Back to Journals » International Journal of General Medicine » Volume 17
Association Between Periodontal Diseases and Hypothyroidism: A Case–Control Study
Authors AlAhmari FM ![]() , Albahouth HS, Almalky HA
, Albahouth HS, Almalky HA ![]() , Almutairi ES, Alatyan MH, Alotaibi LA
, Almutairi ES, Alatyan MH, Alotaibi LA ![]()
Received 19 June 2024
Accepted for publication 13 August 2024
Published 20 August 2024 Volume 2024:17 Pages 3613—3619
DOI https://doi.org/10.2147/IJGM.S476430
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jacopo Manso
Fatemah Mohammed AlAhmari,1 Hind Saleh Albahouth,2 Hadeel Ali Almalky,2 Ebtihal Saad Almutairi,2 Muzun Hamoud Alatyan,2 Lama Ali Alotaibi2
1Department of Periodontics and Community Dentistry, College of Dentistry, King Saud University, Riyadh, Saudi Arabia; 2College of Dentistry, King Saud University, Riyadh, Saudi Arabia
Correspondence: Fatemah Mohammed AlAhmari, King Saud University, Riyadh, Saudi Arabia, Email [email protected]
Objective: Periodontal diseases are chronic inflammatory disorders influenced by systemic health of the individual. This study aimed to investigate the association between hypothyroidism and periodontal disease in a cohort of adult Saudi population.
Methods: This case–control study included 201 adults with hypothyroidism on hormone replacement therapy and 188 healthy controls. The medical files of patients were reviewed to check thyroid stimulation hormone (TSH) and free thyroxine (FT4) levels. Participants completed a questionnaire on demographic and health information, followed by a comprehensive periodontal examination. Pearson chi-square and binary logistic regression analyses determined associations, with a significance set at p ≤ 0.05.
Results: Gingivitis was found in 20.9% of cases and 58% of controls. Periodontitis stages I, II, III and IV were in general higher in cases compared to controls (23.4%, 27.9%, 21.9%, 6% in cases versus 13.8%, 17%, 9.6%, 1.6% in controls, respectively). Mean PPD and CAL values were higher in cases (5.54 ± 2.5 and 3.88 ± 3.1) than in controls (4.03 ± 1.6 and 1.72 ± 2.4). Significant associations between periodontal status and hypothyroidism were found (p < 0.0001). The periodontal status in hypothyroid cases correlated significantly with hormone replacement therapy dose and duration (p < 0.0001).
Conclusion: The findings of the current study showed that, in a cohort of adult Saudi subjects, patients with hypothyroidism have higher prevalence and more severe periodontal disease symptoms compared to controls, suggesting significant association.
Keywords: hypothyroidism, periodontal diseases, hormone replacement therapy, association, case–control study
Introduction
Periodontitis is one of the most common infectious diseases in humans. It is a chronic bacterial infection characterised by persistent inflammation, connective tissue breakdown and alveolar bone destruction. The chronic inflammation associated with the disease is attributed to the subgingival bacteria-induced immune response dysregulation. Severe periodontitis affects 7.4% of the world’s population, making it a serious global public health challenge.1,2 Clinically, the disease can cause impaired function and aesthetics, adversely affects the overall quality of life of affected individuals, and if not properly treated, it will irreversibly progress and result in tooth loss. There is a growing body of evidence that indicates that periodontitis is independently associated with several systemic conditions, including cardiovascular disease, type 2 diabetes, respiratory diseases, premature birth, osteoporosis, Alzheimer’s disease, rheumatoid arthritis, and other autoimmune diseases.2,3
Hypothyroidism is a common endocrine disorder identified as failure of the thyroid gland to produce adequate thyroid hormone to meet the metabolic demands of the body. If left untreated, it can lead to other significant comorbidities, such as hypertension, dyslipidemia, infertility, cognitive impairment, and neuromuscular dysfunction.4 The most common cause of hypothyroidism is primary gland failure, either due to congenital causes, autoimmune thyroiditis, or infiltrative diseases. The disease can also occur due to insufficient thyroid gland stimulation by the hypothalamus or pituitary gland. Iodine deficiency, surgical thyroidectomy, and some medications can also induce hypothyroidism in some patients. Autoimmune thyroid disease is the most common aetiology of hypothyroidism in the United States. In some other countries, iodine deficiency is highly prevalent, causing hypothyroidism affecting children and infants too.5,6
Periodontitis shares risk factors with other chronic noncommunicable diseases and has bidirectional associations with general health and other systemic diseases. There is a growing global consensus that improving oral and periodontal health positively impact the systemic health and well-being. Previous investigations had suggested a reciprocal relationship between endocrine disorders, including hypothyroidism, and periodontal diseases and that this relationship is mediated through the immune system. Hypothyroidism may be associated with an increased risk of periodontal disease.7–9 There is debate whether their concomitance reflects a causal link is coincidence, or the result of one unmasking the other and the data from the Saudi Arabian population are limited. The aim of the current study was to investigate the relationship between hypothyroidism and periodontal status in a cohort of Saudi Arabian adult population.
Materials and Methods
The study was conducted in the outpatient clinic at the College of Dentistry, King Saud university (KSU), Riyadh, Saudi Arabia. The study complies with the Declaration of Helsinki and the protocol was approved by the Institutional Review Board for Health Sciences Colleges Research on Human Subjects, KSU (E-22-7407). Participants were informed about the nature of the study and that they could withdraw at any stage of the investigation without consequences. Adult Saudi patients with primary hypothyroidism diagnosis receiving thyroid hormone replacement therapy were recruited for the study as well as a matched control group comprising healthy individuals. Primary hypothyroidism was defined by elevated TSH levels above 4.0 mIU/L and low free thyroxine (fT4) levels below 0.7 ng/dL. Hypothyroidism was excluded in the control group by confirming that a recent (within the past 6 months) TSH assay fell within the normal range of 0.4–4.0 mIU/L. We reviewed each patient’s medical file to verify TSH and fT4 levels and to ensure that the diagnosis was confirmed by an endocrinologist. The mean TSH level in hypothyroidism cases was 9.3 ± 3.6 mIU/L, while among controls, it was 2.7 ± 1.1 mIU/L (Table 1). Written informed consent was obtained from all participants before the study commencement. Sample size estimation was carried out by conducting a pilot study. Using the 26% prevalence of periodontal disease among healthy subjects, with an odds ratio of 2.0 at 0.05 level of significance and 90% power, keeping all other values constant, a sample of 196 per group was required.
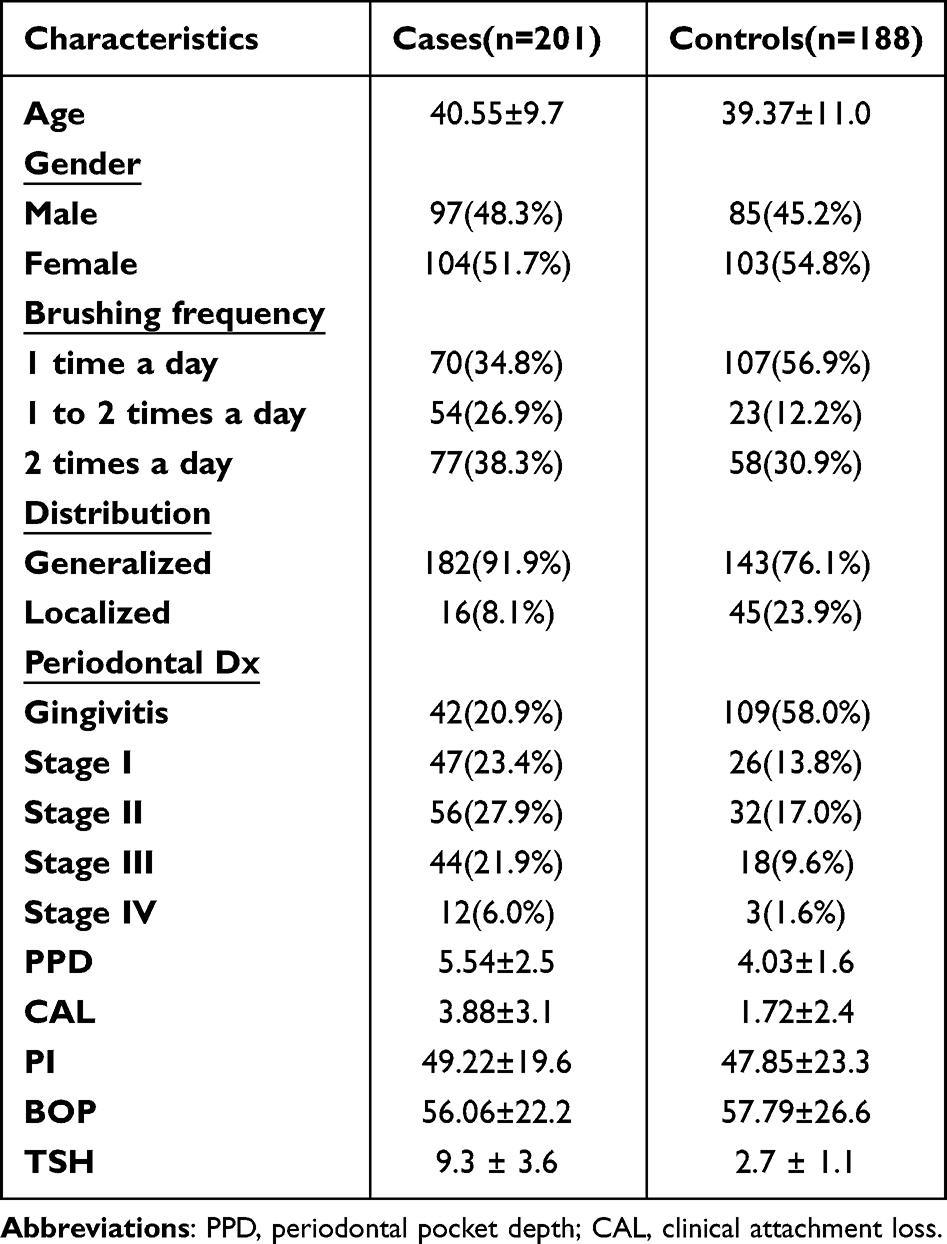 |
Table 1 Demographic and Clinical Characteristics of the Included Sample |
The test group consisted of 201 cases selected according to predefined criteria of being adults (age ≥18 years), diagnosed with primary hypothyroidism and treated with hormone replacement therapy. Cases were excluded if their medical records indicated previous diagnosis of other chronic diseases such as diabetes mellitus or other systemic conditions such as cardiovascular diseases, renal diseases, cancer, and hepatic disorders; received other pharmaceutical agents such as antibiotics, steroids, anti-inflammatory medications and/or bisphosphonates within the past 60 days; and/or received any periodontal treatment in the past 60 days. Female patients were excluded if they were pregnant and/or nursing. The control group consisted of 188 healthy age and gender matching adults. All participants responded to a pre-examination questionnaire to collect information about the age, sex, education level, smoking habits, medical history, oral hygiene behaviours, brushing frequency, duration since hypothyroidism was first diagnosed, and the dose of medication used. The periodontal status of all participants was then assessed via comprehensive full oral exam recording the probing pocket depth (PPD; distance between the marginal gingiva and the bottom of the periodontal pocket, in millimeters), plaque index (PI; The presence or absence of dental plaque at four points mesial, buccal, lingual, and distal on each tooth, determined after the application of a disclosing agent), bleeding on probing (BOP; the occurrence of bleeding within 15 seconds after probing, indicating a positive result) and clinical attachment loss (CAL; distance between the cemento-enamel junction and the bottom of the pocket, in millimeters). A Williams’ periodontal probe (Hu-Friedy® PW6) was utilized for measuring the clinical parameters including PPD and CAL. Six sites per tooth were assessed, and a diagnosis of periodontitis was established when subjects had at least two sites with a PPD ≥ 4 mm and a CAL ≥ 1 mm (one on each tooth). A case with 30% or more of teeth involved was classified as generalized periodontitis. Individuals with mean PPD <3mm and less than 10% bleeding sites with absence of clinically detectable signs of inflammation were categorized as having a healthy periodontium. Classification of periodontitis was determined based on the criteria proposed by the 2017 World Workshop on the Classifications of Periodontal and Peri-implant Diseases and Conditions.3,10
Statistical Analysis
Data were analyzed using IBM SPSS Statistical software for Windows version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics (mean, standard deviation, frequencies, and percentages) were used to describe the quantitative and categorical variables. Pearson chi-square test and odds ratios were used to assess and measure the association between categorical variables and outcome (cases and controls). Student’s t-test for independent samples was used to compare the mean values of quantitative variables between cases and controls. The binary logistic regression was used to identify the independent variables associated with hypothyroidism diagnosis. A p-value of ≤0.05 and 95% confidence intervals were used to report the statistical significance and precision of results.
Results
The sample was classified into 201 hypothyroidism patient (Cases, mean age 40.55 ± 9.7 years, 48.3% males) and 188 healthy subjects (Control, mean age 39.37 ± 11 years, 45.2% males). The characteristics of the two groups are presented in Table 1. A brushing frequency of one time a day was reported for 34.8% and 56.9% and two times a day for 38.3 and 30.9% of the cases and control groups, respectively. The distribution of periodontal disease was generalized in 91.9% of cases and 76.1% among controls. The periodontal status was classified as gingivitis in 20.9% of cases and 58% of controls. Periodontitis classification of stages I, II, III and IV was in general higher in cases compared to controls (23.4%, 27.9%, 21.9%, 6% in cases versus 13.8%, 17%, 9.6%, 1.6% in controls, respectively). The mean values of PI and BOP in cases were 49.22 ± 19.6 and 56.06 ± 22.2 versus 47.85 ± 23.3 and 57.79 ± 26.6 among controls, respectively. The mean values of PPD and CAL in cases were 5.54 ± 2.5 and 3.88 ± 3.1 versus 4.03 ± 1.6 and 1.72 ± 2.4 among controls, respectively (Table 1).
The bivariate analysis conducted to assess the association between demographic and clinical characteristics of the study sample revealed statistically significant association between the periodontal status in terms of distribution of periodontal diseases (generalized vs localized), severity of periodontal diseases, PPD, CAL, and the hypothyroidism diagnosis (p < 0.0001). The odds of having generalized periodontal diseases was 3.58 times more in hypothyroidism cases when compared with controls (p < 0.0001). Similarly, the odds of having stage I, II, III and IV periodontitis was 4.69, 4.54, 6.34, and 10.38 times more in hypothyroidism cases compared with controls, respectively, with differences being statistically significant (p < 0.0001). Differences in the mean values of PPD and CAL were significantly higher in cases compared to the controls (p < 0.0001). The corresponding odds ratios of 1.43 and 1.32 indicated that the odds of having higher PPD and CAL values was 43% and 32% times more in cases when compared with controls, respectively (Table 2). The multivariate logistic regression analysis indicated that two clinical variables, distribution and classification of periodontal diseases were independently associated with hypothyroidism diagnosis (Table 3).
 |
Table 2 Association Between Demographic, Clinical Characteristics, and Periodontal Status |
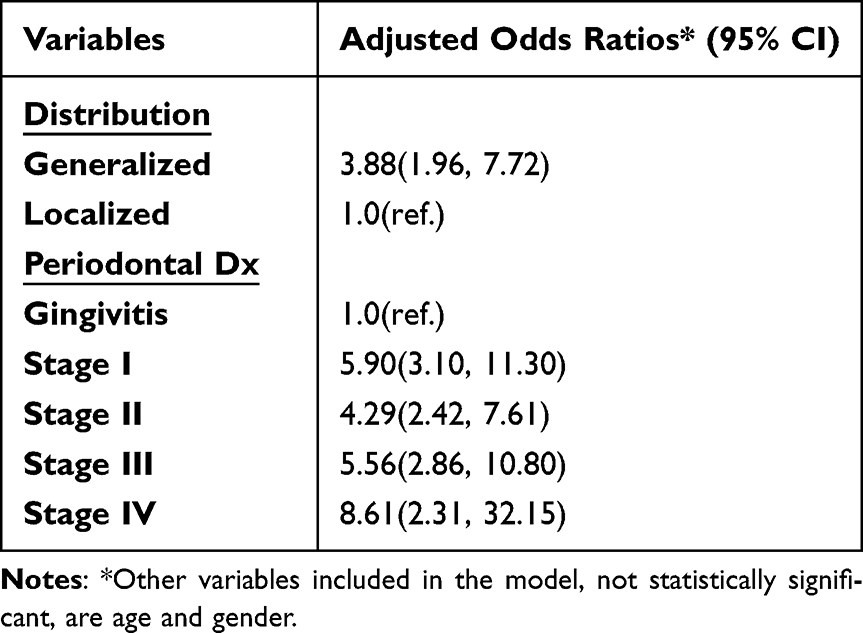 |
Table 3 Clinical Variables Independently Associated with Periodontal Disease (Multivariate Logistic Regression Analysis) |
The periodontal status of the hypothyroidism cases was significantly associated with the hormonal replacement therapy dose and duration (p < 0.0001). Patients on higher doses of medication and for longer duration suffered more severe periodontal tissue destruction as the majority presented with stage II to IV periodontitis (Table 4).
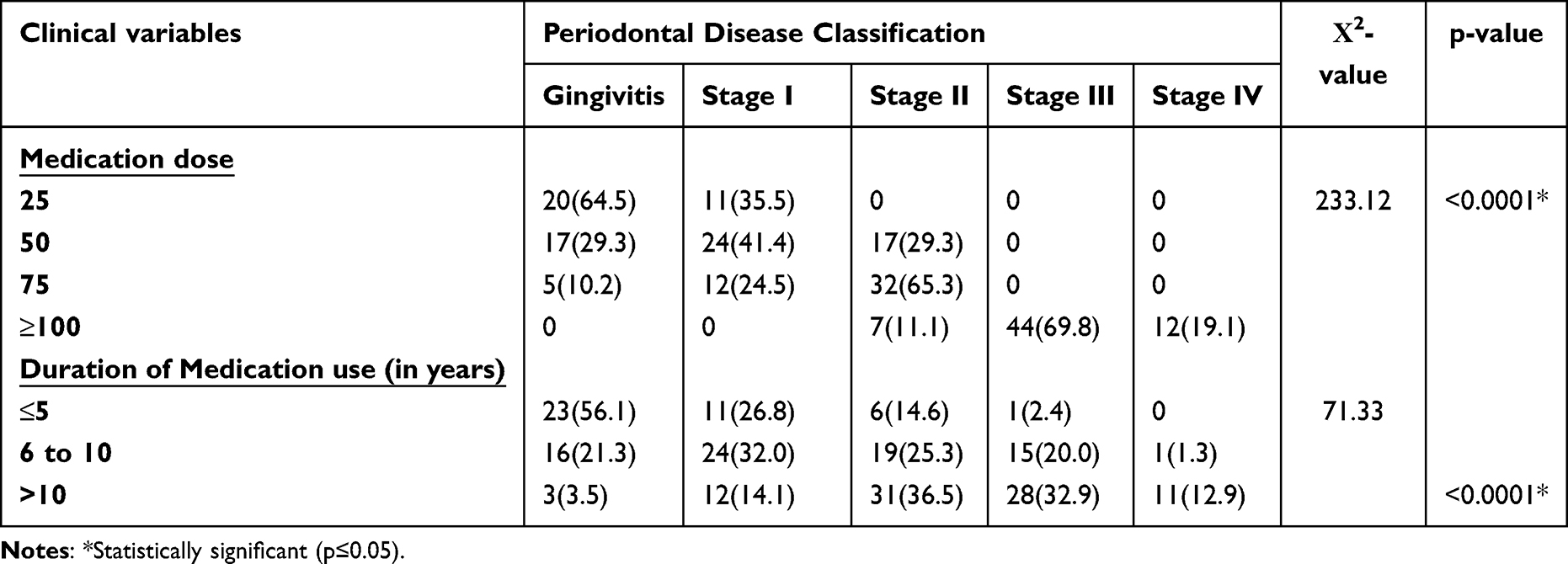 |
Table 4 Association Between Medication Dose, Duration of Use, and Periodontal Status Among Cases |
Discussion
Periodontitis is the most common form of periodontal diseases, which includes a group of inflammatory diseases that affect the periodontal supporting tissues of the teeth. It is commonly regarded a “silent disease” since patients present with no or few symptoms until the disease progresses to destroy the periodontal soft tissues and alveolar bone.11 Periodontitis is considered the main cause of tooth loss after the third decade of life. Current evidence indicates that periodontitis is a complex disease with multiple potential contributing factors including genetics and epigenetics, environmental, and behavioural factors. Low socioeconomic status, poor oral hygiene, psychological stress, advanced age, use of certain medications, and some systemic conditions are well-recognised risk factors that contribute to the initiation and progression of periodontal diseases.11,12
Hypothyroidism is one of the most common hormone deficiency disorders. According to the time of onset, it could be classified as congenital or acquired. Symptoms of hypothyroidism include fatigue, weight gain, alteration in cognition, infertility, menstrual abnormalities, irregular heart rate, and depression. Monotherapy with levothyroxine at doses to normalize the serum thyroid-stimulating hormone (TSH) is the standard of care for treating hypothyroidism.13,14 Studies had previously suggested that hypothyroidism may be associated with an increased risk of periodontal diseases. The present study was conducted to investigate the association between hypothyroidism and periodontal status in a cohort of Saudi Arabian adult population.
We have demonstrated a significantly increased prevalence and severity of periodontitis in subjects with treated hypothyroidism compared to controls. This increase seen in adult Saudi patients diagnosed with hyperthyroidism was similar to reports on other ethnic populations.15–18 In the current study, subjects with hypothyroidism had significantly higher PPD and CAL when compared with matched controls. Attard and Zarb,19 in their study, demonstrated an association between hypothyroidism and peri-implant radiographic bone loss, compared with normal controls.19 Rahangdale and Galgali20 reported statistically significant higher PPD and CAL in hypothyroidism patients in comparison to the controls. They concluded that, since all other variables that might affect the periodontal status of the patients were controlled, the history of hypothyroidism and replacement therapy probably had the main effect on PPD and CAL, the most reliable measure of periodontitis. Our data, together with previous observations, support the generally accepted view that chronic inflammatory periodontal diseases are associated with endocrinal morbidity.
In adults, the integrity of the skeletal structures, including the alveolar bone, is maintained by bone remodelling, a process controlled by thyroid hormones and TSH.21 Animal models of hypothyroidism have demonstrated alterations in bone metabolism, through a mechanism by which thyroid hormone has direct or indirect effects on bone cells.22–24 Feitosa et al22 used an experimental periodontitis model in rats to evaluate, histologically, the influence of thyroid hormones on the rate of periodontal disease progression. The results indicated that hypothyroidism significantly increased the bone loss resulting from ligature-induced periodontitis and the number of TRAP-positive cells on the linear surface of bone crest. They concluded that decreased serum levels of thyroid hormones may enhance periodontitis-related bone loss, as a function of an increased number of resorbing cells. It is possible to speculate that the significant association between higher distribution and severity of periodontal disease in hypothyroidism cases in the current study was related to the negative effect of hypothyroidism on bone remodelling sequence.
The present study is the first to indicate that the periodontal status of the hypothyroidism cases was significantly associated with the hormone replacement therapy dose and duration. Patients on higher doses of medication and for longer duration suffered more severe periodontal tissue destruction. This might imply that the duration of the disease onset and the degree of hormonal deficiency are critical in determining the periodontal tissue response. It has been proposed that the cytokines produced due to thyroid dysfunction might act as initiators for an amplified inflammatory cascade systemically.25 This, in combination with the existing inflammatory reaction in the periodontium due to the endotoxins produced by microbial plaque, might lead to higher local inflammatory mediator concentration in the periodontal tissues, including matrix metalloproteinases, leading to excessive periodontal tissue breakdown. Furthermore, it has been reported that in patients with hypothyroidism using a large dose of thyroxine replacement therapy, the risk of bone fracture increased compared to small doses, which could be attributed to lower bone density and poor bone quality reported with high-versus-low-dose thyroxine replacement.26,27
In summary, we have shown that, in a cohort of adult Saudi subjects, patients with hypothyroidism have higher prevalence and more severe periodontal disease compared to controls, suggesting association. However, it is important to interpret the data carefully, since case–control study is not the best approach to show a cause-and-effect relationship. Furthermore, the result of the current study was based on data collected from a single hospital, and its conclusions might not be entirely generalizable. Despite the limitations, this study offers guidance for future research and presents evidence of correlation from a group that has not been previously explored. The results of this study thus support routine periodontal evaluation for patients with hypothyroidism. Further studies are required to investigate the pathophysiology of periodontal tissue diseases and its relationship to the underlying endocrinal disorder.
Conclusion
The findings of the current study showed that, in a cohort of adult Saudi subjects, patients with hypothyroidism have higher prevalence and more severe periodontal disease symptoms compared to controls, suggesting significant association. However, the study was not sufficiently powered to estimate the association in the general population. Further studies are required to investigate the pathophysiology of the periodontal tissue reaction and its relationship to the underlying endocrinal disorder.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kwon T, Lamster IB, Levin L. Current concepts in the management of periodontitis. Int Dent J. 2021;71(6):462–476.
2. Janakiram C, Dye BA. A public health approach for prevention of periodontal disease. Periodontol. 2020;84(1):202–214. doi:10.1111/prd.12337
3. Papapanou PN, Sanz M, Buduneli N, et al. Periodontitis: consensus report of workgroup 2 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Periodontol. 2018;89(Suppl 1):S173–S182. doi:10.1002/JPER.17-0721
4. Gaitonde DY, Rowley KD, Sweeney LB. Hypothyroidism: an update. Am Fam Physician. 2010;86(3):244–251.
5. Almandoz JP, Gharib H. Hypothyroidism: etiology, diagnosis, and management. Med CLIN North Am. 2012;96(2):203–221. doi:10.1016/j.mcna.2012.01.005
6. Yamada M, Mori M. Mechanisms related to the pathophysiology and management of central hypothyroidism. Nat Clin Pract Endocrinol Metab. 2008;4(12):683–694. doi:10.1038/ncpendmet0995
7. Genco RJ, Borgnakke WS. Risk factors for periodontal disease. Periodontology. 2013;62(1):59–94. doi:10.1111/j.1600-0757.2012.00457.x
8. Araujo VM, Melo IM, Lima V. Relationship between periodontitis and rheumatoid arthritis: review of the literature. Mediators Inflam. 2015;2015:259074. doi:10.1155/2015/259074
9. Winning L, Linden GJ. Periodontitis and systemic disease: association or causality? Cur Oral Health Rep. 2017;4:1–7. doi:10.1007/s40496-017-0121-7
10. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Periodontol. 2018;89(Suppl 1):S159–72. doi:10.1002/JPER.18-0006
11. Papapanou PN, Susin C. Periodontitis epidemiology: is periodontitis under‐recognized, over‐diagnosed, or both? Periodontology. 2017;75(2000):45–51. doi:10.1111/prd.12200
12. Kim TH, Heo SY, Chandika P, et al. A literature review of bioactive substances for the treatment of periodontitis: in vitro, in vivo and clinical studies. Heliyon. 2024;10(2):PMC10826675.
13. Chiovato L, Magri F, Carlé A. Hypothyroidism in context: where we’ve been and where we’re going. Adv Ther. 2019;36:47–58. doi:10.1007/s12325-019-01080-8
14. Barbesino G. Drugs affecting thyroid function. Thyroid. 2010;20(7):763–770. doi:10.1089/thy.2010.1635
15. Zahid TM, Wang BY, Cohen RE. The effects of thyroid hormone abnormalities on periodontal disease status. J Int Acad Periodontol. 2011;13:80–85.
16. Kothiwale S, Panjwani V. Impact of thyroid hormone dysfunction on periodontal disease. J Sci Soc. 2016;43:34–37.
17. Bhankhar RR, Hungund S, Kambalyal P, Singh V, Jain K. Effect of nonsurgical periodontal therapy on thyroid stimulating hormone in hypothyroid patients with periodontal diseases. Ind J Dent Res. 2017;28(1):16–21. doi:10.4103/ijdr.IJDR_174_16
18. Aldulaijan HA, Cohen RE, Stellrecht EM, Levine MJ, Yerke LM. Relationship between hypothyroidism and periodontitis: a scoping review. Clin Exp Dent Res. 2020;6:147–157. doi:10.1002/cre2.247
19. Attard NJ, Zarb GA. A study of dental implants in medically treated hypothyroid patients. Clin Imp Dent Res. 2002;4(4):220–231. doi:10.1111/j.1708-8208.2002.tb00174.x
20. Rahangdale SI, Galgali SR. Periodontal status of hypothyroid patients on thyroxine replacement therapy: a comparative cross-sectional study. J Indian Soc Periodontol. 2018;22:535–540. doi:10.4103/jisp.jisp_316_18
21. Akalin A, Colak O, Alatas O, Efe B. Bone remodelling markers and serum cytokines in patients with hyperthyroidism. Clin Endocrin. 2002;57(1):125–129. doi:10.1046/j.1365-2265.2002.01578.x
22. Feitosa DS, Marques MR, Casati MZ, Sallum EA, Nociti FH, De toledo S. The influence of thyroid hormones on periodontitis-related bone loss and tooth-supporting alveolar bone: a histological study in rats. J Periodontal Res. 2009;44(4):472–478. doi:10.1111/j.1600-0765.2008.01144.x
23. Bassett JH, Williams GR. Role of thyroid hormones in skeletal development and bone maintenance. Endocr Rev. 2016;37(2):135–187. doi:10.1210/er.2015-1106
24. Williams GR, Bassett JHD. Thyroid diseases and bone health. J Endocrinol Invest. 2018;41(1):99–109. doi:10.1007/s40618-017-0753-4
25. Monea A, Elod N, Sitaru A, Stoica A, Monea M. Can thyroid dysfunction induce periodontal disease. Eur Sci J. 2014;10(15):74–83.
26. Ko YJ, Kim JY, Lee J, et al. Levothyroxine dose and fracture risk according to the osteoporosis status in elderly women. J Prev Med Public Health. 2014;47(1):36–46. doi:10.3961/jpmph.2014.47.1.36
27. Karimifar M, Esmaili F, Salari A, Kachuei A, Faragzadegan Z, Karimifar M. Effects of Levothyroxine and thyroid stimulating hormone on bone loss in patients with primary hypothyroidism. J Res Pharm Pract. 2014;3(3):83–87. doi:10.4103/2279-042X.141099
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.