic inflammation has been suggested to play a role in vascular injury and thrombotic events in several liver and vascular disorders.11–13 Inflammatory indices derived from routine blood tests, such as the neutrophil-to-lymphocyte ratio (NLR), systemic immune-inflammation index (SII), and platelet-to-lymphocyte ratio (PLR), have shown prognostic value in conditions including liver cirrhosis, hepatocellular carcinoma, and portal vein thrombosis.14–17 More recently, composite indicators such as the aggregate index of systemic inflammation (AISI), systemic inflammation response index (SIRI), and monocyte-to-lymphocyte ratio (MLR) have emerged as promising tools in evaluating inflammation-related complications in both hepatic and extra-hepatic vascular disorders.18 These indices may reflect immune activation, endothelial dysfunction, and hypercoagulable states.
Our previous work employed a zero-inflated model to explore the clinical and anatomical factors associated with BCS recurrence,19 and further developed a machine learning model based on multiple kernel learning to predict 3-year recurrence risk.20 However, the potential role of inflammation-based indices in predicting recurrence has not been thoroughly investigated. These indices are simple, cost-effective, and may serve as non-invasive tools for risk stratification. Exploring their predictive utility could complement existing anatomical and clinical parameters to improve individualized follow-up strategies. Therefore, this study aimed to evaluate the predictive utility of inflammation-based indices for recurrence in BCS.
Materials and Methods
Study Design
This retrospective study included patients diagnosed with primary BCS at the Affiliated Hospital of Xuzhou Medical University between January 2015 and July 2022. A total of 708 eligible patients were enrolled. Clinical, laboratory, and imaging data were collected and analyzed retrospectively. The diagnosis of BCS was established based on the 2021 consensus criteria issued by the Asian Pacific Association for the Study of the Liver, and was confirmed by imaging modalities including Doppler ultrasound, computed tomography, and angiography.21 After diagnosis, all included patients received initial treatment. Operations were categorized into five main forms: simple balloon dilation, stent implantation, catheter-directed thrombolysis, TIPS, and conservative treatment. Conservative treatment included anticoagulation alone, administered based on clinical evaluation. Anticoagulant options comprised warfarin, new oral anticoagulants (NOACs), or no anticoagulation in selected patients.
The following exclusion criteria were applied: (1) patients with a history of prior BCS treatment, including surgery, interventional therapy, or TIPS; (2) BCS-like manifestations secondary to cardiac disease, constrictive pericarditis, or portal vein thrombosis syndrome; (3) comorbid severe systemic illnesses such as renal failure, advanced heart disease, or malignancies (except hepatocellular carcinoma); (4) secondary BCS due to extrinsic compression from parasites, abscesses, tumors, or surgical injury; (5) failure of revascularization procedures owing to complete occlusion or chronic thrombosis; (6) incomplete or irregular anticoagulation therapy; (7) known allergy to iodine-based contrast agents; (8) pregnancy or lactation; (9) incomplete clinical data or unclear medical history; and (10) patients under 18 years of age.
Baseline Variables and Covariates
Baseline variables were collected from the hospital information system, including demographic characteristics (age and sex), clinical factors (type of BCS, presence of cirrhosis, history of surgery, and use of anticoagulation therapy), and laboratory indicators (white blood cell count, neutrophil count, lymphocyte count, monocyte count, platelet count, hemoglobin, red blood cell count, albumin, and total cholesterol).
Definitions of Systemic Inflammation Indices
Nine systemic inflammation indices were calculated from hematological and biochemical parameters measured at baseline, before any therapeutic intervention, in order to assess their association with post-treatment recurrence risk: neutrophil-to-lymphocyte ratio (NLR), derived neutrophil-to-lymphocyte ratio (dNLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), systemic immune-inflammation index (SII), systemic inflammation response index (SIRI), aggregate index of systemic inflammation (AISI), neutrophil-to-albumin ratio (NAR), and monocyte-to-albumin ratio (MAR). The formulas used for these indices were as follows:
NLR = Neutrophil counts/Lymphocyte counts
dNLR = Neutrophil counts/(White blood cell counts – Neutrophil counts)
PLR = Platelet counts/Lymphocyte counts
LMR = Lymphocyte counts/Monocyte counts
SII = Platelet counts × Neutrophil counts/Lymphocyte counts
SIRI = Neutrophil counts × Monocyte counts/Lymphocyte counts
AISI = Platelet counts × Neutrophil counts × Monocyte counts/Lymphocyte counts
NAR = Neutrophil counts/Serum albumin
MAR = Monocyte counts/Serum albumin
All indices were calculated using absolute cell counts (×109/L) and serum albumin level (g/L) obtained from laboratory test results at the time of diagnosis.
Outcome Definition and Follow-Up
The primary outcome was the first post-treatment recurrence of BCS. Recurrence was defined as a new thrombotic or obstructive event occurring after initial clinical and/or imaging improvement following treatment. It was determined based on both clinical symptoms and imaging findings, and met any of the following criteria: 1) significant restenosis or re-occlusion of the hepatic vein (HV), inferior vena cava (IVC), or their branches, with luminal narrowing exceeding 50% or complete occlusion; 2) new thrombus formation in the HV, IVC, or collateral veins, with evidence of partial or complete vascular blockage, reversed or absent blood flow; 3) reappearance of clinical manifestations suggestive of BCS after a stable period, including hepatic encephalopathy, ascites, lower extremity edema, abdominal wall varicosis, or gastrointestinal bleeding. All recurrence events occurred after initial therapeutic response. Patients who failed to respond to treatment or did not achieve clinical or imaging improvement were not classified as having recurrence.
All patients were regularly followed up every 3–6 months after diagnosis until July 31, 2022, or death. Follow-up was conducted through outpatient visits and telephone interviews. Recurrence events were confirmed by hospital records and imaging. Patients were categorized into recurrence and non-recurrence groups based on whether recurrence occurred before the end of follow-up.
Statistical Analysis
The distribution of continuous variables was evaluated using the Shapiro–Wilk test for normality. All nine inflammation-based indices were log-transformed to approximate normal distributions before analysis. Descriptive statistics were used to summarize baseline characteristics. Continuous variables were expressed as medians and interquartile ranges (IQRs), and categorical variables were presented as frequencies and percentages. Between-group differences (recurrence vs non-recurrence) were assessed using the Mann–Whitney U-test for continuous variables and the chi-square or Fisher’s exact test for categorical variables, as appropriate.
To assess the association between each inflammatory index and recurrence risk, both crude and adjusted logistic regression models were constructed. Adjusted models included potential confounders such as age, sex, and type. In addition, quartile-based logistic regression analyses were conducted to evaluate dose-response relationships. We employed a Weighted Quantile Sum (WQS) regression model to assess the joint effect of the nine inflammatory markers on recurrence risk. Following established practice in mixture epidemiology, we partitioned the data into training (40%) and validation (60%) sets, and conducted 1000 bootstrap iterations to derive stable component weights and index effect estimates.22 Subgroup analyses and interaction tests were performed for key variables, including age group (<50 vs ≥50), sex (male vs female), cirrhosis (yes vs no), and type (HV vs IVC vs MIX). Interaction terms were added to logistic regression models, and the significance of interactions was determined using likelihood ratio tests.
A two-sided P-value < 0.05 was considered statistically significant in all analyses. All statistical analyses were performed using R software (version 4.4.1).
Results
Baseline Characteristics
Among 708 BCS patients, 226 (31.9%) experienced post-treatment recurrence. Compared to those without recurrence, recurrent patients were younger [median age: 45.0 vs 52.0 years, P < 0.001] and more likely to be male (64.2% vs 54.8%, P = 0.023). Values of NLR, dNLR, SII, SIRI, AISI, and NAR were higher in patients with recurrence (all P < 0.01, Table 1), and LMR was lower (P = 0.019). PLR was comparable between groups (P = 0.174, Table 1).
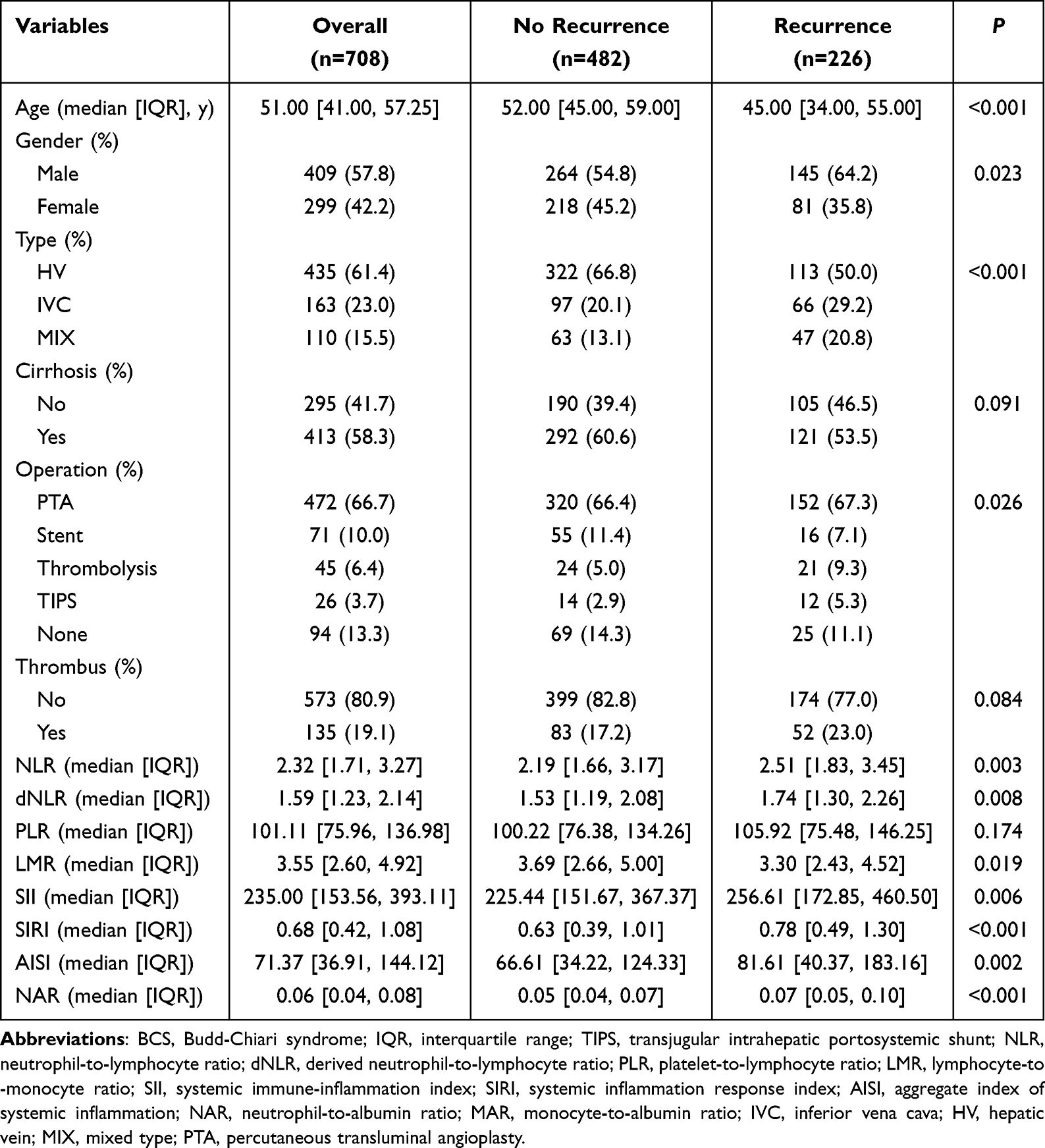 |
Table 1 Baseline Characteristics of BCS Patients with and without Recurrence |
Association Between Systemic Inflammation Indices and Recurrence
Unadjusted logistic regression models (Model 1) showed that elevated levels of NLR, dNLR, SII, SIRI, AISI, NAR, and MAR were associated with higher odds of recurrence. In comparison, higher LMR was associated with lower odds (OR = 0.70, 95% CI: 0.50–0.97, P = 0.033, Table 2). After adjusting for age, sex, BCS type, and cirrhosis in Model 2, associations for NLR, dNLR, PLR, SII, SIRI, and LMR persisted (all P < 0.05).
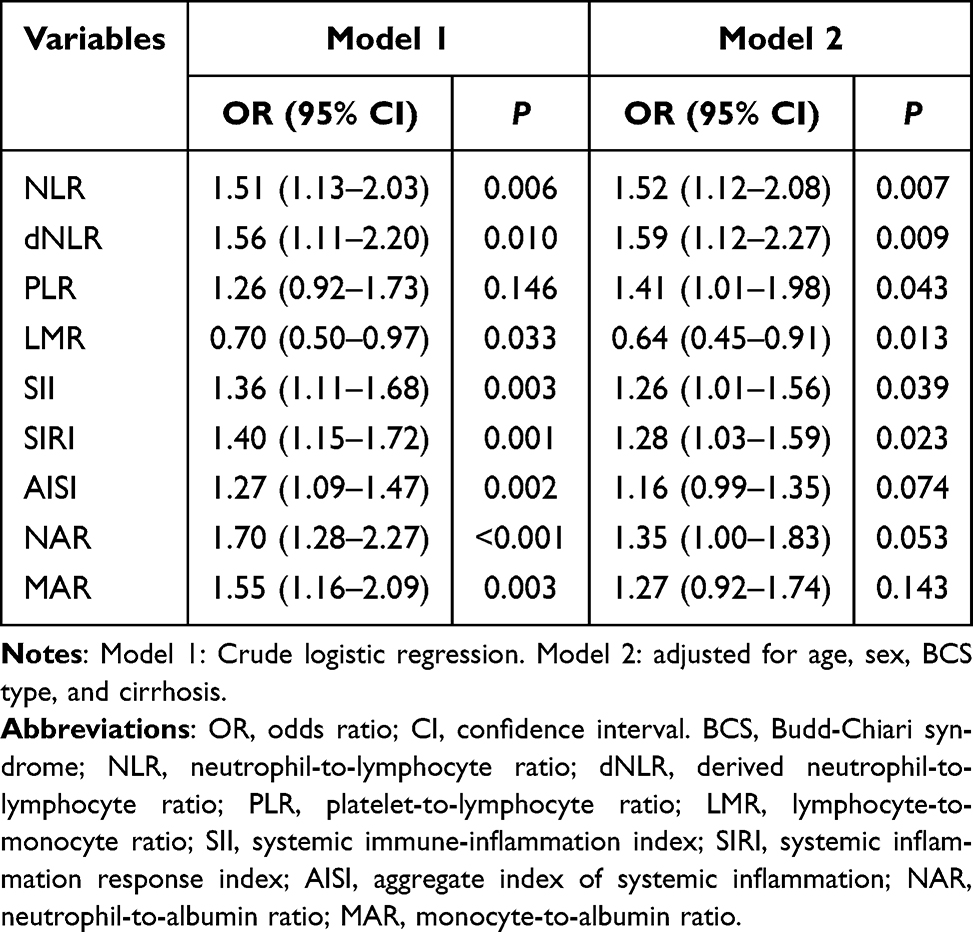 |
Table 2 Association Between Systemic Inflammation Indices and Recurrence in BCS Patients |
In the adjusted model (Model 2), NLR and dNLR showed consistent dose-response relationships with recurrence across quartiles (OR = 1.96, 95% CI: 1.24–3.12; and OR = 1.80, 95% CI: 1.14–2.85, respectively; both P for trend < 0.05, Table 3), while several other indices (including SII, PLR, and SIRI) were associated with increased recurrence risk in the highest quartile, though without clear linear trends.
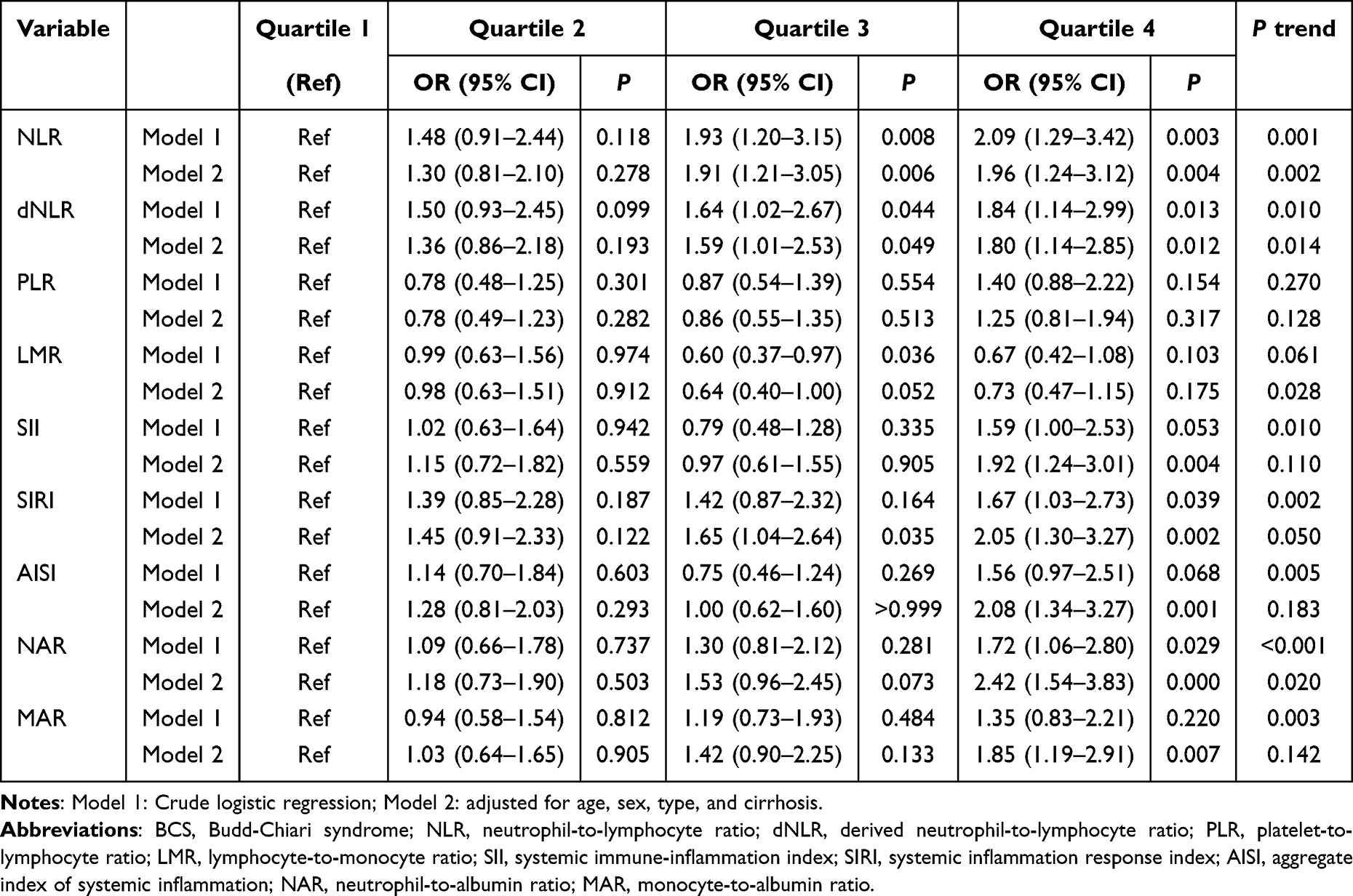 |
Table 3 Associations Between Systemic Inflammation Indices and Recurrence Across Quartiles in BCS Patients |
LMR was inversely associated with recurrence across quartiles. In the adjusted model, a decreasing trend in odds of recurrence was observed with higher LMR levels (P for trend = 0.028), although the pairwise comparisons did not reach conventional significance thresholds.
WQS Analysis of Inflammation Indices
The WQS regression model was used to assess the joint effect of multiple inflammation-related indices on recurrence risk. To ensure directionality consistency across pro-inflammatory markers, LMR was reverse-transformed (1/LMR) prior to inclusion in the WQS model. Among the nine indices included, NAR, MAR, and PLR contributed most to the WQS index, with estimated weights of approximately 0.42, 0.22, and 0.16, respectively (Figure 1).
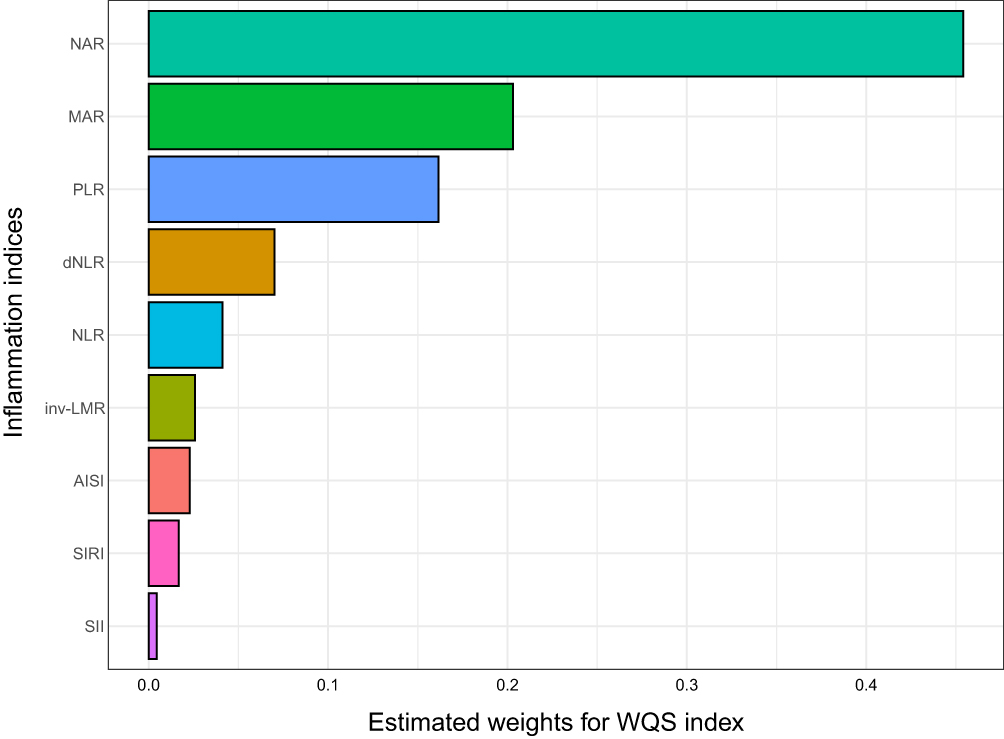 |
Figure 1 Estimated weights of systemic inflammation indices in the weighted quantile sum (WQS) model. Abbreviations: NLR, neutrophil-to-lymphocyte ratio; dNLR, derived neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; LMR, lymphocyte-to-monocyte ratio; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; AISI, aggregate index of systemic inflammation; NAR, neutrophil-to-albumin ratio; MAR, monocyte-to-albumin ratio. |
Subgroup and Interaction Analyses
Subgroup analyses across age, sex, BCS type, and cirrhosis revealed that the associations between inflammation indices and recurrence risk were generally consistent (Figure 2). However, significant interaction effects were observed for NAR (P = 0.031), dNLR (P = 0.048), PLR (P = 0.039), and SII (P = 0.033) by BCS type. In these cases, the estimated effects were more pronounced among patients with IVC-type BCS. In addition, the inverse association between LMR and recurrence appeared more prominent in patients with cirrhosis (OR = 1.86, 95% CI: 1.20–2.92), with a significant interaction by cirrhosis status (P = 0.023).
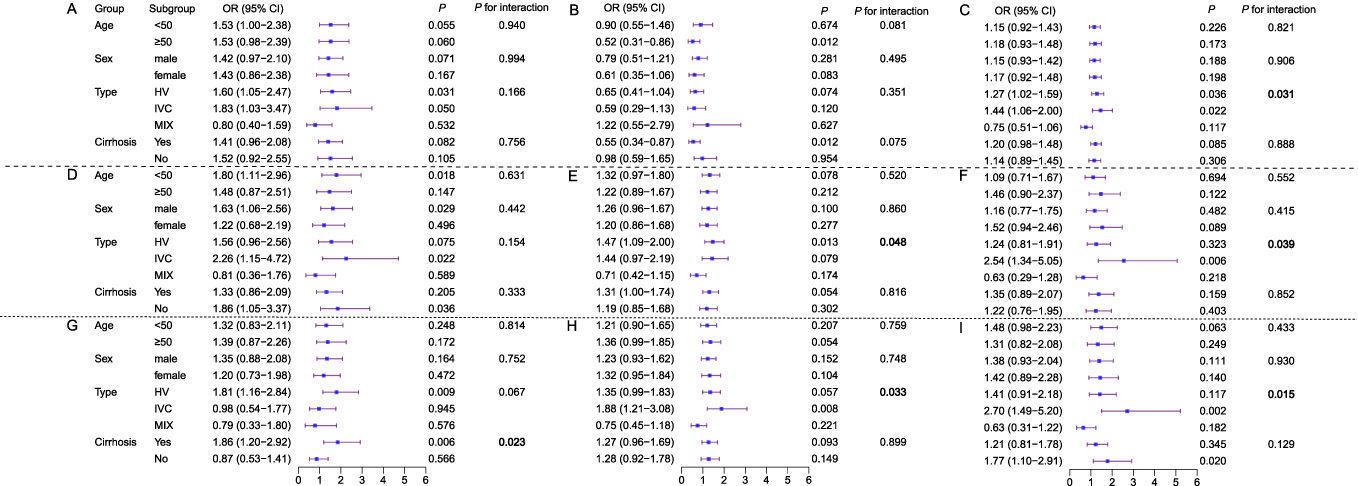 |
Figure 2 Subgroup and interaction analyses of systemic inflammation indices for predicting recurrence in patients with BCS; (A) AISI (Aggregate Index of Systemic Inflammation); (B) MAR (Monocyte-to-Albumin Ratio); (C) NAR (Neutrophil-to-Albumin Ratio); (D) NLR (Neutrophil-to-Lymphocyte Ratio); (E) dNLR (Derived Neutrophil-to-Lymphocyte Ratio); (F) PLR (Platelet-to-Lymphocyte Ratio); (G) LMR (Lymphocyte-to-Monocyte Ratio); (H) SII (Systemic Immune-Inflammation Index); (I) SIRI (Systemic Inflammation Response Index). Bolded P-values indicate statistically significant interaction (P < 0.05). |
Discussion
This study evaluated the association between systemic inflammation indices and recurrence in patients with primary BCS. Among the nine routinely available hematological and biochemical markers assessed, NLR, dNLR, SII, SIRI, and LMR consistently demonstrated independent associations with recurrence, while PLR retained significance after adjustment. Quartile-based analyses further revealed clear dose-response relationships for NLR and dNLR, whereas SII and SIRI were associated with increased recurrence risk only in the highest quartile. Subgroup and interaction analyses indicated that the effects of NAR, dNLR, PLR, and SII were more pronounced in patients with IVC-type BCS, and the inverse association of LMR was stronger in those with cirrhosis. In addition, the WQS model highlighted the joint contribution of NAR, MAR, and PLR, with NAR carrying the greatest weight. These findings suggest that easily obtainable indices could provide valuable information for assessing recurrence risk, offering a cost-effective and clinically accessible approach.
Among the evaluated indices, NLR and dNLR showed the most consistent associations with recurrence in both crude and adjusted models. Quartile-based analyses further demonstrated clear dose-response trends, supporting the robustness of these findings. Elevated NLR/dNLR reflects a state of heightened systemic inflammation and impaired immune regulation, as indicated by neutrophil predominance and relative lymphocyte depletion.23 Previous studies have demonstrated that neutrophil activation and the release of neutrophil extracellular traps (NETs) play a critical role in promoting thrombosis and endothelial injury, thereby contributing to the development and recurrence of venous thrombosis.24,25 Given that BCS is characterized by venous obstruction as its central pathological feature,26 recurrence is likely driven not only by mechanical re-stenosis but also by a persistent proinflammatory and prothrombotic state. The elevation of NLR and dNLR, which reflects an imbalance between inflammation and immune regulation, may exacerbate recurrence risk through several mechanisms. First, neutrophil-mediated inflammatory activation enhances coagulation factor activity, fostering a hypercoagulable state.27 Second, lymphocyte depletion may impair immune regulatory mechanisms and anti-inflammatory responses, thereby limiting the resolution of inflammation.28,29 Third, sustained endothelial injury and secondary fibrogenesis may contribute to a vascular wall microenvironment favoring recurrent occlusion.30,31 Excessive or inadequately cleared NETs can persistently damage endothelial cell junctions, activate procoagulant pathways, and disrupt vascular homeostasis, promoting a cycle of endothelial dysfunction and thrombosis.32
Among the evaluated indices, LMR was the only marker negatively associated with recurrence risk in both adjusted models and quartile-based analyses. A higher LMR reflects a relative abundance of lymphocytes and a lower proportion of monocytes, indicating a more balanced immune state and reduced chronic inflammation.33,34 Lymphocytes are critical for maintaining adaptive immune surveillance and anti-inflammatory responses, while monocytes contribute to chronic inflammation, fibrosis, and endothelial dysfunction. The protective association of LMR was especially pronounced in patients with cirrhosis, where monocyte-driven inflammation is known to exacerbate hepatic fibrogenesis and vascular injury.35 This finding aligns with previous studies in chronic liver disease and hepatocellular carcinoma, where lower LMR has been associated with poor prognosis, greater inflammatory burden, and impaired immune regulation.33,34
In this study, SII and SIRI were positively associated with recurrence risk when treated as continuous variables in adjusted logistic regression models, consistent with prior evidence linking these indices to poor prognosis in hepatocellular carcinoma and other gastrointestinal malignancies.36 However, the quartile-based analyses revealed that these associations were mainly driven by elevated risk in the highest quartile, while intermediate quartiles did not show consistent significance. Furthermore, dose-response trends across quartiles were not statistically robust for SII, and only marginal for SIRI, suggesting a possible threshold effect rather than a linear increase in risk. These findings imply that the proinflammatory burden may need to exceed a certain threshold before it meaningfully influences recurrence risk. These indices reflect the balance between proinflammatory activity and immune regulation. SII integrates the effects of thrombosis-related cellular components, innate immune activation, and suppression of adaptive immunity. SIRI further incorporates monocyte-mediated chronic inflammation and fibrogenic processes, which are known contributors to vascular injury. Notably, both SII and PLR showed stronger associations with recurrence among patients with IVC-type BCS, as evidenced by significant interaction terms. This may reflect greater sensitivity of the IVC subtype to systemic inflammatory states, potentially due to more extensive vascular involvement or underlying prothrombotic predisposition.
In our cohort, younger age was associated with a higher recurrence frequency after treatment for BCS. This finding is consistent with our previous study based on the same cohort, which also identified age as a significant factor influencing recurrence risk.19 Although the mechanisms are not fully understood, possible explanations include a higher prevalence of underlying prothrombotic conditions, longer follow-up duration, and differences in treatment strategies. Further studies are warranted to clarify this association.
This study has several strengths. First, it was conducted using a relatively large, well-characterized cohort of patients with primary BCS, allowing for a meaningful evaluation of recurrence risk in this rare vascular disorder. Second, we comprehensively assessed nine systemic inflammation indices, incorporating neutrophil-, lymphocyte-, monocyte-, platelet-, and albumin-based markers, to capture different facets of the systemic inflammatory response. Third, the consistency of the findings was supported through multiple analytic strategies, including logistic regression, quartile-based trend analyses, weighted quantile sum regression, and subgroup and interaction analyses. Finally, all evaluated indices were derived from routine laboratory parameters, which enhances the clinical feasibility and reproducibility of these findings. However, several limitations should be noted. First, given the rarity of BCS, this study adopted a single-center retrospective design. While this may limit generalizability to some extent, it nevertheless provides valuable clinical insights under realistic constraints. Second, inflammatory indices were assessed only at baseline, which precludes an understanding of their temporal dynamics or changes in response to treatment.
In conclusion, this study found that several systemic inflammation indices were independently associated with the risk of recurrence in patients with BCS. As readily accessible markers derived from routine laboratory tests, these indices may aid in the preliminary assessment of recurrence risk and offer insights into the inflammatory mechanisms underlying disease progression. Further prospective validation and mechanistic studies are needed to support clinical translation and improve patient management.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (XYFY2023-KL188-01) and was conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent.
Author Contributions
Ziyuan Shen and Man Ni - Conceptualization, Writing original draft. Yang Liu and Huijie Zhang - Data curation. Ziyuan Shen and Xing Xing - Methodology, Formal analysis. Qingqiao Zhang, Maoheng Zu, Yan Li, Xing Xing, and Shengli Li - Validation, Writing - revise & editing. All authors have drafted or written, or substantially revised or critically reviewed the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Ziyuan Shen and Man Ni are joint first authors.
Funding
This work was supported by grants from the Construction Project of High-Level Hospitals of Jiangsu Province (GSPJS202411, GSPJS202509, GSPJS202511, GSPSJ20240805), the Medical Technology Innovation Project of Xuzhou Municipal Health Commission (XWKYHT20230072), and the Advanced Program of The Affiliated Hospital of Xuzhou Medical University (PYJH2025203).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Menon KVN, Shah V, Kamath PS. The Budd–Chiari Syndrome. N Engl J Med. 2004;350(6):578–11. doi:10.1056/NEJMra020282
2. Ferral H, Behrens G, Lopera J. Budd-Chiari Syndrome. Am J Roentgenol. 2012;199(4):737–745. doi:10.2214/AJR.12.9098
3. Li Y, De Stefano V, Li H, et al. Epidemiology of Budd-Chiari syndrome: a systematic review and meta-analysis. Clin Res Hepatol Gastroenterol. 2019;43(4):468–474. doi:10.1016/j.clinre.2018.10.014
4. European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Vascular diseases of the liver. J Hepatol. 2016;64(1):179–202. doi:10.1016/j.jhep.2015.07.040
5. Mancuso A. Budd-Chiari syndrome management: lights and shadows. World J Hepatol. 2011;3(10):262–264. doi:10.4254/wjh.v3.i10.262
6. Horton JD, San Miguel FL, Ortiz JA. Budd–Chiari syndrome: illustrated review of current management. Liver Int. 2008;28(4):455–466. doi:10.1111/j.1478-3231.2008.01684.x
7. Srinivasan P, Rela M, Prachalias A, et al. Liver transplantation for Budd-Chiari syndrome. Transplantation. 2002;73(6):973–977. doi:10.1097/00007890-200203270-00026
8. Inchingolo R, Posa A, Mariappan M, et al. Transjugular intrahepatic portosystemic shunt for Budd-Chiari syndrome: a comprehensive review. World J Gastroenterol. 2020;26(34):5060–5073. doi:10.3748/wjg.v26.i34.5060
9. Li WD, Yu H-Y, Qian A-M, et al. Risk factors for and causes and treatment of recurrence of inferior vena cava type of Budd-Chiari syndrome after stenting in China: a retrospective analysis of a large cohort. Eur Radiol. 2017;27(3):1227–1237. doi:10.1007/s00330-016-4482-4
10. Wang Z, Wang Z, Zhang Z, et al. Establishment and validation of a prediction model for the first recurrence of Budd–Chiari syndrome after endovascular treatment: a large sample size, single-center retrospective study. Hepatol Internat. 2023;17(1):159–169. doi:10.1007/s12072-022-10464-y
11. Stark K, Massberg S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat Rev Cardiol. 2021;18(9):666–682. doi:10.1038/s41569-021-00552-1
12. Lisman T, Luyendyk JP. Systemic inflammation and disorders of hemostasis in the AD-ACLF syndrome. J Hepatol. 2021;74(5):1264–1265. doi:10.1016/j.jhep.2020.12.017
13. Nesci A, Ruggieri V, Manilla V, et al. Endothelial dysfunction and liver cirrhosis: unraveling of a complex relationship. Int J Mol Sci. 2024;25(23):12859. doi:10.3390/ijms252312859
14. Rice J, Dodge JL, Bambha KM, et al. Neutrophil-to-lymphocyte ratio associates independently with mortality in hospitalized patients with cirrhosis. Clin Gastroenterol Hepatol. 2018;16(11):1786–1791.e1. doi:10.1016/j.cgh.2018.04.045
15. Nie GL, Yan J, Li Y, et al. Predictive model for non-malignant portal vein thrombosis associated with cirrhosis based on inflammatory biomarkers. World J Gastrointest Oncol. 2024;16(4):1213–1226. doi:10.4251/wjgo.v16.i4.1213
16. Zhang Q, Xu Z, Long L, et al. Predictive value of neutrophil-to-lymphocyte ratio for long-term adverse outcomes in cirrhosis patients post-transjugular intrahepatic portosystemic shunt. Sci Rep. 2025;15(1):797. doi:10.1038/s41598-024-84630-7
17. Zhang L, Fang Y, Xing J, et al. The efficacy of the systemic immune-inflammation index and prognosis nutritional index for the diagnosis of venous thromboembolism in gastrointestinal cancers. J Inflamm Res. 2022;15:4649–4661. doi:10.2147/JIR.S376601
18. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
19. Li S, Liu X, Zhou M, et al. Analysis of risk factors for recurrence of Budd-Chiari syndrome: a retrospective study with zero-inflated model. Medicine. 2025;104(47):e45511. doi:10.1097/MD.0000000000045511
20. Xue W, Xu B, Wang H, et al. Development and validation of a machine learning model based on multiple kernel for predicting the recurrence risk of Budd-Chiari syndrome. Front Physiol. 2025;16:1589469. doi:10.3389/fphys.2025.1589469
21. Shukla A, Shreshtha A, Mukund A, et al. Budd-Chiari syndrome: consensus guidance of the Asian Pacific Association for the study of the liver (APASL). Hepatol Int. 2021;15(3):531–567. doi:10.1007/s12072-021-10189-4
22. Renzetti S, Gennings C, Calza S. A weighted quantile sum regression with penalized weights and two indices. Front Public Health. 2023;11:1151821. doi:10.3389/fpubh.2023.1151821
23. Colling ME, Tourdot BE, Kanthi Y. Inflammation, infection and venous thromboembolism. Circ Res. 2021;128(12):2017–2036. doi:10.1161/CIRCRESAHA.121.318225
24. Yao M, Ma J, Wu D, et al. Neutrophil extracellular traps mediate deep vein thrombosis: from mechanism to therapy. Front Immunol. 2023;14:1198952. doi:10.3389/fimmu.2023.1198952
25. Li W, Wang Z, Su C, et al. The effect of neutrophil extracellular traps in venous thrombosis. Thromb J. 2023;21(1):67. doi:10.1186/s12959-023-00512-4
26. Giri S, Angadi S, Varghese J, et al. Prothrombotic states in portal vein thrombosis and Budd-Chiari syndrome in India: a systematic review and meta-analysis. Indian J Gastroenterol. 2023;42(5):629–641. doi:10.1007/s12664-023-01400-5
27. Potere N, Abbate A, Kanthi Y, et al. Inflammasome signaling, thromboinflammation, and venous thromboembolism. JACC. 2023;8(9):1245–1261. doi:10.1016/j.jacbts.2023.03.017
28. Sheu -T-T, Chiang B-L, Lymphopenia. Lymphopenia-induced proliferation, and autoimmunity. Int J Mol Sci. 2021;22(8):4152. doi:10.3390/ijms22084152
29. Zhang H, Gao J, Tang Y, et al. Inflammasomes cross-talk with lymphocytes to connect the innate and adaptive immune response. J Adv Res. 2023;54:181–193. doi:10.1016/j.jare.2023.01.012
30. Abrashev H, Abrasheva D, Nikolov N, et al. A systematic review of endothelial dysfunction in chronic venous disease—inflammation, oxidative stress, and shear stress. Int J Mol Sci. 2025;26(8):3660. doi:10.3390/ijms26083660
31. Romano E, Rosa I, Fioretto BS, et al. The contribution of endothelial cells to tissue fibrosis. Curr Opin Rheumatol. 2024;36(1):52–60. doi:10.1097/BOR.0000000000000963
32. Qi H, Yang S, Zhang L. Neutrophil extracellular traps and endothelial dysfunction in atherosclerosis and thrombosis. Front Immunol. 2017;8:928. doi:10.3389/fimmu.2017.00928
33. Mano Y, Yoshizumi T, Yugawa K, et al. Lymphocyte-to-monocyte ratio is a predictor of survival after liver transplantation for hepatocellular carcinoma. Liver Transpl. 2018;24(11):1603–1611. doi:10.1002/lt.25204
34. Ha Y, Mohamed Ali MA, Petersen MM, et al. Lymphocyte to monocyte ratio-based nomogram for predicting outcomes of hepatocellular carcinoma treated with sorafenib. Hepatol Int. 2020;14(5):776–787. doi:10.1007/s12072-020-10076-4
35. Krenkel O, Tacke F. Liver macrophages in tissue homeostasis and disease. Nat Rev Immunol. 2017;17(5):306–321. doi:10.1038/nri.2017.11
36. Hu B, Yang X-R, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.