Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Association Between Lactic Dehydrogenase-to-Albumin Ratio and Short-Time Mortality in Patients with Chronic Obstructive Pulmonary Disease
Received 8 February 2025
Accepted for publication 8 July 2025
Published 15 July 2025 Volume 2025:20 Pages 2435—2444
DOI https://doi.org/10.2147/COPD.S521192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fanny Wai San Ko
Xiqing Yao, Haoyue Xue, Jiye Luo
Emergency Department, The First People’s Hospital of Lianyungang, Lianyungang City, 222006, People’s Republic of China
Correspondence: Jiye Luo, Emergency Department, The First People’s Hospital of Lianyungang, Lianyungang City, 222006, People’s Republic of China, Email [email protected]
Purpose: The lactate dehydrogenase-to-albumin ratio (LAR) has emerged as a prognostic marker for critically ill patients, yet its relationship with mortality in chronic obstructive pulmonary disease (COPD) remains poorly understood. Our purpose is to assess the predictive value of LAR in COPD patients.
Patients and Methods: In this retrospective cohort study, data were extracted from the MIMIC IV database. COPD patients were divided into two groups based on 28-day all-cause mortality. To investigate the relationship between LAR and short-term mortality, multivariate Cox regression, receiver operating characteristic (ROC) analysis, and Kaplan–Meier survival analysis were performed.
Results: The study included 1048 COPD patients, with 37% experiencing 28-day mortality. LAR was identified as an independent predictor of 28-day mortality (hazard ratio [HR] 1.01, 95% confidence interval [CI]: 1.01– 1.01, P < 0.001). ROC analysis showed that LAR had an area under the curve (AUC) of 69.48% (95% CI: 65.67– 73.29%), demonstrating superior discriminatory power compared to lactate dehydrogenase (AUC = 66.69%) or albumin (AUC = 36.88%) alone. Additionally, LAR’s predictive performance was comparable to that of the Simplified Acute Physiology Score II (SAPSII), which yielded an AUC of 76.8% (95% CI: 73.54– 80.06%). COPD patients with high LAR values (> 120) had significantly higher 28-day mortality rates (P < 0.001).
Conclusion: Elevated LAR is an independent predictor of 28-day mortality in ICU patients with COPD. LAR proves to be a valuable prognostic tool that may assist in the early identification of high-risk patients with CPPD.
Keywords: COPD, lactate dehydrogenase-to-albumin ratio, 28-day all-cause mortality, MIMIC-IV, critically ill
Introduction
Chronic obstructive pulmonary disease (COPD) is a major global health concern, associated with considerable morbidity and mortality.1 Pulmonary function testing (PFT), including the measurement of forced expiratory volume in one second (FEV₁) and forced vital capacity (FVC), remains the gold standard for the diagnosis of COPD. In 2020, the global prevalence of COPD was estimated at 10.6%, affecting approximately 480 million individuals, and it ranks as the fourth leading cause of death worldwide.2,3 The pathogenesis of COPD is multifactorial, with prolonged exposure to inhaled pollutants—such as tobacco smoke and airborne toxins—playing a key role.4,5 The incidence of acute exacerbations of COPD requiring hospitalization varies between 2% and 19% among intensive care unit (ICU) admissions.6 Patients with COPD exhibit higher death rate in the ICU compared to those without the disease.7 As a result, identifying specific biomarkers for early prognosis is essential for providing timely interventions.
Patients with COPD often exhibit elevated lactic dehydrogenase (LDH) levels.8,9 Increased LDH levels have been linked to compromised pulmonary function, particularly reductions in FVC and FEV1.10 A recent study from the US National Health and Nutrition Examination Surveys (NHANES) found a U-shaped relationship between serum LDH levels and all-cause mortality in patients with COPD.11 However, this study focused on general COPD patients, which may limit the applicability of its findings to those specifically admitted to the ICU. Additionally, study indicated that serum albumin concentrations are significantly reduced in individuals with stable COPD compared to healthy controls, suggesting a substantial impairment in systemic anti-inflammatory and antioxidant mechanisms in these patients. A negative relationship has been observed between serum albumin levels and in-hospital mortality among critically ill COPD patients.12 Since LDH reflects tissue damage and systemic inflammation, while albumin serves as a marker of nutritional and inflammatory status, the combination of these two biomarkers as the LDH-to-albumin ratio (LAR) may offer a more comprehensive prognostic insight into disease severity in COPD patients.
Recent studies suggest that the LAR serves as a valuable prognostic marker for critically ill patients with conditions like stroke-associated pneumonia, lower respiratory tract infection, acute respiratory distress syndrome, and acute kidney injury.13–16 However, the link between LAR and mortality in COPD patients remains poorly understood.
This study aims to explore the relationship between LAR and 28-day mortality in COPD patients, using data from the Medical Information Mart for Intensive Care IV (MIMIC-IV, version 3.1) database.
Materials and Methods
Study Design
This study is a retrospective cohort analysis of 1048 COPD patients, with data obtained from the MIMIC-IV (v3.1) database. Developed and maintained by the Computational Physiology Laboratory at the Massachusetts Institute of Technology, the database contains comprehensive clinical information from 65,366 ICU patients admitted between 2008 and 2022. The data include a variety of clinical variables, such as vital signs, laboratory results, and other relevant medical information. Data extraction was performed by Xiqing Yao, who completed the required online training and exams. All patient data within MIMIC have been rendered fully anonymous in accordance with HIPAA Safe Harbor standards. Under the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (February 18, 2023, China), Article 32(1) permits exemption from formal ethics review for research using “lawfully obtained public data or data generated through unobtrusive observation of public behavior”, and Article 32(2) further allows exemption for studies based solely on “anonymized information or biological samples”, Consistent with these provisions, this study was exempt from institutional ethical approval.
Selection of Study Population
Patients with a diagnosis of COPD were identified according to the Tenth Revision of the International Classification of Diseases (ICD-10) codes (J440, J441, J449). The study inclusion criteria were as follows: (1) patients aged over 18 years, (2) ICU admission for a duration exceeding 24 hours, and (3) measurement of LDH and albumin levels within 24 hours of admission. Following these criteria, the cohort was divided into two subgroups: the 28-day survivors and the 28-day non-survivors.
Variable Extraction
Data extraction was conducted by using Structured Query Language (SQL) within Navicat Premium (Version 16.3). A range of variables, either directly obtained or derived, were incorporated for subsequent analysis. These variables encompassed demographic characteristics (age, sex, race), comorbid conditions (sepsis-3, myocardial infarction, peripheral vascular disease, cerebrovascular disease, diabetes, renal disease, and malignancy), indicators of illness severity (Charlson Comorbidity Index, Simplified Acute Physiology Score II [SAPSII], Sequential Organ Failure Assessment [SOFA]), vital signs (oxygen saturation [SpO2], respiratory rate, systolic and diastolic blood pressure, heart rate [HR]), initial laboratory values (blood urea nitrogen [BUN], sodium, creatinine, potassium, platelets, red blood cells [RBC], white blood cells [WBC], LDH, albumin), and therapeutic interventions (antibiotics, mechanical ventilation, continuous renal replacement therapy [CRRT]).
Variables with missing data exceeding 15% were excluded from the statistical analyses. Since the variable for height had missing data beyond this threshold, leading to the exclusion of body mass index (BMI) from the analysis. No variables exhibited missing data in the range of 5% to 15%. For those variables with missing values below 5%, such as HR, SpO2, potassium, RBC, and WBC, imputation was performed using the mean values. Outliers were managed through the application of the winsorize method.
The primary endpoint of this study was the 28-day all-cause mortality rate.
Statistical Analysis
The normality of continuous data was evaluated through the Skewness-Kurtosis test. Continuous variables exhibiting a normal distribution were expressed as means with standard deviations, while those with a non-normal distribution were described using medians and interquartile ranges (IQR). The Student’s t-test was used to assess differences in continuous variables with a normal distribution. In contrast, for variables that were either non-continuous or did not adhere to a normal distribution, the Mann–Whitney U-test was used. Categorical variables were examined using the chi-squared test or Fisher’s exact test.
Univariate Cox regression was initially conducted to identify potential risk factors. Variables with P-values less than 0.1 were subsequently analyzed in a multivariate Cox regression to assess their independent significance. The predictive accuracy of LAR, lactate dehydrogenase, albumin, SOFA, and SAPSII for 28-day mortality in COPD patients was evaluated using receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC) was calculated to measure prediction accuracy for 28-day mortality. The optimal cut-off value for LAR was determined via the Youden index, and patients were categorized into high and low LAR groups based on this threshold. Kaplan-Meier survival curves were plotted for each group, and the Log Rank test was used to compare the survival outcomes. All statistical tests were two-tailed, with a significance threshold set at P < 0.05. The analysis was performed using R statistical software (version 4.4.2).
Results
Study Population
A total of 1048 patients with COPD extracted from the MMIC-IV database from 2008 to 2022 This group comprised 710 survivors and 388 non-survivors who died within 28 days of hospital admission. The selection procedure for the study cohort is depicted in Figure 1.
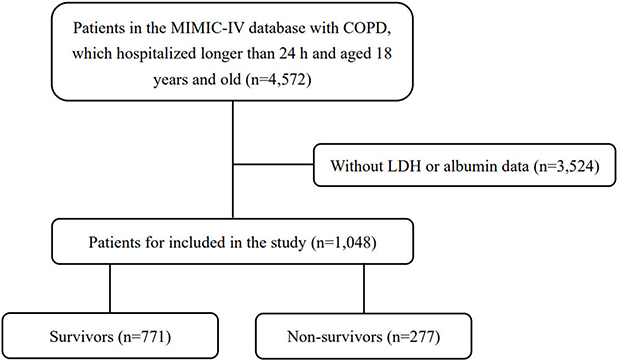 |
Figure 1 Flow chart of the current study. |
Table 1 presents the demographic and clinical characteristics of the study cohort. The overall 28-day all-cause mortality rate was 37%. On average, non-surviving patients were older than survivors (P < 0.001). No significant differences in comorbidity were identified between the two groups, except for a higher prevalence of malignancy in the non-surviving group (P = 0.002). Individuals in the non-survival cohort had elevated severity scores, as assessed by the Charlson Comorbidity Index, SAPSII, and SOFA scores (P < 0.001). Additionally, they presented with higher respiratory rates (P = 0.01) and heart rates (P < 0.001). Laboratory data indicated that the LAR at admission was notably greater in the non-surviving group compared to the survivors (321.6 [82.6, 242.0] vs 148.1 [60.3, 117.0], P < 0.001). LDH levels were significantly higher (P < 0.001) in the non-survival group, while albumin was remarkably lower in the non-survival group (P < 0.001). The RRT was used in 18.4% of the non-survival patients, a proportion significantly greater than that in the survival group (P < 0.001). No significant differences were found between the two groups regarding the administration of antibiotics or vasopressors.
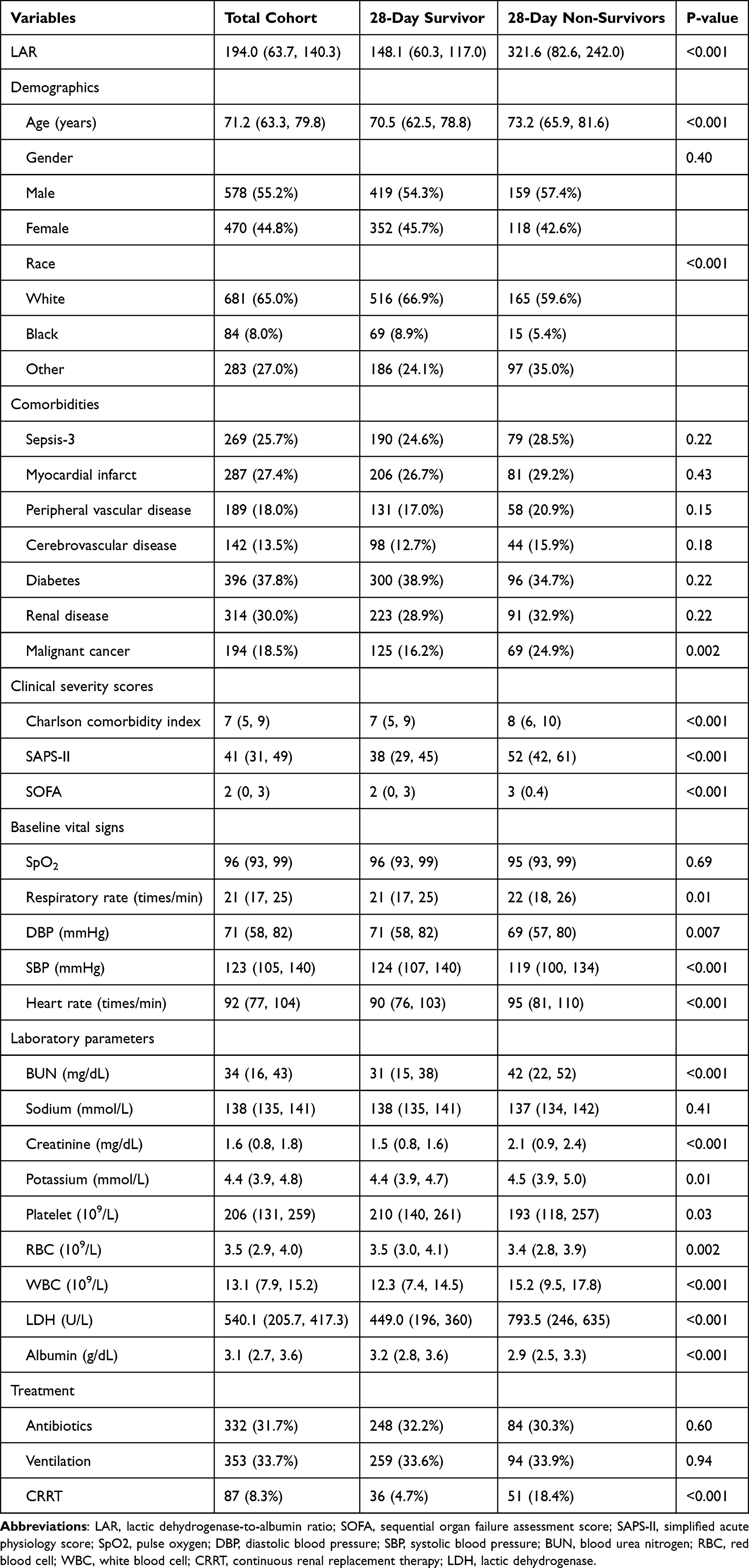 |
Table 1 Baseline Characteristics of Total Cohort, 28-Day Survivors, and 28-Day Non- Survivors |
Correlation Between LAR and 28-Day Mortality
Following the results of the univariate Cox regression analysis, several variables were selected for subsequent examination, including LAR, age, race, malignancy, Charlson Comorbidity Index, SAPS-II, SOFA, CRRT, SpO2, respiratory rate, DBP, SBP, heart rate, BUN, creatinine, potassium, platelets, RBC, and WBC. In the Model I, LAR, along with basic demographic characteristics such as age, sex, and race, were included. The univariate Cox regression analysis demonstrated that LAR was significantly correlated with 28-day all-cause mortality (HR = 1.01; 95% CI, 1.01–1.01; P < 0.001). In the Model II, after adjusting for all included variables, LAR remained a significant independent predictor of 28-day all-cause mortality (HR = 1.01, 95% CI = 1.01–1.01, P = 0.03). Although the HR for LAR per unit increase is 1.01, which is numerically small, interpreting the HR per 100-unit increase provides more clinical relevance. Specifically, a 100-unit increase in LAR corresponds to an HR of approximately 2.7, indicating a 170% increase in hazard. Furthermore, the Charlson Comorbidity Index, SAPS-II, and WBC count were identified as additional independent risk factors for COPD prognosis (Table 2).
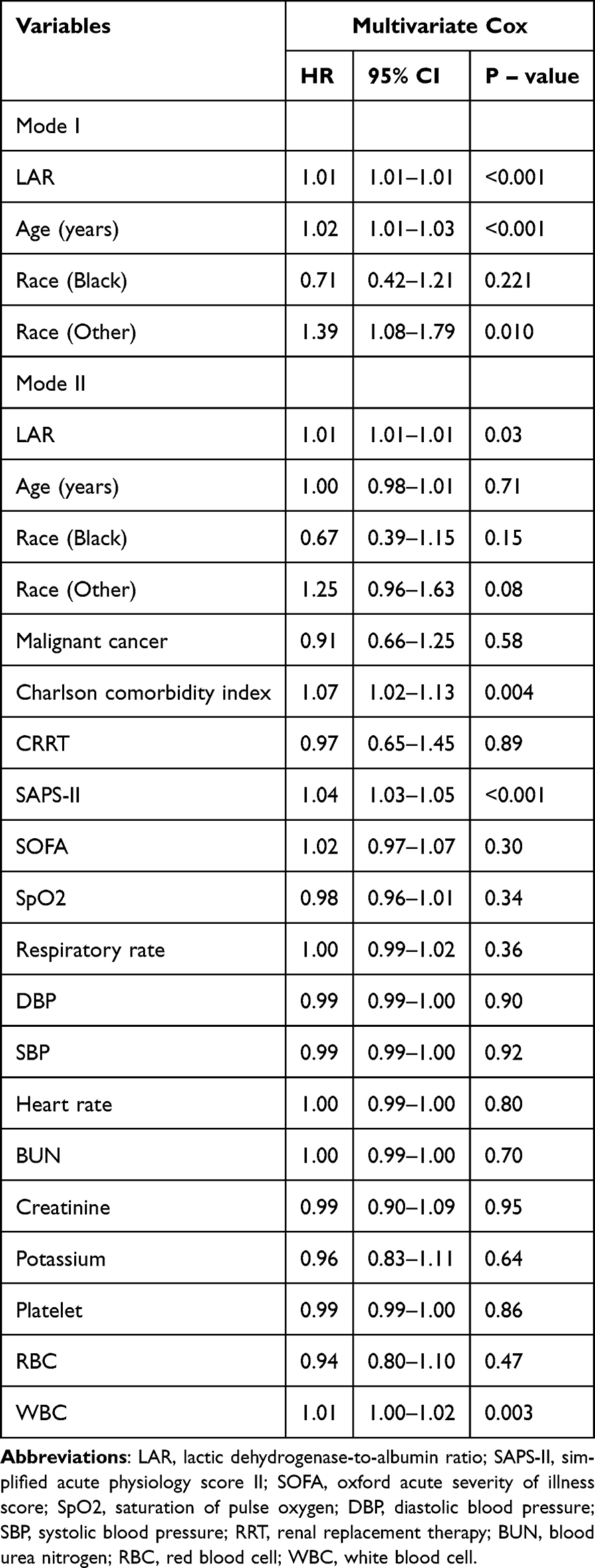 |
Table 2 Multivariate COX Analysis of Risk Factors for 28-Day Mortality |
Survival Analysis
The SAPSII and SOFA scoring systems have been developed and validated as tools for predicting mortality risk in critically ill individuals. In the multivariable Cox regression analysis, SAPSII was demonstrated to be an independent predictor of 28-day all-cause mortality among patients with COPD. To further investigate 28-day mortality in this cohort, ROC curves were generated for variables including LAR, lactic dehydrogenase, albumin, SOFA, and SAPSII (Figure 2).
 |
Figure 2 ROC curve of 28-day mortality in patients with COPD. |
The AUC of LAR was 69.48% (95% CI: 65.67–73.29%), demonstrating superior performance compared to LDH [66.69% (95% CI: 62.72–70.66%)], albumin [36.88% (95% CI: 32.77–40.99%)], and SOFA [61.91% (95% CI: 57.91–65.9%)]. Additionally, LAR’s diagnostic accuracy was found to be comparable to that of SAPSII, which had an AUC of 76.8% (95% CI: 73.54–80.06%). Following this, COPD patients were stratified into two groups based on a LAR cut-off value of 120: high LAR and low LAR. Kaplan-Meier survival analysis indicated that individuals in the high LAR group experienced a significantly higher 28-day mortality rate compared to those in the low LAR group (P < 0.001, Figure 3). This finding was consistent when analyzing in-hospital mortality rates (P < 0.001). Additionally, patients with higher LAR values had prolonged ICU stays (P < 0.001, Table 3).
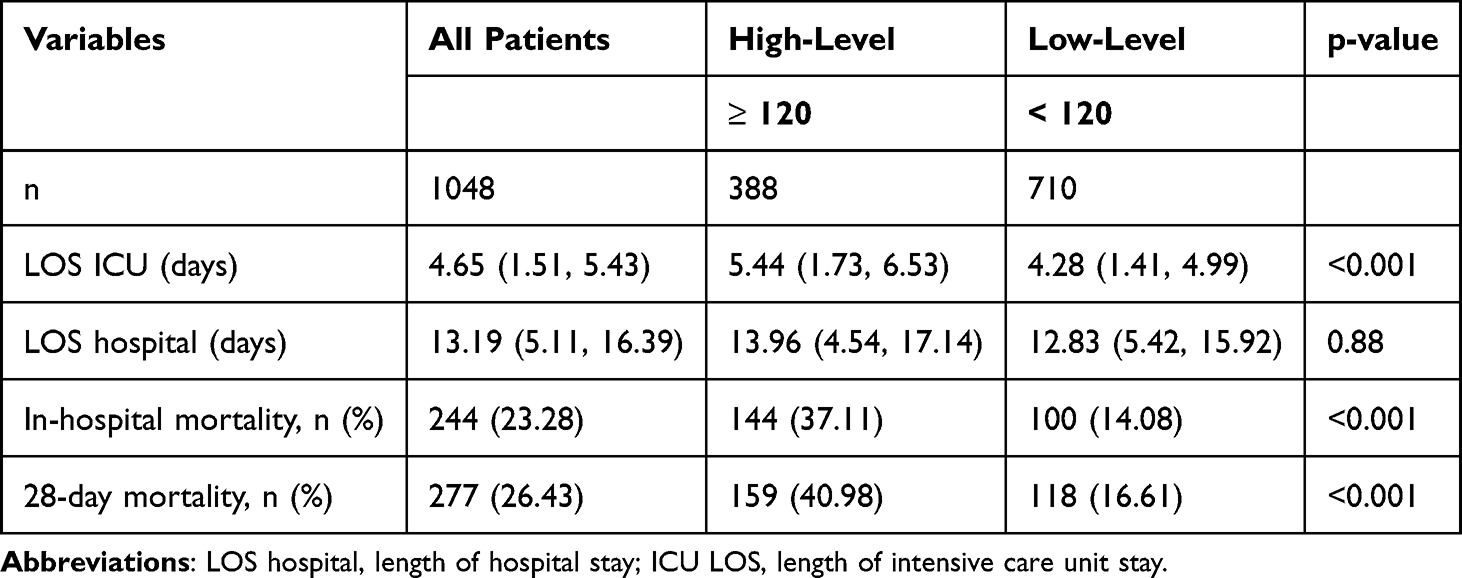 |
Table 3 Relationship Between LAR-Level and Clinical Outcomes |
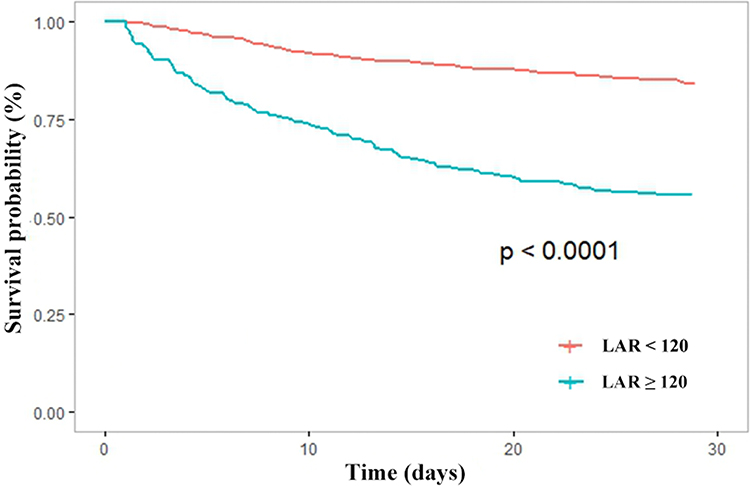 |
Figure 3 Survival curves for the relationship between LAR and risk of 28-day mortality. |
Discussion
The present study identifies the lactic dehydrogenase-to-albumin ratio (LAR) as an independent prognostic factor for 28-day overall mortality in patients with COPD. In comparative analyses, LAR demonstrates superior predictive accuracy (AUC = 69.48%) relative to either LDH (AUC = 66.69%) or albumin (AUC = 36.88%) alone. Additionally, the performance of LAR is found to be on par with that of the SAPSII (AUC = 76.8%). Kaplan-Meier survival analysis further highlights that patients with COPD in high LAR group exhibit a markedly high rate of both 28-day overall mortality and in-hospital mortality.
LAR has increasingly been recognized as a valuable prognostic tool in critically ill patient populations, including those with conditions such as cardiac arrest,17 acute respiratory distress syndrome,13 acute heart failure,18 and pulmonary embolism.19 LDH and albumin are routinely measured in these patients, not only due to their established roles as biomarkers but also because they provide additional insights into the patient’s clinical condition. LDH is a well-established marker of tissue injury and the progression of various pathological conditions,20–22 while albumin is commonly used to assess nutritional status and inflammatory processes.23,24 A retrospective cohort study conducted in Iran found that LAR could predict mortality in COVID-19 patients, with an AUC of 0.768.25 However, no studies have yet used LAR to predict the prognosis in COPD patients. The prognostic value of LAR likely reflects the combined impact of systemic inflammation, oxidative stress, and malnutrition—all of which are prevalent in ICU-admitted COPD patients. Elevated LDH may reflect ongoing tissue damage and inflammatory activation, while low albumin levels can indicate poor nutritional reserves and impaired hepatic function. Together, LAR provides a composite index of physiological stress that is clinically relevant in acute care settings. Our study indicates that LAR is an independent predictor of 28-day mortality in COPD patients. The diagnostic accuracy of LAR (AUC = 69.48%) exceeded that of LDH (AUC = 66.69%) and albumin (AUC = 36.88%) individually. Furthermore, the performance of LAR was comparable to that of SAPSII (AUC = 76.8%). Kaplan-Meier survival analysis revealed that COPD patients with elevated LAR levels experienced significantly higher rates of both 28-day and in-hospital mortality, as well as prolonged hospital stays.
In this study, we compared the LAR, SOFA and SAPSII for predicting 28-day mortality in patients with COPD. The SOFA score is well-established as an effective prognostic tool for mortality in critically ill patients, including those with COPD.26,27 Both SAPSII and SOFA are routinely used in clinical settings to assess the severity of illness in critically ill patients.28,29 In particular, the SOFA score is noted for its utility in predicting the duration of hospital stay and the likelihood of mortality.30 The SAPSII scoring system incorporates a broad range of physiological and clinical parameters, such as respiratory rate (RR), oxygenation index, and additional indicators. Previous research has affirmed the prognostic value of SAPSII in COPD patients.31 Consistent with these findings, multivariate Cox regression analyses have demonstrated that SAPSII is an independent predictor of 28-day mortality in patients with COPD. Our findings indicate that LAR exhibited predictive accuracy comparable to SAPSII. This suggests that LAR, which is calculated using only LDH and albumin, provides similar prognostic insights as SAPSII, despite the latter incorporating a broader array of clinical parameters. Consequently, LAR may offer a more streamlined approach for clinical risk assessment.
This study has several limitations. First, we employed 28-day mortality as the principal prognostic endpoint, without incorporating an evaluation of patient survival status through the MIMIC-IV database. To enhance the precision in assessing the prognostic value of the LAR, a multicenter, prospective study with comprehensive survival data for COPD patients is recommended. Second, the absence of lung function measurements for a substantial proportion of the patient cohort in this investigation limited the capacity to categorize the severity of airflow limitation in all cases of COPD. Third, despite adjusting for multiple clinical covariates, several important potential confounders—such as detailed nutritional status (eg, body mass index, prealbumin), corticosteroid use, and liver dysfunction—were not fully captured in the database and thus not included in our models.
Conclusion
The current study indicates that LAR acts as an independent prognostic factor for 28-day overall mortality in patients with COPD. These findings suggest that LAR could serve as a more convenient tool for anesthesiologists and critical care specialists in comparison to SAPSII, while offering similar accuracy in the prompt identification of COPD patients at high risk for poor outcomes.
Data Sharing Statement
Publicly available datasets were analyzed in this study. This data can be found here: https://physionet.org/content/mimiciv.
Ethics Statement
The research involving human participants underwent review and approval by the Institutional Review Board of the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center. Written informed consent for participation was not deemed necessary for this study in compliance with national legislation and institutional requirements.
Acknowledgments
We would like to thank the Massachusetts Institute of Technology and the Beth Israel Deaconess Medical Center for the MIMIC-IV database.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. They took part in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the global burden of disease study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
2. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
3. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020-50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11(8):e1183–e1193. doi:10.1016/S2214-109X(23)00217-6
4. Chou CH, Chen Y-F, Peng H-C, et al. Environmental pollutants increase the risks of acute exacerbation in patients with chronic airway disease. Front Public Health. 2023;11:1215224. doi:10.3389/fpubh.2023.1215224
5. Hikichi M, Mizumura K, Maruoka S, et al. Pathogenesis of chronic obstructive pulmonary disease (COPD) induced by cigarette smoke. J Thorac Dis. 2019;11(Suppl 17):S2129–s2140. doi:10.21037/jtd.2019.10.43
6. Prediletto I, Giancotti G, Nava S. COPD exacerbation: why it is important to avoid ICU admission. J Clin Med. 2023;12(10):3369. doi:10.3390/jcm12103369
7. Funk GC, Bauer P, Burghuber OC, et al. Prevalence and prognosis of COPD in critically ill patients between 1998 and 2008. Eur Respir J. 2013;41(4):792–799. doi:10.1183/09031936.00226411
8. Skopas V, Papadopoulos D, Trakas N, et al. Lactate dehydrogenase isoenzymes in patients with acute exacerbation of chronic obstructive pulmonary disease: an exploratory cross-sectional study. Respir Physiol Neurobiol. 2021;283:103562. doi:10.1016/j.resp.2020.103562
9. Torres SH, Montes de Oca M, Loeb E, et al. [Lactate dehydrogenase isozymes in skeletal muscle of patients with chronic obstructive pulmonary disease]. Arch Bronconeumol. 2009;45(2):75–80. doi:10.1016/j.arbres.2008.04.001
10. Hu S, Ye J, Guo Q, et al. Serum lactate dehydrogenase is associated with impaired lung function: NHANES 2011-2012. PLoS One. 2023;18(2):e0281203. doi:10.1371/journal.pone.0281203
11. Huang L, Lu Z, Zhou X, et al. U-shaped relationship between serum lactate dehydrogenase with all-cause mortality in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2023;18:305–316. doi:10.2147/COPD.S386269
12. Ling M, Huiyin L, Shanglin C, et al. Relationship between human serum albumin and in-hospital mortality in critical care patients with chronic obstructive pulmonary disease. Front Med. 2023;10:1109910. doi:10.3389/fmed.2023.1109910
13. Zhang F, Zhang M, Niu Z, et al. Prognostic value of lactic dehydrogenase-to-albumin ratio in critically ill patients with acute respiratory distress syndrome: a retrospective cohort study. J Thorac Dis. 2024;16(1):81–90. doi:10.21037/jtd-23-1238
14. Yan D, Huang Q, Dai C, et al. Lactic dehydrogenase to albumin ratio is associated with the risk of stroke-associated pneumonia in patients with acute ischemic stroke. Front Nutr. 2021;8:743216. doi:10.3389/fnut.2021.743216
15. Lee BK, Ryu S, Oh S-K, et al. Lactate dehydrogenase to albumin ratio as a prognostic factor in lower respiratory tract infection patients. Am J Emerg Med. 2022;52:54–58. doi:10.1016/j.ajem.2021.11.028
16. Deng Y, Li X, Lai Q, et al. Prognostic implication of lactic dehydrogenase-to-albumin ratio in critically ill patients with acute kidney injury. Clin Exp Nephrol. 2023;27(4):349–357. doi:10.1007/s10157-023-02321-5
17. Ye L, Lu J, Yuan M, et al. Correlation between lactate dehydrogenase to albumin ratio and the prognosis of patients with cardiac arrest. Rev Cardiovasc Med. 2024;25(2):65. doi:10.31083/j.rcm2502065
18. Xia X, Tan S, Zeng R, et al. Lactate dehydrogenase to albumin ratio is associated with in-hospital mortality in patients with acute heart failure: data from the MIMIC-III database. Open Med. 2024;19(1):20240901. doi:10.1515/med-2024-0901
19. Hu J, Zhou Y. The association between lactate dehydrogenase to serum albumin ratio and in-hospital mortality in patients with pulmonary embolism: a retrospective analysis of the MIMIC-IV database. Front Cardiovasc Med. 2024;11:1398614. doi:10.3389/fcvm.2024.1398614
20. Wulaningsih W, Holmberg L, Garmo H, et al. Serum lactate dehydrogenase and survival following cancer diagnosis. Br J Cancer. 2015;113(9):1389–1396. doi:10.1038/bjc.2015.361
21. Ding J, Karp JE, Emadi A. Elevated lactate dehydrogenase (LDH) can be a marker of immune suppression in cancer: interplay between hematologic and solid neoplastic clones and their microenvironments. Cancer Biomark. 2017;19(4):353–363. doi:10.3233/CBM-160336
22. Heidari Beigvand H, Heidari K, Hashemi B, et al. The value of lactate dehydrogenase in predicting rhabdomyolysis-induced acute renal failure; a narrative review. Arch Acad Emerg Med. 2021;9(1):e24. doi:10.22037/aaem.v9i1.1096
23. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a prospective study. Am J Med. 2020;133(6):713–722.e7. doi:10.1016/j.amjmed.2019.10.031
24. Gremese E, Bruno D, Varriano V, et al. Serum albumin levels: a biomarker to be repurposed in different disease settings in clinical practice. J Clin Med. 2023;12(18):6017. doi:10.3390/jcm12186017
25. Alizadeh N, Tabatabaei FS, Azimi A, et al. Lactate dehydrogenase to albumin ratio as a predictive factor of Covid-19 patients’ outcome; a cross-sectional study. Arch Acad Emerg Med. 2022;10(1):e63.
26. Fayed M, Patel N, Angappan S, et al. Sequential organ failure assessment (SOFA) score and mortality prediction in patients with severe respiratory distress secondary to COVID-19. Cureus. 2022;14(7):e26911. doi:10.7759/cureus.26911
27. Xiao K, Guo C, Su L, et al. Prognostic value of different scoring models in patients with multiple organ dysfunction syndrome associated with acute COPD exacerbation. J Thorac Dis. 2015;7(3):329–336. doi:10.3978/j.issn.2072-1439.2014.11.27
28. Desai N, Gross J. Scoring systems in the critically ill: uses, cautions, and future directions. BJA Educ. 2019;19(7):212–218. doi:10.1016/j.bjae.2019.03.002
29. Sarkar R, Martin C, Mattie H, et al. Performance of intensive care unit severity scoring systems across different ethnicities in the USA: a retrospective observational study. Lancet Digit Health. 2021;3(4):e241–e249. doi:10.1016/S2589-7500(21)00022-4
30. Siddiqui S, Chua M, Kumaresh V, et al. A comparison of pre ICU admission SIRS, EWS and q SOFA scores for predicting mortality and length of stay in ICU. J Crit Care. 2017;41:191–193. doi:10.1016/j.jcrc.2017.05.017
31. Feng Z, Wang T, Liu P, et al. Efficacy of various scoring systems for predicting the 28-day survival rate among patients with acute exacerbation of chronic obstructive pulmonary disease requiring emergency intensive care. Can Respir J. 2017;2017:3063510. doi:10.1155/2017/3063510
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Value of the Albumin Corrected Anion Gap in ICU Patients with Chronic Obstructive Pulmonary Disease and Sepsis: A MIMIC-IV Cohort Study
Zhang B, Bai J, Wang H, Huang F, Miao L, Wang J, Zhou L
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3979-3992
Published Date: 10 December 2025
Association of the Endothelial Activation and Stress Index with Mortality in Critically Ill Patients with Chronic Obstructive Pulmonary Disease: A Retrospective Cohort Study
Li J, Li M, Liang XJ, Zhang S, Dai H, Yang L, Lyu J, Wang Z
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:611259
Published Date: 10 July 2026