Back to Journals » International Journal of Women's Health » Volume 13
Association Between Serious Psychological Distress and Loneliness During the COVID-19 Pandemic: A Cross-Sectional Study with Pregnant Japanese Women
Authors Takeda T ![]() , Yoshimi K
, Yoshimi K ![]() , Kai S, Inoue F
, Kai S, Inoue F
Received 9 September 2021
Accepted for publication 3 November 2021
Published 11 November 2021 Volume 2021:13 Pages 1087—1093
DOI https://doi.org/10.2147/IJWH.S338596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Takashi Takeda,* Kana Yoshimi,* Sayaka Kai, Fumi Inoue
Division of Women’s Health, Research Institute of Traditional Asian Medicine, Kindai University, Osaka, 589-8511, Japan
*These authors contributed equally to this work
Correspondence: Takashi Takeda
Division of Women’s Health, Research Institute of Traditional Asian Medicine, Kindai University, 377-2 Ohno-Higashi, Osaka-Sayama, Osaka, 589-8511, Japan
Tel +81-72-366-0221 (Ext. 3393)
Fax +81-72-366-6661
Email [email protected]
Purpose: Pregnant women are vulnerable to stress. The coronavirus disease 2019 (COVID-19) has caused a global pandemic and created significant stress for many people. Social distancing to reduce the spread of COVID-19 has also reduced social interactions, which has increased social isolation and loneliness. Loneliness is thought to increase perceived stress, cause psychological distress, and increase the risk of mental illness, such as depression. This study examined the association between serious psychological distress (SPD) and loneliness during the COVID-19 pandemic in pregnant Japanese women.
Patients and Methods: An internet survey of 1022 pregnant women in Japan was conducted between June 1 and July 21, 2021. The 6-item Kessler Psychological Distress Scale, 3-item Revised UCLA Loneliness Scale, and Fear of COVID-19 Scale were used as measurement tools. The prevalence of SPD was defined as a K6 score of ≥ 13.
Results: The prevalence of SPD was 16.5%. Multivariate analysis revealed that the risk factors for SPD were younger age (odds ratio [OR] 1.05; 95% confidence interval [CI] 1.01 to 1.10; p = 0.020), history of abortion or miscarriages (OR 1.56; 95% CI 1.04 to 2.36; p = 0.034), unemployment (OR 1.67; 95% CI 1.14 to 2.45; p = 0.008), fear of COVID-19 (OR, 1.12; 95% CI, 1.08 to 1.17; p < 0.001), and loneliness (OR 1.53; 95% CI 1.38 to 1.70; p < 0.001).
Conclusion: Pregnant women in Japan showed a high prevalence of SPD. Younger age, unemployment, history of abortion or miscarriages, fear of COVID-19, and loneliness were independently associated with SPD. Clinicians and health officials should pay particular attention to the psychological health of pregnant women during the COVID-19 pandemic.
Keywords: stress, mental health, social isolation, maternal health
Corrigendum for this paper has been published
Introduction
The coronavirus disease 2019 (COVID-19) outbreak has become a global pandemic that has had an enormous impact on both the physical and psychological health of people around the world.1 A systematic review and meta-analysis has shown that psychological distress in the general population has increased during the COVID-19 pandemic.2 Pregnant women are particularly vulnerable to stress, and stress during pregnancy is also known to increase obstetric complications and adversely affect child development.3 Previous reports have shown that natural disasters affect their mental health.4–6 A recently published systematic review of mental health outcomes in pregnant women during the COVID-19 pandemic has also shown that psychological symptoms, such as depressive symptoms and anxiety, are increasing.7 A stressful life, along with vulnerabilities to stress, causes psychological distress and increases the risk of mental illness, such as depression and anxiety. Given that stress resulting from a severe natural disaster is sudden, while the stress from the COVID-19 pandemic has persisted over time, these types of stress are likely to differ.
While social distancing is recommended for the prevention of COVID-19, this measure reduces social interactions, which in turn increases social isolation and loneliness. The concept of social isolation indicates objective isolation, while loneliness signifies that an individual subjectively feels isolated.8 Loneliness and social isolation are recognized as important healthcare issues and are closely associated with cardiovascular disease, depression, and anxiety.9 Maruyama10 pointed out that pregnant women in Japan tend to be isolated due to social changes, such as the declining birth rate and the shift to nuclear families. An early report about the lockdown in England due to the COVID-19 pandemic revealed that almost one quarter of adults experienced loneliness during that time.11 Moreover, pregnant women tended to avoid regular maternity checkups and social support from local governments due to concerns about COVID-19 infection; this is not only an issue in the UK, but also globally. A recent large-scale international survey of pregnant women revealed that about half of the women reported increased feelings of loneliness during the COVID-19 pandemic.12 In a study of the Spanish population during the initial stage of the COVID-19 pandemic, loneliness was correlated with depression, anxiety, and post-traumatic stress disorder.13 Social support has been identified as a major protective factor against negative mental health outcomes resulting from natural disasters and pandemics,14,15 and recent evidence suggests that it is also associated with lower mental health symptoms in pregnant women during the COVID-19 pandemic.16 The COVID-19 pandemic has resulted in circumstances that may limit many women’s reliance on this major protective factor and contribute to increased loneliness.
Another large-scale survey of psychological distress among the general population in Japan was conducted between August and September 2020.17 In this survey, gender (women), age (younger), income level, employment type, caregiving status, domestic violence experience, and fear of COVID-19 were independently associated with serious psychological distress (SPD). However, this study had not targeted pregnant women, who may have additional risk factors for SPD such as a history of miscarriage and abortion.
A previous report on psychological distress among pregnant Japanese women conducted in September 2020 reported only the psychological status at that point, and did not analyze factors associated with SPD.18 Moreover, no studies have yet analyzed the association between SPD and loneliness in pregnant women during the COVID-19 pandemic. Since the emergence of the delta variant, the COVID-19 situation in Japan has deteriorated rapidly and psychological distress is expected to worsen as a result. Under these circumstances, we felt that there was an urgent need to comprehensively examine the SPD of pregnant women in Japan. Loneliness is a key factor when considering the psychological distress of pregnant women; in Japan, which has experienced an unprecedented number of infections, it is imperative to examine the factors related to SPD in more detail. Then, we investigated a set of previously documented contributors to SPD (age, unemployment, fear of COVID-19), but also risk factors for SPD that have received less empirical attention in pregnant women, that is, history of abortion or miscarriage and loneliness. The aims of this study were to: (1) determine the prevalence of SPD experienced by pregnant women during the COVID-19 pandemic, (2) test whether loneliness is positively associated with SPD in pregnant women, and (3) explore associations between other relevant sociodemographic and psychological factors (age, weeks of gestation, parity, history of abortion or miscarriages, infertility treatment history, employment, income level, fear of COVID-19) and SPD.
Materials and Methods
Ethics Approval and Informed Consent
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. The trial protocol was approved by the Ethics Committee of Kindai University (approval number: R03-032). Before completing the survey, all participants read the description of the study’s purpose and agreed to participate in the study by providing online consent.
Settings and Participants
All participants were recruited from a banner advertisement on the obstetrics and gynecology outpatient reservation site @link (OFFSHORE Co. Ltd., Kobe, Japan). Since @link is a general-purpose appointment application used in obstetrics and gynecology hospitals nationwide (used for about 25% of all deliveries in Japan each year), through this platform, we can obtain survey data representative of the general pregnant women population in Japan. The questionnaire did not collect any personal information. The inclusion criteria were women who were 20 years or older and pregnant. A total of 1032 women responded to the web survey between June 1 and July 21, 2021. Given that respondents had to complete each questionnaire before proceeding to the next, there were no missing data. Of the 1032 respondents, eight under the age of 20 and two of unknown age were excluded (Figure 1). Ultimately, we analyzed data from 1022 pregnant women (mean age = 31.7 years, SD = 4.5; mean gestational weeks = 25.9, SD = 9.8; see Table 1 for participant demographics).
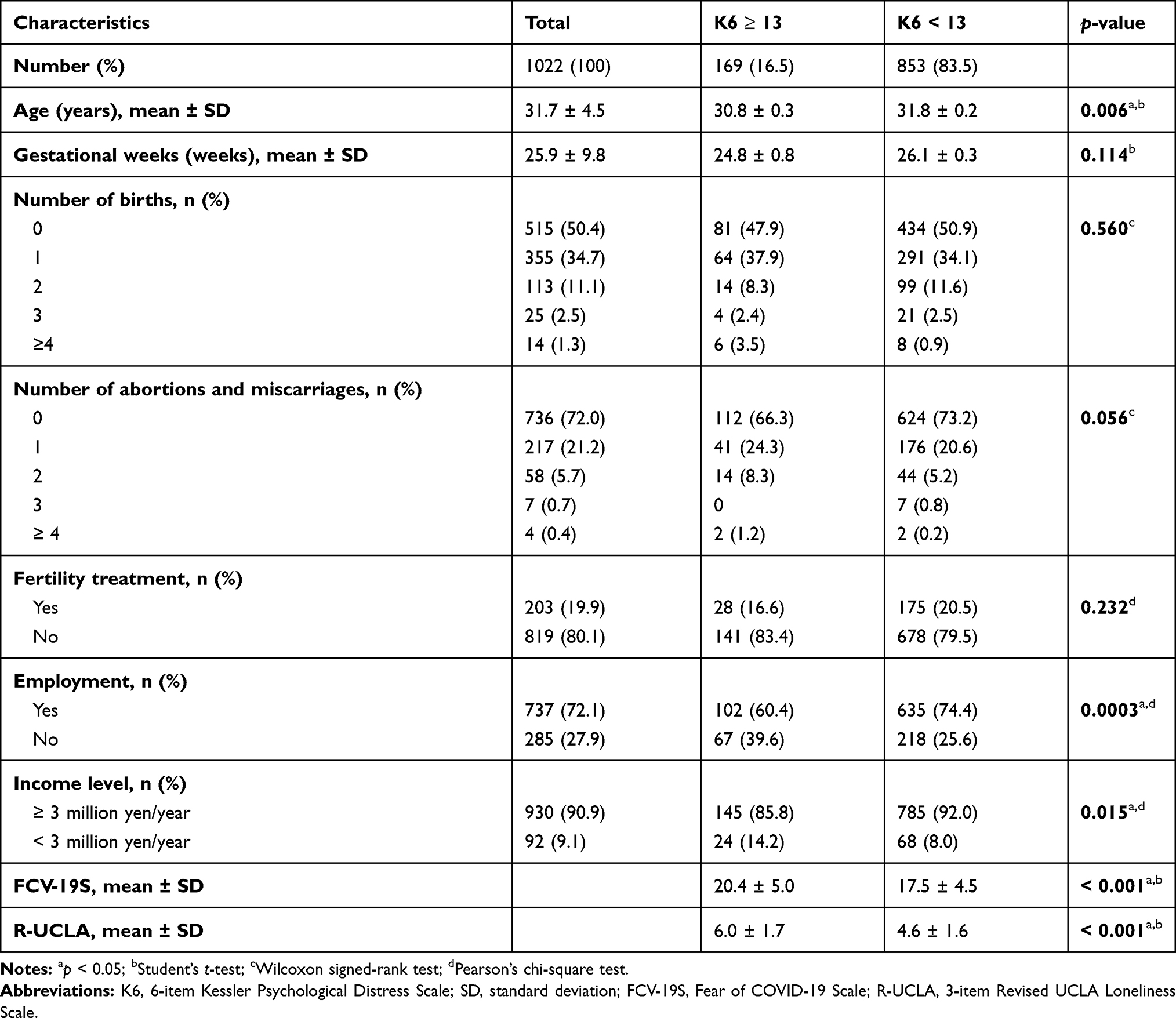 |
Table 1 Characteristics of Study Participants |
 |
Figure 1 Flow chart of the study. |
Questionnaire
The 6-Item Kessler Psychological Distress Scale
To assess psychological distress, we used the Japanese version of the 6-item Kessler Psychological Distress Scale (K6).19 The original version of the K6 was developed in English and then translated into Japanese.20 The reliability and validity of the K6 have been systematically confirmed. The K6 comprises 6 items that are scored using a 5-point response scale ranging from 0 to 4, corresponding to “None of the time” (0 points), “A little of the time” (1 point), “Some of the time” (2 points), “Most of the time” (3 points), and “All of the time” (4 points). The total K6 score ranges from 0 to 24. Cronbach’s alpha coefficient of the K6 was 0.896 in this study. We classified women with a total K6 score ≥ 13 as having SPD according to the criteria defined in the original Kessler scale.21
The 3-Item Revised UCLA Loneliness Scale
To assess loneliness, we used the Japanese version of the 3-item Revised UCLA Loneliness Scale (R-UCLA).22 The original version of the 3-item R-UCLA is the short form of the 21-item R-UCLA.23,24 The reliability and validity of the Japanese version have been established.22 The 3-item R-UCLA comprises three items, each of which is rated on a 4-point response scale ranging from 1 to 4, corresponding to “Never” (1 point), “Rarely” (2 points), “Sometimes” (3 points), and “Always” (4 points). The total R-UCLA score ranges from 3 to 12. The Cronbach’s alpha coefficient of the 3-item R-UCLA was 0.815 in this study.
Fear of COVID-19 Scale
To assess the fear of COVID-19, we used the Japanese version of the Fear of COVID-19 Scale (FCV-19S).25 The original version of the FCV-19S was developed in English26 and then translated into Japanese. The reliability and validity of the Japanese version has been systematically evaluated.25 The FCV-19S comprises 7 items that are scored on a 5-point response scale ranging from 1 to 5, corresponding to “Strongly disagree” (1 point), “Disagree” (2 points), “Neither agree nor disagree” (3 points), “Agree” (4 points), and “Strongly agree” (5 points). The total FCV-19S scores ranges from 7 to 35. The Cronbach’s alpha coefficient of the FCV-19S was 0.823 in this study.
For each participant, we also collected information about age, weeks of gestation, number of previous deliveries, number of abortions or miscarriages, infertility treatment history (Yes, No), employment (Yes, No), and income levels of the entire household (≥ JPY 3.0 million/USD 27200, < JPY 3.0 million/USD 27200). There are no definitive criteria established regarding a cut-off point for low household income in Japan. We selected 3.0 million JPY based on the Overview of the 2019 National Life Basic Survey, which was provided by the Japanese Ministry of Health, Labor and Welfare. Households were divided by income; 13.6% of households reported their income as between “2 million and less than 3 million JPY,” and this was the most frequent income bracket.
Statistical Analysis
Means and standard deviations were calculated for continuous variables and proportions were calculated for categorical variables. Baseline characteristics were compared between the SPD and non-SPD groups using the Student’s t-test, Pearson’s chi-square test, and Wilcoxon signed-rank test, as appropriate. The Pearson’s chi-square test was used for this comparison. Cronbach’s α coefficient was calculated to assess reliability to each scale (K6, 3-item R-UCLA, FCV-19S).
The prevalence of SPD was compared with the data from pregnant women surveyed in Miyagi prefecture, Japan, shortly after the Great East Japan Earthquake; Miyagi prefecture was one of the areas most seriously damaged by the earthquake.6 The Pearson’s chi-square test was used for this comparison. We also compared the K6 scores with data from a previous survey on psychological stress in pregnant women in Japan.18 Effect size was measured using Cramer’s V. The effect sizes of 0.06, 0.17, and 0.29 were judged as small, medium, and large, respectively.27
Multivariate logistic regression analysis was used to identify factors that were significantly associated with SPD. The number of deliveries was divided into two groups (primiparous and multiparous women) and the number of abortions or miscarriages was divided into two groups (those with and without a history of abortion or miscarriages). The model included age, weeks of gestation, parity, history of abortion or miscarriages, infertility treatment history, employment, income level, total 3-item R-UCLA score, and total FCV-19S score. Statistical analyses were performed using JMP Pro 16.0.0 (SAS, Cary, NC, USA). Statistical significance was set at p < 0.05.
Results
Participant characteristics are shown in Table 1. Of the participants, 16.5% had a score of ≥ 13 on the K6, which indicated that they had SPD.
Women with a K6 score ≥ 13 were significantly younger than those with a K6 score < 13. Women with SPD had a significantly lower annual income and were significantly more likely to be unemployed than women without SPD. Women with SPD had significantly higher FCV-19S and R-UCLA scores than women without SPD.
To identify risk factors that were significantly associated with SPD, a multivariate logistic regression analysis was performed (Table 2). The risk factors for SPD were younger age, history of abortions or miscarriages, and unemployment. A high total R-UCLA score and total FCV-19S score were also major risk factors.
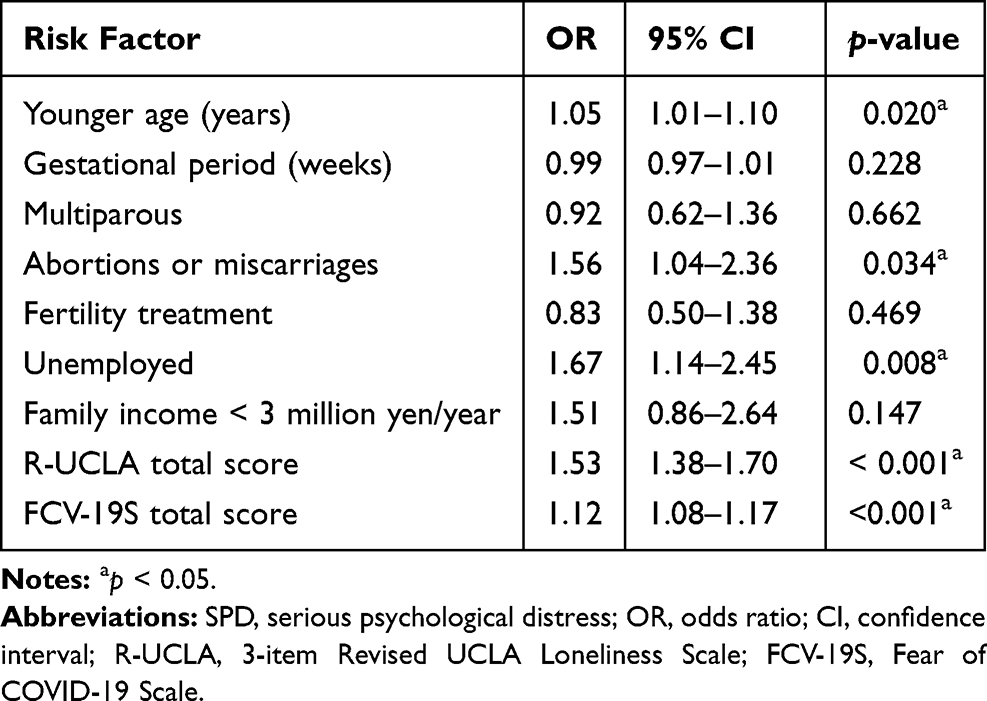 |
Table 2 Multivariate Logistic Regression Analysis of Risk Factors for SPD |
Discussion
Our results revealed a 16.5% prevalence of SPD, which is significantly higher than the prevalence in pregnant women in Miyagi prefecture, Japan, shortly after the Great East Japan Earthquake (4.9%, n = 998; p < 0.0001, Pearson’s chi-square test, Cramer’s V = 0.19).6 Stress resulting from a natural disaster is sudden, but the stress caused by the COVID-19 pandemic has continued over time. At the time of this survey, COVID-19-induced stress had persisted for about 15 months, from the time at which the World Health Organization declared the situation a pandemic in March 2020. In Japan, the fifth wave of infections began in June 2021; therefore, this survey was conducted when the number of COVID-19 patients was increasing rapidly. Unlike most Western countries, the Japanese government did not implement a strict lockdown during the COVID-19 pandemic. Despite having far fewer lockdowns, the rate of suicide among young women has increased dramatically in Japan.28 A previous cohort study showed that psychological distress is one of the major risk factors for suicide.29 This confirms that young Japanese women are in a state of great psychological distress, as demonstrated by our data.
Another large-scale survey of psychological distress among pregnant women in Japan was conducted in September 2020, where the cut-off score for SPD was ≥ 10 on the K6.18 The proportion of women with a K6 score ≥ 10 in our survey was 37.7%, which is significantly higher than that in the large-scale 2020 survey (13.9%, n = 2977; p < 0.0001, Pearson’s chi-square test, Cramer’s V = 0.26); this reveals a significant increase in psychological distress between September 2020 and June/July 2021, when our data were collected. The increasing COVID-19 infection rates in Japan, which are worsening due to the delta variant, may explain the rapid exacerbation of psychological distress.
Our results showed that younger age, unemployment, history of abortion or miscarriages, fear of COVID-19, and loneliness were independently associated with SPD. Another large-scale survey of psychological distress among the general population in Japan showed that gender (women), age (younger), income level, employment type, caregiving status, domestic violence experience, and fear of COVID-19 were independently associated with SPD.17 The results revealed that different factors were associated with SPD according to the population subgroup, but there was no dedicated analysis for the subgroup of pregnant women. Our study complements this study, in that it targeted pregnant women and evaluated loneliness. Pregnant women are a distinct population, and pregnancy-related issues, such as miscarriage history examined in our survey, should be investigated in the context of the pandemic. It has been well established that prenatal loss is a risk factor for maternal psychological distress in subsequent pregnancies.30–32 Our data revealed that a history of abortion or miscarriage was independently associated with SPD, which is consistent with previous reports.
In our study, the socio-economic factors of younger age and unemployment were risk factors for SPD. Concerning the age-related factors that have contributed to psychological distress during the COVID-19 lockdown, young adults have been reported to be most at risk.33 This tendency has also been observed in pregnant women, and it has been reported that younger age is associated with greater psychological distress.34 Our data are consistent with this report. Younger people tend to experience more instability in society and are thought to be more vulnerable to psychological distress. Similarly, unemployment seems to lead to instability in society, which also renders individuals more vulnerable.
Loneliness and social isolation are recognized as important healthcare issues. A recent report during the early stage of the COVID-19 pandemic revealed an association between loneliness and suicidal ideation.35 Moreover, SPD is an obvious risk factor for suicide.29 Given that pregnant women are vulnerable, our findings of a high and exacerbated prevalence of SPD in Japan warrants concern. Effective interventions have been implemented to manage social isolation and loneliness, while maintaining social distancing by using the internet or telephone.8 Social media and mental health apps may be additional options.36 Considering that the participants of these intervention studies were mainly older adults and college students, there is an urgent need for studies that focus on pregnant women.
Our study has several limitations. First, its cross-sectional design makes it impossible to determine causality between SPD and loneliness. Second, we collected data using a self-reported web-based survey. Pregnant women who did not choose to participate may have fewer symptoms than pregnant women who participated, in that they may not have been as interested in the survey. Conversely, it is also possible that women who chose not to participate were experiencing psychological disturbances, such as depression, and chose not to participate due to the perceived effort. It may be useful to examine observable indicators of stress such as cortisol in future research. Third, the study was only conducted in Japan, which limits the generalization of our findings to other countries. Considering that most Western countries were more affected by COVID-19 than Japan, the pandemic-induced impact on psychological distress and loneliness in Western countries may have been more severe than that in Japan. That said, our survey used validated and reliable Japanese versions of questionnaires that are used globally (the K6, R-UCLA, and FCV-19S), which means that our results could be applied not only to pregnant women in Japan, but also to those in other countries.
Conclusion
The present study revealed an association between SPD and loneliness among pregnant women in Japan during the COVID-19 pandemic. Clinicians and health officials should pay special attention to the psychological health of pregnant women during the COVID-19 pandemic.
Data Sharing Statement
The data obtained in this study are available from the corresponding author upon request.
Acknowledgments
We would like to express our gratitude to OFFSHORE Co. Ltd. for helping us with the web-based survey.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported in part by a grant from the KINDAI COVID-19 Control Support Project, Osaka, Japan.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cooke JE, Eirich R, Racine N, Madigan S. Prevalence of posttraumatic and general psychological stress during COVID-19: a rapid review and meta-analysis. Psychiatry Res. 2020;292:113347. doi:10.1016/j.psychres.2020.113347
2. Nochaiwong S, Ruengorn C, Thavorn K, et al. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: a systematic review and meta-analysis. Sci Rep. 2021;11(1):10173. doi:10.1038/s41598-021-89700-8
3. Caparros-Gonzalez RA, Torre-Luque A, Romero-Gonzalez B, Quesada-Soto JM, Alderdice F, Peralta-Ramirez MI. Stress during pregnancy and the development of diseases in the offspring: a systematic-review and meta-analysis. Midwifery. 2021;97:102939. doi:10.1016/j.midw.2021.102939
4. Dong X, Qu Z, Liu F, et al. Depression and its risk factors among pregnant women in 2008 Sichuan earthquake area and non-earthquake struck area in China. J Affect Disord. 2013;151(2):566–572. doi:10.1016/j.jad.2013.06.048
5. Ren JH, Chiang CL, Jiang XL, Luo BR, Liu XH, Pang MC. Mental disorders of pregnant and postpartum women after earthquakes: a systematic review. Disaster Med Public Health Prep. 2014;8(4):315–325. doi:10.1017/dmp.2014.62
6. Watanabe Z, Iwama N, Nishigori H, et al. Psychological distress during pregnancy in Miyagi after the Great East Japan earthquake: the Japan environment and children’s study. J Affect Disord. 2016;190:341–348. doi:10.1016/j.jad.2015.10.024
7. Iyengar U, Jaiprakash B, Haitsuka H, Kim S. One year into the pandemic: a systematic review of perinatal mental health outcomes during COVID-19. Front Psychiatry. 2021;12:674194. doi:10.3389/fpsyt.2021.674194
8. Williams CYK, Townson AT, Kapur M, et al. Interventions to reduce social isolation and loneliness during COVID-19 physical distancing measures: a rapid systematic review. PLoS One. 2021;16(2):e0247139. doi:10.1371/journal.pone.0247139
9. Leigh-Hunt N, Bagguley D, Bash K, et al. An overview of systematic reviews on the public health consequences of social isolation and loneliness. Public Health. 2017;152:157–171. doi:10.1016/j.puhe.2017.07.035
10. Maruyama N. Pregnant women’s loneliness: correlated factors and its impacts on maternal role identification and common complaints during pregnancy. J Jpn Acad Midwif. 2017;31(1):23–33. doi:10.3418/jjam.31.23
11. Mental Health Foundation. Almost a quarter of adults living under lockdown in the UK have felt loneliness; 2020. Available from: https://www.mentalhealth.org.uk/news/almostquarter-adults-living-under-lockdown-uk-have-felt-loneliness.
12. Basu A, Kim HH, Basaldua R, et al. A cross-national study of factors associated with women’s perinatal mental health and wellbeing during the COVID-19 pandemic. PLoS One. 2021;16(4):e0249780. doi:10.1371/journal.pone.0249780
13. Gonzalez-Sanguino C, Ausin B, Castellanos MA, et al. Mental health consequences during the initial stage of the 2020 coronavirus pandemic (COVID-19) in Spain. Brain Behav Immun. 2020;87:172–176. doi:10.1016/j.bbi.2020.05.040
14. Bonanno GA, Ho SAY, Chan JCK, et al. Psychological resilience and dysfunction among hospitalized survivors of the SARS epidemic in Hong Kong: a latent class approach. Health Psychol. 2008;27(5):659–667. doi:10.1037/0278-6133.27.5.659
15. Tsuchiya N, Nakaya N, Nakamura T, et al. Impact of social capital on psychological distress and interaction with house destruction and displacement after the Great East Japan Earthquake of 2011. Psychiatry Clin Neurosci. 2017;71(1):52–60. doi:10.1111/pcn.12467
16. Lebel C, MacKinnon A, Bagshawe M, Tomfohr-Madsen L, Giesbrecht G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J Affect Disord. 2020;277:5–13. doi:10.1016/j.jad.2020.07.126
17. Yoshioka T, Okubo R, Tabuchi T, Odani S, Shinozaki T, Tsugawa Y. Factors associated with serious psychological distress during the COVID-19 pandemic in Japan: a nationwide cross-sectional internet-based study. BMJ Open. 2021;11(7):e051115. doi:10.1136/bmjopen-2021-051115
18. Obata S, Miyagi E, Haruyama Y, et al. Psychological stress among pregnant and puerperal women in Japan during the coronavirus disease 2019 pandemic. J Obstet Gynaecol. 2021;47:2990–3000. doi:10.1111/jog.14877
19. Furukawa TA, Kawakami N, Saitoh M, et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int J Methods Psychiatr Res. 2008;17(3):152–158. doi:10.1002/mpr.257
20. Kessler RC, Andrews G, Colpe LJ, et al. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol Med. 2002;32(6):959–976. doi:10.1017/S0033291702006074
21. Kessler RC, Barker PR, Colpe LJ, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry. 2003;60(2):184–189. doi:10.1001/archpsyc.60.2.184
22. Arimoto A, Tadaka E. Reliability and validity of Japanese versions of the UCLA loneliness scale version 3 for use among mothers with infants and toddlers: a cross-sectional study. BMC Womens Health. 2019;19(1):105. doi:10.1186/s12905-019-0792-4
23. Russell DW. UCLA Loneliness Scale (Version 3): reliability, validity, and factor structure. J Pers Assess. 1996;66(1):20–40. doi:10.1207/s15327752jpa6601_2
24. Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–672. doi:10.1177/0164027504268574
25. Midorikawa H, Aiba M, Lebowitz A, et al. Confirming validity of the Fear of COVID-19 Scale in Japanese with a nationwide large-scale sample. PLoS One. 2021;16(2):e0246840. doi:10.1371/journal.pone.0246840
26. Ahorsu DK, Lin CY, Imani V, Saffari M, Griffiths MD, Pakpour AH. The Fear of COVID-19 Scale: development and initial validation. Int J Ment Health Addict. 2020;1–9. doi:10.1007/s11469-020-00270-8
27. Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York, NY: Routledge Academic; 1998.
28. Tanaka T, Okamoto S. Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nat Hum Behav. 2021;5(2):229–238. doi:10.1007/s11469-020-00270-8
29. Nie J, O’Neil A, Liao B, Lu C, Aune D, Wang Y. Risk factors for completed suicide in the general population: a prospective cohort study of 242, 952 people. J Affect Disord. 2021;282:707–711. doi:10.1016/j.jad.2020.12.132
30. Farren J, Jalmbrant M, Falconieri N, et al. Differences in post-traumatic stress, anxiety and depression following miscarriage or ectopic pregnancy between women and their partners: multicenter prospective cohort study. Ultrasound Obst Gyn. 2021;57(1):141–148. doi:10.1002/uog.23147
31. Farren J, Jalmbrant M, Falconieri N, et al. Posttraumatic stress, anxiety and depression following miscarriage and ectopic pregnancy: a multicenter, prospective, cohort study. Am J Obstet Gynecol. 2020;222(4):367e361–367 e322. doi:10.1016/j.ajog.2019.10.102
32. Hunter A, Tussis L, MacBeth A. The presence of anxiety, depression and stress in women and their partners during pregnancies following perinatal loss: a meta-analysis. J Affect Disord. 2017;223:153–164. doi:10.1016/j.jad.2017.07.004
33. Glowacz F, Schmits E. Psychological distress during the COVID-19 lockdown: the young adults most at risk. Psychiatry Res. 2020;293:113486. doi:10.1016/j.psychres.2020.113486
34. Berthelot N, Lemieux R, Garon-Bissonnette J, Drouin-Maziade C, Martel E, Maziade M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet Gynecol Scand. 2020;99(7):848–855. doi:10.1111/aogs.13925
35. Allan NP, Volarov M, Koscinski B, et al. Lonely, anxious, and uncertain: critical risk factors for suicidal desire during the COVID-19 pandemic. Psychiatry Res. 2021;304:114144. doi:10.1016/j.psychres.2021.114144
36. Chan KL, Chen M. Effects of social media and mobile health apps on pregnancy care: meta-analysis. JMIR Mhealth Uhealth. 2019;7(1):e11836. doi:10.2196/11836
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.