Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Association Between Platelet Indices and Risk of Chronic Obstructive Pulmonary Disease: A Bidirectional Mendelian Randomization Study
Authors Liao W, Lin X, Liu K ![]() , Yang Y
, Yang Y ![]() , Du L, Pan J, Chen F, Ye W
, Du L, Pan J, Chen F, Ye W ![]() , Chen B, Chen R
, Chen B, Chen R ![]() , Chen W, Yao W
, Chen W, Yao W ![]()
Received 1 April 2025
Accepted for publication 9 August 2025
Published 27 August 2025 Volume 2025:20 Pages 2967—2977
DOI https://doi.org/10.2147/COPD.S531797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Weifeng Liao,1,* Xiaoxi Lin,1,* Keyu Liu,2,* Yitian Yang,1,* Lianfang Du,1 Jingjing Pan,1 Feiju Chen,1 Weilong Ye,1 Bainian Chen,1 Riken Chen,1 Wenliang Chen,3,4 Weimin Yao1
1Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524003, People’s Republic of China; 2Department of Anesthesia, The Second Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524003, People’s Republic of China; 3Translational Medicine Center, The Second Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524003, People’s Republic of China; 4The Medical Interdisciplinary Science Research Center of Western Guangdong, The Second Affiliated Hospital of Guangdong Medical University, Zhanjiang, Guangdong, 524003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenliang Chen; Weimin Yao, Email [email protected]; [email protected]
Introduction: Platelet indices are associated with chronic obstructive pulmonary disease (COPD), their causal relationship remains unclear. This study aims to explore the causal relationship between four common platelet indices and COPD using Mendelian randomization (MR), including platelet count (PLT), plateletcrit (PCT), mean platelet volume (MPV), and platelet distribution width (PDW).
Methods: We analyzed summary statistics from European-ancestry genome-wide association studies (GWAS) for platelet indices (UK Biobank, n=408,112) and COPD (FinnGen, n=433,208). MR analyses were performed using Inverse Variance Weighting (IVW), MR Egger (ME), Simple Mode (SM), Weighted Median (WMe), and Weighted Mode (WMo). Heterogeneity between SNPs was assessed using Cochran’s Q test in combination with a random-effects IVW approach. MR-Egger intercept test and MR-PRESSO analysis demonstrate horizontal pleiotropy. Leave-one-out analysis to assess outlier-driven bias.
Results: IVW analysis indicated that higher PLT was suggestively associated with increased COPD risk (OR = 1.054, 95% CI = 1.005– 1.056, p = 0.029, FDR = 0.116). In the reverse direction, COPD was suggestively associated with increased PCT (OR = 1.025, 95% CI = 1.003– 1.048, p = 0.024, FDR= 0.096). No significant associations were observed for MPV or PDW. Sensitivity analyses confirmed the robustness of results, with no signs of pleiotropy or reverse causality.
Conclusion: Our bidirectional MR analysis found no definitive causal relationship between platelet indices and COPD, but observed suggestive associations between higher PLT/PCT and an increased risk of COPD. These findings warrant further investigation into the roles of platelet indices in COPD pathogenesis and their potential as biomarkers or therapeutic targets.
Keywords: platelet count, plateletcrit, mean platelet volume, platelet distribution width, chronic obstructive pulmonary disease, mendelian randomization
Introduction
COPD is a progressive pulmonary disorder characterized by persistent airflow resistance and chronic inflammation,1 emerging as the third leading cause of death globally.2 The rising prevalence of COPD, due to aging populations, insufficient tobacco control, and environmental pollution, results in substantial socioeconomic burden.3
In recent years, there has been increasing interest in using accessible blood biomarkers to improve the diagnosis and prognosis of COPD. Among these biomarkers, platelet indices are promising tools for the evaluation and monitoring of disease progression. Platelet alterations are known to be associated with the incidence and development of COPD. Platelets also regulate various biological processes, including inflammation, endothelial dysfunction, and immunomodulation. It may contribute to COPD pathogenesis by regulating immune responses and thrombosis pathways.4,5 Platelets regulate immune responses by interacting with leukocytes in different pathological and physiological processes such as inflammation, tissue remodeling, and autoimmune diseases, thereby influencing the pathogenesis of respiratory diseases, such as COPD, asthma, etc.6 The release of platelet-derived cytokines (eg, platelet factor 4, transforming growth factor-β) or microvesicles that regulate vascular permeability contribute to the inflammatory regression process by promoting the synthesis of pro-regressive mediators while decreasing pro-inflammatory mediators, making platelets a key player in inflammatory diseases such as pneumonia and acute respiratory distress syndrome.7 Thrombospondin (TSP-1) interaction with integrin-mediated adhesion leads to COPD exacerbations.8
Current clinical data analysis has found that platelet counts and platelet-to-lymphocyte ratios may reflect the neutrophil inflammatory response during COPD exacerbations.9 PDW can be used as a diagnostic marker for COPD with pulmonary hypertension (95% CI: 1.052–1.454, r = 1.237, p < 0.05).10 PDW and MPV are risk factors for COPD with secondary erythrocytosis.11 Thrombocytopenia and high MPV predict mortality in patients with COPD.12,13 However, the causal nature of this relationship remains unclear. Bidirectional Mendelian Randomization (MR) offers a powerful framework for assessing causality by utilizing genetic variants as instrumental variables.14–16 MR results in more reliable causal estimates by minimizing confounding bias (e.g smoking, air pollution, or cardiovascular comorbidities) and reverse causation.17,18 To further validate causality, we tested the opposite direction (from COPD to platelet indices), as platelet alterations may be secondary to COPD-related inflammation or hypoxia, rather than causality. This analysis will strengthen the inference of one-way effects.
In this study, we performed bidirectional MR to investigate the genetic causal relationship between common platelet indices and COPD risk as well as their directional influence. These findings provide insights into the potential application of platelet indices for early diagnosis, prevention, and treatment of COPD.
Methods
Study Design
A bidirectional two-sample MR study was conducted to investigate the causal relationship between platelet indices and COPD using single-nucleotide polymorphisms (SNPs) as instrumental variables (IVs). MR analysis relies on three fundamental assumptions: 1) genetic instruments must be highly associated with exposure; 2) genetic instruments should not be linked to confounding factors; and 3) genetic instruments must affect the outcome only through exposure.15,19,20 These assumptions ensure the validity and reliability of the causal inferences derived from the MR analyses. The overall design of the MR used in this study is illustrated in Figure 1.
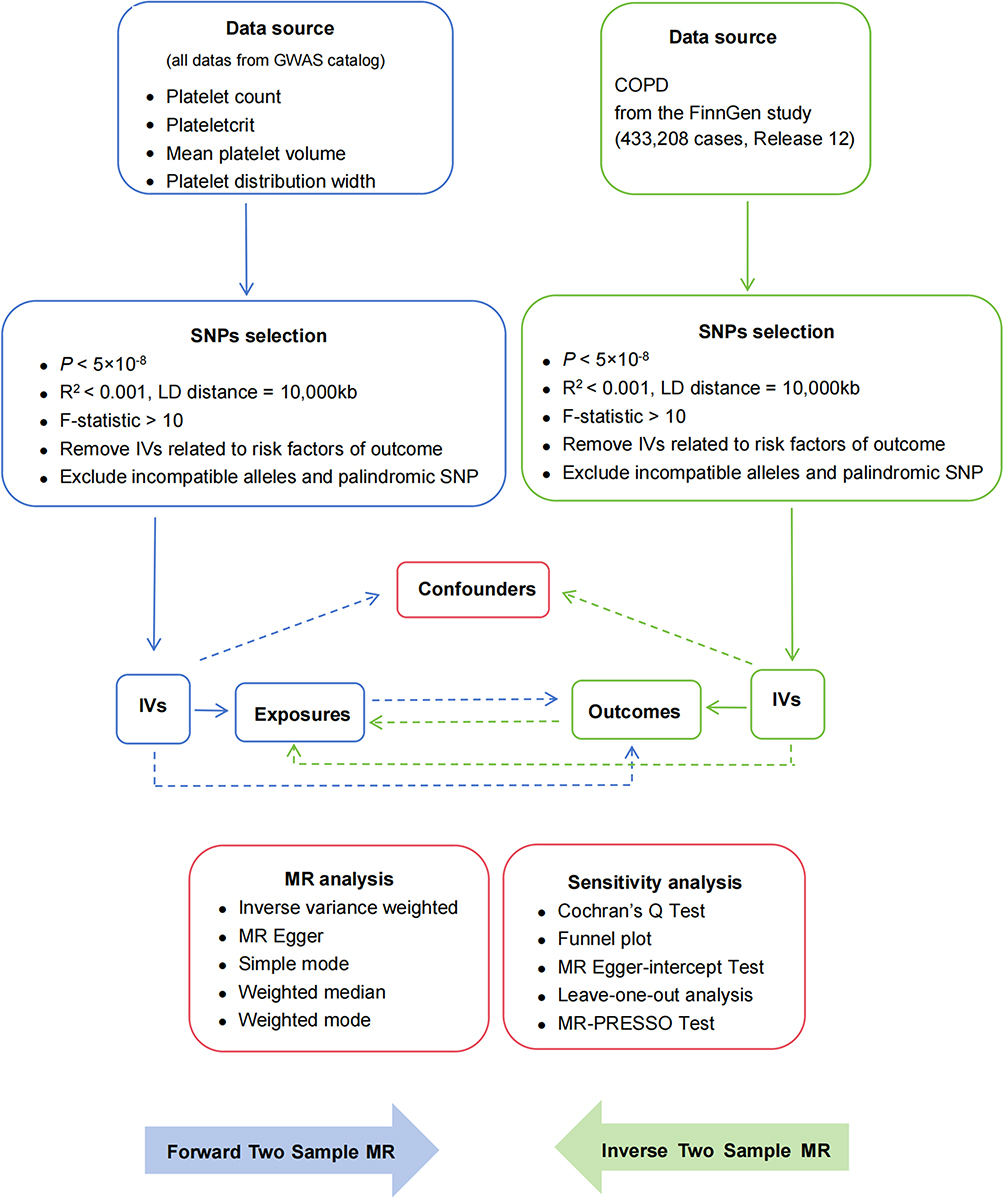 |
Figure 1 Overview of the study design. Abbreviation: SNPs, single-nucleotide polymorphisms. |
Date Sources
Summary statistics of platelet indices were obtained from the MRBase GWAS catalog within the EBI GWAS.21 Four indices (PLT, PCT, PDW, and MPV) associated with platelet phenotypes were used as the exposure factors (https://gwas.mrcieu.ac.uk/). COPD data were sourced from the latest version (Release 12) of the FinnGen study (https://www.finngen.fi/), which included correlated genetic data from 500,000 Finnish biobank samples.22 The platelet indices and COPD datasets were derived from European-ancestry GWAS studies in the UK Biobank and FinnGen to minimize potential population stratification bias. The UK Biobank and FinnGen are two independent samples.23 No additional ethical approval was required as publicly available summary-level data were used. Detailed GWAS information is listed in Table 1. The number of eligible SNPs that were significantly associated with each exposure variable (platelet indices or COPD) is presented in Supplementary Tables S1 and S2.
 |
Table 1 Characteristics of GWAS Used in This Study |
Genetic IVs Selection
SNPs associated with exposure factors were selected based on their genome-wide significance (p < 5×10−8). To account for linkage disequilibrium (LD), SNPs were selected using an R² threshold of < 0.001 and a clumping distance of 10,000 kb. To reduce weak instrument bias, the F-statistic was calculated using the formula (F = β²/se², with β and se as allelic effect value and standard error, respectively) for each instrumental variable (IV), and F > 10 indicates a strong association between the IV and exposure.24 Additionally, incompatible alleles and palindromic SNPs with intermediate allele frequencies were removed to avoid potential bias. Finally, SNPs associated with potential confounders were excluded using the PhenoScanner V2 (http://www.phenoscanner.medschl.cam.ac.uk/).25
Allele Harmonization Process
SNPs with ambiguous strand alignment (A/T or C/G) and intermediate allele frequency (MAF > 0.40) are excluded to avoid coordination errors. For the missing instrumental SNPs in the result dataset, we identified the proxy SNPs with a high LD (r² ≥ 0.80) using the 1000 Genomes European Reference Panel. The agent SNP with the strongest LD is replaced. Use the TwoSampleMR R software package to cross-check effect alleles and frequencies between datasets and manually verify all harmonized SNPs. Strand flipping: Use allele frequency agreement checks to flip non-palindromic SNPs with mismatched strands to the forward strand.
Statistical Analysis
“TwoSampleMR” R package was used for MR analysis, employing methods such as Inverse Variance Weighted (IVW), MR Egger (ME), Simple Mode (SM), Weighted Median (WMe), and Weighted Mode (WMo).26–28 The MR Steiger directionality test was conducted to determine the correctness of the causal effects. The fixed-effect IVW method was accepted as the primary approach for two-sample MR analysis. The MR correlation analysis employed the Benjamini-Hochberg method for multiple testing correction to generate false discovery rate (FDR)-adjusted p-values (Benjamini and Hochberg, 1995). The analysis also reported unadjusted raw p-values. Significant correlations were identified when both raw and FDR-adjusted p-values are less than 0.05. In cases where raw p < 0.05 but FDR-adjusted p >0.05, it is considered as a suggestive association between two factors.29
Heterogeneity among SNPs was assessed using Cochran’s Q test. When heterogeneity (Q_p > 0.05) was observed, the fixed-effects IVW method was applied. Otherwise, the random effects IVW method was used.30,31 The MR-Egger method and “leave-one-out” analyses were performed to evaluate the potential outlier bias.31 The Mendelian randomized pleiotropic residuals and outliers (MR-PRESSO) analysis was performed using the “MRPRESSO” package to assess horizontal pleiotropy and remove influential outliers. After excluding significant outliers, the Mendelian randomization estimate was recalculated.32 All statistical analyses were performed using R statistical software (version 4.3.2).
Results
The Causal Effects of Platelet Indices on COPD
Selection of IVs
To mitigate the potential influence of confounding factors, the IVs for all platelet indices significantly associated with COPD were strictly selected based on a threshold of p < 5×10−8. For univariate MR analysis determining the relationship between PLT and COPD, 976 SNPs were identified. Following integration with the COPD dataset and subsequent exclusion of incompatible alleles and palindromic SNPs (467 SNPs removed) and 21 confounding factors, 488 SNPs were obtained (F-statistics: 37.50–99.13, median: 64.22). Using the same strategies, the 914 SNPs initially identified in PCT were refined to 457 SNPs (F-statistics: 42.67–99.85, median:66.66). Similarly, MPV and PDW analyses yielded 453 SNPs (F-statistics: 38.88–99.71, median: 80.62) and 391 SNPs (F-statistics: 39.76–99.45, median: 66.30), respectively.
In this study, instrumental variables were selected for all platelet indices with F-statistics > 10 as the threshold, minimizing the risk of weak instrument bias and thereby strengthening the validity of the analytical findings. Furthermore, all SNPs potentially associated with outcome risk factors were excluded from the analysis.
Two-Sample MR Analysis results
Two-sample MR analysis revealed a significant association between PLT count and COPD risk (IVW: odds ratio [OR] = 1.054, 95% CI = 1.005–1.056, p = 0.029). After FDR correction of the obtained p-value of 0.029, the p-value was 0.116, which was not statistically significant, suggesting that PLT is a potential risk of COPD. Notably, analysis using all MR methods showed consistent directionality in their β values, suggesting that elevated PLT levels increased the risk of COPD. In contrast, no significant association was observed between COPD and other platelet indices including PCT (IVW: OR = 1.036, 95% CI = 0.988–1.087, p = 0.141), PDW (IVW: OR = 0.963, 95% CI = 0.919–1.010, p = 0.117), and MPV (IVW: OR = 0.994, 95% CI = 0.952–1.039, p = 0.800). The results are shown in Figure 2.
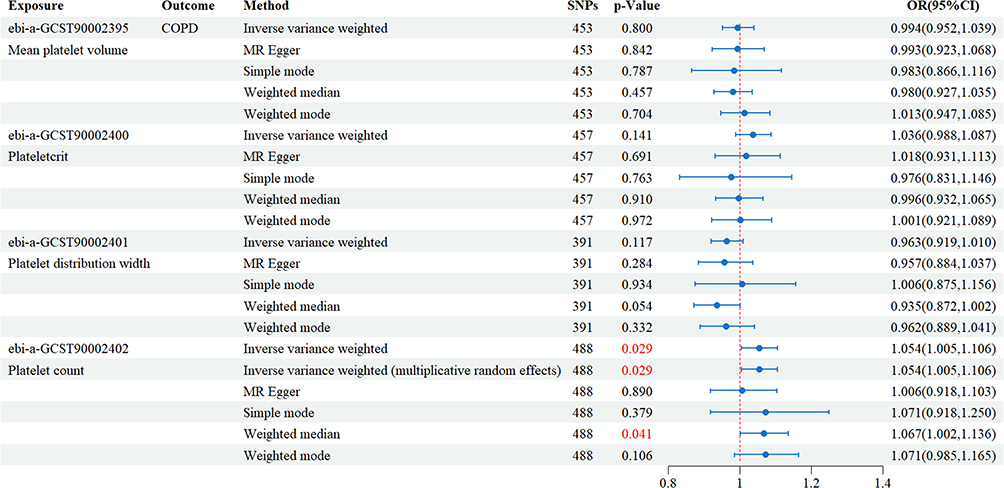 |
Figure 2 MR results of relationship between platelet indices and onset of COPD. Abbreviations: SNPs, single-nucleotide polymorphisms; OR, odds ratio; CI, confidence interval. |
Results of Sensitivity Analysis
For sensitivity analysis, both Cochran’s Q test revealed significant heterogeneity among platelet indices (p < 0.05). To address this heterogeneity and enhance the accuracy of data analysis, the multiplicative random-effects IVW model was employed (p < 0.05), which effectively eliminated the observed heterogeneity (Supplementary Table S3). In addition, the MR-PRESSO global pleiotropy test and the MR-Egger intercept test showed no evidence of significant horizontal pleiotropy (p > 0.05; Table 2).
 |
Table 2 MR-Egger Regression Analysis and MR-PRESSO Analysis of IVs for Platelet Indices (Exposures) and COPD (Outcome) |
The relationships between platelet indices and COPD were further visualized using scatter plots (Figure 3A), funnels (Figure 3B), and forest plots (Supplementary Figure S1). Scatter plots were particularly useful for assessing the strength of the association between selected IVs and outcomes. A clear linear trend in the scatter plot distribution indicated a strong linear relationship between the PLT and COPD risk.
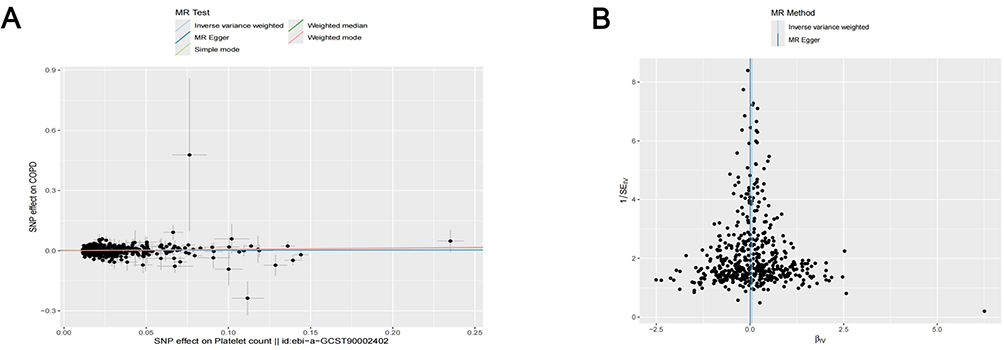 |
Figure 3 Causal effects of PLT on COPD. (A) Scatter plot of PLT on COPD. (B) Funnel plot for precision of the estimate. |
The robustness of the IVW results was confirmed by leave-one-out analysis, in which the sequential exclusion of individual SNPs yielded results consistent with the overall causal effect estimates derived from the IVW method (p < 0.05). Furthermore, the symmetry observed in the funnel plots of PLT and COPD suggested that pleiotropy did not significantly influence the analysis. Finally, leave-one-out analysis demonstrated that the causal relationship between platelet indices and COPD was not driven by a single SNP (Supplementary Figure S2).
The Causal Effects of COPD on Platelet Indices
Selection of IVs
Based on the three core assumptions of the MR two-sample analysis, 23 (F-statistics ranging from 30.62 to 369.53) of 92 SNPs (65 SNPs were removed from linkage imbalance and palindromic alleles, and 4 confounding factors) were selected for subsequent analysis, where COPD was treated as exposure and platelet indices as outcomes.
Two-Sample MR Analysis Results
The causal effect of COPD on platelet indices was evaluated using five MR methods, as shown in Figure 4. The IVW method revealed no significant associations between COPD and PLT, MPV, or PDW (p > 0.05). However, a minor causal relationship was identified between PCT and COPD (IVW, OR = 1.025; 95% CI, 1.003–1.048; p = 0.024). Subsequently, the p-value of 0.024 was corrected by FDR for the given p-value using the Benjamini-Hochberg (BH) method, and the p-value was 0.096, suggesting that PCT is a potential downstream influencing factor for COPD. Moreover, all MR methods demonstrated consistent directional effects (Figure 4).
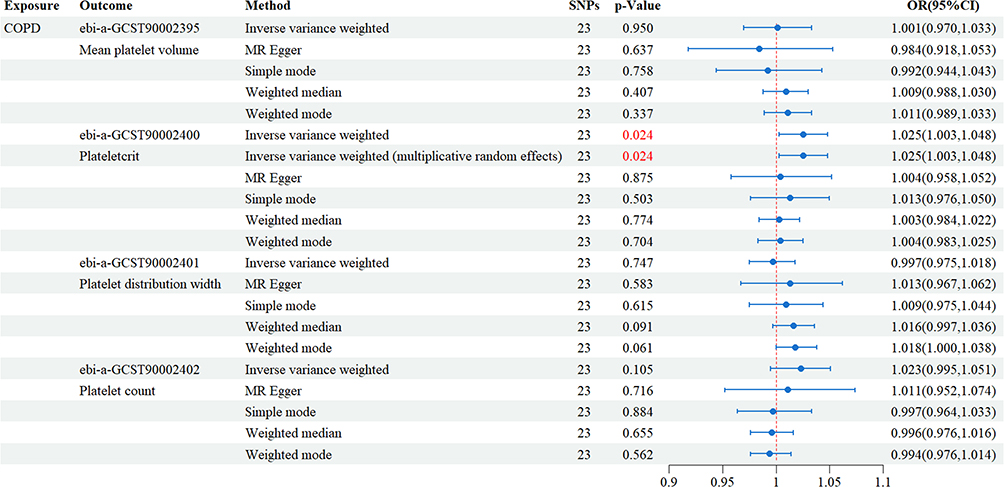 |
Figure 4 Results of inverse Two-sample Mendelian Randomization analysis. Abbreviations: SNPs, single-nucleotide polymorphisms; OR, odds ratio; CI, confidence interval. |
Sensitivity Analysis Results
Sensitivity analysis revealed heterogeneity in the relationship between COPD and PCT, as evidenced by Cochran’s Q test (p < 0.05). The random-effects IVW model effectively eliminated observed heterogeneity (p < 0.05, Supplementary Table S4). In addition, the MR-PRESSO global pleiotropy test and the MR-Egger intercept test showed no significant evidence of horizontal pleiotropy in the COPD-PCT relationship (p > 0.05, Table 3).
 |
Table 3 MR-Egger Regression Analysis and MR-PRESSO Analysis of IVs for COPD (Exposure) and Platelet Indices (Outcomes) |
The relationships between COPD and platelet indices were further visualized using forest plots (Figure 5A), scatter plots (Figure 5B), and funnel plots (Figure 5C). The scatter plots showed a strong linear association between IVs and outcomes, as indicated by the clear linear trend in the data point distribution, suggesting a significant linear relationship between COPD exposure and PCT.
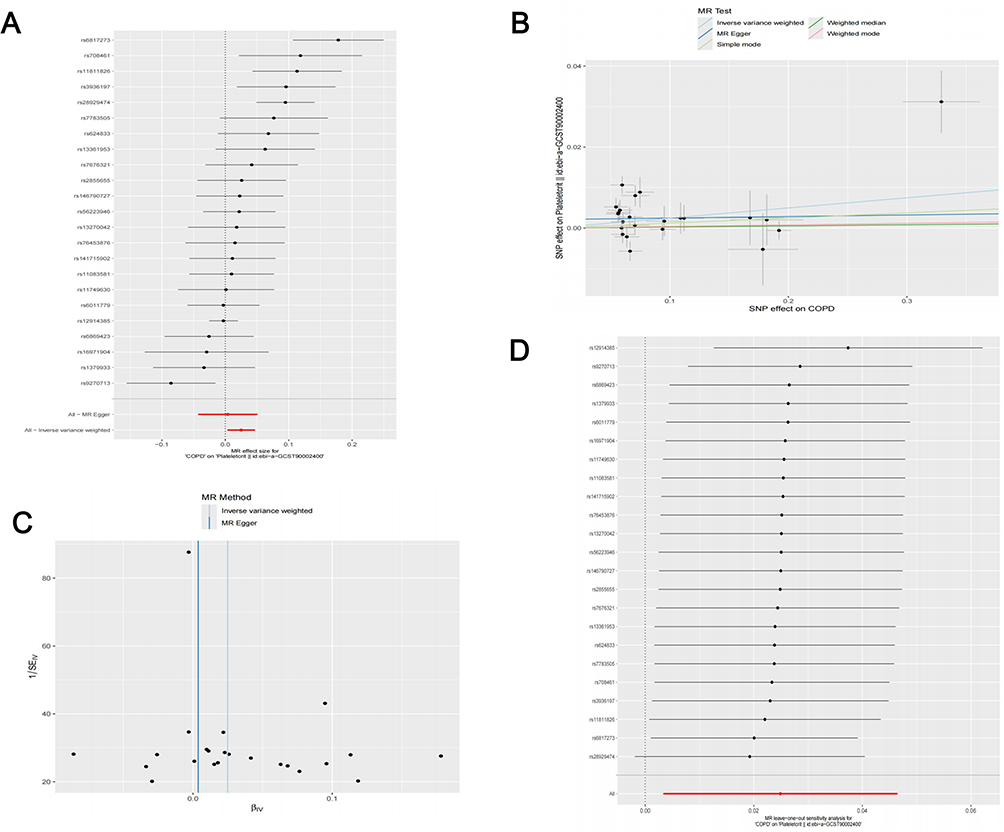 |
Figure 5 Causal relationship between COPD (exposure) and PCT (outcome). (A) The forest plot summarizing overall effects of COPD on PCT. (B) Scatter plot visualizing the effects of COPD on PCT. The 95% CIs for COPD and PCT effects are shown as vertical and horizontal lines, respectively. The fit line’s slope indicates the MR effect per method. (C) Funnel plot for the precision of the estimate. (D) Leave-one-out sensitivity analysis results. |
The symmetrical distribution of the funnel plots for COPD and PCT further supported the absence of significant pleiotropic effects in our analysis. Additionally, leave-one-out analysis demonstrated that the identified causal relationship between platelet indices and COPD was not driven by a single SNP (Figure 5D).
Discussion
In this study, we employed a bidirectional Mendelian Randomization (MR) analysis to investigate the causal relationships between common platelet indices and COPD in European populations. We observed suggestive, but not definitive, evidence that higher PLT may increase COPD risk, and that COPD may increase PCT. No significant associations were found for MPV or PDW.
Exploring platelet index changes in COPD is beneficial for understanding underlying pathophysiological mechanisms. Platelet activation in COPD is primarily caused by chronic inflammation and endothelial dysfunction leading to hypercoagulation. Activated platelets change shape and release pro-inflammatory cytokines and mediators, mediating endothelial adhesion of circulating white blood cells and leading to endothelial cell dysfunction and disease progression in patients.33 Our findings align with and expand upon previous research, providing further insights into the complex relationship between platelet indices and COPD. For instance, Ahamed et al found that PLT levels were positively correlated with COPD severity,34 suggesting that elevated PLT levels may play a role in COPD disease progression. Thus, PDW may serve as a prognostic marker for patients with COPD and pulmonary arterial hypertension.10 Other studies have identified lower MPV in patients with COPD, with MPV levels increasing during the recovery phase.35 Furthermore, Hakim et al observed significantly higher MPV, PDW, and PCT levels in patients with COPD, both with and without diabetes, than in the control group. Notably, COPD patients with diabetes exhibit even higher MPV levels than those without diabetes.36 Several studies have shown that the increased expression of α IIb β 3 integrin leads to significant platelet activation, resulting in increased platelet counts and enhanced platelet aggregation in patients.33,37 Collectively, these findings demonstrate a close relationship between platelet indices and COPD; however, they do not offer evidence for the causal influence of platelet indices on COPD pathogenesis and progression. Our study further revealed that among the platelet indices, increased PLT leads to a higher risk of COPD, while an increase in PCT is the subsequent event resulting from COPD.
This study has several advantages. First, Our MR Study validated the correlation between the platelet indices and COPD. Compared to previous observational studies, MR Analysis is an effective tool for mitigating potential biases such as confounders and reverse causation, thereby improving the reliability of causal reasoning. Second, the datasets used in this study mainly involved populations of European descent, which helps to minimize the effect of population stratification. Third, we used different estimation models and conducted rigorous sensitivity analysis to ensure the reliability and robustness of the obtained results. However, this study has several limitations. First, it was conducted in a single population and further validation was performed across ethnic groups. Second, although rigorous steps were implemented to identify abnormal variants and mitigate horizontal pleiotropy, their effects could not be completely eliminated. This could be attributed to the complex and unclear biological functions of several genetic variants. Finally, we used data from participants of all European ancestry (minimized stratification) but did not specify whether and how each GWAS was adjusted for principal component, genotyping lot, or correlation.
Conclusions
Our bidirectional MR analysis found no definitive causal relationship between platelet indices and COPD, but observed suggestive associations between higher PLT/PCT and increased COPD risk. These findings highlight the need for further research to clarify the roles of platelet indices in COPD pathogenesis and their potential as biomarkers or therapeutic targets. The roles of PLT/PCT in COPD can be further elucidated by longitudinal cohort validation, randomized antiplatelet therapy trials stratified by genetic risk, or functional assays of key SNPs. Moreover, integrating multi-omics data would be beneficial for uncovering the underlying molecular mechanisms accounting for the functions of PLT/PCT on COPD.
Abbreviations
MR, Mendelian randomization; COPD, chronic obstructive pulmonary disease; PLT, platelet count; PCT, plateletcrit; MPV, mean platelet volume; PDW, platelet distribution width; IVW, Inverse Variance Weighting; GWAS, genome-wide association studies; SNPs, single-nucleotide polymorphisms; CI, confidence interval; OR, odds ratio; MR-PRESSO, MR-pleiotropy residual sum and outliers.
Data Sharing Statement
The data that support the findings of this study are openly available in the IEU Open GWAS database (https://gwas.mrcieu.ac.uk/) and the Finngen database (https://www.finngen.fi/fi).
Institutional Review Board Statement
Our study used publicly available GWAS aggregate statistics (no individual-level data). The study is eligible for exemption from ethics approval under Article 32(1) and (2) of the Chinese Measures for the Ethical Review of Life Science and Medical Research Involving Human Subjects (2023) because it involves: (1) conducting the study using legally obtained publicly available data; and (2) studies involving non-invasive observational analysis of existing data. (http://www.nhc.gov.cn/).
Acknowledgments
We are deeply grateful to all individuals who participated in providing the data resources and to the scientific community members who made their data freely available.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Zhanjiang Science and Technology Development Special Projects (Nos. 2021A05086, 2022A01142, and 2022A01110), High-level Talent Startup Fund from the Second Affiliated Hospital of Guangdong Medical University (No.23H03), Guangdong Medical Research Fund Project (No.A2024728 and No.A2024723), and Natural Science Foundation of Basic and Applied Basic Research Fund of Guangdong Province (No. 2022A1515012375).
Disclosure
The authors declare no conflict of interest.
References
1. Patel AR, Patel AR, Singh S, Singh S, Khawaja I. Global Initiative for Chronic Obstructive Lung Disease: the Changes Made. Cureus. 2019;11(6):e4985. doi:10.7759/cureus.4985
2. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of Chronic Obstructive Pulmonary Disease and Its Attributable Risk Factors in 204 Countries and Territories, 1990-2019: results from the Global Burden of Disease Study 2019. BMJ (Clin. Res. Ed,). 2022;378:e069679. doi:10.1136/bmj-2021-069679
3. GBD. Diseases and Injuries Collaborators. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990-2019: a Systematic Analysis for the Global Burden of Disease Study 2019. Lancet). 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9.
4. Mallah H, Ball S, Sekhon J, Parmar K, Nugent K. Platelets in Chronic Obstructive Pulmonary Disease: an Update on Pathophysiology and Implications for Antiplatelet Therapy. Respir Med. 2020;171:106098. doi:10.1016/j.rmed.2020.106098
5. Zinellu A, Paliogiannis P, Sotgiu E, et al. Platelet Count and Platelet Indices in Patients with Stable and Acute Exacerbation of Chronic Obstructive Pulmonary Disease: a Systematic Review and Meta-Analysis. COPD. 2021;18(2):231–245. doi:10.1080/15412555.2021.1898578
6. Chebbo M, Duez C, Alessi MC, Chanez P, Gras D. Platelets: a Potential Role in Chronic Respiratory Diseases? Eur. Respir. Rev. 2021;30(161):210062. doi:10.1183/16000617.0062-2021
7. Ludwig N, Hilger A, Zarbock A, Rossaint J. Platelets at the Crossroads of Pro-Inflammatory and Resolution Pathways during Inflammation. Cells. 2022;11(12):1957. doi:10.3390/cells11121957
8. Teoh CM, Tan SSL, Tran T. Integrins as Therapeutic Targets for Respiratory Diseases. Curr. Mol. Med. 2016;15(8):714. doi:10.2174/1566524015666150921105339
9. Schønberg-Moe A, Csoma B, Bikov A, Müller V, Lázár Z. Platelet Count and Platelet-to-Lymphocyte Ratio at the Onset of a Severe COPD Exacerbation Are Unrelated to the Time till the next Moderate or Severe Relapse. Adv. Med. Sci. 2024;69(1):160–166. doi:10.1016/j.advms.2024.03.003
10. Xie X, Wang Y, Tian S, Cao D. Prognostic and Diagnostic Value of Platelet Distribution Width in COPD Patients with Pulmonary Hypertension: a Retrospective Study. Biotech and App Biochem. 2025;
11. Li J, Xiong Y, Li S, et al. Prevalence and Risk Factors of Pulmonary Embolism in COPD Patients Complicated with Secondary Polycythemia. Int. J. Chronic Obstr. Pulm. Dis. 2024;19:2371–2385. doi:10.2147/COPD.S481905
12. Doganci M, Eraslan Doganay G. Prognostic Significance of Thrombocytopenia and Mean Platelet Volume in COPD Patients with Acute Exacerbations in ICU Settings. Med. Sci. Monit.: Int. Med. J. Exp. Clin. Res. 2024;30:e944946. doi:10.12659/MSM.944946
13. Malerba M, Olivini A, Radaeli A, Ricciardolo FLM, Clini E. Platelet Activation and Cardiovascular Comorbidities in Patients with Chronic Obstructive Pulmonary Disease. Curr. Med. Res. Opin. 2016;32(5):885–891. doi:10.1185/03007995.2016.1149054
14. Richmond RC, Davey Smith G. Mendelian Randomization: concepts and Scope. Cold Spring Harb. Perspect. Med. 2022;12(1):a040501. doi:10.1101/cshperspect.a040501
15. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian Randomisation Studies: a Guide, Glossary, and Checklist for Clinicians. BMJ (Clin. Res. Ed,). 2018;362:k601. doi:10.1136/bmj.k601
16. Sekula P, Del Greco M, Pattaro C, Köttgen A. Mendelian Randomization as an Approach to Assess Causality Using Observational Data. J. Am. Soc. Nephrol.: JASN. 2016;27(11):3253–3265. doi:10.1681/ASN.2016010098
17. Gl C, A G, None S, et al. A Framework for Assessing Selection and Misclassification Bias in Mendelian Randomisation Studies: an Illustrative Example between Body Mass Index and Covid-19. BMJ. 2023;381:1. doi:10.1136/bmj-2022-072148.
18. Skrivankova VW, Richmond RC, Woolf BAR, et al. Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomisation (STROBE-MR): explanation and Elaboration. BMJ (Clin. Res. Ed,). 2021;375:n2233. doi:10.1136/bmj.n2233
19. Lawler T, Warren Andersen S. Serum 25-Hydroxyvitamin D and Cancer Risk: a Systematic Review of Mendelian Randomization Studies. Nutrients. 2023;15(2):422. doi:10.3390/nu15020422
20. Burgess S, Butterworth AS, Thompson JR. Beyond Mendelian Randomization: how to Interpret Evidence of Shared Genetic Predictors. J Clin Epidemiol. 2016;69:208–216. doi:10.1016/j.jclinepi.2015.08.001
21. Vuckovic D, Bao EL, Akbari P, et al. The Polygenic and Monogenic Basis of Blood Traits and Diseases. Cell. 2020;182(5):1214–1231.e11. doi:10.1016/j.cell.2020.08.008
22. Kurki MI, Karjalainen J, Palta P, et al. FinnGen Provides Genetic Insights from a Well-Phenotyped Isolated Population. Nature. 2023;613(7944):508–518. doi:10.1038/s41586-022-05473-8
23. Campos AI, Kho P, Vazquez-Prada KX, et al. Genetic Susceptibility to Pneumonia: a GWAS Meta-Analysis between the UK Biobank and FinnGen. Twin Res. Hum. Genet.: Off. J. Int. Soc. Twin Stud. 2021;24(3):145–154. doi:10.1017/thg.2021.27
24. Pierce BL, Ahsan H, VanderWeele TJ. Power and Instrument Strength Requirements for Mendelian Randomization Studies Using Multiple Genetic Variants. International Journal of Epidemiology. 2011;40(3):740–752. doi:10.1093/ije/dyq151
25. Kamat MA, Blackshaw JA, Young R, et al. PhenoScanner V2: an Expanded Tool for Searching Human Genotype–Phenotype Associations. Bioinformatics. 2019;35(22):4851–4853. doi:10.1093/bioinformatics/btz469
26. Cheng Z, Gao L, Huang P, Luo D, Bi C, Chen X. Genetic Causal Association between Rheumatoid Arthritis and Periodontitis: a Bidirectional Two-Sample Mendelian Randomization Analysis. Clin. Oral Investig. 2024;28(1):107. doi:10.1007/s00784-024-05512-w
27. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet. Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
28. Burgess S, Thompson SG. Interpreting Findings from Mendelian Randomization Using the MR-Egger Method. Eur. J. Epidemiol. 2017;32(5):377–389. doi:10.1007/s10654-017-0255-x
29. Long Y, Tang L, Zhou Y, Zhao S, Zhu H. Causal Relationship between Gut Microbiota and Cancers: a Two-Sample Mendelian Randomisation Study. BMC Med. 2023;21(1):66. doi:10.1186/s12916-023-02761-6
30. Burgess S, Butterworth A, Thompson SG. Mendelian Randomization Analysis with Multiple Genetic Variants Using Summarized Data. Genet. Epidemiol. 2013;37(7):658–665. doi:10.1002/gepi.21758
31. Wang Y, Hu X, Wang X, Li L, Lou P, Liu Z. Exploring the Two-Way Link between Migraines and Venous Thromboembolism: a Bidirectional Two-Sample Mendelian Randomization Study. Thromb. Haemost. 2024;124(11):1053–1060. doi:10.1055/a-2313-0311
32. Li J, Wei J, Wang J, et al. Association between Gut Microbiota and Spinal Stenosis: a Two-Sample Mendelian Randomization Study. Front. Immunol. 2024;15:1360132. doi:10.3389/fimmu.2024.1360132
33. P M, I B, E D, et al. Key Role of Activated Platelets in the Enhanced Adhesion of Circulating Leucocyte-Platelet Aggregates to the Dysfunctional Endothelium in Early-Stage COPD. Front. Immunol. 2024;15. doi:10.3389/fimmu.2024.1441637.
34. Moniruzzaman M, Karim MR, Ahamed F, et al. Platelet Count as a Severity of Chronic Obstructive Pulmonary Disease. Mymensingh Med. J.: MMJ. 2020;29(2):241–247.
35. Wang R, Li J-Y, Cao Z, Li Y. Mean Platelet Volume Is Decreased during an Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Respirol. (Carlt. Vic,). 2013;18(8):1244–1248. doi:10.1111/resp.12143
36. Makhlouf HA, Sadek SH, Nafady AAH. Platelet Function in Diabetic and Nondiabetic Patients with Chronic Obstructive Pulmonary Disease: a Case Control Study. The Clinical Respiratory Journal. 2018;12(1):48–56. doi:10.1111/crj.12477
37. Fawzy A, Anderson JA, Cowans NJ, et al. Association of Platelet Count with All-Cause Mortality and Risk of Cardiovascular and Respiratory Morbidity in Stable COPD. Respiratory Research. 2019;20(1):86. doi:10.1186/s12931-019-1059-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.