Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Association Between Sleep Disorders and Adverse Cardiovascular Outcomes in Patients with Chronic Obstructive Pulmonary Disease: Insights from the UK Biobank
Authors An X, Chen Y, Wang Y, Zhu W, Li F, Shen J, Zhang C, Wu Y ![]() , Yu R
, Yu R
Received 9 March 2026
Accepted for publication 1 June 2026
Published 9 June 2026 Volume 2026:21 607991
DOI https://doi.org/10.2147/COPD.S607991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Xian An,1,* Yuting Chen,2,* Yuan Wang,1 Wenjie Zhu,1 Fan Li,1 Jiran Shen,3 Chengxin Zhang,4 Ye Wu,1 Ronghui Yu5
1Department of Social Medicine and Health Service Management, School of Health Management, Anhui Medical University, Hefei, People’s Republic of China; 2Department of Research, the First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3Department of Cardiovascular Medicine, the First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 4Department of Cardiovascular Surgery, First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 5Department of Cardiology, National Cardiovascular Disease Regional Center for Anhui, the First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ronghui Yu, Department of Cardiology, National Cardiovascular Disease Regional Center for Anhui, the First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China, Tel +86 13901080383, Email [email protected] Ye Wu, Department of Social Medicine and Health Service Management, School of Health Management, Anhui Medical University, Hefei, People’s Republic of China, Tel +86 13966717711, Email [email protected]
Background and Objective: A potential association between sleep disturbances and adverse cardiovascular prognoses has been proposed in patients with chronic obstructive pulmonary disease (COPD), although high-quality confirmatory evidence remains limited. Sleep disturbances may contribute to increased cardiovascular risk through multiple biological pathways, including chronic intermittent hypoxia, systemic inflammation, and metabolic dysregulation. This study aimed to examine the association between sleep disturbances and adverse cardiovascular events in patients with COPD.
Materials and Methods: A prospective cohort study of 21423 UK Biobank participants with COPD. We set the research subjects as non-sleep disorder group and sleep disorder group. Outcomes included stroke, heart failure (HF), atrial fibrillation (AF), angina pectoris, and myocardial infarction (MI). Cox proportional hazards models were applied with adjustment for sociodemographic and lifestyle factors to evaluate the association between sleep disorders and subsequent cardiovascular outcomes.
Results: In this manuscript, compared with COPD patients in the non-sleep disorder group, sleep disorder group had a 79% higher risk of HF (HR = 1.79, 95% CI: 1.57– 2.03). Moreover, sleep disorder had a 49% higher HR for AF (HR = 1.49, 95% CI: 1.32– 1.68) and a 44% higher HR for angina development (HR = 1.44, 95% CI: 1.23– 1.68). The risk of MI was also increased by 0.24-fold in the sleep disorder group (HR = 1.24, 95% CI: 1.01– 1.54). Furthermore, male sex, older age, previous cardiovascular medication use, smoking, and obesity were significantly associated with elevated cardiovascular risk among COPD patients with sleep disorders.
Conclusion: Sleep disorders are associated with an increased risk of adverse cardiovascular outcomes in COPD patients. These findings suggest that identification and appropriate management of sleep disorders could potentially contribute to improved cardiovascular risk profiles in this population.
Keywords: sleep disorders, adverse cardiovascular outcomes, COPD, UKB
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide, seriously affecting the physical and mental health of residents.1–3 Cardiovascular disease (CVD) is one of the important causes of increased mortality in COPD patients.4–6 Research showed that COPD patients with concomitant CVD had significantly increased mortality rates, the incidence rate and mortality of COPD and CVD were interrelated.7,8 A survey based on the National Health and Nutrition Examination in the United States (NHANES) showed that the risk of CVD (including coronary heart disease, heart failure, myocardial infarction, and stroke) in all COPD phenotype patients was significantly higher than that in non-COPD populations.9 COPD was characterized by chronic airway obstruction and abnormal inflammation of the lungs, accompanied by symptoms such as difficulty breathing and coughing, which can easily lead to sleep disorders.10 Sleep was closely related to gas exchange, and changes in nighttime ventilation and respiratory symptoms may lead to difficulty maintaining sleep.11 COPD patients often experienced obstructive sleep apnea (OSA), central sleep apnea (CSA), sleep-related hypoxemia, sleep structural disorders, and insomnia as a result.12–14 A study found that 74.8% of COPD patients had poor sleep quality.15 Susan’s research found that OSA was often comorbid with CVD and had a bidirectional association. OSA increased CVD risk through physiological disorders such as intermittent hypoxia and sympathetic activation.16 Previous studies demonstrated that OSA induced systemic inflammation, oxidative stress, and metabolic dysregulation via chronic intermittent hypoxia, and upregulated the secretion of adipokines including asprosin. Elevated asprosin levels further exacerbated insulin resistance, systemic inflammation, and aberrant fat distribution, collectively contributing to vascular endothelial dysfunction, atherosclerosis, and an increased risk of adverse cardiovascular events.17 The American Heart Association (AHA) pointed out that OSA was a common and frequently underdiagnosed chronic disorder, with a prevalence of 40% to 80% among patients with hypertension, heart failure, coronary artery disease, atrial fibrillation, pulmonary hypertension, and stroke. AHA recommended routine screening and evaluation for OSA in patients with resistant hypertension, pulmonary hypertension, recurrent atrial fibrillation following cardioversion or ablation, NYHA class II–IV heart failure with suspected sleep-disordered breathing, tachy-brady syndrome, ventricular tachycardia, survivors of sudden cardiac death, as well as those with nocturnal angina, myocardial infarction, or arrhythmias.18 In addition, there had been detailed reviews summarizing the relationship between sleep and CVD.19 Multiple research findings indicated that individuals with sleep disorders had an increased risk of CVD and mortality.20–23 Another survey based on UKB showed that compared to the high sleep quality group, the low sleep quality group had a 67% increased risk of CVD.24 Screening for sleep disorders and early treatment in COPD may represent a potential strategy to reduce adverse cardiovascular outcomes in these patients. In summary, we had to consider the impact of sleep disorders on the occurrence of adverse cardiovascular outcomes in COPD patients. The association between these three types may become an emerging direction for improving the prognosis of COPD patients and reducing mortality rates.
In order to expand the previous research results, this manuscript aimed to explore the relationship between sleep disorders and adverse cardiovascular events (including stroke, atrial fibrillation, heart failure, angina pectoris, and myocardial infarction) in patients with COPD.
Materials and Methods
Study Design and Population
This study was a retrospective analysis, with 502112 data sourced from patients diagnosed with COPD in the UK Biobank (UKB) database between 2006 and 2024. Our study was based on an approved UK Biobank application (Application No. 280417). Ethical approval was granted by the North West Research Ethics Committee (11/NW/0382, 21/NW/0157) and the Clinical Research Ethics Committee of The First Affiliated Hospital of Anhui Medical University (PJ 2024–13-46). All participants provided written informed consent. The specific data filtering steps were presented in Figure 1. These patients had varying degrees of sleep disorders and different CVD at the time of diagnosis and after diagnosis. The exclusion criteria were as follows: baseline combined with other severe lung diseases (such as pulmonary fibrosis); sleep data showed extreme outliers; if participants self-reported their diagnosis of heart disease or heart failure (angina, heart attack and stroke) at baseline.
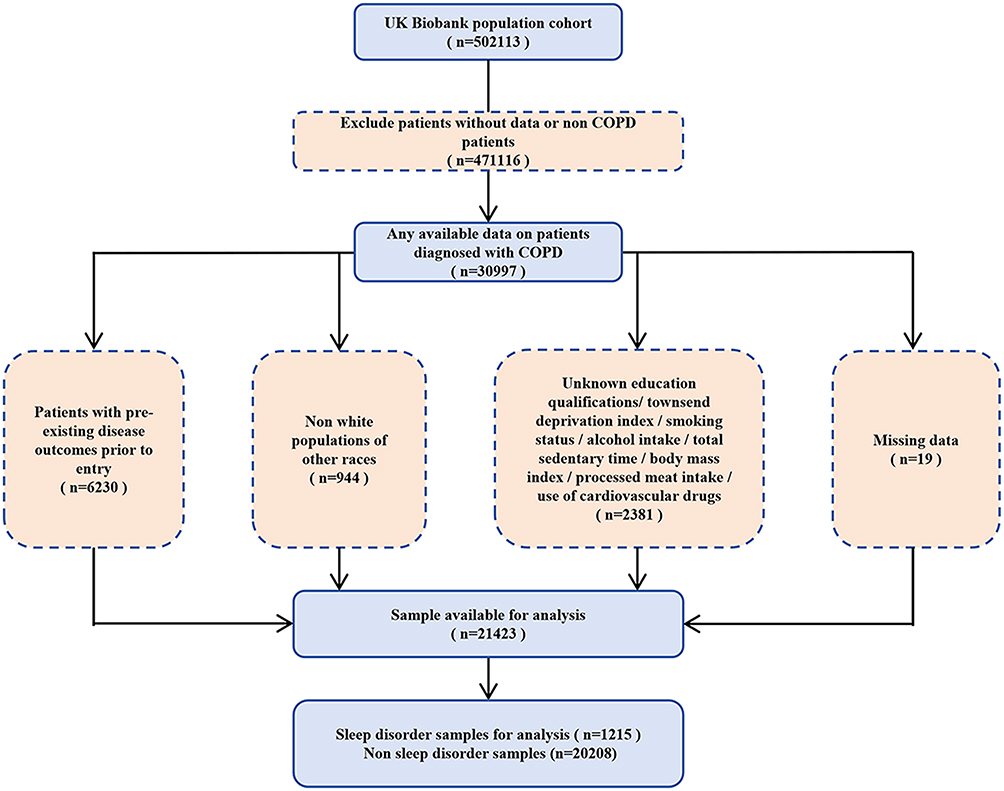 |
Figure 1 Flowchart of the UK Biobank. |
Assessment of Sleep Disorders
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and the International Classification of Diseases, 11th Revision (ICD-11), as well as relevant guidelines from the UK National Institute for Health and Care Excellence (NICE), this study defined sleep disorders as persistent sleep-related abnormal phenotypes that impair daytime function. These phenotypes included insomnia, habitual snoring, OSA, organic or non-organic sleep disorders, restless legs syndrome, and circadian rhythm sleep–wake disorders.25,26 Using the STOP-Bang questionnaire and Epworth Sleepiness Scale (ESS) as auxiliary reference indicators for grouping, individuals with insomnia, habitual snoring, organic or non-organic sleep disorders, or OSA were classified into the sleep disorder group. Among them, insomnia was identified based on self-reported difficulty falling asleep or frequent nighttime awakenings from the UKB baseline touchscreen questionnaire (Field 1200).27,28 Individuals who stayed up late in the short term, experienced transient sleep disturbances, or suffered from temporary poor sleep solely caused by short-term stress were excluded.
Outcome
This study evaluated the association between sleep disorders and adverse cardiovascular events by reviewing the UKB database. To minimize information bias, all key outcomes were confirmed through structured medical records and/or standardized telephone follow-up. The research findings reported in this section cover the following major cardiovascular endpoints: stroke, heart failure (HF), atrial fibrillation (AF), angina pectoris (angina) and myocardial infarction (MI).29
To ensure the accuracy and comparability of the study endpoints, this study adopted unified and clear clinical diagnostic criteria for various cardiovascular events: diagnosis of stroke should be based on clinical manifestations and imaging examinations (such as CT or MRI) to confirm the presence of brain tissue damage;30 using the most widely used natriuretic peptide biomarker NT proBNP in European clinical practice for the diagnosis of HF;31 if the electrocardiogram showed disappearance of sinus P waves and replacement with irregular f waves, and absolute irregularity of RR intervals, the diagnosis was AF;32 angina pectoris needed to be diagnosed through a combination of clinical symptoms, auxiliary examinations, and exclusion of ischemic chest pain; the diagnosis of MI should followed the globally unified dual criteria of myocardial injury and evidence of myocardial ischemia, combined with clinical symptoms, biomarkers, electrocardiogram, and imaging examinations for comprehensive judgment.33 The above results were diagnosed by professional medical staff and the authenticity of the data was guaranteed.
Confounding Factor
The gender and age of the researchers were reported as baseline data. Selected a population with a baseline age of 40~70 years old. The Townsend Deprivation Index (TDI) refered to a standardized tool for measuring the degree of material deprivation based on geographic regions, where the numerical value directly reflected the level of material scarcity in an individual’s region,34 divided into lower, middle and higher school groups based on quartiles. Anthropometric assessments were measured by trained nurses using standard procedures as well as calibrated equipment. Body mass index (BMI) was calculated as (weight in kg)/(height in m)2. Based on the baseline self-report of education level, participants were divided into 6 groups according to the reporting situation. Smoking status was divided into never, previous, and current. One standard drink of alcohol consumption was defined as 8 g (10 mL) of alcohol. The method for calculating weekly alcohol consumption was detailed in a prior UKB study.35 The total sedentary time was defined as the sum of daily TV watching, leisure computer use, and driving time (hours/day) in self-reported data. The frequency of intake of processed meat was divided into once or more daily; 5–6 times a week; 2–4 times a week; once a week; less than once a week and never. The use of cardiovascular drugs, including antihypertensive drugs, lipid-lowering drugs, and blood glucose control drugs, was defined as the used or using. Other drugs unrelated to CVD were not included.
Statistical Analyses
The characteristics of the cohort were summarized as mean and standard deviation (SD) for continuous variables, and frequency and percentage (%) for categorical variables. Due to the fact that alcohol intake was a non-normally distributed continuous variable, median and quartiles were used for description. Given the significant intergroup baseline differences identified via homogeneity testing (P<0.05), propensity score matching was deemed unsuitable for this analysis due to concerns over excessive data loss and reduced statistical power. Therefore, we employed a multivariate Cox proportional hazards regression model, supplemented by subgroup analyses, to rigorously control for potential confounding factors. The associations were investigated using Cox proportional hazard models and were reported as hazard ratio (HR) together with 95% confidence intervals (95% CIs).
Two gradually adjusted models were used to correct confounding factors: minimum correction model (model 1) adjusted for age, sex, TDI and education qualifications; fully corrected model (model 2) further adjusted processed meat intake, smoking status, alcohol intake, total sedentary time and Cardiovascular drugs on the basis of model 1; sensitivity analysis (model 3) additionally adjusted BMI based on model 2. All analyses were conducted with the non-sleep disorders group as the reference group.
Further validation of the association between sleep disorder patients and newly developed CVD using subgroup analysis: strong confounding factors were identified through previous studies and subjected to subgroup analysis. By reducing the confounding effect of covariates in each group, we once again strongly validated the association between sleep disorders and cardiovascular outcomes in COPD patients. Among them, sex was divided into male and female according to the data in the baseline report. Age was divided into two groups: 40–60 and >60. Use of cardiovascular drugs and smoking status were the same as the grouping mentioned above. The grouping of cardiovascular drug use was yes and no. Smoking status was grouped into never, previous, and current. According to the internationally recognized BMI classification standards, BMI was divided into lean (BMI<18.5), normal (18.5–24.9), overweight (25–29.9), and obese (≥30).36
Statistical analysis was conducted using R 4.5.0 software, with a two-tailed P<0.05 indicating statistically significant differences.
Results
Baseline Characteristics of the Study Population
A total of 23804 participants with COPD had data. After excluding the subjects with missing baseline data, 21423 samples were ultimately included in this study (Table 1). UKB enrolled participants between 2006 and 2010. Baseline assessments commenced in April 2007 and concluded in July 2010. In the present study, the observational period was defined as the interval from the diagnosis of sleep disorders to the first incidence of adverse cardiovascular events among patients with COPD. The date of diagnosis was provided by UKB. For participants without subsequent adverse cardiovascular events, the follow-up period was censored on December 31, 2024. During the follow-up period, a total of 5 CVDs were recorded. Among them, 951 cases of stroke occurred; 2631 cases of HF; 3611 cases of AF; 2040 cases of angina; 1352 cases of MI. The mean age was 60.4±6.7 years and 50.3% were men. Compared with sleep disorder group, non-sleep disorder group had a higher proportion of males, higher levels of socioeconomic deprivation, longer sitting time, higher BMI, and higher rates of cardiovascular drug use. In addition, we can observe that the population with the highest TDI among sleep disorder patients had the highest proportion (37.5%), and the population with the lowest education level had the highest proportion (34.2%). Among individuals with sleep disorders group, only 1.3% consumed processed meat daily, while the rest consumed it less frequently.
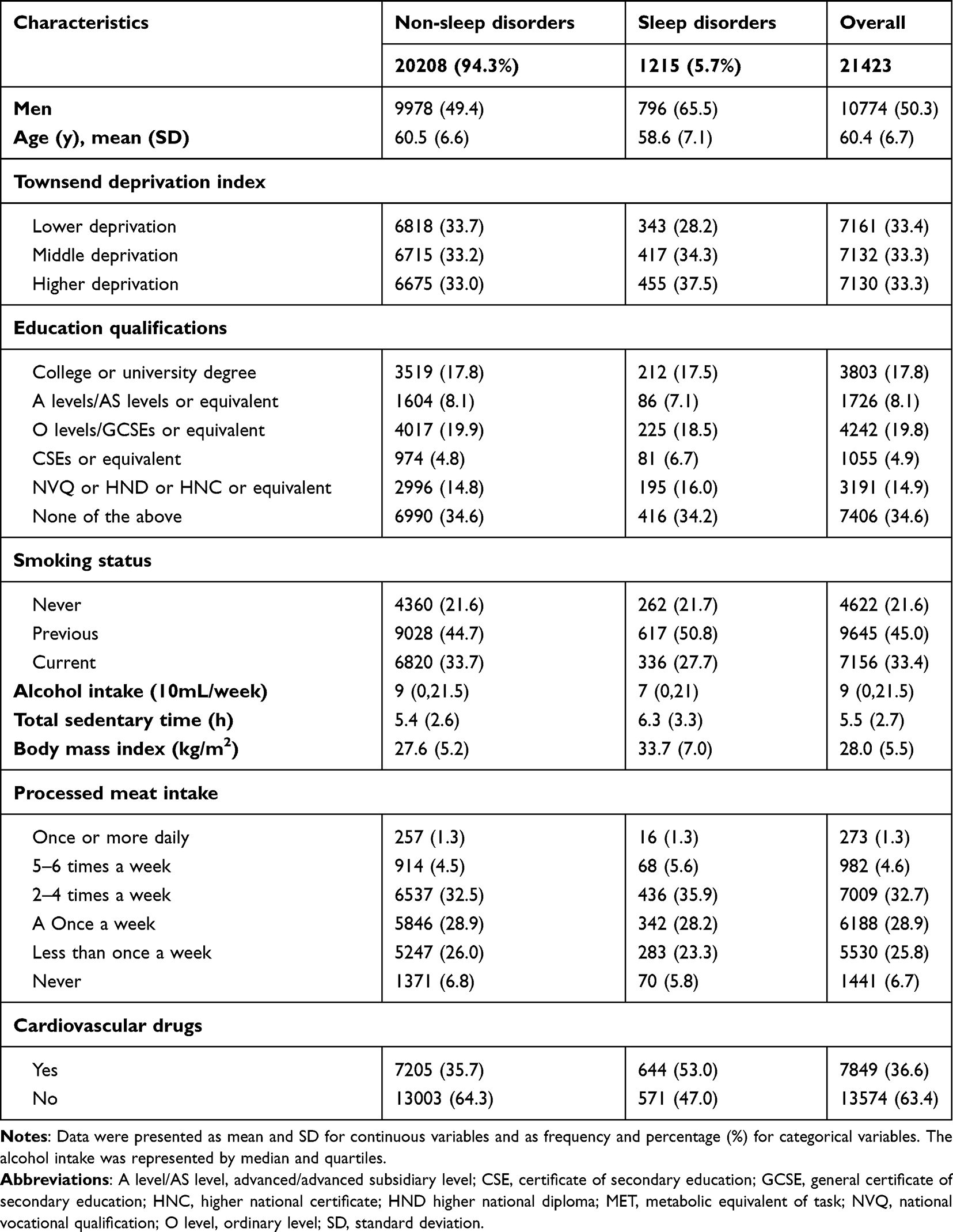 |
Table 1 Cohort Characteristics by Sleep Disorders |
The Association Between Sleep Disorders and Outcome Events
The findings from the multivariate Cox regression model were presented as follows (Figure 2). In the analysis of sleep disorders and stroke, no statistically significant association was observed. Regarding HF, the sleep disorder group showed an elevated hazard compared to the non-sleep disorder group. In model 1, the HR was 2.51 (HR = 2.51, 95% CI: 2.23–2.83). After full adjustment in model 2, the association remained statistically significant (HR = 2.35, 95% CI: 2.08–2.66), reflecting a 135% relative increase in hazard. Model 3 further confirmed this association (HR = 1.79, 95% CI: 1.57–2.03), reflecting a 79% relative increase. For AF, the sleep disorder group was also associated with an elevated hazard. Model 1 reflected an 85% relative increase in hazard (HR = 1.85, 95% CI: 1.65–2.07). After comprehensive covariate adjustment in model 2, the estimate decreased but remained statistically significant (HR = 1.75, 95% CI: 1.56–1.97). Model 3 indicated an association reflecting a 49% relative increase (HR = 1.49, 95% CI: 1.32–1.68). In terms of angina, the sleep disorder group showed an association reflecting a 72% relative increase in hazard in model 1 (HR = 1.72, 95% CI: 1.48–1.99). Following full adjustment in model 2, the estimate was attenuated, reflecting a 55% relative increase (HR = 1.55, 95% CI: 1.33–1.80). Model 3 confirmed a persistent association (HR = 1.44, 95% CI: 1.23–1.68). For MI, in model 1, the sleep disorder group showed an association reflecting a 30% relative increase in hazard (HR = 1.30, 95% CI: 1.06–1.59). In model 2, the estimate reflected a 28% relative increase (HR = 1.28, 95% CI: 1.04–1.57). In model 3, the association reflected a 24% relative increase (HR = 1.24, 95% CI: 1.01–1.54).
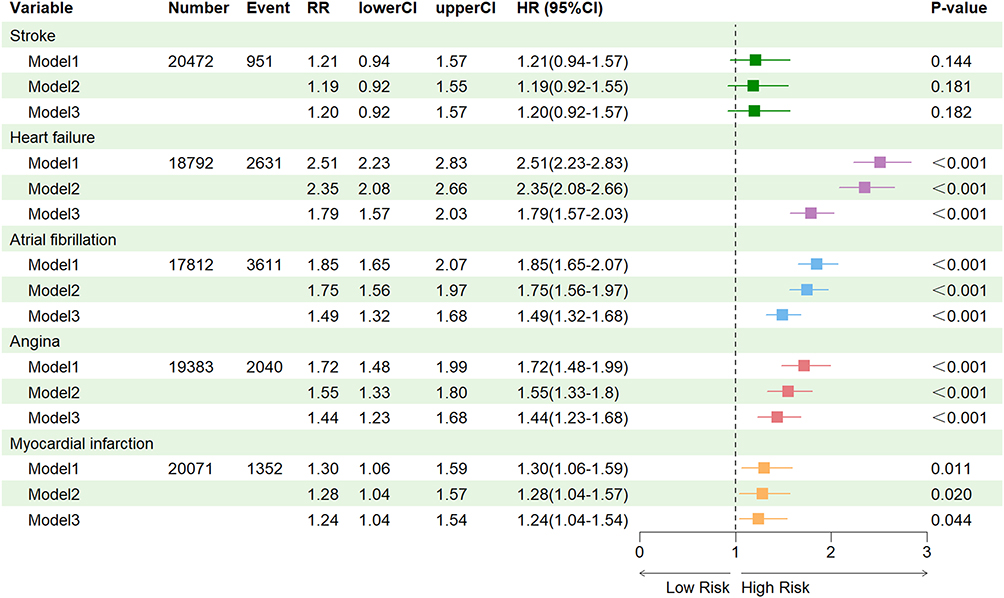 |
Figure 2 Results of Multivariate Cox Regression Analysis. |
Subgroup Analysis results
Prior to subgroup analysis, the five individual CVD outcomes were aggregated into a composite CVD endpoint (n=6476) (Figure 3). Across gender subgroups, participants with sleep disorders showed an association with elevated CVD hazard compared to those without. Specifically, among males, the sleep disorder group showed an association reflecting a 52% relative increase in CVD hazard (HR = 1.52, 95% CI: 1.37–1.70). Among females, the sleep disorder group was also associated with an elevated CVD hazard (HR = 1.74, 95% CI: 1.49–2.04). These associations were statistically significant (P < 0.001). Moreover, the association appeared stronger in males than in females, with a HR of 1.36 (95% CI: 1.29–1.43) for the male-to-female comparison. The association between sleep disorders and CVD hazard was observed across age subgroups. Specifically, among participants aged 40–60 years, the sleep disorder group showed an association reflecting a 52% relative increase in hazard (HR = 1.52, 95% CI: 1.32–1.74). Among participants aged >60 years, the association reflected a 57% relative increase in hazard (HR = 1.57, 95% CI: 1.40–1.76). In the comparison between age subgroups, the HR for participants aged >60 versus 40–60 years was 1.59 (95% CI: 1.51–1.68). Stratified by cardiovascular medication use, the association between sleep disorders and CVD hazard was observed among both users (HR = 1.58, 95% CI: 1.37–1.81) and non-users (HR = 1.57, 95% CI: 1.40–1.77). In the comparison between medication subgroups, participants using cardiovascular medications showed a HR of 1.34 (95% CI: 1.28–1.41) relative to non-users. Moreover, smoking status appeared to modify the association between sleep disorders and CVD hazard. Among never-smokers, the sleep disorder group showed an association reflecting a 47% relative increase in hazard (HR = 1.47, 95% CI: 1.19–1.80). Among former smokers, the association reflected a 61% relative increase in hazard (HR = 1.61, 95% CI: 1.43–1.82), and among current smokers, a 60% relative increase was observed (HR = 1.60, 95% CI: 1.36–1.90). In the comparison across smoking subgroups, the HR for ever-smokers versus never-smokers was 1.12 (95% CI: 1.08–1.16). Regarding BMI, associations were observed across categories: among participants with BMI 25–29.9, the sleep disorder group showed an association reflecting a 47% relative increase in hazard (HR = 1.47, 95% CI: 1.23–1.76). Among participants with BMI ≥30, the association reflected a 75% relative increase in hazard (HR = 1.75, 95% CI: 1.58–1.95). In the continuous analysis of BMI, each unit increase was associated with a 15% relative increase in CVD hazard (HR = 1.15, 95% CI: 1.12–1.19). These HRs denote relative association measures rather than absolute clinical risks; thus, subgroup results should be interpreted with caution.
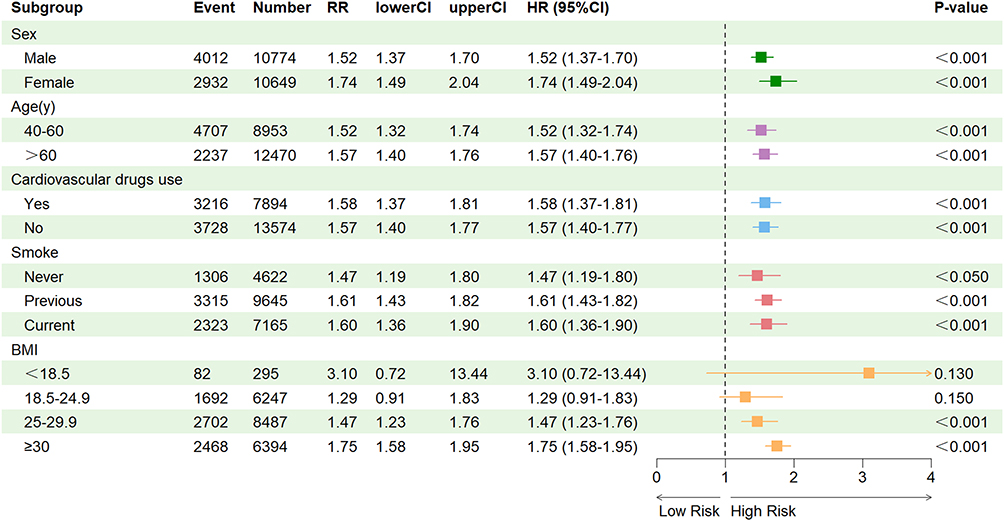 |
Figure 3 Subgroup analysis results. |
Discussion
The main finding of this study was that sleep disorders were associated with an elevated hazard of composite CVD, HF, AF, angina and MI in COPD patients, independent of sociodemographic and lifestyle factors. Subgroup analyses further demonstrated that, after comprehensive adjustment, this association persisted across diverse patient profiles. The results of this manuscript were consistent with a previous study that found an association between sleep disorders and CVD.37,38
Notably, however, no statistically significant association was observed for stroke. This null finding warranted careful consideration. First, the relatively lower incidence of stroke compared to other CVD outcomes in our cohort may have reduced statistical power to detect a modest association. Second, stroke was mainly caused by cerebral vascular atherosclerosis, embolism or vascular rupture, leading to the interruption or leakage of brain blood flow, resulting in cerebral ischemia, hypoxia, edema and neuronal damage.39 Chronic intermittent hypoxia and systemic inflammation might exert more direct effects on myocardial structure, coronary endothelium, and atrial electrophysiology than on cerebral vessels.40–42 These factors highlighted the complexity of cerebrovascular risk in COPD and suggested that stroke might require longer follow-up or distinct mechanistic pathways to manifest.
Under the combined effect of multiple factors such as accelerated social development, changes in residents’ lifestyles, and uneven levels of health awareness, the number of global sleep disorder patients had shown a significant upward trend.43 Among them, the sustained psychological pressure caused by high-intensity occupational competition due to political issues such as Brexit and the suppression of melatonin secretion caused by frequent use of electronic devices before bedtime were the core triggers for inducing sleep rhythm disorders.44–46 It was worth noting that the fluctuations in health-related indicators such as abnormal BMI and excessive alcohol consumption caused by differences in socio-economic development, changes in behavioral habits, and changes in the ecological environment were not only closely related to the occurrence and development of sleep disorders, but also important risk factors for various chronic diseases such as CVDs and metabolic diseases.47,48 The selection of sleep disorders as the theme for discussion not only aimed to explore the aforementioned public health hot issues, but also considered that their association with cardiovascular disease outcomes might be mediated through multiple biological pathways. It had found that intermittent hypoxia resulting from sleep disorders can directly damage the vascular endothelium and promote atherosclerosis via activation of the sympathetic nervous system, oxidative stress, and inflammatory responses.49,50 Chronic systemic inflammation could exacerbate vascular damage and increase the risk of cardiovascular events and sleep disorders were often accompanied by metabolic disorders such as insulin resistance and dyslipidemia and were also important risk factors for cardiovascular disease.17,51,52 In summary, this manuscript chose sleep disorders as the theme for exploration and rigorously evaluated related confounding factors.
It was necessary to elaborate on the advantages of this manuscript. This manuscript explored for the first time the impact of sleep disorders on the risk of CVD outcomes in COPD patients. Elaborated in detail the impact of sleep disorders on the risk of five outcomes: stroke, HF, AF, angina and MI. To ensure the scientific validity and reliability of the study, we conducted subgroup analysis of confounding factors based on the association between sleep disorders and cardiovascular outcomes previously mentioned in this manuscript and the following studies. A study comparing white males and females had found that males had significantly higher CVD mortality rates than females, and smoking was a significant exposure factor.53 Spencer J et al’s study confirmed that smoking was an important confounding factors affecting the quality of life of COPD patients.54 BMI was also a hot topic in current research on CVD. Previous studies had confirmed a significant association between BMI and CVD outcomes in COPD patients.55–57 Therefore, this manuscript further conducted subgroup analysis from five aspects: age, gender, BMI, smoking status and cardiovascular drugs use.58 In addition, using internationally recognized diagnostic methods to group patients results in high diagnostic accuracy.
Nevertheless, some limitations need to be considered when interpreting our results. Firstly, the research subjects were only white Europeans, and the results may not be generalizable to other races. Further exploration and research were needed on the CVD risk of COPD patients based on different ethnicities. Affected by the actual disease incidence, the final dataset of this study contained far more participants without sleep disorders than those with sleep disorders, and the homogeneity test yielded a significant difference at P<0.05. Even though multivariate Cox regression and subgroup analyses were performed to mitigate the effects of sample imbalance, a larger sample size was still needed for further validation. Although several established confounding variables were adjusted for in this study, certain potential confounders remained unmeasured. Relevant examples included medication use and lifestyle factors that were not recorded in the dataset, and these factors might have affected the study outcomes.59 In addition, both the clinical course of COPD and its exacerbations might have influenced the clinical outcomes. However, a discrepancy existed between the recorded COPD diagnosis time in the UKB dataset and the actual disease onset time of the enrolled patients. Furthermore, lung function parameters, such as predicted FEV1% and COPD disease staging information, were not incorporated into the current analysis; therefore, the potential impact of COPD severity on the association between sleep disorders and cardiovascular outcomes could not be adequately assessed. Therefore, this factor needed to be verified separately.60,61 The definition of sleep disorders in this study was mainly based on questionnaire self-assessments or diagnostic records, and different subtypes of sleep disorders (such as obstructive sleep apnea, insomnia) were not distinguished. The magnitude and underlying mechanisms of the associations with cardiovascular disease differed across sleep disorder subtypes.59 The statistical results of the association between sleep disorders and stroke risk in patients with COPD were not significant, which might be due to the small sample size. Data limitations prevented robust comparisons between the group with BMI less than 18.5 and those with BMI between 18.5–24.9. These issues require further in-depth exploration.
In conclusion, this prospective cohort study observed a significant association between sleep disorders and adverse cardiovascular outcomes in patients with COPD, with potentially stronger associations noted in males, individuals with high body weight, smokers, and those with prior cardiovascular medication use. Individuals in these high-risk subgroups, particularly those presenting with symptoms suggestive of sleep disorders such as snoring, daytime sleepiness, nocturnal hypoxia, and morning headaches, may benefit from comprehensive, targeted screening for sleep disturbances. If sleep disorders are identified, multidisciplinary management involving respiratory and sleep medicine specialists, with tailored interventions aligned with the specific sleep disorder subtype, may help optimize the overall care of COPD and potentially improve long-term outcomes. From a public health perspective, such targeted screening in high-risk groups may facilitate early detection and management of modifiable risk factors for adverse cardiovascular outcomes, with the potential to reduce secondary cardiovascular events in patients with COPD, alleviate individual disease burden, and lower the societal healthcare burden associated with cardiovascular complications. These findings highlight the need for future clinical trials to evaluate whether interventions for sleep disorders can reduce cardiovascular risk in COPD patients.
Data Sharing Statement
The UK Biobank resource is accessible to researchers upon application via https://www.ukbiobank.ac.uk.
Ethics Approval and Consent to Participate
This study was a retrospective analysis, with data sourced from patients diagnosed with COPD in the UK Biobank database between 2006 and 2024. This study is based on an approved UK Biobank application (Application Number: 280417). This study was an observational study and no intervention measures were taken on the patients. All patients participating in this study provided informed consent, and informed consent forms can be obtained from the UK Biobank (www.ukbiobank.ac.uk). The UK Biobank study received ethical approval from the North West Research Ethics Committee (Ref. Nos. 11/NW/0382 and 21/NW/0157). The utility of UK Biobank data was approved by the ethics committee of The First Affiliated Hospital of Anhui Medical University (Approval No. PJ 2024-13-46).
Consent for Publication
The authors of this manuscript agree to the public publication of the article.
Acknowledgments
Thank you to all the patients who participated in this manuscript, as well as the authors who completed the manuscript creation. We attest that the article is the Authors’ original work, has not received prior publication and is not under consideration for publication elsewhere.
Funding
This study was supported by grants from the Open Fund Project of Anhui Provincial Laboratory for Inflammatory Immune Diseases (IMMDL202405) and Anhui Provincial Department of Science and Technology (Grants 202427b10020101), research on a new strategy for atrial fibrillation ablation under full three-dimensional radioless guidance.
Disclosure
Xian An and Yuting Chen are co-first authors for this study. The authors report no relationships that could be construed as a conflict of interest.
References
1. Calverley PMA, Walker PP. Contemporary Concise Review 2022: chronic obstructive pulmonary disease. Respirology. 2023;28(5):428–12. doi:10.1111/resp.14489
2. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020-50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11(8):e1183–e1193. doi:10.1016/S2214-109X(23)00217-6
3. Mannino DM, Tal-Singer R. Long-term trends of COPD mortality: gaps and opportunities. Respirology. 2022;27(11):914–915. doi:10.1111/resp.14334
4. Kahnert K, Jorres RA, Behr J, et al. The Diagnosis and Treatment of COPD and Its Comorbidities. Dtsch Arztebl Int. 2023;120(25):434–444. doi:10.3238/arztebl.m2023.027
5. Maclagan LC, Croxford R, Chu A, et al. Quantifying COPD as a risk factor for cardiac disease in a primary prevention cohort. Europ resp J. 2023;62(2):2202364. doi:10.1183/13993003.02364-2022
6. Amegadzie JE, Sadatsafavi M. A long overdue recognition: COPD as a distinct predictor of cardiovascular disease risk. Europ resp J. 2023;62(2):2301167. doi:10.1183/13993003.01167-2023
7. Rabe KF, Hurst JR, Suissa S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. 2018;27(149):180057.
8. Cho EE, Maclagan LC, Chu A, et al. Impact of COPD on cardiovascular risk factors and outcomes in people with established cardiovascular disease. Thorax. 2025;80(5):291–299. doi:10.1136/thorax-2023-220991
9. Cobb K, Kenyon J, Lu J, et al. COPD is associated with increased cardiovascular disease risk independent of phenotype. Respirology. 2024;29(12):1047–1057. doi:10.1111/resp.14799
10. Scaramuzzo G, Ottaviani I, Volta CA, et al. Mechanical ventilation and COPD: from pathophysiology to ventilatory management. Minerva medica. 2022;113(3):460–470. doi:10.23736/S0026-4806.22.07974-5
11. Xu J, Zeng Q, Li S, et al. Inflammation mechanism and research progress of COPD. Front Immunol. 2024;151404615.
12. Sampol J, Miravitlles M, Sáez M, et al. Poor sleep quality, COPD severity and survival according to CASIS and Pittsburgh questionnaires. Sci Rep. 2023;13(1):18656. doi:10.1038/s41598-023-45717-9
13. Koulouris N, Dimakou K, Gourgoulianis K, et al. Self-perceived quality of sleep among COPD patients in Greece: the SLEPICO study. Sci Rep. 2022;12(1):540. doi:10.1038/s41598-021-04610-z
14. Li H, Yang J, Xiao Q, et al. Global prevalence of COPD-OSA overlap syndrome: a systematic review and meta-analysis. Sleep Med. 2025;135106766.
15. Clímaco DCS, Lustosa TC, Silva MVDF, et al. Sleep quality in COPD patients: correlation with disease severity and health status. J Bras Pneumol. 2022;48(3):e20210340. doi:10.36416/1806-3756/e20210340
16. Redline S, Azarbarzin A, Peker Y. Obstructive sleep apnoea heterogeneity and cardiovascular disease. Nat Rev Cardiol. 2023;20(8):560–573.
17. Aksakal A, Kerget B, Özkan HB, et al. Serum asprosin levels in obstructive sleep apnea syndrome: relationship with disease severity and adipose tissue distribution. Sleep Breath. 2026;30(1):18. doi:10.1007/s11325-025-03567-x
18. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;144(3):e56–e67. doi:10.1161/CIR.0000000000000988
19. van Zeller M, Mcnicholas WT. Sleep disordered breathing: OSA-COPD overlap. Expert Rev Respir Med. 2024;18(6):369–379. doi:10.1080/17476348.2024.2373790
20. Korostovtseva L, Bochkarev M, Sviryaev Y. Sleep and cardiovascular risk. Sleep Med Clinics. 2021;16(3):485–497.
21. Diao T, Liu K, Lyu J, et al. Changes in sleep patterns, genetic susceptibility, and incident cardiovascular disease in China. JAMA Network Open. 2024;7(4):e247974. doi:10.1001/jamanetworkopen.2024.7974
22. Figueiro MG, Pedler D. Cardiovascular disease and lifestyle choices: spotlight on circadian rhythms and sleep. Prog Cardiovasc Diseases. 2023;7770–7777.
23. Jaspan VN, Greenberg GS, Parihar S, et al. The role of sleep in cardiovascular disease. Curr Atherosclerosis Rep. 2024;26(7):249–262.
24. Huang B, Duncan MJ, Cistulli PA, et al. Sleep and physical activity in relation to all-cause, cardiovascular disease and cancer mortality risk. Br J Sports Med. 2022;56(13):718–724.
25. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
26. World Health Organization. International Classification of Diseases.
27. Chung F, Abdullah HR, Liao P. STOP-Bang Questionnaire: a practical approach to screen for obstructive sleep apnea. Chest. 2016;149(3):631–638. doi:10.1378/chest.15-0903
28. Guo Q, Song W, Li W, et al. Weighted Epworth sleepiness scale predicted the apnea-hypopnea index better. Respir Res. 2020;21(1):147.
29. Krishnan S, Tan WC, Farias R, et al. Impaired spirometry and COPD increase the risk of cardiovascular disease: a Canadian Cohort Study. Chest. 2023;164(3):637–649. doi:10.1016/j.chest.2023.02.045
30. Walter K. What Is Acute Ischemic Stroke? JAMA. 2022;327(9):885. doi:10.1001/jama.2022.1420
31. Bayes-Genis A, Docherty KF, Petrie MC, et al. Practical algorithms for early diagnosis of heart failure and heart stress using NT-proBNP: a clinical consensus statement from the Heart Failure Association of the ESC. Eur J Heart Fail. 2023;25(11):1891–1898. doi:10.1002/ejhf.3036
32. Falk RH. Atrial fibrillation. N Engl J Med. 2001;344(14):1067–1078. doi:10.1056/NEJM200104053441407
33. Guzik TJ, Mohiddin SA, Dimarco A, et al. COVID-19 and the cardiovascular system: implications for risk assessment, diagnosis, and treatment options. Cardiovasc Res. 2020;116(10):1666–1687. doi:10.1093/cvr/cvaa106
34. Khurshid S, Al-Alusi MA, Churchill TW, et al. Accelerometer-derived “weekend warrior” physical activity and incident cardiovascular disease. JAMA. 2023;330(3):247–252. doi:10.1001/jama.2023.10875
35. Tu SJ, Gallagher C, Elliott AD, et al. Risk thresholds for total and beverage-specific alcohol consumption and incident atrial fibrillation. JACC Clin Electrophysiol. 2021;7(12):1561–1569. doi:10.1016/j.jacep.2021.05.013
36. Mehran L, Mousapour P, Khalili D, et al. BMI variability and incident diabetes mellitus, Tehran Lipid and Glucose Study (TLGS). Sci Rep. 2022;12(1):18370. doi:10.1038/s41598-022-22817-6
37. Li Y, Li F, Wang G, et al. Additive impact of chronic obstructive pulmonary disease (COPD) and cardiovascular disease(CVD) on all-cause and disease-Specific mortality: a longitudinal nationwide population-based study. BMC Pulm Med. 2025;25(1):275.
38. Polman R, Hurst JR, Uysal OF, et al. Cardiovascular disease and risk in COPD: a state of the art review. Expert Rev Cardiovasc Ther. 2024;22(4–5):177–191. doi:10.1080/14779072.2024.2333786
39. Zhao Y, Zhang X, Chen X, et al. Neuronal injuries in cerebral infarction and ischemic stroke: from mechanisms to treatment (Review). Int J Mol Med. 2022;49(2):15. doi:10.3892/ijmm.2021.5070
40. Lin CW, Li JY, Kuo TBJ, et al. Chronic intermittent hypoxia worsens brain damage and sensorimotor behavioral abnormalities after ischemic stroke: effect on autonomic nervous activity and sleep patterns. Brain Res. 2023;1798:148159. doi:10.1016/j.brainres.2022.148159
41. Wei Q, Xu X, Chen L, et al. Effects of chronic intermittent hypoxia on left cardiac function in young and aged mice. Am J Physiol Regul Integr Comp Physiol. 2022;322(3):R241–R252. doi:10.1152/ajpregu.00256.2021
42. Onuki K, Ikeda A, Muraki I, et al. Nocturnal intermittent hypoxia and the risk of cardiovascular disease among Japanese populations: the circulatory risk in communities study (CIRCS). J Atheroscleros Thrombos. 2023;30(9):1276–1287. doi:10.5551/jat.63754
43. Sun S, Chen G. Treatment of circadian rhythm sleep-wake disorders. Curr Neuropharmacol. 2022;20(6):1022–1034. doi:10.2174/1570159X19666210907122933
44. Cecere L, de Novellis S, Gravante A, et al. Quality of life of critical care nurses and impact on anxiety, depression, stress, burnout and sleep quality: a cross-sectional study. Intensive Critical Care Nurs. 2023;79103494.
45. Zheng NS, Annis J, Master H, et al. Sleep patterns and risk of chronic disease as measured by long-term monitoring with commercial wearable devices in the all of us research program. Nature Med. 2024;30(9):2648–2656. doi:10.1038/s41591-024-03155-8
46. Dibben GO, Martin A, Shore CB, et al. Adolescents’ interactive electronic device use, sleep and mental health: a systematic review of prospective studies. J Sleep Res. 2023;32(5):e13899. doi:10.1111/jsr.13899
47. Wei S, Nguyen TT, Zhang Y, et al. Sarcopenic obesity: epidemiology, pathophysiology, cardiovascular disease, mortality, and management. Front Endocrinol. 2023;141185221.
48. Duell PB, Welty FK, Miller M, et al. Nonalcoholic fatty liver disease and cardiovascular risk: a scientific statement from the American Heart Association. Arterioscleros Thrombos Vasc Biol. 2022;42(6):e168–e185. doi:10.1161/ATV.0000000000000153
49. Arnaud C, Billoir E, de Melo Junior AF, Pereira SA, O’Halloran KD, Monteiro EC. Chronic intermittent hypoxia-induced cardiovascular and renal dysfunction: from adaptation to maladaptation. J Physiology. 2023;601(24):5553–5577. doi:10.1113/JP284166
50. Xue J, Allaband C, Zuffa S, et al. Gut microbiota and derived metabolites mediate obstructive sleep apnea induced atherosclerosis. Gut Microbes. 2025;17(1):2474142. doi:10.1080/19490976.2025.2474142
51. Yang DF, Huang WC, Wu CW, Huang CY, Yang YSH, Tung YT. Acute sleep deprivation exacerbates systemic inflammation and psychiatry disorders through gut microbiota dysbiosis and disruption of circadian rhythms. Microbiol Res. 2023;268:127292. doi:10.1016/j.micres.2022.127292
52. Feeney SP, McCarthy JM, Petruconis CR, Tudor JC. Sleep loss is a metabolic disorder. Sci Signal. 2025;18(881):eadp9358. doi:10.1126/scisignal.adp9358
53. Krishnan JK, Rajan M, Banerjee S, et al. Race and sex differences in mortality in individuals with chronic obstructive pulmonary disease. Ann Am Thoracic Soc. 2022;19(10):1661–1668. doi:10.1513/AnnalsATS.202112-1346OC
54. Keene SJ, Driessen JHM, Jordan RE, et al. The independent and combined effects of smoking and chronic obstructive pulmonary disease on body mass index trajectories. Sci Rep. 2025;15(1):32883. doi:10.1038/s41598-025-17270-0
55. Chen R, Cai Y, Chen Q, et al. The association between the BRI and all-cause and cardiovascular mortality in COPD patients. BMC Pulm Med. 2025;25(1):420. doi:10.1186/s12890-025-03868-7
56. Holtjer JCS, Bloemsma LD, Beijers RJHC, et al. Identifying risk factors for COPD and adult-onset asthma: an umbrella review. Eur Respir Rev. 2023;32(168):230009. doi:10.1183/16000617.0009-2023
57. Zhou J, Liu Y, Yang F, et al. Risk factors of sarcopenia in COPD patients: a meta-analysis. Int J Chronic Obstr. 2024;191613–191622.
58. Chen W, Thomas J, Sadatsafavi M, et al. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(8):631–639. doi:10.1016/S2213-2600(15)00241-6
59. Carneiro-Barrera A, Amaro-Gahete FJ, Guillén-Riquelme A, et al. Effect of an interdisciplinary weight loss and lifestyle intervention on obstructive sleep apnea severity: the INTERAPNEA randomized clinical trial. JAMA Network Open. 2022;5(4):e228212. doi:10.1001/jamanetworkopen.2022.8212
60. Singh D, Martinez FJ, Hurst JR, et al. Effect of triple therapy on cardiovascular and severe cardiopulmonary events in chronic obstructive pulmonary disease: a post hoc analysis of a randomized, double-blind, phase 3 clinical trial (ETHOS). Am J Respir Crit Care Med. 2025;211(2):205–214. doi:10.1164/rccm.202312-2311OC
61. Yang H, Ryu MH, Carey VJ, et al. Differential association of COPD subtypes with cardiovascular events and COPD exacerbations. Chest. 2024;166(6):1360–1370. doi:10.1016/j.chest.2024.07.148
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.