Back to Journals » Clinical Interventions in Aging » Volume 17
Association Between Polypharmacy, Anxiety, and Depression Among Chinese Older Adults: Evidence from the Chinese Longitudinal Healthy Longevity Survey
Received 29 November 2021
Accepted for publication 28 February 2022
Published 6 March 2022 Volume 2022:17 Pages 235—244
DOI https://doi.org/10.2147/CIA.S351731
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Zhi-Ying Wu
Cheng Cheng,1 Jie Bai2
1School of Nursing, Shanghai Medical College, Fudan University, Shanghai, People’s Republic of China; 2Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Cheng Cheng, Tel/Fax +86-21-64431003, Email [email protected]
Purpose: To investigate the association between polypharmacy, anxiety, and depression among Chinese older adults.
Patients and Methods: The data used in this study were from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), the 2018 wave. Polypharmacy status was measured by the accumulation of self-reported medications. Anxiety and depression were assessed by the Generalized Anxiety Disorder (GAD-7) scale and the Center for Epidemiologic Studies Depression Scale (CES-D-10), respectively. Logistic regression models were performed.
Results: A total of 2484 Chinese older adults (female: 1321, 53.2%) aged from 60 to 117 years old were included in the analysis. Regression analysis showed that polypharmacy was associated with depression after controlling for the covariates. No association was observed between polypharmacy and anxiety.
Conclusion: There was a suggestive link between polypharmacy and depression among Chinese older adults. Having polypharmacy might be an indicator for the possible depression among this population, but a comprehensive assessment of polypharmacy is necessary.
Keywords: anxiety, depression, multimorbidity, older adults, polypharmacy
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
Polypharmacy is defined as an individual taking 2 to 11 medications concurrently and/or receiving unnecessary/unwanted prescription drugs.1,2 Research has linked polypharmacy with substantial healthcare costs, reduced physical function, and impaired cognitive ability.3 People with polypharmacy may have a higher risk of adverse drug events and drug-drug interactions, which are related to frequent hospital admissions and increased morbidity and mortality.3 Qualitative findings also have shown that polypharmacy poses many challenges in people’s daily lives and may impact their self-perceptions regarding medications.4,5
Polypharmacy is a common concern among older adults due to their geriatric syndromes and age-related physiologic changes.6,7 The prevalence of polypharmacy has been documented before, varying in definitions, research settings, and geographical places. For example, a national survey from Denmark showed that the prevalence of polypharmacy (> 5 different medications) was around 50% among older adults (≥ 75 years old) and 12% among the general population.8 In the US, approximately 40% of older adults (≥ 65 years old) reported having polypharmacy and the rate was 15% for the general population.9 Another population-based study found that more than 35% of Australians aged more than 70 years old were affected by polypharmacy.10 At six tertiary-level hospitals in China, a cohort study found that the prevalence of polypharmacy was 24% among adults aged ≥ 65 years.11 Longitudinal research presented that older adults aged ≥ 80 years reported taking 9.56 ± 5.68 medications regularly and the prevalence of polypharmacy (≥ 6 medications) was 70%.12 A retrospective cross-sectional study found that the prevalence of polypharmacy was 72.2% among 3370 Chinese type 2 diabetes patients and eight medications were prescribed per person approximately. Risk factors related to polypharmacy were age, duration of diseases, length of hospital stay, and comorbidities.13 A study in Germany found that multiple chronic conditions, frailty, high BMI, and poor physical and mental health were associated with excessive polypharmacy.14
Psychological distress in the forms of anxiety and depression is found to be associated with polypharmacy. A meta-analysis showed that people with polypharmacy might have an increased risk of depression.15 Another study in the US identified that having polypharmacy resulted in poor self-reported health status and more symptoms of depression in African Americans.16 However, there is no census regarding such an association.17 Moreover, guidelines based on a single disease model are largely applied and specialist care is still commonly observed in China,18 which are key drivers for polypharmacy. Although a patient with multimorbidity may benefit from the prescription of multiple medicines, it is needed to recognize those who may be at risk of psychological distress due to polypharmacy.
The current study aimed to examine the association between polypharmacy and psychological distress including anxiety and depression among a group of Chinese older adults.
Materials and Methods
Study Design
The current study was a secondary analysis of the latest CLHLS data, the CLHLS 2018 wave.19
The CLHLS is a nationwide, longitudinal survey regarding the aging population administered by Peking University Center for Healthy Aging and Development Studies and the National School of Development of Peking University. More details regarding the CLHLS were previously published.20
Sample
The CLHLS has conducted eight waves of surveys on health status and quality of life from 1998 to 2018 in 22 provinces in China by using a multi-stage random sampling method with unequal proportions. The 2018 wave has surveyed over 15,000 individuals aged more than 65 years old between 2017–2018 from 23 provinces in mainland China. Of those, 10 had been interviewed since 1998 and 30 since 2000. Of 790 had been interviewed since 2002, 1330 since 2005, 2440 since 2008/2009, and 2884 since 2011/2012. Of 3463 people were surveyed in 2014 and 12,411 were first interviewed in 2018.
A structured, face-to-face questionnaire was administered by trained research assistants to collect data of interest. Participants were asked about their sociodemographic information including age, sex, ethnicity, marital status, education, etc. To determine their status of health, participants were asked if they suffered from chronic diseases such as hypertension, diabetes, heart disease, etc., and treatment. Health-related information such as diet and nutrition, drinking and smoking habits, lifestyle were asked. In addition, family information regarding siblings, parents, and children was also surveyed.
To ensure the quality of analysis, the samples with missing values or answers of “I don’t know/have no idea” in any variables of interest would be excluded in this study.
Measures
Dependent Variables
Anxiety was evaluated by the Generalized Anxiety Disorder (GAD-7) scale in this study.21 The GAD-7 includes seven items using a four-point metric, ranging from 0 = “Not at all” to 3 = “Almost every day”. The total scores of GAD-7 range from 0 to 21 with higher scores suggesting more symptoms of anxiety. A cut-off score ≥ 10 was defined as an individual with anxiety symptoms.22 Previous research has validated the GAD-7 in Chinese people and showed good psychometric properties.23 In this study, the Cronbach alpha coefficient of GAD-7 was 0.909.
Depression was evaluated by the Center for Epidemiologic Studies Depression Scale (CES-D-10) in this study. The CES-D-10 includes ten items using a four-point metric, ranging from 0 = “Rarely” to 3 = “Most of the time”. The total scores of CES-D-10 range from 0 to 30 with higher scores suggesting more symptoms of depression. An individual is suggested to have depressive symptoms if he/she scored more than 10 in the CES-D-10.24 Previous research has used CES-D-10 in Chinese people and reported its good validity and reliability.25 In this study, the Cronbach alpha coefficient of CES-D-10 was 0.719.
Independent Variables
The CLHLS survey asked participants to report whether they have had a chronic disease based on a list of 24 diseases, followed by a question regarding treatment “Are you taking medicine for this disease”. The included diseases were hypertension, diabetes, heart disease, stroke/CVD, bronchitis (emphysema, pneumonia, asthma), tuberculosis, cataract, glaucoma, cancer, prostate tumor, Parkinson disease, bedsore, arthritis, dementia, epilepsy, cholecystitis, dyslipidemia, rheumatoid disease, chronic nephritis, mammary gland hyperplasia, uterine tumor, prostatic hyperplasia, and hepatitis. A systematic review has indicated that there was a lack of a universal and accurate definition of polypharmacy and most studies reported category of definitions for polypharmacy was numerical only.26 Therefore, this study used the numerical definition, which calculated the number of medications to define polypharmacy. A participant reported taking five or more medications for different chronic diseases would be considered having polypharmacy in this study.
Covariates
This study controlled a range of possible confounding factors including sociodemographic variables (eg age, residential status, and education level), clinical variables (eg medical history), lifestyles (eg smoking and alcohol consumption), and self-reported health status (eg general health). Quality of life was evaluated with one self-reported question “How do you rate your health at present?”. This question was answered with a five-point scale ranging from 1 (very good) to 5 (very bad).
Statistical Methods
Descriptive analysis was used to describe the general characteristics of the sample. Multivariate logistic regression analysis with forward selection was used to examine the association between polypharmacy (independent variable) and anxiety and depression (dependent variables). In the regression models, having potential anxiety coded as 1 versus no/minor anxiety coded as 0. The base model (Model 1) included polypharmacy and anxiety, model 2 further controlled for sociodemographic variables and lifestyles, and model 3 additionally controlled for clinical variables and self-reported health status. After that, analysis for depression was performed with repeated steps as above. Adjusted odds ratios (OR) and 95% confidence intervals (95% CI) were reported.
Sensitivity analysis approaches were conducted to examine the robustness of the results. The authors performed sensitivity analysis after categorizing cases into “Multimorbidity group” and “None-multimorbidity group” and performed the regression among the “Multimorbidity group”. In this study, multimorbidity refers to a person who has two or more chronic diseases.27
The data analyses were performed by using SPSS software (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp.) The statistical significance was set at a value of p < 0.05.
Ethical Considerations
The Ethics Committees of Human Research at Peking University and Duke University approved the CLHLS study (Reference number: IRB00001052–13074; Pro00062871). Each participant gave informed consent before participation.
The CLHLS data were stored in Peking University Open Research Data Platform and permission to access the raw data was required. This study acquired the data by applying for a data use agreement.
Results
Description of the Sample
A total of 2484 Chinese older adults (female: 1321, 53.2%) aged from 60 to 117 years old were included in the analysis. Rural participants prevailed (1715, 69%). Most participants were living with house members. See Table 1.
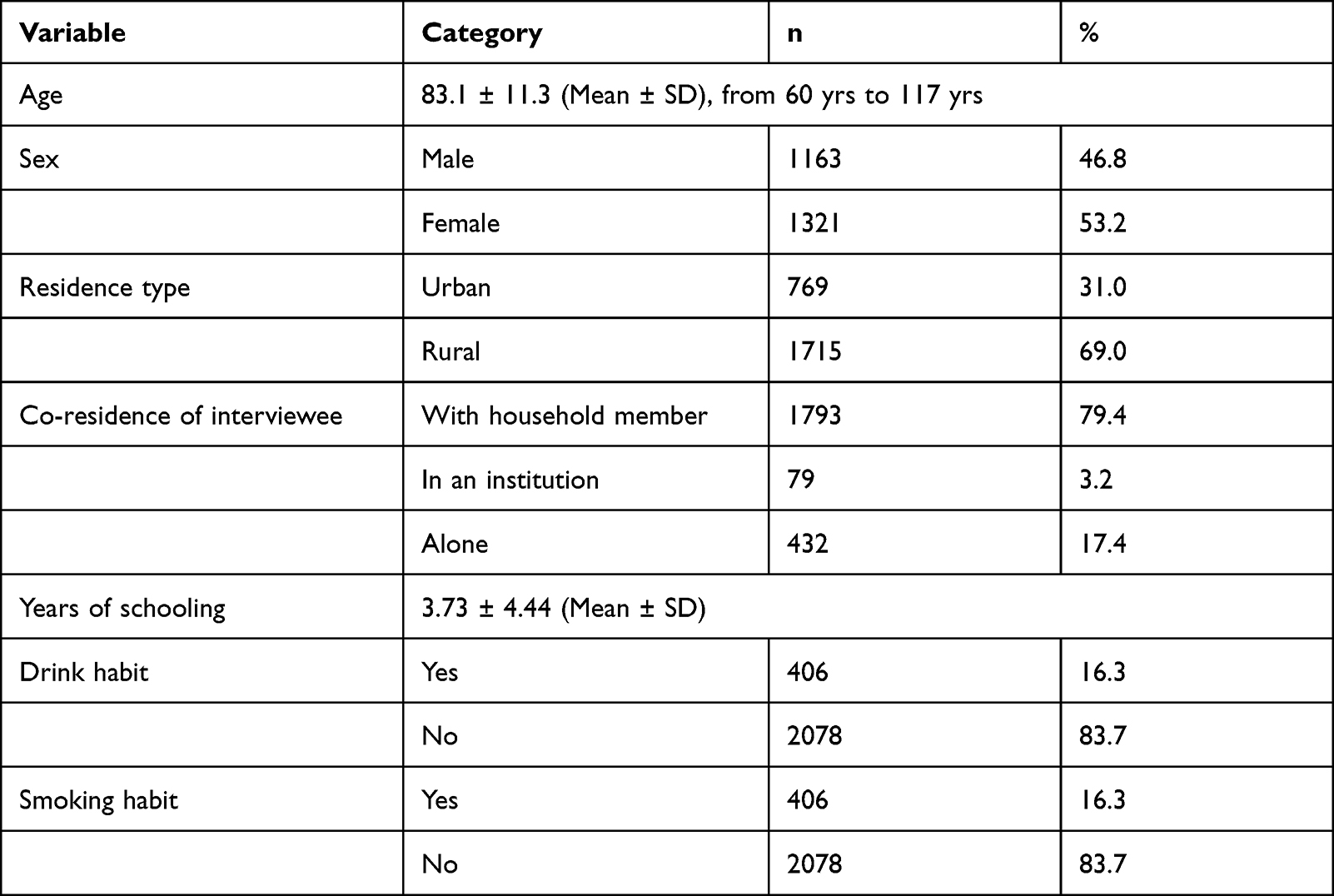 |
Table 1 Description of Sociodemographic Variables, Lifestyles, and Clinical Variables (N = 2484) |
Most participants (68.2%) at least reported having one chronic health condition and almost two in five had multimorbidity. More than half reported taking medications for the corresponding chronic health conditions and the prevalence of polypharmacy was 2.1%. See Table 2.
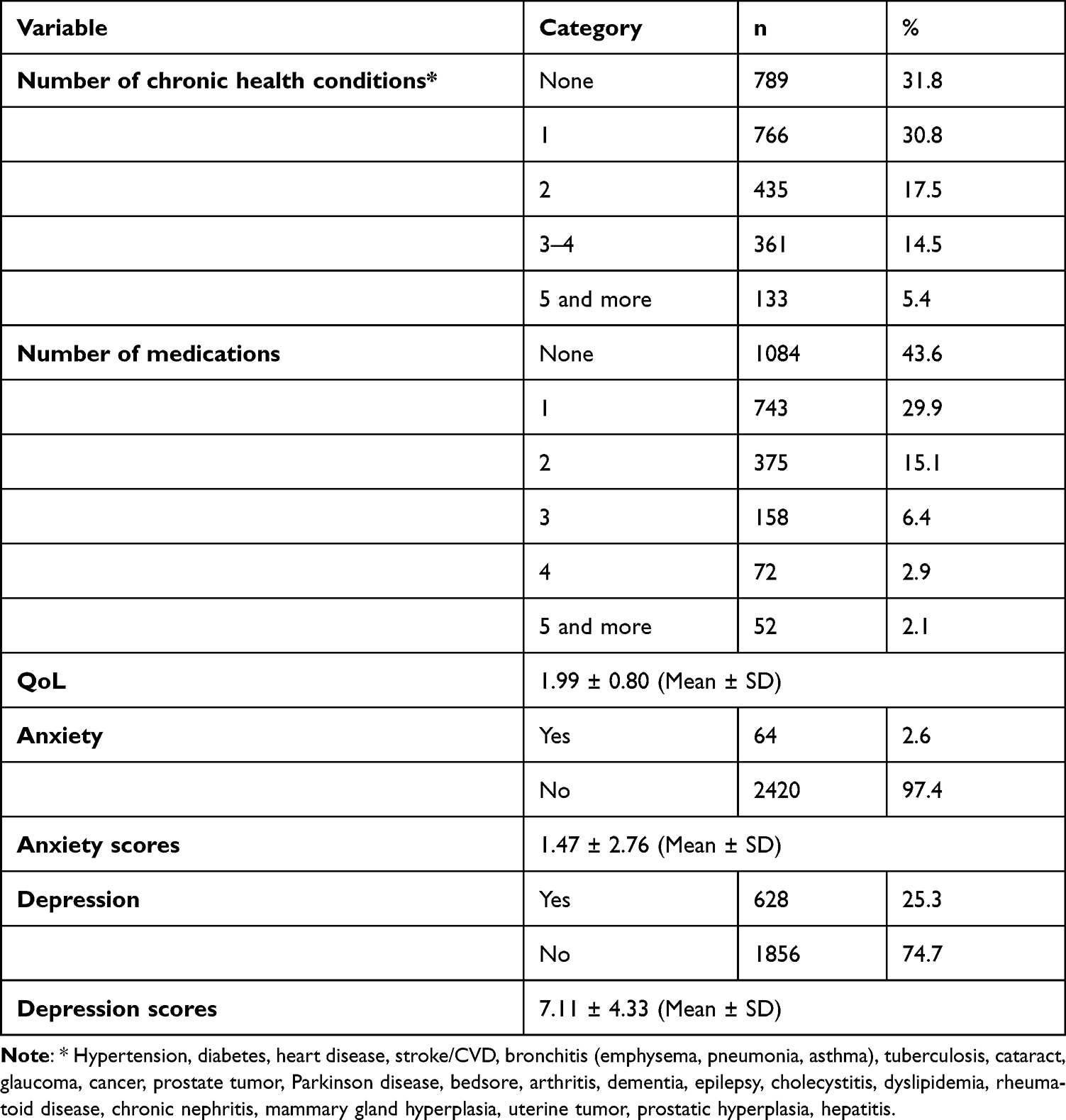 |
Table 2 Description of Clinical Variables, Polypharmacy, QoL, Anxiety, and Depression (N = 2484) |
The mean scores for anxiety and depression were 1.47 ± 2.76 and 7.11 ± 4.33, respectively. Based on the cut-off scores for GAD-722 and CES-D-10,24 there were 64 participants (2.6%) who reported having symptoms of anxiety and 628 (25.3%) for symptoms of depression. See Table 2.
Description of the Regression Models
In the base model (model 1) for anxiety, no association was observed between the number of medications and symptoms of anxiety. After controlling social-demographic and lifestyle-related variables, it showed that participants in rural areas might have more symptoms of anxiety compared with their urban peers (OR, 0.47, p < 0.05). In the final model, there was a significant association between QoL and symptoms of anxiety (OR, 2.01, p < 0.01) whereas no association between the number of medications and symptoms of anxiety was detected. See Table 3.
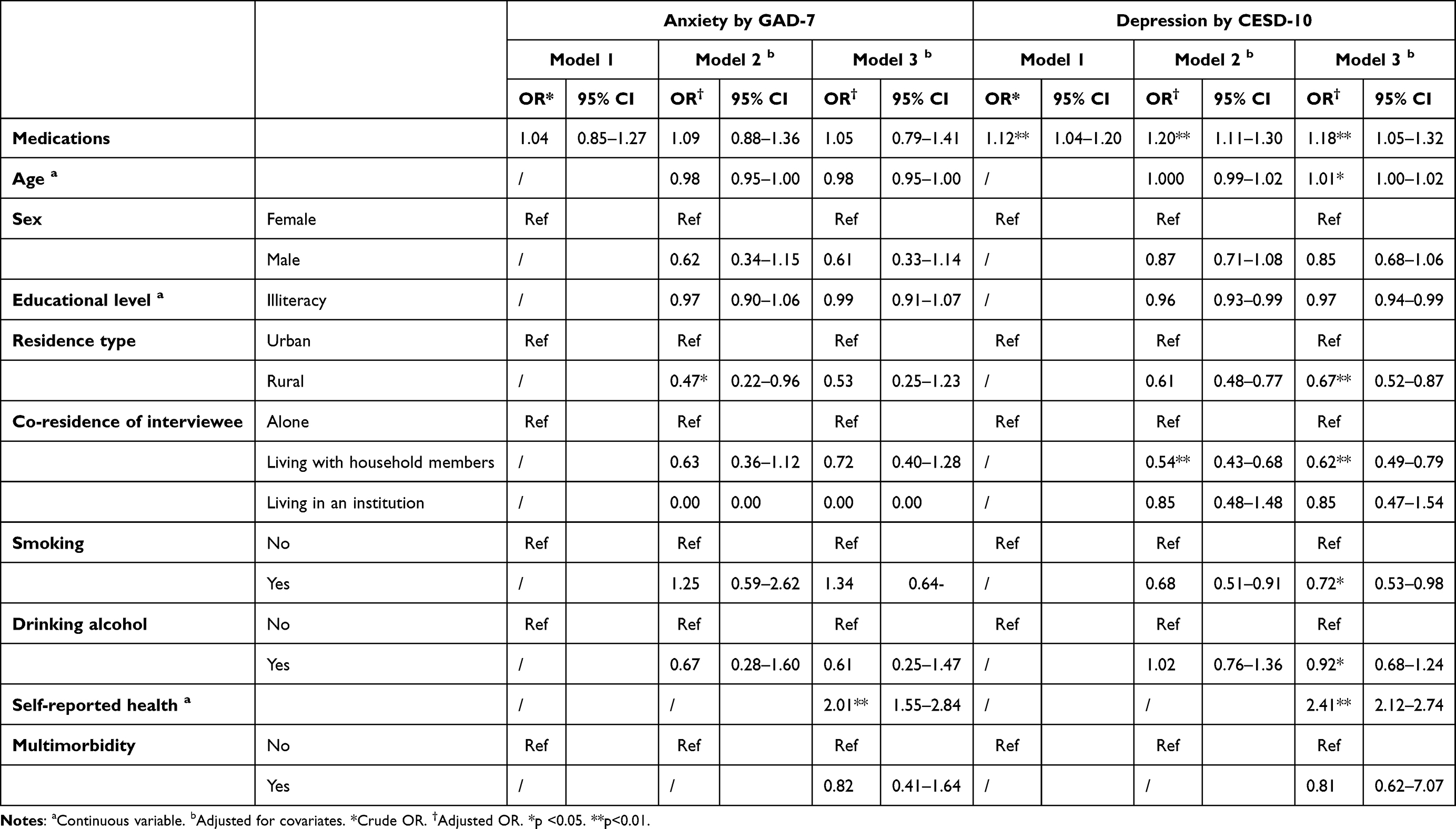 |
Table 3 Logistic Regression Analysis of the Associated Factors of Anxiety and Depression (N = 2484) |
In the base model (model 1) for depression, significant associations were found between the number of medications and symptoms of depression (OR, 1.12, p < 0.01). After controlling for social-demographic and lifestyle-related variables, this association remained (OR, 1.20, p < 0.01). Participants with household members reported fewer symptoms of depression compared with ones who lived alone (OR, 0.54, p < 0.01). In the final model, the number of medications (OR, 1.18, p < 0.01), age (OR, 1.01, p < 0.05), residence type (OR, 0.67, p < 0.01), co-residence of the participants (OR, 0.62, p < 0.01), lifestyle-related variables including smoking (OR, 0.72, p < 0.05) and alcohol consumption (OR, 0.92, p < 0.05), and QoL (OR, 2.41, p < 0.01) were significant variables. See Table 3.
Sensitivity Analysis
Logistic regression analysis was performed among the multimorbidity group that involved participants who reported having two or more chronic diseases. In both analyses, the associations between polypharmacy and anxiety and depression were consistent with the primary analyses.
The controlled model for anxiety showed that rural participants (OR, 0.19, p < 0.05) and participants with poor QoL were vulnerable to anxiety (OR, 3.18, p < 0.01). The controlled model for depression indicated participants with polypharmacy reported more symptoms of depression (OR, 0.49, p < 0.05). In addition, education level (OR, 0.94, p < 0.01), co-residence of the participants (OR, 0.50, p < 0.01), and QoL (OR, 2.44, p < 0.01) were significant variables. See Table 4.
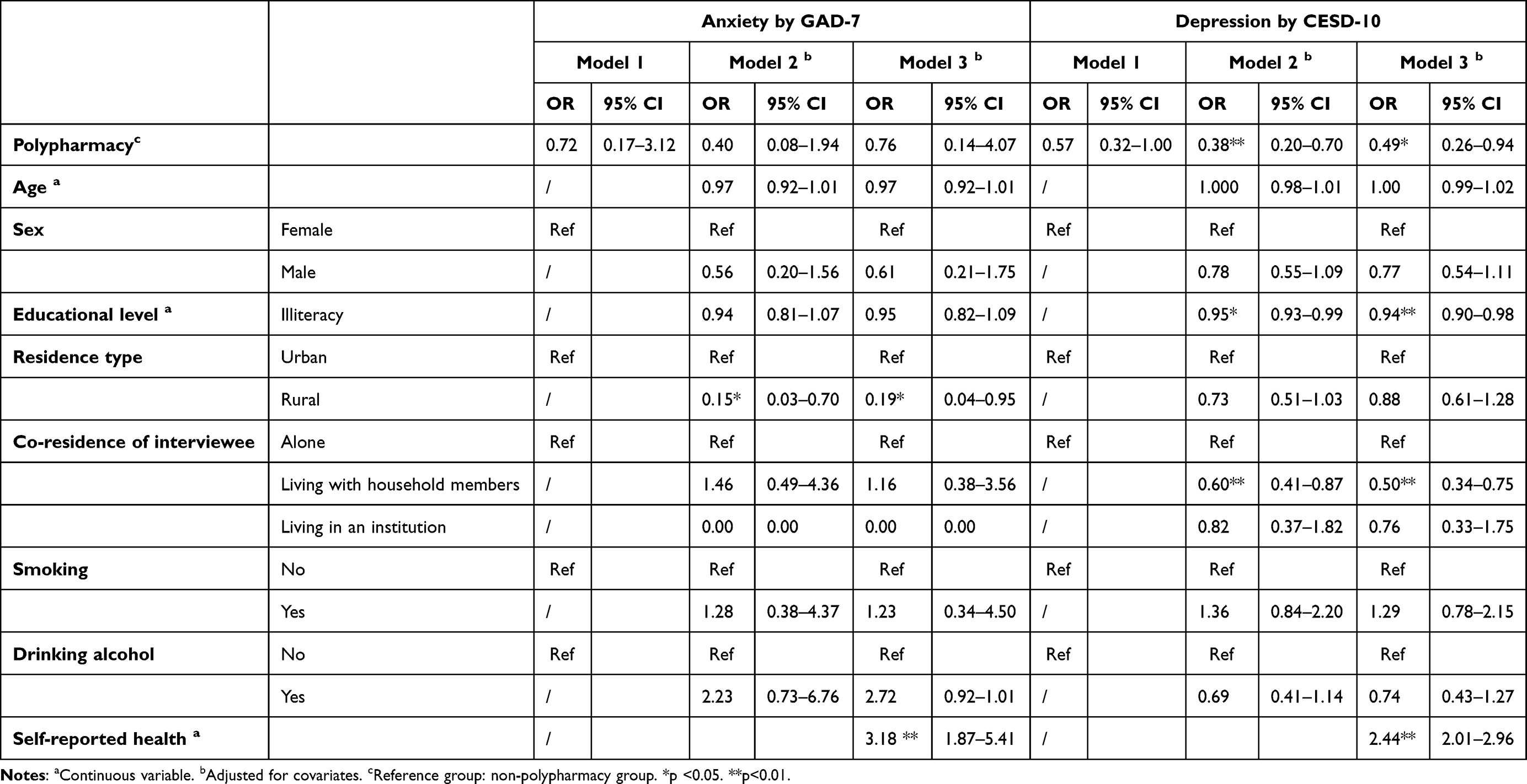 |
Table 4 Sensitivity Analysis of the Associated Factors of Anxiety and Depression Among Multimorbidity Group (n = 929) |
Discussion
The current study has examined the associations between polypharmacy and anxiety and depression in a representative sample of Chinese older adults. The prevalence of polypharmacy was lower than in past studies: A large survey in 17 European countries showed a prevalence of polypharmacy ranging from 26 to 40%.28 Zhang, Jiao, Guo, Bo, Xu and Wu11 conducted a nationwide prospective cohort study that included 9062 Chinese hospitalized patients (aged more than 65 years) and found that the prevalence of polypharmacy was 24%. Another cross-sectional study in China analyzed the prescription data from 720 hospitalized patients (aged more than 50 years) and found that the prevalence of polypharmacy accounted for 50%.29 As the CLHLS surveyed the general older population only, the difference in researched samples and settings might explain this different rate. Also, the large heterogeneity in the definition of polypharmacy makes it challenging to compare the prevalence of polypharmacy across different studies.
In agreement with former research,16 multiple drug use was associated with depression in Chinese older adults, above and beyond confounders. There were several explanations for the mechanism of depression and multiple drug use. First, frailty is a common geriatric syndrome that may cause physiological loss and increased vulnerability to internal and external stressors.30 An increased number of medications might lead to the development of frailty.6 Frailty and depression could reciprocally affect each other over time31 and might share similar reasons.32 That could be the case as the age of the sample in this study ranged between 60 and 117 years old and those participants were vulnerable to frailty. Second, depression and chronic diseases were commonly co-occurred.33 Research showed that people with multimorbidity were two to three times to have depression in contrast to people without multimorbidity or people without chronic conditions.34 The presence of more than one chronic condition needing management and treatment, which usually leads to multiple medications. Conversely, depression is a key factor in poor health, and having depression might delay an improvement in a physical chronic condition.35
A national survey in the US has shown that polypharmacy could contribute to psychological distress among African Americans.36 However, this study did not document the association between medications and anxiety. One possible explanation was the difference in samples and research settings. In addition, using different scales for anxiety might lead to controversial results.
This study involved a nationally representative sample of Chinese older adults and used standardized measurements for anxiety and depression. However, this study was not able to identify causality due to the design nature. This study used self-reported scales to measure the status of polypharmacy and the calculation of multiple medications might result in a bias. As the CLHLS only included medications for a list of physical chronic conditions. The status of psychotropic medicines was lacking, although antipsychotic polypharmacy (APP) is frequently prescribed among people with psychiatric disorders. For example, multiple medications use is suggested if monotherapy not working among people with bipolar disorder.37 Additionally, Traditional Chinese Medicine (TCM) is a significant complementary and alternative treatment in China and a large survey in China showed that around 14% of older adults have used TCM practitioners.38 As a result, information regarding Chinese herbal formulas for treating diseases should be considered. Over-the-counter drugs were excluded in this study, which might also underestimate the status of polypharmacy. Given that the polypharmacy definitions were various, a more comprehensive and holistic evaluation of polypharmacy should be developed and employed in further research.
The results of this study can be translated into clinical practice and research in several ways. First, using multiple medications might be served as an indicator for psychological distress such as depression in older adults. Although the interactions between polypharmacy and anxiety have not yet been clarified, efforts should be made concerning the detection of these potential mental health problems. Second, a healthcare protocol for people with polypharmacy should incorporate elements for the mental aspect, especially in a geriatric setting. Finally, examining polypharmacy in older adults should consider more about geriatric syndrome such as frailty, thus comprehensive geriatric assessments are necessary. Moreover, qualitative findings presented that having polypharmacy might affect one’s self-perception regarding medications4 and develop burdens such as medication fatigue and side effects.39 This might suggest a clue to explore the impact of polypharmacy on people’s mental health by involving those accompanied variables.
Conclusion
The current study has found a possible link between polypharmacy and depression in a national sample of Chinese older adults, suggesting that those with polypharmacy might be at greater risk of developing depression. Having polypharmacy may serve as a screener to identify symptoms of depression among this population. Verification of this finding is required across different settings and further research with comprehensive measures about polypharmacy could help to better explore such an association.
Acknowledgment
The authors acknowledge Peking University Center for Healthy Ageing and Development Studies (PKU CHADS) for sharing the data of the Chinese Longitudinal Healthy Longevity Survey (CLHLS).
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hajjar ER, Cafiero AC, Hanlon JT. Polypharmacy in elderly patients. Am J Geriatr Pharmacother. 2007;5(4):345–351. doi:10.1016/j.amjopharm.2007.12.002
2. Pazan F, Wehling M. Polypharmacy in older adults: a narrative review of definitions, epidemiology and consequences. Eur Geriatr Med. 2021;12(3):443–452. doi:10.1007/s41999-021-00479-3
3. Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13(1):57–65. doi:10.1517/14740338.2013.827660
4. Eriksen CU, Kyriakidis S, Christensen LD, et al. Medication-related experiences of patients with polypharmacy: a systematic review of qualitative studies. BMJ open. 2020;10(9):e036158–e036158. doi:10.1136/bmjopen-2019-036158
5. Palagyi A, Keay L, Harper J, Potter J, Lindley RI. Barricades and brickwalls–a qualitative study exploring perceptions of medication use and deprescribing in long-term care. BMC Geriatr. 2016;16(1):15. doi:10.1186/s12877-016-0181-x
6. Gutiérrez-Valencia M, Izquierdo M, Cesari M, Casas-Herrero Á, Inzitari M, Martínez-Velilla N. The relationship between frailty and polypharmacy in older people: a systematic review. Br J Clin Pharmacol. 2018;84(7):1432–1444. doi:10.1111/bcp.13590
7. Magnuson A, Sattar S, Nightingale G, Saracino R, et al. A practical guide to geriatric syndromes in older adults with cancer: a focus on falls, cognition, polypharmacy, and depression. Am Soc Clin Oncol Educ Book. 2019;39:e96–e109. doi:10.1200/edbk_237641.
8. Kornholt J, Christensen MB. Prevalence of polypharmacy in Denmark. Dan Med J. 2020;67(6):Jun.
9. Kantor ED, Rehm CD, Haas JS, Chan AT, Giovannucci EL. Trends in prescription drug use among adults in the United States from 1999–2012. JAMA. 2015;314(17):1818–1831. doi:10.1001/jama.2015.13766
10. Page AT, Falster MO, Litchfield M, Pearson SA, Etherton-Beer C. Polypharmacy among older Australians, 2006–2017: a population-based study. Med J Aust. 2019;211(2):71–75. doi:10.5694/mja2.50244
11. Zhang XM, Jiao J, Guo N, Bo HX, Xu T, Wu XJ. Association of polypharmacy with falls among older Chinese inpatients: a nationwide cohort study. Geriatr Gerontol Int. 2021;21(9):810–817. doi:10.1111/ggi.14245
12. Wang R, Chen L, Fan L, et al. Incidence and effects of polypharmacy on clinical outcome among patients aged 80+: a five-year follow-up study. PLoS One. 2015;10(11):e0142123. doi:10.1371/journal.pone.0142123
13. Li J, Chattopadhyay K, Xu M, et al. Prevalence and predictors of polypharmacy prescription among type 2 diabetes patients at a tertiary care department in Ningbo, China: a retrospective database study. PLoS One. 2019;14(7):e0220047–e0220047. doi:10.1371/journal.pone.0220047
14. Rieckert A, Trampisch US, Klaaßen-Mielke R, et al. Polypharmacy in older patients with chronic diseases: a cross-sectional analysis of factors associated with excessive polypharmacy. BMC Fam Pract. 2018;19(1):113. doi:10.1186/s12875-018-0795-5
15. Palapinyo S, Methaneethorn J, Leelakanok N. Association between polypharmacy and depression: a systematic review and meta-analysis. J Pharm Pract Res. 2021;51(4):280–299. doi:10.1002/jppr.1749
16. Bazargan M, Smith J, Saqib M, Helmi H, Assari S. Associations between polypharmacy, self-rated health, and depression in African American older adults; mediators and moderators. Int J Environ Res Public Health. 2019;16(9):1574. doi:10.3390/ijerph16091574
17. Choi NG, Marti CN, Kunik ME. Predictors of CNS-active medication use and polypharmacy among homebound older adults with depression. Psychiatr Serv. 2020;71(8):847–850. doi:10.1176/appi.ps.201900551
18. Zhao Y, Zhao S, Zhang L, Haregu TN, Wang H. Impacts of multimorbidity on medication treatment, primary healthcare and hospitalization among middle-aged and older adults in China: evidence from a nationwide longitudinal study. BMC public Health. 2021;21(1):1380. doi:10.1186/s12889-021-11456-7
19. Center for Healthy A, Development S. Data from: the Chinese Longitudinal Healthy Longevity Survey (CLHLS)-longitudinal data (1998–2018). 2020; DRAFT VERSION. Deposited 2020-04-0316:22:09.385. doi:10.18170/DVN/WBO7LK.
20. Zheng Z. Twenty years’ follow-up on elder people’s health and quality of life. China Popul Dev Stud. 2020;3(4):297–309. doi:10.1007/s42379-020-00045-7
21. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
22. Ren Z, Zhou Y, Liu Y. The psychological burden experienced by Chinese citizens during the COVID-19 outbreak: prevalence and determinants. BMC Public Health. 2020;20(1):1617. doi:10.1186/s12889-020-09723-0
23. Niu L, Qiu Y, Luo D, et al. Cross-culture validation of the HIV/AIDS stress scale: the development of a revised Chinese Version. PLoS One. 2016;11(4):e0152990. doi:10.1371/journal.pone.0152990
24. Liu Y, Chen X, Yan Z. Depression in the house: the effects of household air pollution from solid fuel use among the middle-aged and older population in China. Sci Total Environ. 2020;703:134706. doi:10.1016/j.scitotenv.2019.134706
25. Cheng ST, Chan AC. The center for epidemiologic studies depression scale in older Chinese: thresholds for long and short forms. Int J Geriatr Psychiatry. 2005;20(5):465–470. doi:10.1002/gps.1314
26. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(1):230. doi:10.1186/s12877-017-0621-2
27. Almirall J, Fortin M. The coexistence of terms to describe the presence of multiple concurrent diseases. J Comorb. 2013;3(1):4–9. doi:10.15256/joc.2013.3.22
28. Midão L, Giardini A, Menditto E, Kardas P, Costa E. Polypharmacy prevalence among older adults based on the survey of health, ageing and retirement in Europe. Arch Gerontol Geriatr. 2018;78:213–220. doi:10.1016/j.archger.2018.06.018
29. Chen C, Feng Z, Fu Q, et al. Predictors of polypharmacy among elderly patients in china: the role of decision involvement, depression, and taking Chinese medicine behavior. Front Pharmacol. 2021;12:745688. doi:10.3389/fphar.2021.745688
30. Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–1375. doi:10.1016/s0140-6736(19)31786-6
31. Vaughan L, Corbin AL, Goveas JS. Depression and frailty in later life: a systematic review. Clin Interv Aging. 2015;10:1947–1958. doi:10.2147/cia.S69632
32. Mayerl H, Stolz E, Freidl W. Frailty and depression: reciprocal influences or common causes? Soc Sci Med. 2020;263:113273. doi:10.1016/j.socscimed.2020.113273
33. Lotfaliany M, Bowe SJ, Kowal P, Orellana L, Berk M, Mohebbi M. Depression and chronic diseases: co-occurrence and communality of risk factors. J Affect Disord. 2018;241:461–468. doi:10.1016/j.jad.2018.08.011
34. Read JR, Sharpe L, Modini M, Dear BF. Multimorbidity and depression: a systematic review and meta-analysis. J Affect Disord. 2017;221:36–46. doi:10.1016/j.jad.2017.06.009
35. Trivedi MH. The link between depression and physical symptoms. Prim Care Companion J Clin Psychiatry. 2004;6(Suppl 1):12–16.
36. Assari S, Bazargan M. Polypharmacy and psychological distress may be associated in African American adults. Pharmacy. 2019;7(1). doi:10.3390/pharmacy7010014
37. Fountoulakis KN, Grunze H, Vieta E, et al. The International College of Neuro-Psychopharmacology (CINP) treatment guidelines for Bipolar Disorder in adults (CINP-BD-2017), Part 3: the clinical guidelines. Int J Neuropsychopharmacol. 2017;20(2):180–195. doi:10.1093/ijnp/pyw109
38. Aw JYH, Yiengprugsawan VS, Gong CH. Utilization of traditional Chinese medicine practitioners in later life in Mainland China. Geriatrics. 2019;4(3):49. doi:10.3390/geriatrics4030049
39. Yang Z, Zhu Z, Lizarondo L, et al. Experience of chronic noncommunicable disease in people living with HIV: a systematic review and meta-aggregation of qualitative studies. BMC Public Health. 2021;21(1):1651. doi:10.1186/s12889-021-11698-5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.