Back to Journals » Journal of Asthma and Allergy » Volume 15
Association Between Patient Preference for Inhaler Medications and Asthma Outcomes
Authors Nakanishi Y, Iwamoto H ![]() , Miyamoto S, Nakao S, Higaki N, Yamaguchi K
, Miyamoto S, Nakao S, Higaki N, Yamaguchi K ![]() , Sakamoto S, Horimasu Y
, Sakamoto S, Horimasu Y ![]() , Masuda T, Matsumoto N, Nakashima T
, Masuda T, Matsumoto N, Nakashima T ![]() , Onari Y, Fujitaka K, Haruta Y
, Onari Y, Fujitaka K, Haruta Y ![]() , Hamada H
, Hamada H ![]() , Hozawa S
, Hozawa S ![]() , Hattori N
, Hattori N
Received 12 July 2022
Accepted for publication 9 October 2022
Published 25 October 2022 Volume 2022:15 Pages 1539—1547
DOI https://doi.org/10.2147/JAA.S381509
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Yu Nakanishi,1 Hiroshi Iwamoto,1 Shintaro Miyamoto,1 Satoshi Nakao,1 Naoko Higaki,1 Kakuhiro Yamaguchi,1 Shinjiro Sakamoto,1 Yasushi Horimasu,1 Takeshi Masuda,1 Naoko Matsumoto,2 Taku Nakashima,1 Yojiro Onari,3 Kazunori Fujitaka,1 Yoshinori Haruta,4 Hironobu Hamada,5 Soichiro Hozawa,6 Noboru Hattori1
1Department of Molecular and Internal Medicine, Graduate School of Biomedical and Health Sciences, Hiroshima University, Hiroshima, Japan; 2Department of Respiratory Medicine, Hiroshima Red Cross Hospital & Atomic-Bomb Survivors Hospital, Hiroshima, Japan; 3Department of Respiratory Medicine, Hiroshima Mazda Hospital, Hiroshima, Japan; 4Haruta Respiratory Clinic, Hiroshima, Japan; 5Department of Physical Analysis and Therapeutic Sciences, Graduate School of Biomedical and Health Sciences Hiroshima University, Hiroshima, Japan; 6Hiroshima Allergy and Respiratory Clinic, Hiroshima, Japan
Correspondence: Hiroshi Iwamoto, Department of Molecular and Internal Medicine, Graduate School of Biomedical and Health Sciences, Hiroshima University, 1-2-3 Kasumi, Minami-ku, Hiroshima, 734-8551, Japan, Tel +81-82-257-5196, Email [email protected]
Purpose: Asthma guidelines recommend considering the patient preference to optimize medication choices. Patient preference for inhaler medication may affect asthma outcomes, but evidence regarding this is lacking. This study investigated the associations between patient preference for inhaler medications and asthma outcomes.
Patients and Methods: A multicenter questionnaire survey was conducted among 351 adult patients with asthma treated with regular inhaled corticosteroids. Agreement between patients’ preferences and current medication was evaluated using two questions: matched preference was defined as patients answering that the current inhaler medication was the most preferred treatment and they were satisfied with it. Mismatched preference was defined as when patients reported that the current inhaler medication was not the most preferred treatment and/or they were not satisfied with it. We investigated the factors associated with patient preference for asthma inhaler medications.
Results: In total, 269 (76.6%) patients were classified into the matched preference group and 82 (23.4%) patients into the mismatched preference group. Multivariate analyses showed that matched preference was independently associated with higher asthma control test scores (P< 0.001), fewer exacerbations (P=0.009), less regular oral corticosteroid use (P=0.009), and better inhaler adherence (P=0.006) than the mismatched preference group. In subgroup analysis, younger age was associated with matched preference in patients using dry powder inhalers but not in those using pressurized metered dose inhalers.
Conclusion: The use of preference-matched inhaler medication was associated with better asthma outcomes. Evaluation of patients’ preference for inhaler medication might provide useful information for individualized treatment with asthma inhaler medications.
Keywords: patient preference, asthma control, inhaled corticosteroids, inhaler adherence, shared decision-making
Plain Language Summary
The use of asthma inhaler medication that matches patient preference may be associated with better clinical outcomes; however, to date, evidence is lacking.
This study shows that preference-matched inhaled medication was associated with better asthma control, fewer exacerbations, less oral corticosteroid use, and better adherence in a real-world clinical setting.
Introduction
Inhaled corticosteroids (ICS) are the mainstay treatment for asthma and can lead to improved symptom control and reduced exacerbations.1 Various inhaler devices exist for asthma treatment, and device selection, as well as the choice of active drug, are important to achieve significant positive clinical response.2–4 Previous studies have shown that inhalation technique and treatment adherence can be influenced by inhaler device type and patient background characteristics.5–7 Moreover, to optimize the patient-level medication choices, asthma guidelines recommend consideration of patient preference.1,8,9 However, evidence on the influence of patient preference for inhaler medication on asthma outcomes is lacking. In this study, we evaluated patient preference for inhaler medication using self-reported questionnaires and investigated the associations of the answers with asthma control, exacerbation rate, regular oral corticosteroid (OCS) use, and adherence to treatment.
Materials and Methods
Patients
A multicenter cross-sectional study was conducted among adult patients with persistent asthma to investigate their preferences for inhaled asthma medications. Four hundred and seventy-two patients at five hospitals and clinics were enrolled from April 2018 to March 2019. Patients were eligible if they were aged ≥20 years and had physician-diagnosed persistent asthma that required regular administration of ICS. Asthma exacerbations were defined as worsening of asthma with patients requiring administration of systemic corticosteroids. The annual rate of exacerbations in the 2 years before study entry was evaluated using medical records. Patients with less than 2 years of clinical follow-up data before enrollment and those with incomplete data were excluded from the study. Overall, 351 patients were analyzed (Figure 1). All the participants were informed about the study aims, and their participation was voluntary and anonymized. The Medical Ethics Committee of Hiroshima University approved this study (E-1128) and waived the requirement for obtaining signed informed consent as this was a non-invasive questionnaire survey.
 |
Figure 1 Study flow. |
Questionnaires
This study evaluated patient preference for asthma inhaler medication using two questions. One question required the patient to choose the most preferred asthma inhaler medication from the full list of asthma control inhalers with their names and photographs. The other question asked whether the patients were satisfied with their inhaler medication. Matched preference was defined as patients answering that their current inhaler medication was their preferred medication and that they were satisfied with it (Figure 2). Patients were considered to have mismatched preferences when they answered that their preferred inhaler did not match the current inhaler and/or were not satisfied with it. Asthma symptom control was assessed using the asthma control test (ACT); uncontrolled asthma was defined as ACT score ≤19. Self-reported inhaler adherence was ascertained by participant responses to the question, “How frequently do you use your inhaler presently?”. Self-reported inhaler adherence score was rated on a 5-point scale (5 indicating always and 1 indicating never). It was classified as good (≥75% of medication taken) or poor (<75% of medication taken). We also sought information regarding reasons for dissatisfaction with the current inhaler using a multiple choice and free response questionnaire.
 |
Figure 2 Definition of patient preference for inhalers. |
Measurements
Pre-bronchodilator pulmonary function was measured using spirometry, and the percentage of predicted values was calculated using the Japanese reference values.10 Fractional exhaled nitric oxide (FeNO) was analyzed using NIOX VERO® from an aerocrine system, following the recommendations of the European Respiratory Society/American Thoracic Society.11
Statistical Analysis
The results are expressed as mean ± standard deviation. Comparisons of the two groups were made using the chi-square test, Fisher’s exact test, and Mann–Whitney U-test. Univariate and multivariate linear regression model analyses were performed to investigate the clinical predictors of uncontrolled asthma and the number of exacerbations. Logistic regression analysis was performed to determine the predictors of adherence to treatment and regular OCS use. Sex, age, body mass index (BMI), smoking pack years, treatment step, and type of inhaler (dry powder inhaler [DPI] or pressurized metered dose inhaler [pMDI]) were used as independent variables in the multivariate analyses. For multivariate analysis of regular OCS use, the treatment step was not included as an independent variable because all patients with OCS were on step five of treatment, and these two indices were highly correlated. All statistical analyses were performed using the JMP®14 software (SAS Institute Inc., Cary, NC, USA). Results with P-values ≤ 0.05 were considered statistically significant for all the analyses.
Results
Among the 351 patients with asthma, 269 (76.6%) were divided into the matched preference group and 82 (23.4%) into the mismatched preference group (Figure 2). Table 1 compares patient characteristics between the matched and mismatched preference groups. There were no significant differences in age, BMI, smoking history, disease duration of asthma, asthma treatment step, and type of inhaler device between the matched and mismatched preference groups. Regular OCS use was significantly less frequent in the matched preference group than in the mismatched group (3.7% vs 13.4%; P=0.003). The number and types of controller inhaled medications ever used were slightly but significantly lower in the matched-preference group than in the mismatched group (2.06 vs 2.46, P=0.004). The patients achieving > 75% adherence were higher in the matched preference group. Significantly fewer patients with uncontrolled asthma and fewer exacerbation rates were observed in the matched preference group than in the mismatched group (Figure 3).
 |
Table 1 Patient Characteristics |
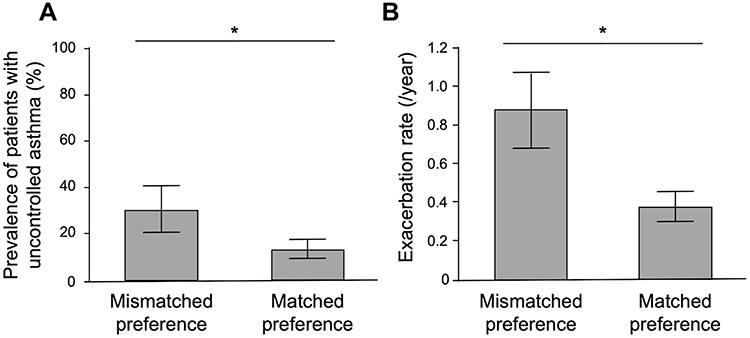 |
Figure 3 Comparison of (A) prevalence of uncontrolled asthma and (B) exacerbation rate between patients of matched and mismatched groups. Error bars represent (A) 95% score confidence intervals and (B) 95% confidence intervals. *P<0.05. |
Tables 2 and 3 show the results of univariate and multivariate regression analyses of the factors associated with uncontrolled asthma symptoms, exacerbation rate, inhaler adherence, and OCS use. Multivariate analyses revealed that matched preference was independently associated with a lower prevalence of patients with uncontrolled asthma, fewer exacerbations, better adherence to medication, and a lower rate of regular OCS use.
 |
Table 2 Univariate and Multivariate Linear and Logistic Regression Analyses for Uncontrolled Asthma, Exacerbation Rate, and Adherence |
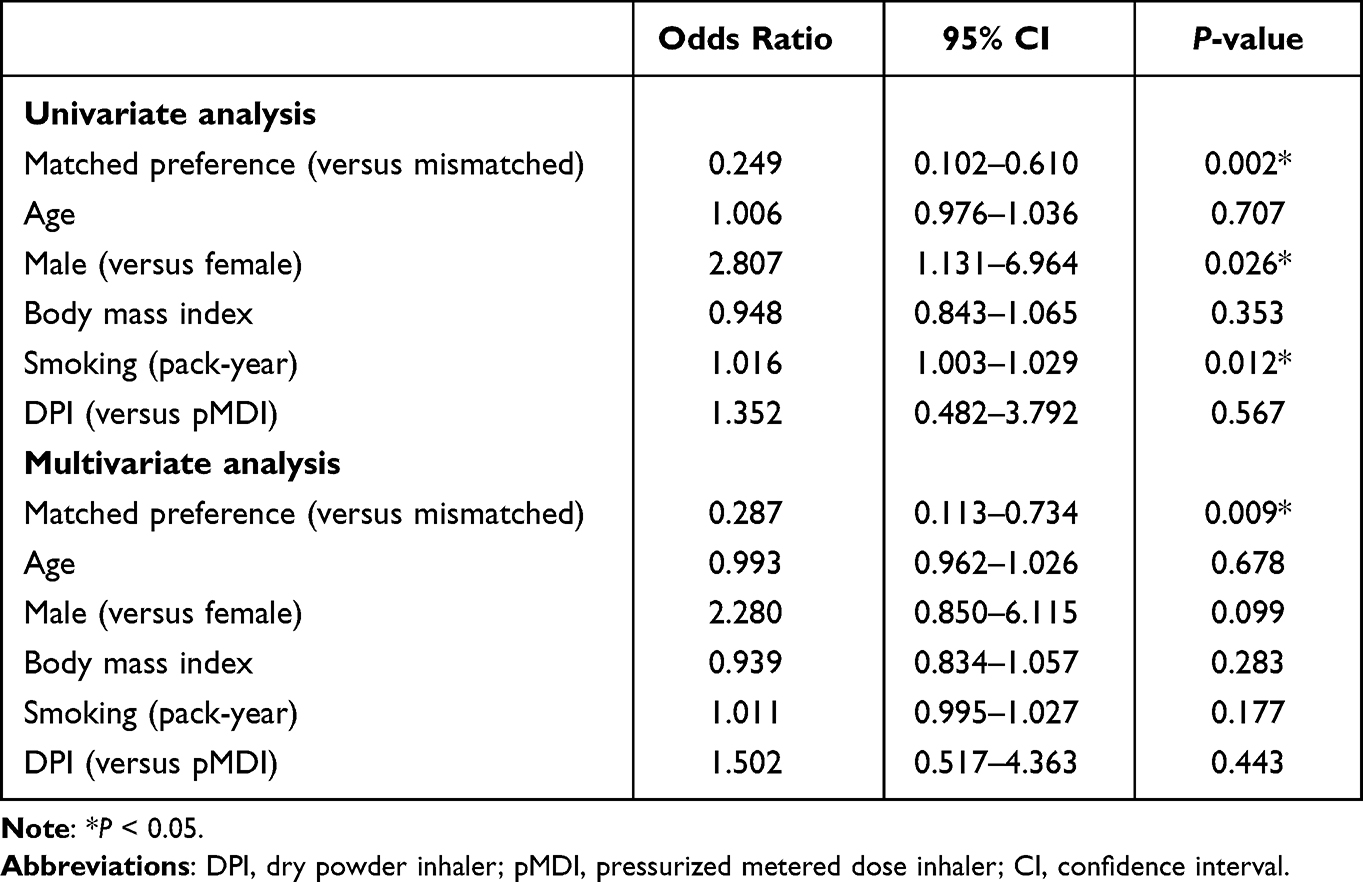 |
Table 3 Univariate and Multivariate Logistic Regression Analyses for Regular Oral Corticosteroid |
Additionally, we asked about the points of dissatisfaction with the current inhaler in the mismatched preference group. Twenty-nine (35%) patients in the mismatched group had a reason for dissatisfaction: No feeling of effect (n = 16), Upper respiratory tract discomfort (n = 6), Difficult to inhale (n = 3), Difficult to handle the device (n = 3), Too much numbers of inhalation (n = 1). On the other hand, 65% did not have any reason for dissatisfaction.
In the subgroup analyses by type of inhaler device, the prevalence of younger patients was significantly higher in the matched preference group among patients using DPI (P<0.05); among patients using pMDI, the prevalence of older patients tended to be higher in the matched group (P=0.087) (Table 4). There was no difference in other variables between patients using DPI and those using pMDI. Patients using DPI and pMDI used regular OCS less frequently and had fewer asthma exacerbations, lower prevalence of uncontrolled asthma, and better adherence in the matched preference group than in the mismatched group.
 |
Table 4 Comparison of Patient Characteristics Between Matched and Unmatched Groups Regarding DPI or pMDI Usage |
Discussion
We demonstrated that agreement between patients’ preferences and their prescribed inhaler medication was associated with fewer patients with uncontrolled asthma symptoms, fewer exacerbations, and a lower rate of regular OCS use irrespective of background characteristics, including the type of inhaler device. Matched preference for inhalers was also positively correlated with treatment adherence. The present results indicate that patient preference may significantly impact asthma outcomes, and investigating patient preference using simple questions could provide useful information for individualized treatment with asthma inhaler medications.
One important finding of this study is that using preference-matched inhalers is independently associated with lower rates of uncontrolled asthma symptoms, exacerbation, and regular OCS use, as well as better adherence to treatment. There have been inconsistent results regarding the association between patient satisfaction with inhaler medication and adherence to treatment and/or asthma outcomes. Small et al showed that patient satisfaction scores evaluated using 13 questions about inhalers were significantly associated with physician-perceived adherence to treatment, while Price et al showed that patient satisfaction scores evaluated using 12 questions were correlated with asthma outcomes but not with adherence scores.2,12 Plaza et al also reported that patients with higher scores on ten questions regarding the extent of satisfaction with an inhaler (FSI-10) had higher adherence and better symptom control.13 This study evaluated the agreement between patients’ preferences and current medication using two questions about their preferred medication and their satisfaction with the current inhaler. Our results showed that more than half of the patients in the mismatched group did not express dissatisfaction with the current inhaler. The reason for this discrepancy is unclear, but we speculate that it may be difficult for patients to identify specific problems, even when they do not prefer inhaler medications. The present results indicate that simple questions regarding patients’ preferences may provide valuable information for selecting asthma inhaler medications. Since asthma is a prevalent disease, many patients are treated by a non-specialist.1,2 Therefore, a simple method to evaluate patient preference would be useful in clinical practice. Further studies are needed to clarify whether switching to preference-matched inhalers can provide useful information for shared decision-making and improve asthma outcomes.
In the present study, subgroup analysis showed that the prevalence of younger patients was higher in the matched preference group among patients using DPI, and the prevalence of older patients tended to be higher in the matched group among patients using pMDI. The former result agrees with a previous report that younger patients showed a higher satisfaction score for inhalers, predominantly (91.2%) consisting of DPI.13 Moreover, Welch et al showed that patient satisfaction score was higher in Turbuhaler users than in pMDI users, primarily in younger patients (mean age, 38.7 years). Consistent with the latter result, Muraki et al showed that among older adult patients (mean age, 62.1 years), 57.4% of the individuals preferred pMDI and 35.3% preferred DPI.14 DPI does not need to be synchronized with breathing and is widely available; however, a thorough understanding of the wide variety of DPI devices available and their techniques and sufficient inspiratory flow rates is necessary.15–17 These device characteristics of DPIs may affect patient preference in older patients,18 and the present results suggest that attention should be paid to patient preference, particularly among older patients using DPIs.
This study has some limitations. First, inhaler handling error was not evaluated in this study. Although patient education was provided by respiratory physicians and non-physician medical staff, handling errors in some patients may have contributed to poor palatability and/or asthma control. Second, we did not include a broad range of patients with asthma during spirometry and FeNO administration in real-world clinical settings. Missing data can potentially decrease the ability to detect differences in these indices. Third, self-reported adherence to inhaler medication could be overestimated, and FSI-10 or electronic monitoring devices could help obtain more accurate information for treatment adherence.13,19 Fourth, three-fourths of the patients did not provide reasons for dissatisfaction with their current inhalers. This could imply that our questionnaire is imprecise and does not cover the entire preference issue. An inhaler-specific questionnaire, such as the FSI-10, might have picked up additional dissatisfaction. Finally, this was a cross-sectional survey; therefore, we did not have data on treatment change after this study and its effect on the patient’s preference and disease outcomes.
Conclusion
In summary, we demonstrated that agreement between patient preference and inhaler medication was associated with fewer patients with uncontrolled symptoms, fewer exacerbations, better adherence to treatment, and less use of regular OCS treatment. Evaluation of patients’ preference for inhaler medication might provide useful information for individualized treatment with asthma inhaler medications.
Abbreviations
ACT, asthma control test; BMI, body mass index; FeNO, fractional exhaled nitric oxide; ICS, inhaled corticosteroids; OCS, oral corticosteroids; DPI, dry powder inhaler; pMDI, pressurized metered dose inhaler.
Ethics Approval and Informed Consent
The study was approved by the Medical Ethics Committee of Hiroshima University and waived the requirement for obtaining signed informed consent (E-1128). All the participants were informed about the study aims, and their participation was voluntary and anonymized. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We thank Gaku Aoki and Tomoyuki Akita (Department of Epidemiology, Infectious Disease Control and Prevention, Institute of Biomedical and Health Sciences Hiroshima University) for their advice in statistical analysis. We also thank Editage English Editing Services (Tokyo, Japan) for English language editing.
Funding
All authors received no funding for this work.
Disclosure
Dr Hiroshi Iwamoto reports personal fees from Astrazeneca, Glaxosmithkline, and Kyorin Pharmaceutical, outside the submitted work. Dr. Yojiro Onari reports personal fees from GlaxoSmithKline, AstraZeneca, Novartis Pharma, Kyorin Pharmaceutical, outside the submitted work. Dr Yasushi Horimasu reports personal fees from Boehringer Ingelheim, outside the submitted work. Dr. Yoshinori Haruta reports personal fees from GlaxoSmithKline, AstraZeneca, Novartis Pharma and Kyorin Pharmaceutical, outside the submitted work. Dr. Soichiro Hozawa reported personal fees from GlaxoSmithKline,AstraZeneca, Novartis Pharma, Kyorin Pharmaceutical, outside the submitted work. Dr Noboru Hattori reports grants from Teijin Pharma and Kyorin Pharmaceutical and personal fees from GlaxoSmithKline, AstraZeneca, Novartis Pharma, and Kyorin Pharmaceutical, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Global strategy for ashtma management and prevention; 2021. Available from: https://ginasthma.org/.
2. Price DB, Román-Rodríguez M, McQueen RB, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract. 2017;5(4):1071–81.e9. doi:10.1016/j.jaip.2017.01.004
3. Ota K, Hasegawa T, Koya T, et al. Analysis of inhaled corticosteroid selection in patients with bronchial asthma using a questionnaire survey–effects of age, gender, and disease severity. Allergol Int. 2009;58(3):365–371. doi:10.2332/allergolint.08-OA-0077
4. Schreiber J, Sonnenburg T, Luecke E. Inhaler devices in asthma and COPD patients - a prospective cross-sectional study on inhaler preferences and error rates. BMC Pulm Med. 2020;20(1):222. doi:10.1186/s12890-020-01246-z
5. Koya T, Hasegawa T, Takasawa J, et al. Influence of adherence to inhaled corticosteroids and inhaler handling errors on asthma control in a Japanese population. Intern Med. 2018;57(23):3357–3363. doi:10.2169/internalmedicine.0986-18
6. Murphy J, McSharry J, Hynes L, Matthews S, Van Rhoon L, Molloy GJ. Prevalence and predictors of adherence to inhaled corticosteroids in young adults (15–30 years) with asthma: a systematic review and meta-analysis. J Asthma. 2021;58(5):683–705. doi:10.1080/02770903.2020.1711916
7. Darbà J, Ramírez G, Sicras A, García-Bujalance L, Torvinen S, Sánchez-de la Rosa R. Identification of factors involved in medication compliance: incorrect inhaler technique of asthma treatment leads to poor compliance. Patient Prefer Adherence. 2016;10:135–145. doi:10.2147/PPA.S95303
8. Nakamura Y, Tamaoki J, Nagase H, et al. Japanese guidelines for adult asthma 2020. Allergol Int. 2020;69(4):519–548. doi:10.1016/j.alit.2020.08.001
9. British Thoraric Society. BTS/SIGN British guideline on the management of asthma; 2019. Available from: https://www.brit-thoracic.org.uk/quality-improvement/guidelines/asthma/.
10. Kubota M, Kobayashi H, Quanjer PH, et al. Reference values for spirometry, including vital capacity, in Japanese adults calculated with the LMS method and compared with previous values. Respir Investig. 2014;52(4):242–250. doi:10.1016/j.resinv.2014.03.003
11. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/rccm.9120-11ST
12. Small M, Anderson P, Vickers A, Kay S, Fermer S. Importance of inhaler-device satisfaction in asthma treatment: real-world observations of physician-observed compliance and clinical/patient-reported outcomes. Adv Ther. 2011;28(3):202–212. doi:10.1007/s12325-010-0108-4
13. Plaza V, Giner J, Calle M, et al. Impact of patient satisfaction with his or her inhaler on adherence and asthma control. Allergy Asthma Proc. 2018;39(6):437–444. doi:10.2500/aap.2018.39.4183
14. Muraki M, Gose K, Hanada S, Sawaguchi H, Tohda Y. Which inhaled corticosteroid and long-acting β-agonist combination is better in patients with moderate-to-severe asthma, a dry powder inhaler or a pressurized metered-dose inhaler? Drug Deliv. 2017;24(1):1395–1400. doi:10.1080/10717544.2017.1378937
15. Turan O, Turan PA, Mirici A. Parameters affecting inhalation therapy adherence in elderly patients with chronic obstructive lung disease and asthma. Geriatr Gerontol Int. 2017;17(6):999–1005. doi:10.1111/ggi.12823
16. Zervas E, Samitas K, Gaga M. Assessment of satisfaction with different dry powder inhalation devices in Greek patients with COPD and asthma: the ANASA study. Int J Chron Obstruct Pulmon Dis. 2016;11:1845–1855. doi:10.2147/COPD.S113870
17. Tang WE, Lee ES, Lim Z, et al. A comparative study evaluating patients’ satisfaction with different dry powder inhalers. Chest. 2017;152(4):A25. doi:10.1016/j.chest.2017.08.055
18. Hira D, Komase Y, Koshiyama S, et al. Problems of elderly patients on inhalation therapy: difference in problem recognition between patients and medical professionals. Allergol Int. 2016;65(4):444–449. doi:10.1016/j.alit.2016.04.002
19. Hesso I, Nabhani Gebara S, Greene G, Co Stello RW, Kayyali R. A quantitative evaluation of adherence and inhalation technique among respiratory patients: an observational study using an electronic inhaler assessment device. Int J Clin Pract. 2020;74(2):e13437. doi:10.1111/ijcp.13437
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pulmonologists’ Opinion on the Use of Inhaled Corticosteroids in Chronic Obstructive Pulmonary Disease Patients in Spain: A Cross-Sectional Survey
Miravitlles M, González-Torralba F, Represas-Represas C, Pomares X, Márquez-Martín E, González C, Amado C, Forné C, Alonso S, Alcázar B, Barrecheguren M, Jurado Mirete JM, Naval E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1577-1587
Published Date: 12 July 2022
Mometasone/Indacaterol/Glycopyrronium (MF/IND/GLY) and MF/IND at Different MF Strengths versus Fluticasone Propionate/Salmeterol Xinafoate (FLU/SAL) and FLU/SAL+ Tiotropium in Patients with Asthma
van Zyl-Smit RN, Chapman KR, Kerstjens HAM, Gessner C, Sagara H, Tanase AM, Hosoe M, Pethe A, Lawrence D, Tillmann HC, D'Andrea P
Journal of Asthma and Allergy 2023, 16:123-134
Published Date: 20 January 2023
Real-World Safety and Effectiveness of Benralizumab in Japanese Patients with Severe Asthma: A Multicenter Prospective Observational Study
Yamaguchi M, Nishimura Y, Takumi Y, Hayashi N, Sakamoto K, Tohda Y
Journal of Asthma and Allergy 2024, 17:45-60
Published Date: 20 January 2024
Effects of ICS + LABA Combination Therapy on Asthma Control: An Observational Study in Real-World Settings
Han P, Wang L
Therapeutics and Clinical Risk Management 2026, 22:547261
Published Date: 7 February 2026
Uncontrolled Asthma and Severe COVID-19: A Prospective Bidirectional Risk Analysis
Selberg S, Karlsson Sundbaum J, Lindberg A, Konradsen JR, Backman H, Hedman L, Stridsman C
Journal of Asthma and Allergy 2026, 19:574350
Published Date: 19 February 2026