Back to Journals » OncoTargets and Therapy » Volume 11
Association between IL-17A G197A polymorphism and gastric cancer risk: an updated meta-analysis based on 6,624 cases and 7,631 controls
Received 7 September 2017
Accepted for publication 1 December 2017
Published 5 February 2018 Volume 2018:11 Pages 703—710
DOI https://doi.org/10.2147/OTT.S151129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Faris Farassati
Lixia Hu,1 Fanliang Kong,1 Yueyin Pan2
1Department of Oncology, The Second People’s Hospital of Hefei, Hefei, Anhui, China; 2Department of Oncology, Anhui Province Hospital, Hefei, Anhui, China
Purpose: Previous studies investigating the association between interleukin-17A (IL-17A) G197A polymorphism and gastric cancer risk have provided inconsistent results. We, therefore, conducted this meta-analysis to clarify the association between IL-17A G197A polymorphism and gastric cancer risk.
Methods: We searched PubMed, Excerpta Medica Database, and CNKI databases to identify relevant studies up to June 10, 2017. A total of 16 case-control studies including 6,624 cases and 7,631 controls were identified.
Results: Overall, significant associations between IL-17A G197A polymorphism and gastric cancer risk were observed (A vs G: OR =1.24, 95% CI =1.14–1.36; AA vs GG: OR =1.63, 95% CI =1.35–1.96; GA vs GG: OR =1.12, 95% CI =1.01–1.25; AA+GA vs GG: OR =1.23, 95% CI =1.11–1.35; AA vs GA+GG: OR =1.54, 95% CI =1.27–1.87). Similar associations were also observed in Asian population (A vs G: OR =1.25, 95% CI =1.15–1.37; AA vs GG: OR =1.62, 95% CI =1.33–1.97; GA vs GG: OR =1.16, 95% CI =1.07–1.25; AA+GA vs GG: OR =1.24, 95% CI =1.15–1.33; AA vs GA+GG: OR =1.51, 95% CI =1.23–1.85), in Caucasian population (AA vs GA+GG: OR =2.19, 95% CI =1.40–3.44), and in the hospital-based controls’ subgroup (A vs G: OR =1.30, 95% CI =1.17–1.45; AA vs GG: OR =1.81, 95% CI =1.46–2.25; AA+GA vs GG: OR =1.27, 95% CI =1.12–1.43; AA vs GA+GG: OR =1.71, 95% CI =1.34–2.18).
Conclusions: The current meta-analysis suggests that IL-17A G197A polymorphism might enhance gastric cancer risk.
Keywords: gastric cancer, polymorphism, meta-analysis, interleukin-17A, rs2275913
Introduction
Interleukin-17 (IL-17) is a relatively newly described family of pro-inflammatory cytokines that consists of six family members (IL-17A–F).1 IL-17 is produced by CD4+ memory T cells, and it is involved in both innate and adaptive immune responses.2,3 It has been reported that IL-17A, a pro-inflammatory cytokine, is associated with the pathogenesis of chronic inflammatory diseases, autoimmune diseases,4,5 and cancer progression.6,7
There are many studies that focus on the relationship between IL-17A G197A polymorphism and gastric cancer.8–23 These studies are all based on experimental results, but their results are always inconsistent. Since 2015, only one meta-analysis has been conducted, and 11 case-control studies were included in this meta-analysis.24 Today, more than five studies that assessed the association between IL-17A G197A polymorphism and the risk of gastric cancer have been published. Therefore, we performed an updated meta-analysis to further determine an accurate relationship between IL-17A G197A polymorphism and gastric cancer susceptibility.
Materials and methods
Publication search
We conducted a publication search in PubMed, Excerpta Medica Database, and CNKI databases (up to June 10, 2017) using the following search strategy: “interleukin-17A or interleukin 17A or IL-17A or IL17A”, “polymorphism”, and “gastric cancer”. No language restrictions were applied. Studies had to meet the following criteria: 1) case-control studies; 2) diagnoses of all patients with malignant tumors were confirmed by pathological or histological examination; 3) the study assessed the association between gastric cancer risk and the IL-17A G197A polymorphism. The following exclusion criteria were used: 1) unpublished studies or abstracts; 2) duplicate publications; and 3) insufficient data were reported.
Data extraction
For each study, the following characteristics were extracted: first author, year of publication, ethnicity, sample size (total cases and controls), source of controls, genotype distributions in cases and controls, and P-value of Hardy–Weinberg equilibrium (HWE).25 Disagreements were resolved by discussion.
Statistical analysis
Odds ratios (ORs) with corresponding 95% CIs were calculated to clarify the strength of the association between IL-17A G197A polymorphism and gastric cancer risk. Five genetic models were assessed: homozygote model (AA vs GG), heterozygote model (GA vs GG), recessive model (AA vs GA+GG), dominant model (AA+GA vs GG), and allele model (A vs G). Subgroup analyses were conducted according to ethnicity and source of controls.
Heterogeneity was calculated by using both χ2-based Q-statistic and I2-statistic.26 If P≥0.1 and I2<50%, the fixed-effects model (Mantel–Haenszel method) was chosen.27 Otherwise, the random effects model (Der Simonian–Laird method) was used.28 Moreover, sensitivity analysis was performed to assess the stability of the results. Publication bias was assessed with funnel plots and Egger’s test.29 All of the statistical tests were carried out with STATA version 12.0 (Stata corporation, College Station, TX, USA). P<0.05 was considered significant, and all P-values were two sided.
Results
Characteristics of eligible studies
A flow diagram illustrating the study selection process is shown in Figure 1. Through literature search and selection, a total of 16 publications8–23 including 6,624 cases and 7,631 controls were included in the meta-analysis. Table 1 shows the main characteristics of the included studies.
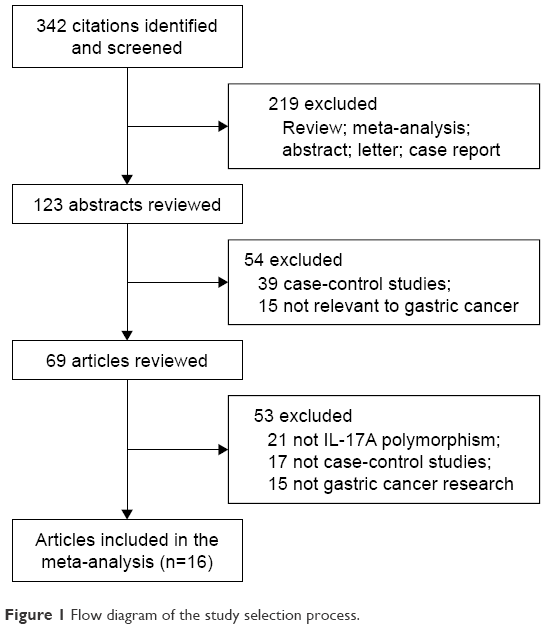 | Figure 1 Flow diagram of the study selection process. |
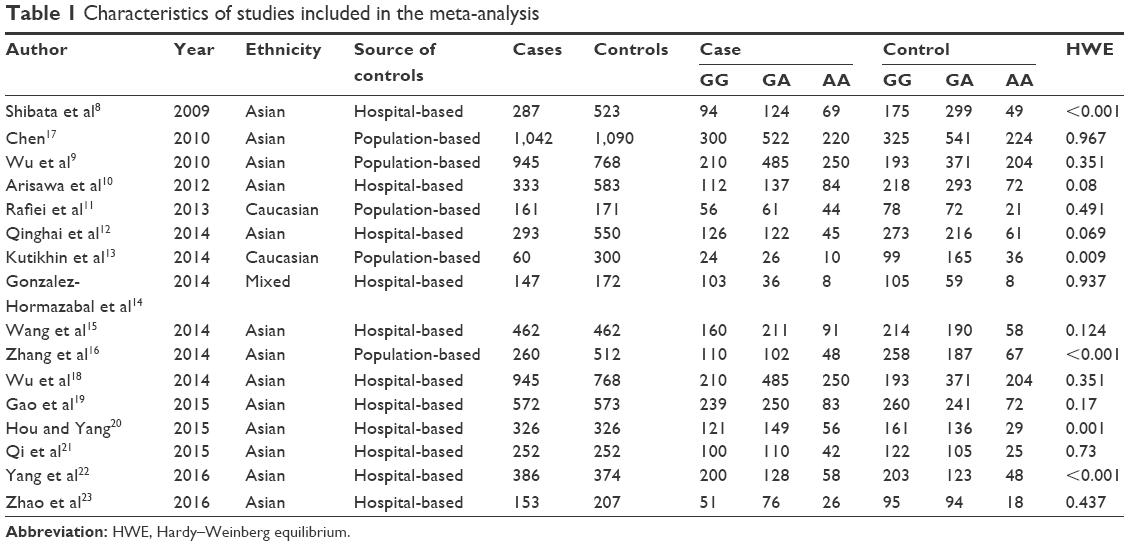 | Table 1 Characteristics of studies included in the meta-analysis |
Meta-analysis
Overall, the IL-17A G197A polymorphism was associated with an increased gastric cancer risk in all genetic models (A vs G: OR =1.24, 95% CI =1.14–1.36, Figure 2; AA vs GG: OR =1.63, 95% CI =1.35–1.96, Figure 3; GA vs GG: OR =1.12, 95% CI =1.01–1.25, Figure 4; AA+GA vs GG: OR =1.23, 95% CI =1.11–1.35, Figure 5; AA vs GA+GG: OR =1.54, 95% CI =1.27–1.87, Figure 6). The HWE of each study was taken into consideration. After eliminating studies whose distribution of genotype in controls deviated from HWE, the outcome remained statistically significant. These results are shown in Table 2.
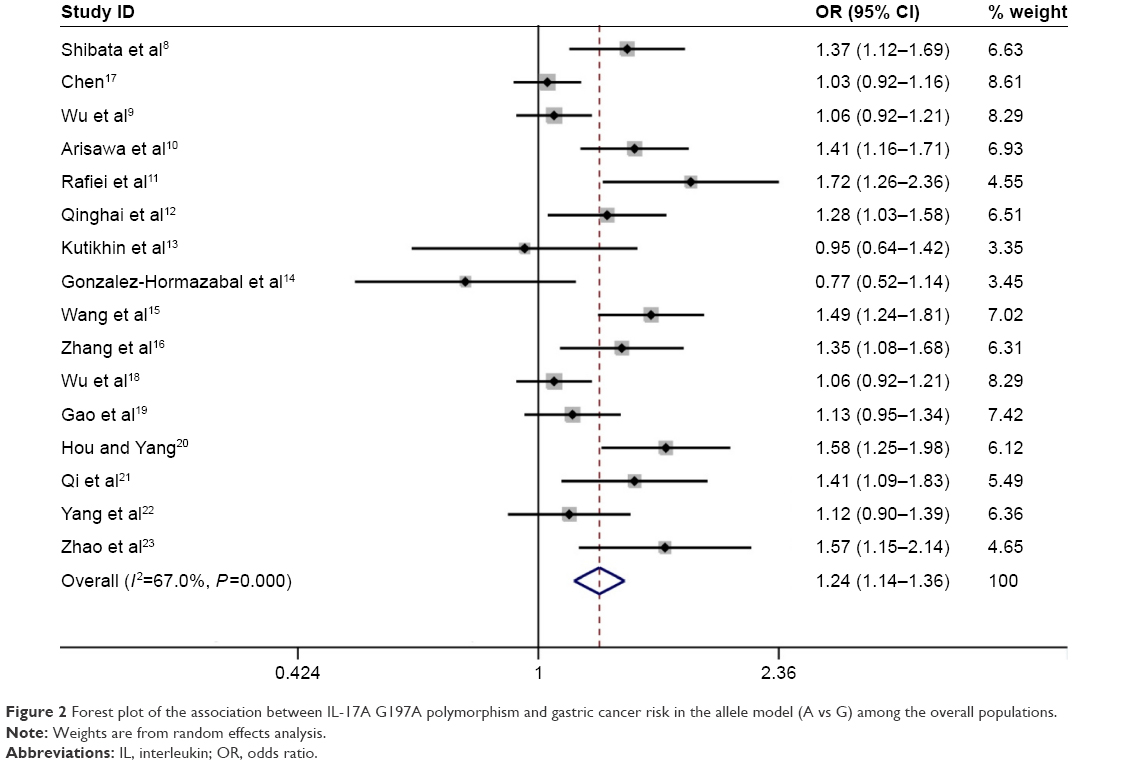 | Figure 2 Forest plot of the association between IL-17A G197A polymorphism and gastric cancer risk in the allele model (A vs G) among the overall populations. |
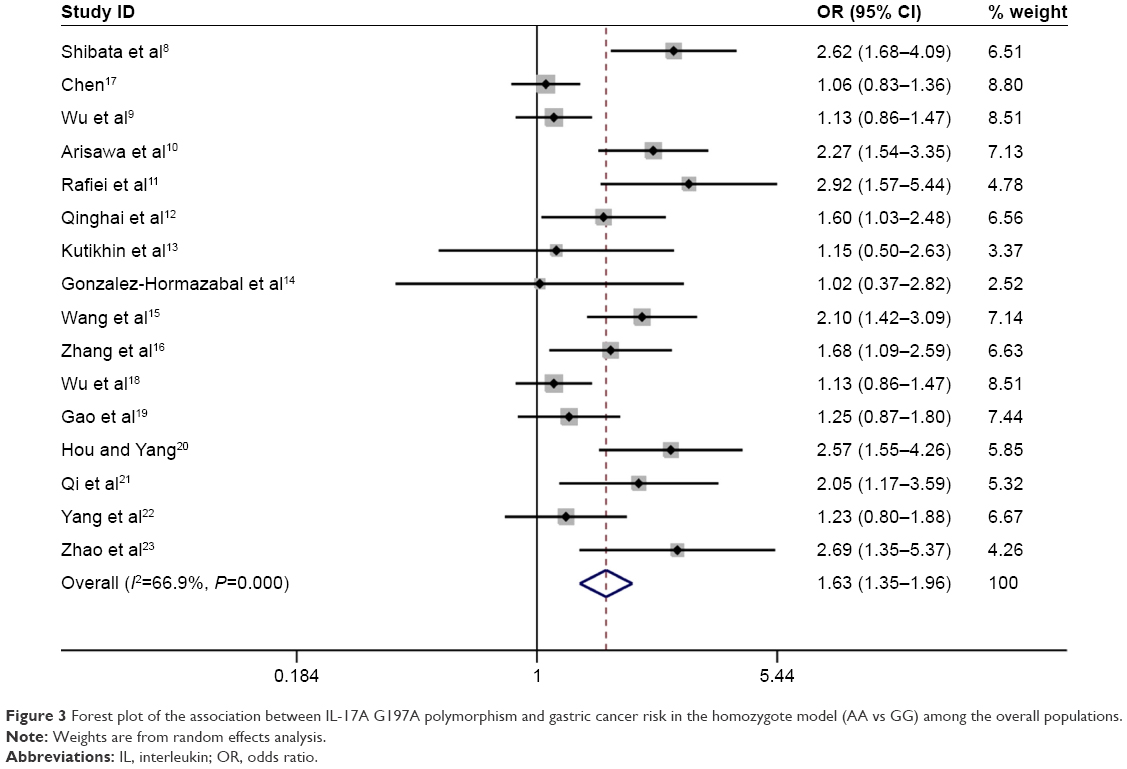 | Figure 3 Forest plot of the association between IL-17A G197A polymorphism and gastric cancer risk in the homozygote model (AA vs GG) among the overall populations. |
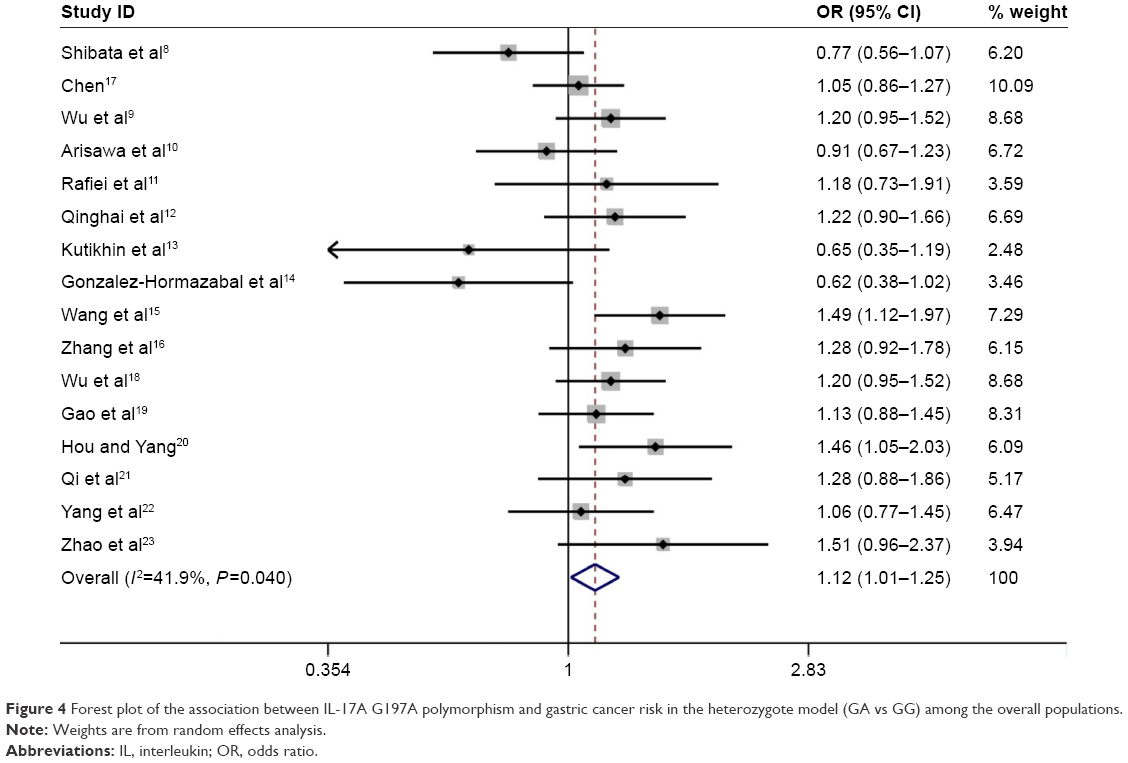 | Figure 4 Forest plot of the association between IL-17A G197A polymorphism and gastric cancer risk in the heterozygote model (GA vs GG) among the overall populations. |
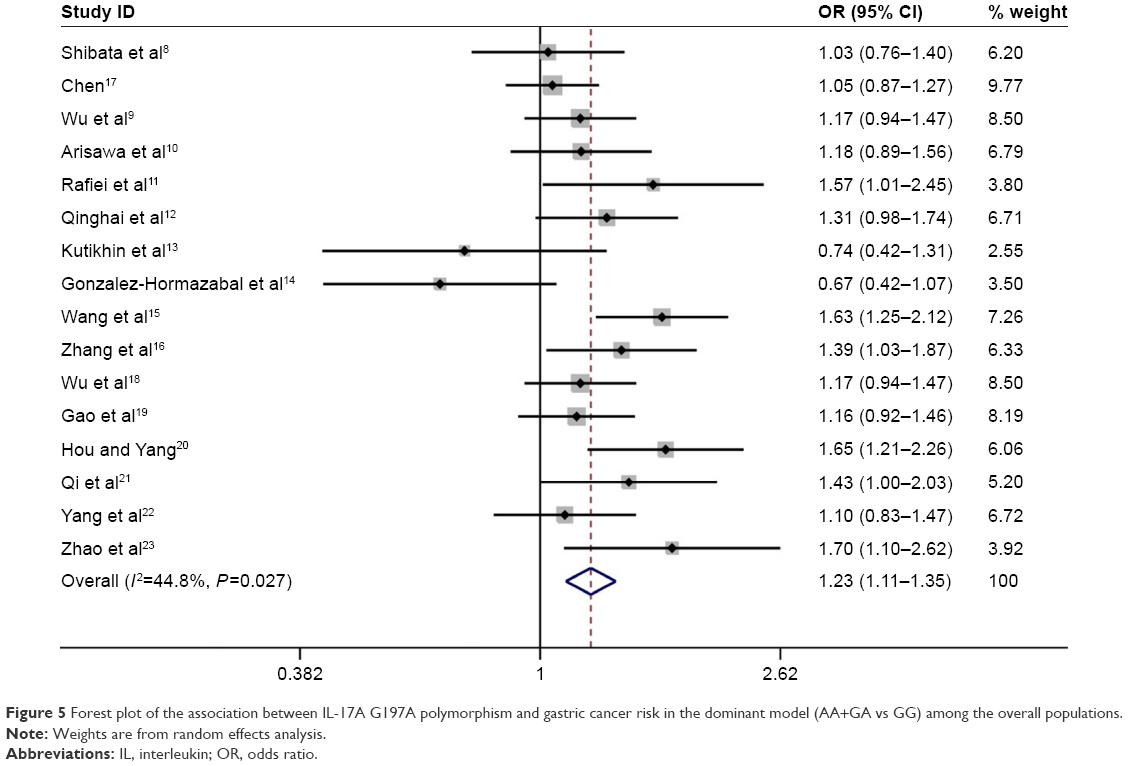 | Figure 5 Forest plot of the association between IL-17A G197A polymorphism and gastric cancer risk in the dominant model (AA+GA vs GG) among the overall populations. |
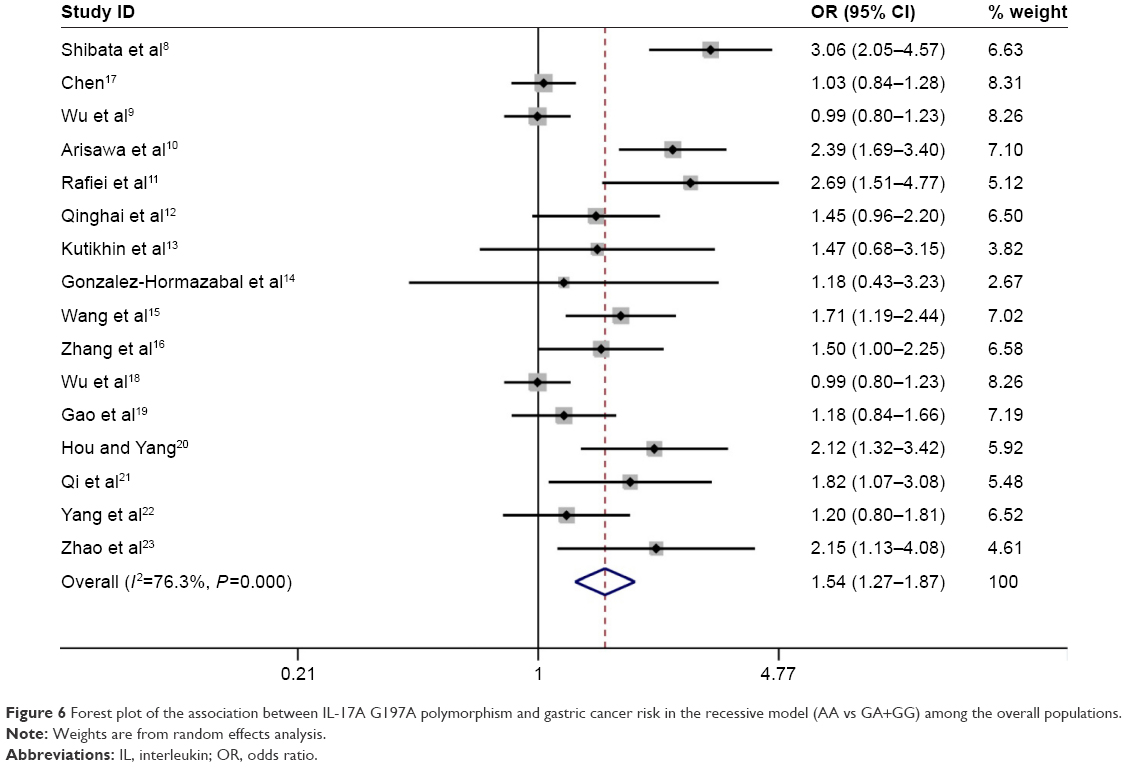 | Figure 6 Forest plot of the association between IL-17A G197A polymorphism and gastric cancer risk in the recessive model (AA vs GA+GG) among the overall populations. |
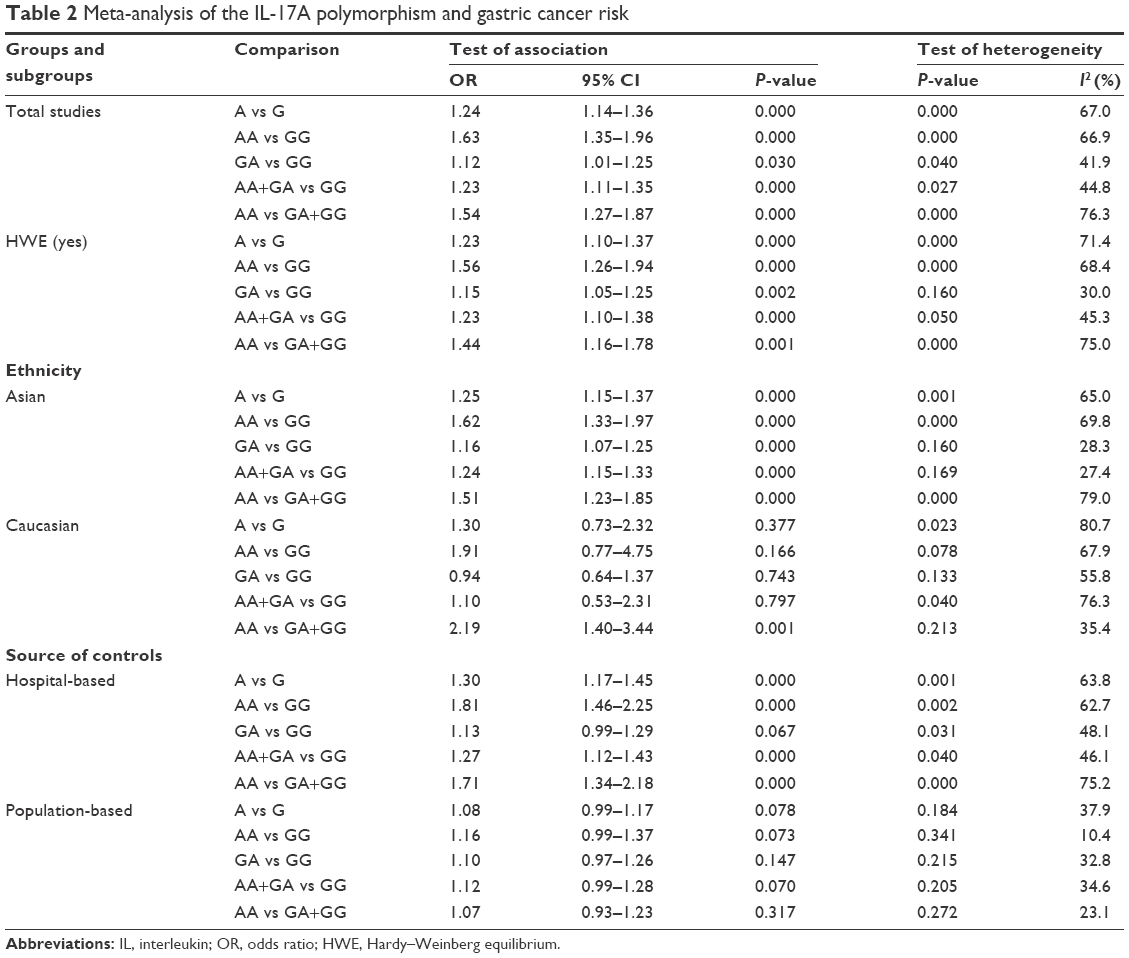 | Table 2 Meta-analysis of the IL-17A polymorphism and gastric cancer risk |
When subgroup analysis was carried out based on ethnicity, significant associations were found in all five genetic models in Asian population (A vs G: OR =1.25, 95% CI =1.15–1.37; AA vs GG: OR =1.62, 95% CI =1.33–1.97; GA vs GG: OR =1.16, 95% CI =1.07–1.25; AA+GA vs GG: OR =1.24, 95% CI =1.15–1.33; AA vs GA+GG: OR =1.51, 95% CI =1.23–1.85), and statistically significant associations were found in the following genetic model in Caucasian population (AA vs GA+GG: OR =2.19, 95% CI =1.40–3.44).
When results were stratified by source of controls, IL-17A G197A polymorphism was associated with a significantly increased gastric cancer risk in the hospital-based controls’ subgroup (A vs G: OR =1.30, 95% CI =1.17–1.45; AA vs GG: OR =1.81, 95% CI =1.46–2.25; AA+GA vs GG: OR =1.27, 95% CI =1.12–1.43; AA vs GA+GG: OR =1.71, 95% CI =1.34–2.18). However, no associations were observed in population-based controls’ subgroup in all five comparison models. All comparisons are listed in Table 2.
Sensitivity analysis and publication bias
Sensitivity analyses showed that omitting an individual study from all the analyses did not affect the pooled ORs significantly and no substantial change was detected, indicating that the overall results of the present study are stable (Figure 7).
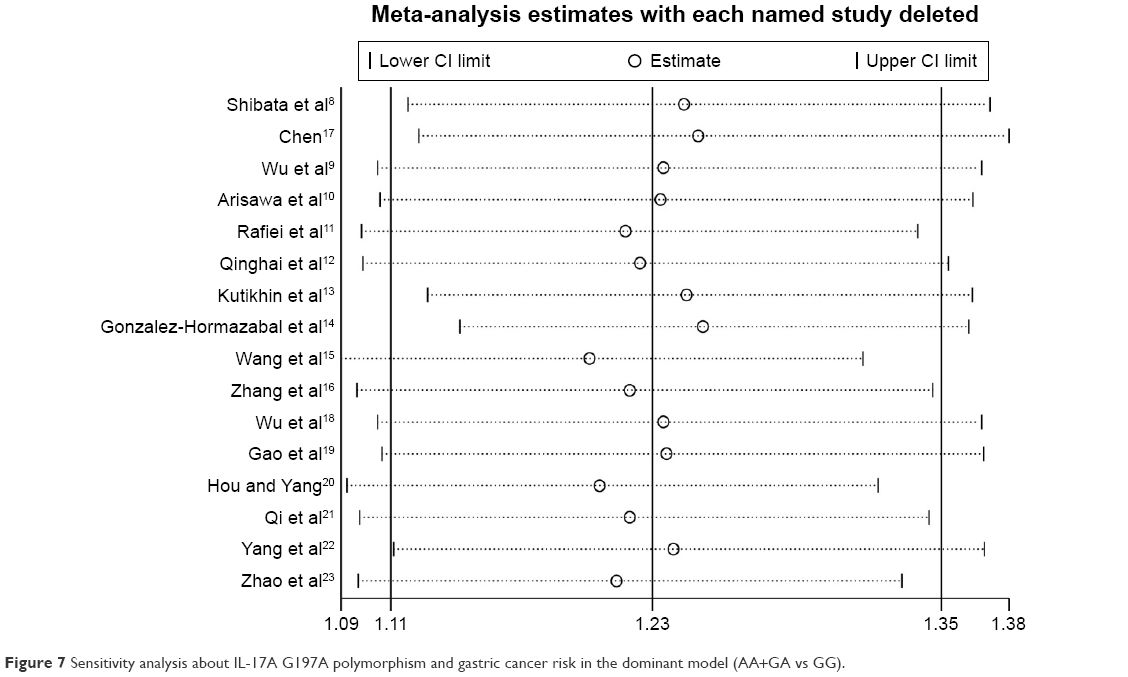 | Figure 7 Sensitivity analysis about IL-17A G197A polymorphism and gastric cancer risk in the dominant model (AA+GA vs GG). |
Begg’s funnel plot was used to assess the publication bias of included literature. The shapes of the funnel plots did not show any evidence of obvious asymmetry, indicating the absence of publication bias (Figure 8).
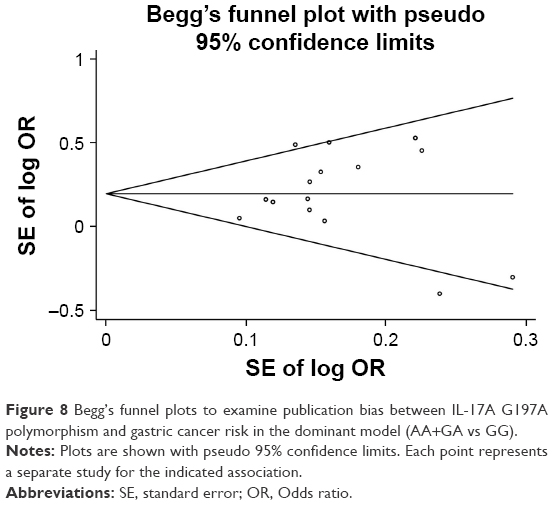 | Figure 8 Begg’s funnel plots to examine publication bias between IL-17A G197A polymorphism and gastric cancer risk in the dominant model (AA+GA vs GG). |
Discussion
Genetic and environmental factors, life style, and Helicobacter pylori infections have been considered as playing essential roles in the development of gastric cancer,30,31 but the precise etiology of the disease remains inconsistent.
IL-17 is a critical inflammatory cytokine that plays an important role in chronic inflammation, autoimmune diseases, and cancer.32 The IL-17A G197A is located in the 5′ region near the IL-17A gene, and it may regulate the gene transcription.33 A previous study has conflicting results about the association between IL-17A G197A polymorphism and gastric cancer risk, which may be because of relatively small sample size and different genetic background.8 Meta-analysis is a powerful method to evaluate gene–disease associations, by collecting all available published studies to obtain more precise results.34
With the development of molecular epidemiology, numerous studies explored the effects of IL-17A G197A polymorphism on gastric cancer susceptibility. In 2014, Yu et al35 carried out a meta-analysis and revealed that the IL-17A G197A polymorphism was associated with a significantly increased gastric cancer risk. In their work, they identified only six case-control studies evaluating the association between the IL-17A G197A polymorphism and gastric cancer risk. In 2015, Li et al24 conducted a meta-analysis to assess the association between IL-17A G197A polymorphism and gastric cancer susceptibility with 11 case-control studies and revealed that IL-17A G197A polymorphism was associated with gastric cancer risk. Therefore, we collected all available published literature and performed an updated meta-analysis of 16 independent case-control studies containing 6,624 cases and 7,631 controls. In the meta-analysis, significant associations between IL-17A G197A polymorphism and gastric cancer risk were observed in all five genetic models. The HWE of each study was taken into consideration. After eliminating studies whose distribution of genotype in controls deviated from HWE, the outcome remained statistically significant. Similar associations were also observed in Asian population (A vs G: OR =1.25, 95% CI =1.15–1.37; AA vs GG: OR =1.62, 95% CI =1.33–1.97; GA vs GG: OR =1.16, 95% CI =1.07–1.25; AA+GA vs GG: OR =1.24, 95% CI =1.15–1.33; AA vs GA+GG: OR =1.51, 95% CI =1.23–1.85), in Caucasian population (AA vs GA+GG: OR =2.19, 95% CI =1.40–3.44), and in the hospital-based controls’ subgroup (A vs G: OR =1.30, 95% CI =1.17–1.45; AA vs GG: OR =1.81, 95% CI =1.46–2.25; AA+GA vs GG: OR =1.27, 95% CI =1.12–1.43; AA vs GA+GG: OR =1.71, 95% CI =1.34–2.18).
Several limitations need to be addressed. First, due to heterogeneity, the results of our meta-analysis should be interpreted. Second, the overall outcomes were based on unadjusted ORs. Lacking the information on detailed individual data limited our more precise analysis on adjusted estimates by other factors like age and sex. This limitation may cause serious confounding bias. Third, meta-analysis is a type of retrospective study, and recall and selection bias may be present.
In conclusion, our meta-analysis revealed that IL-17A G197A polymorphism may increase gastric cancer risk. However, larger studies are still required to assess the interaction of IL-17A G197A polymorphism with gastric cancer risk.
Disclosure
The authors report no conflicts of interest in this work.
References
Kawaguchi M, Adachi M, Oda N, Kokubu F, Huang SK. IL-17 cytokine family. J Allergy Clin Immunol. 2004;114(6):1265–1273; quiz 1274. | ||
Korn T, Bettelli E, Oukka M, Kuchroo VK. IL-17 and Th17 Cells. Annu Rev Immunol. 2009;27:485–517. | ||
Moseley TA, Haudenschild DR, Rose L, Reddi AH. Interleukin-17 family and IL-17 receptors. Cytokine Growth Factor Rev. 2003;14(2):155–174. | ||
Ouyang W, Kolls JK, Zheng Y. The biological functions of T helper 17 cell effector cytokines in inflammation. Immunity. 2008;28(4):454–467. | ||
Steinman L. A brief history of T(H)17, the first major revision in the T(H)1/T(H)2 hypothesis of T cell-mediated tissue damage. Nat Med. 2007;13(2):139–145. | ||
Yang B, Kang H, Fung A, Zhao H, Wang T, Ma D. The role of interleukin 17 in tumour proliferation, angiogenesis, and metastasis. Mediators Inflamm. 2014;2014:623759. | ||
Zou W, Restifo NP. T(H)17 cells in tumour immunity and immunotherapy. Nat Rev Immunol. 2010;10(4):248–256. | ||
Shibata T, Tahara T, Hirata I, Arisawa T. Genetic polymorphism of interleukin-17A and −17F genes in gastric carcinogenesis. Hum Immunol. 2009;70(7):547–551. | ||
Wu X, Zeng Z, Chen B, et al. Association between polymorphisms in interleukin-17A and interleukin-17F genes and risks of gastric cancer. Int J Cancer. 2010;127(1):86–92. | ||
Arisawa T, Tahara T, Shiroeda H, et al. Genetic polymorphisms of IL17A and pri-microRNA-938, targeting IL17A 3′-UTR, influence susceptibility to gastric cancer. Hum Immunol. 2012;73(7):747–752. | ||
Rafiei A, Hosseini V, Janbabai G, et al. Polymorphism in the interleukin-17A promoter contributes to gastric cancer. World J Gastroenterol. 2013;19(34):5693–5699. | ||
Qinghai Z, Yanying W, Yunfang C, Xukui Z, Xiaoqiao Z. Effect of interleukin-17A and interleukin-17F gene polymorphisms on the risk of gastric cancer in a Chinese population. Gene. 2014;537(2):328–332. | ||
Kutikhin AG, Yuzhalin AE, Volkov AN, Zhivotovskiy AS, Brusina EB. Correlation between genetic polymorphisms within IL-1B and TLR4 genes and cancer risk in a Russian population: a case-control study. Tumour Biol. 2014;35(5):4821–4830. | ||
Gonzalez-Hormazabal P, Musleh M, Bustamante M, et al. Role of cytokine gene polymorphisms in gastric cancer risk in Chile. Anticancer Res. 2014;34(7):3523–3530. | ||
Wang N, Yang J, Lu J, et al. IL-17 gene polymorphism is associated with susceptibility to gastric cancer. Tumour Biol. 2014;35(10):10025–10030. | ||
Zhang X, Zheng L, Sun Y, Zhang X. Analysis of the association of interleukin-17 gene polymorphisms with gastric cancer risk and interaction with Helicobacter pylori infection in a Chinese population. Tumour Biol. 2014;35(2):1575–1580. | ||
Chen J. Association Study of Polymorphisms in IL23R and IL17A Genes With the Susceptibility of Gastric Cancer [M.S. thesis]. Nanjing, China: Nanjing Medical University; 2010. | ||
Wu X, Zeng Z, Xu L, et al. Association of interleukin-17 G197A gene polymorphism and interleukin-17 expression with gastric cancer. J Pract Med. 2014;30(1):246–249. | ||
Gao YW, Xu M, Xu Y, Li D, Zhou S. Effect of three common IL-17 single nucleotide polymorphisms on the risk of developing gastric cancer. Oncol Lett. 2015;9(3):1398–1402. | ||
Hou C, Yang F. Interleukin-17A gene polymorphism is associated with susceptibility to gastric cancer. Int J Clin Exp Pathol. 2015;8(6):7378–7384. | ||
Qi WT, Gao JL, Zhang SS. Role of IL-17 gene polymorphisms in the susceptibility to gastric cancer. Genet Mol Res. 2015;14(4):13364–13369. | ||
Yang LJ, Gao W, Bai JY, et al. Correlation between Interleukin-17 gene polymorphism and gastric cancer susceptibility in Han Chinese population. Eur Rev Med Pharmacol Sci. 2016;20(7):1271–1282. | ||
Zhao WM, Shayimu P, Liu L, Fang F, Huang XL. Association between IL-17A and IL-17F gene polymorphisms and risk of gastric cancer in a Chinese population. Genet Mol Res. 2016;15(3). | ||
Li XF, Shen M, Cai JW, et al. Association of interleukin-17 gene polymorphisms and Helicobacter pylori infection with gastric cancer susceptibility: a cumulative and comprehensive meta-analysis. Int J Clin Exp Med. 2015;8(10):17623–17633. | ||
Haber M. Exact significance levels of goodness-of-fit tests for the Hardy-Weinberg equilibrium. Hum Hered. 1981;31(3):161–166. | ||
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. | ||
Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22(4):719–748. | ||
Der Simonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188. | ||
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. | ||
Dong LM, Potter JD, White E, Ulrich CM, Cardon LR, Peters U. Genetic susceptibility to cancer: the role of polymorphisms in candidate genes. JAMA. 2008;299(20):2423–2436. | ||
Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol. 2006;12(3):354–362. | ||
Song X, Qian Y. IL-17 family cytokines mediated signaling in the pathogenesis of inflammatory diseases. Cell Signal. 2013;25(12):2335–2347. | ||
Liu XK, Lin X, Gaffen SL. Crucial role for nuclear factor of activated T cells in T cell receptor-mediated regulation of human interleukin-17. J Biol Chem. 2004;279(50):52762–52771. | ||
Ntais C, Polycarpou A, Ioannidis JP. Meta-analysis of the association of the cathepsin D Ala224Val gene polymorphism with the risk of Alzheimer’s disease: a HuGE gene-disease association review. Am J Epidemiol. 2004;159(6):527–536. | ||
Yu H, Sun S, Liu F, Xu QH. Meta-analysis of associations between interleukin-17 gene polymorphisms and risk of gastric cancer. Asian Pac J Cancer Prev. 214;15(20):8709–8713. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.