Back to Journals » International Journal of Women's Health » Volume 14
Association Between Obstetric History and Urinary Incontinence in a Cohort of Resistance-Trained Women
Authors Wikander L ![]() , Kirshbaum MN, Waheed N, Gahreman DE
, Kirshbaum MN, Waheed N, Gahreman DE ![]()
Received 19 March 2022
Accepted for publication 27 July 2022
Published 2 September 2022 Volume 2022:14 Pages 1211—1218
DOI https://doi.org/10.2147/IJWH.S367110
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Marleen van Gelder
Lolita Wikander,1 Marilynne N Kirshbaum,2 Nasreena Waheed,3 Daniel E Gahreman1,4
1College of Health and Human Sciences, Charles Darwin University, Darwin, Northern Territory, Australia; 2Research and Innovation, Charles Darwin University, Darwin, Northern Territory, Australia; 3College of Nursing and Midwifery, Charles Darwin University, Darwin, Northern Territory, Australia; 4Department of Sport, Exercise, Recreation, and Kinesiology, East Tennessee State University, Johnson City, TN, USA
Correspondence: Lolita Wikander, College of Health and Human Sciences, Charles Darwin University, Darwin, Northern Territory, Australia, Tel +61 421314515, Fax +61 08 8946 6642, Email [email protected]
Purpose: Urinary incontinence has the potential to reduce participation in sport and exercise and diminish athletic performance. The purpose of this study was to explore the association between obstetric history and urinary incontinence in a cohort of resistance-trained women.
Patients and Methods: This international, cross-sectional survey was completed by 1252 women competing in either powerlifting, weightlifting or CrossFit. The Incontinence Severity Index determined the severity of urinary incontinence.
Results: Almost 43% of the participants experienced urinary incontinence in the threemonths prior to the study. The prevalence of urinary incontinence in this cohort according to mode of birth were: caesarean 42.6%, unassisted vaginal 59.3%, vacuum extraction 58.8%, forceps 60.3%, vaginal and caesarean births 66.2%, forceps and vacuum extraction 73.1%. The prevalence of urinary incontinence in the subgroup of women who had undergone urogenital surgery was 63.6%. Kendall’s tau-b indicated that the correlation between ISI score and the number of births was strong and positive (τ = 0.25, p < 0.001).
Conclusion: Our results suggest that both the number of births and mode of birth influenced the likelihood of urinary incontinence in resistance-trained women. Women who had experienced only caesarean births had the lowest likelihood of urinary incontinence, while women who had experienced both vaginal and caesarean births had the most severe and second highest likelihood of urinary incontinence. Women who had undergone urogenital surgery continued to experience a high likelihood of urinary incontinence.
Keywords: strength training, resistance training, pelvic floor, pregnancy
Introduction
Urinary incontinence (UI) is a common pelvic floor disorder affecting between 25% and 45% of women.1 UI can negatively impact women’s quality of life2 and women who experience UI, especially moderate-to-severe UI, are less likely to participate in sport and exercise.3 Furthermore, some women athletes report that UI affects their athletic performance.4 The four main risk factors for UI include age, parity, mode of birth and BMI.1 The association between age, parity and BMI and UI in resistance-trained women has previously been investigated5–9 however, very little is known about the association between obstetric history and UI in resistance-trained women.
There are several important justifications for investigating the association between obstetric history and UI in resistance-trained women. Sports that incorporate resistance training such as CrossFit, weightlifting and powerlifting have become increasingly popular. The World Health Organisation recommends that adults engage in at least two sessions of muscle strengthening activities at a moderate or greater intensity a week10 and organisations, such as Healthy Bones Australia, recommend adults engage in a combination of resistance training, weight bearing impact loading and balance training.11 In contrast, organisations such as Continence Foundation of Australia raise concern, through their Pelvic Floor First initiative, that participating in some forms of resistance training, such as lifting or pressing heavy weights, deadlifts and wide legged or deep squats, should be avoided by many “at risk” women. The list of at risk women includes women who have recently or ever had a baby, menopausal or post-menopausal women, women who have undergone gynaecological surgery and elite athletes.12 This conflicting advice may be confusing for women as there is currently very little research regarding the effect of resistance training on the pelvic floor and UI or the association between obstetric history and UI in resistance-trained women.
Furthermore, informing women of their risk of pelvic floor disorders during childbirth supports their autonomy and right to an informed choice regarding care in pregnancy and childbirth.13 Even in acute and potentially critical circumstances, women require information about the possible risks when confronted with the need for instrumental intervention during the second stage of labour.14 In the case of competitive athletes, consideration should be given to the impact the birthing process may have on their sporting career or ability to continue to participate in their chosen sport at an elite level. It appears that this does not currently take place as there is sparce information available pertaining to the prevalence of UI in athletes according to mode of birth or previous urogenital surgery.
This study is one in a series of studies investigating the prevalence of UI and possible risk factors for UI in women who participate in powerlifting, weightlifting, or CrossFit at a competitive level.5–8 Previous studies investigated the association between age, BMI, parity and UI. This final study focuses on obstetric history, previous urogenital surgery, and UI. The main aim of this study, is to determine the likelihood of UI, athletic UI, and UI during training sets in resistance-trained women according to mode of birth or previous urogenital surgery and investigate the relationship between parity, mode of birth and UI.
Materials and Methods
Data for this study were collected through three cross-sectional surveys that examined the prevalence and risk factors for UI in powerlifters, weightlifters and CrossFit participants.6–8 The surveys utilised the Incontinence Severity Index (ISI); a validated tool to determine the frequency and severity of UI.15 UI was defined as an ISI score greater than zero. All women who had experienced leakage of urine, regardless of context, were considered incontinent when determining the lifetime prevalence of UI. Athletic incontinence was defined as UI during training or competition in otherwise continent women of any age or parity.6 All women, continent and incontinent, were included when determining the correlation between ISI score and possible risk factors. The selection of non-sport related risk factors was based on the four risk factors for UI identified by the International Continence Society as unambiguously associated with UI in young and middle-aged women: age, BMI, parity and mode of delivery.1 Sport-related risk factors were selected based on feedback obtained from the original pilot study.5 A definition for high repetition and heavy sets was not specified and is acknowledged to be sport and athlete specific.
Participants
Women powerlifters, weightlifters and CrossFit participants aged between 20 and 89 years who competed at either a local, national, or international level were eligible to participate. The surveys were prefaced by a research participant information sheet, which provided assurance that the questionnaire was anonymous, and participation was voluntary. Consent to participate was taken by proxy. In addition, participants were informed that they could withdraw from the studies before submitting their responses by closing the browser. Ethics approval was given for this project by the Charles Darwin University Human Research Ethics Committee, approval number H18106 and the study was conducted in accordance with the Declaration of Helsinki.
Procedure
An online survey tool (Qualtrics, Provo, Utah & Seattle, WA, USA) was used to collect data. The survey was circulated through Facebook and emailed to relevant associations, CrossFit boxes and gymnasiums located in English-speaking countries such as the United Kingdom, the United States of America, Australia, Canada, and New Zealand. Participants were recruited by two main methods. Firstly, a list of intermediates was generated by conducting a Google search for “English speaking countries” and combining the results from this search with the term, “powerlifting” or “weightlifting” or “CrossFit”. A recruitment email was then sent to the resulting list of contacts. The second method used Facebook to recruit participants. Facebook groups that were likely to contain competitive women powerlifters, weightlifters or CrossFit participants were identified, contacted, and asked to publish or email a link to the relevant survey. Paid advertisements targeted potential participants, who met the selection criteria, in English-speaking countries using a dedicated Facebook page.
Statistical Analysis
The data were analysed using SPSS 28.0 Inc., Chicago, IL. Central tendency and dispersion were reported as mean ± standard deviation (SD) and descriptive data were presented in percentages and the absolute numbers. The relationship between risk factors and ISI score was investigated using Kendall’s tau-b with the level of significance set at p≤0.05 for all analyses.
Results
All participants from the previous three studies6–8 were included in our analysis along with 129 additional participants previously deleted from the weightlifting study as they were thought to be powerlifters. In total, the cohort for this analysis consisted of 1252 participants made up of 609 powerlifters, 191 weightlifters and 452 CrossFit participants.
Participants of this study were competitive women powerlifters, weightlifters, and CrossFit competitors (Age: 35.75 ± 10.06 years and BMI: 26.73 ± 5.57 kg/m2). The women in this study had participated in some form of strength training for 5.86 ± 4.61 years and had been engaged in their chosen sport for 3.40 ± 2.60 years. Table 1 provides an overview of participant characteristics by continence status.
 |
Table 1 Participants’ Characteristics Stratified by Continence |
The results indicated that 47.2% (N=591) of participants in this study experienced UI at some point in their lifetime and 42.6% (N=533) had experienced UI in the three months prior to the study. Athletic incontinence had been experienced by 20.4% of the women (N=255). We found that 13.8% of the women (N=173) had been continent before commencing their chosen sport but now experienced UI in training or competition but not during everyday activities (Type 1 athletic incontinence). Furthermore, 6.5% of the women (N=82) were incontinent before commencing their chosen sport but are now continent during everyday activities while continuing to experience UI during training or competition (Type 2 athletic incontinence). A breakdown of the prevalence of UI, athletic UI, UI during high repetition sets and UI when wearing a belt, mean number of births and ISI score according to mode of birth, is presented in Table 2. Women who had delivered one child were divided into three groups according to their mode of birth and a breakdown of the prevalence of UI, athletic UI, UI during high repetition sets and UI when wearing a belt, and ISI score according to mode of birth, is provided in Table 3.
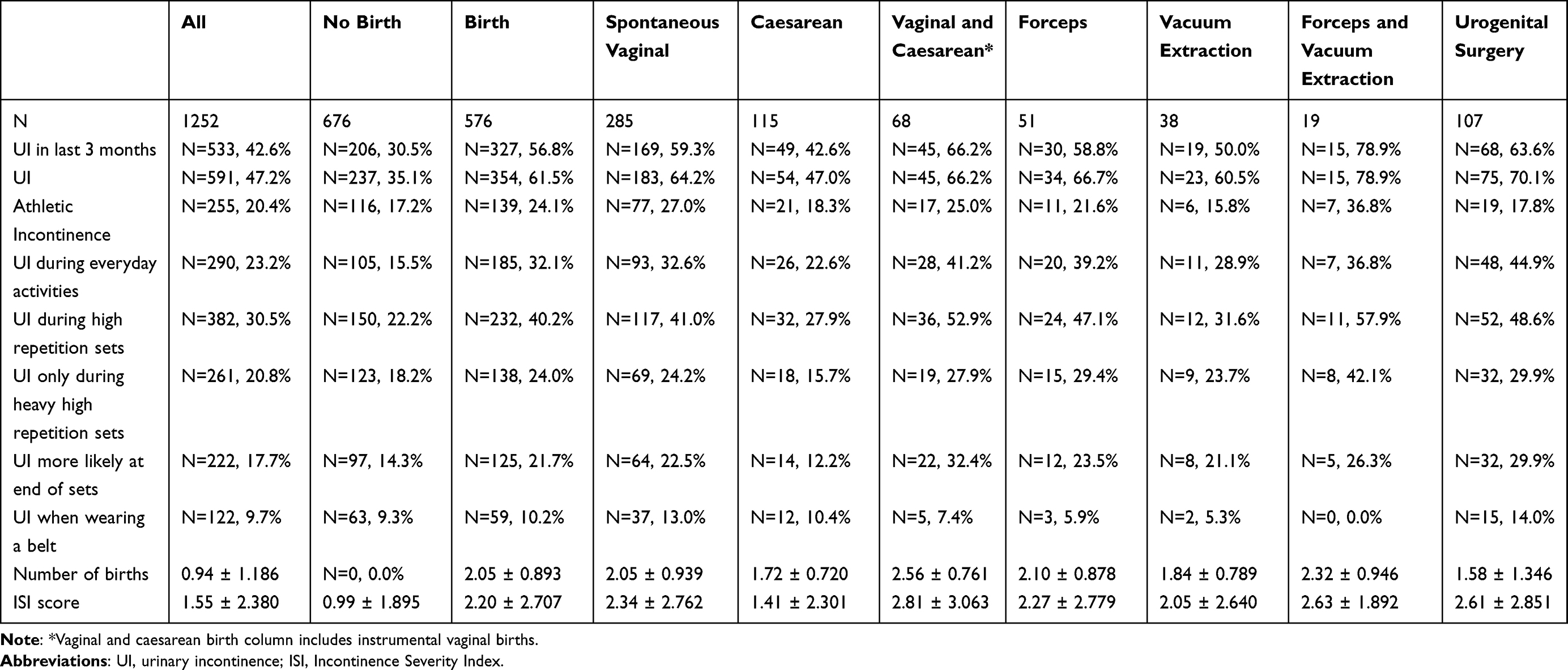 |
Table 2 Prevalence of Urinary and Athletic Incontinence, Triggers for Urinary Incontinence, Number of Births and ISI Scores in Resistance-Trained Women According to Having Given Birth or Not and Mode of Birth |
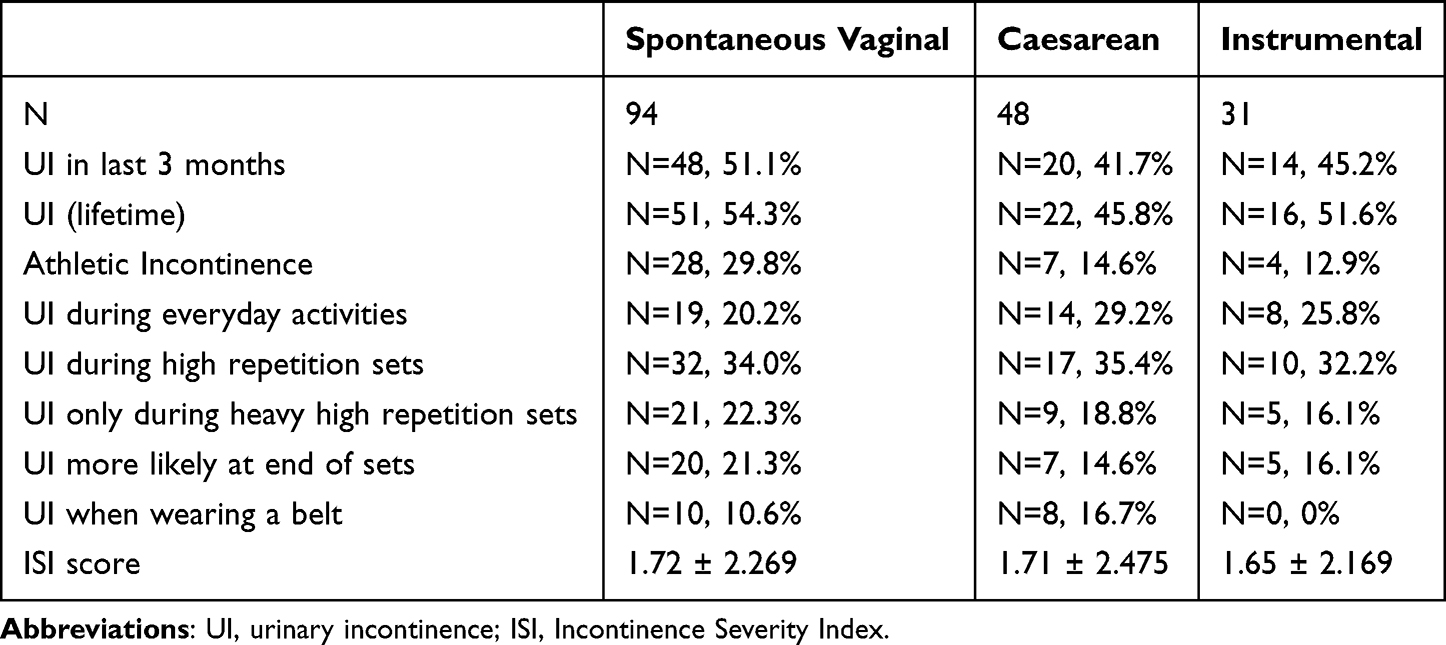 |
Table 3 Prevalence of Urinary and Athletic Incontinence, Triggers for Urinary Incontinence, and ISI Scores, According to Mode of Birth, in Resistance-Trained Women Who Have Only Experienced One Birth |
Kendall’s tau-b indicated that the correlation between ISI score and age (τ = 0.193, p < 0.001), number of births (τ = 0.252, p < 0.001), and BMI (τ = 0.080, p < 0.001) was strong and positive, two-tailed, N = 1252. There was no significant correlation between ISI score and years participating in their relevant sport or strength training.
Discussion
UI According to Obstetric History
Our results showed a difference in the likelihood of UI according to mode of birth. Women who had experienced both forceps and vacuum extraction assisted births were the most likely to have experienced UI at some point in their life (78.9%) and in the last 3 months (78.9%). Women who had experienced only caesarean births were the least likely to have experienced UI at some point in their life (47.0%) and were the least likely to have experienced UI in the 3 months prior to the study (42.6%). Women who had experienced only caesarean births were also the least likely to be incontinent during everyday activities (22.6%). There are minimal data available regarding the likelihood of UI according to mode of delivery in weightlifters and powerlifters. However, women CrossFit participants with a history of vaginal delivery have been found to be 2.1 times more likely to experience UI and 2.4 times more likely to experience UI during CrossFit.16
Our results also found that women who had a history of vaginal delivery were more likely to be incontinent than women who had given birth by caesarean. Caesarean birth has been found to have protective benefits in terms of pelvic floor function.17 In contrast, pelvic floor dysfunction disorders are significantly more common in women who give birth vaginally.18 Vaginal birth has been found to have a strong association with post-partum UI19,20 compared with elective caesarean birth.21 Women who have vaginal births are almost twice as likely to experience long-term stress UI22,23 and instrumental vaginal birth, compared to spontaneous vaginal birth, further increases the risk of stress UI.14,21 In addition to a pronounced reduction in vaginal resting pressure and pelvic floor muscle strength, women who deliver vaginally have less pelvic floor muscle endurance compared to women who deliver by caesarean birth.24 Elective caesarean birth therefore reduces the incidence of pelvic floor damage and dysfunction, such as pelvic organ prolapse and UI.
A meta-analysis has found that elective caesarean birth can reduce the incidence of UI, uterine prolapse and pelvic floor muscle damage.17 However, a retrospective cohort study found that there was only an advantage in performing a caesarean section in women with a history of caesarean births and, while caesarean births seemed to be followed by less postnatal UI than vaginal birth, this advantage disappeared with time and after a second caesarean birth.25 Caesarean birth has primarily been found to have a protective effect against pelvic floor disorders when performed before the woman reaches the second stage of labour.18,26
Theoretical and imaging studies reveal that women who have undergone the second stage of labour may have pelvic floor damage, even if they ultimately deliver via caesarean section.18 Once the woman reaches the second stage, the damage to pelvic floor structures has most likely already occurred and a caesarean birth will have minimal benefit.18 Women who have a spontaneous vaginal birth after a prolonged second stage also have significantly higher odds of reporting UI in the first three months postpartum compared to women whose labour is not prolonged. Operative vaginal birth, following a prolonged second stage, is also significantly more likely to increase the likelihood of UI than a spontaneous birth after a shorter second stage.26 While our results indicated that the prevalence of UI was greater in women who experience multiple instrumental births, it is not clear form our data if this is because of a prolonged second stage or the physical use of instruments to deliver the infant. A shortcoming of our study was that the length of participants' second stage of labour was not captured or investigated and consequently we were unable to determine if women, who experienced an unplanned caesarean birth or assisted vaginal birth, also experienced a long second stage of labour. It is strongly suggested that in future studies the length of the women’s second stage is recorded and analysed.
Mode of Birth, Sporting Activities and UI
Women who had experienced both forceps and vacuum extraction assisted births were most likely to have experienced athletic incontinence (36.8%). Experiencing leakage of urine during training and competition can be distracting for athletes and may indicate that they have surpassed their threshold of intrabdominal pressure and their individual harm/benefit ratio.27 Women who had experienced both forceps and vacuum extraction assisted births were most likely to experience UI during high repetition sets (57.9%), especially if the sets were heavy (42.1%). It is important to note, however, that the number of women in the forceps and vacuum assisted groups was low (N=19) and this may have impacted the results. Athletes who had experienced only caesarean births were the least likely to be incontinent during heavy high repetition sets (15.7%) and at the end of high repetition sets (12.2%). However, the difference between UI during high repetition or high repetition heavy sets was not as evident when only women who had experienced one birth were compared (Table 3). This finding suggests that while mode of birth may influence the prevalence of UI during athletic activity, parity is also likely to be a contributing factor.
Parity
Consequently, in addition to mode of birth, the total number of births a woman has experienced needs consideration. Previously, it was noted that women in the unassisted vaginal birth group were more likely to experience UI than the women who had only experienced caesarean births. However, women in the unassisted vaginal birth group had experienced, on average, more births (2.05 ± 0.939) than the women who had only experienced caesarean births (1.72 ± 0.720). To try and gauge the effect of parity on the prevalence of UI according to mode of birth, an analysis was carried out to determine the prevalence of lifetime UI in women who had only experienced one birth (Table 3) and the assumption that parity influenced the prevalence of UI was supported. Parity also had a strong positive correlation with ISI score (τ = 0.252, p < 0.001).
Repeated spontaneous vaginal births or instrumental births may also have a more detrimental effect on UI than repeated caesarean births. To investigate this possibility, we compared the lifetime prevalence of UI in women who had experienced one unassisted vaginal, caesarean, or instrumental birth with the corresponding prevalence found in the general cohort. Our results showed minimal difference in the prevalence of UI in women who had undergone caesarean birth (1.2 percentage points), a moderate difference for the vaginal birth group (9.9 percentage points) and the largest difference was noted in the instrumental birth group (15.1 percentage points). These results suggest that repeated vaginal or instrumental births may have a more detrimental effect on UI than multiple caesarean births. Considering the possible cumulative effect of parity and mode of birth, it was not surprising that the group of women who had the most severe UI (ISI 2.81 ± 3.063) and the second highest prevalence of UI in the last 3 months (66.2%) were the women who had experienced both vaginal and caesarean births as this group had experienced, on average, the greatest number of births (2.56 ± 0.761).
Urogenital Surgery
Women who had undergone urogenital surgery had the second highest lifetime prevalence of UI (70.1%), were the third most likely group to have been incontinent in the last three months (63.6%) and were the most likely group to experience UI during everyday activities (44.9%). Our study used the question: “have you had any urogenital (reproductive organs or urinary system) surgery?” It is acknowledged that the term did not differentiate between various types of surgery and may have incorporated surgeries unrelated to pelvic floor disorders or UI. Our results, however, indicated that women who had urogenital surgery continued to have a high prevalence of UI.
Limitations
There is reasonable evidence to claim that women who experience moderate-to-severe UI are less likely to participate in sport and exercise.3,28 However, we acknowledge that the objective evidence examining the effect of UI on athletic performance is less robust.4 Currently, there is not enough objective evidence indicating that athletic performance is affected by UI. Furthermore, while our findings provide information for women athletes contemplating motherhood during their athletic career, we recognise the importance of considering possible maternal complications and adverse effects for the child associated with electing a caesarean birth.18 Finally, the cross-sectional design of our study has some inherent, unavoidable biases and is unable to assign and investigate causation. The cross-sectional design meant that it was impossible to avoid potential survivor bias. Bias may have been further introduced through the recruitment of participants through social media and email. It is possible that women who were experiencing UI were more likely to reply to the email or online survey. The women also relied on recall when responding to the survey questions and therefore the data collected may not be as unbiased as data collected using an objective measurement.
Conclusion
Women need access to information specific to their own goals and circumstance when making choices relating to maternity care. Currently, there is minimal information available regarding mode of birth and the prevalence of UI in elite athletes. Our study provides descriptive information to help inform competitive athletes contemplating motherhood during their sporting careers. Additionally, our study informs midwives of the flow on effects a woman’s birth may have on UI during physical exercise later in life. Finally, our study increases the understanding of the relationship between parity, mode of birth and UI and provides information relevant to women athletes who are considering corrective surgery for the management of their UI.
Our results showed a difference in the prevalence of UI according to mode of birth. Women who had experienced only caesarean births had the lowest prevalence of UI and were the least likely to be incontinent during everyday activities and sporting activities such as high repetition sets. The assumption that parity influenced the prevalence of UI was supported and our results suggest that repeated spontaneous vaginal births or instrumental births may have a more detrimental effect on UI than repeated caesarean births. Finally, our results indicate that women who undergo urogenital surgery continue to have a high prevalence of UI.
Acknowledgments
The authors would like to thank all the intermediates who assisted with circulating the questionnaires for this study, especially Antony Lo and Mpho Ncube for advice given on the manuscript. Funding was provided for this study by Charles Darwin University.
Disclosure
MNK, NW and DG declare that they have no competing interests; LW is the secretary of a not-for-profit organisation, Darwin Powersports Incorporated. Darwin Powersports Incorporated promotes strength sports and conducts local powerlifting competitions.
References
1. Milsom I, Altman D, Cartwright R, et al. Committee 1 epidemiology of urinary incontinence and other lower urinary tract symptoms pelvic organ prolapse and anal incontinence. Epidemiology of urinary incontinence in women. In: Abrams P, Cardoso L, Wagg A, Wein A, editors. Incontinence.
2. Abrams P, Smith AP, Cotterill N. The impact of urinary incontinence on health-related quality of life (HRQoL) in a real-world population of women aged 45–60 years: results from a survey in France, Germany, the UK and the USA. BJU Int. 2015;115(1):143–152. doi:10.1111/bju.12852
3. Nygaard I, Girts T, Fultz N, Kinchen K, Pohl G, Sternfeld B. Is urinary incontinence a barrier to exercise in women? Obstet Gynecol. 2005;106(2):307–314. doi:10.1097/01.AOG.0000168455.39156.0f
4. Gram MCD, Bo K. High level rhythmic gymnasts and urinary incontinence: prevalence, risk factors, and influence on performance. Scand J Med Sci Sports. 2020;30(1):159–165. doi:10.1111/sms.13548
5. Wikander L, Cross D, Gahreman DE. Prevalence of urinary incontinence in women powerlifters: a pilot study. Int Urogynecol J. 2019;30(12):2031–2039. doi:10.1007/s00192-019-03870-8
6. Wikander L, Kirshbaum MN, Gahreman DE. Urinary incontinence and women CrossFit competitors. Int J Women Health. 2020;12:1189–1195. doi:10.2147/IJWH.S278222
7. Wikander L, Kirshbaum MN, Waheed N, Gahreman DE. Urinary incontinence in competitive women weightlifters. J Strength Cond Res. 2021. doi:10.1519/JSC.0000000000004052
8. Wikander L, Kirshbaum MN, Waheed N, Gahreman DE. Urinary incontinence in competitive women powerlifters: a cross-sectional survey. Sports Med Open. 2021;7(1):89. doi:10.1186/s40798-021-00387-7
9. Skaug KL, Engh ME, Frawlwy H, Bo K. Prevalence of pelvic floor dysfunction, bother and risk factors and knowledge of the pelvic floor muscles in Norwegian male and female powerlifters and Olympic weightlifters. J Strength Cond Res. 2020. doi:10.1519/JSC.0000000000003919
10. World Health Organisation. Physical activity; 2020. Available from: who.int/news-room/fact-sheets/detail/physical-activity.
11. Healthy Bones Australia. Exercise. Australia HB; 2021.
12. Pelvic Floor First. Promoting Pelvic Floor Safe Exercise Fitness Professional Resource. Continence Foundation of Australia; 2011.
13. Jelovsek JE, Chagin K, Gyhagen M, et al. Predicting risk of pelvic floor disorders 12 and 20 years after delivery. Am J Obstet Gynecol. 2018;218(2):
14. Nilsson I, Akervall S, Milsom I, Gyhagen M. Long-term effects of vacuum extraction on pelvic floor function: a cohort study in primipara. Int Urogynecol J. 2016;27(7):1051–1056. doi:10.1007/s00192-015-2928-x
15. Sandvik H, Espuna M, Hunskaar S. Validity of the incontinence severity index: comparison with pad-weighing tests. Int Urogynecol J Pelvic Floor Dysfunct. 2006;17(5):520–524. doi:10.1007/s00192-005-0060-z
16. Pisani GK, de Oliveira Sato T, Carvalho C. Pelvic floor dysfunctions and associated factors in female CrossFit practitioners: a cross-sectional study. Int Urogynecol J. 2021;32(11):2975–2984. doi:10.1007/s00192-020-04581-1
17. Yang XJ, Sun Y. Comparison of caesarean section and vaginal delivery for pelvic floor function of parturients: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2019;235:42–48. doi:10.1016/j.ejogrb.2019.02.003
18. Schwarzman P, Paz Levy D, Walfisch A, Sergienko R, Bernstein EH, Sheiner E. Pelvic floor disorders following different delivery modes-a population-based cohort analysis. Int Urogynecol J. 2020;31(3):505–511. doi:10.1007/s00192-019-04151-0
19. Siahkal SF, Iravani M, Mohaghegh Z, Sharifipour F, Zahedian M. Maternal, obstetrical and neonatal risk factors’ impact on female urinary incontinence: a systematic review. Int Urogynecol J. 2020;31(11):2205–2224. doi:10.1007/s00192-020-04442-x
20. van Brummen HJ, Bruinse HW, van de Pol G, Heintz AP, van der Vaart CH. The effect of vaginal and cesarean delivery on lower urinary tract symptoms: what makes the difference? Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(2):133–139. doi:10.1007/s00192-006-0119-5
21. Kokabi R, Yazdanpanah D. Effects of delivery mode and sociodemographic factors on postpartum stress urinary incontinency in primipara women: a prospective cohort study. J Chin Medl Assoc. 2017;80:498–502. doi:10.1016/j.jcma.2016.06.008
22. Tahtinen RM, Cartwright R, Tsui JF, et al. Long-term impact of mode of delivery on stress urinary incontinence and urgency urinary incontinence: a systematic review and meta-analysis. Eur Urol. 2016;70(1):148–158. doi:10.1016/j.eururo.2016.01.037
23. Thom DH, Rortveit G. Prevalence of postpartum urinary incontinence: a systematic review. Acta Obstet Gynecol Scand. 2010;89(12):1511–1522. doi:10.3109/00016349.2010.526188
24. Hilde G, Staer-Jensen J, Siafarikas F, Engh ME, Braekken IH, Bo K. Impact of childbirth and mode of delivery on vaginal resting pressure and on pelvic floor muscle strength and endurance. Am J Obstet Gynecol. 2013;208(1):e51–e57. doi:10.1016/j.ajog.2012.10.878
25. Cerruto MA, D’Elia C, Aloisi A, Fabrello M, Artibani W. Prevalence, incidence and obstetric factors’ impact on female urinary incontinence in Europe: a systematic review. Urol Int. 2013;90(1):1–9. doi:10.1159/000339929
26. Brown SJ, Gartland D, Donath S, MacArthur C. Effects of prolonged second stage, method of birth, timing of caesarean section and other obstetric risk factors on postnatal urinary incontinence: an Australian nulliparous cohort study. BJOG. 2011;118(8):991–1000. doi:10.1111/j.1471-0528.2011.02928.x
27. Bo K, Nygaard IE. Is physical activity good or bad for the female pelvic floor? A narrative review. Sports Med. 2020;50(3):471–484. doi:10.1007/s40279-019-01243-1
28. Brennand E, Ruiz-Mirazo E, Tang S, Kim-Fine S; Calgary Women’s Pelvic Health Research G. Urinary leakage during exercise: problematic activities, adaptive behaviors, and interest in treatment for physically active Canadian women. Int Urogynecol J. 2018;29(4):497–503. doi:10.1007/s00192-017-3409-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Therapeutic Exercise Progression in Patients with Nonspecific Low Back Pain: A Systematic Review
Tuninetti A, Barbari V, Storari L, Bisconti M, Piano L, Dunning J, Mourad F, Maselli F
Journal of Pain Research 2025, 18:6397-6407
Published Date: 29 November 2025