Back to Journals » OncoTargets and Therapy » Volume 12
Association between potentially functional polymorphisms of chemokine family members and the survival of esophageal cancer patients in a Chinese population
Authors Du JL, Li GN, He RW, Zhang SZ ![]() , Zhang X, Huang ZG
, Zhang X, Huang ZG
Received 26 October 2018
Accepted for publication 26 April 2019
Published 13 June 2019 Volume 2019:12 Pages 4631—4641
DOI https://doi.org/10.2147/OTT.S192362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr XuYu Yang
Jin-Lin Du,1 Ge-Nan Li,2 Rong-Wei He,1 Shi-Zhuo Zhang,1 Xing Zhang,1 Zhi-Gang Huang1
1Department of Epidemiology and Health Statistics, School of Public Health, Guangdong Medical University, Dongguan, Guangdong, 523808, People’s Republic of China; 2Department of Hospital Nutrition, First Affiliated Hospital of PLA General Hospital, Beijing, 100048, People’s Republic of China
Background: The chemokine family plays an important role in the growth, invasion, and metastasis of tumors. However, most studies have only focused on a few genes or a few gene loci, and thus could not reveal the associations between functional polymorphisms of chemokine family members and tumor progression. This study aimed to determine the associations between single nucleotide polymorphisms (SNPs) of chemokine family members and the prognosis of esophageal cancer (EC).
Methods: The Cox risk proportional model and log-rank test were used to analyze the associations of 16 potentially functional SNPs in 13 genes from the chemokine family with the survival of 729 Chinese patients with EC.
Results: Prognostic analysis on the 16 SNPs showed that different genotypes of 5 SNPs were associated with patients’ survival and the risk of death. Multivariate Cox regression analysis showed that the risk of death was higher in CCL26rs2302009 genotype A/C carriers than in A/A carriers and it was also higher in CX3CL1rs2239352 genotype T/T carriers than in C/C carriers. Stepwise Cox regression analysis showed that CCL26rs2302009 genotype A/C was an independent prognostic factor of EC, and its association with increased risk of death was stronger in patients who were ≤60 years old, female, with tumors located in the middle part of esophagus, with undifferentiated or poorly differentiated tumors, with early-stage pathologic type disease, with the longest diameter of tumor ≤5cm than in their counterparts.
Conclusion: These findings suggest that CCL26rs2302009 may be a candidate biomarker for EC and its effect on death risk are associated with the histological grade, pathologic type, and the longest diameter of tumor.
Keywords: esophageal cancer, prognosis, single nucleotide polymorphism, chemotactic factor
Introduction
China has the highest incidence and mortality of esophageal cancer (EC) in the world, with over 50% of new cases and deaths of EC occurring in China every year. More than 90% of patients are diagnosed at middle or late stages.1 Although rapid progress has been made in the treatments of EC, its prognosis remains poor, with a 5-year survival rate of approximately 20% for patients with middle-stage or advanced EC.2 Currently, the main prognostic factors of EC are TNM stage and treatment methods. However, heterogeneity in tumor progression and prognosis has been observed among EC patients who had the same clinical features and underwent the same treatment regimens, which suggests the existence of other important factors that may affect the prognosis. Therefore, the identification of other potential prognostic factors of EC, such as specific biomarkers, is now under investigation.
Dysregulated inflammatory response is known to be associated with increased risk of some chronic diseases, including cancers. Chemokines are a group of small-molecule cytokines (relative molecular weight, 8–14kDa) that have chemo attractant activity. These cytokines all contain 4 conservative cytokines and are classified into CXC, CC, CX3C, and C subfamilies. Chemokine receptors, a group of G protein-coupling transmembrane receptors (GPCR) which mediate functions of chemokines, are usually expressed on the membrane of immunocytes, endothelial cells, and other cells. Chemokine receptors are also classified into 4 subfamilies according to their ligands.3 By binding to specific GPCR, chemokines play roles in many normal biological processes, such as hematopoietic cell genesis, leukocyte migration and homing, and embryonic development, and some pathologic processes, such as inflammatory diseases, virus infection, graft rejection, and malignant tumorigenesis.4 Some studies showed that chemokines play important roles in the growth, angiogenesis, and metastasis of many types of tumor.5 Tumor-associated chemokines not only can promote the proliferation of tumor cells and inhibit apoptosis but also are involved in the migration of tumor cells, angiogenesis of tumors, infiltration of lymphocytes in tumor tissues, and organ-specific metastasis of tumor cells.5 For example, some members of the CC and CXC subfamilies are involved in the angiogenesis of tumors and can promote the invasion and organ-specific metastasis of breast cancer, prostatic cancer, malignant melanoma, and lung cancer.6–9 Abnormal expression of chemokines, such as CXC (α) and CC (β), may affect the tumorigenesis, progression, and prognosis of many types of tumors, including EC.8–11 For example, the high expression of CXCL12 and its receptor CXCR4 was shown to be associated with the invasion and metastasis of EC, and continuous expression of CXCR4 after preoperative radio chemotherapy was associated with early relapse and poor prognosis of EC .9–11
The associations between the polymorphisms of a few genes in the chemokine family and the progression and prognosis of tumors have been studied. CXCL12rs1801157 has been reported to be associated with the risk of breast, lung, rectal, and liver cancers and may be a predictive marker of the lymph node metastasis of colon cancer and distant metastasis of lung cancer.12–14 CXCL14rs2237062 was associated with the progression of HBV-related liver cancer in Chinese populations.15 The C>A mutation of CCL22rs4359426 may aggravate H. pylori infections, increasing the risk of gastric cancer.16 Schimanski et al found that the genotype GA/AA of CXCL12rs1801157 was associated with distant metastasis of EC, which suggested that CXCL12rs1801157 may be a potential prognostic marker of EC.17 Although these studies have shown the associations between polymorphisms of some genes in the chemokine family and the prognosis of some tumors, most studies have only focused on a few genes/polymorphisms, and thus could not reveal associations between functional polymorphisms of chemokine family members and tumor progression. In addition, the results from European and American populations may not be used to predict the situation in Chinese populations.
In the present study, we used the improved multiple ligase detection reaction (iMLDR) genotyping to detect potentially functional SNPs of chemokine family members and to determine their associations with the prognosis of Chinese patients with EC.
Materials and methods
Study population
A total of 729 patients with newly diagnosed EC between January 1, 2004 and December 31, 2013 at Cixian People’s Hospital (Handan, Hebei, People's Republic of China) were selected. All the diagnoses were confirmed pathologically. No patients had a history of other tumors as well as a history of chemotherapy or radiotherapy. Tumor tissue sampling was performed after the doctors explained the potential usage and risks in detail to patients and/or family members. The informed consent was signed by patients and/or family members before sampling. Patients or their family members were interviewed after discharge every 6 months for the first year and every year thereafter until death. The follow-up was ended on August 1, 2015. Patient data were strictly conducted in accordance with the Declaration of Helsinki.
Cixian People’s Hospital affiliated with Guangdong Medical University. Permission to use the data and follow-up results were granted by the Institutional Ethics Review Board of Guangdong Medical University (No. PJ2015042KT).
SNP selection and genotyping
Potentially functional polymorphisms in chemokine family genes were screened using HapMap database (
The genomic DNA was extracted from the 729 EC samples using the AxyPrepMultisource Genomic DNA Minprep Kit (Axygen Bioscience, Union City, CA, USA). SNPs were typed using the imLDRTMMultisource SNP Typing Kit. Blank control in 1 well and repeated samples in 5 parallel wells were set in every 96-well plate for quality control. The SNPs with inconsistent genotypes in repeated samples were excluded, and those with consistent genotypes and with a call rate >95% were considered qualified. MAFs of the SNPs were compared with those in the HapMap-HCB (Han Chinese) database: the SNPs with a MAF difference <0.05 were considered qualified, whereas those with a MAF difference >0.05 were subjected to re-typing to rule out the mistakes in typing. The D’ values between every two SNPs were analyzed using the Haplo View software to rule out the mistakes in typing.
Statistical analysis
Hardy–Weinberg equilibrium of the genotypes of identified SNPs among patients was assessed using a goodness-of-fit chi-square test. The median survival was calculated using the Kaplan–Meier method. Survival curves were plotted using the Kaplan–Meier method, and survival data were compared using the log-rank test. Univariate and multivariate Cox proportional hazard regression analyses were performed to estimate the crude or adjusted HR and their 95% CIs, with adjustment of age, gender, smoking history, histological type, clinical stage, and treatment. Cox stepwise regression analysis was also conducted to determine predictive factors of the prognosis of EC, with a significance level of 0.05 for entering and 0.10 for removing the respective explanatory variables. The associations between CCL26 rs2302009 genotypes and EC survival were evaluated by stratified analysis of age, gender, histological types, anatomical site, pathologic grade, pathologic type, TNM stage, and longest diameter of tumor. All the statistical analyses were carried out using SAS statistical package version 9.1 (SAS Institute Inc., Cary, NC, USA).
Results
Clinicopathologic characteristics of patients
Of the 729 patients, 676 were followed, with a follow-up rate of 92.7%. Among the followed-up patients, 241 died. The median survival time was 63.0 months. Age, histological type, and tumor location had no relationship with the patient survival. Gender, histological grade, pathologic type (according to the classification of International Union Against Cancer, the pathological types of early EC include erosive type, plaque type, hidden type and nipple type according to its morphology, while the middle and late EC included medullary type, mushroom type, ulcerative type, constrictive type, intraluminal type and undefined type), TNM stage, and the longest diameter of tumor were associated with the patient survival (Table 1).
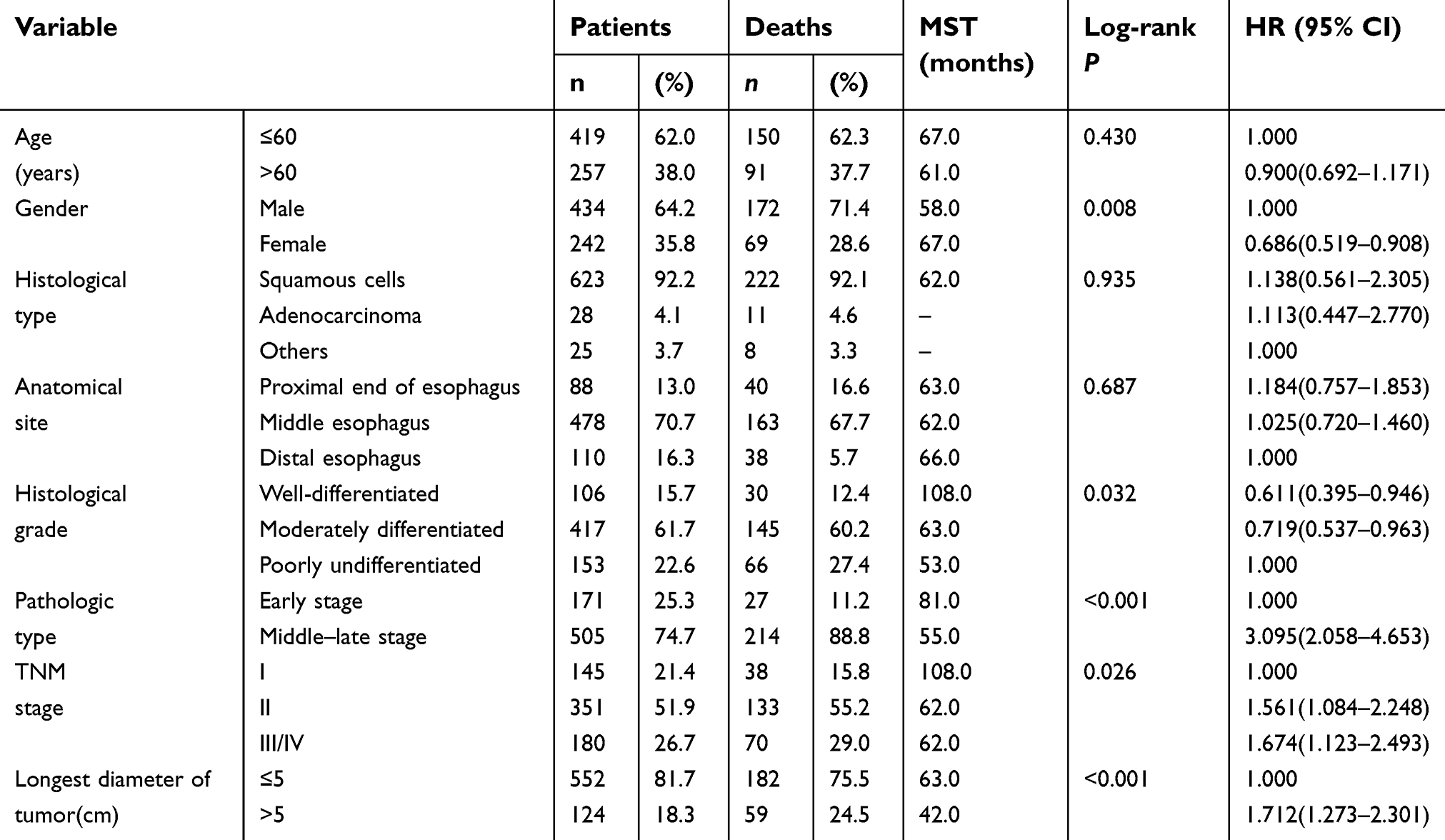 | Table 1 Patient characteristics and features |
Associations of SNPs of chemokine family members with the patient survival
We identified 17 potentially functional SNPs in 14 genes from the chemokine family. Among the 17 SNPs, rs3136667 showed three genotypes (C, G, and A) according to the data in the NCBI database. In addition, the primers for extension could not be designed because both ends of its sequence were G. Therefore, rs3136667 was excluded, and 16 SNPs in 13 genes were finally selected. For the 16 SNPs, the call rates of genotyping were all above 90%, and their MAF and Hardy–Weinberg equilibrium values were all above 0.05. These genes and SNPs are presented in Table 2. Prognostic analysis on the 16 SNPs showed that different genotypes of 5 SNPs were associated with the patient survival.
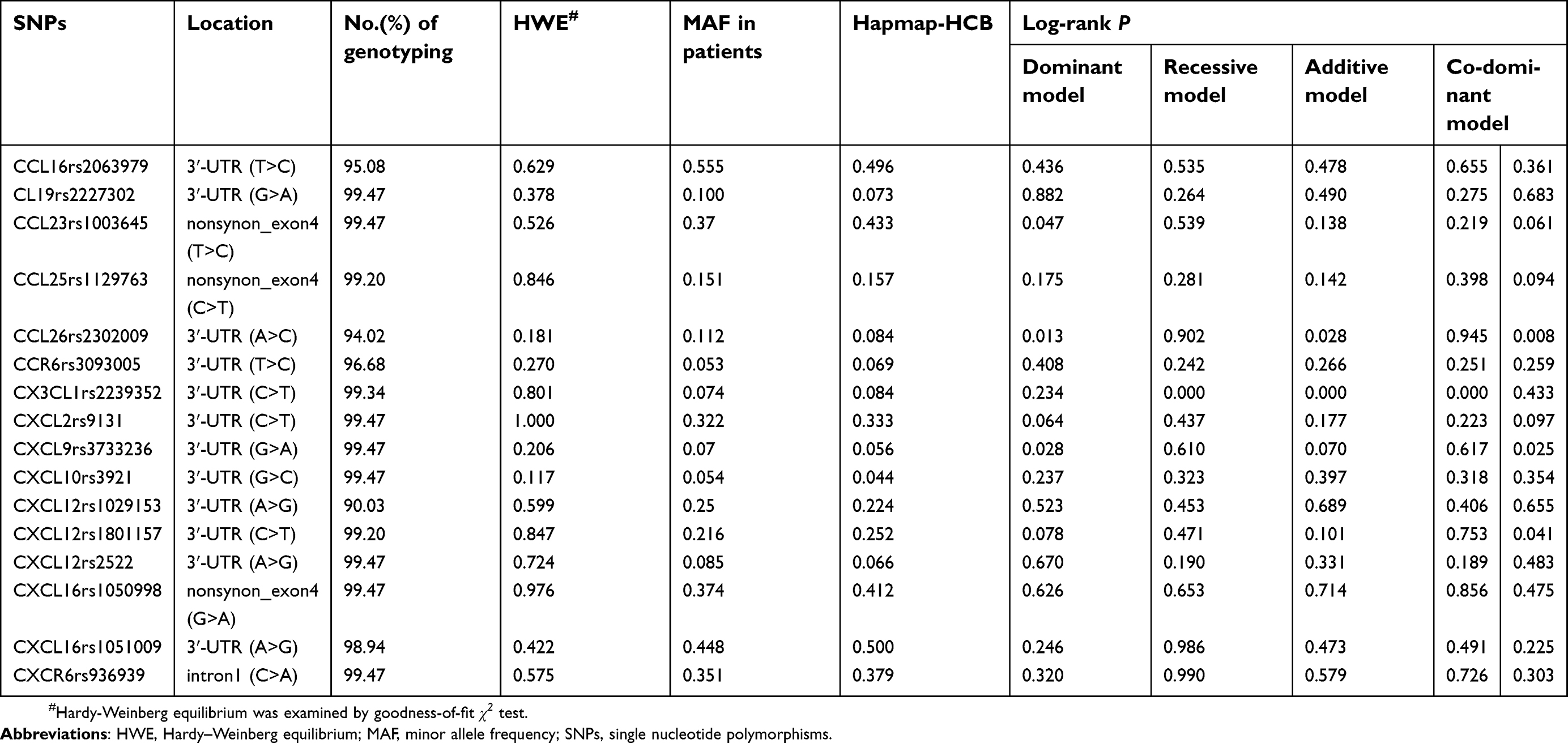 | Table 2 Genotyping of selected SNPs of chemokine family and their associations with esophageal cancer survival in genetic models |
Multivariate Cox regression analysis on the prognostic values of the 5 SNPs showed that CCL26rs2302009 and CX3CL1rs2239352 were associated with the prognosis of EC patients (Table 3). After adjustment of age, gender, histological type, tumor location, histological grade, pathologic type, TNM stage, and the longest diameter of tumor, the heterozygous mutation genotype A/C of CCL26rs2302009 and the homozygous mutation genotype T/T of CX3CL1rs2239352 were associated with increased risk of death. The risk of death among patients who carried both risk genotypes was increased by 303.7% as compared with that among patients who carried only one or none of the two risk genotypes.
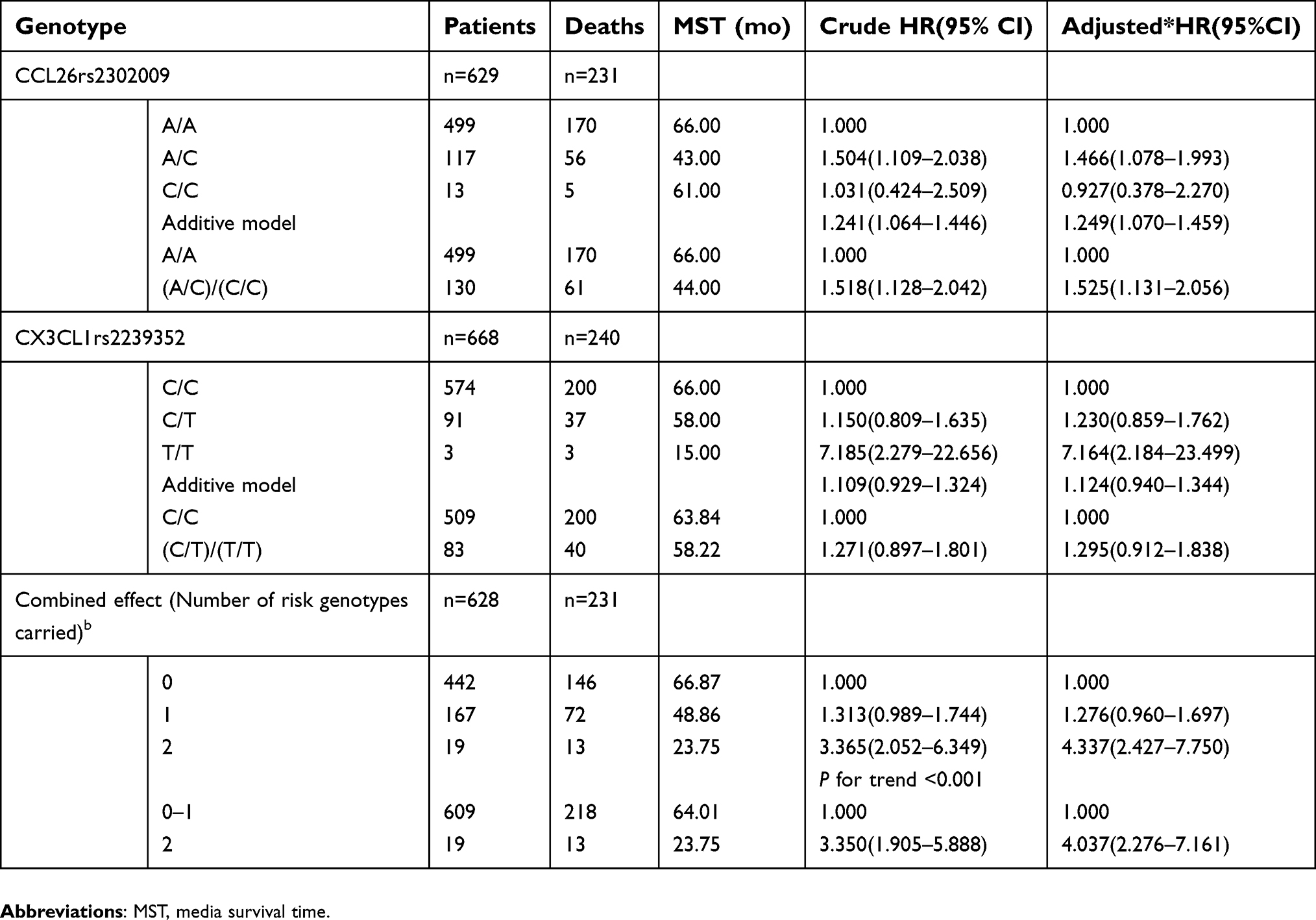 | Table 3 Polymorphisms of chemokine family and their associations with esophageal cancer survival |
Independent predictors of the patient survival
To identify independent prognostic factors, age, gender, histological type, tumor location, histological grade, pathologic type, TNM stage, the longest diameter of tumor, CCL26rs2302009 genotypes, and CX3CL1rs2239352 genotypes were included in stepwise Cox regression analysis. Histological grade, pathologic type, the longest diameter of tumor, and CCL26rs2302009 genotype A/C were identified as independent prognostic factors (Table 4).
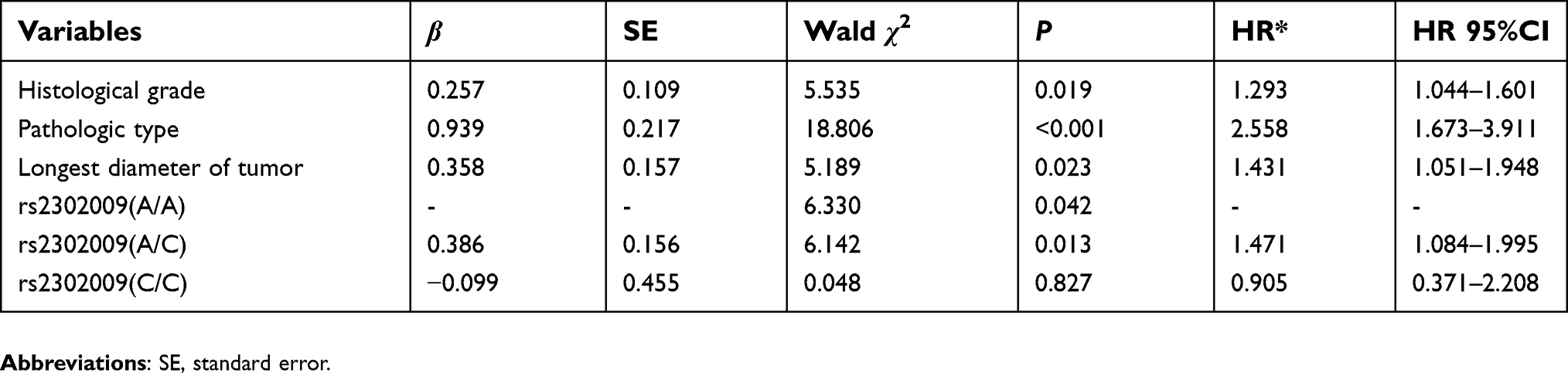 | Table 4 Multivariate Cox regression analysis on esophageal cancer related survival |
Stratified analysis on the prognostic value of CCL26rs2302009 genotype A/C
Stratified analysis showed that the association between CCL26rs2302009 genotype A/C and the increased risk of death was stronger in patients who were ≤60 years old, female, with tumors located in the middle part of esophagus, with undifferentiated or poorly differentiated tumors, with early-stage pathologic type disease, with the longest diameter of tumor ≤5cm than in their counterparts (Table 5). Kaplan–Meier plots of EC-specific survival by rs2302009 genotypes and histological grade, pathologic type or the longest diameter are shown in Figures 1, 2 and 3.
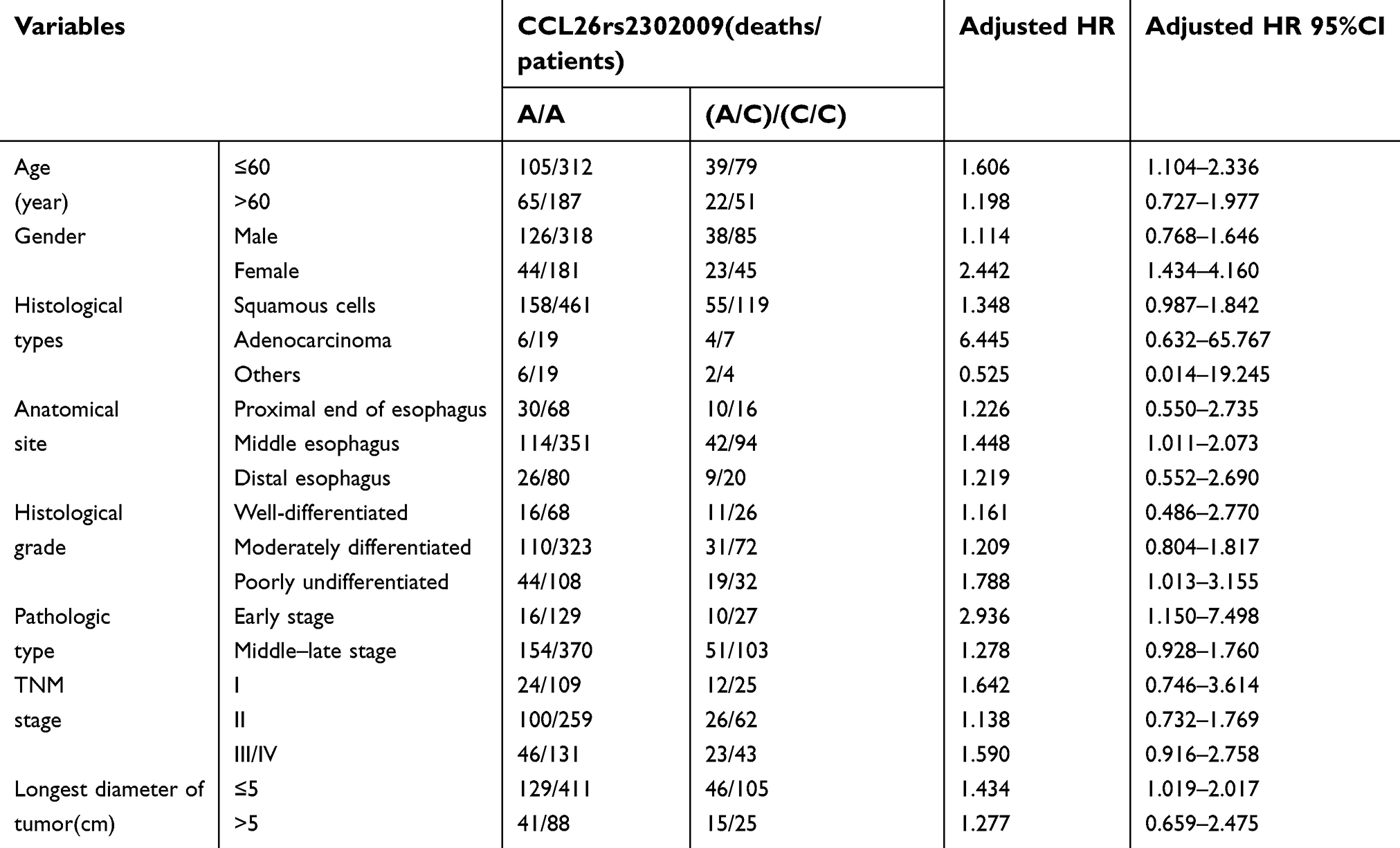 | Table 5 Stratified analysis of variants genotypes associated with EC survival |
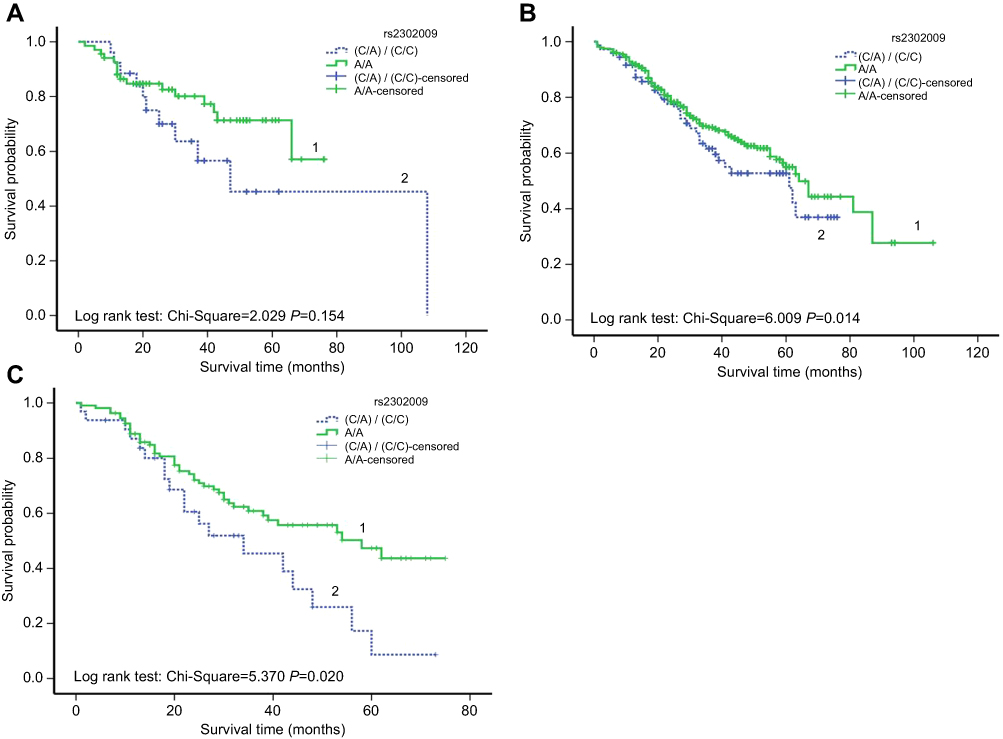 | Figure 1 Kaplan-Meier plots of survival by CCL26rs2302009 genotypes and histological grade in EC-specific survival. (A) Strata with the well-differentiated histological grade (log-rank P=0.154); “1” means patients with genotype (A/A) and with the well-differentiated histological grade; “2” means patients with genotype (C/A)/(C/C) and with the well-differentiated histological grade. (B) Strata with the moderately-differentiated histological grade (log-rank P=0.014 );“1” means patients with genotype (A/A) and with the moderately-differentiated histological grade; and “2” means patients with genotype (C/A)/(C/C) and with the moderately-differentiated histological grade. (C) Strata with the poorly-undifferentiated histological grade (log-rank P=0.020);“1” means patients with genotype (A/A) and with the poorly-undifferentiated histological grade; and “2” means patients with genotype (C/A)/(C/C) and with the poorly-undifferentiated histological grade. |
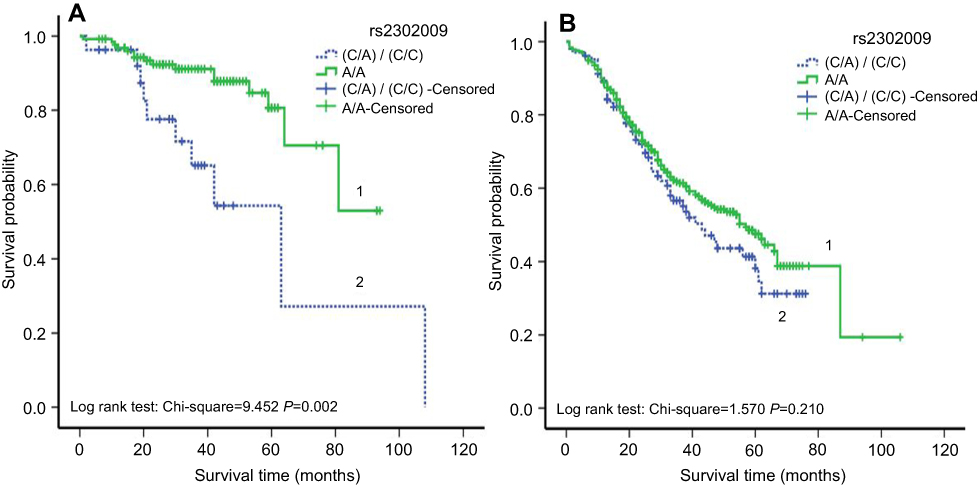 | Figure 2 Kaplan-Meier plots of survival by CCL26rs2302009 genotypes and pathologic type in EC-specific survival. (A) Strata with the early stage of pathologic type (log-rank P=0.002); “1” means patients with genotype (A/A) and with the early stage of pathologic type; “2” means patients with genotype (C/A)/(C/C) and with the early stage of pathologic type. (B) Strata with the middle-late stage of pathologic type (log-rank P=0.210 ); “1” means patients with genotype (A/A) and with the middle-late stage of pathologic type; and “2” means patients with genotype (C/A)/(C/C) and with the middle-late stage of pathologic type. |
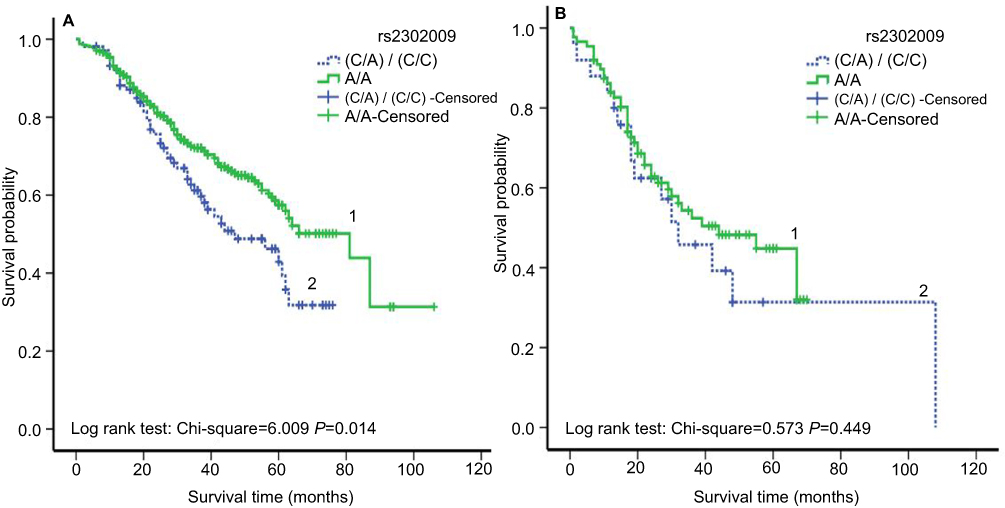 | Figure 3 Kaplan-Meier plots of survival by CCL26rs2302009 genotypes and the longest diameter of tumor in EC-specific survival. (A) Strata with ≤5cm of the longest diameter (log-rank P=0.014); “1” means patients with genotype (A/A) and with ≤5cm of the longest diameter; “2” means patients with genotype (C/A)/(C/C) and with ≤5cm of the longest diameter. (B) Strata with >5cm of the longest diameter (log-rank P=0.449 ); “1” means patients with genotype (A/A) and with >5cm of the longest diameter; and “2” means patients with genotype (C/A)/(C/C) and with >5cm of the longest diameter. |
Discussion
In the present study, we analyzed the associations between potentially functional SNPs of genes from the chemokine family and prognosis of EC patients after surgery. Multivariate Cox regression analysis showed that CCL26rs2302009 and CX3CL1rs2239352 genotypes were associated with the prognosis. Stepwise Cox regression analysis showed that histological grade, pathologic type, the longest diameter of tumor, and CCL26rs2302009 genotype A/C were the independent prognostic factors. These findings suggest that, in addition to pathologic stage, pathologic type, and the longest diameter of tumor, CCL26 rs2302009 may be a candidate biomarker for the prediction of the survival of EC patients and may affect the risk of death.
In 2001, Muller et al found that tumor cells may achieve organ-specific metastasis through the binding of chemokines and their receptors.18–20 Since then, accumulating evidence showed that the specific binding of chemokines and their receptors played a key role in the growth, invasion, and metastasis of malignant tumors.20,21 The poor prognosis of malignant tumor is associated with tumor metastasis, which is a highly tissue- and organ-selective, complex process.22 CCL26 is a member of the chemokine CC subfamily and acts on eosinophil granulocytes and T lymphocytes.22 Its receptor CCR3 is produced by epithelial cells and may contribute to the accumulation and local infiltration of eosinophil granulocytes. As the activator of CCR3, CCL26 attracts and activates eosinophil granulocytes, basophils, and Type 2 helper (Th2) T lymphocytes. CCL26 is also an antagonist of CCR1, CCR2, and CCR5.23 Heresi et al found that CCL26 inhibited the function of monocyte chemotactic protein-1 (MCP-1, also termed CCL2).23–25 Therefore, we consider that CCL26 may regulate the inflammation. CCL26 has been reported to be expressed in several types of solid tumor and plays important roles in the migration, infiltration, metastasis, and prognosis of the tumor.24,25 Blanchard et al reported that external stimulation or damage may induce the activation of CCL26.26 CCL26 gene products have a chemotactic effect on eosinophil granulocytes. The secretion from eosinophil granulocytes contains vascular endothelial growth factor, and the accumulation of eosinophil granulocytes may improve angiogenesis in tumor tissues. This may explain, in part, the role of CCL26rs2302009 mutation in facilitating tumor metastasis and causing poor prognosis. CCL26 may attract macrophages to secrete abundant cytokines, induce angiogenesis, and lead to the deterioration of the tumor.27 It is noteworthy that CCL26 is also an activator of CX3CR1. When the expression of CX3CR1 is low, both CCL26 and CX3CL1 attract eosinophil granulocytes to accumulate in tumor tissues.28 In the present study, we found that CCL26 mutations were associated with poor prognosis of EC patients after surgery. A similar result was reported by Yang et al in a tissue microarray study.29
In the present study, we found that CCL26rs2302009 genotype A/C could be an independent prognostic factor of EC after surgery. Stratified analysis showed that the association of CCL26rs2302009 genotype A/C with increased risk of death was stronger in patients who were ≤60 years old, female, with tumors located in the middle part of the esophagus, with undifferentiated or poorly differentiated tumors, with early-stage pathologic type disease, and with the longest diameter of tumor ≤5cm than in their counterparts. This finding may be used to guide the individualized therapy for EC. In an extensive genomic study on 117 patients with eosinophilic esophagitis conducted by Blanchard et al, the CCL26rs2302009 mutation was found in people who were susceptible to eosinophilic esophagitis, and this mutation increased the stability of CCL26 mRNA.26 Therefore, we speculate that CCL26rs2302009 genotype A/C may increase the stability of CCL26 mRNA in EC patients, and affect the transcription and expression of the CCL26 gene. The continuous expression of CCL26 in esophageal tissues may induce severe infiltration of the eosinophil granulocytes and angiogenesis in the tumor tissues, leading to the metastasis of the tumor and resulting in poor prognosis. However, the biological effects of CCL26 and its receptor CCR3 are complex and may be affected by other factors. For example, abnormal expression of CCL26 is regulated by the signal transducer and activator of transcription 6 (STAT6) or other signaling pathways.30 The synergetic effect of CCL26 and CX3CL1 may induce high expression of CX3CR1, attracting eosinophil granulocytes to accumulate in the tumor tissues.28 However, the exact biological mechanisms and associated with signaling pathways need to be determined in future functional studies.
Several limitations of the present study need to be mentioned. First, EC patients were selected from a single hospital, with limited representativeness for general application. Second, due to the genotyping failure, other SNPs were not included in statistical analyses to analyze their associations with the prognosis of EC, which suggested the existence of information bias. Third, the exact biological mechanisms are still unclear and need to be validated through functional analyses in large cohort studies involving multiple races.
Conclusion
In the chemokine family, CCL26rs2302009 genotype A/C is associated with the poor prognosis of EC patients and may be a candidate prognostic factor of EC.
Ethics approval and consent to participate
This manuscript was approved by the Institutional Ethics Review Board of Guangdong Medical University.
Abbreviation list
SNPs, single nucleotide polymorphisms; EC, esophageal cancer; GPCR, G protein-coupling transmembrane receptors; MAF, a minor allele frequency; iMLDR, the improved multiple ligase detection reaction.
Acknowledgments
We acknowledge the participants of this study for their contribution to making this study possible. We are also grateful to the staff at Cixian People’s Hospital for their efforts in the data linkage and follow-up. This work was supported by grants from the Natural Science Fund Project of Guangdong province, China (No.2016A030313683), the Social Science and Technology Development Project of Dongguan, Guangdong Province, China (No.2013108101052, 2014108101051, 2016108101039), the priority discipline Public Health and Preventive Medicine Project of Guangdong province, China (No.4SG17043), and the Characteristics of Innovative Projects of Colleges and Universities of Guangdong province, China (No.2015KTSCX052).
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
2. Zhang H, Ping Y, Du X. [Study on factors influencing survival in patients with cancer of the esophagus after resection by Cox proportional hazard model]. Zhonghua Zhong Liu Za Zhi. 1999;21(1):32–34.
3. Fridman WH, Pages F, Sautes-Fridman C, Galon J. The immune contexture in human tumours: impact on clinical outcome. Nat Rev Cancer. 2012;12(4):298–306. doi:10.1038/nrc3245
4. Mishra PBD, Ben-Baruch A. Chemokines at the crossroads of tumor-fibroblast interactions that promote malignancy. J Leukoc Biol. 2011;89(1):9. doi:10.1189/jlb.0310182
5. Zhang J, Patel L, Pienta KJ. CC chemokine ligand 2 (CCL2) promotes prostate cancer tumorigenesis and metastasis. Cytokine Growth Factor Rev. 2010;21(1):41–48. doi:10.1016/j.cytogfr.2009.11.009
6. Wolf MJ, Seleznik GM, Zeller N, Heikenwalder M. The unexpected role of lymphotoxin beta receptor signaling in carcinogenesis: from lymphoid tissue formation to liver and prostate cancer development. Oncogene. 2010;29(36):5006–5018. doi:10.1038/onc.2010.260
7. Colotta F, Allavena P, Sica A, Garlanda C, Mantovani A. Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis. 2009;30(7):1073–1081. doi:10.1093/carcin/bgp127
8. Ben-Baruch A. The multifaceted roles of chemokines in malignancy. Cancer Metastasis Rev. 2006;25(3):357–371. doi:10.1007/s10555-006-9003-5
9. Zlotnik A, Burkhardt AM, Homey B. Homeostatic chemokine receptors and organ-specific metastasis. Nat Rev Immunol. 2011;11(9):597–606. doi:10.1038/nri3049
10. Moser B, Wolf M, Walz A, Loetscher P. Chemokines: multiple levels of leukocyte migration control. Trends Immunol. 2004;25(2):75–84. doi:10.1016/j.it.2003.12.005
11. Mantovani A, Sica A, Sozzani S, Allavena P, Vecchi A, Locati M. The chemokine system in diverse forms of macrophage activation and polarization. Trends Immunol. 2004;25(12):677–686. doi:10.1016/j.it.2004.09.015
12. Muller A, Homey B, Soto H, et al. Involvement of chemokine receptors in breast cancer metastasis. Nature. 2001;410(6824):50–56. doi:10.1038/35065016
13. Murakami T, Maki W, Cardones AR, et al. Expression of CXC chemokine receptor-4 enhances the pulmonary metastatic potential of murine B16 melanoma cells. Cancer Res. 2002;62(24):7328–7334.
14. Kang Y, Siegel PM, Shu W, et al. A multigenic program mediating breast cancer metastasis to bone. Cancer Cell. 2003;3(6):537–549.
15. Soria G, Yaal-Hahoshen N, Azenshtein E, et al. Concomitant expression of the chemokines RANTES and MCP-1 in human breast cancer: a basis for tumor-promoting interactions. Cytokine. 2008;44(1):191–200. doi:10.1016/j.cyto.2008.08.002
16. Wang G, Yu D, Tan W, Zhao D, Wu C, Lin D. Genetic polymorphism in chemokine CCL22 and susceptibility to Helicobacter pylori infection-related gastric carcinoma. Cancer. 2009;115(11):2430–2437. doi:10.1002/cncr.24255
17. Wiley HE, Gonzalez EB, Maki W, Wu MT, Hwang ST. Expression of CC chemokine receptor-7 and regional lymph node metastasis of B16 murine melanoma. J Natl Cancer Inst. 2001;93(21):1638–1643.
18. Mulller AHB, Soto H, Soto H, et al. Involvement of chemokine receptors in breastcancer metastasis. Nature. 2001;410(6824):7. doi:10.1038/35065016
19. Sarvaiya PJ, Guo D, Ulasov I, Gabikian P, Lesniak MS. Chemokines in tumor progression and metastasis. Oncotarget. 2013;4(12):2171–2185. doi:10.18632/oncotarget.1426
20. Tanaka T, Bai Z, Srinoulprasert Y, Yang BG, Hayasaka H, Miyasaka M. Chemokines in tumor progression and metastasis. Cancer Sci. 2005;96(6):317–322. doi:10.1111/j.1349-7006.2005.00059.x
21. Comar M, Zanotta N, Zanconati F, et al. Chemokines involved in the early inflammatory response and in pro-tumoral activity in asbestos-exposed workers from an Italian coastal area with territorial clusters of pleural malignant mesothelioma. Lung Cancer. 2016;94:61–67. doi:10.1016/j.lungcan.2016.01.020
22. Heiman AS, Abonyo BO, Darling-Reed SF, Alexander MS. Cytokine-stimulated human lung alveolar epithelial cells release eotaxin-2 (CCL24) and eotaxin-3 (CCL26). J Interferon Cytokine Res. 2005;25(2):82–91. doi:10.1089/jir.2005.25.82
23. Heresi GA, Wang J, Taichman R, et al. Expression of the chemokine receptor CCR7 in prostate cancer presenting with generalized lymphadenopathy: report of a case, review of the literature, and analysis of chemokine receptor expression. Urol Oncol. 2005;23(4):261–267. doi:10.1016/j.urolonc.2005.02.004
24. Sugaya M. Chemokines and skin diseases. Arch Immunol Ther Exp (Warsz). 2015;63(2):109–115. doi:10.1007/s00005-014-0313-y
25. Prakash S, Agrawal S, Vahed H, et al. Dendritic cells from aged subjects contribute to chronic airway inflammation by activating bronchial epithelial cells under steady state. Mucosal Immunol. 2014;7(6):1386–1394. doi:10.1038/mi.2014.28
26. Blanchard C, Stucke EM, Rodriguez-Jimenez B, et al. A striking local esophageal cytokine expression profile in eosinophilic esophagitis. J Allergy Clin Immunol. 2011;127(1):
27. Roth N, Stadler S, Lemann M, Hosli S, Simon HU, Simon D. Distinct eosinophil cytokine expression patterns in skin diseases - the possible existence of functionally different eosinophil subpopulations. Allergy. 2011;66(11):1477–1486. doi:10.1111/j.1398-9995.2011.02694.x
28. Nakayama TWY, Oiso N, Oiso N, et al. Eotaxin-3/CC chemokine ligand 26 is a functional ligand for CX3CR1. J Immunol. 2010;185(11):8. doi:10.4049/jimmunol.0904126
29. Yang X. Expression and clinical significance of CCL26 in esophageal squamous cell carcinoma tissues. China Oncology. 2015;25(1):13–18.
30. Krishnamurthy P, Sherrill JD, Parashette K, et al. Correlation of increased PARP14 and CCL26 expression in biopsies from children with eosinophilic esophagitis. J Allergy Clin Immunol. 2014;133(2):577–580. doi:10.1016/j.jaci.2013.09.031
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.