Back to Journals » Patient Preference and Adherence » Volume 20
Association Between Mind Mapping Combined with Teach-Back and Follow-Up Adherence After Percutaneous Coronary Intervention: An Exploratory Study
Authors Wang X, Wei J, Wu Y, Lei L, Zhou T, Lin L
Received 13 February 2026
Accepted for publication 2 May 2026
Published 19 May 2026 Volume 2026:20 603390
DOI https://doi.org/10.2147/PPA.S603390
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Emma Veale
Xiaofang Wang, Jia Wei, Yanni Wu, Lei Lei, Tian Zhou, Lin Lin
Department of Cardiovascular Medicine, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, 710004, People’s Republic of China
Correspondence: Lin Lin; Department of Cardiovascular Medicine, The Second Affiliated Hospital of Xi’an Jiaotong University, No. 5 Jianqiang Road, Xincheng District, Xi’an, Shanxi Province, 710004, People’s Republic of China, Email [email protected] Xiaofang Wang, Department of Cardiovascular Medicine, The Second Affiliated Hospital of Xi’an Jiaotong University, No. 5 Jianqiang Road, Xincheng District, Xi’an, Shanxi Province, 710004, People’s Republic of China, Email [email protected]
Background: Suboptimal follow-up adherence after percutaneous coronary intervention (PCI) compromises secondary prevention and elevates the risk of major adverse cardiovascular events (MACEs). Conventional health education is often insufficient, necessitating a structured, practical, and evidence-based nursing protocol.
Objective: To identify factors influencing post-PCI follow-up adherence and assess the association between a mind mapping combined with teach-back educational intervention and levels of adherence and MACEs.
Methods: This single-center retrospective study analyzed data from a real-world nursing quality improvement initiative, including patients undergoing PCI during January, 2024-November, 2024. Patients were divided into mind mapping + teach-back or routine education group. Propensity score matching was employed to balance baseline characteristics. Follow-up adherence (≥ 3 complete visits) and 12-month MACE incidence were compared. Multivariable logistic regression was used to identify adherence factors. Kaplan-Meier and Log rank tests were utilized to compare MACE-free survival.
Results: After matching (63 patients per group), baseline characteristics were balanced. High follow-up adherence was observed more frequently in the mind mapping + teach-back group (79.4% vs. 61.9%, P = 0.031). The combined intervention was independently associated with higher adherence (OR = 2.658, 95% CI: 1.042– 6.783, P = 0.041). The mind mapping + teach-back group showed a lower observed 12-month MACE incidence (11.1% vs. 20.6%, P = 0.048) and a higher MACE-free survival rate (log-rank P = 0.042).
Conclusion: In this exploratory study, the mind mapping combined with teach-back method was associated with better follow-up adherence; a lower incidence of MACE was also observed, although this finding is exploratory given the limited sample size and event numbers. It may represent a promising and operable nursing practice tool. These findings suggest a potential benefit that warrants further investigation; our results provide preliminary evidence to inform the design of future prospective randomized controlled trials, rather than immediate integration into clinical practice.
Keywords: percutaneous coronary intervention, follow-up adherence, mind mapping, teach-back method
Introduction
Coronary atherosclerotic heart disease (CAD) remains a leading global cause of mortality and disability.1 Percutaneous coronary intervention (PCI), a pivotal method for revascularization, effectively alleviates angina symptoms, improves myocardial perfusion, and significantly reduces mortality in patients with acute coronary syndromes (ACS).2 However, PCI is a mechanical intervention, not a curative treatment. The atherosclerotic process persists, leaving patients at continued risk of in-stent restenosis, neoatherosclerosis, and progression of non-target lesions, which sustains a substantial incidence of major adverse cardiovascular events (MACEs).3–5 Therefore, identifying key influencing factors and developing targeted, actionable nursing interventions are crucial for improving long-term patient outcomes.
Systematic outpatient follow-up is central to secondary prevention post-PCI, playing a vital role in monitoring disease status, evaluating treatment efficacy, and managing risk factors.6,7 Nevertheless, real-world data indicate generally poor follow-up adherence among post-PCI patients.8 This not only directly results in suboptimal control of risk factors such as hypertension, dyslipidemia, and hyperglycemia but also significantly elevates the risk of recurrent MACEs.9 Consequently, systematically identifying factors affecting adherence is a prerequisite for constructing effective intervention strategies. Existing research suggests that patient follow-up adherence is a complex behavior driven by multidimensional factors encompassing socioeconomic characteristics, clinical status, psychological elements, and healthcare system support.10,11 However, studies have largely been confined to correlational analyses, lacking systematically validated intervention strategies built upon these identified factors.
Developing targeted interventions based on identified key factors is essential for improving post-PCI patient prognosis. Conventional health education often relies on a unidirectional information delivery model, featuring fragmented content and lacking verification of comprehension, which can lead to incomplete patient understanding or execution errors. Hence, there is a need to introduce structured, visual, and interactive educational strategies.12,13 Mind mapping, through its graphical structure, can present complex post-procedural management knowledge in a highly logical and intuitive manner, facilitating patient comprehension and memory.7 The teach-back method, as a bidirectional communication strategy, employs a cyclical process of patient restatement-nurse clarification to ensure accurate grasp of core information and timely correction of misconceptions.14 The combined mind mapping with teach-back model theoretically synergizes cognitive reinforcement and communication efficacy to enhance patient self-management capability and follow-up adherence. Through a clear behavioral and biological pathway, effective health education enhances patient adherence to secondary prevention, which directly leads to better control of core risk factors (such as blood pressure and LDL-C levels), ultimately translating into the reduction of long-term MACE incidence. However, the application value of this combined model in post-PCI patient management, particularly its impact on MACE incidence in real-world clinical settings, has not been thoroughly investigated. While interventional studies evaluating these educational tools exist in other chronic disease domains, there remains a notable lack of real-world observational evidence specifically within post-PCI populations to validate the clinical impact of this combined model.
Therefore, this study aimed, through a single-center retrospective observational cohort design, first to explore factors influencing follow-up adherence after PCI, and then to preliminarily assess the association between a nurse-led, mind mapping combined with teach-back educational intervention and subsequent levels of follow-up adherence and MACE incidence in real-world clinical practice. The results are expected to provide crucial preliminary evidence and hypotheses for designing future prospective randomized controlled trials.
Materials and Methods
Study Population
A retrospective cohort design was adopted, consecutively enrolling CAD patients who successfully underwent PCI in the Department of Cardiology of our hospital between January 1, 2024, and November 30, 2024. It is important to clarify that the structured educational interventions (mind mapping combined with teach-back) and the standardized follow-up schedule were implemented as part of a routine nursing quality improvement initiative within our department during this period. The present study is a retrospective analysis of the clinical data generated from this real-world practice. Intervention allocation was non-random and subject to the clinical discretion of attending nurses, which introduced inherent selection bias and confounding by indication. Patient data were retrieved and collected via the hospital’s electronic medical record (EMR) system. The study protocol was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University (Approval No.: XJTUAE2023-1719) with a waiver of informed consent due to the retrospective nature. This study was conducted in accordance with the Declaration of Helsinki.
Grouping
This was a retrospective cohort study. Based on clearly documented health education methods in the electronic nursing records, patients were naturally categorized into two groups: the mind mapping + teach-back group (receiving mind mapping combined with teach-back) and the routine education group (receiving routine health education).
In clinical practice, nurses typically conduct a comprehensive assessment of the patient’s comprehension ability, educational background, willingness to communicate, and clinical condition when selecting specific educational methods, with the aim of adopting the most appropriate approach to enhance the effectiveness of health education. Therefore, the division into the intervention and control groups in this study reflects the personalized decision‑making inherent in actual nursing practice rather than random allocation.
To minimize measurement bias, the nursing team administering the intervention was independent of the researchers responsible for data collection and outcome assessment. Furthermore, the researchers adjudicating follow-up adherence and MACEs were blinded to group assignment.
Routine education group received routine health education, delivered by routine ward nurses. This included: (1) Format: A 10–15 minute verbal education session by the responsible nurse, supplemented by a standardized paper-based Post-PCI Rehabilitation Guidance Manual; (2) Content: Covering CAD medication, lifestyle modifications, symptom recognition/management, and the importance of follow-up; (3) Process characteristics: This process did not utilize structured mind mapping tools nor systematically implement the teach-back method to verify patient understanding.
Mind mapping + teach-back group received mind mapping combined with teach-back health education. During the study period, our department utilized a specialized nursing assignment model where a designated team of six specialist cardiac nurses administered this advanced education. These nurses possessed an average of over three years of clinical experience in cardiovascular nursing and were dedicated to delivering these structured educational sessions, while general ward staff managed routine patient care. The intervention pathway was defined as the addition of the following standardized steps to all routine education content: (1) Nurse Training: Nurses participating in the intervention were provided with a 4‑hour standardized training session. The training covered: (a) the theoretical basis of mind mapping and its application in health education; (b) the core steps and communication skills of the teach‑back method; (c) the structure and key teaching points of department’s standardized mind map for post‑PCI management; and (d) simulation exercises and feedback on frequently encountered issues. After the training, a case‑based assessment was conducted to ensure all nurses had mastered the standardized procedure. Furthermore, weekly peer-review sessions were conducted throughout the implementation period to ensure consistency and quality in the delivery of the education. (2) Tool (Figure S1): Use of a standardized post-PCI management mind map designed for this study as a visual aid; (3) Process (Figure S2): Each education session lasted approximately 20–25 minutes. Nurses first provided systematic instruction following the mind map’s logical structure (four modules: medication, follow-up examinations, symptom monitoring, lifestyle). Subsequently, the teach-back method was executed: patients were asked to restate key points in their own words. Nurses immediately clarified and corrected any errors or omissions, repeating this cycle until key information was accurately grasped by the patient.
Inclusion Criteria
Age ≥ 18 years; clinical diagnosis of CAD and successful PCI [success defined as post-procedural residual stenosis < 20% in the target vessel and Thrombolysis In Myocardial Infarction (TIMI) flow grade 3]; and availability of complete clinical records and 12-month follow-up data.
Exclusion Criteria
Severe cognitive impairment, mental illness, or communication barriers preventing cooperation with education or follow-up; comorbidities such as malignant tumors or end-stage hepatic/renal failure; and in-hospital mortality.
Data Collection
Data were extracted from the EMR system, PCI procedure records, and outpatient follow-up databases, including demographics (age, gender, education level, living situation, monthly household income); medical history (smoking, alcohol use [defined as consuming at least one standard alcoholic beverage per week on average over the past year], hypertension, diabetes, dyslipidemia); clinical data [total number of stents, left ventricular ejection fraction (LVEF)]; and anxiety/depression symptoms (Symptoms of anxiety and depression were assessed using the Hospital Anxiety and Depression Scale (HADS). HADS score ≥8 indicating clinically significant symptoms15).
Follow-up adherence was assessed at 1, 3, 6, and 12 months post-PCI. All follow-ups were conducted by a dedicated team of research coordinators, blinded to group assignment and not involved in the intervention, via outpatient review or standardized telephone interviews. A complete follow-up required simultaneous fulfillment of: ① completion of an outpatient or telephone follow-up visit; ② documentation of four core indicators: blood pressure, lipid profile, medication adherence. In line with a prior clinical study,16 and the follow-up schedule of the present study, a patient who completed at least three full follow-up visits was defined as belonging to the high adherence.
MACEs, the composite endpoint within 12 months post-PCI, was recorded, including cardiac death, non-fatal stroke, non-fatal myocardial infarction, repeat coronary revascularization, and re-hospitalization for congestive heart failure.17
Statistical Analysis
Statistical analyses were performed using SPSS software (version 22.0). Baseline characteristics were summarized using descriptive statistics: continuous variables as mean ± standard deviation (SD) and categorical variables as frequencies and percentages. To address the confounding inherent in the non-randomized design, propensity score matching (PSM) was performed. Propensity scores, derived from a logistic regression model including all baseline characteristics, were used to match each patient in the mind mapping + teach-back group with one patient from the routine education group (1:1 nearest neighbor matching without replacement, caliper=0.02). Balance was assessed and confirmed using standardized mean differences (SMDs < 0.1) and a Love plot. For the handling of missing data, a complete-case analysis approach was adopted, as the proportion of missing values across all variables was minimal (< 5%). To assess the independent effect of the educational intervention on follow-up adherence, a multivariable logistic regression model was constructed, with high adherence as the outcome variable and group assignment as the primary predictor. Variables with P < 0.05 in univariate analysis were included as covariates to adjust for potential confounding. Before multivariable regression, variance inflation factor (VIF) was checked for multicollinearity, and all VIF values were < 5, indicating acceptable collinearity. The model included 5 predictor variables with 89 outcome events (high adherence), yielding approximately 18 events per variable, which exceeds the commonly recommended minimum of 10 events per variable and indicates adequate statistical power with a low risk of overfitting. No data imputation was performed, as patients with missing key data were excluded per the eligibility criteria. MACE incidence was compared between groups, and Kaplan-Meier survival curves were plotted. The Log rank test was used to compare MACE-free survival rates. All tests were two-tailed, with P < 0.05 considered statistically significant.
Results
Baseline Characteristics
Prior to PSM, significant differences existed between the mind mapping + teach-back (n = 89) and routine education (n = 111) groups across several baseline indicators (Table 1). Specifically, the mean age in the mind mapping + teach-back group (61.84 ± 7.55 years) was significantly lower than the routine education group (65.97 ± 9.70 years, P = 0.001). Statistically significant differences were also observed in education level (P = 0.002) and monthly household income distribution (P = 0.045), indicating systematic imbalance in sociodemographic characteristics pre-matching.
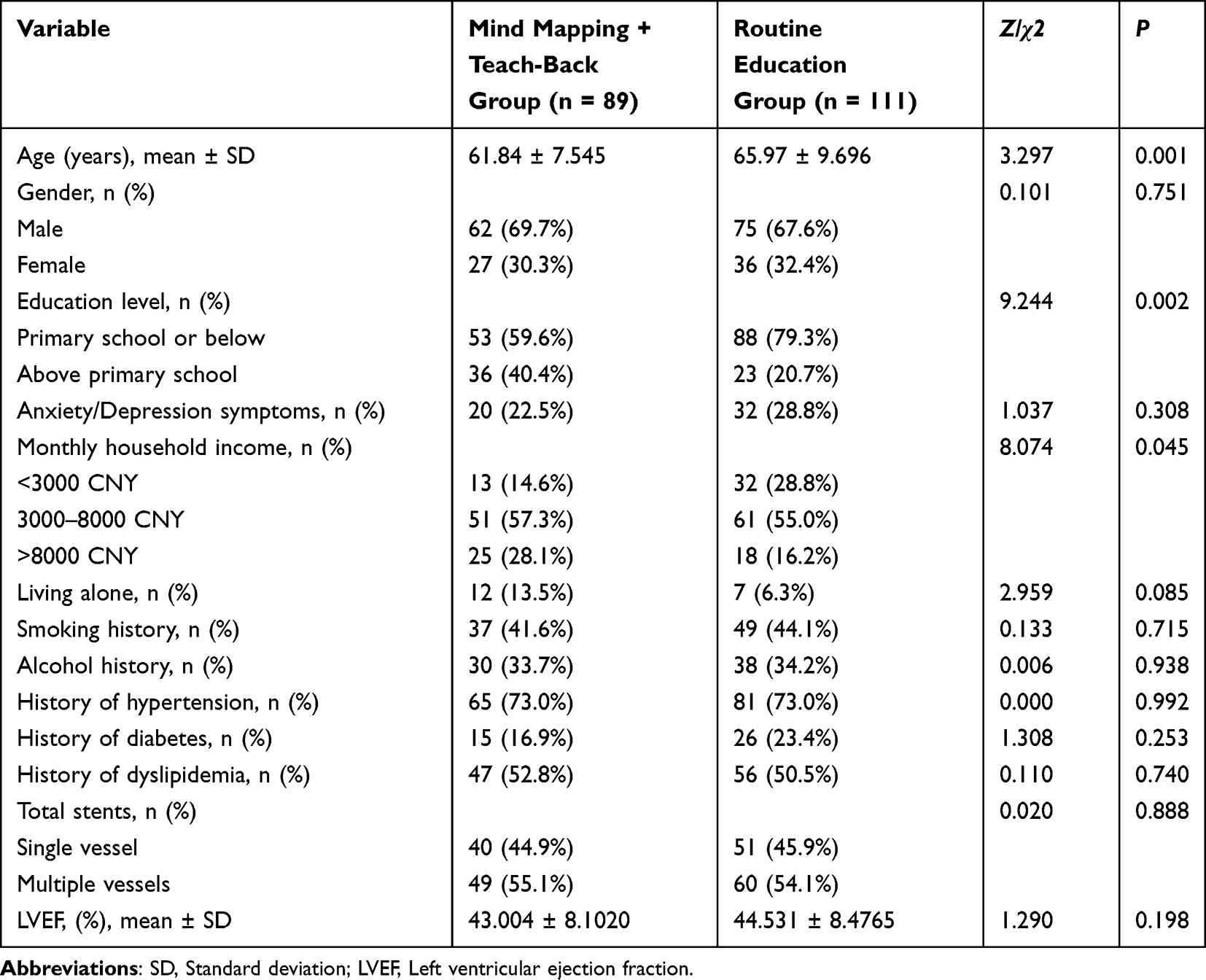 |
Table 1 Comparison of Baseline Characteristics Between Groups Before Matching |
After PSM, 63 patients remained in each group (Table 2). Post-matching analysis revealed no statistically significant differences (all P > 0.05) between groups for all key baseline variables, including age, gender, education level, anxiety/depression symptoms, monthly household income, living alone status, comorbidities (hypertension, diabetes, dyslipidemia), total stent count, and LVEF. PSM effectively improved the balance of baseline characteristics. The comparison of balance before and after matching is illustrated in Figure 1, indicating that PSM controlled for baseline confounding to a considerable extent, providing a comparable foundation for subsequent effect assessment.
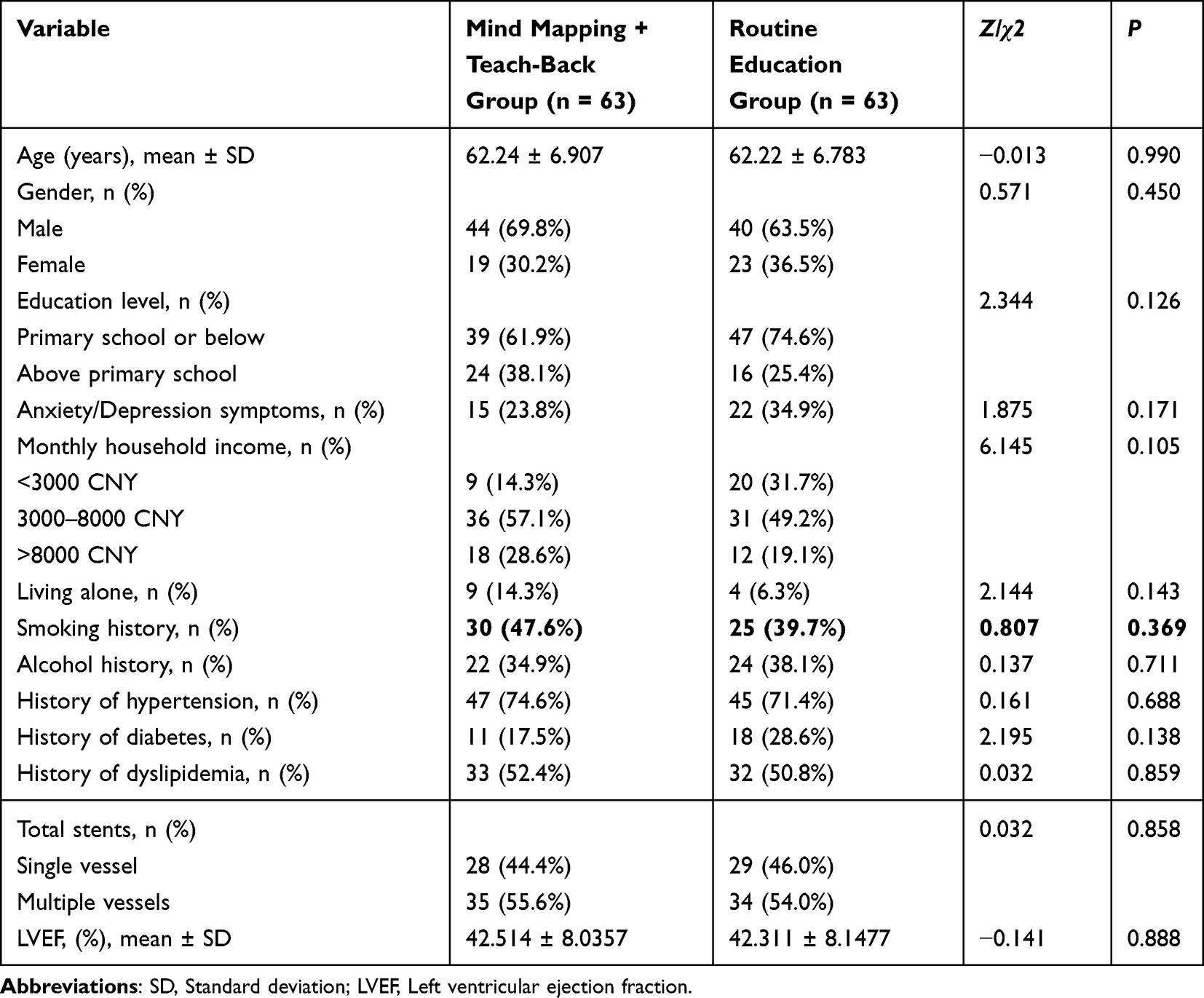 |
Table 2 Comparison of Baseline Characteristics Between Groups After Matching |
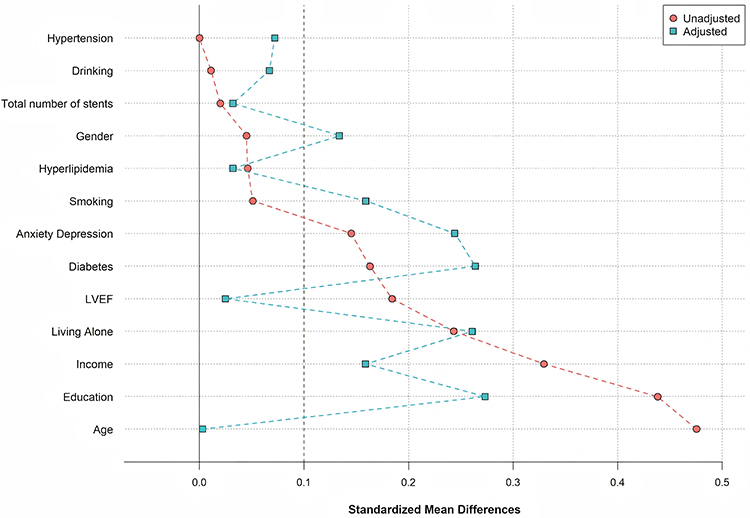 |
Figure 1 Distribution of standardized mean differences for baseline covariates before and after propensity score matching. |
Comparison of Follow-up Adherence
As shown in Table 3, using ≥ 3 follow-up visits as the criterion for high adherence, the proportion of patients with high adherence was 79.4% in the mind mapping + teach-back group, significantly higher than 61.9% in the routine education group (χ2 = 4.63, P = 0.031).
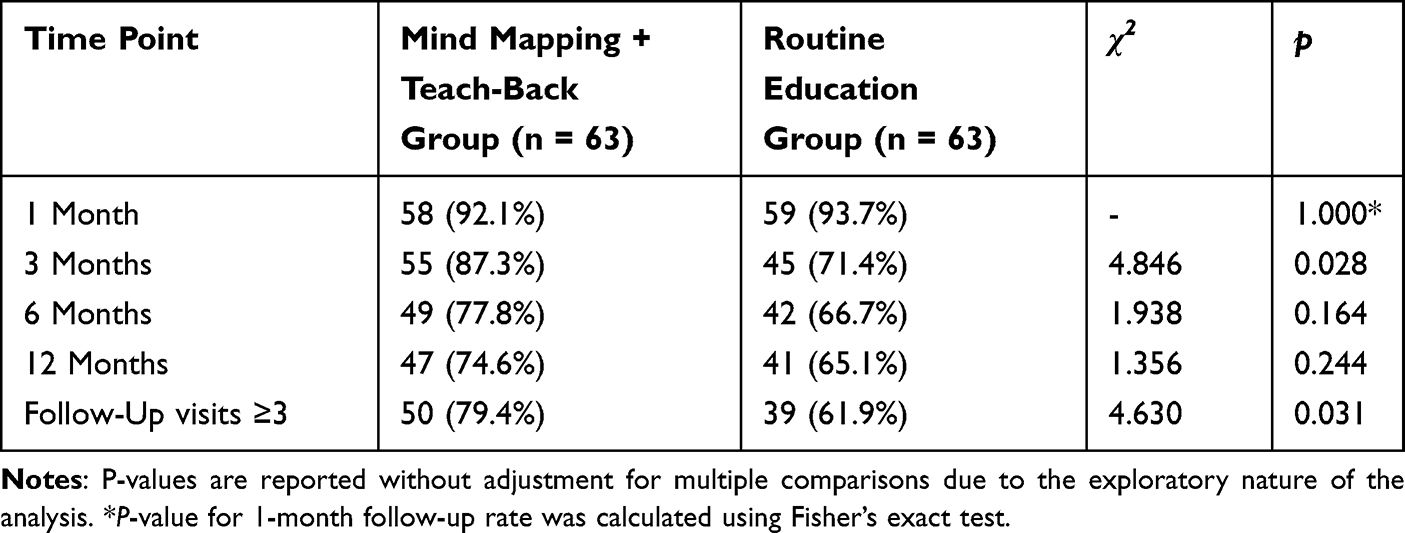 |
Table 3 Comparison of Follow-up Adherence Rates at Different Time Points Between Groups |
Multivariable Logistic Regression Analysis for Follow-up Adherence
To identify factors associated with achieving high follow-up adherence, a multivariable logistic regression analysis was performed (Figure 2). The model included variables significant in univariate analysis. Results indicated that, after adjusting for potential confounders, the mind mapping combined with teach-back intervention (OR = 2.658, 95% CI: 1.042–6.783, P = 0.041) and higher monthly household income (OR = 2.258, 95% CI: 1.058–4.815, P = 0.035) were independently associated with a higher likelihood of high follow-up adherence. The relatively wide confidence intervals reflect the limited sample size, and these associations should be interpreted with caution. Conversely, living alone was independently associated with a lower likelihood of high adherence (OR = 0.187, 95% CI: 0.046–0.759, P = 0.019). Education level and anxiety/depression symptoms did not show statistically significant associations with follow-up adherence (both P > 0.05).
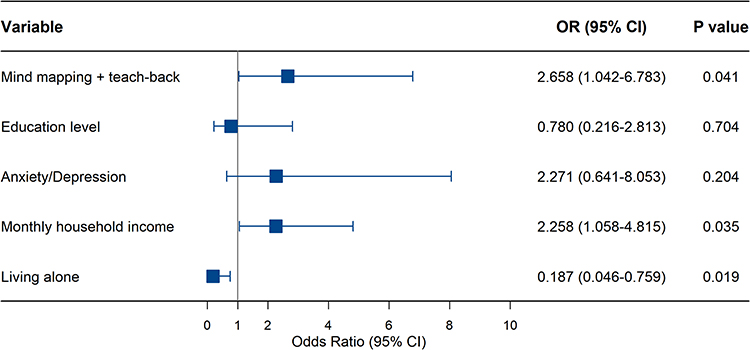 |
Figure 2 Forest plot of multivariable logistic regression analysis for factors associated with high follow-up adherence. Abbreviations: OR, Odds ratio; CI, Confidence interval. |
Impact of Nursing Practice on MACE Incidence
Given the low total number of MACE events, the following comparisons should be interpreted as exploratory. Follow-up data at 12 months post-PCI showed the overall MACE incidence was 11.1% (7/63) in the mind mapping + teach-back group, showing a lower observed frequency compared to 20.6% (13/63) in the routine education group (OR = 0.48, 95% CI: 0.18–1.31; χ2 = 3.91, P = 0.048) (Table 4). Kaplan-Meier survival curve analysis further confirmed a significantly higher MACE-free survival rate in the mind mapping + teach-back group (Log-rank P = 0.042) (Figure 3). However, due to the limited statistical power, these preliminary findings warrant further validation in larger prospective trials.
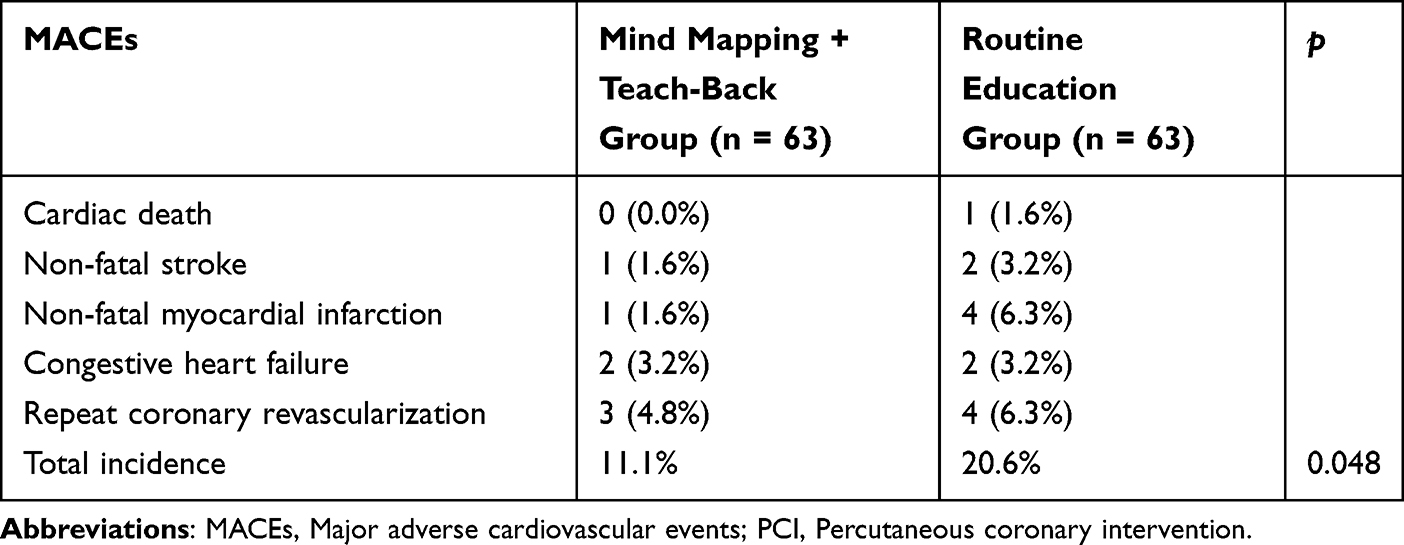 |
Table 4 Comparison of MACEs Between Groups at 12 months Post-PCI |
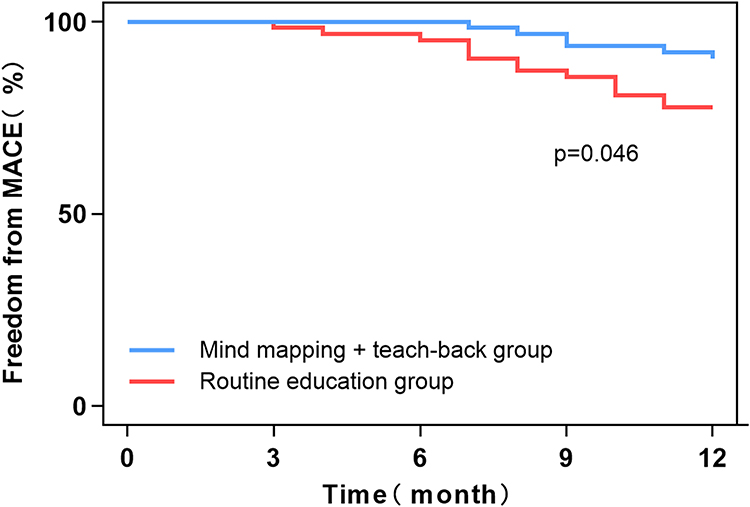 |
Figure 3 Kaplan-Meier curves for MACE-free survival between groups over 12 months post-PCI. Abbreviations: MACE, Major adverse cardiovascular event; PCI, Percutaneous coronary intervention. |
Discussion
In this single-center, retrospective, exploratory study, we observed that the mind mapping combined with teach-back method was associated with improved follow-up adherence and a lower incidence of MACEs at 12 months in post-PCI patients after balancing measured baseline characteristics using PSM. However, before interpreting these findings, several critical methodological limitations must be explicitly acknowledged, as they fundamentally constrain the inferences that can be drawn from this study.
First and foremost, the non-randomized, retrospective design with clinician-determined intervention allocation introduces a high risk of selection bias and confounding by indication. In our study, the intervention was applied at nurses’ discretion, potentially influenced by patient characteristics such as perceived cooperativeness or education level. For instance, nurses might have preferentially utilized the more time-intensive combined method for patients who demonstrated higher intrinsic motivation or engagement. Consequently, the observed improvements in adherence and MACE reduction might partially reflect the patients’ underlying compliance rather than the exclusive effect of the intervention itself, fundamentally limiting our ability to draw definitive causal conclusions.
The identification of lower household income and living alone as independent risk factors for poor follow-up adherence aligns with prior evidence highlighting socioeconomic and social support barriers to sustained healthcare engagement.18–20 Notably, the mind mapping combined with teach-back intervention remained independently associated with higher adherence even after accounting for these factors. While this association is encouraging, it must be interpreted with caution due to the aforementioned potential for residual confounding by unmeasured patient factors.
From a mechanistic perspective, the combined method may address several limitations of conventional health education. Mind mapping organizes complex information visually, potentially reducing cognitive load and enhancing recall.21,22 The teach-back method promotes active learning through iterative verification, which may improve comprehension and self-efficacy.23,24 Regarding clinical implementation, adopting this combined approach presented certain challenges. Initially, the teach-back method increased the duration of each education session (by approximately 5–10 minutes), briefly adding to the nurses’ workload in a busy ward setting. However, several facilitators supported its successful adoption. The visual nature of the mind map provided a clear, structured guide for nurses, which standardized the delivery of information and ultimately enhanced communication efficiency. Furthermore, patients generally exhibited high acceptance of the graphical format, which lowered the cognitive threshold for understanding complex secondary prevention strategies.
Our findings should be contextualized within broader efforts to stratify post-PCI risk and optimize follow-up. Recent studies emphasize the value of integrated risk assessment tools for predicting cardiovascular outcomes. For instance, the R‑CHADS2 score has been validated for predicting contrast-induced nephropathy and MACEs in STEMI patients after PCI, underscoring the need for structured post-procedural monitoring.25 Similarly, inflammatory and nutritional indices such as the C‑reactive protein‑albumin‑lymphocyte (CALLY) index have been linked to clinical outcomes in heart failure populations, reflecting the multifactorial nature of cardiovascular prognosis.26 While our intervention focused on educational reinforcement, future strategies could incorporate such prognostic markers to tailor follow-up intensity and content.
Despite balancing observed covariates through PSM, residual imbalance may still persist for certain variables that were included in the matching process. For instance, although standardized mean differences for monthly household income and living alone were below 0.1 after matching, the possibility of residual confounding due to the categorical nature of these variables or unmeasured dimensions (eg, depth of social support, financial stress) cannot be fully excluded. This reduction in sample size, combined with the relatively low number of MACE events (n=20), limits the statistical power and may affect the stability of our survival analyses. Therefore, while PSM improves comparability, our findings should be interpreted as exploratory and hypothesis-generating rather than confirmatory.
In summary of our limitations, despite our use of PSM to balance measured covariates, unmeasured confounding (eg, by patient engagement, health literacy, or subtle clinician preferences) remains a plausible alternative explanation for the observed associations. This fundamental limitation precludes causal inference. Second, the single-center setting and the relatively small sample size after matching, particularly for the analysis of infrequent MACE events, limit the statistical power and generalizability of our findings. Third, we did not apply statistical correction for multiplicity in this exploratory context; therefore, the observed statistical significances should be considered as preliminary and interpreted alongside effect sizes and confidence intervals. Additionally, exploring the integration of digital mind maps with remote teach-back methods via mobile health technology is a promising direction. To mitigate allocation bias and improve health equity in the future, standardized screening pathways (eg, using validated health literacy tools upon admission) should be implemented to ensure equitable distribution of educational resources. Additionally, our operationalization of high adherence (≥3 complete visits) was based on a pragmatic threshold derived from the scheduled follow-up protocol; the dichotomization may have led to some misclassification, and its association with long-term clinical outcomes requires further validation. Further investigation into the intervention’s effects on broader outcomes such as quality of life and cost-effectiveness is also warranted.
Conclusion
In summary, this exploratory study suggests that a combined mind mapping and teach-back educational intervention was associated with improved follow-up adherence. However, these findings must be interpreted with extreme caution due to the limited statistical power resulting from the small sample size and low number of clinical events. The findings underscore the potential value of structured patient education while acknowledging the substantial influence of socioeconomic factors. These observations are strictly hypothesis-generating; further rigorous, adequately powered prospective studies are needed to establish causality and to optimize implementation strategies before making any definitive clinical recommendations.
Data Sharing Statement
Data will be available upon reasonable request to the corresponding author.
Ethics Statement
The study protocol was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University (Approval No.: XJTUAE2023-1719) with a waiver of informed consent due to the retrospective nature. This study was conducted in accordance with the Declaration of Helsinki.
Funding
This study was supported by Key Research and Development Program of Shaanxi Province (No. S2024-YF-YBSF-0966).
Disclosure
The authors report no conflict of interest.
References
1. Palaniappan LP, Allen NB, Almarzooq ZI, et al. 2026 heart disease and stroke statistics: a report of US and global data from the American heart association. Circulation. 2026. doi:10.1161/CIR.0000000000001412
2. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(3):e18–11. doi:10.1161/CIR.0000000000001038
3. Fong Y. Importance of Postoperative Follow-Up for Patient Outcome. JAMA Surg. 2023;158(12):1301–1302. doi:10.1001/jamasurg.2023.4535
4. Ren XY, Li YF, Liu HQ, et al. Anti-inflammatory therapy progress in major adverse cardiac events after pci: chinese and western medicine. Chin J Integr Med. 2023;29(7):655–664. doi:10.1007/s11655-023-3638-8
5. Nishikawa R, Shiomi H, Morimoto T, et al. Effects of peripheral artery disease on long-term outcomes after percutaneous coronary intervention versus coronary artery bypass grafting in patients with severe coronary artery disease. J Cardiol. 2024;84(4):279–286. doi:10.1016/j.jjcc.2023.12.004
6. Ha Dinh TT, Bonner A, Clark R, Ramsbotham J, Hines S. The effectiveness of the teach-back method on adherence and self-management in health education for people with chronic disease: a systematic review. JBI Database System Rev Implement Rep. 2016;14(1):210–247. doi:10.11124/jbisrir-2016-2296
7. Mathews L, Mok Y, Ding N, et al. Social support, social isolation, and outpatient cardiac rehabilitation participation among older adults in the community: the ARIC study. J Am Heart Assoc. 2024;13(9):e033171. doi:10.1161/JAHA.123.033171
8. Kareem H, Shetty PN, Devasia T, et al. Impact of socioeconomic status on adverse cardiac events after coronary angioplasty: a cohort study. Heart Asia. 2018;10(2):e010960. doi:10.1136/heartasia-2017-010960
9. Xie G, Sun Y, Myint PK, et al. Six-month adherence to Statin use and subsequent risk of major adverse cardiovascular events (MACE) in patients discharged with acute coronary syndromes. Lipids Health Dis. 2017;16(1):155. doi:10.1186/s12944-017-0544-0
10. Khatib R, Marshall K, Silcock J, Forrest C, Hall AS. Adherence to coronary artery disease secondary prevention medicines: exploring modifiable barriers. Open Heart. 2019;6(2):e000997. doi:10.1136/openhrt-2018-000997
11. Bahit MC, Korjian S, Daaboul Y, et al. Patient adherence to secondary prevention therapies after an acute coronary syndrome: a scoping review. Clin Ther. 2023;45(11):1119–1126. doi:10.1016/j.clinthera.2023.08.011
12. Xiong R, Wang N, He J. Effects of mind mapping combined with microvideo explanation on disease perception control and nursing cooperation during membrane induction therapy in patients with infectious nonunion after tibial trauma. Emerg Med Int. 2022;2022:4439595. doi:10.1155/2022/4439595
13. Wang F, Feng WM, Zhu M, et al. A study on the effect of using the video teach-back method in continuous nursing care of stroke patients. Front Public Health. 2024;12:1275447. doi:10.3389/fpubh.2024.1275447
14. Sajadi AS, Babajani A, Maroufi SS, Sarraf N. Using the mind map method in medical education, its advantages and challenges: a systematic review. J Educ Health Promot. 2024;13:483. doi:10.4103/jehp.jehp_1323_23
15. Fomenko A, Dummler D, Akturk Z, et al. Hospital anxiety and depression scale anxiety subscale (Hads-A) for detecting anxiety disorders in adults. Cochrane Database Syst Rev. 2025;7(7):CD015456. doi:10.1002/14651858.CD015456
16. Zhang GC, Jiajin L, Zhixian O, et al. Study on the influence of follow-up compliance on risk factors of patients with coronary heart disease afterinterventional treatment. Pract Clin J Integr Trad. 2024;24(18):1–5. doi:10.13638/j.issn.1671-4040.2024.18.001
17. Rosner GF, Kirtane AJ, Genereux P, et al. Impact of the presence and extent of incomplete angiographic revascularization after percutaneous coronary intervention in acute coronary syndromes: the acute catheterization and urgent intervention triage strategy (ACUITY) trial. Circulation. 2012;125(21):2613–2620. doi:10.1161/CIRCULATIONAHA.111.069237
18. Sarnak MJ, Amann K, Bangalore S, et al. Chronic kidney disease and coronary artery disease: JACC state-of-the-art review. J Am Coll Cardiol. 2019;74(14):1823–1838. doi:10.1016/j.jacc.2019.08.1017
19. Singh A, Udayakumar B, Duraisamy Ravilla T, Ponnappan V, Krishnadas R, Satyavageeswaran P. Factors affecting follow-up adherence of glaucoma patients. Ophthalmic Epidemiol. 2024;31(1):37–45. doi:10.1080/09286586.2023.2199842
20. Soo Hoo SY, Gallagher R, Elliott D. Predictors of cardiac rehabilitation attendance following primary percutaneous coronary intervention for ST-elevation myocardial infarction in Australia. Nurs Health Sci. 2016;18(2):230–237. doi:10.1111/nhs.12258
21. Tariq H, Ahmed S, Ahmed S, et al. Efficacy of nicorandil in preventing myocardial injury and cardiovascular outcomes in patients undergoing percutaneous coronary intervention (PCI): a systematic review and meta-analysis. Cureus. 2024;16(8):e66938. doi:10.7759/cureus.66938
22. Zhang J, Jiao X, Ma X, et al. Effect of nursing care based on goal-oriented mind mapping model on the prognosis of patients with severe brain injury. Medicine. 2024;103(41):e39896. doi:10.1097/MD.0000000000039896
23. Alilu L, Pazirofteh S, Habibzadeh H, Rasouli J. The impact of teach-back training method (TBTM) on treatment adherence in hemodialysis patients: a randomized controlled trial. Ann Med Surg. 2024;86(5):2723–2728. doi:10.1097/MS9.0000000000001906
24. Gullet A, Tastan S. The effect of discharge training based on teach-back method on discharge readiness and satisfaction: a randomized controlled trial. Worldviews Evid Based Nurs. 2025;22(4):e70062. doi:10.1111/wvn.70062
25. Sahin YB, Kiziltunc E, Candemir M. R2CHADS2 score: an effective risk stratification tool for contrast-induced nephropathy and cardiovascular outcomes in STEMI patients undergoing PCI. Angiology. 2025;33197251383333. doi:10.1177/00033197251383333
26. Candemir M, Kiziltunc E, Yamak BA. Association between the C-reactive protein-albumin-lymphocyte (CALLY) index and length of hospital stay in patients with heart failure. Angiology. 2025;33197251338416. doi:10.1177/00033197251338416
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.