Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Association between Prognostic Nutritional Index and Mortality Risk in Critically Ill Patients with Chronic Obstructive Pulmonary Disease: A Retrospective Study
Received 25 January 2025
Accepted for publication 1 May 2025
Published 15 May 2025 Volume 2025:20 Pages 1493—1508
DOI https://doi.org/10.2147/COPD.S517676
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Qiu-Die Liu, Dao-Xin Wang
Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Dao-Xin Wang, Email [email protected]
Background: The Prognostic Nutritional Index (PNI), an integrative measure of body’s immune and nutritional status, has demonstrated its prognostic value across a range of diseases. However, its role in critically ill patients with Chronic Obstructive Pulmonary Disease (COPD) remains unclear. This study investigates the association between PNI levels and clinical outcomes in critically ill COPD patients, with a focus on identifying its role as a potential predictor of mortality.
Methods: A retrospective analysis of 1,250 critically ill COPD patients from the MIMIC-IV (v2.2) database was conducted. Patients were grouped by PNI tertiles. Primary and secondary outcomes were 28-day and 90-day mortality, respectively. Associations were evaluated using restricted cubic splines, Cox proportional hazards regression analysis, and Kaplan‒Meier survival curves. The predictive performance of PNI was assessed via receiver operating characteristic (ROC) curves analysis, and a nomogram integrating Boruta-selected features was developed to enhance clinical utility.
Results: The final cohort comprised 1,250 critically ill COPD patients, with observed mortality rates of 25.3% and 33.2% at 28 and 90 days, respectively. Higher PNI levels were associated with reduced risk of both 28-day and 90-day mortality [28-day HR: 0.95 (95% CI: 0.93– 0.97), P < 0.001; 90-day HR: 0.94 (95% CI: 0.93– 0.96), P < 0.001]. Restricted cubic spline analysis confirmed this trend. Furthermore, ROC analysis demonstrated the utility of PNI as a predictor for 28-day mortality (AUC: 0.61). Boruta-selected features reinforced the importance of PNI, and the constructed nomogram exhibited excellent predictive accuracy (AUC: 0.712).
Conclusion: Higher PNI is linked to reduced mortality risk in critically ill COPD patients, indicating its potential as a prognostic marker.
Keywords: chronic obstructive pulmonary disease (COPD), the prognostic nutritional index (PNI), MIMIC-IV
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a common respiratory condition that imposes a substantial burden on healthcare systems worldwide, often requiring admission to intensive care units (ICUs).1 It frequently necessitates intensive care unit (ICU) admissions due to its severe exacerbations and comorbidities.2 The incidence of COPD has been rising in recent years. According to the GOLD 2022 report, the global prevalence of COPD is 11.7%, and it is the third leading cause of death worldwide.3 This disease encompasses a spectrum of lung conditions characterized by irreversible tissue damage, leading to diminished pulmonary function.4 It is primarily characterized by chronic cough, sputum production, dyspnoea, and chest tightness, along with systemic symptoms such as weight loss and anorexia.5 Previous studies have reported that biomarkers such as blood eosinophil count, platelet-to-lymphocyte ratio (PLR) and systemic immune inflammatory index (SII) are associated with adverse clinical outcomes in patients with COPD.6,7 However, given the limited progress in improving clinical outcomes in this highly heterogeneous disease, there remains a strong need to identify and validate novel prognostic biomarkers to enhance risk stratification and guide personalized management strategies. Identifying high-risk individuals promptly could enhance prognostic strategies and optimize therapeutic outcomes.
The Prognostic Nutritional Index (PNI), calculated using serum albumin and lymphocyte counts, serves as a novel and practical marker for assessing immunonutritional status.8 Albumin serves as a marker of the body’s nutritional state, has antioxidant and anti-inflammatory capacities.9 Lymphocytes, a subtype of white blood cells, are crucial to the immune system, serving as key regulators of immune defense and memory. The PNI provides a comprehensive assessment of both nutritional and immune status and is easily accessible, making it a valuable tool for prognostication in clinical practice. PNI has been shown to have significant predictive value for various types of cancer.10,11 Recent studies have extended its utility to non-neoplastic diseases, such as cardiovascular diseases, autoimmune disorders, neonatal respiratory distress syndrome, and cerebrovascular diseases.12–15
COPD is characterized by systemic inflammation and nutritional impairments that significantly impact disease progression and patient outcomes.16,17 Given that malnutrition and immune dysfunction are prevalent in COPD patients, PNI’s dual assessment of nutritional status and immune function makes it a particularly promising marker for this population. However, the role of PNI in predicting outcomes for critically ill COPD patients remains insufficiently explored. Our primary hypothesis is that PNI values are significantly associated with mortality risk in critically ill patients with COPD, with lower values potentially indicating poorer outcomes. The main purpose of our study is to explore whether PNI could serve as a valuable prognostic indicator for mortality outcomes in this specific patient population, thereby potentially guiding early intervention strategies.
In this study, we aim to investigate the relationship between PNI scores and adverse health outcomes in critically ill COPD patients, with the goal of providing new insights into early prediction of clinical outcomes in this population.
Materials and Methods
Database introduction
This study utilized data from the MIMIC-IV (version 2.2) database, a publicly accessible and comprehensive electronic health record repository. Maintained by the Massachusetts Institute of Technology Laboratory for Computational Physiology, MIMIC-IV contains detailed clinical data from over 70,000 patients admitted to the Beth Israel Deaconess Medical Center (Boston, Massachusetts) between 2008 and 2019.18 The database includes demographic, clinical, laboratory, and outcome data for over 70,000 patients, providing a robust resource for retrospective analyses. The first author, Qiudie Liu (certification number: 62816135), was authorized to access the MIMIC-IV database after completing required training.
Population Selection Criteria
A total of 1,250 COPD patients were identified from the MIMIC-IV database using International Classification of Diseases (ICD) 9th, 10th Revision codes (J44, J440, J449, J441, 49,120, 49,121, 49,122, 496). Patients were included if they met the following criteria: (1) age ≥18 years; (2) first ICU admission; and (3) availability of complete data for calculating the Prognostic Nutritional Index (PNI). Exclusion criteria included repeated ICU admissions (n = 3,180), ICU stays shorter than 24 hours (n = 1,824), and missing PNI data (n = 2,190). After applying these criteria, the final cohort comprised 1,250 patients.
Data Extraction and PNI
Data extraction was conducted using PostgreSQL to retrieve relevant variables from the MIMIC-IV database. The collected data encompassed demographics, vital signs, laboratory parameters, comorbidities, severity scores, and therapeutic interventions. All variables were limited to the first 24 hours admission to the hospital to ensure consistency. Demographic variables included age and gender, while vital signs comprised mean blood pressure (MBP), heart rate, oxygen saturation (SpO2), and temperature. Comorbidities included myocardial infarction, cerebrovascular disease, severe liver disease, renal disease, cancer, diabetes. Laboratory parameters included white blood cell, hemoglobin, platelets, serum creatinine (SCr), anion gap, albumin, blood urea nitrogen (BUN), serum sodium, serum potassium, serum calcium, international normalized ratio (INR), and prothrombin time (PT), lymphocytes. Illness severity scores included the admission severity evaluated by acute physiology score III (APS III), sequential organ failure assessment (SOFA) and the Charlson comorbidity index (CCI), life-sustaining interventions included vasopressors and Renal Replacement Therapy (RRT). The Prognostic Nutritional Index (PNI) was calculated using the formula: = (10×serum albumin [g/dL]) + (0.005×lymphocytes [K/µL]).19 All data were retrieved from records generated within the first 24 hours following the patient’s admission to the hospital.
Groups and Clinical Outcome
Patients were categorized into three groups based on tertiles of the PNI levels, Tertile (T)1: ≤ 29; T2: 29–35; T3: > 35. Primary outcomes focused on 28-day all-cause mortality. Secondary outcomes included hospital mortality,90-day mortality and the lengths of hospital and ICU stays.
Statistical Analysis
Statistical analyses were conducted to ensure robust and reliable findings. Continuous variables were presented as means ± standard deviations (SD) for normally distributed data or medians with interquartile ranges (IQR) for non-normally distributed data. Parametric tests, including the t-test or ANOVA, were applied to normally distributed variables, while non-parametric tests, such as the Mann–Whitney U-test and Kruskal–Wallis test, were used for skewed distributions. Categorical variables were expressed as frequencies and percentages and analyzed using the Chi-square test. Missing data for variables with less than 5% were imputed using mean or median value.
Survival analyses were performed using Kaplan-Meier curves to evaluate the incidence of 28-day and 90-day mortality across PNI tertile groups. Differences between survival curves were tested using the Log rank test. The association between PNI and mortality outcomes was further assessed using multivariate Cox proportional hazards models. Results were reported as hazard ratios (HR) with 95% confidence intervals (CI). Three models were constructed with increasing levels of adjustment: Model I: unadjusted; Model II: adjusted for age, myocardial infarct, cerebrovascular disease, diabetes, renal disease, malignant cancer, severe liver disease; Model 3: further adjusted for the variables in Model II plus hemoglobin, platelets, WBC, creatinine, calcium, sodium, potassium, INR, PT, APTT, anion gap, BUN, chloride.
Subgroup analyses were performed to examine the consistency of PNI’s prognostic value across different patient groups, including variations by age, gender, cerebrovascular disease, severe liver disease, congestive heart failure, renal disease, malignant cancer, sepsis, and the use of vasopressors. Receiver operating characteristic (ROC) curve analyses were employed to compare the predictive performance of PNI with other indicators, including APSIII and SOFA scores. To explore potential nonlinear relationships between PNI and mortality outcomes, a restricted cubic spline (RCS) regression model with four knots was applied.
The Boruta algorithm was used to identify the most important features for predicting mortality in our cohort. This feature selection method determines feature importance by comparing the Z-value of each feature with the Z-value of its corresponding “shadow feature.20 If the Z-value of a true feature significantly exceeds the maximum Z-value of shadow features in multiple tests, it is classified as “important” (green area). Conversely, features with Z-values not exceeding the shadow features’ maximum are classified as “unimportant” (red area).
A nomogram was developed based on the results of the Boruta algorithm and clinical considerations to predict mortality risk in critically ill COPD patients. The dataset was divided into training and validation sets at a 7:3 ratio. The area under the curve (AUC) was used to evaluate the performance of the model to predict the risk of severity transformation. During internal validation, a calibration curve was plotted based on 1000 bootstrap resamples to assess predictive accuracy.21 The closer the calibration curve to the 45-degree diagonal line, the better the performance of the prediction model.
All data analyses were carried out using R software, version 4.4.2, and SPSS version 27.0, with statistical significance set at a two-sided p-value of less than 0.05.
Results
Patient Characteristics
Data from 1250 patients diagnosed with COPD were extracted from the MIMIC-IV (Figure 1). Patient characteristics, divided by PNI tertile, were displayed in Table 1. Patients with higher PNI values (T3) had significantly lower WBC, BUN, APTT, and PT levels compared to those with lower PNI values (T1). Additionally, patients in the higher PNI tertile presented with lower disease severity scores (APSIII and SOFA) at admission. The prevalence of malignant cancer was significantly higher in the lower PNI tertile group (P < 0.001). Regarding therapeutic interventions, the use of vasopressors, RRT, and mechanical ventilation was significantly lower in patients with higher PNI tertiles compared to those in lower tertiles.
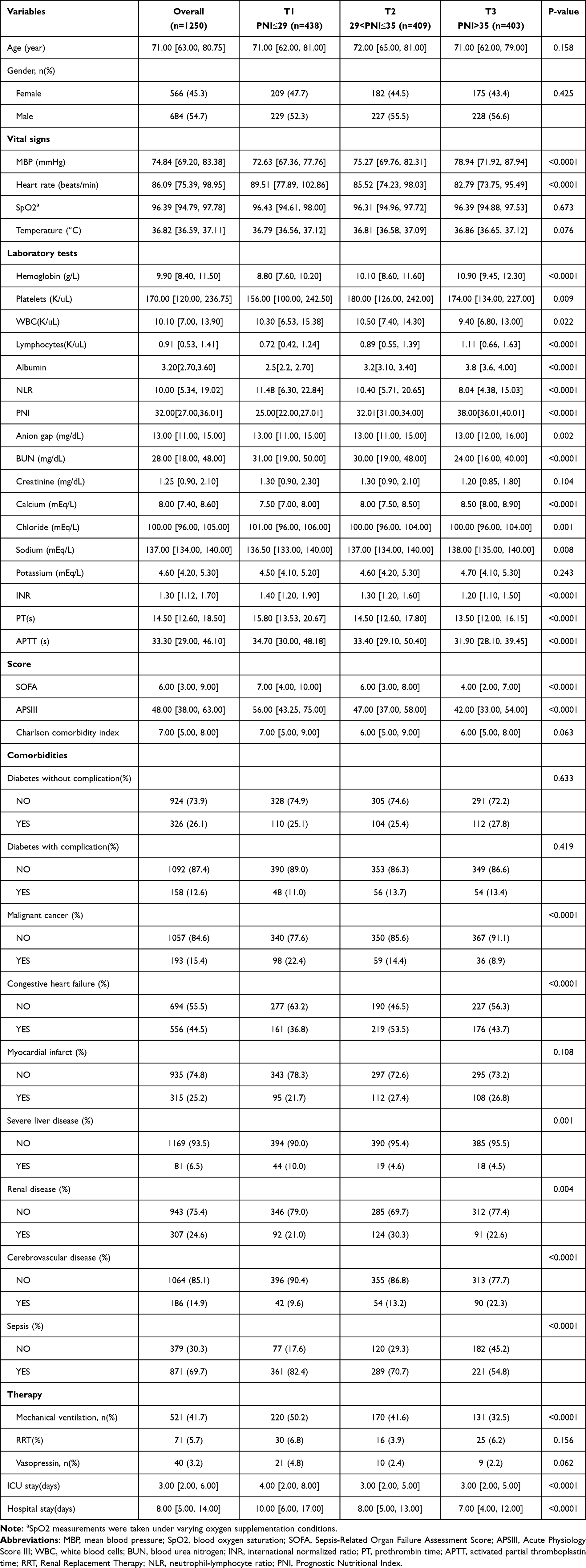 |
Table 1 Baseline Characteristics of Patients Stratified by PNI Tertiles |
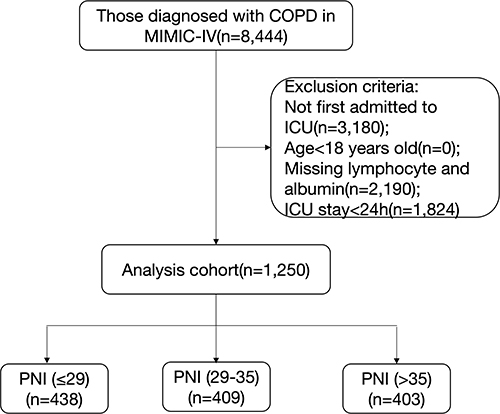 |
Figure 1 Selection of the study population from the MIMIC-IV database. Abbreviations: COPD, chronic obstructive pulmonary disease; PNI, Prognostic Nutritional Index; ICU, intensive care unit. |
Clinical Outcomes
According to PNI levels, the mortality rates in the T1, T2, and T3 groups were 34.7%, 21.0%, and 19.4% at 28 days, and 45.2%, 28.6%, and 24.8% at 90 days, respectively (Table 2). These results demonstrate that mortality rates decreased progressively with increasing PNI levels. This inverse relationship was further illustrated by the Kaplan-Meier survival curves (Figure 2), which showed significant separation between the tertiles (log-rank P < 0.001).
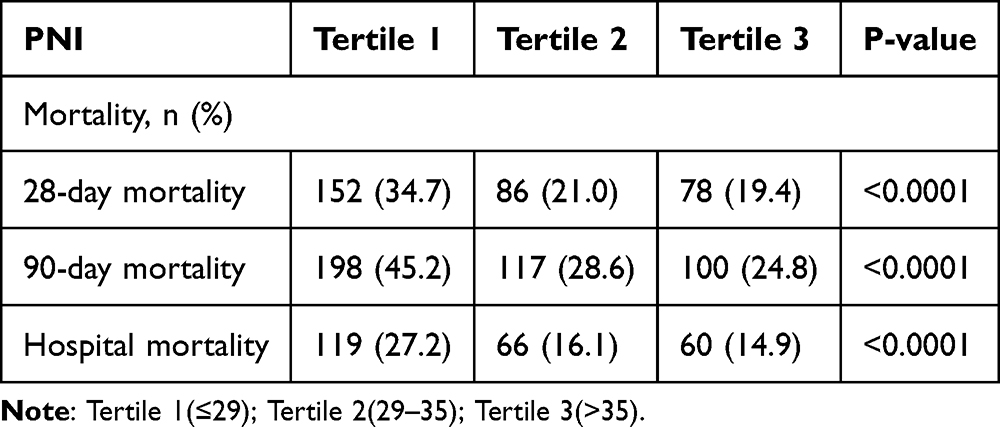 |
Table 2 28-Day Mortality and 90-Day Mortality |
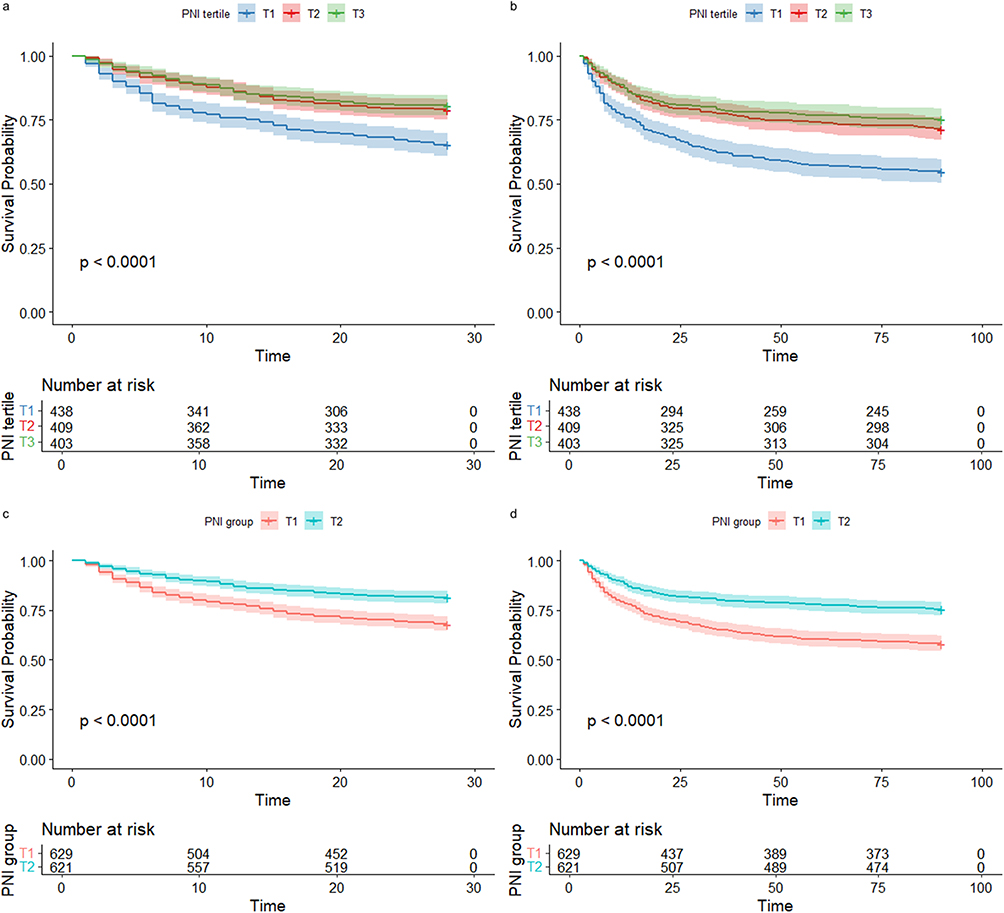 |
Figure 2 Kaplan-Meier survival curves for all-cause mortality by PNI. Note: (a) 28-day and (b) 90-day mortality: Stratification across PNI tertiles ((T1: ≤29; T2: 29–35; T3: >35)) shows progressively better survival, with a turning point at PNI = 32.00, as indicated by restricted cubic spline (RCS) analysis, where PNI is regrouped into T1 (PNI < 32) and T2 (PNI ≥ 32), revealing significantly lower survival in T1 (P < 0.0001) for both (c) 28-day and (d) 90-day mortality. |
Association between All-Cause Mortality and PNI
In the Cox regression analysis, the results revealed an association between higher PNI and reduced risks of 28-day mortality across various models: unadjusted [HR, 0.94 (0.93–0.96), P < 0.001], partly adjusted [HR, 0.94 (0.93–0.96), P < 0.001], and fully adjusted [HR, 0.95 (0.91–0.94), P < 0.001] when PNI was treated as a continuous variable. Similarly, PNI was correlated with 90-day mortality across the unadjusted [HR, 0.94 (0.93–0.96), P < 0.001], partly adjusted [HR, 0.95 (0.93–0.96), P < 0.001], and fully adjusted [HR, 0.94 (0.93–0.96), P < 0.001] models (Table 3). Furthermore, when PNI was categorized as a nominal variable, individuals in the higher tertiles demonstrated significantly lower risks of 28-day and 90-day mortality in all three models. For 28-day mortality, patients in Tertile 2 had the lowest risk (HR = 0.55, 95% CI: 0.42–0.72, P < 0.001), while for 90-day mortality, the risk was lowest in Tertile 3 (HR = 0.53, 95% CI: 0.40–0.70, P < 0.001).
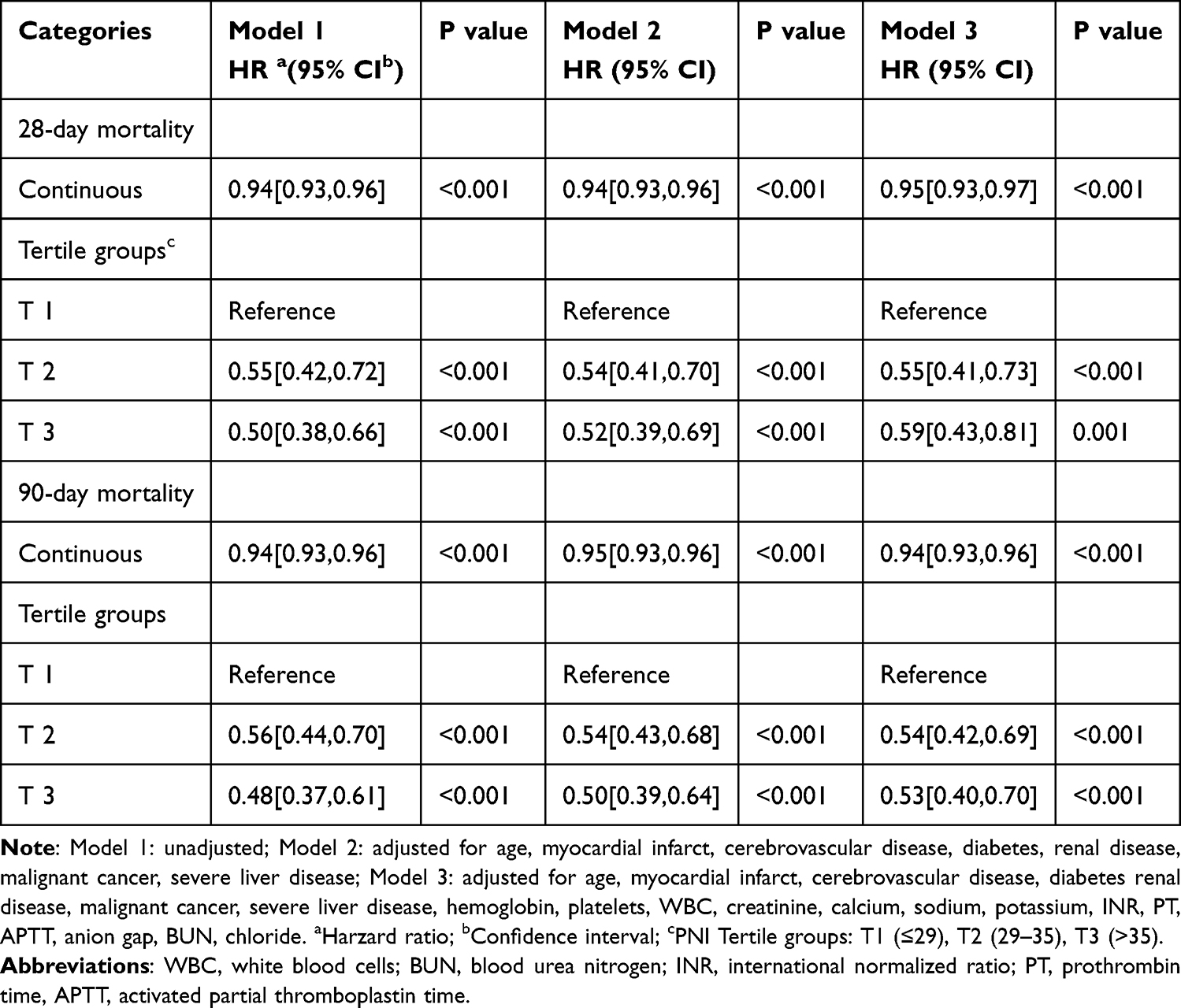 |
Table 3 Cox Proportional Hazard Ratios (HRs) for All-Cause Mortality |
Restricted Cubic Spline
The restricted cubic spline (RCS) analysis for both 28-day and 90-day mortality (Figure 3) revealed an L-shaped association between PNI and mortality risk, with an inflection point around PNI = 32.00, indicating a nonlinear relationship. Below this inflection point, the risk of mortality decreased sharply with increasing PNI, while above PNI = 32.00, the reduction in mortality risk became less pronounced. According to the Cox proportional hazards regression model (Table 3), the lowest 28-day mortality risk was observed in Tertile 2 (HR = 0.55, 95% CI: 0.42–0.72, P < 0.001), suggesting a potential nonlinear association with a nadir at moderate PNI levels. In contrast, for 90-day mortality, the risk was lowest in Tertile 3 (HR = 0.53, 95% CI: 0.40–0.70, P < 0.001). This suggests that while increasing PNI generally correlates with better outcomes, the relationship may be more complex at different time points.
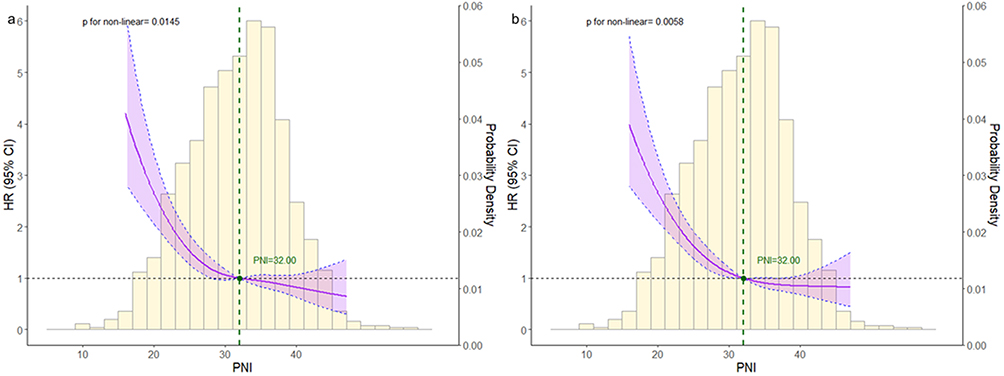 |
Figure 3 RCS analysis of 28-day (a) and 90-day (b) mortality. Abbreviation: HR, hazard ratio; CI, confidence interval. Note: The curves represent the estimated adjusted hazard ratios, with shaded ribbons indicating the 95% confidence intervals. The vertical dotted line marks the turning point of the curve (PNI = 32), where the hazard ratio equals 1.0. The horizontal dashed line represents a hazard ratio of 1.0. The columns represent the histogram of the PNI distribution in the study population. |
ROC Curve Analysis
ROC curves were generated to assess the predictive performance of PNI, APSIII, SOFA, and the combined APSIII+PNI model for 28-day mortality in patients with COPD (Figure 4). Among these, the APSIII score alone demonstrated the highest discriminative ability, with an AUC of 0.75 (95% CI: 0.68–0.82). The combined APSIII+PNI model yielded a slightly lower AUC of 0.72 (95% CI: 0.64–0.79), and the difference was statistically significant when compared with APSIII alone (Z=2.436, p=0.0148). The PNI-only model showed moderate predictive ability with an AUC of 0.61 (95% CI: 0.53–0.68). These results suggest that while PNI has independent prognostic value, combining it with APSIII does not enhance predictive performance beyond using APSIII alone, possibly due to some overlap in the physiological parameters they assess.
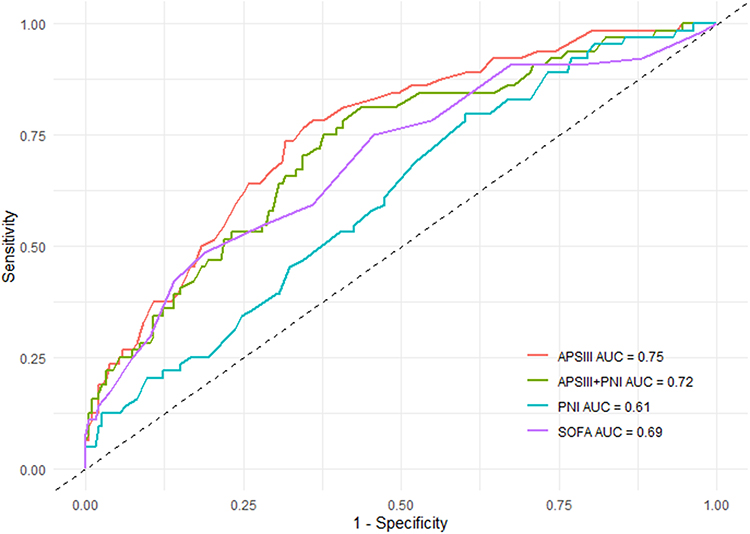 |
Figure 4 ROC Curve for 28-day all-cause Mortality. Abbreviations: PNI, Prognostic Nutritional Index; APSIII, Acute Physiology Score III; SOFA, Sequential Organ Failure Assessment. |
Subgroup Analysis
Subgroup analysis across various demographic and clinical strata consistently showed that higher PNI was associated with reduced 28-day mortality in COPD patients (Figure 5). Importantly, a significant interaction was detected only in the vasopressor subgroup (p for interaction < 0.05), suggesting potential effect modification, whereas no such interactions were observed in other subgroups.
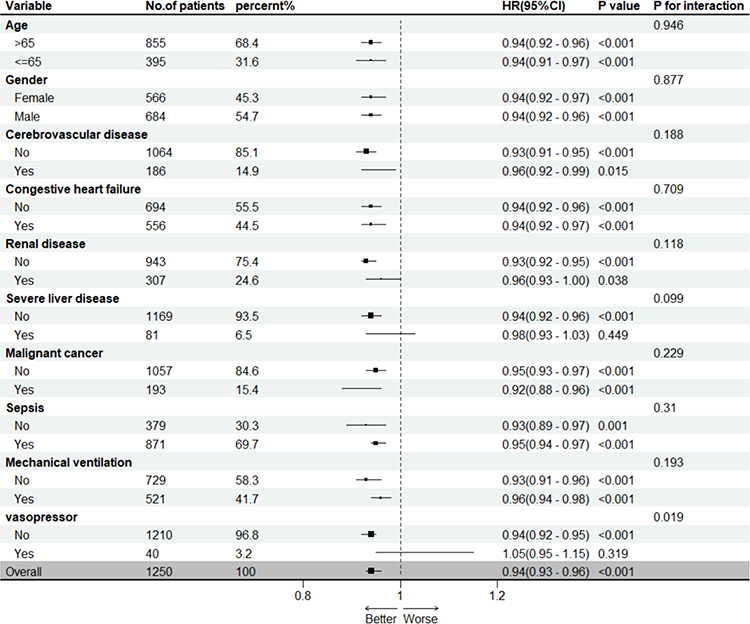 |
Figure 5 Subgroup analysis of associations between PNI and 28-day mortality. Abbreviations: PNI, Prognostic Nutritional Index; HR, hazard ratio; CI, confidence interval. |
Boruta Algorithm
Figure 6 illustrates the feature selection results based on the Boruta algorithm. Variables in the green area are identified as important predictive features, while variables in the red area represent unimportant features. PNI was identified as an important predictor with a high Z-score, reinforcing its significance in mortality prediction for critically ill COPD patients. Other important features included age, APSIII, SOFA, MBP, SpO2, WBC count, neutrophil count, serum creatinine, and temperature.
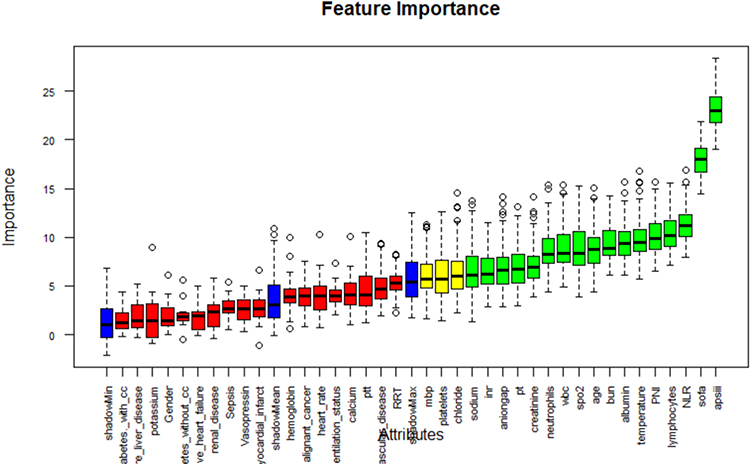 |
Figure 6 Feature selection based on the Boruta algorithm. Note: The horizontal axis is the name of each variable, and the vertical axis is the Z value of each variable. Boxplots represent the distribution of Z scores for each variable during the Boruta feature selection process. Green: confirmed important variables; Red: rejected variables; Yellow: tentative variables; Blue: shadow attributes used as reference to evaluate importance. |
Nomogram Building and Validation
Based on the Boruta algorithm results and clinical considerations, we constructed a nomogram prediction model incorporating eleven variables (age, PNI, MBP, SpO2, WBC count, neutrophil count, serum creatinine, temperature, APSIII, and SOFA) to predict mortality in critically ill patients with COPD (Figure 7). The model demonstrated robust discriminatory power, with an AUC of 0.783 (95% CI: 0.735–0.800) in the training set and 0.712 (95% CI: 0.648–0.776) in the validation set (Figure 8a and b). Furthermore, the calibration curve graphs showed good alignment between predicted probabilities and actual outcomes (Figure 9a and b), particularly in the training set, though with some deviation in the validation set at higher probability ranges.
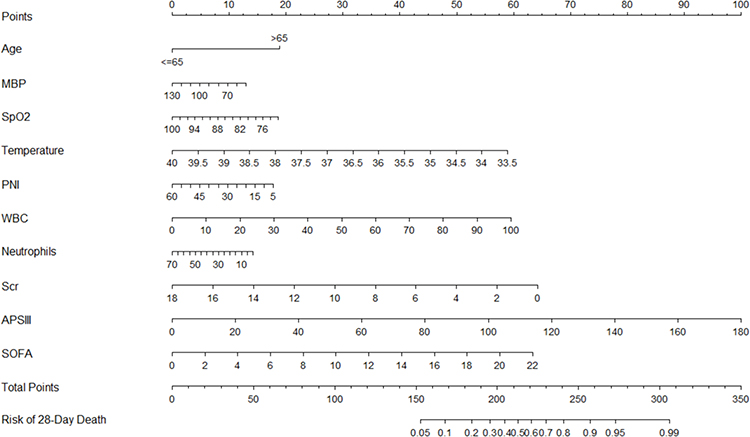 |
Figure 7 Nomogram for predicting 28-day mortality in patients with COPD. Abbreviations: PNI, Prognostic Nutritional Index; APSIII, Acute Physiology Score III; SOFA, Sequential Organ Failure Assessment; WBC, white blood cell; MBP, mean blood pressure; Scr, serum creatinine. Note: Scores are assigned to each predictor based on its contribution to the model. The total score, derived by summing individual scores, corresponds to the estimated probability of 28-day mortality shown on the bottom scale. |
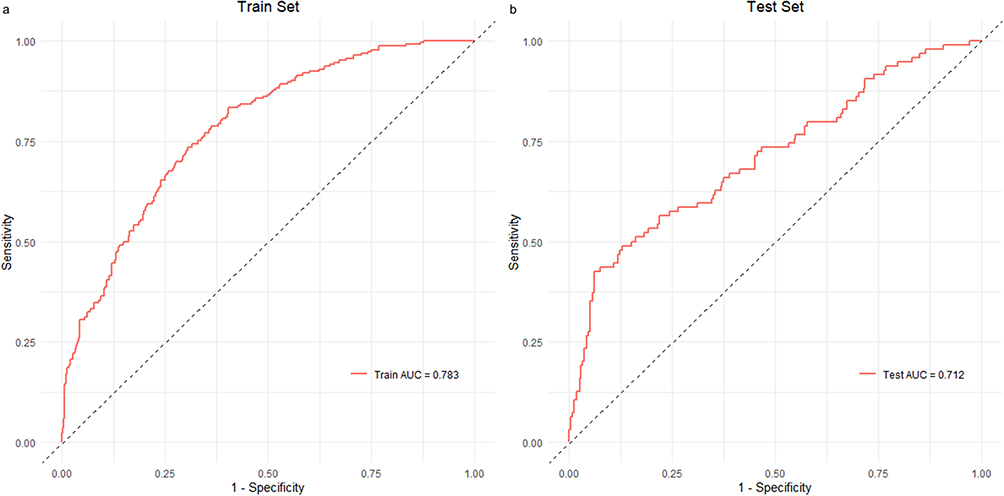 |
Figure 8 Receiver operating characteristic (ROC) curve of the nomogram training and validation cohort. Note: The ROC curve shows the discriminative ability of the nomogram, with an area under the curve (AUC) of 0.783 (a) in the training cohort and an area under the curve (AUC) of 0.712 (b) in the validation cohort. |
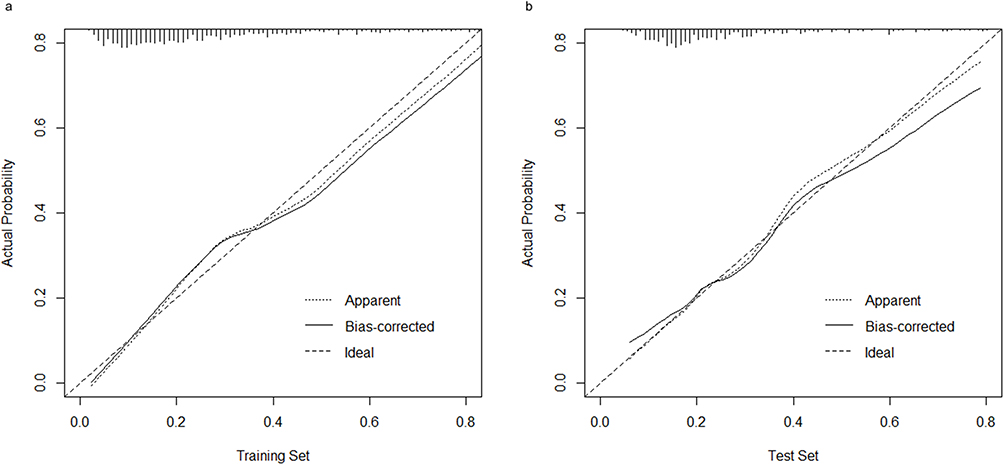 |
Figure 9 Calibration curve of the nomogram in the training and validation cohort. Note: The calibration curve demonstrates the agreement between the predicted and observed 28-day mortality. (a) shows the calibration curve of the training set and (b) shows the calibration curve of the validation set. The 45° dashed line is the reference line. The dotted line shows the performance of the current nomogram, and the solid line is bias-corrected by bootstrapping. |
Discussion
This study highlights a significant inverse relationship between PNI and mortality in critically ill COPD patients. Lower PNI levels were strongly associated with higher risks of 28-day mortality [HR: 0.95 (95% CI: 0.93–0.97), P < 0.001] and 90-day mortality [HR: 0.94 (95% CI: 0.93–0.96), P < 0.001], suggesting its potential as a robust prognostic marker. The PNI demonstrated moderate predictive performance for 28-day mortality with an AUC of 0.61, indicating its utility as an independent prognostic indicator.
APSIII is a widely used scoring system in ICU practice, reflecting the acute physiological status of patients and serving as the core component of the APACHE II score.22 It includes 12 variables such as temperature, mean arterial pressure, heart rate, and WBC count, providing a comprehensive method to assess illness severity. However, APSIII does not incorporate nutritional markers such as serum albumin, which are critical determinants of prognosis, especially in chronic conditions like COPD.23 The Prognostic Nutritional Index (PNI), by integrating serum albumin and lymphocyte count, reflects both nutritional status and immune function, potentially offering complementary prognostic information.
In our study, APSIII alone demonstrated the highest predictive value for 28-day mortality in COPD patients (AUC = 0.75). Interestingly, the addition of PNI slightly reduced the AUC to 0.72, with this difference being statistically significant (Z = 2.436, p = 0.0148). This finding suggests that while PNI captures nutritional dimensions not included in APSIII, its integration with APSIII may introduce redundancy due to overlapping inflammatory components already assessed by APSIII. The standalone PNI model (AUC = 0.61) showed moderate predictive ability, indicating its value as an independent prognostic tool, particularly in settings where comprehensive physiological scoring may not be feasible.
The Boruta algorithm identified PNI as an important predictor with a high Z-score, confirming its relevance in mortality prediction for critically ill COPD patients. This finding supports the use of PNI in prognostic models and risk stratification tools. Based on these results, we developed a nomogram that integrates PNI with other clinically relevant variables to provide a practical tool for mortality risk assessment in critically ill COPD patients. The nomogram demonstrated good discriminative ability (AUC = 0.783 in the training set, 0.712 in the validation set) and reasonable calibration, suggesting its potential utility in clinical decision-making.
Relation to Previous Research
Extensive research underscores the intricate connection between nutritional and immune status and disease prognosis. The PNI, encapsulating both dimensions, has emerged as a valuable prognostic marker, particularly in oncology, where it has demonstrated predictive utility in cancers such as non-small cell lung cancer.24 Recent studies have shown that lower PNI at admission correlates with increased mortality risk in patients with severe COVID-19.25,26 Research has also demonstrated that preoperative PNI is closely associated with prognosis in patients with hepatocellular carcinoma (HCC), serving as a predictor of postoperative recurrence and survival.27
Several prior investigations have evaluated the prognostic significance of PNI in individuals diagnosed with COPD. For example, a retrospective analysis involving 91 COPD patients identified a significant negative correlation between PNI and the risk of exacerbations in elderly patients.28 However, their analysis was limited to general hospital admissions, lacking a focus on critically ill patients in ICU settings. In contrast, our study specifically targets this high-risk subgroup, characterized by higher disease severity and complexity, where mortality risks are markedly elevated. By examining critically ill COPD patients, we demonstrated that lower PNI levels are strongly associated with increased all-cause mortality, emphasizing the importance of PNI as a practical and effective prognostic tool in ICU settings.
PNI and COPD
Serum albumin, a major plasma protein, is a conventional marker of nutritional status and plays essential roles in maintaining oncotic pressure, exerting antioxidant effects, and modulating immune responses.29 Hypoalbuminemia is common in critical illnesses and has been associated with poor outcomes in various diseases.30 Similarly, lymphocyte count reflects cellular immune capacity, with lymphopenia indicating immune suppression and heightened susceptibility to infections.31 In COPD patients, lymphopenia is often linked to worse prognoses, compounding the challenges of disease management.32,33
The clinical course of COPD is multifactorial, involving interactions between systemic inflammation, immune dysfunction, and nutritional deficiencies. These complexities often limit the utility of single predictive markers. The PNI addresses this gap by integrating albumin and lymphocyte counts, creating a holistic measure that reflects both nutritional and immune status. This dual assessment enhances its predictive value, enabling more accurate risk stratification and prognostic evaluation in COPD patients, particularly those with severe disease presentations.
The relationship between PNI and mortality in COPD patients is complex and multifaceted. Poor nutritional status, a hallmark of COPD, is associated with reduced exercise capacity, delayed recovery, and heightened susceptibility to complications.34 Malnutrition exacerbates muscle wasting, prolongs hospital stays, and impairs wound healing, contributing to worse clinical outcomes.35 Furthermore, systemic inflammation and metabolic stress, characteristic of COPD, amplify nutritional deficits, creating a vicious cycle that undermines recovery. Low PNI levels are also linked to higher incidences of comorbidities, such as cancer and renal dysfunction, which independently elevate mortality risk.14,36 As PNI integrates albumin and lymphocyte levels, it offers a simple yet powerful method for assessing immune-nutritional status using routine blood tests, facilitating early risk identification and intervention.
Limitations of the Study
Despite the significant findings of this study, several limitations must be acknowledged. First, the retrospective design utilizing the MIMIC-IV database introduces inherent limitations such as dependence on pre-existing data and potential for residual confounding, even after multivariate adjustments. Important factors that might influence both PNI and outcomes, such as detailed nutritional history, physical activity levels, and socioeconomic status, were not available for analysis. Second, the single-center nature of the MIMIC-IV database may limit the generalizability of our findings to broader COPD populations with different demographic characteristics or treatment protocols. Variations in clinical practices and resource availability across institutions could influence both PNI levels and patient outcomes. Third, our study evaluated PNI at a single time point and did not assess dynamic changes in PNI over time, which might provide deeper insights into its prognostic utility. Additionally, data on specific nutritional support interventions were unavailable, limiting our understanding of how these treatments might interact with PNI and influence mortality risk. Fourth, while our nomogram demonstrated good predictive performance, external validation in independent cohorts is necessary to confirm its clinical utility. Future research should prioritize large-scale, multi-center prospective studies to validate these findings across diverse COPD populations and explore the impact of nutritional interventions on PNI and clinical outcomes.
Conclusion
Our study identified a significant negative correlation between PNI and all-cause mortality in patients with COPD. PNI shows promise as a predictor of mortality risk in this cohort. However, further validation through prospective, large-scale, multi-center studies is needed to confirm these findings.
Data Sharing Statement
The datasets generated and/or analysed during the current study are available in the MIMIC-IV database (https://physionet.org/content/mimiciv/2.2/).
Ethics Approval and Informed Consent
The data were extracted from the MIMIC IV, which is considered the largest open-source and freely accessible clinical database in critical care. Qiudie Liu completed the data research training program of the Collaborative Institutional Training Initiative (record ID 62816135) and gained access to the database. In this study, the MIT Institutional Review Board waived informed consent and approved the sharing of the research resource since it involved an analysis of public databases. According to item 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects: research using legally obtained public data, or conducting research through observation, data generated without interfering with public behavior, and research using anonymous information data are exempt from ethical review. The data use protocol and ethical guidelines were strictly followed, and the study was conducted for scientific research analysis only. The study adhered to the ethical principles of the Declaration of Helsinki and respected the privacy and data confidentiality of the participants.
Consent for Publication
All participants agreed to publish the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Key Laboratory of Respiratory Inflammatory Injury and Precision Diagnosis and Treatment, Chongqing Municipal Health And Health Committee, Chongqing 400010, China and the National Natural Science Foundation of China (Grant no. 82270091).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the Global Burden of Disease Study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
2. Zijlstra GJ. Different oxygenation targets for stable COPD and acute exacerbations in the ICU. Intensive Care Med. 2023;49(11):1428–1429. doi:10.1007/s00134-023-07206-5
3. Adeloye D, Chua S, Lee C, et al. Global and regional estimates of COPD prevalence: systematic review and meta-analysis. J Glob Health. 2015;5(2):020415. doi:10.7189/jogh.05.020415
4. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/s0140-6736(22)00470-6
5. Ritchie AI, Wedzicha JA. Definition, causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations. Clin Chest Med. 2020;41(3):421–438. doi:10.1016/j.ccm.2020.06.007
6. Cai C, Zeng W, Wang H, Ren S. Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Monocyte-to-Lymphocyte Ratio (MLR) as biomarkers in diagnosis evaluation of acute exacerbation of chronic obstructive pulmonary disease: a retrospective, observational study. Int J Chron Obstruct Pulmon Dis. 2024;19:933–943. doi:10.2147/copd.S452444
7. Halpin DMG, Healey H, Skinner D, Carter V, Pullen R, Price D. Exacerbation history and blood eosinophil count prior to diagnosis of COPD and risk of subsequent exacerbations. Eur Respir J. 2024;64(4):2302240. doi:10.1183/13993003.02240-2023
8. Cai B, Luo L, Zhu C, et al. Corrigendum: influence of body composition assessment with bioelectrical impedance vector analysis in cancer patients undergoing surgery. Front Oncol. 2024;14:1378338. doi:10.3389/fonc.2024.1378338
9. Belinskaia DA, Voronina PA, Shmurak VI, Jenkins RO, Goncharov NV. Serum albumin in health and disease: esterase, antioxidant, transporting and signaling properties. Int J Mol Sci. 2021;22(19):10318. doi:10.3390/ijms221910318
10. Wang Z, Zhao S, Zhang X, et al. Effect of prognostic nutritional index on laboratory parameters and survival in metastatic colorectal cancer patients treated with fruquintinib: a retrospective study. PeerJ. 2024;12:e18565. doi:10.7717/peerj.18565
11. Mi HL, Wei WL, Zhang DH, Liang HY, Yue CF, Xu JN. Neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and prognostic nutritional index as prognostic markers for lung carcinoma. Br J Hosp Med. 2024;85(10):1–13. doi:10.12968/hmed.2024.0270
12. Solano S, Yang M, Tolomeo P, et al. Clinical characteristics and outcomes of patients with heart failure with preserved ejection fraction and with reduced ejection fraction according to the prognostic nutritional index: findings from PARADIGM-HF and PARAGON-HF. J Am Heart Assoc. 2024;14:e037782. doi:10.1161/jaha.124.037782
13. Huang L, Chen X, Zhang Y. Low Prognostic Nutritional Index (PNI) level is associated with an increased risk of neonatal respiratory distress syndrome in preterm infants with different gestational ages: a retrospective study. Int J Gen Med. 2024;17:5219–5231. doi:10.2147/ijgm.S486224
14. Peng F, Chen W, Zhou W, et al. Low prognostic nutritional index associated with cardiovascular disease mortality in incident peritoneal dialysis patients. Int Urol Nephrol. 2017;49(6):1095–1101. doi:10.1007/s11255-017-1531-0
15. Wang Y, Zhang G, Shen Y, et al. Relationship between prognostic nutritional index and post-stroke cognitive impairment. Nutr Neurosci. 2024;27(11):1330–1340. doi:10.1080/1028415x.2024.2330786
16. Hogg JC, Timens W. The pathology of chronic obstructive pulmonary disease. Annu Rev Pathol. 2009;4:435–459. doi:10.1146/annurev.pathol.4.110807.092145
17. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
18. Johnson AEW, Bulgarelli L, Shen L, et al. Author Correction: MIMIC-IV, a freely accessible electronic health record dataset. Sci Data. 2023;10(1):219. doi:10.1038/s41597-023-02136-9
19. Wang X, Wang Y. The prognostic nutritional index is prognostic factor of gynecological cancer: a systematic review and meta-analysis. Int J Surg. 2019;67:79–86. doi:10.1016/j.ijsu.2019.05.018
20. Yue S, Li S, Huang X, et al. Machine learning for the prediction of acute kidney injury in patients with sepsis. J Transl Med. 2022;20(1):215. doi:10.1186/s12967-022-03364-0
21. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–1370. doi:10.1200/jco.2007.12.9791
22. Fan S, Ma J. The value of five scoring systems in predicting the prognosis of patients with sepsis-associated acute respiratory failure. Sci Rep. 2024;14(1):4760. doi:10.1038/s41598-024-55257-5
23. Nicholson JP, Wolmarans MR, Park GR. The role of albumin in critical illness. Br J Anaesth. 2000;85(4):599–610. doi:10.1093/bja/85.4.599
24. Wang Z, Wang Y, Zhang X, Zhang T. Pretreatment prognostic nutritional index as a prognostic factor in lung cancer: review and meta-analysis. Clinica Chimica Acta. 2018;486:303–310. doi:10.1016/j.cca.2018.08.030
25. Wei W, Wu X, Jin C, et al. Predictive significance of the Prognostic Nutritional Index (PNI) in patients with severe COVID-19. J Immunol Res. 2021;2021:9917302. doi:10.1155/2021/9917302
26. Liu G, Zhang S, Mao Z, Wang W, Hu H. Clinical significance of nutritional risk screening for older adult patients with COVID-19. Eur J Clin Nutr. 2020;74(6):876–883. doi:10.1038/s41430-020-0659-7
27. Zeng L, Tang Y, Huang X, Pei W, Liao Y, Liu J. Combined impact of prognostic nutritional index, fibrinogen-to-albumin ratio, and neutrophil-to-lymphocyte ratio on surgical outcomes and prognosis in hepatocellular carcinoma. Am J Cancer Res. 2025;15(2):439–451. doi:10.62347/rtmf3105
28. Suzuki E, Kawata N, Shimada A, et al. Prognostic Nutritional Index (PNI) as a potential prognostic tool for exacerbation of COPD in elderly patients. Int J Chron Obstruct Pulmon Dis. 2023;18:1077–1090. doi:10.2147/copd.S385374
29. Roche M, Rondeau P, Singh NR, Tarnus E, Bourdon E. The antioxidant properties of serum albumin. FEBS Letters. 2008;582(13):1783–1787. doi:10.1016/j.febslet.2008.04.057
30. Chen G, Wu D, Guo W, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Invest. 2020;130(5):2620–2629. doi:10.1172/jci137244
31. Ayala A, Herdon CD, Lehman DL, Ayala CA, Chaudry IH. Differential induction of apoptosis in lymphoid tissues during sepsis: variation in onset, frequency, and the nature of the mediators. Blood. 1996;87(10):4261–4275. doi:10.1182/blood.V87.10.4261.bloodjournal87104261
32. Zinellu A, Zinellu E, Mangoni AA, et al. Clinical significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in acute exacerbations of COPD: present and future. Eur Respir Rev. 2022;31(166):220095. doi:10.1183/16000617.0095-2022
33. Liao QQ, Mo YJ, Zhu KW, et al. Platelet-to-Lymphocyte Ratio (PLR), Neutrophil-to-Lymphocyte Ratio (NLR), Monocyte-to-Lymphocyte Ratio (MLR), and Eosinophil-to-Lymphocyte Ratio (ELR) as biomarkers in patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD). Int J Chron Obstruct Pulmon Dis. 2024;19:501–518. doi:10.2147/copd.S447519
34. Matsumura T, Mitani Y, Oki Y, et al. Comparison of geriatric nutritional risk index scores on physical performance among elderly patients with chronic obstructive pulmonary disease. Heart Lung. 2015;44(6):534–538. doi:10.1016/j.hrtlng.2015.08.004
35. Lobo DN, Gianotti L, Adiamah A, et al. Perioperative nutrition: recommendations from the ESPEN expert group. Clin Nutr. 2020;39(11):3211–3227. doi:10.1016/j.clnu.2020.03.038
36. Cadwell JB, Afonso AM, Shahrokni A. Prognostic nutritional index (PNI), independent of frailty is associated with six-month postoperative mortality. J Geriatr Oncol. 2020;11(5):880–884. doi:10.1016/j.jgo.2020.03.013
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.