Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Association Between Neck-to-Limb Length Ratio and Cardiovascular Events in a Chinese Population
Authors Li X, Hu T, Xu Y, Lu X, Su Y, Xiao Y, Wang Y, Ma X, Bao Y ![]()
Received 14 June 2025
Accepted for publication 31 July 2025
Published 13 August 2025 Volume 2025:18 Pages 2863—2872
DOI https://doi.org/10.2147/DMSO.S543163
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Donald McClain
Xiaoya Li,1,* Tingting Hu,1,* Yiting Xu,1,* Xuhong Lu,1 Yingying Su,1 Yunfeng Xiao,2 Yufei Wang,1 Xiaojing Ma,1 Yuqian Bao1
1Department of Endocrinology and Metabolism, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai Clinical Center for Diabetes, Shanghai Diabetes Institute, Shanghai Key Laboratory of Diabetes Mellitus, Shanghai, 200233, People’s Republic of China; 2Department of Radiology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, 200233, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuqian Bao, Department of Endocrinology and Metabolism, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai Diabetes Institute, 600 Yishan Road, Shanghai, 200233, People’s Republic of China, Tel +86-21-64369181, Fax +86-21-64368031, Email [email protected] Xiaojing Ma, Department of Endocrinology and Metabolism, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai Diabetes Institute, 600 Yishan Road, Shanghai, 200233, People’s Republic of China, Tel +86-21-64369181, Fax +86-21-64368031, Email [email protected]
Aim: Obesity contributes to cardiovascular (CV) events. This study aimed to identify the most effective anthropometric indicators that add predictive value to body mass index (BMI) for subsequent CV events in individuals without carotid plaques, improving early risk stratification in subclinical populations.
Methods: This longitudinal study enrolled 1043 participants from a community-based cohort in Shanghai (2013– 2014) and followed them for CV events through 2021– 2022. The CV events included ischemic heart disease (myocardial infarction, unstable angina pectoris, hospitalization for heart failure, and coronary revascularization), ischemic stroke, and CV death. Carotid plaque was excluded via ultrasound. Visceral fat area (VFA) was assessed using magnetic resonance imaging. The neck circumference (NC), neck-to-height ratio (NHtR), waist-to-height ratio (WHtR), waist-to-hip ratio (WHR), neck-to-limb length ratio (NLR), and waist-to-limb length ratios (WLR) were calculated.
Results: Multivariable linear regression analysis revealed a significant positive correlation between various obesity-related indices (BMI, waist circumference, NC, NHtR, WHtR, WHR, NLR, and WLR) and VFA (all P < 0.001). Over a mean follow-up period of 7.6 years, 97 CV events (9.3%) were recorded. Cox proportional hazards regression demonstrated that elevated NLR was significantly associated with an increased CV risk with hazard ratios of 1.28 (95% confidence interval [CI]: 1.08– 1.52). Notably, the NLR significantly improved the predictive capacity of CV events (C-statistic, 0.671 [95% CI: 0.616– 0.726], P = 0.002; NRI, 0.090 [95% CI: 0.003– 0.177], P < 0.001; IDI, 0.007 [95% CI: 0.000– 0.019], P < 0.001).
Conclusion: NLR was correlated with visceral fat content, and significantly enhanced the predictive value of BMI for CV risk in individuals without baseline carotid plaque. These findings support their use in routine clinical assessment to enhance early prevention efforts.
Keywords: obesity, cardiovascular disorder, body mass index, visceral fat, neck-to-height ratio, neck-to-limb length ratio
Introduction
Cardiovascular diseases (CVD) are the leading causes of death among noncommunicable diseases worldwide and account for approximately one-third of all fatalities.1 A substantial body of clinical and epidemiological research has established obesity as a major contributing factor to the incidence of CVD.2 The prevalence of obesity is increasing at an unprecedented rate, with recent projections from the World Obesity Federation indicating that approximately 3.3 billion adults may be classified as overweight or obese by 2035.3 This trend poses considerable challenges to individuals, societies, and healthcare systems worldwide.
Obesity is characterized by excessive accumulation of adipose tissue. Visceral fat, which is located around the abdominal organs within the mesentery and omentum, is of particular concern. Visceral fat is metabolically active and plays a critical role in endocrine regulation, metabolism, and the immune response. During the progression of obesity, visceral fat secretes free fatty acids (FFAs), glycerol, and a range of proinflammatory and profibrotic cytokines into the portal circulation.4 Dysfunctional visceral fat is recognized as a key etiological factor in the development of CVD, contributing to CV risk independently of total body fat.5,6 Given the strong link between visceral adiposity and CVD, the accurate assessment of visceral fat accumulation is crucial for effective risk stratification.
Obesity diagnosis in medicine primarily relies on body mass index (BMI), which can lead to misdiagnosis and negative consequences for both patients and society. Recent clinical guidelines suggest combining BMI with body fat measurements to improve obesity detection and reduce misclassification risk.7 Visceral fat area (VFA) is primarily measured using advanced imaging techniques such as magnetic resonance imaging (MRI) or computed tomography. Although these methods provide a precise evaluation of visceral fat, they are costly and not widely accessible in routine clinical and public health settings. This limitation underscores the need for practical and reliable surrogate markers of visceral adiposity that can be used in diverse healthcare settings.
Anthropometric indicators such as neck circumference (NC), neck-to-height ratio (NHtR), waist-to-height ratio (WHtR), waist-to-hip ratio (WHR), neck-to-limb length ratio (NLR), and waist-to-limb length ratio (WLR) are inexpensive and accessible alternatives for estimating visceral fat and assessing cardiovascular events risk.8–10 These indicators have been shown to correlate reasonably well with measures of adiposity and are simple to obtain in clinical practice, making them useful tools for large-scale population studies and routine screenings. Among them, NC primarily reflects upper-body subcutaneous adipose tissue (SAT), as visceral fat is absent in the neck region.11 Anatomically, neck adipose tissue (NAT) includes both superficial (subcutaneous and subplatysmal) and deeper ectopic fat depots (eg, perivascular, prevertebral), especially in obesity.12 These deeper depots are associated with adipose dysfunction, characterized by increased inflammation, dysregulated lipid metabolism, and elevated postprandial non-esterified fatty acids release—all of which contribute to insulin resistance and atherosclerosis.13 Importantly, NAT surrounding the carotid artery exhibits heightened inflammatory gene expression in individuals with carotid stenosis, suggesting a local pro-inflammatory environment.14 Given its anatomical proximity to the vasculature, NAT also influence vascular function through adipokine and vasoactive mediator secretion, consistent with observed associations between NC and arterial stiffness or carotid intima-media thickness.11 Collectively, these findings support the biological plausibility of NC-based indices as markers of cardiometabolic risk and underscore the need for their further investigation in longitudinal studies.
The present study aimed to evaluate the predictive value of NC-related anthropometric indicators for incident CVD in a Chinese cohort. Notably, we focused on a subgroup of participants without baseline carotid plaques. This subgroup analysis represents a novel aspect of our work and provides important insights into early CV risk stratification, which has been underexplored in previous studies.
Methods
Study Design and Population
In this longitudinal study, participants were enrolled from four communities in Shanghai and underwent a baseline data collection, including standardized questionnaires, comprehensive physical examinations, and body composition measurement between 2013 and 2014.15 After excluding those with malignant tumors, severe hepatic and renal dysfunction, receiving steroid or replacement therapy, or missing data, 1707 participants were followed up via telephone interviews and electronic health records between 2021 and 2022. Finally, 1043 (583 male, 43.3%) participants without baseline carotid plaques were included in the analysis after excluding those lost to follow-up (n=336) and those who died due to non-CV events (n=31).
Baseline Data Collection
Data on demographic characteristics, medical history, family history, therapeutic agent use, and lifestyle were collected by trained technicians using a standardized questionnaire. Current smokers were defined as those who smoked at least one cigarette daily for at least 6 months.16 Alcohol use was defined as alcohol consumption at least once a week in the past 6 months. Physical activity was classified as light, moderate, and vigorous.17 A food frequency questionnaire was used to collect data on habitual dietary intake. The diet quality score was defined based on five dietary behaviors. Each dietary behavior was scored as 1 for healthy and 0 otherwise, and individual component scores were summed to obtain a dietary quality score ranging from 0 to 5, with a higher score indicating a healthier diet.18
Anthropometric and Visceral Fat Area Measurement
Anthropometric indicators including height, body weight, NC, NHtR, WHtR, WHR, NLR, and WLR were measured and calculated according to a standardized protocol. NC assessment occurred with participants standing and their heads in a horizontal plane. The tape’s upper edge was placed inferior to the thyroid cartilage protrusion, aligned perpendicularly to the neck’s longitudinal axis to avoid compressing the skin, and the NC measurement was documented. BMI was calculated as weight in kilograms divided by the squared height in meters. Blood pressure was assessed three times using a calibrated mercury sphygmomanometer after a 10-min rest. The average systolic and diastolic blood pressures (SBP and DBP, respectively) of the three readings were used for subsequent analysis.
VFA was assessed using a 3.0 T clinical MRI scanner (Archiva, Philips Medical System, Amsterdam, The Netherlands), equipped with the abdominal coil. Scans were acquired at the abdominal level spanning the L4-L5 vertebrae with participants in the supine position. Two trained observers performed segmentation of the images into VFA using SLICE-O-MATIC image analysis software (version 4.2; Tomovision Inc., Montreal, QC, Canada). In cases where results differed by >10%, a third observer blinded to the initial results reanalyzed the images.19
Laboratory Measurements
Blood samples were drawn after an overnight fast of at least 10 h for laboratory tests according to a standardized protocol,15 including triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting plasma glucose (FPG), fasting insulin (FINS), and hemoglobin A1c (HbA1c). Participants with no history of diabetes underwent a 75-g oral glucose tolerance test, and those with a history of diabetes received 100-g of steamed bread meal to measure the 2 h plasma glucose (2hPG). The homeostatic model assessment of insulin resistance (HOMA-IR) was calculated as [FINS (mU/L) × FPG (mmol/L)] /22.5.
Carotid Ultrasonography
All participants underwent carotid ultrasonography using a high-resolution B-mode ultrasonographic device (VOLUSON 730, EXPERT, GE, USA). Carotid plaque was defined as a focal wall thickness of the common carotid artery ≥ 1.5 mm or more than 50% thicker than the adjacent wall.20
Outcomes
The primary endpoints were CV events including ischemic heart disease (myocardial infarction, unstable angina pectoris, hospitalization for heart failure, and coronary revascularization), ischemic stroke, or death due to CV events. Information on the clinical outcomes was collected via telephone interviews between 2021 and 2022. Subsequently, event information was confirmed using electronic health records, coded by two trained physicians, and classified using the International Classification of Diseases (ICD-10) codes (CV events: I00-I99). Self-reported events and electronic records showed great consistency, with a sensitivity of 96.7% and a specificity of 99.8%.
Definitions
Hypertension was defined according to the 2020 guidelines of the International Society of Hypertension as SBP ≥ 140 mmHg, DBP ≥ 90 mmHg, and/or current use of antihypertensive medication.21 Diabetes was diagnosed based on the 2023 American Diabetes Association criteria.22 Dyslipidemia was defined according to the 2024 Guidelines for the Management of Dyslipidemia in Adults.23
Statistical Analysis
All the variables were subjected to normality tests. Normally distributed variables are shown as mean ± standard deviation, and skewed variables are presented as medians with interquartile ranges (25% and 75%). The Student’s t-test or Wilcoxon signed-rank test was used to compare normally distributed and non-normally distributed variables, respectively. The chi-squared test was used for comparison between groups of categorical variables.
Linear regression analysis was used to explore the association between the obesity indicators and VFA. The model was adjusted for age and sex. All baseline variables were included as candidates in the LASSO-Cox model. By applying the least absolute shrinkage and selection operator (LASSO) algorithm, the most important variables (lambda.min) for identifying cardiovascular events in individuals without carotid plagues were determined. Cox regression analysis was performed to analyze the association between anthropometric indicators and CV events adjusted for selected confounding factors. In addition, the incremental predictive values of NC, hip circumference (HC), NHtR, WHtR, WHR, NLR, and WLR beyond BMI for CV events were evaluated using C-statistics, integrated discrimination improvement (IDI) and net reclassification improvement (NRI). All analyses were conducted using R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria), and a two-tailed P < 0.05 was considered statistically significant.
Results
Baseline Characteristics
In total, 1043 participants, aged 50–80 years, without baseline carotid plaques were analyzed. During a mean follow-up of 7.6 years, 97 CV events were identified, of which 40 were due to ischemic heart disease, 52 were due to stroke, and 5 were due to cardiovascular death. The baseline characteristics of the study participants, including the non-CV (n=946) and CV (n=97) event groups, are detailed in Table 1. Compared with the non-CV event group, the CV event group showed a higher percentage of males and older age and had a higher incidence of diabetes and hypertension. Moreover, participants who developed CV events had higher baseline VFA, waist circumference (WC), NC, HC, NHtR, WHtR, WHR, NLR, WLR, SBP, DBP, FPG, 2hPG, HbA1c, FINS, HOMA-IR, and TG (all P < 0.05). There were no significant differences in the proportions of smoking, alcohol use, physical activity, diet quality score, family history of CVD, or dyslipidemia between the two groups (P > 0.05).
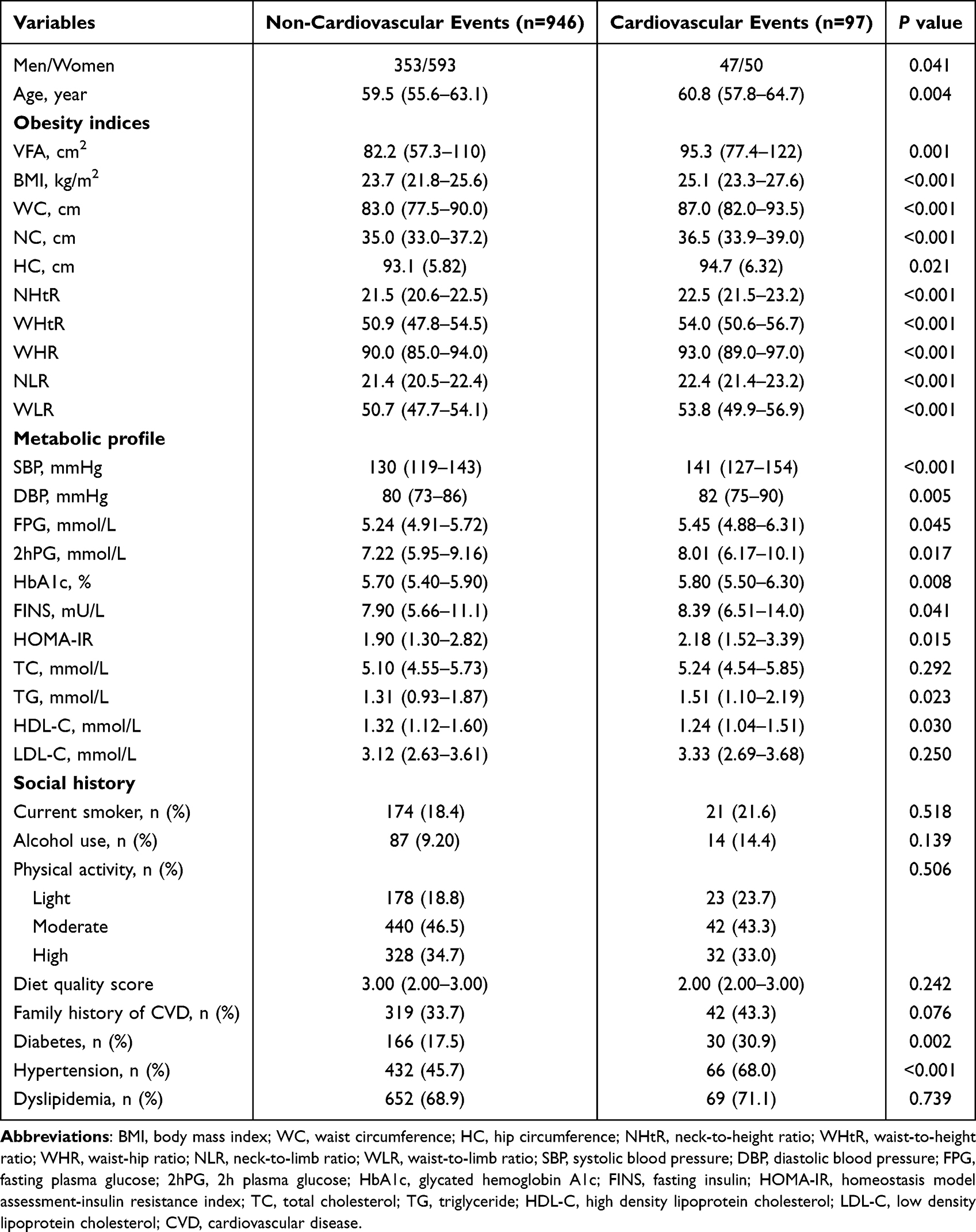 |
Table 1 Baseline Characteristics of Study Participants According to the Incidence of Cardiovascular Events |
Anthropometric Indicators of Adiposity and VFA
Table 2 shows the relationships between BMI, WC, NC, NHtR, WHtR, WHR, NLR, WLR, and VFA. After adjusting for age and sex, linear regression analysis revealed a positive correlation between the anthropometric indicators (BMI, WC, NC, NHtR, WHtR, WHR, NLR, and WLR) and VFA (all P < 0.001).
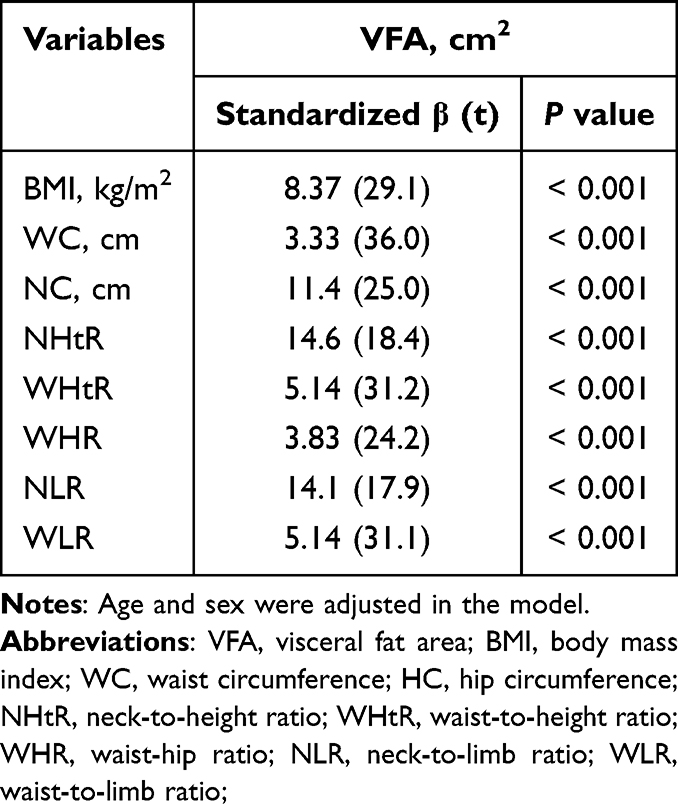 |
Table 2 Multivariable Linear Regression Analysis for the Associations Between Obesity Indices and Visceral Fat Area |
Baseline Anthropometric Indicators and CV Events in Participants Without Carotid Plaque
Table 3 shows that increased WC, NC, NHtR, WHtR, WHR, NLR, and WLR were positively associated with the risk of CV events in participants without baseline carotid plaques (all P < 0.05). Using a Lasso-Cox regression model to account for potential multicollinearity and confounding factors (Figure 1), we found that the associations between NLR and cardiovascular events risk in participants without baseline carotid plaques remained robust and statistically significant.
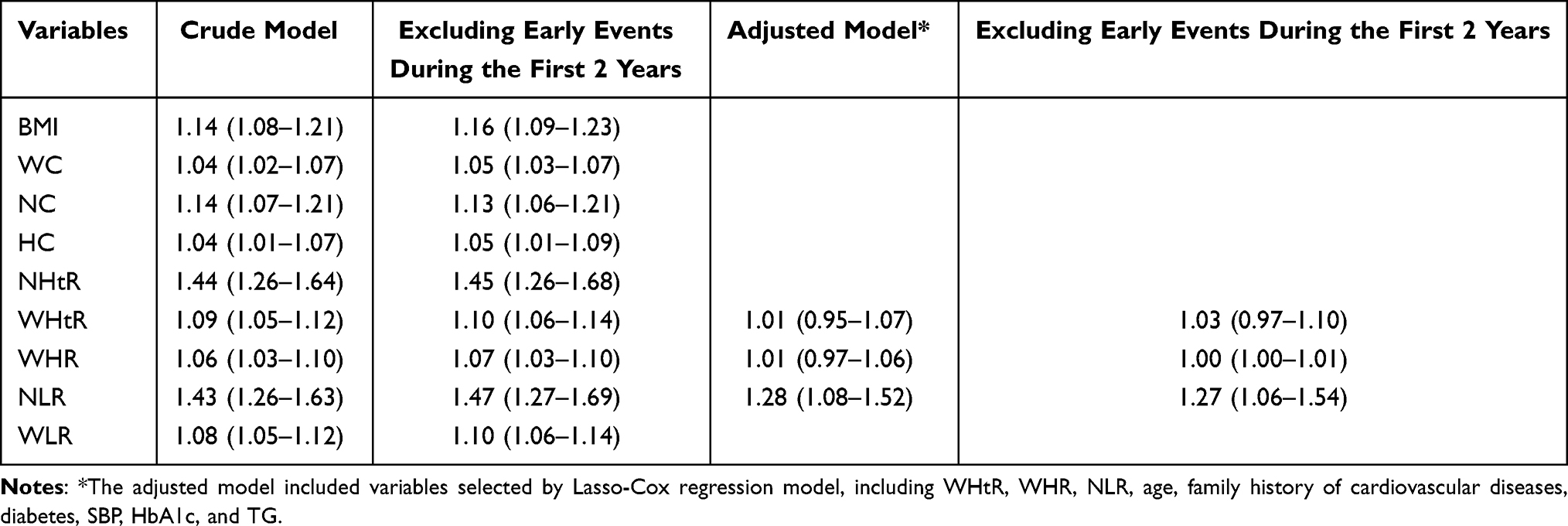 |
Table 3 The Association Between Baseline Anthropometric Indicators and Cardiovascular Events in Participants Without Baseline Carotid Plaque |
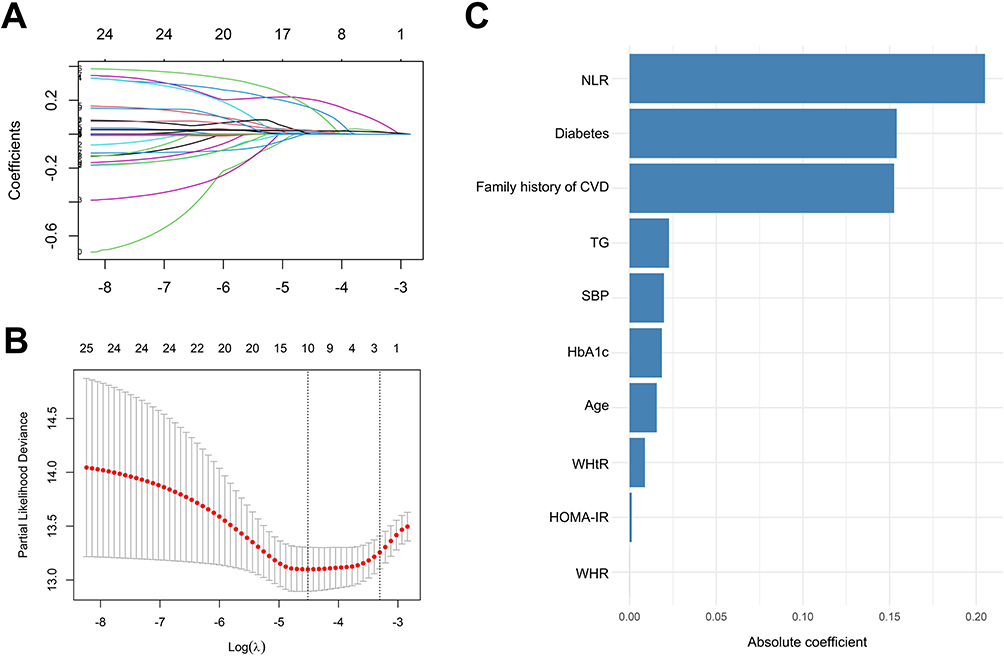 |
Figure 1 LASSO-Cox model of all baseline variables. (A) LASSO regression coefficient plot; (B) Cross-validation error plot; (C) Variable importance. |
NLR Enhances Predictive Accuracy for CV Events Beyond BMI
Furthermore, to evaluate the discriminatory ability of the models, we calculated the C-statistic and further assessed model improvement using IDI and NRI. NLR improved the discriminative performance (C-statistic 0.671, 95% CI 0.616–0.726, P = 0.002) and exerted excess improvement in the estimated NRI (0.090, 95% 0.003–0.177, P < 0.001) and IDI (0.007, 95% CI 0.000–0.019, P < 0.001) as well (Table 4).
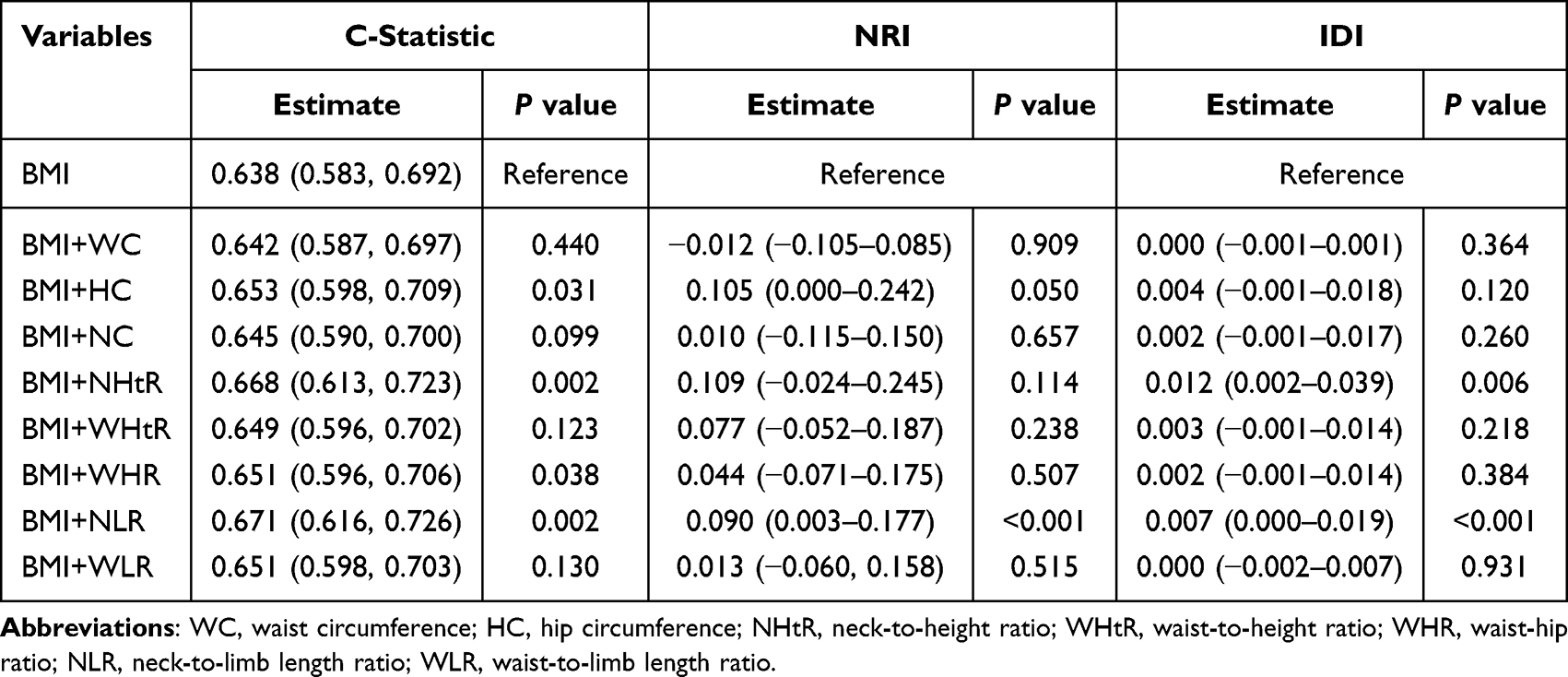 |
Table 4 Comparison of the Predictive Performance for Cardiovascular Events Among Obesity Indices in Participants Without Carotid Plaque |
Discussion
To the best of our knowledge, this is the first study to demonstrate that, over a mean follow-up of 7.6 years, NC-adjusted indices, particularly the NHtR and NLR, significantly enhanced the predictive value of BMI for CV events in participants without carotid plaque. By demonstrating that NLR improved CVD risk prediction beyond BMI in a subclinical population free of overt atherosclerosis, this study addresses a critical gap in early risk stratification. Our findings highlight the potential of these simple and accessible indices for early detection and intervention in this overlooked group. Given their practicality, these indices may serve as valuable tools for enhancing CVD risk stratification in primary prevention settings.
Considering the high mortality rate associated with CVD, it is essential to conduct an in-depth investigation of its risk factors. In this study, the CV event group had a higher percentage of older adults and male and demonstrated a higher prevalence of diabetes and hypertension than the non-CV event group. These findings align with the established risk factors for CVD, including age, sex, and metabolic disorders, all of which are well-documented contributors to CV morbidity and mortality.24 Since VFA has been widely recognized as an independent cardiovascular events risk factor, we further explored the associations between various anthropometric measures and VFA. The positive correlation observed between VFA and several anthropometric measurements underscores the potential of these parameters as proxies for visceral fat accumulation. This is particularly valuable in clinical settings where imaging modalities such as MRI, which directly measures VFA, may not be readily available.
Our findings align with current 2019 ACC/AHA guideline25 and 2021 ESC guidelines26 that emphasize obesity screening for CVD prevention but extend their clinical utility by demonstrating that NLR improves risk prediction beyond BMI. These simple, reproducible measures better reflect visceral fat distribution and remained predictive even in individuals without carotid plaque. Incorporating such indices into routine assessments could enhance early risk stratification, supporting more refined and proactive primary prevention strategies.
Neck fat accumulation is a proxy for upper-body subcutaneous fat and is estimated by measuring the NC at the level of the laryngeal prominence.27 Prior studies established NC as a simple and effective tool to estimate CV events risk, positively correlating with VAT, insulin resistance, and metabolic syndrome, especially in women.28,29 A prospective cohort study demonstrated that the number of CV event risk factors in participants increased from 2.6, 3.0, and 3.4 to 3.5, 4.1, and 4.7 in the low-, medium-, and high-NC cohorts, respectively, compared with baseline in a high-risk population.30 Building on this, NLR integrates NC with limb length, potentially capturing central fat accumulation, stature, and muscle mass. The relationship between the NHtR, NLR, and VFA was particularly strong, suggesting that this novel ratio could reflect central adiposity and its associated metabolic disturbances. This association may be due to the anatomical and physiological implications of upper limb length relative to NC, possibly capturing a distribution of body fat that is metabolically unfavorable.
Our previous study demonstrated that NC predicts CV risk in middle-aged and older adults, especially in men.31 In the present study, we further adjusted NC for height and limb length, and found that the normalized indices, remained significant predictors of CV events. Importantly, their predictive utility persisted in individuals without baseline carotid plaque, reinforcing their value in early risk detection before overt structural vascular changes occur.
The results of the multivariable analyses and predictive performance analyses underscore the inadequacy of BMI as a standalone measure of CV risk, as it does not account for fat distribution or differentiate between lean and fat mass.32 Conversely, NC is closely related to central adiposity, reflecting the distribution of fat around the neck and upper body.33,34 By incorporating neck circumference and upper limb length, the NHtR and NLR may offer insights into central fat accumulation and associated metabolic disturbances.
Several studies have emphasized the association between central obesity and increased CV risk,35 highlighting the need for indicators that better capture visceral fat distribution. The strong correlation between NLR and VFA suggests that NLR could serve as a surrogate marker for visceral adiposity, a hypothesis supported by recent research that has validated the association between NC and insulin resistance, hypertension, and dyslipidemia, all of which are key components of metabolic syndrome. In terms of the mechanism, upper-body subcutaneous and visceral fat accounts for most of systemic FFA release under basal and insulin-suppressed conditions.20,35 They exacerbate endothelial dysfunction, promote thrombosis, and impair vascular function, thereby contributing to the pathophysiology of CVD.36 This makes NC-related indices practical and effective tools for clinical and public health settings, where advanced imaging techniques are not always available.
This study involved a cohort of 1043 participants with a mean follow-up of 7.6 years, providing robust longitudinal data. The NHtR and NLR can be incorporated into routine clinical assessments to enhance the early detection of CV risk, particularly in individuals who may not exhibit traditional markers of CVD, such as carotid plaques. Comprehensive baseline data collection allowed the control of potential confounding factors, thereby enhancing the validity of the results. However, this study had several limitations. First, its single-center design raises concerns about the potential for selection bias. By focusing solely on a single center, the sample population may not adequately represent broader demographic diversity and variability in healthcare practices. Second, the absence of neck adiposity measurements precludes the inclusion of more nuanced indicators for the prognostication of CV events. Although we adjusted for multiple cardiometabolic risk factors, residual confounding cannot be fully excluded.
Further research is warranted to validate the predictive value of NC-corrected indicators in diverse populations and explore the underlying mechanisms. It is possible that the NLR captures elements of body fat distribution, muscle mass, and possibly inflammatory status that are not adequately reflected in traditional metrics. Understanding these mechanisms may inform targeted interventions aimed at reducing central adiposity and its associated risks.
Conclusions
In summary, this longitudinal cohort study highlights the importance of using alternative anthropometric indicators, particularly NLR, to predict CV risk in individuals without overt carotid atherosclerosis. These findings support the integration of NC-related indices into routine clinical evaluation to enhance early cardiovascular events risk stratification and guide preventive strategies. Moreover, further external validation is warranted before these measures can be widely recommended for routine clinical use.
Abbreviations
2hPG, 2 h plasma glucose; BMI, body mass index; CI, confidence interval; CV, cardiovascular; CVD, cardiovascular disease; DBP, diastolic blood pressure; FFA, free fatty acid; FINS, fasting insulin; FPG, fasting plasma glucose; HbA1c, hemoglobin A1c; HC, hip circumference; HDL-C, high-density lipoprotein cholesterol; HOMA-TR, homeostatic model assessment of insulin resistance; LDL-C, low-density lipoprotein cholesterol; MRI, magnetic resonance imaging; NC, neck circumference; SBP, systolic blood pressure; TC, total cholesterol; TG, triglyceride; VFA, visceral fat area; NHtR, neck-to-height ratio; NLR, neck-to-limb length ratio; WHR, waist-to-hip ratio; WHtR, waist-to-height ratio; WLR, waist-to-limb length ratio.
Data Sharing Statement
The data that support the findings of this study are not publicly available due to privacy restrictions but are available from the corresponding author upon reasonable request.
Statement of Ethics
This study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all study participants. The study protocol was approved by the Ethics Committee of Shanghai Sixth People’s Hospital affiliated Shanghai Jiao Tong University School of Medicine (approved number: 2023-KY-132[K]).
Acknowledgments
We would like to thank all the involved clinicians, nurses, and technicians for helping with the study. We are grateful to all participants for their dedication to data collection and laboratory measurements.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by National Natural Science Foundation of China (82400999), China Postdoctoral Science Foundation (2024M762052), Shanghai Research Center for Endocrine and Metabolic Diseases (2022ZZ01002), National Key Clinical Specialty (Z155080000004), Clinical Research Project of Health Industry of Shanghai Municipal Health Commission (20224Y0155), and Shanghai Rising Star of Medical Talent’ Youth Development Program (YYXX202302).
Disclosure
The abstract of this paper was presented at the American Diabetes Association® 85th Scientific Sessions as a poster presentation (432-P). The poster’s abstract was published in Diabetes. 2025; Volume 74, Issue Supplement_1: https://diabetesjournals.org/diabetes/article/74/Supplement_1/432-P/160327/432-P-Association-between-Neck-to-Limb-Length-and. The authors report no competing interests in this work.
References
1. Magnussen C, Ojeda FM, Leong DP, et al. Global effect of modifiable risk factors on cardiovascular disease and mortality. N Engl J Med. 2023;389(14):1273–1285.
2. Koliaki C, Liatis S, Kokkinos A. Obesity and cardiovascular disease: revisiting an old relationship. Metabolism. 2019;92:98–107. doi:10.1016/j.metabol.2018.10.011
3. Federation W O. Obesity Atlas 2024. 2024. Available from: https://data.worldobesity.org/publications/?cat=22.
4. Ibrahim MM. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev. 2010;11(1):11–18. doi:10.1111/j.1467-789X.2009.00623.x
5. t m P-W, Poirier P, Burke LE, et al. Obesity and cardiovascular disease: a scientific statement from the American heart association. Circulation. 2021;143(21):e984–e1010. doi:10.1161/CIR.0000000000000973
6. Kim MS, Kim WJ, Khera AV, et al. Association between adiposity and cardiovascular outcomes: an umbrella review and meta-analysis of observational and Mendelian randomization studies. Eur Heart J. 2021;42(34):3388–3403. doi:10.1093/eurheartj/ehab454
7. Rubino F, Cummings DE, Eckel RH, et al. Definition and diagnostic criteria of clinical obesity. Lancet Diabetes Endocrinol. 2025;13(3):221–262. doi:10.1016/S2213-8587(24)00316-4
8. Yang X, Chen S, Zhou Z, et al. Neck-to-height ratio and arterial stiffness in Chinese adults: cross-sectional associations in a community-based cohort. J Hypertens. 2021;39(6):1195–1202. doi:10.1097/HJH.0000000000002751
9. Taxová Braunerová R, Kunešová M, Heinen MM, et al. Waist circumference and waist-to-height ratio in 7-year-old children-WHO childhood obesity surveillance initiative. Obes Rev. 2021;22(6):e13208. doi:10.1111/obr.13208
10. Zhou B, Bennett JE, Wickham AP, et al. General and abdominal adiposity and hypertension in eight world regions: a pooled analysis of 837 population-based studies with 7·5 million participants. Lancet. 2024;404(10455):851–863. doi:10.1016/S0140-6736(24)01405-3
11. Cresswell E, Basty N, Atabaki Pasdar N, et al. The value of neck adipose tissue as a predictor for metabolic risk in health and type 2 diabetes. Biochem Pharmacol. 2024;223:116–171. doi:10.1016/j.bcp.2024.116171
12. Pandzic Jaksic V, Grizelj D, Livun A, et al. Neck adipose tissue - tying ties in metabolic disorders. Horm Mol Biol Clin Investig. 2018;33(2). doi:10.1515/hmbci-2017-0075
13. Arias-Tellez MJ, Acosta FM, Garcia-Rivero Y, et al. Neck adipose tissue accumulation is associated with higher overall and central adiposity, a higher cardiometabolic risk, and a pro-inflammatory profile in young adults. Int J Obes Lond. 2021;45(4):733–745. doi:10.1038/s41366-020-00701-5
14. Pandzic Jaksic V, Grizelj D, Livun A, et al. Inflammatory gene expression in neck perivascular and subcutaneous adipose tissue in men with carotid stenosis. Angiology. 2022;73(3):234–243. doi:10.1177/00033197211012539
15. Hu T, Shen Y, Cao W, et al. The association and joint effect of adipocyte fatty acid binding protein and obesity phenotype with cardiovascular events. J Clin Endocrinol Metab. 2023;108(9):2353–2362. doi:10.1210/clinem/dgad110
16. Yang G, Fan L, Tan J, et al. Smoking in China: findings of the 1996 national prevalence survey. JAMA. 1999;282(13):1247–1253. doi:10.1001/jama.282.13.1247
17. Tran VD, Do VV, Pham NM, et al. Validity of the international physical activity questionnaire-short form for application in Asian countries: a study in Vietnam. Eval Health Prof. 2020;43(2):105–109. doi:10.1177/0163278718819708
18. Norde MM, Bromage S, Marchioni DML, et al. The global diet quality score as an indicator of adequate nutrient intake and dietary quality - a nation-wide representative study. Nutr J. 2024;23(1):42. doi:10.1186/s12937-024-00949-x
19. Hu T, Xu Y, Li X, et al. Optimal skeletal muscle mass index and incident cardiovascular events: insights from a longitudinal analysis. Eur J Cardiovasc Nurs. 2025. doi:10.1093/eurjcn/zvaf107
20. Hedblad B, Wikstrand J, Janzon L, et al. Low-dose metoprolol CR/XL and fluvastatin slow progression of carotid intima-media thickness: main results from the Beta-Blocker cholesterol-lowering asymptomatic plaque study (BCAPS). Circulation. 2001;103(13):1721–1726. doi:10.1161/01.CIR.103.13.1721
21. Unger T, Borghi C, Charchar F, et al. 2020 international society of hypertension global hypertension practice guidelines. J Hypertens. 2020;38(6):982–1004. doi:10.1097/HJH.0000000000002453
22. ElSayed NA, Aleppo G, Bannuru RR. 2. diagnosis and classification of diabetes: standards of care in Diabetes—2024. Diabetes Care. 2024;47(Suppl 1):S20–s42. doi:10.2337/dc24-S002
23. ZW W, YL G. Chinese guideline for lipid management (primary care version 2024)]. Zhonghua Xin Xue Guan Bing Za Zhi. 2024;52(4):330–337. doi:10.3760/cma.j.cn112148-20240102-00002
24. J SUN, MA C, ZHAO M, et al. Daytime napping and cardiovascular risk factors, cardiovascular disease, and mortality: a systematic review. Sleep Med Rev. 2022;65:101682. doi:10.1016/j.smrv.2022.101682
25. Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140(11):e596–e646. doi:10.1161/CIR.0000000000000678
26. Antoniades C, West HW. ESC CVD prevention guidelines 2021: improvements, controversies, and opportunities. Cardiovasc Res. 2022;118(2):e17–e19. doi:10.1093/cvr/cvab371
27. Preis SR, Massaro JM, Hoffmann U, et al. Neck circumference as a novel measure of cardiometabolic risk: the Framingham heart study. J Clin Endocrinol Metab. 2010;95(8):3701–3710. doi:10.1210/jc.2009-1779
28. Rosenquist KJ, Massaro JM, Pencina KM, et al. Neck circumference, carotid wall intima-media thickness, and incident stroke. Diabetes Care. 2013;36(9):e153–4. doi:10.2337/dc13-0379
29. Ben-Noun L, Sohar E, Laor A. Neck circumference as a simple screening measure for identifying overweight and obese patients. Obes Res. 2001;9(8):470–477. doi:10.1038/oby.2001.61
30. Dai Y, Wan X, Li X, et al. Neck circumference and future cardiovascular events in a high-risk population--A prospective cohort study. Lipids Health Dis. 2016;15(1):46. doi:10.1186/s12944-016-0218-3
31. Hu T, Shen Y, Cao W, et al. Neck circumference for predicting the occurrence of future cardiovascular events: a 7.6-year longitudinal study. Nutr, Metab Cardiovasc Dis. 2022;32(12):2830–2838. doi:10.1016/j.numecd.2022.08.023
32. Sweatt K, Garvey WT, Martins C. Strengths and Limitations of BMI in the diagnosis of obesity: what is the path forward? Curr Obes Rep. 2024;13(3):584–595. doi:10.1007/s13679-024-00580-1
33. Li HX, Zhang F, Zhao D, et al. Neck circumference as a measure of neck fat and abdominal visceral fat in Chinese adults. BMC Public Health. 2014;14(1):311. doi:10.1186/1471-2458-14-311
34. Nielsen S, Guo Z, Johnson CM, et al. Splanchnic lipolysis in human obesity. J Clin Invest. 2004;113(11):1582–1588. doi:10.1172/JCI21047
35. Goh LG, Dhaliwal SS, Welborn TA, et al. Anthropometric measurements of general and central obesity and the prediction of cardiovascular disease risk in women: a cross-sectional study. BMJ Open. 2014;4(2):e004138. doi:10.1136/bmjopen-2013-004138
36. Liao GZ, Liu HH, He CH, et al. Free fatty acids: independent predictors of long-term adverse cardiovascular outcomes in heart failure patients. Lipids Health Dis. 2024;23(1):343. doi:10.1186/s12944-024-02332-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.