Back to Journals » Journal of Multidisciplinary Healthcare » Volume 9
Association between sociodemographic characteristics of female community health volunteers and their knowledge and performance on maternal and child health services in rural Nepal
Authors Acharya D ![]() , Singh JK
, Singh JK ![]() , Adhikari S, Jain V
, Adhikari S, Jain V
Received 20 October 2015
Accepted for publication 13 January 2016
Published 21 March 2016 Volume 2016:9 Pages 111—120
DOI https://doi.org/10.2147/JMDH.S98700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dilaram Acharya,1,2 Jitendra Kumar Singh,3,4 Samaj Adhikari,5 Varidmala Jain6
1Department of Community Medicine, Kathmandu University, Devdaha Medical College and Research Institute, Devdaha-10, Rupandehi, Nepal; 2Department of Public Health, Purbanchal University, Sanjeevani College of Medical Sciences, Butwal, Rupandehi, Nepal; 3Department of Community Medicine and Public Health, Janaki Medical College, Tribhuvan University, Janakpur, Nepal; 4Department of Community Medicine, Institute of Medical Sciences, Banaras Hindu University, India; 5Institute of Medicine, Maharajgunj Medical Campus,Tribhuvan University, Kathmandu, Nepal; 6Department of Public Health, Faculty of Health Sciences, Sam Higginbottom Institute of Agriculture,Technology and Sciences, Allahabad, India.
Background: Engaging community health volunteers and community health workers to provide maternal and child health (MCH) care services in resource-poor settings is one of the global and widely used concepts. Despite a great role of female community health volunteers (FCHVs) in MCH services in Nepal, few research studies have been performed in this area. Our research aimed to assess the knowledge and performance of FCHVs on MCH services associated with their sociodemographic characteristics.
Methods: A cross-sectional survey was conducted to assess the knowledge and performance on selected MCH services of FCHVs using structured questionnaire in 16 village development committees of Dhanusha district, Southern Terai, Nepal, from the first of January to the end of February of 2014. A total of 138 FCHVs were selected by using multistage random sampling technique. Logistic regression was employed to examine the association between selected sociodemographic characteristics and knowledge and performance on MCH services of FCHVs after adjusting for significant variables associated with knowledge and performance and within-cluster effect.
Results: Our findings demonstrated that sociodemographic characteristics were associated independently with good knowledge of FCHVs on MCH services: education level secondary and above (adjusted odds ratio [aOR] 5.2; 95% confidence interval [CI] 2.2–12.2); residing in Mother and Infant Research Activities, nongovernmental organization working area (aOR 3.7; 95% CI 1.5–8.8); and middle caste (aOR 3.3; 95% CI 1.0–10.3). Similarly, satisfactory performance of FCHVs significantly associated with MCH services were education level secondary and above (aOR 8.9; 95% CI 3.2–24.3) and residing in Mother and Infant Research Activities working areas (aOR 9.0; 95% CI 3.5–22.6).
Conclusion: The study recommends considering education level while recruiting rural FCHVs and capacity enhancement through additional training and development programs in collaboration with developmental partner.
Keywords: FCHV, knowledge, performance, sociodemographic characteristics, Nepal
Introduction
The earliest concept of community health workers in the world came into existence from Chinese barefoot doctors program and Thailand village health volunteers and communicators.1,2 Community health volunteers and community health workers are potential assets to deal with many maternal and child health (MCH) problems in resource-limited settings. Community health volunteers from Bangladesh demonstrated the good knowledge and management of childhood illness.3–5 The concept of female community health volunteer (FCHV) program in Nepal was introduced in 1988–1989.6,7 Broadly, the chief goal of FCHV program is to help in achieving national health goal through community involvement. FCHVs, the self-motivated cadres selected by local mother’s group, address MCH through promotional and preventive measures in conjunction with reducing child acute respiratory tract infections and diarrheal diseases and newborn care through curative measures. FCHVs are the major backbone in implementing public health programs, namely, family planning, safe motherhood, vitamin A supplementation, deworming, sick child care, and immunization. There are altogether 50,000 FCHVs in Nepal operating in each village development committee (VDC) under Family Health Division, Ministry of Health.6,8 The major health challenges of Nepal are life expectancy, infant, maternal, and under five mortality. High poverty, illiteracy, and geographical barrier are the key factors that affect the health status among Nepalese.9 In Nepal, according to Nepal Demographic and Health Survey, infant mortality rate is 45 per thousand and under five mortality rate is 54.5 per thousand. Similarly, maternal mortality ratio is 229 per hundred thousands live births and institutional delivery is 35.3%.10 There has been improvement in health indicators pertaining to MCH, thanks to the active role of FCHVs.11
The major responsibilities of FCHVs delegated to them in delivering maternal health service delivery include counseling and advice during pregnancy, focusing on nutrition, antenatal care, immunization, iron and folate consumption, and postpartum visit. Similarly, in child health service delivery, they participate in delivering essential new born care (safe cord clamping, cord stump care, early breast feeding, and prevention of hypothermia), treating the child with acute respiratory tract infections, and early referral of the sick child. Assessing the knowledge and performance of health workers is essential; many countries focus on them as they are good assets for achieving the millennium development goals.12 Various sociodemographic correlates determine the level of knowledge and performance of community health workers. Community health workers of higher age group have better performance on service delivery.13 Female health workers of higher age group are established members of society and have already obtained enough exposures earlier. Educational level affects knowledge and performance of health workers. Literate workers are better owing to enhanced service delivery skills. Community health workers who have obtained higher level of education outperform those who are illiterate.14 Similarly, work experience as a health volunteer affects the level of knowledge and performance. Experienced ones outperform the naïve ones.15 Prior studies of Ethiopia and Nigeria, respectively, demonstrated work experience as a strong predictor of knowledge and practice toward tuberculosis control and injection safety among health workers.13,16
There is a synergistic effect of local nongovernmental organizations (NGOs) and performance of community health workers. In Nepal, Mother and Infant Research Activities (MIRA) is an NGO that conducts studies, launches interventions for improving maternal and infant health, and trains FCHVs. An effective program of neonatal sepsis identification and management with collaboration of local NGOs with community health volunteers has been reported in a previously published Nepalese article.17 An analytical report on national survey of FCHVs of Nepal reported that the highest percentage of FCHVs is in the age group 30–39 years. About 62% of FCHVs are literate, of which 42% have completed primary school or have ever gone to secondary education. Additionally, the same report highlighted that the FCHVs had better knowledge of MCH compared with rural women and performed better in terms of pregnancy counseling, and >90% of them could provide essential newborn care.8 This study aims to highlight sociodemographic factors associated with knowledge and performance of FCHVs in delivering MCH services in rural Nepal.
Materials and methods
Study subjects and setting
A cross-sectional survey assessing knowledge and performance of FCHV on MCH services using a structured questionnaire was used in 16 VDCs of Dhanusha district of Nepal from the first of January to the end of February of 2014. Among these 16 VDCs, six were engaged in MIRA, an NGO working in Dhanusha district, Nepal. The district was selected purposively because approximately all the indicators of MCH service utilization in this district were found lower as compared to adjacent district and national figure.6,17,18
Study design and sampling
This was a cross-sectional study conducted among 138 FCHVs working in 16 VDCs of Dhanusha district of Nepal. The sample size for this study was calculated by using a sample size calculator for finite population.19 There are 101 VDCs in Dhanusha district and 909 FCHVs working in rural area. Hence, the population size (N) is 909. P is taken as 0.12 (proportion of FCHVs in Dhanusha who miscategorized infant weight in a trial by MIRA is 12%).20 The permissible margin of error in the estimated value was taken as 5% with degree of assurance as 95% confidence level. After entering all the values in the calculator, we obtained 134 FCHVs as the sample size. Taking all the FCHVs available during the survey in 16 VDCs, the total number of FCHVs included in this study became 138 as the final sample. Multistage random sampling was adopted to select FCHVs. Dhanusha district of Nepal was selected purposively. Out of seven primary health care centers (PHCCs) in Dhanusha district, four PHCCs were randomly selected. Then, the list of VDCs in the selected PHCCs was obtained from the District Public Health Office, Dhanusha. There were 35 VDCs in these four PHCCs. Altogether, 16 VDCs (four from each PHCC) were selected randomly to meet 138 FCHVs.
Data management and statistical analysis
A face-to-face interview was conducted using structured questionnaire. The outcome variables of the study were the knowledge and performance of FCHVs on MCH services. Assessment of knowledge and performance of FCHVs on MCH services was based on the several parameters of MCH services that are obtained from maternal and newborn health counseling package “Jeevan Suraksha” developed by United States Agency for International Development, which has been adopted by the Department of Health Services, Ministry of Health and Population, Government of Nepal, National Nutrition Policy and Strategy, and National FCHV Programme Revised Strategy of Nepal.21–23 Assessment of knowledge of FCHVs was assessed on the basis of the following ten major MCH parameters recommended by the Government of Nepal (see Supplementary Materials):
- minimum number of antenatal care visit recommended;
- total number of iron/folic acid tablets to be consumed during pregnancy;
- dose for tetanus toxoid immunization;
- dose of deworming;
- presence of skilled birth attendants provides safe delivery;
- number of postnatal visits recommended by the Government of Nepal;
- number of iron tablets to be consumed postpartum;
- dose of vitamin A;
- number and time for child immunization; and
- additional food intake required.
Assessment of performance of FCHVs was on the basis of the following ten parameters of MCH services recommended by the Government of Nepal:
- create community awareness to promote health and healthy behaviors;
- counsel pregnant women on antenatal visit and postnatal visit;
- counsel pregnant women for safe delivery (skilled birth attendants/institutional delivery);
- conduct regular mothers meeting;
- counsel pregnant women for additional diet;
- counsel postnatal mothers on breastfeeding, weaning, and growth monitoring;
- distribute condom, pills, oral rehydration solution packets, and vitamin A capsules;
- mobilize mother and children for immunization;
- refer complicated cases to health institution; and
- regular reporting of pregnancy to health facilities.
One score (0 or 1) was assigned for each parameter by asking the respondents for their knowledge and performance regarding MCH services. For knowledge, we assigned score 0 for each of the incorrect answer and score 1 for each of the correct answer. Similarly, a score was assigned for each of the parameter of performance. We assigned score 0 if there was no task performed by FCHVs and score 1 if there was partial or full task performed by FCHVs. As the score of these parameters ranged between 0 and 1, the total possible maximum score is 10 for each knowledge and performance. The sum of scores for all the parameters for each participant was calculated and taken as the level of knowledge and performance. The median for knowledge and performance was calculated. The total scores for each respondent were then split in median. If the correct answers were equal or more than the median score, the FCHV’s knowledge was considered “Good.” If the correct answers were less than the median, the knowledge was considered “Poor.” Similarly, performance was considered “Satisfactory” for equal and more than median scores and “Unsatisfactory” for scores less than the mean.24
Age of FCHVs was categorized as <35 years, 35–45 years, and >45 years. Education was recorded as literate/primary and secondary and above. Ethnicity/caste was based on the caste system in Nepal and was divided into three major groups based on available literature and similarities between the caste/ethnic groups: advantaged/upper caste (Brahmin, Chhetri, and Bhumihaar), middle caste (Yadav, Koiri, Sudi/Teli), and lower caste (Dalit, Janjati, Mandal).25 Religion was categorized as Hindu and Muslims/others (Christian, Boudha). Working experience as a health volunteer was recorded as <10 years and ≥10 years. Residential and working areas of FCHVs were categorized as MIRA and non-MIRA.
Knowledge in terms of good and poor category and performance in terms of satisfactory and unsatisfactory category were taken as the dependent variables. Age, education, caste, religion, work experience as a health volunteer, and place of residence at MIRA working area were taken as explanatory variables. The association between independent variables and the level of knowledge and performance were examined using chi-square (χ2) test in univariate analysis. Then, the effect of each of the explanatory variables was adjusted for all other variables together in a multivariable logistic regression model. A P-value ≤0.05 was considered statistically significant. Data were analyzed using Statistical Package for Social Sciences Version 20.0 for Windows.
Ethics
This study obtained the ethical approval from the Institutional Review Board of Banarus Hindu University, India, and written approval letter was obtained from District Health Office, Janakpur. The aims and objectives of the study were explained to the respondents before data collection. FCHVs provided written informed consent before an interview. Personal identifiers were removed before data analysis.
Results
Differentials in characteristics of respondents’ between known levels of knowledge and performances
In a total of 138 FCHVs, three-quarters of them (76.9%) were >35 years of age. Majority of them had more than secondary and above level of education (61.6%), believed in the Hindu religion (79.0%), work experience as volunteer ≥10 years (65.2%), and area of residence non-MIRA area (62.3%). The unadjusted odds ratio shows that all the sociodemographic variables of the FCHVs were associated with good knowledge of MCH services except the religion. However, only the age, educational level, and area of residence where MIRA is working were associated with satisfactory level of performance on MCH care services (Table 1).
 | Table 1 Knowledge and performance of FCHVs on MCH services according to sociodemographic characteristics |
Factors associated with knowledge and performance of FCHVs on maternal child health services
The multiple logistic regression analysis was employed to analyze the factors associated with knowledge and performance of FCHVs on MCH services (Table 2). Adjusting for significant variables associated with knowledge and performance and within-cluster effect, level of education and area of residence where MIRA is working were significantly associated with both the knowledge and the performance of FCHVs. FCHVs who had education level secondary and above were likely to have good knowledge (adjusted odds ratio [aOR] 5.2; 95% confidence interval [CI] 2.2–12.2) and satisfactory performance (aOR 8.9; 95% CI 3.2–24.3) on MCH services than only literate and primary level of education. FCHVs who were residing in MIRA working areas were more likely to have good knowledge (aOR 3.7; 95% CI 1.5–8.8) and satisfactory performance (aOR 9.0; 95% CI 3.5–22.6) on MCH services than those who were residing beyond MIRA working areas. The result also revealed that middle caste FCHVs were more likely to have good knowledge (aOR 3.3; 95% CI 1.0–10.3) on MCH services than upper and lower caste.
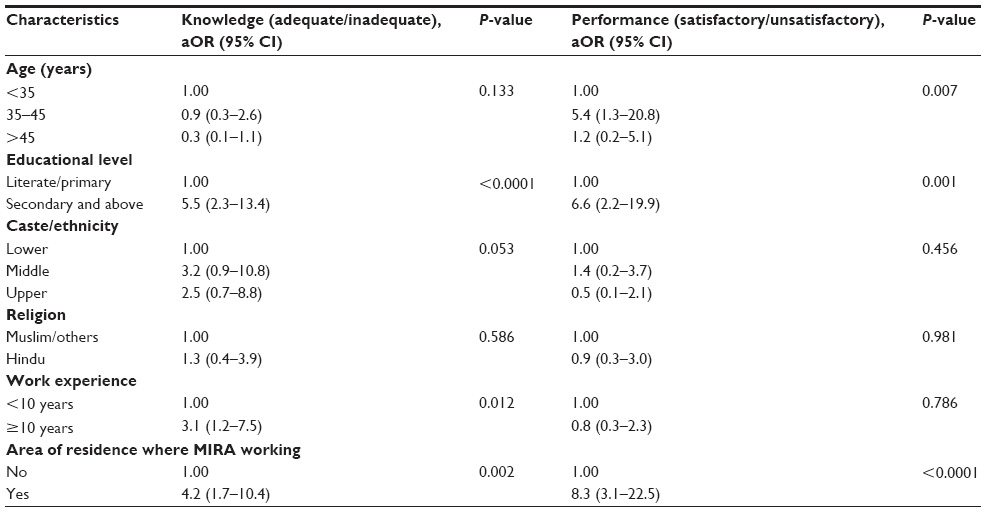 | Table 2 Multiple logistic regression model for knowledge and performance on MCH service of FCHVs |
Discussion
Previously published research articles on FCHVs highlighted the detection and management of low-birth weight babies, early pregnancy detection, and use of FCHVs for childhood illness from user perspectives.20,26,27 Our study demonstrated that knowledge and performance of FCHVs on MCH services are affected by selected sociodemographic factors in rural Nepal.
Increased level of education among FCHVs and their area of residence where MIRA is working are significantly associated with good knowledge and satisfactory performance on MCH services. FCHVs who had attained higher educational level were more likely to have sound knowledge and satisfactory performance, which could be attributed to contribution of school health curriculum and enhancement of service delivery skills with increasing educational level. Contrarily, a study done in India revealed that overqualified (with higher education) community health workers are less interested in field-based work and had lower performance level.28 However, this is consistent with one of the major findings of the Kenyan study that demonstrated that the higher level of education of community health workers was associated with better performance of maternal health services.14 Additionally, the finding in this study is similar with Nigerian and Bangladeshi studies.29,30 MIRA, an NGO working for capacity improvement of FCHVs in Dhanusha district of Nepal, might influence the better knowledge and performance on MCH services.17 For the better performance of MCH service delivery in rural Nepal, therefore, more focus is needed on upgrading the level of education and engaging the development partners that can assist in improving FCHVs’ knowledge and performance.
This study has strengths as it has identified some predictors on knowledge and performance of FCHVs on MCH services in rural Nepal based on primary data. However, this is not free from its limitations. As this cross-sectional study covered only a small area of Southern Terai, Nepal, the findings cannot be generalized to whole FCHVs existing in Nepal. Further study on FCHVs taking a large sample size and more variables is recommended.
Conclusion
Level of education and area of residence of FCHVs where an NGO is working influenced positively the knowledge and performance of MCH services. The study recommends considering level of education while recruiting rural FCHVs and capacity enhancement through additional training and development programs in collaboration with developmental partners.
Acknowledgments
We would like to thank our research assistants and all FCHVs for their kind cooperation during this study. We are grateful to Deepak Adhikari, PhD (Department of Anatomy and Developmental Biology, Monash University, Melbourne, Victoria, Australia) for final English check and editing of our manuscript.
Author contributions
DA and JKS participated in the study design. DA and JKS performed statistical analysis and wrote manuscript with significant contribution from SA. SA and VJ contributed to the analysis, interpretation of the results, literature review, and revision of the manuscript. All the authors contributed in revision and agreed on the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Kc N, Kc A, Sharma N, et al. Community participation and mobilization in community-based maternal, newborn and child health programmes in Nepal. J Nepal Health Res Counc. 2011;9(2):101–106. | |
Kawakatsu Y, Sugishita T, Kioko J, Ishimura A, Honda S. Factors influencing the performance of community health workers in Kisumu West, Kenya. Prim Health Care Res Dev. 2012;13(04):294–300. | |
Rashid SF, Hadi A, Afsana K, Begum SA. Acute respiratory infections in rural Bangladesh: cultural understandings, practices and the role of mothers and community health volunteers. Trop Med Int Health. 2001;6(4):249–255. | |
Hadi A. Management of acute respiratory infections by community health volunteers: experience of Bangladesh Rural Advancement Committee (BRAC). Bull World Health Organ. 2003;81(3):183–189. | |
Brown A, Malca R, Zumaran A, Miranda JJ. On the front line of primary health care: the profile of community health workers in rural Quechua communities in Peru. Hum Resour Health. 2006;4(1):11. | |
Department of Health Services. Annual report. Department of Health Services 2070/71 (2013/2014) Kathmandu: Department of Health Services, Ministry of Health and Population, Government of Nepal (GoN); 2014. Available from: http://dohs.gov.np/wp-content/uploads/2014/04/Annual_Report_2070_71.pdf. Accessed February 18, 2016. | |
Glenton C, Scheel IB, Pradhan S, Lewin S, Hodgins S, Shrestha V. The FCHV programme in Nepal: decision makers’ perceptions of volunteerism, payment and other incentives. Soc Sci Med. 2010;70(12): 1920–1927. | |
New ERA. An analytical report on national survey of female community health volunteers of Nepal. Kathmandu: United States Agency for International Development (USAID); 2007. Available from: https://dhsprogram.com/pubs/pdf/FR181/FCHV_Nepal2007.pdf. Accessed February 18, 2016. | |
Deslich BJ. Health Issues in Nepal. 2003. Available from: http://w3.whosea.org/drd/hlth_sit_nepal.htm. Accessed February 18, 2016. | |
Ministry of Health and Population. Nepal Demographic and Health Survey. Kathmandu: 2011. Available from: http://dhsprogram.com/pubs/pdf/FR257/FR257%5B13April2012%5D.pdf Nepal and Calverton, Maryland, U.S.A.: Ministry of Health and Population, New ERA and ICF International; 2012. kathmandu: 2012. Accessed February 18, 2016. | |
Selemani M, Masanja IM, Kajungu D, et al. Health worker factors associated with prescribing of artemisinin combination therapy for uncomplicated malaria in rural Tanzania. Malar J. 2013;12(1):334. | |
Haines A, Sanders D, Lehmann U, et al. Achieving child survival goals: potential contribution of community health workers. Lancet. 2007;369(9579):2121–2131. | |
Gizaw GD, Alemu ZA, Kibret KT. Assessment of knowledge and practice of health workers towards tuberculosis infection control and associated factors in public health facilities of Addis Ababa, Ethiopia: a cross-sectional study. Arch Public Health. 2015;73(1):15. | |
Crispin N, Wamae A, Ndirangu M, et al. Effects of selected socio-demographic characteristics of community health workers on performance of home visits during pregnancy: a cross-sectional study in Busia District, Kenya. Glob J Health Sci. 2012;4(5):78. | |
Khiavi RF. Factors affecting the performance of health workers about family planning programs. WALIA J. 31(S1):175–179, 2015. | |
Onyemocho A, Anekoson JI, Pius EO. Knowledge and practice of injection safety among workers of Nigerian prison service health facilities in Kaduna state. Am J Public Health Res. 2013;1(7):171–176. | |
Shrestha BP, Bhandari B, Manandhar DS, Osrin D, Costello A, Saville N. Community interventions to reduce child mortality in Dhanusha, Nepal: study protocol for a cluster randomized controlled trial. Trials. 2011;12(1):136. | |
Department of Health Services. Annual Report. 2012/2013. Available from: http://dohs.gov.np/wp-content/uploads/2014/04/Annual_Report_2069_70.pdf. Accessed February 18, 2016. | |
Kotrlik J, Higgins C. Organizational research: determining appropriate sample size in survey research appropriate sample size in survey research. Inform Tech Learn Perform J. 2001;19(1):43. | |
Amano S, Shrestha B, Chaube S, et al. Effectiveness of FCHVs in the detection and management of low-birth-weight in Nepal. Rural Remote Health. 2014;14(1):2508. | |
Department of Health Service, Population MoHa. National Nutrition Policy and strategy. Kathmandu: Ministry of Health and Population, Department of Health Services, Child Health Division, Nutrition Section; 2004. Available from http://dohs.gov.np/wpcontent/uploads/chd/Nutrition/Nutrition_Policy_and_Strategy_2004.pdf. Accessed on March 3, 2016. | |
Department of Health Service, Population MoHa. National FCHV Program Revised Strategy. Kathmandu: Department of Health Service, Ministry of Health and Population. 2004. Available from http://www.mohp.gov.np/images/pdf/policy/FCHV%20Strategy.pdf. Accessed March 03, 2016. | |
McPherson RA, Tamang J, Hodgins S, et al. Process evaluation of a community-based intervention promoting multiple maternal and neonatal care practices in rural Nepal. BMC Pregnancy Childbirth. 2010;10(1):31. | |
Khun M, Heng C, Kasuya H, Sakamoto J. Knowledge, attitudes and practices towards avian influenza A (H5N1) among Cambodian women: a cross-sectional study. Asian Pac J Trop Med. 2012;5(9): 727–734. | |
Khanal V, Adhikari M, Sauer K, Zhao Y. Factors associated with the introduction of prelacteal feeds in Nepal: findings from the Nepal demographic and health survey 2011. Int Breastfeed J. 2013;8(1):9. | |
Andersen K, Singh A, Shrestha MK, Shah M, Pearson E, Hessini L. Early pregnancy detection by FCHVs in Nepal facilitated referral for appropriate reproductive health services. Glob Health Sci Pract. 2013;1(3):372–381. | |
Miyaguchi M, Yasuoka J, Poudyal AK, Silwal RC, Jimba M. FCHVs service utilization for childhood illness- improving quality of health services only is not enough: a cross-sectional study in mid-western region, Nepal. BMC Health Serv Res. 2014;14:383. | |
Sharma R, Webster P, Bhattacharyya S. Factors affecting the performance of community health workers in India: a multi-stakeholder perspective. Glob Health Act. 2014;7:25352. | |
Ryan JM, John GC, Brieger WR. Five-year knowledge retention by volunteer primary health workers in western Nigeria. Int Q Community Health Educ. 1990;11(2):123–133. | |
Ahmed SM, Hossain MA. Knowledge and practice of unqualified and semi-qualified allopathic providers in rural Bangladesh: implications for the HRH problem. Health Policy. 2007;84(2):332–343. |
Supplementary materials
 | Figure S1 Survey questionnaire. |
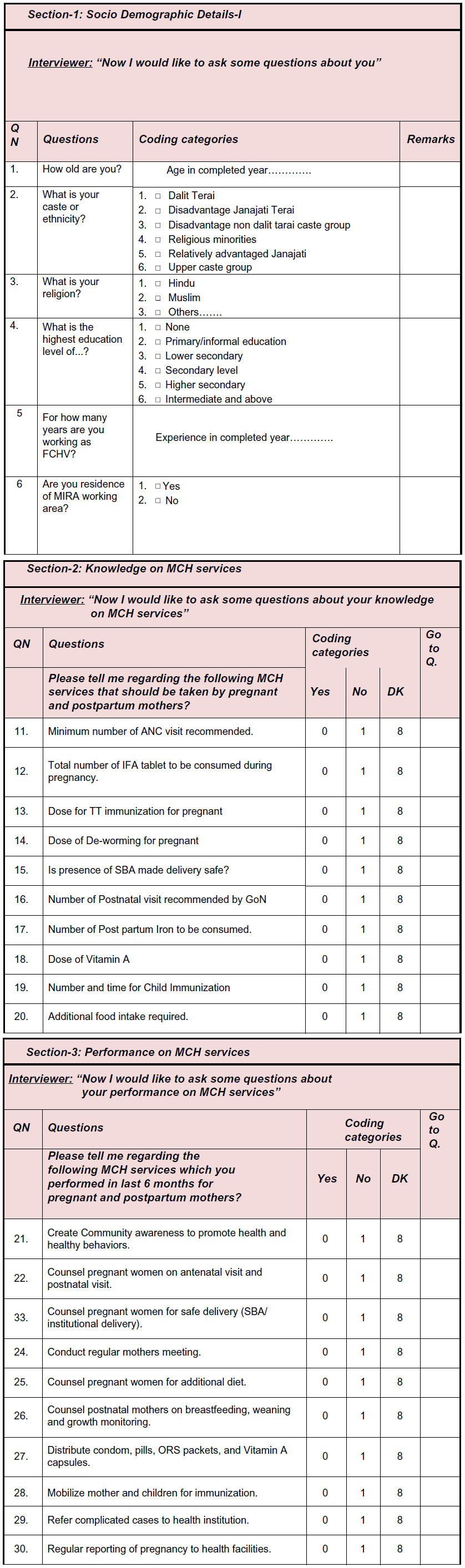 | Abbreviations: MIRA, Mother and Infant Research Activities, IFA, iron and folic acid ; TT, tetanus toxoid; SBA, skilled birth attendants; GoN, Government of Nepal; ORS, oral rehydration salt; DK, do not know; ANC, antenatal care. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.