Back to Journals » Vascular Health and Risk Management » Volume 21
Association Between Sarcopenia Index and Incident Cardiovascular Events in a Chinese Aging Population: Prospective Analysis of the CHARLS Study
Authors Zhao A, Yang L, Zha Q, Zhang J, Zhang H, Tang Z, Wang Y, Chen J, Yang K, Liu Y, Sun J
Received 21 June 2025
Accepted for publication 6 October 2025
Published 4 November 2025 Volume 2025:21 Pages 895—905
DOI https://doi.org/10.2147/VHRM.S548650
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Akash Batta
Anqi Zhao,1,* Ling Yang,1,* Qing Zha,1,* Junfeng Zhang,1 Huili Zhang,1 Zhengde Tang,1 Yanping Wang,1 Jiawei Chen,1 Ke Yang,2 Yan Liu,1 Jiateng Sun3
1Department of Cardiology, Shanghai Ninth People’s Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Cardiovascular Medicine, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, People’s Republic of China; 3Department of Cardiology, Renji Hospital, School of Medicine, Shanghai Jiaotong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Liu, Department of Cardiology, Shanghai Ninth People’s Hospital, Shanghai Jiaotong University School of Medicine, 639 Zhizaoju Road, Shanghai, 200011, People’s Republic of China, Tel +86 21 23271699, Fax +86 21 63136856, Email [email protected] Jiateng Sun, Department of Cardiology, Renji Hospital, School of Medicine, Shanghai Jiaotong University, 160 Pujian Road, Shanghai, 200127, People’s Republic of China, Tel/Fax +86 21 68383477, Email [email protected]
Purpose: The Sarcopenia Index (SI), derived from the serum creatinine to cystatin C ratio, is a potential biomarker for cardiovascular disease (CVD). However, its prognostic significance for incident CVD in aging Chinese populations remains insufficiently characterized, despite established links between sarcopenia and CVD progression.
Patients and Methods: This prospective cohort study utilized data from the China Health and Retirement Longitudinal Study (CHARLS). A total of 4979 participants aged > 45 years without prevalent CVD at baseline were included (mean age 58.0 years). Participants were categorized into Sarcopenia Index (SI) tertiles as follows: Q1 (SI ≤ 71.10), Q2 (71.10 < SI ≤ 84.75), and Q3 (SI > 84.75). Incident CVD events were assessed over a 9-year follow-up period. Multivariable Cox proportional hazards models, adjusted for demographic factors, comorbidities, and lipid profiles, were employed to evaluate associations. Restricted cubic spline (RCS) analysis was used to evaluate the dose-response relationship between SI and CVD risk.
Results: In the total population, the cumulative incidence of CVD was 23.5%. The lowest SI tertile (Q1) exhibited the highest cumulative CVD incidence (27.0%), compared to Q2 (23.2%) and Q3 (20.4%). After multivariable adjustment, individuals in Q1 showed a significantly increased risk of CVD compared to those in Q3 (HR: 1.249, 95% CI: 1.054, 1.478, P=0.010). RCS analysis confirmed a non-linear inverse association between SI and CVD risk (P for non-linearity = 0.003). Significant associations were particularly pronounced in males, current smokers, non-drinkers, urban residents, individuals with body mass index (BMI) ≥ 28 kg/m2, and participants without hypertension or diabetes (all P < 0.05).
Conclusion: Reduced SI independently predicts elevated CVD risk in aging adults, underscoring its potential as an accessible, cost-effective screening biomarker. Integration of SI into routine clinical assessments may enhance early risk stratification and guide targeted preventive strategies, particularly for high-risk subgroups.
Keywords: sarcopenia index, cardiovascular disease, CHARLS, aging, cardiovascular events
Introduction
Cardiovascular disease (CVD) continues to be the leading cause of morbidity and mortality worldwide, exerting an increasing burden in China, particularly with the growth of the elderly population.1 Addressing this challenge, research increasingly emphasizes the pivotal role of sarcopenia in CVD development and progression, highlighting a reciprocal, causative relationship that accelerates both muscle deterioration and cardiovascular decline. Sarcopenia is notably prevalent in geriatric populations, where it has been associated with elevated risks of heart failure, atrial fibrillation, and atherosclerosis.2–6 Emerging evidence suggests these associations stem from interconnected mechanisms, including endothelial dysfunction, oxidative stress, chronic low-grade inflammation, mitochondrial impairments in skeletal muscles, and disrupted insulin signaling.2,7–9
In clinical practice, sarcopenia diagnosis typically involves functional assessments, such as handgrip strength, chair-stand tests, gait speed, and 6-minute walk tests,10 or imaging techniques, such as Magnetic Resonance Imaging (MRI), Computed Tomography (CT), Dual energy X-ray absorptiometry (DXA), to measure muscle mass.11 However, these advanced tools often pose practical and economic challenges, driving interest in novel, cost-effective biomarkers. The Sarcopenia Index (SI) represents one such option, calculated by dividing serum creatinine (mg/dL) by serum cystatin C (mg/dL) and multiplying by 100.12 While the SI has gained traction for sarcopenia screening, its potential to predict long-term cardiovascular outcomes in community settings remains underexplored, particularly among middle-aged and older Chinese adults.
To address this gap, the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative cohort, has been utilized to examine whether the SI can effectively predict cardiovascular events within this population. Insights from CHARLS may contribute to developing practical, scalable strategies for early detection and intervention, ultimately alleviating the significant CVD burden in aging societies.
Methods
Study Population and Design
CHARLS is a nationally representative cohort aimed at investigating the health and aging of adults in China (http://charls.pku.edu.cn/). The baseline survey conducted in 2011 (Wave 1) utilized a multistage stratified probability-proportional-to-size sampling method, enrolling 25,873 individuals from 10,257 households across 150 counties/districts and 450 communities nationwide. This cohort has been followed biennially, with subsequent waves in 2013, 2015, 2018, and 2020. Comprehensive methodologies for sampling, anthropometry, and blood biomarker collection have been described previously.13
All participants provided written informed consent, and the study adhered to the Declaration of Helsinki, receiving approval from the Peking University Institutional Review Board (IRB00001052-11015). Standardized face-to-face questionnaires were administered by trained interviewers during each wave to collect sociodemographic information, medical histories, health behaviors, cognitive function, and depressive symptoms.14
For the current analysis, inclusion criteria required participants to be free of CVD at baseline (2011–2012), after excluding those with missing serum creatinine or cystatin C measurements, those without continuous cardiovascular follow-up, there were 5040 eligible participants. Participants who lacked baseline information (eg, age, smoking and alcohol consumption) were also excluded, the final analytical sample comprised 4979 individuals. Figure 1 outlines the inclusion and exclusion steps in detail.
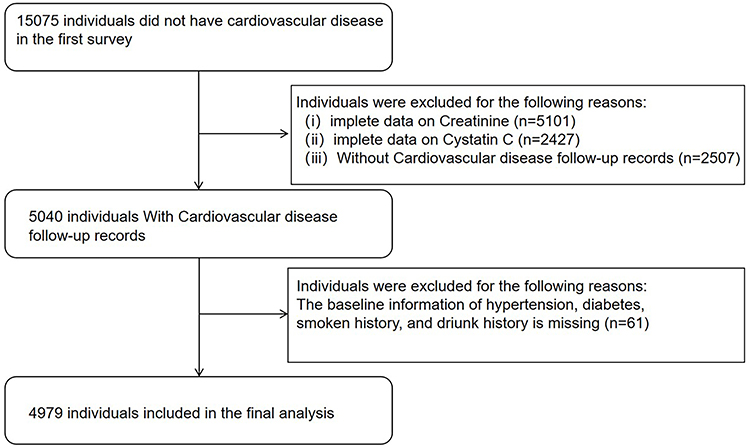 |
Figure 1 Flowchart of study participants. |
Data Collection
Data collection in this cardiovascular clinical study was structured to capture a comprehensive range of baseline information, including demographic, anthropometric, biochemical, and clinical variables.1,15,16 Demographic data encompassed gender, age, place of residence (urban or rural), and educational background (illiteracy, primary school, junior high school, or high school or above). Anthropometric parameters emphasized body mass index (BMI), categorizing participants as normal weight (BMI < 24), overweight (BMI 24–27.9) or obese (BMI ≥ 28).
Biochemical evaluations included fasting blood glucose, glycated hemoglobin (HbA1c), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C). Serum creatinine and cystatin C levels were used to calculate the sarcopenia index (SI) with the formula: SI = (serum creatinine (mg/dL) / cystatin C (mg/dL)) × 100. The triglyceride-glucose index (TyG), an indicator of insulin resistance, was determined as ln [TG (mg/dL) × fasting plasma glucose (mg/dL) / 2].2,3,17
Clinical data included self-reported histories of hypertension, diabetes, cancer, and kidney diseases. Information on smoking status and alcohol consumption were classified as “never”, “past” or “current”. All data were collected using standardized questionnaires and validated laboratory protocols, ensuring the consistency and reliability essential for robust cardiovascular research. Renal insufficiency is defined as eGFR less than or equal to 60 mL/min/1.73m2, while eGFR is calculated by CKD-EPI, according to serum creatinine, age and gender of the participants.
Outcome
The outcome of this study was the incidence of CVD based on previous study, including heart attack, coronary heart disease, angina and congestive heart failure during the follow-up period.18,19 Information on CVD diagnoses was gathered through standardized questions administered during the CHARLS surveys. Participants were asked: “Have you been diagnosed with heart attack, coronary heart disease, angina, congestive heart failure, or other heart problems by a doctor?” and “Are you currently receiving any of the following treatments (eg, taking Chinese medicine, taking Western medicine, other treatments, or any combination of the above) for heart disease or its complications?” These questions aimed to capture both self-reported diagnoses and ongoing treatment regimens related to CVD.
To ensure data accuracy and reliability, outcome events were assessed by rigorously trained interviewers using standardized questionnaires. All data collection processes adhered to strict quality assurance protocols, including systematic recording and inspection procedures, to minimize errors and enhance the validity of the findings. This approach ensured the consistency and reliability of the outcome data throughout the study period.
Statistical Analysis
This study examined the relationship between the SI and CVD risk. The study population was divided into SI tertiles: Q1 (SI ≤ 71.10), Q2 (71.10 < SI ≤ 84.75), and Q3 (SI > 84.75).
Data normality was evaluated using the Shapiro–Wilk test and histogram visualization. Continuous variables with normal distribution are presented as mean ± standard deviation, while non-normally distributed variables are shown as median (interquartile range). All continuous variables in our study are non-normal distributed, so all the continuous variables are shown as median (interquartile range). Categorical variables are expressed as frequencies and percentages (n (%)). Group comparisons across SI tertiles were conducted using one-way ANOVA for normally distributed data, the Kruskal–Wallis test for non-normally distributed data, and the chi-square test for categorical variables.
The association between SI and CVD incidence was analyzed using univariate and multivariate logistic regression, with odds ratios (ORs) and 95% confidence intervals (CIs) reported. The multivariate model adjusted for age, gender, BMI, smoking and alcohol consumption, education, hypertension, diabetes, and LDL-C level. A restricted cubic spline model (four knots) was applied to explore potential non-linear relationships.
Univariate Cox regression was performed, followed by the inclusion of select variables (P < 0.05) into multivariate Cox proportional hazards models to assess the independent effect of clinical factors on CVD risk.
Cumulative event incidence curve illustrated incidence of CVD across SI tertiles. Subgroup analyses, stratified by age, gender, hypertension, diabetes, smoking consumption, alcohol consumption, residence, and obesity, along with interaction tests, evaluated effect modification and the consistency of the SI-CVD association across diverse subgroups.
All statistical analyses, unless otherwise specified, were conducted using SPSS 25.0. A two-sided P-value < 0.05 was considered statistically significant. The Restricted Cubic Spline (RCS) model was implemented using R language version 4.4.2.
Results
Baseline Characteristics of Study Participants
The basic characteristics of study participants are summarized in Table 1. This study analyzed data from 4979 individuals (Figure 1), with a mean age of 58 years and a slight female predominance (54.1%). The majority were non-hypertensive (75.9%) and non-diabetic (94.6%), and nearly half (48.9%) had an illiteracy educational level. The mean BMI was 23.01 kg/m2, and the SI level was 77.76.
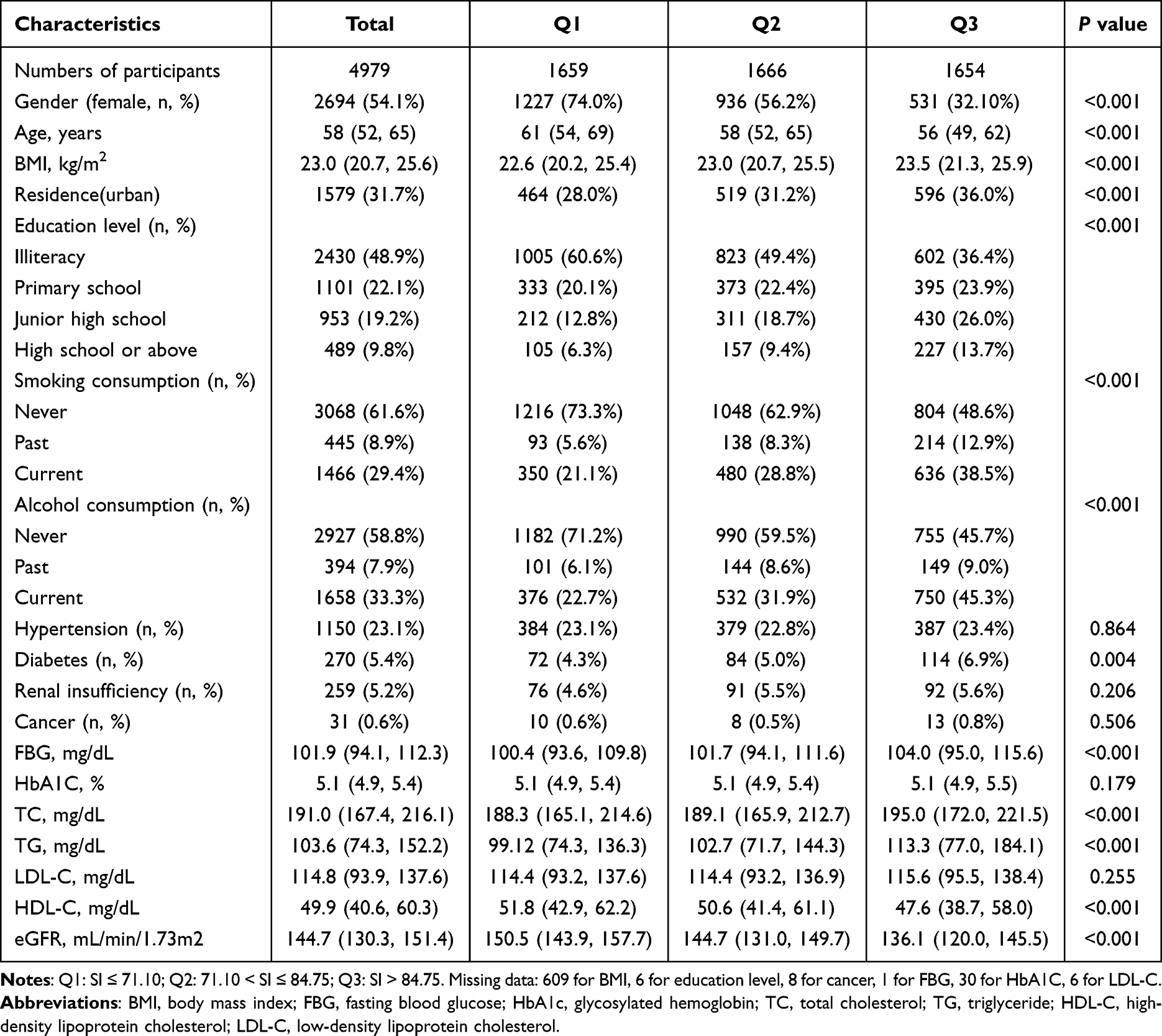 |
Table 1 Baseline Characteristics of Participants |
Participants were categorized into tertiles (Q1-Q3) based on SI levels. A clear trend was observed across SI tertiles, with individuals in higher SI groups exhibiting characteristics indicative of a less favorable metabolic profile. Specifically, higher SI levels were significantly associated with younger age, urban residence, higher education level, current smoking, and alcohol consumption (P < 0.05).
Additionally, participants in higher SI tertiles showed elevated levels of BMI, fasting blood glucose, total cholesterol, triglycerides, and the TyG index. Conversely, HDL-C levels were significantly reduced in the higher SI groups. Differences in diabetes distribution among groups were also observed.
These findings highlight a strong correlation between higher SI levels and a cluster of cardiometabolic risk factors.
Incidence of Cardiovascular Disease and SI Tertiles
This study examined the association between the SI and the incidence of CVD. Over a 9-year follow-up period, 1172 participants (23.5%) developed new-onset CVD. The distribution of CVD events across these tertiles was as follows: 337 participants in the highest SI group (Q3), and 448 and 387 participants in the other two groups, respectively (Figure 2A). Cumulative event incidence curve (Figure 2B) demonstrated a progressive decrease in cumulative CVD incidence across SI tertiles: 27.0% (Q1), 23.2% (Q2), and 20.4% (Q3). The Log rank test identified a statistically significant difference in CVD incidence among the tertiles (P < 0.001), reinforcing the link between lower SI levels and elevated CVD risk.
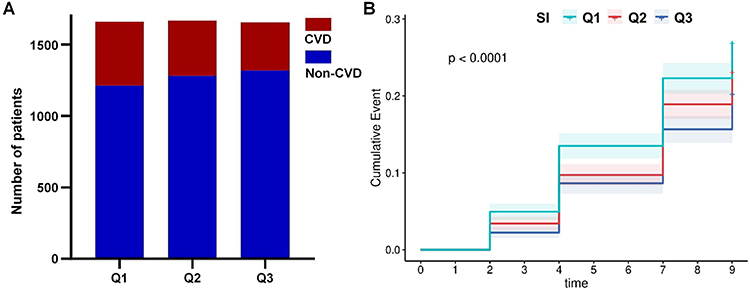 |
Figure 2 Incidence of cardiovascular disease in 2020 and the cumulative event incidence curve of new-onset CVD based on SI levels. Q1: SI ≤ 71.10; Q2: 71.10 < SI ≤ 84.75; Q3: SI > 84.75. (A). The blue column indicates the individuals without cardiovascular diseases in 2020; The red column indicates the individuals with cardiovascular diseases in 2020. (B). Kaplan-Meier survival analysis demonstrated significant difference in CVD incidence among the tertiles. |
Univariable and Multivariable Regression Analyses of SI and CVD Risk
Univariable analysis (Supplementary Figure 1) initially suggested that lower SI levels were associated with a higher risk of CVD (HR, 95% CI: 1.385, 1.202–1.595 for Q1, P < 0.001; HR, 95% CI: 1.158, 1.001–1.340 for Q2, P = 0.049). However, significant differences (P < 0.05) in the distribution of established CVD risk factors (age, gender, hypertension, diabetes, smoking and alcohol consumption, BMI, LDL-C, and education) were observed among the SI tertiles, highlighting the need for multivariable adjustment.
After adjusting for these above confounding factors (age, gender, residence, hypertension, diabetes, smoking consumption, alcohol consumption, BMI, LDL-C and education) in a multivariable model (Figure 3), the relationship between SI and CVD risk was clarified. Lower SI levels remained a significant risk factor for CVD (HR, 95% CI: 1.249, 1.054–1.478 for Q1, P = 0.010). This adjusted analysis, along with the identification of other significant risk factors, provides a more accurate assessment of the independent contribution of SI to the CVD risk.
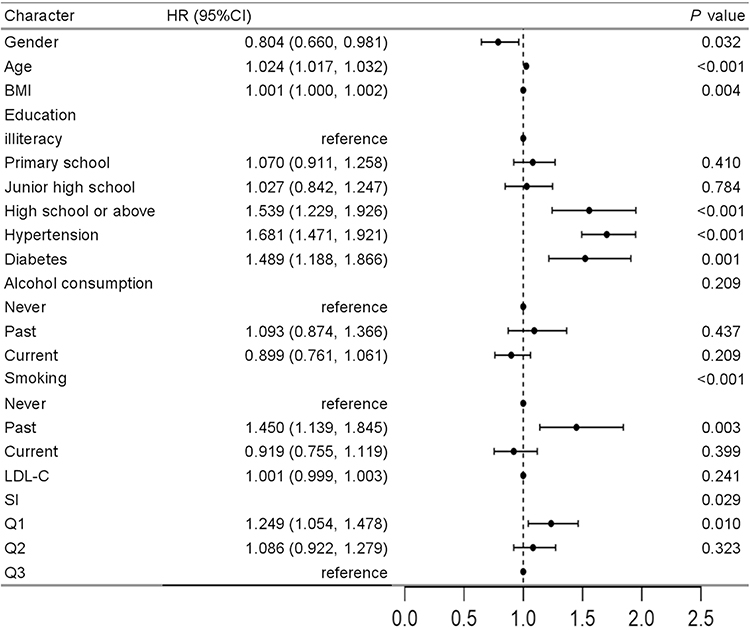 |
Figure 3 Multivariable analysis of risk factors of CVD. Adjusted Model included age, gender, hypertension, diabetes, smoking consumption, alcohol consumption, BMI, LDL-C, education and SI levels. |
Logistic regression models showed a similar pattern (Table 2). And in the fully adjusted model, which accounted for age, gender, hypertension, diabetes, smoking consumption, alcohol consumption, BMI, LDL-C, and education, the risk of CVD occurrence for individuals in Q1 was higher (OR: 1.256, 95% CI: 1.032–1.530, P < 0.05) compared with Q3.
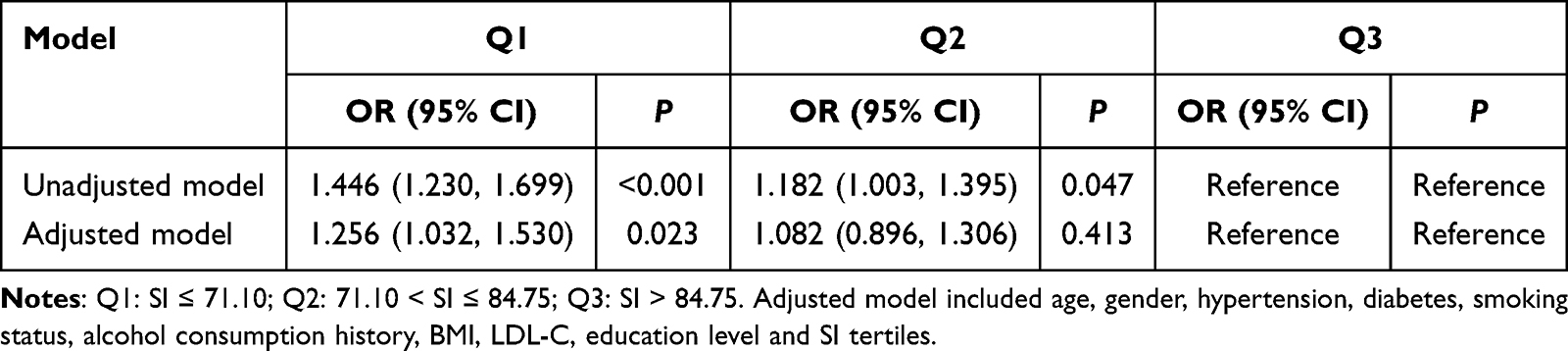 |
Table 2 Binary Logistic Regression Analysis |
Non-Linear Relationship Between SI and CVD
Further analysis, treating SI as a continuous variable (Figure 4), identified a non-linear relationship between SI levels and CVD risk (P = 0.003). The exposure–response relationship exhibited a U-shaped pattern: the lowest hazard was observed at SI values approximately between 90 and 110. While lower SI (< 80) was associated with an elevated risk.
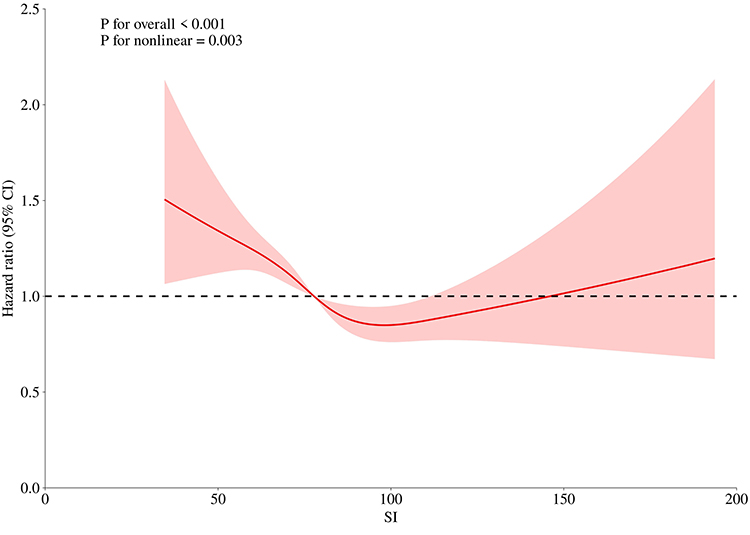 |
Figure 4 Non-linear relationship between SI levels and CVD risk. |
Subgroup Analyses and Interaction Effects
Subgroup analyses (Supplementary Figure 2) were performed to evaluate the consistency of the SI-CVD relationship across various patient populations. In the fully adjusted model (Figure 5), Reduced baseline SI was associated with increased CVD risk in males, current smokers, non-drinkers, BMI ≥ 28kg/m2 and participants without hypertension or diabetes (P < 0.05). Crucially, no significant interactions were detected among the subgroups, indicating that the effect of SI on CVD risk, while potentially more pronounced in certain groups, remains broadly consistent across the studied population. Additional analysis revealed a combined effect of smoking status and SI on CVD onset, underscoring the importance of considering lifestyle factors alongside SI when evaluating CVD risk (interaction P = 0.034). In addition, among the participants without renal insufficiency, reduced SI level was also associated with increased CVD risk (P < 0.05) (Supplementary Figure 3).
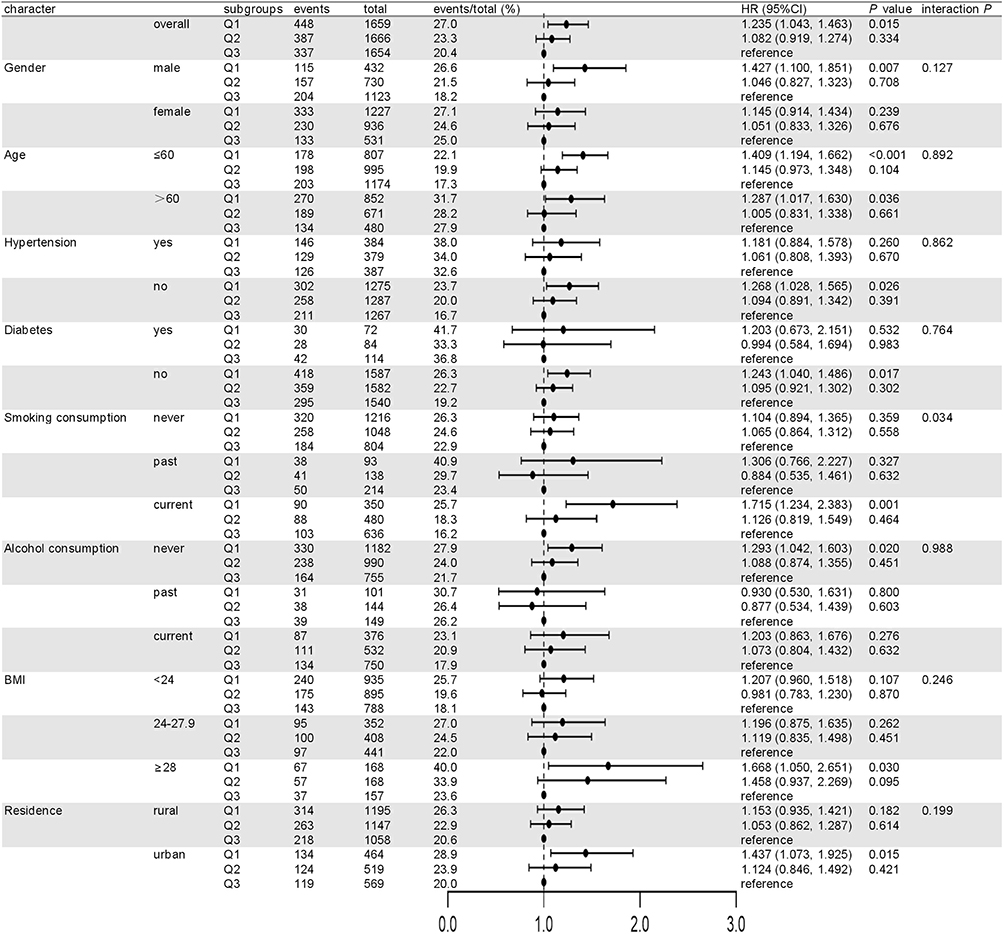 |
Figure 5 Subgroup analysis for the effect of SI on the risk of CVD. Adjusted model included age, gender, hypertension, diabetes, smoking consumption, alcohol consumption, BMI, LDL-C and education. |
Discussion
This study reveals that a lower SI is independently linked to a higher incidence of CVD in a nationally representative cohort of Chinese adults. Even after adjusting for potential confounders such as age, gender, and obesity, the association between lower SI and increased CVD risk remained strong. These findings highlight predictive value of SI in identifying individuals at elevated risk of CVD, presenting a promising opportunity to enhance clinical risk assessment and reduce cardiovascular events.
The Sarcopenia Index, derived from serum creatinine and cystatin C, two routinely measured renal filtration markers,20–22 which has been thoroughly validated for diagnosing sarcopenia and evaluating cancer.12,23,24 This study revealed an inverse relationship between SI tertiles and the incidence of CVD in the general aging population, observed over a 9-year follow-up period within the CHARLS cohort. Importantly, this association remained statistically significant after multivariable adjustment for demographic variables and established cardiovascular risk factors, underscoring the potential role of lower SI as an independent predictor of future CVD events. Further analysis using RCS clarified the nature of this association, demonstrating a non-linear dose-response relationship between continuous SI levels and CVD incidence. Notably, there is a significant lack of data regarding the association between SI and cardiovascular risk specifically within the Chinese population. Lower sarcopenia index was an effective marker for assessing mortality in a Chinese cohort with middle-aged and older adults. And our recent work showed that lower SI effectively predicts aortic valve sclerosis (AVSc) in Coronary Artery Disease (CAD) patients. And a single study in the United States highlighted SI’s predictive performance for cardiovascular death. However, studies explicitly examining SI and CVD incidence remain limited. Thus, our findings provide novel evidence of SI’s predictive capacity for CVD events in this demographic, reinforcing its broader prognostic utility as suggested by existing mortality studies.
Beyond establishing satisfactory discriminability within the overall study population, our Cox regression analysis further elucidated the predictive performance of the SI for CVD across distinct demographic and clinical subgroups. This stratified approach aligns with existing evidence demonstrating significant correlations between SI and traditional sarcopenia metrics, such as total body muscle mass, trunk muscle mass, and skeletal muscle mass index.25 Notably, prior research indicates superior diagnostic utility of SI for sarcopenia in males compared to females,25 a finding congruent with our observation of enhanced CVD predictive value specifically within the male subgroup. Furthermore, our analysis within the obese subgroup corroborates recent findings from the CHARLS database that identified associations between sarcopenia/pre-sarcopenia and CVD prevalence in individuals with obesity.26 Crucially, our study provides novel confirmation of the predictive value of SI for incident cardiovascular events within this high-risk population. Given the substantially elevated baseline CVD risk inherent to obesity, the integration of SI into routine monitoring protocols for these individuals could potentially create a valuable window for initiating early, targeted interventions. Intriguingly, SI demonstrated a more pronounced early warning capacity for CVD among participants without hypertension and diabetes. This phenomenon may stem from the fact that the potent and well-established pathological impacts of metabolic diseases on the cardiovascular system27 could partially mask or overshadow the independent predictive contribution of SI in affected individuals. So, SI may be particularly useful for identifying at-risk individuals without hypertension and diabetes. Previous studies have confirmed greater accuracy in diagnosing sarcopenia in participants patients without renal insufficiency,28 however, in this study, SI performed well in participants with renal insufficiency, as well as in participants without renal insufficiency in early identification of CVD risk. Moreover, our analysis confirmed the stable predictive value in participants aged 60 years or less (interaction P = 0.892). However, smoking status was found to significantly affect the predictive efficacy of SI (interaction P = 0.034), potentially mediated through tobacco components (nicotine, tar, CO, etc)., caused the inflammatory cascades, endothelial dysfunction, and lipid metabolism disorder.29
While the precise pathophysiological mechanisms linking the SI to CVD remain under investigation, current evidence underscores significant associations. SI correlates with subclinical features of CVD,28 demonstrates potential as a biomarker for predicting adverse cardiovascular outcomes following specific procedures, and may act as an early indicator of chronic kidney disease.28,30–34 Early detection of sarcopenia, enabled by accessible metrics like SI, is vital as it facilitates timely interventions. SI could be implematend in various clinical practice, such as integration into annual health checks, used in cardiac rehabilitation programs incorporating exercise prescriptions, applied in preventive cardiology settings, which aimed at reducing cardiovascular mortality in individuals with low SI and potentially halting or reversing adverse cardiovascular progression. However, conventional methods for diagnosing sarcopenia, including CT, MRI, DXA, and Bioelectrical Impedance Analysis (BIA),10 are fraught with limited access, radiation exposure, and high costs, thereby limiting their practicality for widespread community use. In this context, SI, derived from readily available serum creatinine and cystatin C levels, offers a valuable, affordable, and non-invasive surrogate metric, potentially bridging this critical diagnostic gap in identifying individuals at heightened cardiovascular risk associated with sarcopenia.
Limitations
In summary, our study provides the first compelling evidence in a Chinese cohort that lower SI levels are strongly associated with increased CVD risk. As a simple and reliable surrogate marker of sarcopenia, SI can help identify individuals at higher risk for cardiovascular events and may inform earlier interventions. Integrating SI into routine health screenings could substantially improve prevention strategies, especially in subgroups such as obese, non-hypertensive or non-diabetic individuals. Future research with exploration of the underlying mechanism is required to further confirm our findings and optimize SI-based CVD prevention protocols.
However, there are several limitations in the current study. First, this observational study’s design presents inherent challenges in establishing a definitive causal link between SI and CVD occurrences. Second, dependence on self-reported data from the CHARLS database introduces potential biases. Third, serum creatinine or cystatin concentration is significantly impacted by several factors other than renal function and muscle metabolism, such as inflammation, smoking, obesity, diet content, certain medications, and endocrine disorders. The findings should be interpreted cautiously in the above population. Fourth, although encompassing subjects aged 45 and above, further studies are required to assess applicability in younger populations. Fifth, we have not been able to analyze the association between sarcopenia index and all-cause death, Major Adverse Cardiovascular Events (MACE) incidence in the present study and future studies are needed to pinpoint this important questions.
Conclusion
Reduced SI independently predicts elevated CVD risk in aging adults, underscoring its potential as an accessible, cost-effective screening biomarker. Integration of SI into routine clinical assessments may enhance early risk stratification and guide targeted preventive strategies, particularly for high-risk subgroups.
Abbreviations
CHARLS, China Health and Retirement Longitudinal Study; CVD, cardiovascular disease; SI, sarcopenia index.
Ethical Approval
All participants provided written informed consent, and the study adhered to the Declaration of Helsinki, receiving approval from the Peking University Institutional Review Board (IRB00001052-11015).
Author Contributions
Study conception and design: J.S., Y.L. and K.Y. Data analysis: H.Z., J.C., Z.T., J.Z. and Y.W. Data acquisition: A.Z., L.Y., Q.Z. Paper preparation: J.S., L.Y. and K.Y. All authors reviewed the results and agreed on the journal to which the article has been submitted. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Natural Science Foundation of China (82070401), the Cross-disciplinary Research Fund of Shanghai Ninth People’s Hospital, Shanghai JiaoTong University School of Medicine (Grant No. JYJC202413) and sponsored by the Shanghai Pujiang Program (22PJD044).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019. J Am College Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
2. Curcio F, Testa G, Liguori I, et al. Sarcopenia and heart failure. Nutrients. 2020;12(1):211. doi:10.3390/nu12010211
3. Damluji AA, Alfaraidhy M, AlHajri N, et al. Sarcopenia and cardiovascular diseases. Circulation. 2023;147(20):1534–1553. doi:10.1161/CIRCULATIONAHA.123.064071
4. Zuo X, Li X, Tang K, et al. Sarcopenia and cardiovascular diseases: a systematic review and meta‐analysis. J Cachexia Sarcopenia Muscle. 2023;14(3):1183–1198. doi:10.1002/jcsm.13221
5. Gungor O, Sevinc M, Ulu S, Kocyigit I. Sarcopenia and cardiovascular disease in patients with and without kidney disease: what do we know? Int Urol Nephrol. 2022;55(5):1161–1171. doi:10.1007/s11255-022-03393-0
6. Zhang N, Zhu WL, Liu XH, et al. Prevalence and prognostic implications of sarcopenia in older patients with coronary heart disease. J Geriatr Cardiol. 2019;16(10):756–763. doi:10.11909/j.issn.1671-5411.2019.10.002
7. Shim GY, Kim M, Won CW. Cross‐sectional and longitudinal association between atrial fibrillation and sarcopenia: findings from the Korean frailty and aging cohort study. J Cachexia Sarcopenia Muscle. 2023;15(1):434–441. doi:10.1002/jcsm.13401
8. Nishikawa H, Fukunishi S, Asai A, Yokohama K, Nishiguchi S, Higuchi K. Pathophysiology and mechanisms of primary sarcopenia (review). IntJ Mol Med. 2021;48(2). doi:10.3892/ijmm.2021.4989
9. Cho M-R, Lee S, Song S-K. A review of sarcopenia pathophysiology, diagnosis, treatment and future direction. J Korean Med Sci. 2022;37(18). doi:10.3346/jkms.2022.37.e146
10. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised european consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
11. Beaudart C, McCloskey E, Bruyère O, et al. Sarcopenia in daily practice: assessment and management. BMC Geriatr. 2016;16(1). doi:10.1186/s12877-016-0349-4
12. Lin Y-L, Chen S-Y, Lai Y-H, et al. Serum creatinine to cystatin c ratio predicts skeletal muscle mass and strength in patients with non-dialysis chronic kidney disease. Clin Nutr. 2020;39(8):2435–2441. doi:10.1016/j.clnu.2019.10.027
13. Chen X, Crimmins E, Hu PP, et al. Venous blood-based biomarkers in the China health and retirement longitudinal study: rationale, design, and results from the 2015 wave. Am J Epidemiol. 2019;188(11):1871–1877. doi:10.1093/aje/kwz170
14. Wu Z, Zhang H, Miao X, et al. High-intensity physical activity is not associated with better cognition in the elder: evidence from the China health and retirement longitudinal study. Alzheimer’s Res Ther. 2021;13:182.
15. Shen Y, Shi Q, Nong K, et al. Exercise for sarcopenia in older people: a systematic review and network meta‐analysis. J Cachexia Sarcopenia Muscle. 2023;14(3):1199–1211. doi:10.1002/jcsm.13225
16. Chen L-K, Liu L-K, Woo J, et al. Sarcopenia in Asia: consensus report of the asian working group for sarcopenia. J Am Med Directors Assoc. 2014;15(2):95–101. doi:10.1016/j.jamda.2013.11.025
17. Sanchez-Rodriguez D, Marco E, Cruz-Jentoft AJ. Defining sarcopenia: some caveats and challenges. Curr Opin Clin Nutr Metab Care. 2020;23(2):127–132. doi:10.1097/MCO.0000000000000621
18. Ren Q, Huang Y, Liu Q, Chu T, Li G, Wu Z. Association between triglyceride glucose-waist height ratio index and cardiovascular disease in middle-aged and older Chinese individuals: a nationwide cohort study. Cardiovasc Diabetol. 2024;23(1). doi:10.1186/s12933-024-02336-6
19. Huang Q, Jiang Z, Shi B, et al. Characterisation of cardiovascular disease (cvd) incidence and machine learning risk prediction in middle-aged and elderly populations: data from the China health and retirement longitudinal study (charls). BMC Public Health. 2025;25:518.
20. Malmgren L, Grubb A. Muscle mass, creatinine, cystatin c and selective glomerular hypofiltration syndromes. Clin Kidney J. 2023;16(8):1206–1210. doi:10.1093/ckj/sfad086
21. Fujita K, Ohkubo H, Nakano A, et al. Serum creatinine/cystatin c ratio is a surrogate marker for sarcopenia in patients with idiopathic pulmonary fibrosis. BMC Pulm Med. 2022;22(1). doi:10.1186/s12890-022-02000-3
22. Ren C, Su H, Tao J, Xie Y, Zhang X, Guo Q. Sarcopenia index based on serum creatinine and cystatin c is associated with mortality, nutritional risk/malnutrition and sarcopenia in older patients. Clin Interventions Aging. 2022;17:211–221. doi:10.2147/CIA.S351068
23. Kashani KB, Frazee EN, Kukrálová L, et al. Evaluating muscle mass by using markers of kidney function: development of the sarcopenia index. Crit Care Med. 2017;45(1):e23–e29. doi:10.1097/CCM.0000000000002013
24. Wilkinson TJ, Baker LA, Watson EL, Smith AC, Yates T. Diagnostic accuracy of a ‘sarcopenia index’ based on serum biomarkers creatinine and cystatin c in 458,702 uk biobank participants. Clin Nutr ESPEN. 2024;63:207–213. doi:10.1016/j.clnesp.2024.06.041
25. Yamada Y, Umegaki H, Sugimoto T, et al. Relationship of creatinine cystatin c ratio with muscle mass and grip strength in memory clinic outpatients. Exp Gerontol. 2022;168:111935. doi:10.1016/j.exger.2022.111935
26. Jiang M, Ren X, Han L, Zheng X. Associations between sarcopenic obesity and risk of cardiovascular disease: a population-based cohort study among middle-aged and older adults using the charls. Clin Nutr. 2024;43(3):796–802. doi:10.1016/j.clnu.2024.02.002
27. Nagy AC, Zaninotto P, Steptoe A, Shim E-J. Cvd incidence and mortality among people with diabetes and/or hypertension: results from the English longitudinal study of ageing. PLoS One. 2024;19:e0303306.
28. Campos AM, Moura FA, Santos SN, Freitas WM, Sposito AC. Sarcopenia, but not excess weight or increased caloric intake, is associated with coronary subclinical atherosclerosis in the very elderly. Atherosclerosis. 2017;258:138–144. doi:10.1016/j.atherosclerosis.2017.01.005
29. Kondo T, Nakano Y, Adachi S, Murohara T. Effects of tobacco smoking on cardiovascular disease. Circ J. 2019;83(10):1980–1985. doi:10.1253/circj.CJ-19-0323
30. Thongprayoon C, Cheungpasitporn W, Kashani K. Serum creatinine level, a surrogate of muscle mass, predicts mortality in critically ill patients. J Thoracic Dis. 2016;8(5):E305–E311. doi:10.21037/jtd.2016.03.62
31. Plytzanopoulou P, Politis P, Papachrysanthou T, et al. Creatinine index as a predictive marker of sarcopenia in patients under hemodialysis. Int Urol Nephrol. 2021;54(7):1565–1573. doi:10.1007/s11255-021-03032-0
32. Aldenbratt A, Lindberg C, Johannesson E, Hammarsten O, Svensson MK. Estimation of kidney function in patients with primary neuromuscular diseases: is serum cystatin c a better marker of kidney function than creatinine? J Nephrol. 2021;35(2):493–503. doi:10.1007/s40620-021-01122-x
33. Viollet L, Gailey S, Thornton DJ, et al. Utility of cystatin c to monitor renal function in duchenne muscular dystrophy. Muscle Nerve. 2009;40(3):438–442. doi:10.1002/mus.21420
34. Adingwupu OM, Barbosa ER, Palevsky PM, Vassalotti JA, Levey AS, Inker LA. Cystatin c as a gfr estimation marker in acute and chronic illness: a systematic review. Kidney Med. 2023;5(12):100727. doi:10.1016/j.xkme.2023.100727
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Dual Role of Extracellular Vesicles in Aging and Age-Related Diseases: Pathophysiology and Therapeutic Potential
Zhu Y, Fang X, Zhang S, Liao Y, Lin H, Chen P, Yang M, Huang J, Wang X
International Journal of Nanomedicine 2026, 21:589123
Published Date: 4 March 2026
Prediction Model for Frailty in Middle-Aged and Older Adults with Cardiovascular Disease
Yang X, Zhou H, Huang C, Yuan M, Du X, Zhang C
Vascular Health and Risk Management 2026, 22:581066
Published Date: 17 March 2026