Back to Journals » International Journal of Women's Health » Volume 17
Association Between Reproductive Lifespan and All-Cause and Cardiovascular Mortality in Women Aged 65 Years and Older: A Cohort Study Using NHANES 1999–2018 Data
Authors Chen X, Li C ![]() , Bai Y, Li L
, Bai Y, Li L ![]()
Received 17 September 2025
Accepted for publication 19 December 2025
Published 25 December 2025 Volume 2025:17 Pages 5609—5622
DOI https://doi.org/10.2147/IJWH.S568174
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Xiaohui Chen, Chunxue Li, Yue Bai, Lin Li
Department of Cardiovascular, The Second Hospital of Jilin University, Changchun, People’s Republic of China
Correspondence: Lin Li, Department of Cardiovascular, The Second Hospital of Jilin University, No. 218, Zi Qiang Street, Nanguan Zone, Changchun, Jilin, 130041, People’s Republic of China, Tel +8619975320351, Email [email protected]
Purpose: The association between reproductive lifespan and all-cause and cardiovascular mortality in women aged ≥ 65 years remains unclear. We examined this association in a nationally representative sample of older US women using NHANES data.
Patients and Methods: The study included postmenopausal women aged 65 years and older from the NHANES database as our study cohort. Throughout the analyses, NHANES sampling weights were applied to account for the complex survey design, and multiple imputation were used to deal with missing values. Multivariable Cox regression, restricted cubic splines, Kaplan–Meier survival curves, and subgroup analyses were used to estimate the associations between reproductive lifespan and both all-cause and cardiovascular mortality. Additionally, sensitivity analyses were performed to verify the robustness of the results.
Results: Among 4514 participants followed for a median of 101 months, all-cause mortality occurred in 1843 (38.67%) and cardiovascular mortality in 512 (10.74%). A linear relationship was observed between reproductive lifespan and all-cause mortality; in the fully adjusted model, for each additional year of reproductive lifespan, the risk of all-cause mortality decreased by 1% (HR = 0.99, 95% CI 0.98– 0.99, p < 0.001). Conversely, the relationship between reproductive lifespan and cardiovascular mortality followed an L-shaped curve. Further threshold-effect analysis identified an inflection point at 36 years: for reproductive lifespan < 36 years, each additional year conferred a 2% reduction in cardiovascular mortality risk (HR = 0.98, 95% CI 0.95– 1.00, p = 0.033), whereas the protective effect plateaued when reproductive lifespan ≥ 36 years.
Conclusion: Short reproductive lifespan may be associated with an increased risk of all-cause and cardiovascular mortality. Greater attention should be given to women with a short reproductive lifespan.
Keywords: reproductive lifespan, all-cause mortality, cardiovascular mortality, NHANES, cohort study
Introduction
Estrogen, a protective sex hormone, is widely recognized for its beneficial effects on cardiovascular health. This leads to sex differences in cardiovascular health: men have a higher incidence of CVD, whereas women experience myocardial infarction approximately 10 years later and exhibit lower cardiovascular mortality.1–3 Following menopause, the decline in estrogen levels significantly increases the risk of cardiovascular mortality in women.4,5 With increasing life expectancy, women now spend nearly 40% of their lives in the postmenopausal state.6 Consequently, female-specific indicators, such as menstrual factors, are increasingly recognized for their significant influence on women’s health. However, associations of age at menarche or menopause with all-cause or cardiovascular mortality remain inconsistent.7–10 Reproductive lifespan, defined as the period between menarche and menopause, is a critical indicator of a woman’s reproductive health and can be used to estimate cumulative estrogen exposure.8,11–13 Previous studies have linked a shorter reproductive lifespan to a higher risk of cardiovascular disease and a longer reproductive lifespan to lower all-cause mortality.8,13,14 Population aging is a global phenomenon, and cardiovascular mortality increases with age.15 The United Nations’ World Population Prospects 2024 defines aging by the proportion of the population aged ≥65 years; however, the relationship between reproductive lifespan and mortality risk in women aged ≥65 remains unclear.16
We hypothesized that reproductive lifespan is associated with all-cause and cardiovascular mortality among women aged 65 years and older and then analyzed data from NHANES (1999–2018). To our knowledge, this is the first nationally representative study to evaluate the association in US women aged 65 years and older.
Materials and Methods
Study Design and Population
The National Health and Nutrition Examination Survey (NHANES), managed by the National Center for Health Statistics (NCHS) within the US Centers for Disease Control and Prevention (CDC), employs a complex, stratified, multistage probability design to assess the health and nutritional status of the US population.17 Conducted biennially and reviewed by the NCHS Research Ethics Review Board, the programme requires all participants to provide written informed consent. Because the anonymised datasets are publicly available, secondary analyses are exempt from additional institutional review board approval and can be downloaded directly from the NHANES portal (http://www.cdc.gov/nchs/nhanes.htm).18 This investigation followed the STROBE Statement for reporting observational research and conformed to the ethical principles of the Declaration of Helsinki.19,20
Data were extracted from ten consecutive cycles of NHANES (1999–2018), conducted immediately before the COVID-19 pandemic and with publicly available mortality follow-up. Among 51,423 women who completed the interview component, 5140 were postmenopausal and aged≥65 years, after excluding 626 participants with missing information on vital status, age at menarche, or menopausal status, the final analytic cohort comprised 4514 women (Figure 1).
 |
Figure 1 Flowchart of study population. |
We calculated reproductive lifespan as the age at menopause minus the age at menarche in postmenopausal women.11 Age at menarche and age at menopause were determined based on their responses to questions in the reproductive health questionnaire: “Age when first menstrual period occurred” and “Age at last menstrual period”.
The primary outcomes of this study were all-cause and cardiovascular mortality, which were obtained from the National Death Index (NDI) up to December 31, 2019.21 Cardiovascular mortality was documented using the International Classification of Diseases, 10th Revision (I00–I09, I11, I13, and I20–I51) coding system. Additionally, the number of survival months from the study’s commencement to the occurrence of death or the follow-up endpoint was calculated.
Based on clinical experience and previous research, the covariates in our study included age, marital status, race/ethnicity, education level, family income, smoking status, alcohol use, and body mass index (BMI).22,23 To mitigate the influence of other reproductive factors on all-cause and cardiovascular mortality, we included contraceptives use, number of pregnancies female hormone use as covariates. Since reproductive lifespan was defined from age at menarche and menopause, these two variables were excluded from the primary covariate set; for subgroup analyses they were subsequently categorized around their weighted mean values. Furthermore, the study participants were drawn from 10 cycles of NHANES, and to minimize the bias associated with longer follow-up periods, we included NHANES cycles as covariates.
Age is calculated by the CDC from the participant’s self-reported date of birth collected at the household interview. Marital status was categorized as married/living with a partner or living alone. The race-ethnicity classification adheres to NHANES standards: Mexican American, Other Hispanic, Non-Hispanic black, Non-Hispanic white, or Others,24 The education level was categorized as follows: less than high school (less than 9th grade), high school or equivalent (9–11th grade), and above high school (High school graduate/GED or equivalent, Some college or AA degree, College graduate or above).25 The ratio of family income to poverty (PIR) was used to characterize family income level and was categorized into low (PIR≤1.30), medium (1.30 < PIR≤3.50), and high (PIR > 3.50) groups.26 Smoking status was categorized as never (smoked <100 cigarettes in life), former (smoked ≥100 cigarettes in their lifetime but does not currently smoke), and current (smoked ≥100 cigarettes in their lifetime and currently smokes). Alcohol use was classified as never, former, mild, moderate or heavy according to the method published in previous NHANES-based studies.27 BMI was calculated from self-reported height and weight (kg/m2), in subgroup analyses, categorized as <25 and ≥25 kg/m2, to determine whether the individual is overweight.28 Contraceptives use was determined based on participants’ responses to the question “Have you ever taken birth control pills?” Number of pregnancies was categorized into four groups: ≤2, 3, 4 and ≥5.29 No multicollinearity was detected among all the covariates. The results of the multicollinearity test are presented in Supplementary Table 1.
In accordance with NHANES analytic guidelines, sampling weights and design variables were incorporated into all analyses; the Mobile Examination Center (MEC) examination weight served as the primary weight, together with strata (SDMVSTRA) and primary sampling units (SDMVPSU), to yield nationally representative estimates of the US civilian non-institutionalized population. The weights were calculated as follows: for 1999–2002, weight = (2/10)*(4-year MEC examination weight); for all other cycles, weight = (1/10)*(2-year MEC examination weight). After applying these weights, the analytic sample corresponded to an estimated15,446,717postmenopausal women aged ≥ 65 years in the US population.
Statistical Analysis
In this study, categorical variables are presented as unweighted number (weighted percentage), continuous variables are summarized as mean (standard deviation) if normally distributed, or as median (interquartile range, IQR) if skewed. Group comparisons were conducted using the χ2-test for categorical variables, one-way analysis of variance (ANOVA) for normally distributed continuous variables, and the Kruskal–Wallis test for skewed continuous variables. Multivariable Cox regression analysis was conducted to examine the association between reproductive lifespan and all-cause and cardiovascular mortality following multiple imputation of missing data (marital status: 49, 1.09%; education level: 11, 0.24%; family income: 458, 10.15%; smoking status: 5, 0.11%; alcohol use: 342, 7.58%; BMI: 134, 2.97%; contraceptives use: 15, 0.33%; number of pregnancies: 6, 0.13%; female hormone use: 27, 0.60%). Prior to analysis, we evaluated the proportional-hazards assumption using Schoenfeld residuals, as shown in Supplementary Figures 1 and 2. Reproductive lifespan was analyzed both continuously—hazard ratios (HRs) expressed per one-year increase—and categorically. Four models were constructed: Model 1 was a crude model without any covariate adjustments. Model 2 was adjusted for sociodemographic characteristics including age, marital status, race/ethnicity, education level, and family income. Model 3 further adjusted for smoking status, alcohol use, and BMI. Model 4 further adjusted for contraceptives use, number of pregnancies, female hormone use and NHANES cycles. Additionally, after adjusting for variables in Model 4, restricted cubic splines (RCS) were provided to further explore the dose–response relationship between reproductive lifespan and both all-cause and cardiovascular mortality risk. The cumulative mortality rates were assessed using Kaplan–Meier survival curves based on the binary classification of reproductive lifespan and were evaluated utilizing the Log rank test. Participants lost to follow-up were censored at their last known time point.
Furthermore, we performed the following sensitivity analysis. First, to examine potential effect modification we treated reproductive lifespan as binary (< 35 vs ≥ 35 years). Survey-weighted Cox models included cross-product terms between reproductive lifespan and each of the following modifiers: age at menarche (< 13 vs ≥ 13 years), age at menopause (< 48 vs ≥ 48 years), contraceptive use, female hormone use, BMI (< 25 vs ≥ 25 kg/m2), marital status, race/ethnicity, education, and family income. The p for interaction was derived from the likelihood-ratio test. Stratum-specific hazard ratios are displayed for visual inspection. Second, restricted mean survival time was compared between the dichotomized reproductive lifespan groups to quantify the associated clinical benefit. Additionally, we performed multivariable analyses on the following modified datasets as sensitivity analyses to verify result robustness: 1. Used tertiles of reproductive lifespan. 2. Excluded all participants with any missing covariates. 3. Added surgical menopause as an adjusted covariate. 4. Excluded participants who had undergone surgical menopause. 5. Excluded participants with age at menarche > 20 years or age at menopause > 60 or < 30 years.30
All analyses were performed using the statistical software packages R4.2.2 (http://www.R-project.org, The R Foundation)and Free Statistics software version 2.3.Statistics were considered significant when two-sided p values were <0.05.
Results
Characteristics of the Participants
The baseline characteristics of the 4514 participants with available data are presented in Table 1. Over a median follow-up of 101 months, 1843 (38.67%) all-cause mortality and 512 (10.74%) cardiovascular mortality were recorded. Participants were dichotomized according to their reproductive lifespan values, using the median value of 35 years as the cut-off, yielding 2088 individuals with reproductive lifespan < 35 years and 2426 with reproductive lifespan≥35 years. Compared with those in the shorter reproductive lifespan (< 35years) group, participants with longer reproductive lifespan (≥ 35years) were more likely to have a partner, higher educational attainment, and greater family income. They also exhibited earlier age at menarche, later age at menopause, and differed with respect to race/ethnicity, smoking status, and alcohol use.
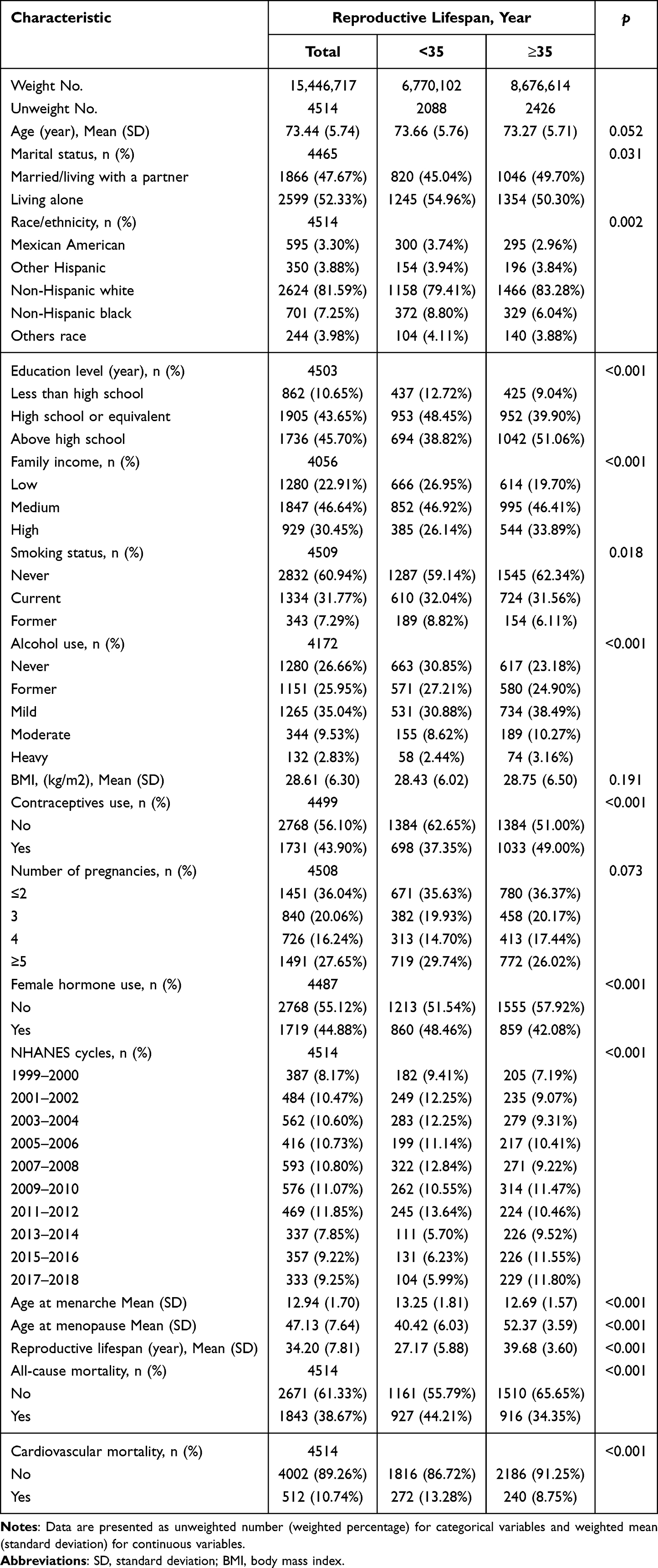 |
Table 1 Baseline Characteristics of Study Participants by Binary Classification of Reproductive Lifespan |
Association of Reproductive Lifespan with All-Cause and Cardiovascular Mortality
Multivariable Cox regression was used to examine the associations between reproductive lifespan and both all-cause and cardiovascular mortality, treating reproductive lifespan as continuous, dichotomized (Table 2). In the fully adjusted model, each 1-year increase in reproductive lifespan was associated with a 1% lower risk of all-cause mortality and a 2% lower risk of cardiovascular mortality. When reproductive lifespan was analyzed categorically, compared with those whose reproductive lifespan was≥35 years, participants with reproductive lifespan < 35 years had a 13% higher risk of all-cause mortality and a 33% higher risk of cardiovascular mortality. These associations remained statistically significant across all adjusted models.
 |
Table 2 Multivariable Regression Between Reproductive Lifespan and All-Cause and Cardiovascular Mortality Risk |
RCS were employed to model the dose–response relationship, and non-linearity was formally evaluated with the generalized additive model for associations between reproductive lifespan and both all-cause (Figure 2) and cardiovascular mortality (Figure 3). A significant non-linear association with cardiovascular mortality was observed (p for non-linearity =0.031). A two-segment linear regression identified the inflection point at 36 years, after which a piecewise Cox proportional-hazards model was fitted (Table 3). Cardiovascular mortality declined progressively with increasing reproductive lifespan up to 36 years, with no further reduction beyond this threshold.
 |
Table 3 Threshold Effect Analysis of the Relationship Between Reproductive Lifespan and Cardiovascular Mortality Risk |
 |
Figure 2 Dose-response relationship between reproductive lifespan and all-cause mortality. NHANES examination weights (MEC), strata (SDMVSTRA) and PSU (SDMVPSU) applied. Solid and shaded represent the predicted value and 95% CI. They were adjusted for age, marital status, race/ethnicity, education level, family income, smoking status, alcohol use, BMI, contraceptives use, number of pregnancies, female hormone use and NHANES cycles. 99% of the data is shown. |
 |
Figure 3 Dose-response relationship between reproductive lifespan and cardiovascular mortality. NHANES examination weights (MEC), strata (SDMVSTRA) and PSU (SDMVPSU) applied. Solid and shaded represent the predicted value and 95% CI. They were adjusted for age, marital status, race/ethnicity, education level, family income, smoking status, alcohol use, BMI, contraceptives use, number of pregnancies, female hormone use and NHANES cycles. 99% of the data is shown. |
Kaplan-Meier survival curves for all-cause and cardiovascular mortality according to binary reproductive lifespan are shown in Figures 4 and 5, respectively. With the median (35 years) as the cut-off, participants with reproductive lifespan<35 years exhibited significantly higher risks of both all-cause and cardiovascular mortality than those with reproductive lifespan≥35 years.
 |
Figure 4 Kaplan–Meier curves of all-cause mortality according to reproductive lifespan status for women aged 65 years and older. NHANES examination weights (MEC), strata (SDMVSTRA) and PSU (SDMVPSU) applied. Participants were split at the median reproductive lifespan (median = 35 years). The numbers at risk are shown below the plots. |
 |
Figure 5 Kaplan–Meier curves of cardiovascular mortality according to reproductive lifespan status for women aged 65 years and older. NHANES examination weights (MEC), strata (SDMVSTRA) and PSU (SDMVPSU) applied. Participants were split at the median reproductive lifespan (median = 35 years). The numbers at risk are shown below the plots. |
Sensitivity Analysis
Subgroup analyses (Supplementary Table 2) showed no significant interactions (all p for interaction > 0.05). Restricted mean survival time analysis (Supplementary Table 3) confirmed that women with a reproductive lifespan ≥35 years had significantly longer mean survival, indicating a clinical benefit. Additionally, we conducted multivariable analyses across several modified datasets, and the robustness of the findings was confirmed (Supplementary Tables 4–8).
Discussions
In our study, leveraging the large-scale, nationally representative NHANES database, we validated that a shorter reproductive lifespan is associated with an increased risk of all-cause mortality among US women aged 65 and older: reproductive lifespan showed an inverse linear association with all-cause mortality: every additional year of reproductive lifespan was linked to a proportional reduction in death risk. In contrast, its relationship with cardiovascular mortality was L-shaped, plateauing after 36 years. An article from Circulation emphasized that it is essential to incorporate female-specific risk factors into quantitative risk assessments conducted across the lifespan.31
An article from Circulation emphasized that it is essential to incorporate female-specific risk factors into quantitative risk assessments conducted across the lifespan. Compared with studying menarche or menopause in isolation, reproductive lifespan offers a more comprehensive measure of cumulative estrogen exposure.13 Although reproductive lifespan is jointly determined by age at menopause and age at menarche, Table 1 shows that the variation in menopausal age is substantially greater than that in menarcheal age. These results are consistent with those reported by other researchers.32,33 Consequently, differences in reproductive lifespan appear to be primarily driven by the timing of menopause, even though age at menarche remains an important contributing factor. According to longitudinal analyses of US women, the mean age at menarche decreased by 1.2 years between 1959 and 2018, in contrast to a 1.5-year increase in menopausal age, resulting in a net gain of 2.1 years in reproductive lifespan.11 Many reproductive traits in women are known to be highly heritable; age at menopause, in particular, is highly heritable; nevertheless, it is also influenced by multiple environmental and lifestyle factors.34–38
Cardiovascular disease remains the leading cause of death in women. While estrogen confers cardioprotection, the onset of menopause and accompanying ovarian failure lead to a marked increase in coronary heart disease prevalence.39 As the population ages, the health of older women has become an expanding public-health priority, with female-specific risk factors receiving increasing attention.40,41 To further elucidate sex-specific determinants of all-cause and cardiovascular mortality among postmenopausal women, numerous studies have been conducted on reproductive factors. Despite differences in study populations, grouping criteria, and adjustment variables, early menopause appears to be consistently recognized as a risk factor. A systematic review that included 32 studies indicated that women who experienced menopause before age 45 had a cardiovascular disease mortality rate of 1.19 (95% CI 1.08–1.31) compared with those who reached menopause at or after age 45.42 The 2021 ESC Guidelines on Cardiovascular Disease Prevention designate premature menopause as a sex-specific risk factor for CVD.43 A study utilizing the NHANES database reported that earlier menopause is associated with an elevated risk of cardiovascular disease (CVD), further supporting a bidirectional relationship whereby early-onset CVD also significantly increases the risk of premature menopause.44 However, a Mendelian randomization study found no association between age at menopause and cardiovascular disease.9 Menarche marks the onset of menstruation and sexual maturity within the reproductive endocrine system and has also been shown to be associated with cardiovascular health. In the Nurses’ Health Study, multivariable adjustment showed that compared with women who experienced menarche at 13 years, menarche at ≤10 years had a cardiovascular disease risk of 1.22 (95% CI 1.09–1.36).10 They have also observed that early age at menopause and a shorter reproductive lifespan were associated with a higher risk of cardiovascular disease. A study conducted on Swedish women confirmed that a shorter reproductive lifespan is associated with an increased risk of cardiovascular events and all-cause mortality. This association remained consistent after excluding women who underwent surgical menopause.45 This is consistent with our findings. However, it is important to note that a minority of studies have reached different conclusions. For instance, a study from Norway reported that among women aged 60 years or older, the risk of atrial fibrillation was not associated with age at menarche, reproductive lifespan, or age at menopause.46 Indeed, it has even been reported that a longer reproductive lifespan and cumulative estrogen exposure were associated with an increased risk of all-cause mortality.47 And a multivariable-adjusted, twin-matched, case-control analysis showed no significant association between the reproductive period and mortality.48 Given the marked heterogeneity across current findings, large-scale, prospective cohort studies are now urgently warranted. Moreover, the biological pathways linking reproductive lifespan to cardiovascular health—and ultimately to mortality—remain poorly delineated. Although estrogen-driven activation of genomic (ERα/ERβ) and non-genomic (GPER) receptors has been postulated to confer cardioprotection in women by modulating calmodulin, caveolin-1, RhoA, nitric oxide, and Mdm2 via functional interactions with G-protein–coupled receptor kinase-2 (GRK2), 40 rigorous mechanistic studies are still required to validate these hypotheses and to uncover any additional mediators.49
Our study utilized complete-cycle data from the NHANES database prior to the COVID-19 pandemic, the survey was meticulously designed, collected, and processed in accordance with NHANES standards to minimize non-sampling and measurement errors, and sampling weights and design variables were employed to increase the extrapolation of results. Then, we identified a threshold relationship between reproductive lifespan and cardiovascular mortality, with the inflection point located near the median—an observation not previously reported. This finding underscores the need for heightened surveillance of women whose reproductive lifespan falls below the median. Moreover, we conducted sensitivity analyses to ensure the robustness of our findings. Collectively, these measures enhance the accuracy and validity of our results. However, our research has certain limitations. First, as a retrospective cohort study, there is a potential for recall bias. Additionally, despite adjustment for an extensive covariate set, residual or unmeasured confounding cannot be ruled out. Third, the race-ethnicity classification adheres to NHANES standards; however, collapsing minority groups such as Asians and American Indians/Alaska Natives into an “other” category may obscure important between-group differences. In addition, the cross-sectional design of NHANES means that period-specific reproductive-hormone data and details on the timing and dosage of female hormone use are unavailable. Therefore, large prospective cohorts with repeated hormone measurements and long-term mortality follow-up are needed to clarify the relationship between reproductive lifespan and both all-cause and cardiovascular mortality.
Conclusion
Reproductive lifespan may be associated with all-cause and cardiovascular mortality; in particular, we observed an L-shaped relationship between reproductive lifespan and cardiovascular death, with a critical threshold at 36 years. This easily ascertained variable could be considered as a female-specific risk enhancer in cardiovascular risk assessment. Further prospective, longitudinal studies are warranted to confirm its clinical significance.
Abbreviations
NHANES, National Health and Nutrition Examination Survey; NCHS, National Center for Health Statistics; CDC, US Centers for Disease Control and Prevention; NDI, National Death Index; BMI, body mass index; PIR, ratio of family income to poverty; MEC, Mobile Examination Center; IQR, interquartile range; HRs, hazard ratios; RCS, restricted cubic splines; CVD, cardiovascular disease.
Data Sharing Statement
The National Health and Nutrition Examination Survey (NHANES) data are publicly available at https://wwwn.cdc.gov/nchs/nhanes. Further inquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
NHANES is conducted by the Centers for Disease Control and Prevention (CDC) and the National Center for Health Statistics (NCHS). The National Center for Health Statistics Research Ethics Review Board (NCHS ERB) reviewed and approved the study, all participants signed written informed consent.The analyses presented in this article were exempt from approval by The Second Hospital of Jilin University based on national legislation guidelines, item 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China.
Acknowledgments
We gratefully thank Jie Liu (Department of Vascular and Endovascular Surgery, Chinese PLA General Hospital) for his contribution to the statistical support, consultations, and comments regarding the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Regitz-Zagrosek V, Kararigas G. Mechanistic pathways of sex differences in cardiovascular disease. Physiol Rev. 2017;97(1):1–37. doi:10.1152/physrev.00021.2015
2. Morselli E, Santos RS, Criollo A, Nelson MD, Palmer BF, Clegg DJ. The effects of oestrogens and their receptors on cardiometabolic health. Nat Rev Endocrinol. 2017;13(6):352–364. doi:10.1038/nrendo.2017.12
3. Lv Y, Cao X, Yu K, et al. Gender differences in all-cause and cardiovascular mortality among US adults: from NHANES 2005-2018. Front Cardiovasc Med. 2024;11:1283132. doi:10.3389/fcvm.2024.1283132
4. Thurston RC, Bhasin S, Chang Y, et al. Reproductive hormones and subclinical cardiovascular disease in midlife women. J Clin Endocrinol Metab. 2018;103(8):3070–3077. doi:10.1210/jc.2018-00579
5. Dunneram Y, Greenwood DC, Cade JE. Diet, menopause and the risk of ovarian, endometrial and breast cancer. Proc Nutr Soc. 2019;78(3):438–448. doi:10.1017/S0029665118002884
6. Dong L, Teh DBL, Kennedy BK, Huang Z. Unraveling female reproductive senescence to enhance healthy longevity. Cell Res. 2023;33(1):11–29. doi:10.1038/s41422-022-00718-7
7. Charalampopoulos D, McLoughlin A, Elks CE, Ong KK. Age at menarche and risks of all-cause and cardiovascular death: a systematic review and meta-analysis. Am J Epidemiol. 2014;180(1):29–40. doi:10.1093/aje/kwu113
8. Lockhart PA, Martin P, Johnson MA, Shirtcliff E, Poon LW. The relationship of fertility, lifestyle, and 7.longevity among women. J Gerontol a Biol Sci Med Sci. 2017;72(6):754–759. doi:10.1093/gerona/glw158
9. Ardissino M, Slob EAW, Carter P, et al. Sex-specific reproductive factors augment cardiovascular disease risk in women: a mendelian randomization study. J Am Heart Assoc. 2023;12(5):e027933. doi:10.1161/JAHA.122.027933
10. Ley SH, Li Y, Tobias DK, et al. Duration of reproductive life span, age at menarche, and age at menopause are associated with risk of cardiovascular disease in women. J Am Heart Assoc. 2017;6(11):e006713. doi:10.1161/JAHA.117.006713
11. Appiah D, Nwabuo CC, Ebong IA, Wellons MF, Winters SJ. Trends in age at natural menopause and reproductive life span among US women, 1959-2018. JAMA. 2021;325(13):1328–1330. doi:10.1001/jama.2021.0278
12. Mansoor H, Elgendy IY, Segal R, Hartzema A. Duration of reproductive years and the risk of cardiovascular and cerebrovascular events in older women: insights from the national health and nutrition examination survey. J Womens Health. 2017;26(10):1047–1052. doi:10.1089/jwh.2016.6013
13. Mishra SR, Chung HF, Waller M, Mishra GD. Duration of estrogen exposure during reproductive years, age at menarche and age at menopause, and risk of cardiovascular disease events, all-cause and cardiovascular mortality: a systematic review and meta-analysis. BJOG. 2021;128(5):809–821. doi:10.1111/1471-0528.16524
14. Yan Y, Lu H, Lin S, Zheng Y. Reproductive factors and risk of cardiovascular diseases and all-cause and cardiovascular mortality in American women: NHANES 2003-2018. BMC Womens Health. 2024;24(1):222. doi:10.1186/s12905-024-03055-6
15. Mensah GA, Fuster V, Murray CJL, Roth GA, Global Burden Of Cardiovascular Diseases and Risks Collaborators. Global burden of cardiovascular diseases and risks, 1990-2022. J Am Coll Cardiol. 2023;82(25):2350–2473. doi:10.1016/j.jacc.2023.11.007
16. United Nations. World population prospects 2024: summary of results. Available from: https://population.un.org/wpp/.
17. National Center for Health Statistics. NHANES survey methods and analytic guidelines. Available from: https://wwwn.cdc.gov/nchs/nhanes/AnalyticGuidelines.aspx.
18. University of Connecticut. Guidance on secondary analysis of existing data sets. Available from: https://ovpr.uconn.edu/services/ricslirb-2/researcher-guide/secondary-analysis-of-data-sets/.
19. STROBE Statement. Strengthening the reporting of observational studies in epidemiology. Available from: https://www.strobe-statement.org/.
20. The World Medical Association. Declaration of Helsinki (Medical Research Involving Human Subjects). Available from https://www.wma.net/what-we-do/medical-ethics/declaration-of-helsinki/.
21. National Center for Health Statistics. 2019 Public-Use Linked Mortality Files. Available from https://www.cdc.gov/nchs/data-linkage/mortality-public.htm.
22. Liu Q, Zhang Y, Chen S, et al. Association of the triglyceride-glucose index with all-cause and cardiovascular mortality in patients with cardiometabolic syndrome: a national cohort study. Cardiovasc Diabetol. 2024;23(1):80. doi:10.1186/s12933-024-02152-y
23. Xiao Q, Cai B, Yin A, et al. L-shaped association of serum 25-hydroxyvitamin D concentrations with cardiovascular and all-cause mortality in individuals with osteoarthritis: results from the NHANES database prospective cohort study. BMC Med. 2022;20(1):308. doi:10.1186/s12916-022-02510-1
24. Yu WM, Chen YP, Cheng AL, et al. Machine learning-driven prediction models and mechanistic insights into cardiovascular diseases: deciphering the environmental endocrine disruptors nexus. J Transl Med. 2025;23(1):1272. doi:10.1186/s12967-025-07223-6
25. Wu Z, Wei L, Zhang H. The relationship between number of pregnancies and serum 25-hydroxyvitamin D levels in women with a prior pregnancy: a cross - sectional analysis, machine learning - based prediction model, and SHAP - assisted feature importance evaluation. Front Endocrinol. 2025;16:1589002. doi:10.3389/fendo.2025.1589002
26. Zhang Y, Lu J, Huang S, Chen Y, Fang Q, Cao Y. Sex differences in the association between serum α-Klotho and depression in middle-aged and elderly individuals: a cross-sectional study from NHANES 2007-2016. J Affect Disord. 2023;337:186–194. doi:10.1016/j.jad.2023.05.073
27. Chen H, Tang H, Huang J, Luo N, Zhang X, Wang X. Life’s essential 8 and mortality in us adults with chronic kidney disease. Am J Nephrol. 2023;54(11–12):516–527. doi:10.1159/000533257
28. Wang YX, Arvizu M, Rich-Edwards JW, et al. Menstrual cycle regularity and length across the reproductive lifespan and risk of premature mortality: prospective cohort study. BMJ. 2020;371:m3464. doi:10.1136/bmj.m3464
29. Zuo R, Xu J, He L, Wang Y, Tang J. Associations between reproductive factors and the prevalence of depression: findings from the National health and nutrition examination survey (NHANES) 2005-2018. BMC Public Health. 2024;24(1):2761. doi:10.1186/s12889-024-20213-5
30. Demakakos P, Pashayan N, Chrousos G, Linara-Demakakou E, Mishra GD. Childhood experiences of parenting and age at menarche, age at menopause and duration of reproductive lifespan: evidence from the English Longitudinal Study of Ageing. Maturitas. 2019;122:66–72. doi:10.1016/j.maturitas.2019.01.010
31. Wenger NK, Lloyd-Jones DM, Elkind MSV, et al. Call to action for cardiovascular disease in women: epidemiology, awareness, access, and delivery of equitable health care: a presidential advisory from the American heart association. Circulation. 2022;145(23):e1059–e1071. doi:10.1161/CIR.0000000000001071
32. Wu Q, Yan Y, La R, et al. Association of reproductive lifespan and age at menopause with depression: data from NHANES 2005-2018. J Affect Disord. 2024;356:519–527. doi:10.1016/j.jad.2024.04.077
33. Yan Y, Chen J, Qin J, Yu M, Du M. Association of cardiovascular health with reproductive lifespan and pregnancy loss: insights from NHANES 2005-2018. Front Endocrinol. 2025;16:1597097. doi:10.3389/fendo.2025.1597097
34. McGrath IM, Mortlock S, Montgomery GW. Genetic regulation of physiological reproductive lifespan and female fertility. Int J Mol Sci. 2021;22(5):2556. doi:10.3390/ijms22052556
35. Camaioni A, Ucci MA, Campagnolo L, De Felici M, Klinger FG, Italian Society of Embryology, Reproduction and Research (SIERR). The process of ovarian aging: it is not just about oocytes and granulosa cells. J Assist Reprod Genet. 2022;39(4):783–792. doi:10.1007/s10815-022-02478-0
36. Huang J, Zhang Y, King L, et al. Associations of urinary heavy metals with age at menarche, age at menopause, and reproductive lifespan: a cross-sectional study in U.S. women. Ecotoxicol Environ Saf. 2024;283:116950. doi:10.1016/j.ecoenv.2024.116950
37. Gonzalez-Martin R, Grau-Perez M, Sebastian-Leon P, et al. Association of blood cadmium and lead levels with self-reported reproductive lifespan and pregnancy loss: the national health and nutrition examination survey 1999-2018. Environ Res. 2023;233:116514. doi:10.1016/j.envres.2023.116514
38. Liu L, Wei R, Tang Y, Zhang X, Zhao R, Lu C. Association of dietary flavonoid intake with reproductive lifespan: a cross-sectional study. Eur J Nutr. 2025;64(3):126. doi:10.1007/s00394-025-03641-w
39. Stevenson JC. A woman’s journey through the reproductive, transitional and postmenopausal periods of life: impact on cardiovascular and musculo-skeletal risk and the role of estrogen replacement. Maturitas. 2011;70(2):197–205. doi:10.1016/j.maturitas.2011.05.017
40. Cho L, Davis M, Elgendy I, et al. Summary of updated recommendations for primary prevention of cardiovascular disease in women: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(20):2602–2618. doi:10.1016/j.jacc.2020.03.060
41. Ivey SL, Hanley HR, Taylor C, et al. Early identification and treatment of women’s cardiovascular risk factors prevents cardiovascular disease, saves lives, and protects future generations: policy recommendations and take action plan utilizing policy levers. Clin Cardiol. 2022;45(11):1100–1106. doi:10.1002/clc.23921
42. Muka T, Oliver-Williams C, Kunutsor S, et al. Association of age at onset of menopause and time since onset of menopause with cardiovascular outcomes, intermediate vascular traits, and all-cause mortality: a systematic review and meta-analysis. JAMA Cardiol. 2016;1(7):767–776. doi:10.1001/jamacardio.2016.2415
43. Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice: developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Rev Esp Cardiol. 2022;75(5):429. doi:10.1016/j.rec.2022.04.003
44. Zhang Z, Hu Y, Cui X, Lu M, Zhang M, Li C. Menopausal age and cardiovascular disease risk in American women: evidence from the national health and nutrition examination survey. Climacteric. 2024;27(2):159–164. doi:10.1080/13697137.2023.2273526 PMID: 37921228.
45. Carlqvist E, Johnson L, Nilsson PM. Shorter reproductive life span is associated with increased cardiovascular risk and total mortality in Swedish women from an observational, population-based study. Maturitas. 2022;164:69–75. doi:10.1016/j.maturitas.2022.06.005
46. Morooka H, Haug EB, Malmo V, et al. Association of age at menarche, reproductive lifespan and age at menopause with the risk of atrial fibrillation: the HUNT study. Maturitas. 2024;185:107979. doi:10.1016/j.maturitas.2024.107979
47. Jaspers L, Kavousi M, Erler NS, Hofman A, Laven JS, Franco OH. Fertile lifespan characteristics and all-cause and cause-specific mortality among postmenopausal women: the Rotterdam Study. Fertil Steril. 2017;107(2):448–456.e1. doi:10.1016/j.fertnstert.2016.11.006
48. Li X, Wang S, Dunk M, et al. Association of life-course reproductive duration with mortality: a population-based twin cohort study. Am J Obstet Gynecol. 2022;227(5):748.e1–748.e13. doi:10.1016/j.ajog.2022.06.053
49. Fu L, Adu-Amankwaah J, Sang L, et al. Gender differences in GRK2 in cardiovascular diseases and its interactions with estrogen. Am. J Physiol Cell Physiol. 2023;324(2):C505–C516. doi:10.1152/ajpcell.00407.2022
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.