Back to Journals » Risk Management and Healthcare Policy » Volume 16
Association Between Sunlight Exposure and Mental Health: Evidence from a Special Population Without Sunlight in Work
Authors Wang J, Wei Z, Yao N, Li C, Sun L ![]()
Received 17 May 2023
Accepted for publication 10 June 2023
Published 14 June 2023 Volume 2023:16 Pages 1049—1057
DOI https://doi.org/10.2147/RMHP.S420018
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Jie Wang,1,2 Zhen Wei,1,2 Nan Yao,1,2 Caifeng Li,1,2 Long Sun1,2
1Centre for Health Management and Policy Research, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 2NHC Key Laboratory of Health Economics and Policy Research, Shandong University, Jinan, People’s Republic of China
Correspondence: Long Sun, Centre for Health Management and Policy Research, School of Public Health, Cheeloo College of Medicine, Shandong University, 44 Wenhuaxi Road, Jinan, Shandong, 250012, People’s Republic of China, Tel +86 531-88382678, Email [email protected]
Purpose: In recent years, mental health problems have become the most serious social problems worldwide. Past studies have proposed that some links exist between sunlight and mental health; however, relevant studies examining low-dose sunlight exposure populations are lacking. We conducted a study among a group of operating room nurses (ORNs) who work long hours in operating rooms and have limited sunlight exposure. We aim to add to and refine previous researches on the association between mental health and sunlight exposure in community population.
Patients and Methods: A total of 787 ORNs were interviewed and analyzed. Mental health, sunlight exposure duration, sociodemographic and work-related variables, and chronic diseases were evaluated. The Kessler 10 scale (K10) was used to assess participants’ mental health status, and their sunlight exposure duration was assessed using their self-reports. Multiple linear regression analysis was adopted to examine the association between sunlight exposure and mental health.
Results: The average K10 score of ORNs was 25.41. ORNs exhibit poorer mental health than other populations. Poor mental health was negatively associated with greater sunlight exposure hours per day (β=− 0.378) and sleep regularity (β=− 3.341). Poor mental health was positively associated with chronic disease (β=3.514).
Conclusion: This study indicated that the positive association between sunlight exposure and mental health existed. Appropriate enhancement of sunlight exposure will be beneficial to mental health. Hospitals, related organizations and individuals should pay greater attention to ORNs’ mental health and sunlight exposure conditions. More policy recommendations as well as building structure recommendations should be proposed.
Keywords: sunlight exposure, mental health, operating room nurses, China
Introduction
The World Health Organization (WHO) reinforces that there is no health without mental health.1 Globally, nearly one billion people suffering from mental health problems.2 Worryingly, the number of mental disorder cases increased by 48.1% from 1990 to 2019.3 Depression and anxiety cases have increased by 25% from 2019 to 2022.4 In addition, mental disorders was a leading cause of disability and can precipitate many negative outcomes, including distress, family breakdown, deterioration of chronic diseases and even suicide.5–10
Humans may not survive healthily without sunlight. Along with facilitating sterilization and energy supply, sunlight provided protection against a wide range of diseases—not only physical diseases but also mental disorders.11 This had been supported by a number of studies conducted in people with mental disorders. A study demonstrated that long-term exposure to moderate levels of ultraviolet B can inhibit the development of depression in Taiwan, China.12 Besides, light therapy is effective in treating seasonal affective disorder as well as non-seasonal depression.13,14 Another study also found that mental illnesses patients living in rooms with better sunlight tend to have shorter hospital stays.15 More sunlight exposure was beneficial, the lack of it was detrimental. The association between sunlight and schizophrenia was also been proposed, it was that lack of sunlight exposure may increase the risk of hospital admission for people with schizophrenia.16 In addition, some ecological studies using regional sunlight data put forward similar arguments. It was reported that people living in areas with longer and higher sunlight exposure levels exhibit fewer depressive symptoms17 and were less likely to report suicidal thought18 Additionally, seasonal increases in sunlight duration are associated with decreases in mental health distress.19 Sunlight was also found to play a moderating role in the relationship between PM2.5 and depression.20
All these studies presented links between sunlight exposure and mental disorders. However, some inadequacies should be considered to get the conclusion about the associations between sunlight exposure and mental health.
Firstly, previous studies have focused on patients with mental disorders, such as depression,12 schizophrenia16 and have lacked exploration of the general community population. Secondly, many of these previous studies were ecological studies of the population and presented sunlight through objective meteorological data,12,17,21,22 such as daytime sunshine hours and ultraviolet (UV) index. This neglected the characteristics of sunlight; regional sunlight data do not represent an individuals’ actual receiving sunlight; rather, it is closely related to their living environment and habits. Hence, self-reported data are, indubitably, a preferable alternative. Thirdly, a study on submarine personnel23 said that artificial light can also reduce depression levels. Almost all the past studies ignored the effect of artificial light, thus, eliminating the interference caused by different artificial light sources was needed in further study.
Actually, there were also some studies did not support the positive associations between sunlight exposure and mental health. For example, in a study of 13,938 Spanish university graduates, it reported that people living in areas with longer daylight hours had higher risk of depression.24 Besides, in the Cooper Center Longitudinal Study from 2013 to 2019, tanning-bed use which brought longer exposure to the sun increased unhealthy psychological symptoms.25 In addition to suggesting an inverse correlation, some studies also suggested that the relationship between the sunlight exposure and mental health cannot be proven clearly. Sunlight exposure and other meteorological factors were not associated with depressive symptoms in two community populations studies.26 Similarly, a study in Finnish adults found the average amount of sunshine in a year was also not related to the total number of depressive symptoms.18 The different findings reminded us further research is required to explore the association between sunlight exposure and mental health and new evidence in this regard would be highly meaningful.
To enrich evidences about the associations between sunlight exposure and mental health, operating room nurses (ORNs) were interviewed in this study. There were several reasons to select ORNs to explore the association. Firstly, ORNs was a very special population without sunlight exposure in work because no windows exist in operating rooms. For most of the time, they were exposed to artificial light that met the lighting requirements of the operating room. These artificial lights had a similar intensity, therefore, the study of the ORNs facilitated the exclusion of part of artificial light’s interference and focused more on the effect sunlight. Secondly, ORNs worked in operating rooms for long time per day, even longer than surgeons; thus, focusing on their mental health status is necessary. Simultaneously, their working hours are predominantly during the day, thus their sunlight exposure out of work would be also short. Fewer previous studies had been conducted on populations who are continuously exposed to low levels of sunlight. Our study would add evidence to the lack. Thirdly, compared to the submarine workers23 who also worked without exposure to sunlight, ORNs had normal social interaction and work characteristics, so ORNs were more representative. These characteristics made them become suitable candidates for studying the association between sunlight exposure and mental health.
To address the gaps in previous research, we conducted this study on ORNs in Shandong Province, China. We aimed to demonstrate the association between sunlight exposure and mental health. This study can contribute evidence to deeply explore the association mechanism prevalent in the real world and provide novel ideas for treating mental disorders.
Materials and Methods
Participants and Data Collection
This cross-sectional study was conducted in Shandong Province, China. Shandong Province is located on the eastern coast of China, between 34°-38°north latitude and 114°-122°east longitude, and belongs to the mid-latitude region. All participants were ORNs from several general hospitals, selected between December 2021 and January 2022. A convenience sampling method was used; we completed the following steps: Firstly, we assessed the online questionnaires carefully and delivered them to nursing supervisors. Secondly, they forwarded the questionnaires to ORNs through WeChat groups, and the nurses filled these voluntarily. Finally, 787 eligible questionnaires were collected; the average response time for each questionnaire was approximately 29 minutes.
Measures
Mental Health
Mental health was measured using the Chinese version of the Kessler 10 (K10) scale.27 This scale has been demonstrated to exhibit great reliability and validity in the Chinese population.28,29 It is a 10 items self-report scale rated on a five-point Likert scale, ranging from “barely = 1” to “all the time= 5”. The final score is the sum of all item scores, with higher scores reflecting a worse mental health status. Prior studies have used the K10 scale to estimate mental health and psychological distress,30 and to screen for depression and anxiety.31–33
Sunlight Exposure Hours/Day
Sunlight exposure hours were evaluated using the question, “In the last three months, how many hours have you been exposed to sunlight each weekday?” The number of hours was responded to by ORNs. Herein, self-reported hours were analyzed as continuous variables.
Social-Demographic Variables
The main socio-demographic variables were gender, age, height, weight, marital status, religious beliefs, and academic degree. Gender was coded as men (1) or women (0). Height and weight were calculated as body mass index (BMI) and were analyzed as continuous variables. The response alternatives to the questions regarding marital status were single, married, divorced, widowed, and others. Considering the small proportion of the latter three answers, single was recorded as never married (1), and married, divorced, widowed, and others were combined as ever married (2). Similarly, religious beliefs were coded as yes (1) or no (0). Academic degree was asked using one question regarding the highest degree, and the responses alternatives were doctors, master, bachelor, junior college, technical secondary school, and others. As most ORNs obtained a bachelor’s degree, we recorded it as a bachelor’s degree or above (1) and lower than a bachelor’s degree (2).
Work-Related Variables
The work-related variables analyzed in this study included professional title, appointed way, working years in the department and operating room, working days per week, income per month, and job familiarity. Professional titles were coded as intermediate and above (1), and junior and below (2). The appointment method was recorded as an official in preparation (1) and another way (2). Working years in department and operating room were evaluated using the following questions: “How many years have you worked in this unit?” and “How many years have you been engaged in this major in this unit?” Additionally, ORNs’ monthly income was also asked and categorized into less than 5000 (1), 5001–10,000 (2), 10,001–15,000 (3), greater than 15,000 (4). Job familiarity was coded as extremely familiar (1), familiar (2) and general, or below (3).
Chronic Disease
Chronic disease status was collected using ORNs’ self-report, and the question used was, “Do you suffer any chronic diseases?” The answers were binary variables coded as yes (1) or no (0).
Statistical Methods
IBM SPSS Statistics 24.0 (web version) was used to analyze the data. Continuous variables are means and standard deviations and categorical variables are numbers and percentages. t-tests or one-way analysis of variance (ANOVA) were used to assess the mean differences for variables across mental health. Multiple linear regression analysis was performed to examine the relationship between these variables and mental health. All significance tests were two-tailed, and a p-value of <0.05 was considered statistically significant.
Results
Sample Characteristics and Single Analysis for the Factors Associated with Mental Health Among the ORNs in Shandong, China
In this study, we interviewed 787 ORNs in Shandong Province, China. The sample characteristics and single-factor analyses are presented in Table 1. The percentage of women was higher than that of men (80.6% vs 19.4%). The sample population’s mean age was 33.87 (SD=7.07) and the mean BMI was 22.86 (SD=4.22). Overall, 159 participants (20.2%) reported that they were unmarried, and 634 (79.8%) were ever married. Most participants had a bachelor’s degree or above and had no religious beliefs, with percentages of 93.6% and 97.3%, respectively. The mean K10 score of all sample ORNs populations was 25.41 (SD=8.52). The results revealed that sleep regularity (t=−6.189, p<0.001), chronic disease (t=5.383, p<0.001), and sunlight exposure hours per day (r=−0.078, p=0.028) were associated with mental health. Table 1 provides the detailed information.
 |
Table 1 Sample Characteristics and Single Analysis for the Factors Associated with Mental Health Among the Operating Room Nurses |
Multiple Linear Regression Analysis for the Association Between Sunlight Exposure Hours/Day and Mental Health
A multiple linear regression model was used to analyze the factors associated with mental health (Table 2). After controlling for work-related variables, the results revealed that poor mental health was negatively associated with more sunlight exposure hours per day (β=−0.378, p=0.046). Further, we found that poor mental health was positively associated with chronic disease (β=3.514, p<0.001) and negatively related to sleep regularity (β=−3.341, p<0.001). The multiple linear regression model that we constructed was effective (adjusted R2=0.080, p<0.001).
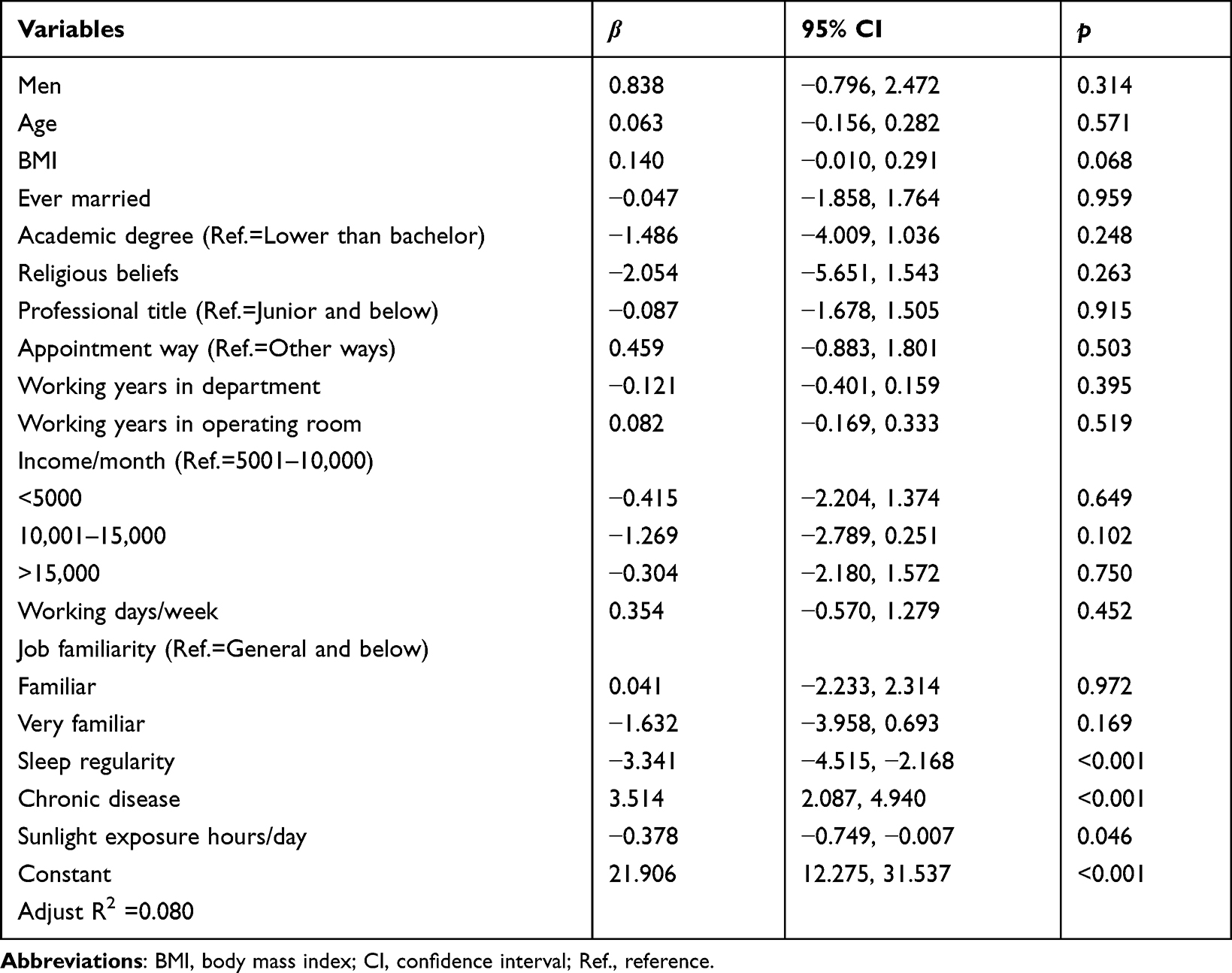 |
Table 2 Multiple Linear Regression Analysis for the Association Between Sunlight Exposure and Mental Health |
Discussion
We surveyed ORNs and obtained the following critical findings. First, the mean K10 score of ORNs was 25.41(>25), suggesting that they had a relatively high level of psychological distress.29 Second, we found that sleep regularity, chronic diseases, and sunlight exposure time were associated with mental health. Third, sunlight exposure time still exhibited a positive correlation with mental health after adjusting for the multiple linear regression model; that is, as the sunlight exposure time increased, the mental health status improved.
Results regarding ORNs’ mental health status were not optimistic. Of the 787 study subjects, 314 (39.9%) exhibited a score greater than or equal to 30 on the K10 scale—the fourth level of the scale’s evaluation,29 indicating a poor psychological condition and a high risk of developing psychological disorders. The mean score was 25.41, which was significantly higher than that of the general population.34
Suffering from chronic diseases is associated with a higher risk of developing mental disorders. This finding is consistent with the results of previous studies. Patients with chronic diseases are more likely to be depressed and anxious than other people.35 Physical pain increases patients’ psychological stress; therefore, depressive symptoms increase with the diagnosis of chronic illness.36
High sleep regularity was associated with great mental health. This is consistent with the results of previous studies and popular perception. Sleep regularity is defined as the degree to which an individual exhibits a consistent sleep duration across days.37 High sleep regularity helps keep the body and mind in great condition, and poor sleep regularity is associated with mental illness.38 For example, insomnia symptoms’ severity is related to the severity of symptoms of depression and anxiety.39
As the duration of sunlight exposure increased, survey respondents’ mental health status improved. This discovery is enlightening for this low-dose sunlight exposure population; thus, exploring this improvement in mental health status is essential. From a physiological perspective, several explanations exist, the first of which is the role of vitamin D. Multiple cross-sectional studies,40,41 longitudinal studies,42 and meta-analyses43,44 have demonstrated that vitamin D deficiency is associated with an increased risk of depression, and vitamin D supplementation may be beneficial in treating patients with depression.45 Sunlight exposure has been—and will continue—being the primary source of vitamin D for most people.46,47 Thus, sunlight may affect mental health by affecting vitamin D levels in the body. It is also worth noting that our study was conducted in December to January, three months prior to which the solar UV intensity was at a low level and the UV levels would not be sufficient to meet the body’s needs.48 Then the sunlight exposure duration of our study became particularly important in the production of vitamin D. Second, serum cortisol levels are significantly positively correlated with mental health scale scores,49 and light is the primary medium regulating the body’s circadian cortisol rhythm.50 Third, decreased sunlight exposure is usually accompanied by a decrease in physical activity,51 which can cause neuroplasticity, inflammation, oxidative stress, and changes in the endocrine system.52 These are closely related to the occurrence of mental disorders; thus, the association between sunlight and mental health has been established. This is a complex process, and more researches are needed to further demonstrate this process using more suitable approaches, such as personal monitoring.
Our study had some limitations. First, this was a cross-sectional study and the causal association between mental health and sunlight could not be verified. Whether increased sunlight exposure leads to improved mental health, or good mental health seeks more sunlight, or a combination of the two cannot be verified and requires further research. Second, sunlight exposure was measured using self-reported daily sunlight exposure duration, which fully considered individual characteristics; however, inevitably, recall bias may affect the results’ accuracy. Third, this study’s participants were all ORNs from Shandong; thus, they may not be representative of other regions. Finally, we cannot rule out the presence of other contributing factors, such as diet, medication, more work-related variables, though we adjusted for some confounding factors.
Despite these limitations, this study may help explore the association between sunlight exposure and mental health. This is consistent with the view held in most previous studies that mental health status improves with increased sunlight exposure time. This is a new study of low-level sunlight exposure population of great importance. Indubitably, further studies are needed to explore the causal inference, action mechanism, and most suitable duration and intensity between sunlight exposure and mental health. Additionally, the differences in various mental disorders should be considered.
Implications
Mental disorders are usually underdiagnosed and untreated owing to stigma, the lack of effective treatments and inadequate mental health services.53 Simultaneously, in the treatment of mental disorders, more than half of people stop taking their medication within 60 days of starting treatment.54 Therefore, exploring an easy, convenient, and accessible way to improve mental health and relieving symptoms of mental disorders is particularly important.
Our research supports the role of sunlight in improving mental health; therefore, indubitably, our research will help provide an available method for the prevention and treatment of mental disorders, and also provide advice on the construction of space structures in various workplaces, such as hospitals. For example, increasing the number of windows in the ward to improve sunlight status or adopting outdoor rehabilitation measures. In the future, we need to conduct further research along this direction and collaborate with more researchers to contribute to the mental health problems that plague people worldwide.
Conclusion
ORNs exhibit poorer mental health than other populations, and those with chronic illnesses, as well as irregular sleep, have poorer mental health. In the low-level sunlight exposure group, nurses’ mental health was better with longer sunlight exposure time. Therefore, more attention should be paid to the mental health of ORNs and strategies or policies should be adopted to protect the mental health of ORNs, and nurses themselves should pay attention to regular work and rest and obtain greater sunlight exposure.
Abbreviations
ORNs, Operating room nurses; K10, The Kessler 10 Scale; WHO, World Health Organization; UV, Ultraviolet; BMI, body mass index; SD, Standard deviation; CI, Confidence interval; Ref., Reference.
Ethics Approval and Consent to Participate
The study was approved by the institutional review board of Shandong University School of Public Health (LL20210101). Informed consent was obtained from all participants of the study. The guidelines outlined in the Declaration of Helsinki were followed of this study.
Acknowledgments
We would like to thank all the subjects for their participation in this study.
Funding
This research was supported by the National Social Science Foundation of China (71974114). The funding sources had no involvement in study design; in the collection, analysis and interpretation of data; in the writing of the article; and in the decision to submit the article for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO director-general launches mental health action plan; 2018. Available from: https://www.who.int/director-general/speeches/detail/who-director-general-launches-mental-health-action-plan.
2. The Lancet Global Health. Mental health matters. Lancet Glob Health. 2020;8(11):e1352. doi:10.1016/S2214-109X(20)30432-0
3. GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3
4. World Health Organization. WISH summit calls for sustainable mega sports event legacies which boost physical activity; 2022. Available from: https://www.who.int/news/item/06-10-2022-wish-summit-calls-for-sustainable-mega-sports-event-legacies-which-boost-physical-activity.
5. Dalle Grave R. Nutrition and fitness: mental Health. Nutrients. 2020;12(6):1804. doi:10.3390/nu12061804
6. Li Z, Li Y, Chen L, Chen P, Hu Y. Prevalence of depression in patients with hypertension: a systematic review and meta-analysis. Medicine. 2015;94(31):e1317. doi:10.1097/MD.0000000000001317
7. Liu BP, Qin P, Liu YY, Yuan L, Gu LX, Jia CX. Mental disorders and suicide attempt in rural China. Psychiatry Res. 2018;261:190–196. doi:10.1016/j.psychres.2017.12.087
8. Richmond-Rakerd LS, D’Souza S, Milne BJ, Caspi A, Moffitt TE. Longitudinal associations of mental disorders with physical diseases and mortality among 2.3 million New Zealand Citizens. JAMA Netw Open. 2021;4(1):e2033448. doi:10.1001/jamanetworkopen.2020.33448
9. Schulz R, Drayer RA, Rollman BL. Depression as a risk factor for non-suicide mortality in the elderly. Biol Psychiatry. 2002;52(3):205–225. doi:10.1016/s0006-3223(02)01423-3
10. Walker ER, McGee RE, Druss BG. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry. 2015;72(4):334–341. doi:10.1001/jamapsychiatry.2014.2502
11. Razzaque MS. Sunlight exposure: do health benefits outweigh harm? J Steroid Biochem Mol Biol. 2018;175:44–48. doi:10.1016/j.jsbmb.2016.09.004
12. Luo CW, Chen SP, Chiang CY, et al. Association between ultraviolet B exposure levels and depression in Taiwanese adults: a nested case-control study. Int J Environ Res Public Health. 2022;19(11):6846. doi:10.3390/ijerph19116846
13. Pjrek E, Friedrich ME, Cambioli L, et al. The efficacy of light therapy in the treatment of seasonal affective disorder: a meta-analysis of randomized controlled trials. Psychother Psychosom. 2020;89(1):17–24. doi:10.1159/000502891
14. Tao L, Jiang R, Zhang K, et al. Light therapy in non-seasonal depression: an update meta-analysis. Psychiatry Res. 2020;291:113247. doi:10.1016/j.psychres.2020.113247
15. Benedetti F, Colombo C, Barbini B, Campori E, Smeraldi E. Morning sunlight reduces length of hospitalization in bipolar depression. J Affect Disord. 2001;62(3):221–223. doi:10.1016/S0165-0327(00)00149-X
16. Gu S, Huang R, Yang J, et al. Exposure-lag-response association between sunlight and schizophrenia in Ningbo, China. Environ Pollut. 2019;247:285–292. doi:10.1016/j.envpol.2018.12.023
17. O’Hare C, O’Sullivan V, Flood S, Kenny RA. Seasonal and meteorological associations with depressive symptoms in older adults: a geo-epidemiological study. J Affect Disord. 2016;191:172–179. doi:10.1016/j.jad.2015.11.029
18. Komulainen K, Hakulinen C, Lipsanen J, et al. Associations of long-term solar insolation with specific depressive symptoms: evidence from a prospective cohort study. J Psychiatr Res. 2022;151:606–610. doi:10.1016/j.jpsychires.2022.05.038
19. Beecher ME, Eggett D, Erekson D, et al. Sunshine on my shoulders: weather, pollution, and emotional distress. J Affect Disord. 2016;205:234–238. doi:10.1016/j.jad.2016.07.021
20. Wang R, Liu Y, Xue D, Yao Y, Liu P, Helbich M. Cross-sectional associations between long-term exposure to particulate matter and depression in China: the mediating effects of sunlight, physical activity, and neighborly reciprocity. J Affect Disord. 2019;249:8–14. doi:10.1016/j.jad.2019.02.007
21. Huibers MJH, de Graaf LE, Peeters FPML, Arntz A. Does the weather make us sad? Meteorological determinants of mood and depression in the general population. Psychiatry Res. 2010;180(2–3):143–146. doi:10.1016/j.psychres.2009.09.016
22. Kim SY, Bang M, Wee JH, et al. Short- and long-term exposure to air pollution and lack of sunlight are associated with an increased risk of depression: a nested case-control study using meteorological data and national sample cohort data. Sci Total Environ. 2021;757:143960. doi:10.1016/j.scitotenv.2020.143960
23. Ahmadi K, Hazrati M, Ahmadizadeh M, Noohi S. Effect of radiance-dimmer devices simulating natural sunlight rhythm on the plasma melatonin levels and anxiety and depression scores of the submarine personnel. Iran J Psychiatry. 2019;14(2):147–153.
24. Henríquez-Sánchez P, Doreste-Alonso J, Martínez-González MA, Bes-Rastrollo M, Gea A, Sánchez-Villegas A. Geographical and climatic factors and depression risk in the SUN project. Eur J Public Health. 2014;24(4):626–631. doi:10.1093/eurpub/cku008
25. Kinser K, Barlow CE, Leonard D, et al. Tanning bed use and depression in a preventive medicine cohort: the Cooper Center Longitudinal Study. J Am Acad Dermatol. 2020;83(4):1200–1202. doi:10.1016/j.jaad.2020.02.037
26. Kerr DCR, Shaman J, Washburn IJ, et al. Two longterm studies of seasonal variation in depressive symptoms among community participants. J Affect Disord. 2013;151(3):837–842. doi:10.1016/j.jad.2013.07.019
27. Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–976. doi:10.1017/s0033291702006074
28. Bu XQ, You LM, Li Y, et al. Psychometric properties of the Kessler 10 scale in Chinese parents of children with cancer. Cancer Nurs. 2017;40(4):297–304. doi:10.1097/NCC.0000000000000392
29. Zhou C, Chu J, T W. Reliability and validity of 10-item Kessler Scale (K10) Chinese version in evaluation of mental health status of Chinese population; 2008. Available from: https://www.webofscience.com/wos/alldb/full-record/CSCD:3457129.
30. O’Connor SS, Beebe TJ, Lineberry TW, Jobes DA, Conrad AK. The association between the Kessler 10 and suicidality: a cross-sectional analysis. Compr Psychiatry. 2012;53(1):48–53. doi:10.1016/j.comppsych.2011.02.006
31. Amare T, Getinet W, Shumet S, Asrat B. Prevalence and associated factors of depression among PLHIV in Ethiopia: systematic review and meta-analysis, 2017. AIDS Res Treat. 2018;2018:5462959. doi:10.1155/2018/5462959
32. Bougie E, Arim RG, Kohen DE, Findlay LC. Validation of the 10-item Kessler Psychological Distress Scale (K10) in the 2012 Aboriginal Peoples Survey. Health Rep. 2016;27(1):3–10.
33. Gou C, Wang Y, Yang R, Huang R, Zhang Q, Zou J. Oral health-related quality of life and parental anxiety in Chinese children undergoing Dental General Anesthesia: a prospective study. BMC Oral Health. 2021;21(1):664. doi:10.1186/s12903-021-01994-2
34. Andrews G, Slade T. Interpreting scores on the Kessler Psychological Distress Scale (K10). Aust N Z J Public Health. 2001;25(6):494–497. doi:10.1111/j.1467-842X.2001.tb00310.x
35. Wu T, Jia X, Shi H, et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. 2021;281:91–98. doi:10.1016/j.jad.2020.11.117
36. Airaksinen J, Gluschkoff K, Kivimäki M, Jokela M. Connectivity of depression symptoms before and after diagnosis of a chronic disease: a network analysis in the U.S. Health and Retirement Study. J Affect Disord. 2020;266:230–234. doi:10.1016/j.jad.2020.01.170
37. Burke TA, Hamilton JL, Seigel D, et al. Sleep irregularity and nonsuicidal self-injurious urges and behaviors. Sleep. 2022;45(6):zsac084. doi:10.1093/sleep/zsac084
38. Lunsford-Avery JR, Engelhard MM, Navar AM, Kollins SH. Validation of the sleep regularity index in older adults and associations with cardiometabolic risk. Sci Rep. 2018;8(1):14158. doi:10.1038/s41598-018-32402-5
39. Lewis R, Roden LC, Scheuermaier K, et al. The impact of sleep, physical activity and sedentary behaviour on symptoms of depression and anxiety before and during the COVID-19 pandemic in a sample of South African participants. Sci Rep. 2021;11(1):24059. doi:10.1038/s41598-021-02021-8
40. Hoogendijk WJG, Lips P, Dik MG, Deeg DJH, Beekman ATF, Penninx BWJH. Depression is associated with decreased 25-hydroxyvitamin D and increased parathyroid hormone levels in older adults. Arch Gen Psychiatry. 2008;65(5):508–512. doi:10.1001/archpsyc.65.5.508
41. Lee DM, Tajar A, O’Neill TW, et al. Lower vitamin D levels are associated with depression among community-dwelling European men. J Psychopharmacol. 2011;25(10):1320–1328. doi:10.1177/0269881110379287
42. Milaneschi Y, Shardell M, Corsi AM, et al. Serum 25-hydroxyvitamin D and depressive symptoms in older women and men. J Clin Endocrinol Metab. 2010;95(7):3225–3233. doi:10.1210/jc.2010-0347
43. Anglin RES, Samaan Z, Walter SD, McDonald SD. Vitamin D deficiency and depression in adults: systematic review and meta-analysis. Br J Psychiatry. 2013;202:100–107. doi:10.1192/bjp.bp.111.106666
44. Annweiler C, Rastmanesh R, Richard-Devantoy S, Beauchet O. The role of vitamin D in depression: from a curious idea to a therapeutic option. J Clin Psychiatry. 2013;74(11):1121–1122. doi:10.4088/JCP.13ac08783
45. Parker GB, Brotchie H, Graham RK. Vitamin D and depression. J Affect Disord. 2017;208:56–61. doi:10.1016/j.jad.2016.08.082
46. Holick MF. Biological effects of sunlight, ultraviolet radiation, visible light, infrared radiation and vitamin D for health. Anticancer Res. 2016;36(3):1345–1356.
47. Wacker M, Holick MF. Sunlight and vitamin D: a global perspective for health – PubMed; 2013. https://pubmed.ncbi.nlm.nih.gov/24494042/.
48. Engelsen O. The relationship between ultraviolet radiation exposure and vitamin D status. Nutrients. 2010;2(5):482–495. doi:10.3390/nu2050482
49. Jia Y, Liu L, Sheng C, et al. Increased serum levels of cortisol and inflammatory cytokines in people with depression. J Nerv Ment Dis. 2019;207(4):271–276. doi:10.1097/NMD.0000000000000957
50. Hadlow NC, Brown S, Wardrop R, Henley D. The effects of season, daylight saving and time of sunrise on serum cortisol in a large population. Chronobiol Int. 2014;31(2):243–251. doi:10.3109/07420528.2013.844162
51. Thomas J, Al-Anouti F. Sun exposure and behavioral activation for hypovitaminosis D and depression: a controlled pilot study. Community Ment Health J. 2018;54(6):860–865. doi:10.1007/s10597-017-0209-5
52. Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, Stubbs B. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. 2019;107:525–539. doi:10.1016/j.neubiorev.2019.09.040
53. Smith K. Mental health: a world of depression. Nature. 2014;515(7526):181. doi:10.1038/515180a
54. Olfson M, Marcus SC, Tedeschi M, Wan GJ. Continuity of antidepressant treatment for adults with depression in the United States. Am J Psychiatry. 2006;163(1):101–108. doi:10.1176/appi.ajp.163.1.101
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Parental Involvement, Academic Self-Efficacy, and Depression on Academic Performance Among Chinese Students During COVID-19 Pandemic
Kang L, Li C, Chen D, Bao X
Psychology Research and Behavior Management 2024, 17:201-216
Published Date: 18 January 2024