Back to Journals » International Journal of General Medicine » Volume 13
Association Between Serum Calcium and Phosphorus Levels and Insulin-Like Growth Factor-1 in Chinese Children and Adolescents with Short Stature
Authors Sun M, Yan W, Zhao Q, Ji B, Ban B ![]() , Zhang M
, Zhang M
Received 19 August 2020
Accepted for publication 30 October 2020
Published 17 November 2020 Volume 2020:13 Pages 1167—1173
DOI https://doi.org/10.2147/IJGM.S276261
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Minghui Sun,1 Wenhua Yan,2,3 Qianqian Zhao,2,3 Baolan Ji,2,3 Bo Ban,2,3 Mei Zhang2,3
1Department of Clinical Medicine, Jining Medical University, Jining, Shandong 272067, People’s Republic of China; 2Department of Endocrinology, Affiliated Hospital of Jining Medical University, Jining Medical University, Jining, Shandong 272029, People’s Republic of China; 3Chinese Research Center for Behavior Medicine in Growth and Development, Jining, Shandong 272029, People’s Republic of China
Correspondence: Mei Zhang
Department of Endocrinology, Affiliated Hospital of Jining Medical University, Jining Medical University, 89 Guhuai Road, Jining, Shandong 272029, People’s Republic of China
Tel +86-0537-2903690
Email [email protected]
Bo Ban
Chinese Research Center for Behavior Medicine in Growth and Development, 89 Guhuai Road, Jining, Shandong 272029, People’s Republic of China
Email [email protected]
Objective: The aim of this study was to investigate the effect of serum calcium and phosphorus levels on the insulin-like growth factor 1 (IGF-1) in Chinese children and adolescents with short stature.
Methods: In this cross-sectional analysis, the clinical data of 747 children with height below – 2 SD who were evaluated at the Department of Endocrinology, Affiliated Hospital of Jining Medical University from March 1, 2013, to February 28, 2019, were selected. Anthropometric and biochemical indicators were measured. The relationship between the serum calcium and phosphorus levels and IGF-1 was analysed.
Results: The univariate analysis results showed that serum calcium or phosphorus was significantly associated with IGF-1 SDS. In addition, after adjusting for possible confounding factors, a linear relationship between serum calcium and IGF-1 SDS and a non-linear relationship between serum phosphorus and IGF-1 SDS were observed by smooth curve fitting. The results of the fully adjusted linear regression showed that serum calcium was positively associated with IGF-1 SDS (β 1.07, 95% CI 0.21, 1.92; p = 0.015). In the multivariate piecewise linear regression, when the serum phosphorus level was greater than 1.26 mmol/L, the IGF-1 SDS increased with the increase in serum phosphorus (β 1.92, 95% CI 1.36, 2.48; p < 0.001). However, we did not observe a significant relationship when the serum phosphorus level was less than 1.26 mmol/L (p = 0.223).
Conclusion: This study demonstrated that in Chinese children and adolescents with short stature, circulating calcium and phosphorus concentrations may be associated with the regulation of IGF-1 levels, and this relationship merits further investigation.
Keywords: calcium, phosphorus, IGF-1, short stature
Introduction
The definition of short stature is based on statistics, assuming that the normal values for the specific population are within the range of ±2 standard deviations (SDs), adjusted for sex and age. A child whose height is below −2SD is considered to be of short stature.1,2 Growth hormone (GH) and growth hormone receptors (GHRs) combine to activate the JAK-STAT signalling pathway and then stimulate the synthesis and secretion of insulin-like growth factor 1 (IGF-1) from the liver and other tissues.3,4 IGF-1 concentrations are low in growth hormone-deficient (GHD) patients, and there are also reports that low concentrations of IGF-1 are still observed in some children with idiopathic short stature who have normal GH levels.5
IGF-1 can promote bone formation by causing differentiation and regeneration of epiphyseal chondrocytes and can also effectively promote bone metabolism.6 Schlechter et al believe that IGF-l has a direct growth-promoting effect on long bones.7 IGF-1 in bone enhances the osteoblastic function of osteoblasts by stimulating osteoblast proliferation, thereby promoting bone mineralization.8 The main factors affecting liver synthesis and release of IGF-1 are GH, insulin, nutritional status, and IGF-binding protein.9,10
Calcium and phosphorus are both important components of the bone mineral phase. Previous studies on serum calcium and phosphorus levels have mainly focused on cardiovascular disease and chronic kidney disease.11,12 There are few studies on the correlation between IGF-1 and serum calcium and phosphorus levels. A review based on 14 reports summarizing the clinical effects of IGF-1 administration found that IGF-1 increases bone resorption and bone formation; therefore, there also may be a potential interaction between calcium and IGF1 in bone metabolism.13 Cross-sectional data from the third US Health and Nutrition Examination Survey (NHANES III) showed an overall positive correlation between circulating levels of IGF-1 and IGFBP3 and serum calcium.14 Several studies have shown that GH treatment can increase serum phosphorus levels in patients with X-linked hypophosphatemia (XLH).15,16 The increase in glomerular filtration rate and proximal convoluted tubular phosphate transport caused by GH may be mediated by IGF-1.17 In other words, the increase of serum phosphorus level after GH treatment may be related to IGF-1 in XLH population. Until now, the association between IGF-1 levels and serum calcium and phosphorus concentrations in children with short stature has not been studied. The aim of this study was to examine the relationship between IGF-1 and serum calcium and phosphorus levels in Chinese children and adolescents with short stature.
Subjects and Methods
Study Subjects
The subjects were enrolled from cohort GDDSD study (Growth and Development Diseases in Shandong Province: a cohort follow-up study, http://www.chictr.org.cn, ChiCTR1900026510). We reviewed the medical records of short stature children and adolescents who were evaluated at the Department of Endocrinology, Affiliated Hospital of Jining Medical University, between March 1, 2013, and February 28, 2019, and conducted a cross-sectional analysis. The inclusion criteria were as follows: the individual’s height below –2 SD in the normal population with the same race, age, sex, and other factors. The exclusion criteria were as follows: children with allergic purpura, skeletal dysplasia, chromosomal abnormalities, thyroid dysfunction, congenital heart disease, or intracranial tumours and those with incomplete data on IGF-1 and serum calcium and phosphorus.
According to the inclusion and exclusion criteria, 747 children and adolescents (540 males and 207 females) aged 10.23 ± 3.47 years were enrolled in this study (Table 1). The study was approved by the Human Ethics Committee of the Affiliated Hospital of Jining Medical University (Shandong, China).
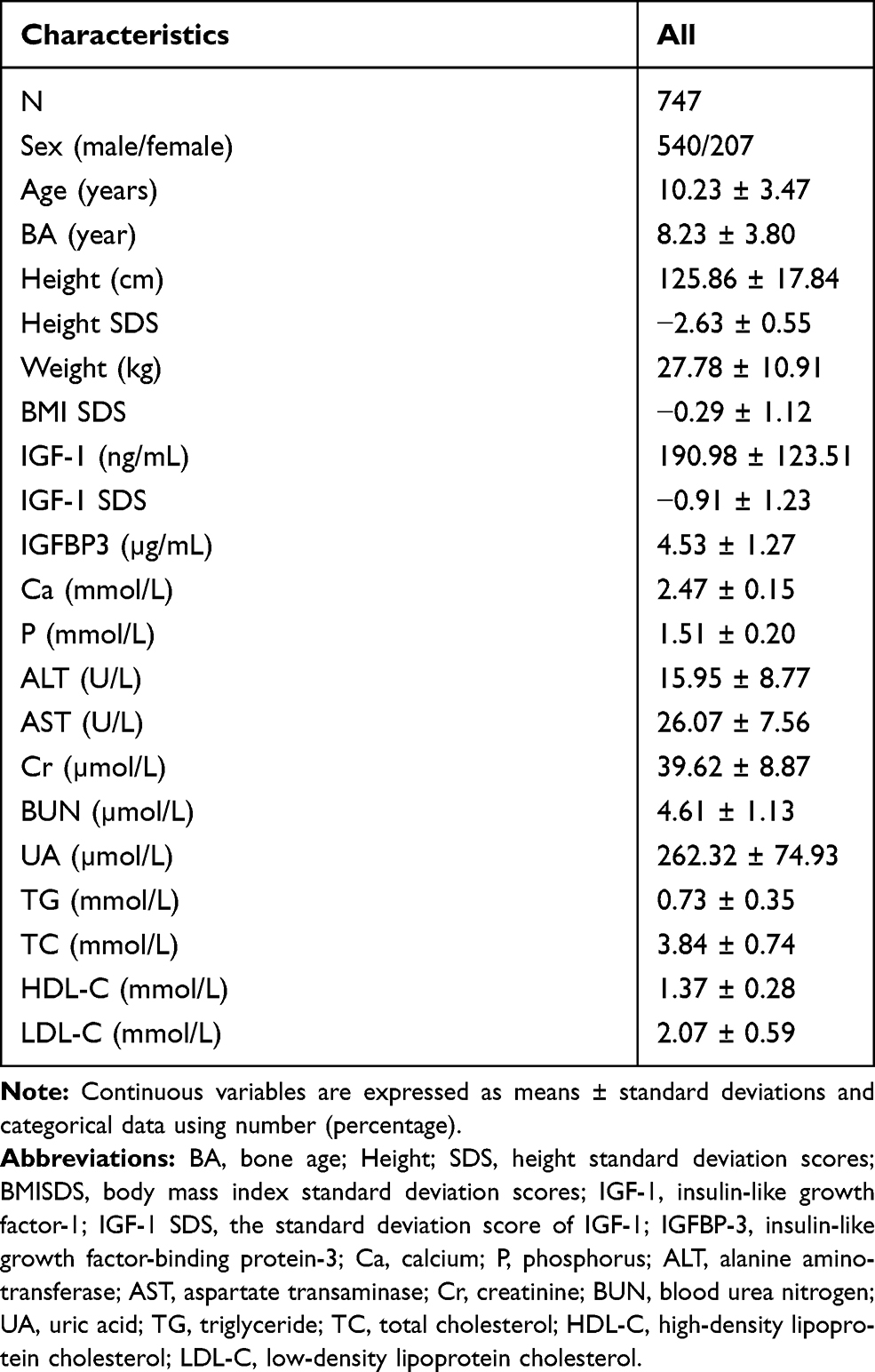 |
Table 1 Clinical Characteristics of Subjects |
Anthropomorphic Measurements
With no shoes and no covering on the head, the height of each patient was measured with the same height measuring instrument (produced by Nantong Best Industrial Co. Ltd., Jiangsu, China) with an allowable error range of 0.1 cm. The height SDS was calculated based on the normal range of Chinese children.18 Weight was measured with the same electronic scale from the same manufacturer (Xiang shan Weighing Apparatus Co. Ltd., Guangdong, China) and was accurate within ± 0.1 kg. Body mass index (BMI) was calculated as the ratio between the obtained body weight in kilograms and the height in metres squared. The BMI standard deviation score (BMI SDS) was calculated according to 2009 growth graphs for Chinese children and adolescents.19 The stage of puberty was assessed by physical examinations according to Tanner staging.20 The criteria for prepuberty were as follows: for boys, testicular volume less than 4 mL evaluated by an orchiometer according to Prader with no pubic hair; for girls, no breast development or pubic hair.21,22 The bone age (BA) was measured by taking an X-ray of the left hand including the hand bone, wrist, and 3–4 cm of the radial ulnar stem. The BA was reviewed according to the Greulich-Pyle method by a senior doctor who was specifically hired by our institution.
Laboratory Measurements
Serum IGF-1 and IGFBP-3 levels were measured by the chemiluminescence immunometric method (DPC IMMULITE 1000 analyser, SIEMENS, Germany) with intra- and interassay CVs for IGF-1 of 3.0% and 6.2%, respectively, and intra- and interassay CVs for IGFBP-3 of 4.4% and 6.6%. The IGF-1 standard deviation score (IGF-1 SDS) adjusted for age and sex was determined according to IGF-1 levels of healthy Japanese children and adolescents of the same age and sex.23 Liver function (including alanine aminotransferase (ALT) and AST levels), renal function (including Cr, blood urea nitrogen (BUN), and uric acid (UA)), blood lipid indices (including total cholesterol (TC), high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein C (LDL-c), triglycerides (TGs), and fasting blood glucose (FBG)), and serum calcium and phosphorus were measured by a biochemical automatic analyser (Cobas c702, Roche; Shanghai, China).
Statistical Analysis
All statistical analyses were performed with R statistical software (https://www.r-project.org) and Empower Stats (http://www.empowerstats.com, X&Y Solutions, Inc. Boston MA). Normally distributed variables were expressed as the mean ± standard deviation (SD). We investigated the relationship between IGF-1 and serum calcium and phosphorus levels using a smooth curve fit after adjusting for potential confounders. Finally, a multivariate piecewise linear regression model was applied to examine the threshold association of IGF-1 and serum phosphorus levels. Statistical significance was accepted at a two-sided p value <0.05.
Results
Subject Characteristics
The clinical characteristics of all participants are described in Table 1. A total of 747 children and adolescents with short stature aged 10.23 ± 3.47 years were included in the study. The mean IGF-1 SDS of the participants was −0.91 ± 1.23. The mean levels of serum calcium and phosphorus were 2.47 ± 0.15 and 1.51 ± 0.20 mmol/L, respectively.
Associations Between IGF-1 and Anthropometrical and Biochemical Variables
As shown in Table 2, univariate linear regression analysis was performed to determine the relationships between clinical parameters and IGF-1 SDS. For the unadjusted model, we observed a significant positive correlation between serum calcium or phosphorus and IGF-1 SDS (p = 0.036, p <0.001, respectively). Other variables that remained significantly associated with IGF-1 SDS were sex, age, weight, BMI SDS, AST, Cr, UA, LDL-c, FBG, and puberty stage (p < 0.05). No significant association was observed between IGF-1 SDS and ALT, BUN, TC, TG or HDL-c (p > 0.05).
 |
Table 2 Univariate Analysis of Associations with IGF-1 SDS |
Linear Regression Results of Serum Calcium and IGF-1 SDS
Smooth curve fitting was performed after adjusting for possible confounding factors, including sex, age, bone age, puberty stage, weight, BMI SDS, Cr, UA, TC, TG, ALT, AST and FBG. As shown in Figure 1A, a linear relationship was found between serum calcium levels and IGF-1 SDS in participants. Then, adjusted linear regression was performed in Table 3, and the results showed that serum calcium was positively associated with IGF-1 SDS (β 1.07, 95% CI 0.21, 1.92; p = 0.015).
 |
Table 3 Threshold Effects of IGF-1SDS with Serum Calcium and Phosphorus Were Analyzed Using Piecewise Linear Regression |
 |
Figure 1 Relationship between serum calcium and phosphorus levels and IGF-1 concentration in adolescents. (A) Serum calcium and IGF-1SDS. (B) Serum phosphorus and IGF-1 SDS. Adjusted for sex, age, puberty stage, weight, BMI SDS, Cr, UA, TC, TG, ALT, AST, FPG. |
Independent Correlation Between Serum Phosphorus Levels and IGF-1 SDS by Multivariate Piecewise Linear Regression
Similarly, smooth curve fitting was performed after adjusting for possible confounding factors. As shown in Figure 1B, the participants’ serum phosphorus levels exhibited non-linear relationships with IGF-1 SDS, and the resulting curve exhibited a two-stage change and a breakpoint. When the serum phosphorus value was less than the breakpoint, there was a negative relationship between serum phosphorus and IGF-1 SDS; however, if the value was greater than the breakpoint, there was a positive relationship between serum phosphorus and IGF-1 SDS.
As shown in Table 3, we further analysed the threshold effect based on curve fitting, and the data indicated that the inflection point of serum phosphorus was 1.26 mmol/L. Specifically, IGF-1 SDS levels decreased with serum phosphorus when the serum phosphorus level was less than 1.26 mmol/L, but the difference was not statistically significant (β −1.36, 95% CI −3.53, 0.82; p = 0.223). However, when the serum phosphorus level was greater than 1.26 mmol/L, the IGF-1 SDS increased with the increase in serum phosphorus (β 1.92, 95% CI 1.36, 2.48; p < 0.001).
Discussion
In this study, we observed a positive correlation between serum calcium and IGF-1, and there was a non-linear relationship between serum phosphorus and IGF-1 SDS in children and adolescents with short stature. The turning point for serum phosphorus was 1.26 mmol/L. There was a positive correlation between serum phosphorus and IGF-1 SDS when the serum phosphorus concentration was greater than 1.26 mmol/L.
Calcium and phosphorus play important roles in many biological processes, and studies have shown that they may have a positive regulatory role in cell growth and proliferation. Calcium is needed for muscle contraction, hormone release, blood clotting concatenation and neuronal excitation. Phosphorus is involved in the body’s energy metabolism, nucleic acid synthesis, and cell signalling conduction and cell membrane stabilization. Chad H. Stahl et al found that limited calcium and phosphate diets reduced stem cell proliferation and subsequent growth potential in newborn pigs.24,25 A study by Burak toprak et al found that calcium and phosphorus levels in cord blood were related to birth size parameters.26 It is known that the main “endocrine” function of IGF-1 is to broker the growth-promoting effect of pituitary GH.27 Therefore, the relationship between calcium and phosphorus and IGF-1 is worth further discussion. One study suggested that breast milk stimulates IGF-1 secretion in infant mice, and phosphorus insufficiency disables this ability and causes dwarfism-like symptoms.28 In an intervention study involving 57 boys by C Hoppe et al found that ingesting large amounts of milk minerals (Ca and P) had no independent effect on IGF-1.29 However, in some observational studies on men and women, as the intake of multiple minerals increased (including Ca and P), the molar ratio of IGF-1 in circulation tended to increase.30,31 The reason for the difference may be due to the age and nutritional status of the study population.
Analysis of cross-sectional data from the third National Health and Nutrition Survey of the National Center for Health Statistics in the United States revealed positive correlations between serum calcium levels and IGF-1. In particular, these associations were observed in people aged<60 and non-Hispanic whites.14 The difference between our research and theirs is that the population we studied is patients with short stature. We also found a positive correlation between serum calcium and IGF-1. However, our research subjects are all Asian children and adolescents with short stature, so there was no further stratification analysis according to age and race. At present, there are few studies on the relationship between IGF-1 and serum phosphorus. Several studies on XLH have observed that renal phosphate reabsorption and increases in serum phosphate levels during GH treatment are thought to be mediated by IGF-I.15–17 It is suggested that circulating IGF-1 may contribute to the level of serum phosphorus, thus meriting further investigation. The main clinical finding in patients with XLH is growth failure with skeletal deformities. However, short stature caused by specific diseases such as skeletal dysplasia has been excluded from our research. In our population, we have also observed that there is a correlation between phosphorus and IGF-I. Laura J et al observed that in a model of phosphorus-deficient pigs, the levels of IGF-1 message and levels of IGFBP3 transcript were increased compared with those in phosphorus-adequate groups.32 This is contrary to our observations of a correlation between serum phosphorus and serum IGF-1 and a positive correlation after the inflection point. The serum phosphorus levels of the patients we included were within the normal range, and the population before and after the inflection point was not specific. There are more male patients than females in our study population. This is similar to some previous reports,33–35 considering that men may be more willing to seek medical treatment due to social, family values and other factors.
The concentration of IGF-1 in children with short stature can affect subsequent growth potential. The results of this study show that increased levels of serum calcium and phosphorus may affect the concentration of IGF-1. Although studies have reported that mild elevations of serum phosphate in the normal population are associated with cardiovascular disease risk,36 there have been no reports of children and adolescents with short stature. Subsequent studies need to further determine whether increasing the serum calcium and phosphorus concentration within the normal range can increase the height benefit in children with short stature and simultaneously evaluate whether this will have an impact on cardiovascular health. A limitation of this study is that the cross-sectional analysis performed in this study did not allow us to determine causality. Additionally, calcium and phosphorus metabolism-related hormones were not evaluated in this study. Vitamin D, which is related to calcium and phosphorus metabolism, may increase IGF-I concentrations by augmenting intestinal calcium absorption, as a high-calcium rescue diet has been reported to normalize IGF-I levels in vitamin D receptor knockout mice and intake of calcium was positively associated with circulating IGF-I in humans.37,38 Nevertheless, we still need to pay attention to the hormone information related to the regulation of serum calcium and phosphorus metabolism in the future. At the same time, additional research is needed to fully elucidate the underlying mechanism of the association between serum calcium or phosphorus levels and IGF-1.
In conclusion, we described a positive correlation between IGF-1 and serum calcium and a non-linear relationship between IGF-1 and serum phosphorus by adjusting for potential confounding factors in children and adolescents with short stature. This finding suggests that serum calcium and phosphorus levels in children and adolescents with short stature may affect IGF-1 concentrations.
Abbreviations
BA, bone age; Height SDS, height standard deviation scores; BMI, body mass index; BMI SDS, body mass index standard deviation scores; IGF-1, insulin-like growth factor-1; IGF-1 SDS, the standard deviation score of IGF-1; IGFBP-3, insulin-like growth factor-binding protein-3; Ca, calcium; P, phosphorus; FPG, fasting plasma glucose; ALT, alanine aminotransferase; AST, aspartate transaminase; Cr, creatinine; UA, uric acid; TG, triglyceride; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
Data Sharing Statement
The datasets used and/or analysed in the current study are available from the corresponding authors upon reasonable request.
Ethics Approval and Consent to Participate
Human Ethics Committee of the Affiliated Hospital of Jining Medical University approved the study. All procedures were performed in accordance with ethical standards laid out in the Declaration of Helsinki. All of the families of the patients were informed of the aims of the study, and written informed consent was obtained from the parents of the patients.
Consent for Publication
All authors have read and approved the content, and they agree to submit it for consideration for publication in the journal.
Acknowledgments
The authors thank all the staff members in our institution.
Funding
This study was supported by Jining Science and Technology Bureau (No. 2019SMNS023), Research Fund for Lin He’s Academician Workstation of New Medicine and Clinical Translation in Jining Medical University (JYHL2018FZD03). This work was supported by Research Fund for Teacher Research Support Fund in Jining Medical University (JYFC2018FKJ124).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Collett-Solberg PF, Ambler G, Backeljauw PF, et al. Diagnosis, genetics, and therapy of short stature in children: a Growth Hormone Research Society International perspective. Horm Res Paediatr. 2019;92(1):1–14. doi:10.1159/000502231
2. Grunauer M, Jorge AAL. Genetic short stature. Growth Hormone & IGF Research. 2018;38:29–33. doi:10.1016/j.ghir.2017.12.003
3. Lin S, Li C, Li C, Zhang X. Growth hormone receptor mutations related to individual dwarfism. Int J Mol Sci. 2018;19(5):1433. doi:10.3390/ijms19051433
4. Bergan-Roller HE, Sheridan MA. The growth hormone signaling system: insights into coordinating the anabolic and catabolic actions of growth hormone. Gen Comp Endocrinol. 2018;258:119–133. doi:10.1016/j.ygcen.2017.07.028
5. Stawerska R, Czkwianianc E, Smyczyńska J, Hilczer M, Lewiński A. Nutritional status in short stature children is related to both ghrelin and insulin-like growth factor I concentrations. J Pediatr Gastroenterol Nutr. 2017;64(5):812–817. doi:10.1097/MPG.0000000000001387
6. Zhao Q, Zhang M, Chu Y, et al. Association between insulin-like growth factor-1 and relative skeletal maturation: a retrospective cohort study of short children and adolescents. Biomed Res Int. 2020;2020:8052143. doi:10.1155/2020/8052143
7. Schlechter NL, Russell SM, Spencer EM, Nicoll CS. Evidence suggesting that the direct growth-promoting effect of growth hormone on cartilage in vivo is mediated by local production of somatomedin.. Proc Natl Acad Sci U S A. 1986;83(20):7932–7934. doi:10.1073/pnas.83.20.7932
8. Rinderknecht E, Humbel RE. Primary structure of human insulin-like growth factor II. FEBS Lett. 1978;89(2):283–286. doi:10.1016/0014-5793(78)80237-3
9. Berryman DE, Glad CA, List EO, Johannsson G. The GH/IGF-1 axis in obesity: pathophysiology and therapeutic considerations. Nat Rev Endocrinol. 2013;9(6):346–356. doi:10.1038/nrendo.2013.64
10. Møller N, Jørgensen JO. Effects of growth hormone on glucose, lipid, and protein metabolism in human subjects. Endocr Rev. 2009;30(2):152–177. doi:10.1210/er.2008-0027
11. Palmer SC, et al. Serum levels of phosphorus, parathyroid hormone, and calcium and risks of death and cardiovascular disease in individuals with chronic kidney disease: a systematic review and meta-analysis. JAMA. 2011;305(11):1119–1127. doi:10.1001/jama.2011.308
12. Zhu GH, Sun XP, Liu Z, et al. The relation between serum phosphorus levels and long-term mortality in Chinese patients with ST-segment elevation myocardial infarction. J Geriatr Cardiol. 2019;16(10):775–781. doi:10.11909/j.issn.1671-5411.2019.10.004
13. Locatelli V, Bianchi VE. Effect of GH/IGF-1 on bone metabolism and osteoporosis. Int J Endocrinol. 2014;2014:235060. doi:10.1155/2014/235060
14. Van Hemelrijck M, Shanmugalingam T, Bosco C, Wulaningsih W, Rohrmann S. The association between circulating IGF1, IGFBP3, and calcium: results from NHANES III. Endocr Connect. 2015;4(3):187–195. doi:10.1530/EC-15-0039
15. Seikaly MG, Brown R, Baum M. The effect of recombinant human growth hormone in children with X-linked hypophosphatemia. Pediatrics. 1997;100(5):879–884. doi:10.1542/peds.100.5.879
16. Baroncelli GI, Bertelloni S, Ceccarelli C, Saggese G. Effect of growth hormone treatment on final height, phosphate metabolism, and bone mineral density in children with X-linked hypophosphatemic rickets. J Pediatr. 2001;138(2):236–243. doi:10.1067/mpd.2001.108955
17. Živičnjak M, Schnabel D, Staude H, et al. Three-year growth hormone treatment in short children with X-linked hypophosphatemic rickets: effects on linear growth and body disproportion. J Clin Endocrinol Metab. 2011;96(12):E2097–E2105. doi:10.1210/jc.2011-0399
18. Li H, Ji CY, Zong XN, Zhang YQ. Height and weight standardized growth charts for Chinese children and adolescents aged 0 to 18 years. Zhonghua Er Ke Za Zhi. 2009;47(7):487–492.
19. Li H, Ji CY, Zong XN, Zhang YQ. Body mass index growth curves for Chinese children and adolescents aged 0 to 18 years. Zhonghua Er Ke Za Zhi. 2009;47(7):493–498.
20. Tanner JM, Whitehouse RH. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty.. Arch Dis Child. 1976;51(3):170–179. doi:10.1136/adc.51.3.170
21. Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Arch Dis Child. 1970;45(239):13–23. doi:10.1136/adc.45.239.13
22. Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls.. Arch Dis Child. 1969;44(235):291–303. doi:10.1136/adc.44.235.291
23. Isojima T, Shimatsu A, Yokoya S, et al. Standardized centile curves and reference intervals of serum insulin-like growth factor-I (IGF-I) levels in a normal Japanese population using the LMS method. Endocr J. 2012;59(9):771–780. doi:10.1507/endocrj.ej12-0110
24. Alexander LS, Mahajan A, Odle J, Flann KL, Rhoads RP, Stahl CH. Dietary phosphate restriction decreases stem cell proliferation and subsequent growth potential in neonatal pigs. J Nutr. 2010;140(3):477–482. doi:10.3945/jn.109.117390
25. Mahajan A, Alexander LS, Seabolt BS, et al. Dietary calcium restriction affects mesenchymal stem cell activity and bone development in neonatal pigs. J Nutr. 2011;141(3):373–379. doi:10.3945/jn.110.131193
26. Colak A, Yildiz O, Toprak B, Turkon H, Halicioglu O, Coker I. Correlation between calcium and phosphorus in cord blood and birth size in term infants. Minerva Pediatr. 2016;68(3):182–188.
27. Laviola L, Natalicchio A, Giorgino F. The IGF-I signaling pathway. Curr Pharm Des. 2007;13(7):663–669. doi:10.2174/138161207780249146
28. Nakamura A, Miyado K, Yamatoya K, Kawano N, Umezawa A. Breast milk stimulates growth hormone secretion in infant mice, and phosphorus insufficiency disables this ability and causes dwarfism-like symptoms. Regen Ther. 2015;2:49–56. doi:10.1016/j.reth.2015.11.001
29. Hoppe C, Mølgaard C, Dalum C, Vaag A, Michaelsen KF. Differential effects of casein versus whey on fasting plasma levels of insulin, IGF-1 and IGF-1/IGFBP-3: results from a randomized 7-day supplementation study in prepubertal boys. Eur J Clin Nutr. 2009;63(9):1076–1083. doi:10.1038/ejcn.2009.34
30. Giovannucci E, Pollak M, Liu Y, et al. Nutritional predictors of insulin-like growth factor I and their relationships to cancer in men. Cancer Epidemiol Biomarkers Prev. 2003;12(2):84–89.
31. Norat T, Dossus L, Rinaldi S, et al. Diet, serum insulin-like growth factor-I and IGF-binding protein-3 in European women. Eur J Clin Nutr. 2007;61(1):91–98. doi:10.1038/sj.ejcn.1602494
32. Hittmeier LJ, Grapes L, Lensing RL, Rothschild MF, Stahl CH. Genetic background influences metabolic response to dietary phosphorus restriction. J Nutr Biochem. 2006;17(6):385–395. doi:10.1016/j.jnutbio.2005.08.008
33. Wu D, Chen R-M, Chen S-K, et al. Final adult height of children with idiopathic short stature: a multicenter study on GH therapy alone started during peri-puberty. BMC Pediatr. 2020;20(1):138. doi:10.1186/s12887-020-02034-8
34. Nam H-K, Kim HR, Lee K-H, Rhie Y-J. Idiopathic short stature phenotypes among Korean children: cluster analysis. Tohoku J Exp Med. 2019;248(3):193–200. doi:10.1620/tjem.248.193
35. Majewska KA, Kedzia A, Kontowicz P, et al. Polymorphism of the growth hormone gene GH1 in Polish children and adolescents with short stature. Endocrine. 2020;69(1):157–164. doi:10.1007/s12020-020-02305-5
36. Calvo MS, Uribarri J. Public health impact of dietary phosphorus excess on bone and cardiovascular health in the general population. Am J Clin Nutr. 2013;98(1):6–15. doi:10.3945/ajcn.112.053934
37. Song Y, Kato S, Fleet,JC. Vitamin D receptor (VDR) knockout mice reveal VDR-independent regulation of intestinal calcium absorption and ECaC2 and calbindin D9k mRNA. J Nutr. 2003;133(2):374–380. doi:10.1093/jn/133.2.374
38. Crowe FL, Key TJ, Allen NE, et al. The association between diet and serum concentrations of IGF-I, IGFBP-1, IGFBP-2, and IGFBP-3 in the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev. 2009;18(5):1333–1340. doi:10.1158/1055-9965.EPI-08-0781
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.